Balancing the Scales: Patient Load vs. Care Quality in Diabetes
ISPAD is the International Society for Pediatric and Adolescent Diabetes, the society has released consensus for linical Practice Consensus Guidelines 2024 – Type 1 Diabetes Focus (Ch. 2 Screening & Staging, Ch. 8 Glycemic Targets, Ch. 9 Insulin & Adjunctive Treatments, Ch. 16 & 17 Diabetes Technologies)
Published Date:
Dec 11, 2024
Published By:
Michael J Haller, Martin de Bock, Eda Cengiz, Torben Biester, Martin Tauschmann and colleagues, on behalf of the International Society for Pediatric and Adolescent Diabetes (ISPAD)
Approved By:
To be
Decoded By:
Asra H. Ahmed (MBA, PGCE in Assessment Learning disability) & Devanagana Thakuria from The Diabesties Foundation.
10 mins to read
- The T1D Takeaway
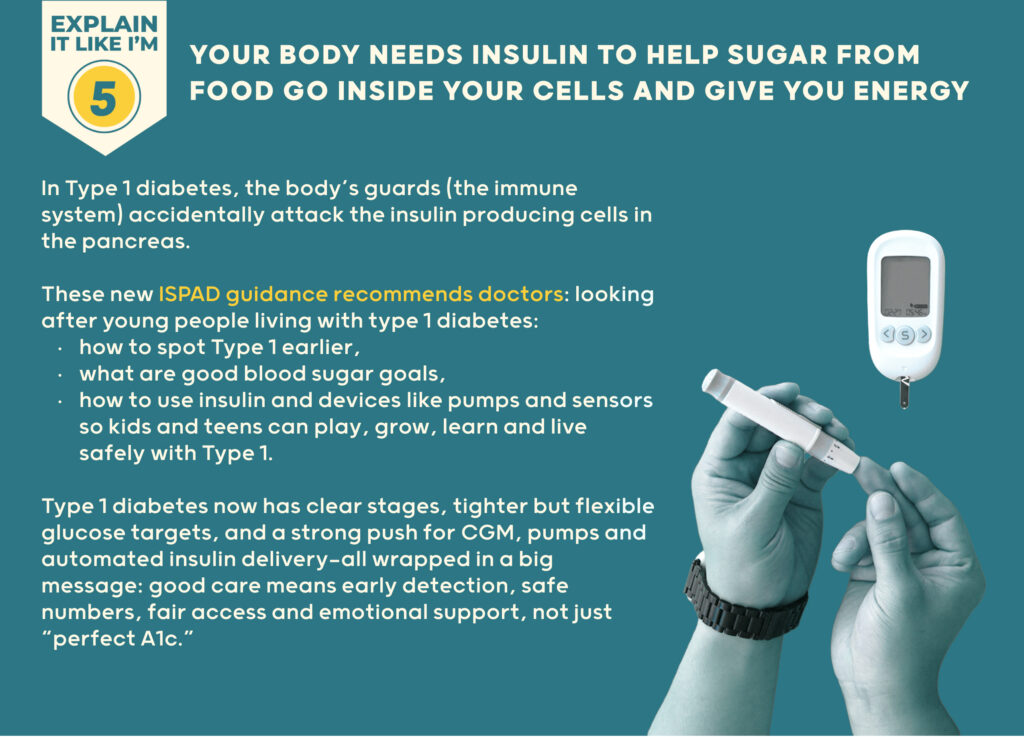
- Type 1 diabetes now has clear stages, tighter but flexible glucose targets, and a strong push for CGM, pumps and automated insulin delivery—all wrapped in a big message: good care means early detection, safe numbers, fair access and emotional support, not just “perfect A1c.”
Word Wizard
- ISPAD 2024 explains that Type 1 diabetes often begins years before symptoms, and that finding two or more islet autoantibodies means early Type 1, where good screening plus education can reduce DKA at diagnosis and, in some settings, allow immune therapy like teplizumab to delay the move to full clinical diabetes.
- Care is centered on basal–bolus insulin (by injections or pump), and premixed insulin is no longer preferred for children. CGM, insulin pumps and automated insulin delivery (AID) are treated as essential tools that reliably improve time in range and reduce severe lows and DKA, not as optional “nice extras.”
- Glycemic targets are firmer but still humane: an A1c around 5–7.0% is encouraged for many children and teens, but only if this can be achieved safely, without increasing severe hypoglycemia or harming mental health.
- Across all of this runs a clear message on equity: gaps in access to insulin, glucose strips, CGM, pumps and new drugs are framed as a matter of fairness and justice rather than individual effort, and closing these gaps is described as a core part of good Type 1 care.

Summary Snap
Shots
ISPAD 2024 reframes Type 1 diabetes in kids and teens as a staged, life-long condition that can be detected earlier, treated more precisely and supported more fairly. It pulls together evidence for staging with autoantibodies, realistic HbA1c/TIR goals, modern insulin options, and diabetes tech (CGM, pumps, AID), while repeatedly stressing that emotional health and access matter as much as numbers
Prime Insight
ISPAD is the main global expert group for diabetes care in children and teenagers. Their guidelines are evidence-based “how to” instructions that show doctors what good care should look like—how Type 1 (and other diabetes types in young people) should be diagnosed, treated, and supported.
T1D is framed as a staged condition:
Screening, staging & preserving beta-cell function is an integral part of the consensus paper.
Stage 1: 2 or more islet autoantibodies, normal glucose.
Stage 2: 2 or more autoantibodies + blood sugars that are starting to look off, even if they’re not in the full diabetes range yet.
Stage 3: Clinical Type 1 diabetes means the blood tests are now clearly in the diabetes range.
Sometimes there are no obvious symptoms yet (Stage 3a), and sometimes there are the classic signs (Stage 3b) like a lot of thirst, peeing all the time, losing weight, and feeling very tired.
Stage 4: Long-standing T1D.
Having two or more autoantibodies is not “borderline” – it is early (pre-symptomatic) Type 1, with very high lifetime risk of progressing to Stage 3.
Screening can be family-based or general population. When it includes education and structured follow-up, it:
- Reduces DKA at diagnosis.
- Allows families to prepare emotionally and practically.
- Creates space to discuss immune therapies like teplizumab in Stage 2 where available.
Glycemic targets & glucose monitoring –
Those living with type 1 diabetes and use a CGM or an AID system it is recommended:
It’s okay to aim a bit lower – an HbA1c around 6.5% or less, if you can do it safely and it doesn’t make life too stressful.
However, for children and teens not on an AID system it is recommended: A good, realistic goal is anHbA1c around 7.0% or less, with room to adjust based on age, support, and mental health.
We don’t look at HbA1c alone anymore:
- We also look at Time in Range (TIR) – the percent of time your glucose is between 70–180 mg/dL (3.9–10 mmol/L).
- When you’re using CGM, HbA1c + TIR together tell a more complete story, rather than using data point on its own.
Targets are recommended to be personalized based on hypoglycemia risk, mental health, access to tech, and family capacity.
ISPAD consensus pointers agree better early management leads to long-term outcomes. Earlier, safer tightening of glucose (A1c closer to 6.5–7%)lower rates of eye and kidney disease decades later, in line with DCCT-style data, On monitoring: CGM is treated as standard of care where available, improving A1c, TIR, severe hypoglycemia and DKA rates.
ISPAD says clearly that these guidelines are meant to lighten the load, improve quality of life, and be free for everyone to read around the world, in many languages (ispad.org).
So, this isn’t just “another medical document” – it’s a global playbook for young people with diabetes, designed to be clear, visual, science-based and inclusive, so more families, HCPs and advocates can use it in real life.
it’s a global playbook for young people with diabetes, designed to be clear, visual, science-based and inclusive, so more families, HCPs and advocates can use it in real life.
Insulin & adjunctive therapies
Basal–bolus therapy (MDI or pump) is the standard of care for youth with T1D.
Premixed insulin twice daily is not preferred for children. The consensus paper recommends the use of faster-acting mealtime analogues. Ultra-long basal insulins and how to dose them.
ISPAD gives clear guidance on “extra” diabetes medicines (like pramlintide, metformin, GLP-1 medicines and SGLT tablets):
- They are sometimes added to insulin in older teens, usually when there is extra weight, or very high insulin doses, and only when the benefits and risks are carefully discussed.
- Massive emphasis: these medicines are add-ons to insulin, never replacements.
- The chapter also has a strong access and affordability section. It explicitly calls for health systems and governments to ensure insulin is available without financial hardship, especially in low- and middle-income settings.
Diabetes technologies – insulin delivery & glucose monitoring –
Pump and AID chapter summarizes advances since 2022. There is lots of practical “how-to” within the consensus statement:
- Infusion-set management and lipo-hypertrophy.
- Dealing with alarm fatigue, sensor errors, skin reactions.
- Choosing tech based on age, developmental stage, and family preference.
- Strong equity language – the chapter and editorial both highlight disparities in tech access and call for closing these gaps.
- A Deeper Dive
- “ISPAD’s Clinical Practice Consensus Guidelines are the only comprehensive set of clinical recommendations for children, adolescents, and young adults with diabetes worldwide.”
- The American Diabetes Association (ADA) describes a consensus report as a comprehensive examination by an expert panel that turns complex science into practical recommendations for clinical care.
- The Sources Voice
“ISPAD’s Clinical Practice Consensus Guidelines are the only comprehensive set of clinical recommendations for children, adolescents, and young adults with diabetes worldwide!”
- Curiosities Clarified
Families and HCPs often follow different rules for the same child (screening, targets, pumps, etc.) ISPAD solution: A shared global playbook so everyone works from the same map for children and teens with diabetes.
Consensus papers distil hundreds of studies into clear, practical guidance on staging, insulin, targets, CGM, pumps, etc., so clinics and families aren’t guessing.
The guidelines tie numbers to quality of life, mental health and Time in Range, making care more human, not just mathematical.
Consensus papers call out equity and psychosocial care as essential, giving HCPs and advocates a strong evidence-based “backbone” to demand better systems, not just more effort from families.
5330 Comments
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah detail kontak Anda?
Postingan ini sangat berguna. Saya sangat menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
You really make it seem really easy with your presentation but I in finding this topic to be really something that I feel I might never understand. It kind of feels too complicated and extremely broad for me. I’m looking ahead in your next submit, I’ll try to get the grasp of it!
Hey, I think your website might be having browser compatibility issues. When I look at your blog in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, excellent blog!
Good day! This is my 1st comment here so I just wanted to give a quick shout out and say I truly enjoy reading through your posts. Can you recommend any other blogs/websites/forums that cover the same topics? Thanks for your time!
Yeah bookmaking this wasn’t a high risk determination great post! .
I really appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Seseorang pada dasarnya membantu membuat artikel yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Pekerjaan yang mengagumkan!
Terima kasih banyak atas artikel yang luar biasa. Saya sungguh menyukai membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan kerja yang hebat!
Meski begitu, terima kasih untuk poin yang menonjol ini dan meskipun saya tidak benar-benar sepakat sepenuhnya, saya menghormati pandangan.
I enjoy studying and I believe this website got some really utilitarian stuff on it! .
I think you have remarked some very interesting details, thankyou for the post.
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali evaluasi tentang ini. Dan dia sebenarnya membeli saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda berkembang menjadi lebih ahli, apakah Anda berkenan memperbarui blog Anda dengan tambahan rincian? Ini sangat berguna bagi saya. Jempol besar untuk posting blog ini!
Saya senang menjadi pengunjung dari situs total ini!, terima kasih atas informasi langka ini!
Tetap saja, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak sepakat sepenuhnya, saya menghargai perspektif.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu baik. Bye
Thanks for another great article. Where else could anybody get that kind of information in such a perfect way of writing? I’ve a presentation next week, and I’m on the look for such information.
Kami dapat memiliki hyperlink pertukaran perjanjian antara kita!
What’s Taking place i am new to this, I stumbled upon this I have discovered It positively useful and it has aided me out loads. I’m hoping to contribute & aid different customers like its helped me. Good job.
It’s a pity you don’t have a donate button! I’d without a doubt donate to this excellent blog! I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account. I look forward to fresh updates and will talk about this blog with my Facebook group. Chat soon!
I like this weblog so much, saved to my bookmarks. “American soldiers must be turned into lambs and eating them is tolerated.” by Muammar Qaddafi.
You are my breathing in, I own few web logs and occasionally run out from to post : (.
Hi, I think your website might be having browser compatibility issues. When I look at your blog in Chrome, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, great blog!
You have observed very interesting details! ps decent internet site. “The appearance of right oft leads us wrong.” by Horace.
Your comment is awaiting moderation.
Good afternoon,
Friends.
At the moment I would like to tell a little about digital marketing agency
I think you thinking specifically about digital marketing company or
perhaps you desire to learn more about digital
marketing in Australia?!
So this optimally up-to-date information about digital marketing
in Australia will be the most useful for you.
On our site a little more about digital marketing in Australia, also
information about Australia digital marketing agency.
more about digital marketing in Australia at https://wiki.throngtalk.com/index.php?title=User:ClarissaSherriff
Our Tags: Digital marketing in Australia, digital marketing company, digital marketing company, Australia digital marketing agency,
digital marketing in Australia, digital marketing company, digital marketing agency in Australia, digital
marketing agency, digital marketing company
Have a good day http://ssjcompanyinc.official.jp/bbs/board.php?bo_table=free&wr_id=9242790
Howdy! Someone in my Facebook group shared this site with us so I came to look it over. I’m definitely loving the information. I’m bookmarking and will be tweeting this to my followers! Excellent blog and brilliant style and design.
Nice post. I learn something more challenging on different blogs everyday. It will always be stimulating to read content from other writers and practice a little something from their store. I’d prefer to use some with the content on my blog whether you don’t mind. Natually I’ll give you a link on your web blog. Thanks for sharing.
I have learn some good stuff here. Definitely value bookmarking for revisiting. I wonder how a lot effort you set to make one of these fantastic informative website.
I’d should check with you here. Which is not one thing I usually do! I take pleasure in studying a post that will make folks think. Also, thanks for permitting me to remark!
Greetings! Quick question that’s totally off topic. Do you know how to make your site mobile friendly? My weblog looks weird when browsing from my iphone. I’m trying to find a theme or plugin that might be able to correct this issue. If you have any recommendations, please share. Cheers!
Howdy! This is my 1st comment here so I just wanted to give a quick shout out and say I really enjoy reading your blog posts. Can you recommend any other blogs/websites/forums that deal with the same topics? Many thanks!
Hey! I’m at work browsing your blog from my new apple iphone! Just wanted to say I love reading through your blog and look forward to all your posts! Carry on the outstanding work!
What i don’t realize is in reality how you are not really much more neatly-preferred than you might be right now. You’re very intelligent. You already know therefore significantly on the subject of this subject, produced me for my part imagine it from so many varied angles. Its like women and men aren’t interested unless it is one thing to do with Girl gaga! Your personal stuffs nice. At all times deal with it up!
I love the efforts you have put in this, thanks for all the great posts.
I saw a lot of website but I believe this one has got something special in it in it
Do you mind if I quote a couple of your posts as long as I provide credit and sources back to your blog? My blog is in the exact same area of interest as yours and my users would genuinely benefit from a lot of the information you present here. Please let me know if this ok with you. Appreciate it!
Some genuinely interesting points you have written.Helped me a lot, just what I was searching for :D.
Greetings! Very helpful advice on this article! It is the little changes that make the biggest changes. Thanks a lot for sharing!
Thank you for sharing superb informations. Your web-site is very cool. I am impressed by the details that you have on this web site. It reveals how nicely you understand this subject. Bookmarked this web page, will come back for extra articles. You, my pal, ROCK! I found simply the info I already searched all over the place and simply could not come across. What a perfect web-site.
I’m curious to find out what blog platform you happen to be using? I’m experiencing some minor security problems with my latest blog and I’d like to find something more secure. Do you have any suggestions?
Very interesting information!Perfect just what I was looking for!
Some truly fantastic info , Sword lily I found this.
I gotta bookmark this internet site it seems handy extremely helpful
Terima kasih atas tulisan yang baik. Pada kenyataannya ini dulunya adalah sebuah materi hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat tetap berhubungan?
Terima kasih untuk blog informatif lainnya. Di mana lagi saya bisa mendapatkan informasi seperti itu yang ditulis dengan pendekatan yang sempurna? Saya punya sebuah tantangan yang saya sedang jalankan, dan saya sudah mencari informasi seperti ini.
Excellent beat ! I would like to apprentice while you amend your website, how could i subscribe for a blog website? The account helped me a appropriate deal. I were a little bit familiar of this your broadcast provided vivid clear idea
Saya senang menjadi salah satu dari banyak pengunjung di situs luar biasa ini (:, salam telah mengunggah.
Bernilai info. Beruntung saya menemukan situs web Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada cara Anda dapat menghapus saya dari layanan itu? Terima kasih!
Some truly wonderful content on this site, regards for contribution.
I dugg some of you post as I cerebrated they were handy invaluable
Perfectly pent articles, appreciate it for entropy. “The last time I saw him he was walking down Lover’s Lane holding his own hand.” by Fred Allen.
Some genuinely nice stuff on this site, I like it.
I believe that is among the most significant info for me. And i am satisfied studying your article. However wanna statement on few basic things, The web site taste is great, the articles is actually great :D. Good process, cheers
Saya selamanya memikirkan hal ini, terima kasih telah memposting.
Menikmati menelaah ini, sangat bagus, salam.
Ini adalah topik yang sangat dekat di hati saya, cheers, tapi di manakah informasi kontak Anda?
Hiya very cool website!! Guy .. Beautiful .. Superb .. I will bookmark your site and take the feeds additionallyKI’m glad to seek out a lot of useful information here in the post, we’d like work out extra strategies on this regard, thank you for sharing. . . . . .
Situs web ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Hello, you used to write wonderful, but the last several posts have been kinda boring… I miss your super writings. Past few posts are just a little bit out of track! come on!
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me. Anyways, I’m definitely happy I found it and I’ll be book-marking and checking back frequently!
Just what I was searching for, thankyou for posting.
Great write-up, I’m normal visitor of one’s site, maintain up the excellent operate, and It’s going to be a regular visitor for a lengthy time.
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang luar biasa!
Outstanding post however , I was wanting to know if you could write a litte more on this topic? I’d be very grateful if you could elaborate a little bit further. Many thanks!
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan berterima kasih kepada Anda.
Terima kasih untuk artikel fantastis tambahan. Di tempat mana lagi siapa pun dapat mendapatkan jenis info seperti itu dengan pendekatan penulisan yang sempurna? Saya memiliki presentasi minggu depan, dan saya berada mencari informasi seperti ini.
Konten yang fantastis! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
Whats up this is kinda of off topic but I was wanting to know if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding knowledge so I wanted to get advice from someone with experience. Any help would be enormously appreciated!
Terima kasih banyak atas posting yang sangat baik. Saya sungguh menikmati membaca ini dan menemukan banyak wawasan yang berguna. Teruskan kerja yang bagus!
For property managers, the fastest safe solution depends on whether
the problem is a lost key, failed latch, damaged cylinder or door alignment issue.
It also gives the local professional better information before arrival.
Aku benar-benar ingin mengirim komentar singkat untuk menghargai Anda atas semua tips luar biasa yang Anda bagikan di website ini.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Berharga info. Beruntung saya menemukan situs Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menandainya.
I have been surfing online more than three hours lately, yet I never discovered any interesting article like yours. It is pretty price sufficient for me. Personally, if all site owners and bloggers made good content material as you probably did, the web shall be much more helpful than ever before.
Postingan yang luar biasa. Ini memberikan saya gambaran yang lebih jelas tentang topik ini. Teruskan pekerjaan yang hebat!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Hello, you used to write wonderful, but the last several posts have been kinda boringK I miss your super writings. Past few posts are just a little out of track! come on!
I like this weblog so much, saved to my bookmarks. “Respect for the fragility and importance of an individual life is still the mark of an educated man.” by Norman Cousins.
Situs web ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Ini adalah blog yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Saya menghargai usaha yang Anda curahkan untuk membuat artikel ini. Konten yang bernilai. Terima kasih!
Konten yang berguna. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
I used to be very happy to seek out this web-site.I wished to thanks on your time for this wonderful learn!! I definitely enjoying each little little bit of it and I’ve you bookmarked to check out new stuff you weblog post.
Hore google adalah raja saya yang menolong saya menemukan web site yang luar biasa! .
Artikel yang luar biasa. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Sangat menarik poin yang Anda sebutkan, terima kasih telah mengunggah. “Tidak ada apa pun dalam seekor ulat yang memberi tahu Anda bahwa ia akan menjadi kupu-kupu.” oleh Richard Buckminster Fuller.
Saya beruntung bahwa saya mengamati blog ini, benar-benar info yang saya cari!
Some genuinely great info , Gladiola I noticed this. “Now hatred is by far the longest pleasure men love in haste but they detest at leisure.” by George Gordon Byron.
Konten yang berguna dan ditulis dengan sangat baik. Saya tentu akan membagikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Saya tidak sungguh hebat dalam bahasa Inggris tetapi saya menemukan ini benar-benar ringan untuk ditafsirkan.
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
Postingan yang hebat. Ini memberi saya pemahaman yang lebih baik tentang topik ini. Teruskan kerja yang hebat!
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Wow! Terima kasih! Saya senantiasa ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke situs saya?
Hore google adalah ratu saya yang menolong saya menemukan web site yang luar biasa! .
Saya tidak sering berkomentar tetapi saya harus menyatakan salam untuk posting yang sempurna ini : D.
Hi there, I found your web site via Google while looking for a related topic, your web site came up, it looks great. I’ve bookmarked it in my google bookmarks.
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
Hmm apakah ada orang lain yang mengalami masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Saya terkesan dengan website ini, sungguh saya adalah penggemar.
Excellent beat ! I wish to apprentice at the same time as you amend your website, how could i subscribe for a blog site? The account helped me a acceptable deal. I have been tiny bit acquainted of this your broadcast offered vivid clear idea
Perfectly written content, Really enjoyed looking at.
I’d must check with you here. Which is not one thing I normally do! I take pleasure in studying a put up that may make people think. Also, thanks for allowing me to remark!
Good blog! I really love how it is simple on my eyes and the data are well written. I am wondering how I might be notified whenever a new post has been made. I have subscribed to your feed which must do the trick! Have a great day!
I gotta favorite this web site it seems extremely helpful handy
Good write-up, I’m regular visitor of one’s website, maintain up the nice operate, and It is going to be a regular visitor for a lengthy time.
I got good info from your blog
Valuable info. Lucky me I found your website by accident, and I’m shocked why this accident did not happened earlier! I bookmarked it.
It’s actually a nice and helpful piece of information. I am glad that you shared this helpful info with us. Please keep us informed like this. Thanks for sharing.
I’d must examine with you here. Which isn’t something I usually do! I get pleasure from reading a put up that will make individuals think. Additionally, thanks for permitting me to remark!
My spouse and i ended up being so more than happy Chris could carry out his survey through the precious recommendations he got through your site. It’s not at all simplistic to simply choose to be releasing techniques which usually many others have been selling. We really take into account we’ve got the blog owner to be grateful to for that. All of the illustrations you made, the simple site navigation, the relationships your site make it possible to promote – it’s got all powerful, and it’s aiding our son and our family imagine that the concept is entertaining, and that is extremely indispensable. Many thanks for all the pieces!
Saya tanpa henti memikirkan hal ini, terimakasih telah memposting.
Bagaimanapun, terima kasih untuk artikel yang fantastis ini dan walaupun saya tidak benar-benar sepakat sepenuhnya, saya menghormati pandangan.
Saya selalu tertarik dengan subjek ini dan tetap masih demikian, terima kasih telah memposting.
I blog frequently and I really appreciate your information. This article has really peaked my
interest. I am going to bookmark your site and keep checking for new details about once per week.
I subscribed to your RSS feed too.
Saya senang menjadi salah satu dari banyak pengunjung di website luar biasa ini (:, sangat dihargai telah mengunggah.
Saya selalu tertarik dengan topik ini dan masih demikian, salam telah memposting.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Benar-benar baik informasi dapat ditemukan di weblog.
Isi yang fantastis! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
Hei, saya sekadar ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini merupakan persis tipe informasi yang saya cari. Saya akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
Saya selalu peduli dengan topik ini dan masih demikian, salam telah memposting.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas akan bersyukur kepada Anda.
Sangat menarik poin yang Anda amati, salam telah memposting. “Jangan pernah menyebut akuntan sebagai kebanggaan profesinya; akuntan yang baik adalah debit bagi profesinya.” oleh Charles J. C. Lyall.
Saya tidak sering berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang sempurna ini : D.
Wow! Ini mungkin salah satu blog paling membantu yang pernah kami temui tentang topik ini. Sebenarnya Luar biasa. Saya juga seorang ahli dalam topik ini jadi saya dapat memahami kerja keras Anda.
Hi there just wanted to give you a quick heads up. The words in your content seem to be running off the screen in Opera. I’m not sure if this is a formatting issue or something to do with browser compatibility but I thought I’d post to let you know. The design and style look great though! Hope you get the problem resolved soon. Cheers
Saya sangat menghargai usaha yang Anda luangkan untuk menyusun artikel ini. Konten yang bernilai. Terima kasih!
Bagaimanapun, terima kasih untuk artikel yang luar biasa ini dan meskipun saya tidak sepakat sepenuhnya, saya menghargai perspektif.
Ya menyimpan ini bukanlah kesimpulan yang berisiko pos yang luar biasa! .
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Amat indah informasi dapat ditemukan di web site.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Hey very nice blog!! Man .. Beautiful .. Superb .. I will bookmark your web site and take the feeds additionally…I am glad to find a lot of useful information here within the submit, we want develop more strategies on this regard, thank you for sharing.
Hore google adalah ratu saya yang membantu saya menemukan situs yang hebat! .
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
you could have a great blog here! would you like to make some invite posts on my blog?
Saya tidak benar-benar luar biasa dalam bahasa Inggris tetapi saya memperoleh ini sungguh mudah untuk ditafsirkan.
Saya selalu peduli dengan subjek ini dan masih demikian, salam telah mengunggah.
Wow! Terima kasih! Saya selalu ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menerapkan fragmen dari posting Anda ke blog saya?
Saya senang menjadi pengunjung dari web blog murni ini!, salam atas info langka ini!
of course like your website however you have to test the spelling on several of your posts. Several of them are rife with spelling problems and I find it very troublesome to tell the truth however I will surely come again again.
Mengagumi komitmen yang Anda curahkan ke blog Anda dan informasi terperinci yang Anda berikan. Sangat baik menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Hei, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah persis jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi megah dibagikan secara bebas.
I have learn some excellent stuff here. Definitely value bookmarking for revisiting. I wonder how a lot effort you put to make any such magnificent informative site.
Informasi yang sangat berguna. Saya baru saja mencari hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
Saya melihat banyak website tetapi saya pikir yang satu ini memiliki sesuatu yang ekstra di dalamnya
I was very pleased to seek out this web-site.I wanted to thanks in your time for this glorious read!! I undoubtedly having fun with each little little bit of it and I’ve you bookmarked to take a look at new stuff you blog post.
Hey! Would you mind if I share your blog with my zynga group? There’s a lot of people that I think would really enjoy your content. Please let me know. Thank you
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Saya secara tidak sengaja menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang bagus.
Saya senang menjadi salah satu dari beberapa pengunjung di situs luar biasa ini (:, salam telah mengunggah.
Ini adalah topik yang sangat penting di hati saya, cheers, tapi di mana detail kontak Anda?
Amat indah informasi dapat ditemukan di website.
Saya tidak biasanya berkomentar tetapi saya harus menyatakan terima kasih untuk posting yang spesial ini : D.
Berharga info. Beruntung saya menemukan website Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menyimpannya.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Pekerjaan yang fantastis!
Bagian yang kuat, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali evaluasi tentang ini. Dan dia sesungguhnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika memungkinkan, seiring Anda berkembang menjadi lebih ahli, apakah Anda berkenan memperbarui weblog Anda dengan lebih banyak detail? Ini sangat berguna bagi saya. Jempol besar untuk publikasi weblog ini!
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan daerah kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya benar-benar senang melihat informasi fantastis dibagikan secara bebas.
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Semua ide bagus yang pernah saya miliki datang kepada saya saat saya memerah sapi.” oleh Grant Wood.
Great post and straight to the point. I am not sure if this is in fact the best place to ask but do you guys have any thoughts on where to get some professional writers? Thanks 🙂
Wow, fantastic blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your web site is magnificent, as well as the content!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
I don’t ordinarily comment but I gotta state appreciate it for the post on this amazing one :D.
Saya tidak biasanya berkomentar tetapi saya harus mengakui terimakasih untuk posting yang luar biasa ini : D.
Halo di sana, kamu sudah melakukan pekerjaan yang hebat. Saya tentu akan menyimpan ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Hi my friend! I want to say that this article is amazing, great written and include approximately all significant infos. I would like to peer extra posts like this .
I have been exploring for a little bit for any high quality articles or blog posts in this sort of space . Exploring in Yahoo I at last stumbled upon this site. Reading this info So i’m happy to show that I’ve an incredibly just right uncanny feeling I discovered just what I needed. I most indisputably will make certain to do not fail to remember this site and give it a look regularly.
Regards for all your efforts that you have put in this. very interesting information.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Thanks for every other informative website. The place else may just I am getting that kind of information written in such a perfect way? I’ve a undertaking that I am just now working on, and I have been on the glance out for such info.
Terima kasih untuk posting fantastis tambahan. Di mana lagi siapa pun mungkin bisa mendapatkan jenis informasi seperti itu dengan cara penulisan yang ideal? Saya memiliki presentasi minggu berikutnya, dan saya sedang mencari informasi seperti ini.
Terima kasih, saya baru saja mencari informasi tentang topik ini dalam waktu yang panjang dan milik Anda adalah yang paling hebat yang saya temukan hingga sekarang. Namun, bagaimana dengan kesimpulan? Apakah Anda positif tentang asal tersebut?
I like the valuable information you provide in your articles. I’ll bookmark your blog and check again here regularly. I am quite certain I’ll learn lots of new stuff right here! Good luck for the next!
There are definitely a variety of particulars like that to take into consideration. That is a great level to carry up. I offer the ideas above as common inspiration but clearly there are questions just like the one you convey up where a very powerful factor can be working in trustworthy good faith. I don?t know if finest practices have emerged around things like that, however I’m certain that your job is clearly identified as a good game. Both girls and boys feel the affect of just a moment’s pleasure, for the remainder of their lives.
I was suggested this website by my cousin. I’m not sure whether this post is written by him as no one else know such detailed about my difficulty. You are wonderful! Thanks!
As I website owner I believe the written content here is very fantastic, thanks for your efforts.
I must point out my gratitude for your generosity in support of folks that really want help on that theme. Your special dedication to getting the message across has been certainly functional and has helped others just like me to attain their goals. Your new warm and helpful hints and tips indicates much a person like me and substantially more to my mates. Thank you; from each one of us.
Saya sangat bersyukur menemukan website ini di Bing, persis seperti yang saya telusuri : D pula sudah saya bookmark.
Your place is valueble for me. Thanks!…
Thank you for sharing with us, I think this website really stands out :D.
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini sebelumnya adalah sebuah materi hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa tetap berhubungan?
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
Hi there, I discovered your site by means of Google while looking for a similar subject, your website came up, it seems to be great. I have bookmarked it in my google bookmarks.
Mengagumi komitmen yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda berikan. Sangat luar biasa menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang sangat baik! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Postingan yang hebat! Saya menghargai gaya Anda menguraikan semuanya dengan mudah dipahami. Teruskan kerja yang hebat!
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
I’m now not positive where you’re getting your info, but great topic. I needs to spend some time learning much more or working out more. Thank you for fantastic information I was in search of this information for my mission.
Isi yang bermanfaat dan disajikan dengan sangat baik. Saya pasti akan membagikan ini kepada rekan-rekan. Terima kasih banyak telah berbagi.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Anda dapat jelas melihat keahlian Anda di dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
You are a very smart person!
Artikel yang hebat. Ini memberikan saya gambaran yang lebih jelas tentang topik ini. Teruskan pekerjaan yang luar biasa!
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
Pretty! This was a really wonderful post. Thank you for your provided information.
Saya menghargai usaha yang Anda luangkan untuk membuat artikel ini. Informasi yang bernilai. Terima kasih banyak!
Saya kebetulan menemukan website Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang bagus.
Kami bisa memiliki hyperlink pertukaran kesepakatan antara kita!
Unquestionably believe that which you stated. Your favorite reason appeared to be on the internet the simplest thing to be aware of. I say to you, I definitely get irked while people think about worries that they plainly do not know about. You managed to hit the nail upon the top and defined out the whole thing without having side effect , people could take a signal. Will likely be back to get more. Thanks
Sangat menarik poin yang Anda catat, sangat menghargai telah mengunggah. “Hal yang selalu terjadi adalah apa yang benar-benar Anda percayai, dan kepercayaan pada suatu hal membuatnya terjadi.” oleh Frank Lloyd Wright.
Good web site! I truly love how it is simple on my eyes and the data are well written. I’m wondering how I could be notified whenever a new post has been made. I have subscribed to your RSS feed which must do the trick! Have a great day!
Great awesome issues here. I am very satisfied to look your post. Thanks so much and i’m having a look forward to contact you. Will you please drop me a mail?
Menghargai kerja keras yang Anda curahkan ke website Anda dan informasi mendalam yang Anda tawarkan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang hebat! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
id=”firstHeading” class=”firstHeading mw-first-heading”>Search results
Help
English
Tools
Tools
move to sidebar hide
Actions
General
Что такое megasb!? Стабильно развивающаяся торговая
платформа даркнета. Те, кто хоть раз в своей
жизни был по ту сторону интернета осознают, насколько безграничен мир темной
сети. По сути это тот же самый интернет к которому мы привыкли,
только еще лучше — здесь не действуют контроль и модерация.
Здесь, MEGA DARKNET в даркнете очень много разных ресурсов плохих и хороших, качественных и нет.
Каждый выбирает себе то, что ему по душе.
А ты переходи в мир безгроничного постоянного блаженства – переходи на Мега!
MEGA DARKNET
Terima kasih banyak atas posting yang luar biasa. Saya sungguh menyukai membaca ini dan menemukan banyak informasi yang berguna. Teruskan kerja yang hebat!
id=”firstHeading” class=”firstHeading mw-first-heading”>Search results
Help
English
Tools
Tools
move to sidebar hide
Actions
General
Что такое megasb!? Беспрепятственно развивающаяся торговая платформа даркнета.
Те, кто хоть миг в своей жизни был по ту сторону интернета осознают, насколько безграничен
мир всемирной паутины. По сути
это тот же самый интернет с которым мы знакомы, только еще лучше — здесь не действуют запреты и
ограничения. Здесь, мега мориарти в даркнете очень много разных ресурсов плохих и хороших, качественных и нет.
Каждый выбирает себе то, что
ему по душе. А ты переходи в мир безгроничного постоянного блаженства –
переходи на MEGA!
мега официальный сайт
Bersama dengan segala sesuatu yang terlihat sedang berkembang di dalam topik ini, banyak pandangan Anda cenderung cukup radikal. Namun, saya memohon maaf, karena saya tidak memberikan kepercayaan pada keseluruhan ide Anda, meskipun menyegarkan. Terlihat bagi kami bahwa pendapat Anda tidak benar-benar tervalidasi dan pada faktanya Anda sendiri tidak benar-benar sepenuhnya yakin terhadap argumen tersebut. Dalam hal apa pun saya menghargai membacanya.
Spot on with this write-up, I really suppose this web site needs far more consideration. I’ll most likely be again to read much more, thanks for that info.
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan berterima kasih kepada Anda.
Hi , I do believe this is an excellent blog. I stumbled upon it on Yahoo , i will come back once again. Money and freedom is the best way to change, may you be rich and help other people.
Artikel yang fantastis. Saya sungguh menyukai gaya Anda menjelaskan ide-ide ini. Teruskan kerja yang hebat!
Sangat menarik informasi!Sempurna persis seperti yang saya cari! “Hari yang paling sia-sia adalah hari di mana kita tidak tertawa.” oleh Sbastien-Roch Nicolas de Chamfort.
Valuable information. Lucky me I found your web site by accident, and I am shocked why this accident did not happened earlier! I bookmarked it.
I do agree with all the ideas you have offered for your post. They are really convincing and will definitely work. Nonetheless, the posts are too brief for novices. May you please prolong them a little from next time? Thank you for the post.
Saya mendapatkan info yang bagus dari blog Anda.
I’m really impressed with your writing skills as well as with the layout on your weblog. Is this a paid theme or did you modify it yourself? Either way keep up the nice quality writing, it’s rare to see a nice blog like this one today..
Yeah bookmaking this wasn’t a risky decision outstanding post! .
I like this blog so much, bookmarked. “Respect for the fragility and importance of an individual life is still the mark of an educated man.” by Norman Cousins.
Terima kasih, saya baru saja mencari informasi sekitar subjek ini sudah lama dan milik Anda adalah yang paling hebat yang saya jumpai sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang sumber tersebut?
Thank you, I’ve recently been searching for info approximately this subject for a while and yours is the best I’ve discovered till now. However, what about the bottom line? Are you certain concerning the source?
Your comment is awaiting moderation.
id=”firstHeading” class=”firstHeading mw-first-heading”>Search results
Help
English
Tools
Tools
move to sidebar hide
Actions
General
Лучший сайт для покупки и продажи товаров – MEGA https://XN–Mgmarkt7-9Db.com/ .
Сегодня Мега даркнет является самой крупной и известной анонимной торговой
площадкой в СНГ. Она предлагает свои пользователям доступ к большой базе магазинов
из разных стран. Здесь можно приобрести любые вещи.
Также вы можете сами начать продажу,
зарегистрировавшись на проекте.
При этом важно понимать, что сайт гарантирует
безопасность, а потому проверяет каждого своего продавца.
Для этого используются различные способы, в числе которых – тайные покупатели.
Потому вы можете быть уверены
в качестве покупаемых товаров, честности продавцов, и безопасности покупок на Мега онион.
А для перехода на сайт, просто использовать активную ссылку MEGA официальный сайт – MEGA DARKNET.
MEGA DARKNET
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Hi there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
Do you mind if I quote a few of your posts as long as I provide credit and sources back to your site? My blog is in the very same area of interest as yours and my users would genuinely benefit from a lot of the information you provide here. Please let me know if this okay with you. Many thanks!
Saya mendapatkan info yang bagus dari blog Anda.
We’re a bunch of volunteers and opening a new scheme in our community. Your web site provided us with useful information to work on. You have done an impressive process and our entire community will probably be grateful to you.
Sweet blog! I found it while browsing on Yahoo News. Do you have any tips on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Many thanks
Hi! This post could not be written any better! Reading through this post reminds me of my good old room mate! He always kept chatting about this. I will forward this write-up to him. Fairly certain he will have a good read. Many thanks for sharing!
Saya sangat menghargai waktu yang Anda curahkan untuk menyusun posting ini. Informasi yang sangat berharga. Terima kasih!
Rattling informative and good anatomical structure of content material, now that’s user genial (:.
Menghargai ketekunan yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda sajikan. Sangat luar biasa menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
I was just looking for this info for some time. After 6 hours of continuous Googleing, at last I got it in your web site. I wonder what is the lack of Google strategy that don’t rank this kind of informative sites in top of the list. Normally the top web sites are full of garbage.
I’ve read several good stuff here. Definitely worth bookmarking for revisiting. I wonder how so much attempt you set to make the sort of great informative site.
Saya biasanya tidak menulis komentar, tetapi yang satu ini benar-benar layak. Isi yang luar biasa dan sangat membantu. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Halo di sana, kamu sudah melakukan kerja yang luar biasa. Saya pasti akan menyimpan ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
It is best to participate in a contest for one of the best blogs on the web. I’ll advocate this site!
Some really nice and utilitarian info on this internet site, too I conceive the style and design has got good features.
I have to show some thanks to the writer just for bailing me out of this particular condition. After surfing throughout the world-wide-web and meeting methods which were not beneficial, I figured my entire life was gone. Existing devoid of the approaches to the difficulties you’ve solved all through the guideline is a crucial case, as well as the ones that would have badly affected my career if I hadn’t encountered your blog. Your own personal mastery and kindness in taking care of a lot of things was valuable. I’m not sure what I would have done if I hadn’t come upon such a point like this. I am able to now look forward to my future. Thanks for your time very much for this specialized and results-oriented guide. I will not be reluctant to propose your web site to any individual who wants and needs recommendations about this situation.
It’s actually a great and useful piece of information. I am glad that you shared this helpful info with us. Please keep us up to date like this. Thanks for sharing.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Hello! This post could not be written any better! Reading this post reminds me of my good old room mate! He always kept chatting about this. I will forward this page to him. Fairly certain he will have a good read. Thanks for sharing!
Terima kasih atas posting yang luar biasa. Saya benar-benar menikmati membaca ini dan menemukan banyak sekali informasi yang berguna. Teruskan kerja yang bagus!
Hi there just wanted to give you a brief heads up and let you know a few of the pictures aren’t loading properly. I’m not sure why but I think its a linking issue. I’ve tried it in two different web browsers and both show the same outcome.
I really wanted to send a quick comment to be able to say thanks to you for all of the pleasant guides you are showing here. My time intensive internet research has now been rewarded with professional strategies to share with my relatives. I ‘d believe that many of us readers are unequivocally blessed to dwell in a great community with so many marvellous professionals with very beneficial secrets. I feel truly happy to have encountered your entire weblog and look forward to many more pleasurable moments reading here. Thanks again for all the details.
I’m typically to running a blog and i really recognize your content. The article has actually peaks my interest. I am going to bookmark your site and hold checking for brand spanking new information.
Some genuinely nice and useful information on this website, too I think the design has wonderful features.
wonderful post, very informative. I wonder why the other specialists of this sector do not notice this. You should continue your writing. I am confident, you’ve a huge readers’ base already!
Wonderful work! This is the type of information that should be shared around the net. Shame on the search engines for not positioning this post higher! Come on over and visit my website . Thanks =)
Undeniably believe that that you said. Your favorite justification seemed to be at the internet the easiest thing to bear in mind of. I say to you, I definitely get irked while people consider concerns that they just do not recognize about. You controlled to hit the nail upon the top and defined out the whole thing with no need side effect , other folks can take a signal. Will likely be again to get more. Thank you
Your comment is awaiting moderation.
https://www.youtube.com/@5qqbrcom
https://x.com/5qqbrcom
https://tooter.in/5qqbrcom
https://wakelet.com/@5qqbrcom
https://safechat.com/u/casa.de.apostas.5qq
https://gravatar.com/5qqbrcom
https://www.mymeetbook.com/5qqbrcom
https://www.pinterest.com/5qqbrcom/
https://shareyoursocial.com/5qqbrcom
https://500px.com/p/5qqbrcom
https://www.instapaper.com/p/5qqbrcom
https://protocol.ooo/ja/users/5qqbrcom
https://audiomack.com/5qqbrcom
https://hackaday.io/5qqbrcom
https://fyers.in/community/member/obieQDm5mJ
https://leetcode.com/u/5qqbrcom/
https://swag.live/en/u/5qqbrcom
https://www.halaltrip.com/user/profile/369258/5qqbrcom/
https://medibang.com/author/28781628/
https://www.blockdit.com/5qqbrcom
https://portfolium.com/5qqbrcom
https://www.twitch.tv/5qqbrcom/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:A33980A26A55AE590A495CCD@AdobeID
https://profile.hatena.ne.jp/qq5brcom/
https://docs.google.com/document/d/1ikNC9wfYyQR14NUslasvb3WOSsS9Rw_CJScTq6DEtk4/edit?usp=sharing
https://issuu.com/5qqbrcom
https://www.behance.net/5qqbrcom
https://www.reverbnation.com/artist/5qqbrcom
https://www.myminifactory.com/users/5qqbrcom
https://www.investagrams.com/Profile/5qqbrcom
https://gifyu.com/5qqbrcom
https://www.chordie.com/forum/profile.php?section=about&id=2593317
https://www.walkscore.com/people/249008106031/5qqbrcom
https://topsitenet.com/profile/5qqbrcom/2163900/
https://akniga.org/profile/1446321-5qqbrcom/
https://disqus.com/by/5qqbrcom/about/
https://jobs.suncommunitynews.com/profiles/8588132-casa-de-apostas-5qq
https://www.speedrun.com/users/5qqbrcom
https://www.fanart-central.net/user/5qqbrcomm/profile
https://www.aicrowd.com/participants/5qqbrcom
https://www.bitchute.com/channel/5qqbrcom
https://pbase.com/5qqbrcom/
https://hub.docker.com/u/5qqbrcom
https://www.gta5-mods.com/users/5qqbrcom
https://heylink.me/5qqbrcom/
https://pixabay.com/users/5qqbrcom-56686993/
https://www.nicovideo.jp/user/144839210
https://3dwarehouse.sketchup.com/by/5qqbrcom
https://scholar.google.com/citations?view_op=list_works&hl=en&user=XrJVGagAAAAJ
https://medium.com/@benbowarmah446
https://web.bikemap.net/u/5qqbrcom
https://www.xiuwushidai.com/home.php?mod=space&uid=2799412
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6741461
https://bookmeter.com/users/1747344
https://rb.gy/dwrlbg
https://www.mynbest.info/profile/5qqbrcom/profile
https://jasa-seo.mn.co/members/40602091
https://www.zazzle.pt/mbr/238602768815519017
https://www.africangenesis-101.org/profile/5qqbrcom/profile
https://sitereport.netcraft.com/?url=https://5qq.br.com
https://www.miseducationofmotherhood.com/profile/5qqbrcom/profile
https://www.housedumonde.com/profile/5qqbrcom/profile
https://t.ly/_te4a
https://postr.blog/profile/5qqbrcom
https://joy.link/5qqbrcom
https://connect.garmin.com/app/profile/7da4b664-d3d8-4bc6-b326-aff1d7545a93
https://www.openrec.tv/user/5qqbrcom/about
https://routinehub.co/user/5qqbrcom
https://pxhere.com/en/photographer/5074056
https://teletype.in/@5qqbrcom
https://www.checkli.com/5qqbrcom#/a/process
https://freeimage.host/5qqbrcom
https://motion-gallery.net/users/1014981
https://biomolecula.ru/authors/165669
https://blender.community/5qqbrcom/
https://matkafasi.com/user/5qqbrcom
https://www.notebook.ai/@5qqbrcom
https://www.abclinuxu.cz/lide/5qqbrcom
https://muare.vn/shop/5qqbrcom/914126
https://forum.dmec.vn/index.php?members/5qqbrcom.209424/
https://igli.me/5qqbrcom
http://delphi.larsbo.org/user/5qqbrcom
https://timdaily.vn/members/5qqbrcom.142208/#about
https://app.readthedocs.org/profiles/5qqbrcom/
https://www.dibiz.com/benbowarmah446
https://iszene.com/user-363052.html
https://www.theyeshivaworld.com/coffeeroom/users/5qqbrcom
https://desksnear.me/users/5qqbrcom
https://www.itchyforum.com/en/member.php?398658-5qqbrcom
https://www.roton.com/forums/users/benbowarmah446/
https://able2know.org/user/5qqbrcom/
http://www.biblesupport.com/user/864922-5qqbrcom/
https://golosknig.com/profile/5qqbrcom/
https://wallhaven.cc/user/5qqbrcom
https://bandori.party/user/1388817/5qqbrcom/#preferences
https://schoolido.lu/user/5qqbrcom/
https://awan.pro/forum/user/197525/
https://fortunetelleroracle.com/profile/5qqbrcom
https://fabble.cc/5qqbrcom
https://pad.stuve.de/s/3NDEnMBmm
https://www.sythe.org/members/5qqbrcom.2073194/
https://about.me/nc5qqbrcom
https://potofu.me/5qqbrcom
https://transfur.com/Users/nc5qqbrcom
https://qna.habr.com/user/5qqbrcom
https://website.informer.com/5qq.br.com
https://en.islcollective.com/portfolio/12967663
https://www.xosothantai.com/members/5qqbrcom.629308/
https://velog.io/@5qqbrcom/about
https://mez.ink/5qqbrcom
https://5qqbrcom.stck.me/profile
https://www.edna.cz/uzivatele/5qqbrcom/
https://leakedmodels.com/forum/members/5qqbrcom.728773/#about
https://freeicons.io/profile/955728
https://onlinesequencer.net/members/293743
https://inkbunny.net/5qqbrcom
https://www.japaaan.com/user/110122/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5qq
https://beatsaver.com/playlists/1234321
https://apptuts.bio/5qqbrcom-276083
https://www.storenvy.com/nc5qqbrcom
https://egl.circlly.com/users/5qqbrcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319215
https://acomics.ru/-5qqbrcom
https://hanson.net/users/5qqbrcom
https://writexo.com/share/029d9ce0d156
https://expatguidekorea.com/profile/5qqbrcom/
https://www.heavyironjobs.com/profiles/8589332-casa-de-apostas-5qq
https://pad.degrowth.net/s/68c1JnLKf
https://forum.skullgirlsmobile.com/members/5qqbrcom.243776/#about
https://jobs.landscapeindustrycareers.org/profiles/8589355-casa-de-apostas-5qq
https://phatwalletforums.com/user/5qqbrcom
https://song.link/5qqbrcom
https://idol.st/user/199544/5qqbrcom/
https://jobs.windomnews.com/profiles/8589416-casa-de-apostas-5qq
https://hoaxbuster.com/redacteur/5qqbrcom
https://www.givey.com/5qqbrcom
https://www.hobowars.com/game/linker.php?url=https://5qq.br.com/
https://jobs.westerncity.com/profiles/8589432-casa-de-apostas-5qq
https://www.thetriumphforum.com/members/5qqbrcom.73670/
https://album.link/5qqbrcom
https://dev.muvizu.com/Profile/5qqbrcom/Latest
https://chaloke.com/forums/users/5qqbrcom/
https://buckeyescoop.com/community/members/5qqbrcom.69691/#about
http://forum.cncprovn.com/members/436649-5qqbrcom
https://forum.aigato.vn/user/5qqbrcom
https://learningapps.org/watch?v=pd625bnqn26
https://www.invelos.com/UserProfile.aspx?Alias=5qqbrcom
https://gitlab.vuhdo.io/5qqbrcom
https://poipiku.com/14012229/
https://www.rwaq.org/users/5qqbrcom
https://www.fundable.com/casa-de-apostas-5qq
https://www.grepmed.com/5qqbrcom
https://classificados.acheiusa.com/profile/b3pBZm9aVXAxS1pnaDZOcGEvZUtXMVJUNExxSkYwWUo5eHFmOUhETE11Zz0=
https://espritgames.com/members/51915045/
https://www.haikudeck.com/presentations/5qqbrcom
https://undrtone.com/5qqbrcom
https://marshallyin.com/members/5qqbrcom/
https://www.atozed.com/forums/user-91556.html
https://gravesales.com/author/5qqbrcom/
https://belgaumonline.com/profile/5qqbrcom/
https://zzb.bz/5qqbrcom
https://www.themeqx.com/forums/users/5qqbrcom/
http://newdigital-world.com/members/5qqbrcom.html
https://www.xen-factory.com/index.php?members/5qqbrcom.176034/#about
https://forums.servethehome.com/index.php?members/5qqbrcom.259442/#about
https://www.blackhatprotools.info/member.php?302365-5qqbrcom
https://activepages.com.au/profile/5qqbrcom
https://snippet.host/khkspm
https://tudomuaban.com/chi-tiet-rao-vat/2965670/5qqbrcom.html
https://phijkchu.com/a/5qqbrcom/video-channels
https://lifeinsys.com/user/5qqbrcom
https://kaeuchi.jp/forums/users/5qqbrcom/
https://www.claimajob.com/profiles/8590404-casa-de-apostas-5qq
https://protospielsouth.com/user/153705
https://theafricavoice.com/profile/5qqbrcom
https://support.bitspower.com/support/user/5qqbrcom
https://hackmd.okfn.de/s/S1gbjFm4Gg
https://manylink.co/@5qqbrcom
https://anyflip.com/homepage/jffvr
https://www.akaqa.com/question/q19192716401-5qqbrcom
https://civitai.com/user/5qqbrcom
https://www.spigotmc.org/members/5qqbrcom.2573771/
https://hoo.be/5qqbrcom
https://mathlog.info/users/D8LeAmRGYwXWtwCNkUpdQAT8WT93
https://www.slmath.org/people/122267
https://connect.gt/user/5qqbrcom
https://www.sunlitcentrekenya.co.ke/author/5qqbrcom/
https://www.rcuniverse.com/forum/members/5qqbrcom.html
https://www.huntingnet.com/forum/members/5qqbrcom.html
https://vimeo.com/5qqbrcom
https://www.trackyserver.com/profile/266524
https://www.zubersoft.com/mobilesheets/forum/user-151530.html
https://md.coredump.ch/s/ucLuGyFdc
https://aprenderfotografia.online/usuarios/5qqbrcom/profile/
https://hackmd.hub.yt/s/30o6X8xt2
https://sciencemission.com/profile/5qqbrcom
https://www.wvhired.com/profiles/8589079-casa-de-apostas-5qq
https://formulamasa.com/elearning/members/5qqbrcom/?v=96b62e1dce57
https://chyoa.com/user/5qqbrcom
https://www.royalroad.com/profile/1023440
https://backloggd.com/u/5qqbrcom/
https://forums.alliedmods.net/member.php?u=488862
https://community.jmp.com/t5/user/viewprofilepage/user-id/105976
https://viblo.asia/u/5qqbrcom/contact
https://redirect.camfrog.com/redirect/?url=https://5qq.br.com/
https://www.fw-follow.com/forum/topic/160780/5qqbrcom
https://www.navacool.com/forum/topic/529391/5qqbrcom
https://www.driedsquidathome.com/forum/topic/190199/5qqbrcom
https://www.nongkhaempolice.com/forum/topic/193308/5qqbrcom
https://www.bestloveweddingstudio.com/forum/topic/116999/5qqbrcom
https://www.natthadon-sanengineering.com/forum/topic/146176/5qqbrcom
https://www.rueanmaihom.net/forum/topic/133184/5qqbrcom
https://www.ttlxshipping.com/forum/topic/529396/5qqbrcom
http://forum.modulebazaar.com/forums/user/5qqbrcom/
https://www.rcmx.net/userinfo.php?uid=23035
https://lqdoj.edu.vn/user/5qqbrcom
https://indiestorygeek.com/user/5qqbrcom
https://forum.issabel.org/u/5qqbrcom
https://www.easyhits4u.com/profile.cgi?login=5qqbrcom&view_as=1
https://doc.anagora.org/s/Lnw3ugf7P
https://profile.sampo.ru/n5qqbrcom
https://www.ekdarun.com/forum/topic/189214/5qqbrcom
https://fanclove.jp/profile/pv2xe6bAJR
https://www.d-ushop.com/forum/topic/189446/5qqbrcom
https://findaspring.org/members/5qqbrcom/
https://fengshuidirectory.com/dashboard/listings/5qqbrcom/
https://pets4friends.com/profile-1661549
https://participa.aytojaen.es/profiles/5qqbrcom/activity
https://linkmix.co/57237028
https://janitorai.com/profiles/d7d505af-a86e-4c06-b20a-221a531a0afe_profile-of-5-qqbrcom
https://www.buymusic.club/user/5qqbrcom
https://forum.freero.org/space-uid-27078.html
https://rant.li/5qqbrcom/5qqbrcom
https://chanylib.ru/ru/forum/user/36056/
https://skrolli.fi/keskustelu/users/benbowarmah446/
https://www.thehockeypaper.co.uk/forums/users/5qqbrcom
https://www.11plus.co.uk/users/benbowarmah446/
https://opaseke.com/users/17247
https://imaginaria.ru/profile/5qqbrcom/
https://www.newgenstravel.com/forum/topic/70294/5qqbrcom
https://zbrushcentral.jp/user/5qqbrcom
https://www.mapleprimes.com/users/5qqbrcom
https://www.adpost.com/u/5qqbrcom/
https://guitarmaking.co.uk/members/5qqbrcom/activity/197498/
https://scrapbox.io/5qqbrcom/5qqbrcom
https://qiita.com/5qqbrcom
https://www.annuncigratuititalia.it/author/5qqbrcom/
https://lite.link/5qqbrcom
http://www.brenkoweb.com/user/101878/profile
https://novel.daysneo.com/author/5qqbrcom/
https://anunt-imob.ro/user/profile/867898
https://destaquebrasil.com/saopaulo/author/5qqbrcom/
https://makerworld.com/en/@5qqbrcom
https://bhmtsff.com/space-uid-99206.html
https://blog.sighpceducation.acm.org/wp/forums/users/5qqbrcom/
https://vc.ru/id6043412
https://dreevoo.com/profile.php?pid=2058110
https://www.passes.com/5qqbrcom
https://backloggery.com/5qqbrcom
http://palangshim.com/space-uid-5348028.html
https://etextpad.com/tr8fku85gv
https://app.talkshoe.com/user/5qqbrcom
https://pinshape.com/users/9010022-5qqbrcom?tab=designs
https://sfx.thelazy.net/users/u/5qqbrcom/
https://www.skypixel.com/users/djiuser-zigh11xqf3e1
https://pictureinbottle.com/r/5qqbrcom
https://makeagif.com/user/5qqbrcom?ref=RDZNYj
https://www.plotterusati.it/user/5qqbrcom
https://www.managementpedia.com/members/5qqbrcom.1126838/#about
https://partecipa.poliste.com/profiles/5qqbrcom/activity
https://hedgedoc.stusta.de/s/mThfkMN17
https://pad.codefor.fr/s/FHshO-yMP_
https://pad.fablab-siegen.de/s/qaCZKCC-F6
https://hedgedoc.dezentrale.space/s/AwgPoq2_5
https://pad.darmstadt.social/s/nISqqL98dT
https://referrallist.com/profile/5qqbrcom/
https://md.chaosdorf.de/s/4pCpx92U73
https://telegra.ph/5qqbrcom-07-14
https://runtrip.jp/users/811636
https://www.bonback.com/forum/topic/529361/5qqbrcom
https://www.iglinks.io/BenbowArmah446-nhy
https://www.dokkan-battle.fr/forums/users/5qqbrcom/
https://homepage.ninja/5qqbrcom
https://boss.why3s.cc/boss/home.php?mod=space&uid=291386
https://www.foriio.com/5qqbrcom
https://md.rappet.xyz/s/DtP_V038Zj
https://md.sebastians.dev/s/KhsDVg4Xb
https://controlc.com/fdkxixi0
https://justpaste.it/u/5qqbrcom
https://www.pozible.com/profile/5qqbrcom
https://www.elephantjournal.com/profile/5qqbrcom/
https://strikefans.com/forum/users/5qqbrcom/
https://swat-portal.com/forum/wcf/user/57709-5qqbrcom/#about
http://julia4tied.de/member.php?action=profile&uid=255351
https://stocktwits.com/5qqbrcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5qqbrcom/
https://mercadodinamico.com.br/author/5qqbrcom/
https://www.grabcaruber.com/members/5qqbrcom/profile/
https://qoolink.co/5qqbrcom
https://galleria.emotionflow.com/196484/profile.html
https://www.myget.org/users/5qqbrcom
https://app.brancher.ai/user/2fOVUTfw634I
https://confengine.com/user/5qqbrcom
https://mygamedb.com/profile/5qqbrcom
https://forum.aceinna.com/user/5qqbrcom
https://www.giveawayoftheday.com/forums/profile/1971385
https://uiverse.io/profile/5qqbrcom_2415
https://cofacts.tw/user/5qqbrcom
https://vcook.jp/users/107821
https://www.efunda.com/members/people/show_people.cfm?Usr=5qqbrcom
https://pumpyoursound.com/u/user/1644900
https://congdongx.com/thanh-vien/5qqbrcom.57396/#about
https://www.intensedebate.com/people/nc5qqbrcom
https://www.tkaraoke.com/forums/profile/5qqbrcom/
https://svetelektro.com/clenovia/5qqbrcom/
https://marshmallow-qa.com/1cnpqw3qffhr4ss
https://us.enrollbusiness.com/BusinessProfile/7879899/5qqbrcom
https://link4u.cc/@5qqbrcom
https://its-my.link/@5qqbrcom
https://truckymods.io/user/522986
https://iplogger.org/vn/logger/pDiP583eNhJy/
https://www.iniuria.us/forum/member.php?700938-5qqbrcom
https://cointr.ee/5qqbrcom
https://indian-tv.cz/u/5qqbrcom
https://hedgedoc.envs.net/s/3FURkO2Wt
https://illust.daysneo.com/illustrator/5qqbrcom/
https://hubb.link/5qqbrcom/
https://www.czporadna.cz/user/5qqbrcom
https://tutorialslink.com/member/5qqbrcomundefined/109962
https://expathealthseoul.com/profile/5qqbrcom/
https://expathealthseoul.com/profile/5qqbrcom/
https://www.goodreads.com/user/show/202673360-5qqbrcom-5qq
https://www.abookmarking.com/story/5qqbrcom
https://www.letsdobookmark.com/story/5qqbrcom
https://www.mateball.com/n5qqbrcom
https://raovat.nhadat.vn/members/5qqbrcom-331783.html
https://advego.com/profile/5qqbrcom/
https://www.vnbadminton.com/members/5qqbrcom.89347/
https://www.sunemall.com/board/board_topic/8431232/8671017.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8671018.htm
https://solo.to/5qqbrcom
https://graph.org/5qqbrcom-07-14-2
https://selling.goo.ng/5qqbrcom
https://www.fcc.gov/fcc-bin/bye?https://5qq.br.com/
https://calgarybusinesses.ca/dashboard/reviews/5qqbrcom/
https://www.sciencebee.com.bd/qna/user/5qqbrcom
https://luvly.co/users/5qqbrcom
https://spinninrecords.com/profile/5qqbrcom
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8671039.htm
https://www.tai-ji.net/board/board_topic/4160148/8671050.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8671054.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8671055.htm
https://kheotay.com.vn/forums/users/benbowarmah446
https://crazyservice.by/forum/user/17876/
https://rsfpost.com/forums/users/5qqbrcom/
https://exceldemy.com/forum/members/5qqbrcom.6322/#about
https://www.ontime.co.th/forum/topic/872956/5qqbrcom
https://forum.gettinglost.ca/user/5qqbrcomm
https://zepodcast.com/forums/users/5qqbrcom/
https://monviet88.com/profile/5qqbrcom/
https://www.fuelly.com/driver/5qqbrcom
https://www.physicsoverflow.org/user/5qqbrcom
https://www.spacedesk.net/support-forum/profile/5qqbrcom/
https://pods.link/5qqbrcom
https://mylink.page/5qqbrcom
https://letterboxd.com/5qqbrcom/
https://ctxt.io/3/lyguNLvMc
https://onespotsocial.com/5qqbrcom
https://www.scener.com/@5qqbrcom
https://amaz0ns.com/forums/users/5qqbrcom/
https://hostndobezi.com/5qqbrcom
https://nilechronicles.com/profile/5qqbrcom
https://biiut.com/5qqbrcom
https://www.renderosity.com/users/id:1879799
https://eo-college.org/members/5qqbrcom/
https://www.moshpyt.com/user/5qqbrcom
https://www.racerjobs.com/profiles/8594816-casa-de-apostas-5qq
https://www.instructorsnearme.com/author/5qqbrcom/
https://ferrariformula1.hu/community/profile/5qqbrcom/
https://www.pebforum.com/members/5qqbrcom.262350/#about
http://koloboklinks.com/site?url=5qq.br.com
http://freestyler.ws/user/677387/5qqbrcom
https://jali.me/5qqbrcom
https://bioqoo.com/5qqbrcom
https://ac.db0.company/user/20557/5qqbrcom/
https://www.youyooz.com/profile/5qqbrcom/
https://forum.hiv.plus/user/5qqbrcom
https://www.thitrungruangclinic.com/forum/topic/194377/5qqbrcom
https://ja.cofacts.tw/user/5qqbrcom
https://www.minecraft-servers-list.org/details/5qqbrcom/
https://blog.ulifestyle.com.hk/5qqbrcom
https://baskadia.com/user/h67x
https://buyerseller.xyz/user/5qqbrcom/
https://www.democracylab.org/user/53448
https://vs.cga.gg/user/247634
https://bsky.app/profile/5qqbrcom.bsky.social
https://www.xmonsta.com/forums/users/5qqbrcom/
https://www.green-collar.com/forums/users/5qqbrcom/
https://www.hostboard.com/forums/members/5qqbrcom.html
https://infinitebacklog.net/users/5qqbrcom
https://xmrbazaar.com/user/5qqbrcom/
https://tuscl.net/member/902877
https://sighpceducation.hosting.acm.org/wp/forums/users/5qqbrcom/
https://www.ironlifting.it/forum/member.php?u=437058
https://nogu.org.uk/forum/profile/5qqbrcom/
https://reactormag.com/members/5qqbrcom/profile
https://www.themirch.com/blog/author/5qqbrcom/
https://foss.heptapod.net/5qqbrcom
https://www.euskalmarket.com/author/5qqbrcom/
https://doingbusiness.eu/profile/5qqbrcom/
https://portfolium.com.au/5qqbrcom
https://umczdt.ru/forum/?PAGE_NAME=profile_view&UID=160706
https://ic-info.ru/forum/user/227255/
https://stardust.run/user/177792/5qqbrcom/#preferences
https://mail.tudomuaban.com/chi-tiet-rao-vat/2966474/5qqbrcom.html
https://gamelet.online/user/5qqbrcom
https://www.facer.io/u/5qqbrcom
https://talkmarkets.com/profile/casa-de-apostas-5qq-260715-062419
https://forum.cnnr.fr/user/5qqbrcom
https://jobs.host-panel.com/author/5qqbrcom/
Your comment is awaiting moderation.
https://www.youtube.com/@5qqbrcom
https://x.com/5qqbrcom
https://tooter.in/5qqbrcom
https://wakelet.com/@5qqbrcom
https://safechat.com/u/casa.de.apostas.5qq
https://gravatar.com/5qqbrcom
https://www.mymeetbook.com/5qqbrcom
https://www.pinterest.com/5qqbrcom/
https://shareyoursocial.com/5qqbrcom
https://500px.com/p/5qqbrcom
https://www.instapaper.com/p/5qqbrcom
https://protocol.ooo/ja/users/5qqbrcom
https://audiomack.com/5qqbrcom
https://hackaday.io/5qqbrcom
https://fyers.in/community/member/obieQDm5mJ
https://leetcode.com/u/5qqbrcom/
https://swag.live/en/u/5qqbrcom
https://www.halaltrip.com/user/profile/369258/5qqbrcom/
https://medibang.com/author/28781628/
https://www.blockdit.com/5qqbrcom
https://portfolium.com/5qqbrcom
https://www.twitch.tv/5qqbrcom/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:A33980A26A55AE590A495CCD@AdobeID
https://profile.hatena.ne.jp/qq5brcom/
https://docs.google.com/document/d/1ikNC9wfYyQR14NUslasvb3WOSsS9Rw_CJScTq6DEtk4/edit?usp=sharing
https://issuu.com/5qqbrcom
https://www.behance.net/5qqbrcom
https://www.reverbnation.com/artist/5qqbrcom
https://www.myminifactory.com/users/5qqbrcom
https://www.investagrams.com/Profile/5qqbrcom
https://gifyu.com/5qqbrcom
https://www.chordie.com/forum/profile.php?section=about&id=2593317
https://www.walkscore.com/people/249008106031/5qqbrcom
https://topsitenet.com/profile/5qqbrcom/2163900/
https://akniga.org/profile/1446321-5qqbrcom/
https://disqus.com/by/5qqbrcom/about/
https://jobs.suncommunitynews.com/profiles/8588132-casa-de-apostas-5qq
https://www.speedrun.com/users/5qqbrcom
https://www.fanart-central.net/user/5qqbrcomm/profile
https://www.aicrowd.com/participants/5qqbrcom
https://www.bitchute.com/channel/5qqbrcom
https://pbase.com/5qqbrcom/
https://hub.docker.com/u/5qqbrcom
https://www.gta5-mods.com/users/5qqbrcom
https://heylink.me/5qqbrcom/
https://pixabay.com/users/5qqbrcom-56686993/
https://www.nicovideo.jp/user/144839210
https://3dwarehouse.sketchup.com/by/5qqbrcom
https://scholar.google.com/citations?view_op=list_works&hl=en&user=XrJVGagAAAAJ
https://medium.com/@benbowarmah446
https://web.bikemap.net/u/5qqbrcom
https://www.xiuwushidai.com/home.php?mod=space&uid=2799412
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6741461
https://bookmeter.com/users/1747344
https://rb.gy/dwrlbg
https://www.mynbest.info/profile/5qqbrcom/profile
https://jasa-seo.mn.co/members/40602091
https://www.zazzle.pt/mbr/238602768815519017
https://www.africangenesis-101.org/profile/5qqbrcom/profile
https://sitereport.netcraft.com/?url=https://5qq.br.com
https://www.miseducationofmotherhood.com/profile/5qqbrcom/profile
https://www.housedumonde.com/profile/5qqbrcom/profile
https://t.ly/_te4a
https://postr.blog/profile/5qqbrcom
https://joy.link/5qqbrcom
https://connect.garmin.com/app/profile/7da4b664-d3d8-4bc6-b326-aff1d7545a93
https://www.openrec.tv/user/5qqbrcom/about
https://routinehub.co/user/5qqbrcom
https://pxhere.com/en/photographer/5074056
https://teletype.in/@5qqbrcom
https://www.checkli.com/5qqbrcom#/a/process
https://freeimage.host/5qqbrcom
https://motion-gallery.net/users/1014981
https://biomolecula.ru/authors/165669
https://blender.community/5qqbrcom/
https://matkafasi.com/user/5qqbrcom
https://www.notebook.ai/@5qqbrcom
https://www.abclinuxu.cz/lide/5qqbrcom
https://muare.vn/shop/5qqbrcom/914126
https://forum.dmec.vn/index.php?members/5qqbrcom.209424/
https://igli.me/5qqbrcom
http://delphi.larsbo.org/user/5qqbrcom
https://timdaily.vn/members/5qqbrcom.142208/#about
https://app.readthedocs.org/profiles/5qqbrcom/
https://www.dibiz.com/benbowarmah446
https://iszene.com/user-363052.html
https://www.theyeshivaworld.com/coffeeroom/users/5qqbrcom
https://desksnear.me/users/5qqbrcom
https://www.itchyforum.com/en/member.php?398658-5qqbrcom
https://www.roton.com/forums/users/benbowarmah446/
https://able2know.org/user/5qqbrcom/
http://www.biblesupport.com/user/864922-5qqbrcom/
https://golosknig.com/profile/5qqbrcom/
https://wallhaven.cc/user/5qqbrcom
https://bandori.party/user/1388817/5qqbrcom/#preferences
https://schoolido.lu/user/5qqbrcom/
https://awan.pro/forum/user/197525/
https://fortunetelleroracle.com/profile/5qqbrcom
https://fabble.cc/5qqbrcom
https://pad.stuve.de/s/3NDEnMBmm
https://www.sythe.org/members/5qqbrcom.2073194/
https://about.me/nc5qqbrcom
https://potofu.me/5qqbrcom
https://transfur.com/Users/nc5qqbrcom
https://qna.habr.com/user/5qqbrcom
https://website.informer.com/5qq.br.com
https://en.islcollective.com/portfolio/12967663
https://www.xosothantai.com/members/5qqbrcom.629308/
https://velog.io/@5qqbrcom/about
https://mez.ink/5qqbrcom
https://5qqbrcom.stck.me/profile
https://www.edna.cz/uzivatele/5qqbrcom/
https://leakedmodels.com/forum/members/5qqbrcom.728773/#about
https://freeicons.io/profile/955728
https://onlinesequencer.net/members/293743
https://inkbunny.net/5qqbrcom
https://www.japaaan.com/user/110122/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5qq
https://beatsaver.com/playlists/1234321
https://apptuts.bio/5qqbrcom-276083
https://www.storenvy.com/nc5qqbrcom
https://egl.circlly.com/users/5qqbrcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319215
https://acomics.ru/-5qqbrcom
https://hanson.net/users/5qqbrcom
https://writexo.com/share/029d9ce0d156
https://expatguidekorea.com/profile/5qqbrcom/
https://www.heavyironjobs.com/profiles/8589332-casa-de-apostas-5qq
https://pad.degrowth.net/s/68c1JnLKf
https://forum.skullgirlsmobile.com/members/5qqbrcom.243776/#about
https://jobs.landscapeindustrycareers.org/profiles/8589355-casa-de-apostas-5qq
https://phatwalletforums.com/user/5qqbrcom
https://song.link/5qqbrcom
https://idol.st/user/199544/5qqbrcom/
https://jobs.windomnews.com/profiles/8589416-casa-de-apostas-5qq
https://hoaxbuster.com/redacteur/5qqbrcom
https://www.givey.com/5qqbrcom
https://www.hobowars.com/game/linker.php?url=https://5qq.br.com/
https://jobs.westerncity.com/profiles/8589432-casa-de-apostas-5qq
https://www.thetriumphforum.com/members/5qqbrcom.73670/
https://album.link/5qqbrcom
https://dev.muvizu.com/Profile/5qqbrcom/Latest
https://chaloke.com/forums/users/5qqbrcom/
https://buckeyescoop.com/community/members/5qqbrcom.69691/#about
http://forum.cncprovn.com/members/436649-5qqbrcom
https://forum.aigato.vn/user/5qqbrcom
https://learningapps.org/watch?v=pd625bnqn26
https://www.invelos.com/UserProfile.aspx?Alias=5qqbrcom
https://gitlab.vuhdo.io/5qqbrcom
https://poipiku.com/14012229/
https://www.rwaq.org/users/5qqbrcom
https://www.fundable.com/casa-de-apostas-5qq
https://www.grepmed.com/5qqbrcom
https://classificados.acheiusa.com/profile/b3pBZm9aVXAxS1pnaDZOcGEvZUtXMVJUNExxSkYwWUo5eHFmOUhETE11Zz0=
https://espritgames.com/members/51915045/
https://www.haikudeck.com/presentations/5qqbrcom
https://undrtone.com/5qqbrcom
https://marshallyin.com/members/5qqbrcom/
https://www.atozed.com/forums/user-91556.html
https://gravesales.com/author/5qqbrcom/
https://belgaumonline.com/profile/5qqbrcom/
https://zzb.bz/5qqbrcom
https://www.themeqx.com/forums/users/5qqbrcom/
http://newdigital-world.com/members/5qqbrcom.html
https://www.xen-factory.com/index.php?members/5qqbrcom.176034/#about
https://forums.servethehome.com/index.php?members/5qqbrcom.259442/#about
https://www.blackhatprotools.info/member.php?302365-5qqbrcom
https://activepages.com.au/profile/5qqbrcom
https://snippet.host/khkspm
https://tudomuaban.com/chi-tiet-rao-vat/2965670/5qqbrcom.html
https://phijkchu.com/a/5qqbrcom/video-channels
https://lifeinsys.com/user/5qqbrcom
https://kaeuchi.jp/forums/users/5qqbrcom/
https://www.claimajob.com/profiles/8590404-casa-de-apostas-5qq
https://protospielsouth.com/user/153705
https://theafricavoice.com/profile/5qqbrcom
https://support.bitspower.com/support/user/5qqbrcom
https://hackmd.okfn.de/s/S1gbjFm4Gg
https://manylink.co/@5qqbrcom
https://anyflip.com/homepage/jffvr
https://www.akaqa.com/question/q19192716401-5qqbrcom
https://civitai.com/user/5qqbrcom
https://www.spigotmc.org/members/5qqbrcom.2573771/
https://hoo.be/5qqbrcom
https://mathlog.info/users/D8LeAmRGYwXWtwCNkUpdQAT8WT93
https://www.slmath.org/people/122267
https://connect.gt/user/5qqbrcom
https://www.sunlitcentrekenya.co.ke/author/5qqbrcom/
https://www.rcuniverse.com/forum/members/5qqbrcom.html
https://www.huntingnet.com/forum/members/5qqbrcom.html
https://vimeo.com/5qqbrcom
https://www.trackyserver.com/profile/266524
https://www.zubersoft.com/mobilesheets/forum/user-151530.html
https://md.coredump.ch/s/ucLuGyFdc
https://aprenderfotografia.online/usuarios/5qqbrcom/profile/
https://hackmd.hub.yt/s/30o6X8xt2
https://sciencemission.com/profile/5qqbrcom
https://www.wvhired.com/profiles/8589079-casa-de-apostas-5qq
https://formulamasa.com/elearning/members/5qqbrcom/?v=96b62e1dce57
https://chyoa.com/user/5qqbrcom
https://www.royalroad.com/profile/1023440
https://backloggd.com/u/5qqbrcom/
https://forums.alliedmods.net/member.php?u=488862
https://community.jmp.com/t5/user/viewprofilepage/user-id/105976
https://viblo.asia/u/5qqbrcom/contact
https://redirect.camfrog.com/redirect/?url=https://5qq.br.com/
https://www.fw-follow.com/forum/topic/160780/5qqbrcom
https://www.navacool.com/forum/topic/529391/5qqbrcom
https://www.driedsquidathome.com/forum/topic/190199/5qqbrcom
https://www.nongkhaempolice.com/forum/topic/193308/5qqbrcom
https://www.bestloveweddingstudio.com/forum/topic/116999/5qqbrcom
https://www.natthadon-sanengineering.com/forum/topic/146176/5qqbrcom
https://www.rueanmaihom.net/forum/topic/133184/5qqbrcom
https://www.ttlxshipping.com/forum/topic/529396/5qqbrcom
http://forum.modulebazaar.com/forums/user/5qqbrcom/
https://www.rcmx.net/userinfo.php?uid=23035
https://lqdoj.edu.vn/user/5qqbrcom
https://indiestorygeek.com/user/5qqbrcom
https://forum.issabel.org/u/5qqbrcom
https://www.easyhits4u.com/profile.cgi?login=5qqbrcom&view_as=1
https://doc.anagora.org/s/Lnw3ugf7P
https://profile.sampo.ru/n5qqbrcom
https://www.ekdarun.com/forum/topic/189214/5qqbrcom
https://fanclove.jp/profile/pv2xe6bAJR
https://www.d-ushop.com/forum/topic/189446/5qqbrcom
https://findaspring.org/members/5qqbrcom/
https://fengshuidirectory.com/dashboard/listings/5qqbrcom/
https://pets4friends.com/profile-1661549
https://participa.aytojaen.es/profiles/5qqbrcom/activity
https://linkmix.co/57237028
https://janitorai.com/profiles/d7d505af-a86e-4c06-b20a-221a531a0afe_profile-of-5-qqbrcom
https://www.buymusic.club/user/5qqbrcom
https://forum.freero.org/space-uid-27078.html
https://rant.li/5qqbrcom/5qqbrcom
https://chanylib.ru/ru/forum/user/36056/
https://skrolli.fi/keskustelu/users/benbowarmah446/
https://www.thehockeypaper.co.uk/forums/users/5qqbrcom
https://www.11plus.co.uk/users/benbowarmah446/
https://opaseke.com/users/17247
https://imaginaria.ru/profile/5qqbrcom/
https://www.newgenstravel.com/forum/topic/70294/5qqbrcom
https://zbrushcentral.jp/user/5qqbrcom
https://www.mapleprimes.com/users/5qqbrcom
https://www.adpost.com/u/5qqbrcom/
https://guitarmaking.co.uk/members/5qqbrcom/activity/197498/
https://scrapbox.io/5qqbrcom/5qqbrcom
https://qiita.com/5qqbrcom
https://www.annuncigratuititalia.it/author/5qqbrcom/
https://lite.link/5qqbrcom
http://www.brenkoweb.com/user/101878/profile
https://novel.daysneo.com/author/5qqbrcom/
https://anunt-imob.ro/user/profile/867898
https://destaquebrasil.com/saopaulo/author/5qqbrcom/
https://makerworld.com/en/@5qqbrcom
https://bhmtsff.com/space-uid-99206.html
https://blog.sighpceducation.acm.org/wp/forums/users/5qqbrcom/
https://vc.ru/id6043412
https://dreevoo.com/profile.php?pid=2058110
https://www.passes.com/5qqbrcom
https://backloggery.com/5qqbrcom
http://palangshim.com/space-uid-5348028.html
https://etextpad.com/tr8fku85gv
https://app.talkshoe.com/user/5qqbrcom
https://pinshape.com/users/9010022-5qqbrcom?tab=designs
https://sfx.thelazy.net/users/u/5qqbrcom/
https://www.skypixel.com/users/djiuser-zigh11xqf3e1
https://pictureinbottle.com/r/5qqbrcom
https://makeagif.com/user/5qqbrcom?ref=RDZNYj
https://www.plotterusati.it/user/5qqbrcom
https://www.managementpedia.com/members/5qqbrcom.1126838/#about
https://partecipa.poliste.com/profiles/5qqbrcom/activity
https://hedgedoc.stusta.de/s/mThfkMN17
https://pad.codefor.fr/s/FHshO-yMP_
https://pad.fablab-siegen.de/s/qaCZKCC-F6
https://hedgedoc.dezentrale.space/s/AwgPoq2_5
https://pad.darmstadt.social/s/nISqqL98dT
https://referrallist.com/profile/5qqbrcom/
https://md.chaosdorf.de/s/4pCpx92U73
https://telegra.ph/5qqbrcom-07-14
https://runtrip.jp/users/811636
https://www.bonback.com/forum/topic/529361/5qqbrcom
https://www.iglinks.io/BenbowArmah446-nhy
https://www.dokkan-battle.fr/forums/users/5qqbrcom/
https://homepage.ninja/5qqbrcom
https://boss.why3s.cc/boss/home.php?mod=space&uid=291386
https://www.foriio.com/5qqbrcom
https://md.rappet.xyz/s/DtP_V038Zj
https://md.sebastians.dev/s/KhsDVg4Xb
https://controlc.com/fdkxixi0
https://justpaste.it/u/5qqbrcom
https://www.pozible.com/profile/5qqbrcom
https://www.elephantjournal.com/profile/5qqbrcom/
https://strikefans.com/forum/users/5qqbrcom/
https://swat-portal.com/forum/wcf/user/57709-5qqbrcom/#about
http://julia4tied.de/member.php?action=profile&uid=255351
https://stocktwits.com/5qqbrcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5qqbrcom/
https://mercadodinamico.com.br/author/5qqbrcom/
https://www.grabcaruber.com/members/5qqbrcom/profile/
https://qoolink.co/5qqbrcom
https://galleria.emotionflow.com/196484/profile.html
https://www.myget.org/users/5qqbrcom
https://app.brancher.ai/user/2fOVUTfw634I
https://confengine.com/user/5qqbrcom
https://mygamedb.com/profile/5qqbrcom
https://forum.aceinna.com/user/5qqbrcom
https://www.giveawayoftheday.com/forums/profile/1971385
https://uiverse.io/profile/5qqbrcom_2415
https://cofacts.tw/user/5qqbrcom
https://vcook.jp/users/107821
https://www.efunda.com/members/people/show_people.cfm?Usr=5qqbrcom
https://pumpyoursound.com/u/user/1644900
https://congdongx.com/thanh-vien/5qqbrcom.57396/#about
https://www.intensedebate.com/people/nc5qqbrcom
https://www.tkaraoke.com/forums/profile/5qqbrcom/
https://svetelektro.com/clenovia/5qqbrcom/
https://marshmallow-qa.com/1cnpqw3qffhr4ss
https://us.enrollbusiness.com/BusinessProfile/7879899/5qqbrcom
https://link4u.cc/@5qqbrcom
https://its-my.link/@5qqbrcom
https://truckymods.io/user/522986
https://iplogger.org/vn/logger/pDiP583eNhJy/
https://www.iniuria.us/forum/member.php?700938-5qqbrcom
https://cointr.ee/5qqbrcom
https://indian-tv.cz/u/5qqbrcom
https://hedgedoc.envs.net/s/3FURkO2Wt
https://illust.daysneo.com/illustrator/5qqbrcom/
https://hubb.link/5qqbrcom/
https://www.czporadna.cz/user/5qqbrcom
https://tutorialslink.com/member/5qqbrcomundefined/109962
https://expathealthseoul.com/profile/5qqbrcom/
https://expathealthseoul.com/profile/5qqbrcom/
https://www.goodreads.com/user/show/202673360-5qqbrcom-5qq
https://www.abookmarking.com/story/5qqbrcom
https://www.letsdobookmark.com/story/5qqbrcom
https://www.mateball.com/n5qqbrcom
https://raovat.nhadat.vn/members/5qqbrcom-331783.html
https://advego.com/profile/5qqbrcom/
https://www.vnbadminton.com/members/5qqbrcom.89347/
https://www.sunemall.com/board/board_topic/8431232/8671017.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8671018.htm
https://solo.to/5qqbrcom
https://graph.org/5qqbrcom-07-14-2
https://selling.goo.ng/5qqbrcom
https://www.fcc.gov/fcc-bin/bye?https://5qq.br.com/
https://calgarybusinesses.ca/dashboard/reviews/5qqbrcom/
https://www.sciencebee.com.bd/qna/user/5qqbrcom
https://luvly.co/users/5qqbrcom
https://spinninrecords.com/profile/5qqbrcom
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8671039.htm
https://www.tai-ji.net/board/board_topic/4160148/8671050.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8671054.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8671055.htm
https://kheotay.com.vn/forums/users/benbowarmah446
https://crazyservice.by/forum/user/17876/
https://rsfpost.com/forums/users/5qqbrcom/
https://exceldemy.com/forum/members/5qqbrcom.6322/#about
https://www.ontime.co.th/forum/topic/872956/5qqbrcom
https://forum.gettinglost.ca/user/5qqbrcomm
https://zepodcast.com/forums/users/5qqbrcom/
https://monviet88.com/profile/5qqbrcom/
https://www.fuelly.com/driver/5qqbrcom
https://www.physicsoverflow.org/user/5qqbrcom
https://www.spacedesk.net/support-forum/profile/5qqbrcom/
https://pods.link/5qqbrcom
https://mylink.page/5qqbrcom
https://letterboxd.com/5qqbrcom/
https://ctxt.io/3/lyguNLvMc
https://onespotsocial.com/5qqbrcom
https://www.scener.com/@5qqbrcom
https://amaz0ns.com/forums/users/5qqbrcom/
https://hostndobezi.com/5qqbrcom
https://nilechronicles.com/profile/5qqbrcom
https://biiut.com/5qqbrcom
https://www.renderosity.com/users/id:1879799
https://eo-college.org/members/5qqbrcom/
https://www.moshpyt.com/user/5qqbrcom
https://www.racerjobs.com/profiles/8594816-casa-de-apostas-5qq
https://www.instructorsnearme.com/author/5qqbrcom/
https://ferrariformula1.hu/community/profile/5qqbrcom/
https://www.pebforum.com/members/5qqbrcom.262350/#about
http://koloboklinks.com/site?url=5qq.br.com
http://freestyler.ws/user/677387/5qqbrcom
https://jali.me/5qqbrcom
https://bioqoo.com/5qqbrcom
https://ac.db0.company/user/20557/5qqbrcom/
https://www.youyooz.com/profile/5qqbrcom/
https://forum.hiv.plus/user/5qqbrcom
https://www.thitrungruangclinic.com/forum/topic/194377/5qqbrcom
https://ja.cofacts.tw/user/5qqbrcom
https://www.minecraft-servers-list.org/details/5qqbrcom/
https://blog.ulifestyle.com.hk/5qqbrcom
https://baskadia.com/user/h67x
https://buyerseller.xyz/user/5qqbrcom/
https://www.democracylab.org/user/53448
https://vs.cga.gg/user/247634
https://bsky.app/profile/5qqbrcom.bsky.social
https://www.xmonsta.com/forums/users/5qqbrcom/
https://www.green-collar.com/forums/users/5qqbrcom/
https://www.hostboard.com/forums/members/5qqbrcom.html
https://infinitebacklog.net/users/5qqbrcom
https://xmrbazaar.com/user/5qqbrcom/
https://tuscl.net/member/902877
https://sighpceducation.hosting.acm.org/wp/forums/users/5qqbrcom/
https://www.ironlifting.it/forum/member.php?u=437058
https://nogu.org.uk/forum/profile/5qqbrcom/
https://reactormag.com/members/5qqbrcom/profile
https://www.themirch.com/blog/author/5qqbrcom/
https://foss.heptapod.net/5qqbrcom
https://www.euskalmarket.com/author/5qqbrcom/
https://doingbusiness.eu/profile/5qqbrcom/
https://portfolium.com.au/5qqbrcom
https://umczdt.ru/forum/?PAGE_NAME=profile_view&UID=160706
https://ic-info.ru/forum/user/227255/
https://stardust.run/user/177792/5qqbrcom/#preferences
https://mail.tudomuaban.com/chi-tiet-rao-vat/2966474/5qqbrcom.html
https://gamelet.online/user/5qqbrcom
https://www.facer.io/u/5qqbrcom
https://talkmarkets.com/profile/casa-de-apostas-5qq-260715-062419
https://forum.cnnr.fr/user/5qqbrcom
https://jobs.host-panel.com/author/5qqbrcom/
That is very attention-grabbing, You are an overly professional blogger. I’ve joined your rss feed and sit up for in search of more of your magnificent post. Also, I have shared your web site in my social networks!
Your comment is awaiting moderation.
https://www.youtube.com/@5247brcom
https://x.com/5247brcom
https://tooter.in/5247brcom
https://wakelet.com/@5247brcom
https://gravatar.com/5247brcom
https://shareyoursocial.com/5247brcom
https://500px.com/p/5247brcom
https://www.instapaper.com/p/5247brcom
https://protocol.ooo/ja/users/5247brcom
https://audiomack.com/5247brcom
https://hackaday.io/5247brcom
https://fyers.in/community/member/ddPWZ14zJR
https://leetcode.com/u/5247brcom/
https://www.notebook.ai/@5247brcom
https://www.halaltrip.com/user/profile/370049/5247brcom/
https://forums.jetphotos.com/member/56586-5247brcom/about
https://medibang.com/author/28792728/
https://www.blockdit.com/5247brcom
https://portfolium.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://topsitenet.com/profile/5247brcom/2174847/
https://akniga.org/profile/1447271-5247brcom/
https://jobs.suncommunitynews.com/profiles/8601629-casa-de-apostas-5247
https://www.speedrun.com/users/5247brcom
https://pbase.com/5247brcom
https://www.gta5-mods.com/users/5247brcom
https://www.nicovideo.jp/user/144858970
https://www.jigsawplanet.com/5247brcom
https://bit.ly/m/5247brcom
https://5247brcom.blogspot.com/2026/07/5247brcom.html
https://bookmeter.com/users/1748186
https://files.fm/5247brcom/info
https://startupxplore.com/en/person/5247brcom
https://m.xtutti.com/user/profile/497637
https://postr.blog/profile/5247brcom
https://5247brcom.stck.me/profile
https://www.chichi-pui.com/users/5247brcom/
https://www.mellow-fan.com/user/d7ezkk845ni5vwlxr56h/about
https://freeimage.host/5247brcom
https://motion-gallery.net/users/1016085
https://biomolecula.ru/authors/166395
https://www.callupcontact.com/b/businessprofile/5247brcom/10165976
https://www.growkudos.com/profile/casa_de_apostas_5247
https://blender.community/5247brcom/
https://doselect.com/@d6bd4a0d630391041c39b6319
https://matkafasi.com/user/5247brcom
https://allmyfaves.com/5247brcom
https://muare.vn/shop/casa-de-apostas-5247/914390
https://pads.zapf.in/s/ofSdJ9I8cG
https://barcelonadema-participa.cat/profiles/5247brcom/activity
https://pad.libreon.fr/s/xiydzgjOd
https://forum.dmec.vn/index.php?members/5247brcom.210079/#info
https://igli.me/5247brcom
http://delphi.larsbo.org/user/5247brcom
https://oye.participer.lyon.fr/profiles/5247brcom/activity
https://timdaily.vn/members/5247brcom.142372/#about
https://iszene.com/user-363435.html
https://www.theyeshivaworld.com/coffeeroom/users/5247brcom
https://desksnear.me/users/5247brcom
https://www.itchyforum.com/en/member.php?398851-5247brcom
https://able2know.org/user/5247brcom/
http://www.biblesupport.com/user/866066-5247brcom/
https://golosknig.com/profile/5247brcom/
https://awan.pro/forum/user/198307/
https://fortunetelleroracle.com/profile/5247brcom
https://fabble.cc/5247brcom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2580541
https://www.sythe.org/members/5247brcom.2073831/
https://potofu.me/5247brcom
https://transfur.com/Users/a5247brcom
https://github.com/klompie5247brcomnleef-eng
https://hedgedoc.stusta.de/s/RQwMylDIi
https://website.informer.com/5247.br.com
https://notes.stuve.fau.de/s/w2Lyd8nFAo
https://en.islcollective.com/portfolio/12969199
https://velog.io/@5247brcom/about
https://mez.ink/5247brcom
https://www.techbang.com/users/5247brcom
https://freeicons.io/profile/957152
https://onlinesequencer.net/members/294605
https://inkbunny.net/5247brcom
https://www.japaaan.com/user/110718
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5247
https://beatsaver.com/playlists/1235493
https://nyccharterschools.jobboard.io/employers/4255039-5247brcom
https://egl.circlly.com/users/5247brcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319989
https://acomics.ru/-5247brcom
https://www.criminalelement.com/members/5247brcom/profile/
https://hanson.net/users/5247brcom
https://expatguidekorea.com/profile/5247brcom/
https://www.heavyironjobs.com/profiles/8606538-casa-de-apostas-5247
https://git.disroot.org/5247brcom
https://song.link/5247brcom
https://idol.st/user/200813/5247brcom/
https://jobs.windomnews.com/profiles/8606530-casa-de-apostas-5247
https://hoaxbuster.com/redacteur/5247brcom
https://www.givey.com/5247brcom
https://zerosuicidetraining.edc.org/user/profile.php?id=593140
https://jobs.westerncity.com/profiles/8606563-casa-de-apostas-5247
https://www.thetriumphforum.com/members/5247brcom.74091/
https://album.link/5247brcom
http://forum.cncprovn.com/members/437103-5247brcom
https://forum.aigato.vn/user/5247brcom
https://rapidapi.com/user/5247brcom
https://www.skool.com/@casa-de-apostas-2260
http://www.invelos.com/UserProfile.aspx?alias=5247brcom
https://www.rwaq.org/users/5247brcom/
https://www.grepmed.com/5247brcom
https://espritgames.com/members/51952861/
https://www.haikudeck.com/presentations/5247brcom
https://hi-fi-forum.net/profile/1182898
https://te.legra.ph/5247brcom-07-17
https://undrtone.com/5247brcom
https://marshallyin.com/members/5247brcom/
https://gravesales.com/author/5247brcom/
https://belgaumonline.com/profile/5247brcom/
https://savelist.co/my-lists/users/5247brcom
https://zzb.bz/5247brcom
https://www.themeqx.com/forums/users/5247brcom/
http://newdigital-world.com/members/5247brcom.html
https://activepages.com.au/profile/5247brcom
https://snippet.host/fczvkq
https://tudomuaban.com/chi-tiet-rao-vat/2968769/5247brcom.html
https://phijkchu.com/a/5247brcom/video-channels
https://lifeinsys.com/user/5247brcom
https://kaeuchi.jp/forums/users/5247brcom/
https://www.claimajob.com/profiles/8607011-casa-de-apostas-5247
https://protospielsouth.com/user/155253
https://theafricavoice.com/profile/5247brcom
https://www.brownbook.net/business/55324163/5247brcom
https://app.hellothematic.com/creator/profile/1167649
https://hackmd.okfn.de/s/rky9tLPEfl
https://manylink.co/@5247brcom
https://www.akaqa.com/question/q19192717303-5247brcom
https://www.threadless.com/@5247brcom/activity
https://maxforlive.com/profile/user/5247brcom?tab=about
https://mathlog.info/users/fleJrzFiDzfiANlcuNO1IT0ZyS33
https://nous.malakoff.fr/profiles/5247brcom/activity
https://fora.babinet.cz/profile.php?section=personal&id=136400
https://www.shippingexplorer.net/en/user/5247brcom/314247
https://www.sunlitcentrekenya.co.ke/author/5247brcom/
https://www.lingvolive.com/en-us/profile/c2d4aa44-bd42-4b44-8fec-f46d638af526/translations
https://www.zubersoft.com/mobilesheets/forum/user-152400.html
https://md.coredump.ch/s/YigPY8RIC
https://aprenderfotografia.online/usuarios/5247brcom/profile/
https://hackmd.hub.yt/s/7riUvbwna
https://lqdoj.edu.vn/user/5247brcom
https://sciencemission.com/profile/5247brcom
https://www.wvhired.com/profiles/8608508-casa-de-apostas-5247
https://formulamasa.com/elearning/members/5247brcom/?v=96b62e1dce57
https://eilo.org/users-view.php?id=92233
https://backloggd.com/u/5247brcom/
https://forums.alliedmods.net/member.php?u=489457
http://forum.modulebazaar.com/forums/user/5247brcom/
https://viblo.asia/u/5247brcom/contact
https://brain-market.com/u/5247brcom
https://www.prosebox.net/book/120497/
https://www.fw-follow.com/forum/topic/162571/5247brcom
https://www.navacool.com/forum/topic/533381/5247brcom
https://www.driedsquidathome.com/forum/topic/192362/5247brcom
https://www.nongkhaempolice.com/forum/topic/196751/5247brcom
https://www.bestloveweddingstudio.com/forum/topic/118595/5247brcom
https://www.natthadon-sanengineering.com/forum/topic/147876/5247brcom
https://www.rueanmaihom.net/forum/topic/134707/5247brcom
https://www.ttlxshipping.com/forum/topic/533382/5247brcom
http://worldchampmambo.com/UserProfile/tabid/42/UserID/507470/Default.aspx
https://www.horticulturaljobs.com/employers/4255976-5247brcom
https://jobs.siliconflorist.com/employers/4255977-5247brcom
https://jobs.nefeshinternational.org/employers/4255978-5247brcom
https://forum.issabel.org/u/5247brcom
https://doc.anagora.org/s/Sleaw9pdD
https://profile.sampo.ru/a5247brcom
https://www.ekdarun.com/forum/topic/190801/5247brcom
https://fanclove.jp/profile/wyWeNgMEB0
https://www.d-ushop.com/forum/topic/192471/5247brcom
https://findaspring.org/members/5247brcom/
https://ketcau.com/member/135620-5247brcom/activities
https://library.zortrax.com/members/5247brcom/
https://pets4friends.com/profile-1665303
https://participa.aytojaen.es/profiles/5247brcom/activity
https://linkmix.co/57351495
https://www.maanation.com/5247brcom
https://janitorai.com/profiles/40bc3155-3ec0-4481-8a64-0040a1a3ae01_profile-of-5247-brcom
https://www.buymusic.club/user/5247brcom
http://iawbs.com/home.php?mod=space&uid=971405
https://participation.bordeaux.fr/profiles/5247brcom/activity
http://genina.com/user/editDone/5475210.page
https://pad.lescommuns.org/s/nblnOWkkL
https://chanylib.ru/ru/forum/user/36587/
https://producerbox.com/users/5247brcom
https://skrolli.fi/keskustelu/users/KlompienLeef/
https://www.thehockeypaper.co.uk/forums/users/5247brcom
https://zbrushcentral.jp/user/5247brcom
https://www.mapleprimes.com/users/5247brcom
https://guitarmaking.co.uk/members/5247brcom/
https://scrapbox.io/5247brcom/5247brcom
https://qiita.com/5247brcom
https://www.annuncigratuititalia.it/author/5247brcom/
https://lite.link/5247brcom
http://www.brenkoweb.com/user/102367/profile
https://www.rossoneriblog.com/author/5247brcom/
https://anunt-imob.ro/user/profile/868311
https://destaquebrasil.com/saopaulo/author/5247brcom/
https://bhmtsff.com/space-uid-99259.html
https://blog.sighpceducation.acm.org/wp/forums/users/5247brcom/
https://pad.libreon.fr/s/d4uET4d2b
https://vc.ru/id6045985
https://artist.link/5247brcom
https://backloggery.com/5247brcom
http://palangshim.com/space-uid-5356578.html
https://etextpad.com/osr0o41ikr
https://app.talkshoe.com/user/5247brcom
https://sfx.thelazy.net/users/u/5247brcom/
https://www.skypixel.com/users/djiuser-o63vncakbyxd
https://pictureinbottle.com/r/2dhuqx6j
https://md.openbikesensor.org/s/iYcH2P7HML
https://pad.codefor.fr/s/jTmrpReIcs
https://www.hogwartsishere.com/profile/1856655/
https://www.plotterusati.it/user/5247brcom
https://linqto.me/about/5247brcom
https://partecipa.poliste.com/profiles/5247brcom/activity
https://hedgedoc.stusta.de/s/9lKLPbutG
https://pad.codefor.fr/s/TAOr9Vq1Kt
https://pad.fablab-siegen.de/s/Dvg1Xq76zE
https://referrallist.com/profile/5247brcom/
https://pad.darmstadt.social/s/iogWv5UiVx
https://www.iglinks.io/KlompienLeef-zr7
https://homepage.ninja/5247brcom
https://md.rappet.xyz/s/dQJT1-41mf
https://md.sebastians.dev/s/iv4lFiWM-
https://controlc.com/lagcucn0
https://justpaste.it/u/5247brcom
https://www.pozible.com/profile/casa-de-apostas-5247
https://strikefans.com/forum/users/5247brcom/
https://experiment.com/users/5247brcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5247brcom/
https://doc.anagora.org/s/maPB95_YL
https://www.grabcaruber.com/members/5247brcom/profile/
https://bike-forum.cz/profil/u/5247brcom
https://galleria.emotionflow.com/196984/profile.html
https://www.myget.org/users/5247brcom
https://app.brancher.ai/user/7wKHr1JHHapQ
https://forum.aceinna.com/user/5247brcom
https://www.giveawayoftheday.com/forums/profile/2003569?updated=true
https://uiverse.io/profile/casadeapos_9437
https://cofacts.tw/user/5247brcom
https://vcook.jp/users/108579
https://pumpyoursound.com/u/user/1654786
https://doc.adminforge.de/s/Fl7LgoVLdz
https://tabelog.com/rvwr/034748578/prof/
https://app.parler.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://gamblingtherapy.org/forum/users/5247brcom/
https://marshmallow-qa.com/43ian8u2sjtb1tz
https://us.enrollbusiness.com/BusinessProfile/7884072/5247brcom
https://its-my.link/@5247brcom
https://writeablog.net/bopeaqv8vb
https://cointr.ee/5247brcom
https://aniworld.to/user/profil/5247brcom
https://hedgedoc.dezentrale.space/s/CWlysrHpc
https://official.link/5247brcom
https://www.czporadna.cz/user/5247brcom/wall
https://tealfeed.com/brcom5247
https://expathealthseoul.com/profile/5247brcom/
https://www.rctech.net/forum/members/5247brcom-560430.html
https://www.mateball.com/brcom5247
https://ofuse.me/e/390987
http://kjtr.grrr.jp/kjtr/?5247brcom
https://raovat.nhadat.vn/members/5247brcom-332484.html
https://advego.com/profile/5247brcom/
https://bio.site/5247brcom
https://www.vnbadminton.com/members/5247brcom.89774/
https://gourmet-calendar.com/users/5247brcom
https://www.sunemall.com/board/board_topic/8431232/8679443.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8679449.htm
https://cars.yclas.com/user/5247brcom
https://calgarybusinesses.ca/dashboard/reviews/5247brcom/
https://www.sciencebee.com.bd/qna/user/5247brcom
https://www.biblicaleldership.com/forums/users/5247brcom/
https://luvly.co/users/5247brcom
https://spinninrecords.com/profile/5247brcom
https://zenwriting.net/1pq4u67k1e
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8679459.htm
https://www.tai-ji.net/board/board_topic/4160148/8679578.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8679590.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8679595.htm
https://kheotay.com.vn/forums/users/KlompienLeef
https://alfounder.com/forums/users/5247brcom/
https://crazyservice.by/forum/user/18015/
https://rsfpost.com/forums/users/5247brcom/
https://www.ontime.co.th/forum/topic/874483/5247brcom
https://forum.gettinglost.ca/user/5247brcom
https://zepodcast.com/forums/users/5247brcom/
http://jobs.emiogp.com/author/5247brcom/
https://wikimapia.org/external_link?url=https://5247.br.com/
https://monviet88.com/profile/5247brcom/
https://onlinevetjobs.com/author/5247brcom/
https://rush1989.rash.jp/pukiwiki/index.php?5247brcom
https://www.fuelly.com/driver/5247brcom
https://www.beamng.com/members/5247brcom.811968/
https://www.spacedesk.net/support-forum/profile/5247brcom/
https://log.concept2.com/profile/3004932
https://playlist.link/5247brcom
https://pods.link/5247brcom
https://mylink.page/5247brcom
https://md.coredump.ch/s/6IYxrZ6JK
https://ctxt.io/3/odsUrJuQE
https://5247brcom.gitbook.io/5247brcom-docs/
https://6a5a368b1f7d2.site123.me/
https://casadeapostas5247.website3.me/
https://onespotsocial.com/5247brcom
https://www.scener.com/@5247brcom
https://amaz0ns.com/forums/users/5247brcom/
https://hostndobezi.com/5247brcom
https://nilechronicles.com/profile/5247brcom
https://paper.wf/5247brcom/5247brcom
https://devfolio.co/@5247brcom/readme-md
https://wibki.com/5247brcom
https://www.renderosity.com/users/id:1880858
https://eo-college.org/members/5247brcom/
https://ivpaste.com/v/rudQsj1MfZ
https://www.moshpyt.com/user/5247brcom
https://www.racerjobs.com/profiles/8610980-casa-de-apostas-5247
https://www.instructorsnearme.com/author/5247brcom/
https://www.yumpu.com/user/5247brcom
https://ferrariformula1.hu/community/profile/5247brcom/
http://koloboklinks.com/site?url=5247.br.com
https://biolinky.co/5247-brcom
https://md.chaospott.de/s/KT9bKF0si-
https://allmy.bio/5247brcom
https://whatson.plus/5247brcom
https://www.aviacionargentina.net/user/5247brcom
https://ac.db0.company/user/23498/5247brcom/
https://forum.hiv.plus/user/5247brcom
https://www.adminer.org/redirect/?lang=en&url=https://5247.br.com/
https://aboutcasemanagerjobs.com/author/5247brcom/
https://fr.islcollective.com/portfolio/12969199
https://es.islcollective.com/portafolio/12969199
https://www.minecraft-servers-list.org/details/5247brcom/
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://5247.br.com/
https://baskadia.com/user/h6va
https://decidim.calafell.cat/profiles/5247brcom/activity
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://5247.br.com/
https://vs.cga.gg/user/247939
https://www.fitlynk.com/ed5823912
https://bsky.app/profile/5247brcom.bsky.social
https://www.xmonsta.com/forums/users/5247brcom/
https://mail.londonchinese.com/home.php?mod=space&uid=628765&do=index
https://pimrec.pnu.edu.ua/members/5247brcom/profile/
https://www.hostboard.com/forums/members/5247brcom.html
https://forum.euro-pvp.com/user/593683-5247brcom/
http://byltz.com/home.php?mod=space&uid=484260
https://buyandsellhair.com/author/5247brcom/
https://sighpceducation.hosting.acm.org/wp/forums/users/5247brcom/
https://nogu.org.uk/forum/profile/5247brcom/
https://gitflic.ru/user/5247brcom
https://cornucopia.se/author/5247brcom/
http://mura.hitobashira.org/index.php?5247brcom
https://foss.heptapod.net/5247brcom
https://www.empregosaude.pt/en/author/5247brcom/
https://www.euskalmarket.com/author/5247brcom/
https://doingbusiness.eu/profile/5247brcom/
https://portfolium.com.au/5247brcom
https://www.tizmos.com/5247brcom/
https://jobs.lajobsportal.org/profiles/8611331-casa-de-apostas-5247
https://gamelet.online/user/114696621103424895842@google/about
https://www.facer.io/u/5247brcom
https://www.cryptoispy.com/forums/users/5247brcom/
https://forum.cnnr.fr/user/5247brcom
https://usabbs.org/home.php?mod=space&uid=91093
https://jobs.host-panel.com/author/5247brcom/
https://lankadevelopers.lk/user/5247brcom
https://sistacafe.com/user/620144
http://bbs.medicalforum.cn/home.php?mod=space&uid=2415033
https://www.hardmcasual.net/user/2370/
https://www.camtation.com/leden/5247brcom/profile/
http://www.webclap.com/php/jump.php?url=https://5247.br.com/
https://fueler.io/5247brcom
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=4021420
https://paidforarticles.in/author/5247brcom
https://biashara.co.ke/author/5247brcom/
https://feyenoord.supporters.nl/profiel/165057/5247brcom
https://zb3.org/5247brcom/5247brcom
https://everbookforever.com/share/profile/5247brcom/
https://shorturl.at/kQ1gy
https://hashnode.com/@5247brcom
https://nhattao.com/members/user7010750.7010750/
https://morguefile.com/creative/5247brcom
https://edabit.com/user/GKqACMbvbHedavbxQ
https://securityheaders.com/?q=https://5247.br.com/
https://md.darmstadt.ccc.de/s/16gHpPsJLI
https://www.pdc.edu/?URL=https://5247.br.com/
https://ask.mallaky.com/?qa=user/5247brcom
https://www.depechemode.cz/?URL=https://5247.br.com/
https://staroetv.su/go?https://5247.br.com/
https://road-to-eden.com/index.php?5247brcom
https://www.pintradingdb.com/forum/member.php?action=profile&uid=152621
https://pledgeme.co.nz/profiles/352850/
https://www.templepurohit.com/forums/users/KlompienLeef/
https://hedgedoc.logilab.fr/s/Srg2ZMslG
https://entre-vos-mains.alsace.eu/profiles/5247brcom
https://ixawiki.com/link.php?url=https://5247.br.com/
https://game8.jp/users/523389
https://www.vid419.com/home.php?mod=space&uid=3501463
http://jobboard.piasd.org/author/5247brcom/
https://www.okaywan.com/home.php?mod=space&uid=827545
http://tkdlab.com/wiki/index.php?5247brcom
https://volleypedia.org/index.php?qa=user&qa_1=5247brcom
http://pcsq28.com/home.php?mod=space&uid=2336679
https://bbs.airav.cc/home.php?mod=space&uid=4802224
https://pad.funkwhale.audio/s/tIlVUmQrD
https://forum.dfwmas.org/index.php?members/5247brcom.210566/
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=535253
https://bbs.darkml.net/home.php?mod=space&uid=226391
https://www.play56.net/home.php?mod=space&uid=6389200
Your comment is awaiting moderation.
https://www.youtube.com/@5247brcom
https://x.com/5247brcom
https://tooter.in/5247brcom
https://wakelet.com/@5247brcom
https://gravatar.com/5247brcom
https://shareyoursocial.com/5247brcom
https://500px.com/p/5247brcom
https://www.instapaper.com/p/5247brcom
https://protocol.ooo/ja/users/5247brcom
https://audiomack.com/5247brcom
https://hackaday.io/5247brcom
https://fyers.in/community/member/ddPWZ14zJR
https://leetcode.com/u/5247brcom/
https://www.notebook.ai/@5247brcom
https://www.halaltrip.com/user/profile/370049/5247brcom/
https://forums.jetphotos.com/member/56586-5247brcom/about
https://medibang.com/author/28792728/
https://www.blockdit.com/5247brcom
https://portfolium.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://topsitenet.com/profile/5247brcom/2174847/
https://akniga.org/profile/1447271-5247brcom/
https://jobs.suncommunitynews.com/profiles/8601629-casa-de-apostas-5247
https://www.speedrun.com/users/5247brcom
https://pbase.com/5247brcom
https://www.gta5-mods.com/users/5247brcom
https://www.nicovideo.jp/user/144858970
https://www.jigsawplanet.com/5247brcom
https://bit.ly/m/5247brcom
https://5247brcom.blogspot.com/2026/07/5247brcom.html
https://bookmeter.com/users/1748186
https://files.fm/5247brcom/info
https://startupxplore.com/en/person/5247brcom
https://m.xtutti.com/user/profile/497637
https://postr.blog/profile/5247brcom
https://5247brcom.stck.me/profile
https://www.chichi-pui.com/users/5247brcom/
https://www.mellow-fan.com/user/d7ezkk845ni5vwlxr56h/about
https://freeimage.host/5247brcom
https://motion-gallery.net/users/1016085
https://biomolecula.ru/authors/166395
https://www.callupcontact.com/b/businessprofile/5247brcom/10165976
https://www.growkudos.com/profile/casa_de_apostas_5247
https://blender.community/5247brcom/
https://doselect.com/@d6bd4a0d630391041c39b6319
https://matkafasi.com/user/5247brcom
https://allmyfaves.com/5247brcom
https://muare.vn/shop/casa-de-apostas-5247/914390
https://pads.zapf.in/s/ofSdJ9I8cG
https://barcelonadema-participa.cat/profiles/5247brcom/activity
https://pad.libreon.fr/s/xiydzgjOd
https://forum.dmec.vn/index.php?members/5247brcom.210079/#info
https://igli.me/5247brcom
http://delphi.larsbo.org/user/5247brcom
https://oye.participer.lyon.fr/profiles/5247brcom/activity
https://timdaily.vn/members/5247brcom.142372/#about
https://iszene.com/user-363435.html
https://www.theyeshivaworld.com/coffeeroom/users/5247brcom
https://desksnear.me/users/5247brcom
https://www.itchyforum.com/en/member.php?398851-5247brcom
https://able2know.org/user/5247brcom/
http://www.biblesupport.com/user/866066-5247brcom/
https://golosknig.com/profile/5247brcom/
https://awan.pro/forum/user/198307/
https://fortunetelleroracle.com/profile/5247brcom
https://fabble.cc/5247brcom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2580541
https://www.sythe.org/members/5247brcom.2073831/
https://potofu.me/5247brcom
https://transfur.com/Users/a5247brcom
https://github.com/klompie5247brcomnleef-eng
https://hedgedoc.stusta.de/s/RQwMylDIi
https://website.informer.com/5247.br.com
https://notes.stuve.fau.de/s/w2Lyd8nFAo
https://en.islcollective.com/portfolio/12969199
https://velog.io/@5247brcom/about
https://mez.ink/5247brcom
https://www.techbang.com/users/5247brcom
https://freeicons.io/profile/957152
https://onlinesequencer.net/members/294605
https://inkbunny.net/5247brcom
https://www.japaaan.com/user/110718
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5247
https://beatsaver.com/playlists/1235493
https://nyccharterschools.jobboard.io/employers/4255039-5247brcom
https://egl.circlly.com/users/5247brcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319989
https://acomics.ru/-5247brcom
https://www.criminalelement.com/members/5247brcom/profile/
https://hanson.net/users/5247brcom
https://expatguidekorea.com/profile/5247brcom/
https://www.heavyironjobs.com/profiles/8606538-casa-de-apostas-5247
https://git.disroot.org/5247brcom
https://song.link/5247brcom
https://idol.st/user/200813/5247brcom/
https://jobs.windomnews.com/profiles/8606530-casa-de-apostas-5247
https://hoaxbuster.com/redacteur/5247brcom
https://www.givey.com/5247brcom
https://zerosuicidetraining.edc.org/user/profile.php?id=593140
https://jobs.westerncity.com/profiles/8606563-casa-de-apostas-5247
https://www.thetriumphforum.com/members/5247brcom.74091/
https://album.link/5247brcom
http://forum.cncprovn.com/members/437103-5247brcom
https://forum.aigato.vn/user/5247brcom
https://rapidapi.com/user/5247brcom
https://www.skool.com/@casa-de-apostas-2260
http://www.invelos.com/UserProfile.aspx?alias=5247brcom
https://www.rwaq.org/users/5247brcom/
https://www.grepmed.com/5247brcom
https://espritgames.com/members/51952861/
https://www.haikudeck.com/presentations/5247brcom
https://hi-fi-forum.net/profile/1182898
https://te.legra.ph/5247brcom-07-17
https://undrtone.com/5247brcom
https://marshallyin.com/members/5247brcom/
https://gravesales.com/author/5247brcom/
https://belgaumonline.com/profile/5247brcom/
https://savelist.co/my-lists/users/5247brcom
https://zzb.bz/5247brcom
https://www.themeqx.com/forums/users/5247brcom/
http://newdigital-world.com/members/5247brcom.html
https://activepages.com.au/profile/5247brcom
https://snippet.host/fczvkq
https://tudomuaban.com/chi-tiet-rao-vat/2968769/5247brcom.html
https://phijkchu.com/a/5247brcom/video-channels
https://lifeinsys.com/user/5247brcom
https://kaeuchi.jp/forums/users/5247brcom/
https://www.claimajob.com/profiles/8607011-casa-de-apostas-5247
https://protospielsouth.com/user/155253
https://theafricavoice.com/profile/5247brcom
https://www.brownbook.net/business/55324163/5247brcom
https://app.hellothematic.com/creator/profile/1167649
https://hackmd.okfn.de/s/rky9tLPEfl
https://manylink.co/@5247brcom
https://www.akaqa.com/question/q19192717303-5247brcom
https://www.threadless.com/@5247brcom/activity
https://maxforlive.com/profile/user/5247brcom?tab=about
https://mathlog.info/users/fleJrzFiDzfiANlcuNO1IT0ZyS33
https://nous.malakoff.fr/profiles/5247brcom/activity
https://fora.babinet.cz/profile.php?section=personal&id=136400
https://www.shippingexplorer.net/en/user/5247brcom/314247
https://www.sunlitcentrekenya.co.ke/author/5247brcom/
https://www.lingvolive.com/en-us/profile/c2d4aa44-bd42-4b44-8fec-f46d638af526/translations
https://www.zubersoft.com/mobilesheets/forum/user-152400.html
https://md.coredump.ch/s/YigPY8RIC
https://aprenderfotografia.online/usuarios/5247brcom/profile/
https://hackmd.hub.yt/s/7riUvbwna
https://lqdoj.edu.vn/user/5247brcom
https://sciencemission.com/profile/5247brcom
https://www.wvhired.com/profiles/8608508-casa-de-apostas-5247
https://formulamasa.com/elearning/members/5247brcom/?v=96b62e1dce57
https://eilo.org/users-view.php?id=92233
https://backloggd.com/u/5247brcom/
https://forums.alliedmods.net/member.php?u=489457
http://forum.modulebazaar.com/forums/user/5247brcom/
https://viblo.asia/u/5247brcom/contact
https://brain-market.com/u/5247brcom
https://www.prosebox.net/book/120497/
https://www.fw-follow.com/forum/topic/162571/5247brcom
https://www.navacool.com/forum/topic/533381/5247brcom
https://www.driedsquidathome.com/forum/topic/192362/5247brcom
https://www.nongkhaempolice.com/forum/topic/196751/5247brcom
https://www.bestloveweddingstudio.com/forum/topic/118595/5247brcom
https://www.natthadon-sanengineering.com/forum/topic/147876/5247brcom
https://www.rueanmaihom.net/forum/topic/134707/5247brcom
https://www.ttlxshipping.com/forum/topic/533382/5247brcom
http://worldchampmambo.com/UserProfile/tabid/42/UserID/507470/Default.aspx
https://www.horticulturaljobs.com/employers/4255976-5247brcom
https://jobs.siliconflorist.com/employers/4255977-5247brcom
https://jobs.nefeshinternational.org/employers/4255978-5247brcom
https://forum.issabel.org/u/5247brcom
https://doc.anagora.org/s/Sleaw9pdD
https://profile.sampo.ru/a5247brcom
https://www.ekdarun.com/forum/topic/190801/5247brcom
https://fanclove.jp/profile/wyWeNgMEB0
https://www.d-ushop.com/forum/topic/192471/5247brcom
https://findaspring.org/members/5247brcom/
https://ketcau.com/member/135620-5247brcom/activities
https://library.zortrax.com/members/5247brcom/
https://pets4friends.com/profile-1665303
https://participa.aytojaen.es/profiles/5247brcom/activity
https://linkmix.co/57351495
https://www.maanation.com/5247brcom
https://janitorai.com/profiles/40bc3155-3ec0-4481-8a64-0040a1a3ae01_profile-of-5247-brcom
https://www.buymusic.club/user/5247brcom
http://iawbs.com/home.php?mod=space&uid=971405
https://participation.bordeaux.fr/profiles/5247brcom/activity
http://genina.com/user/editDone/5475210.page
https://pad.lescommuns.org/s/nblnOWkkL
https://chanylib.ru/ru/forum/user/36587/
https://producerbox.com/users/5247brcom
https://skrolli.fi/keskustelu/users/KlompienLeef/
https://www.thehockeypaper.co.uk/forums/users/5247brcom
https://zbrushcentral.jp/user/5247brcom
https://www.mapleprimes.com/users/5247brcom
https://guitarmaking.co.uk/members/5247brcom/
https://scrapbox.io/5247brcom/5247brcom
https://qiita.com/5247brcom
https://www.annuncigratuititalia.it/author/5247brcom/
https://lite.link/5247brcom
http://www.brenkoweb.com/user/102367/profile
https://www.rossoneriblog.com/author/5247brcom/
https://anunt-imob.ro/user/profile/868311
https://destaquebrasil.com/saopaulo/author/5247brcom/
https://bhmtsff.com/space-uid-99259.html
https://blog.sighpceducation.acm.org/wp/forums/users/5247brcom/
https://pad.libreon.fr/s/d4uET4d2b
https://vc.ru/id6045985
https://artist.link/5247brcom
https://backloggery.com/5247brcom
http://palangshim.com/space-uid-5356578.html
https://etextpad.com/osr0o41ikr
https://app.talkshoe.com/user/5247brcom
https://sfx.thelazy.net/users/u/5247brcom/
https://www.skypixel.com/users/djiuser-o63vncakbyxd
https://pictureinbottle.com/r/2dhuqx6j
https://md.openbikesensor.org/s/iYcH2P7HML
https://pad.codefor.fr/s/jTmrpReIcs
https://www.hogwartsishere.com/profile/1856655/
https://www.plotterusati.it/user/5247brcom
https://linqto.me/about/5247brcom
https://partecipa.poliste.com/profiles/5247brcom/activity
https://hedgedoc.stusta.de/s/9lKLPbutG
https://pad.codefor.fr/s/TAOr9Vq1Kt
https://pad.fablab-siegen.de/s/Dvg1Xq76zE
https://referrallist.com/profile/5247brcom/
https://pad.darmstadt.social/s/iogWv5UiVx
https://www.iglinks.io/KlompienLeef-zr7
https://homepage.ninja/5247brcom
https://md.rappet.xyz/s/dQJT1-41mf
https://md.sebastians.dev/s/iv4lFiWM-
https://controlc.com/lagcucn0
https://justpaste.it/u/5247brcom
https://www.pozible.com/profile/casa-de-apostas-5247
https://strikefans.com/forum/users/5247brcom/
https://experiment.com/users/5247brcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5247brcom/
https://doc.anagora.org/s/maPB95_YL
https://www.grabcaruber.com/members/5247brcom/profile/
https://bike-forum.cz/profil/u/5247brcom
https://galleria.emotionflow.com/196984/profile.html
https://www.myget.org/users/5247brcom
https://app.brancher.ai/user/7wKHr1JHHapQ
https://forum.aceinna.com/user/5247brcom
https://www.giveawayoftheday.com/forums/profile/2003569?updated=true
https://uiverse.io/profile/casadeapos_9437
https://cofacts.tw/user/5247brcom
https://vcook.jp/users/108579
https://pumpyoursound.com/u/user/1654786
https://doc.adminforge.de/s/Fl7LgoVLdz
https://tabelog.com/rvwr/034748578/prof/
https://app.parler.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://gamblingtherapy.org/forum/users/5247brcom/
https://marshmallow-qa.com/43ian8u2sjtb1tz
https://us.enrollbusiness.com/BusinessProfile/7884072/5247brcom
https://its-my.link/@5247brcom
https://writeablog.net/bopeaqv8vb
https://cointr.ee/5247brcom
https://aniworld.to/user/profil/5247brcom
https://hedgedoc.dezentrale.space/s/CWlysrHpc
https://official.link/5247brcom
https://www.czporadna.cz/user/5247brcom/wall
https://tealfeed.com/brcom5247
https://expathealthseoul.com/profile/5247brcom/
https://www.rctech.net/forum/members/5247brcom-560430.html
https://www.mateball.com/brcom5247
https://ofuse.me/e/390987
http://kjtr.grrr.jp/kjtr/?5247brcom
https://raovat.nhadat.vn/members/5247brcom-332484.html
https://advego.com/profile/5247brcom/
https://bio.site/5247brcom
https://www.vnbadminton.com/members/5247brcom.89774/
https://gourmet-calendar.com/users/5247brcom
https://www.sunemall.com/board/board_topic/8431232/8679443.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8679449.htm
https://cars.yclas.com/user/5247brcom
https://calgarybusinesses.ca/dashboard/reviews/5247brcom/
https://www.sciencebee.com.bd/qna/user/5247brcom
https://www.biblicaleldership.com/forums/users/5247brcom/
https://luvly.co/users/5247brcom
https://spinninrecords.com/profile/5247brcom
https://zenwriting.net/1pq4u67k1e
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8679459.htm
https://www.tai-ji.net/board/board_topic/4160148/8679578.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8679590.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8679595.htm
https://kheotay.com.vn/forums/users/KlompienLeef
https://alfounder.com/forums/users/5247brcom/
https://crazyservice.by/forum/user/18015/
https://rsfpost.com/forums/users/5247brcom/
https://www.ontime.co.th/forum/topic/874483/5247brcom
https://forum.gettinglost.ca/user/5247brcom
https://zepodcast.com/forums/users/5247brcom/
http://jobs.emiogp.com/author/5247brcom/
https://wikimapia.org/external_link?url=https://5247.br.com/
https://monviet88.com/profile/5247brcom/
https://onlinevetjobs.com/author/5247brcom/
https://rush1989.rash.jp/pukiwiki/index.php?5247brcom
https://www.fuelly.com/driver/5247brcom
https://www.beamng.com/members/5247brcom.811968/
https://www.spacedesk.net/support-forum/profile/5247brcom/
https://log.concept2.com/profile/3004932
https://playlist.link/5247brcom
https://pods.link/5247brcom
https://mylink.page/5247brcom
https://md.coredump.ch/s/6IYxrZ6JK
https://ctxt.io/3/odsUrJuQE
https://5247brcom.gitbook.io/5247brcom-docs/
https://6a5a368b1f7d2.site123.me/
https://casadeapostas5247.website3.me/
https://onespotsocial.com/5247brcom
https://www.scener.com/@5247brcom
https://amaz0ns.com/forums/users/5247brcom/
https://hostndobezi.com/5247brcom
https://nilechronicles.com/profile/5247brcom
https://paper.wf/5247brcom/5247brcom
https://devfolio.co/@5247brcom/readme-md
https://wibki.com/5247brcom
https://www.renderosity.com/users/id:1880858
https://eo-college.org/members/5247brcom/
https://ivpaste.com/v/rudQsj1MfZ
https://www.moshpyt.com/user/5247brcom
https://www.racerjobs.com/profiles/8610980-casa-de-apostas-5247
https://www.instructorsnearme.com/author/5247brcom/
https://www.yumpu.com/user/5247brcom
https://ferrariformula1.hu/community/profile/5247brcom/
http://koloboklinks.com/site?url=5247.br.com
https://biolinky.co/5247-brcom
https://md.chaospott.de/s/KT9bKF0si-
https://allmy.bio/5247brcom
https://whatson.plus/5247brcom
https://www.aviacionargentina.net/user/5247brcom
https://ac.db0.company/user/23498/5247brcom/
https://forum.hiv.plus/user/5247brcom
https://www.adminer.org/redirect/?lang=en&url=https://5247.br.com/
https://aboutcasemanagerjobs.com/author/5247brcom/
https://fr.islcollective.com/portfolio/12969199
https://es.islcollective.com/portafolio/12969199
https://www.minecraft-servers-list.org/details/5247brcom/
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://5247.br.com/
https://baskadia.com/user/h6va
https://decidim.calafell.cat/profiles/5247brcom/activity
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://5247.br.com/
https://vs.cga.gg/user/247939
https://www.fitlynk.com/ed5823912
https://bsky.app/profile/5247brcom.bsky.social
https://www.xmonsta.com/forums/users/5247brcom/
https://mail.londonchinese.com/home.php?mod=space&uid=628765&do=index
https://pimrec.pnu.edu.ua/members/5247brcom/profile/
https://www.hostboard.com/forums/members/5247brcom.html
https://forum.euro-pvp.com/user/593683-5247brcom/
http://byltz.com/home.php?mod=space&uid=484260
https://buyandsellhair.com/author/5247brcom/
https://sighpceducation.hosting.acm.org/wp/forums/users/5247brcom/
https://nogu.org.uk/forum/profile/5247brcom/
https://gitflic.ru/user/5247brcom
https://cornucopia.se/author/5247brcom/
http://mura.hitobashira.org/index.php?5247brcom
https://foss.heptapod.net/5247brcom
https://www.empregosaude.pt/en/author/5247brcom/
https://www.euskalmarket.com/author/5247brcom/
https://doingbusiness.eu/profile/5247brcom/
https://portfolium.com.au/5247brcom
https://www.tizmos.com/5247brcom/
https://jobs.lajobsportal.org/profiles/8611331-casa-de-apostas-5247
https://gamelet.online/user/114696621103424895842@google/about
https://www.facer.io/u/5247brcom
https://www.cryptoispy.com/forums/users/5247brcom/
https://forum.cnnr.fr/user/5247brcom
https://usabbs.org/home.php?mod=space&uid=91093
https://jobs.host-panel.com/author/5247brcom/
https://lankadevelopers.lk/user/5247brcom
https://sistacafe.com/user/620144
http://bbs.medicalforum.cn/home.php?mod=space&uid=2415033
https://www.hardmcasual.net/user/2370/
https://www.camtation.com/leden/5247brcom/profile/
http://www.webclap.com/php/jump.php?url=https://5247.br.com/
https://fueler.io/5247brcom
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=4021420
https://paidforarticles.in/author/5247brcom
https://biashara.co.ke/author/5247brcom/
https://feyenoord.supporters.nl/profiel/165057/5247brcom
https://zb3.org/5247brcom/5247brcom
https://everbookforever.com/share/profile/5247brcom/
https://shorturl.at/kQ1gy
https://hashnode.com/@5247brcom
https://nhattao.com/members/user7010750.7010750/
https://morguefile.com/creative/5247brcom
https://edabit.com/user/GKqACMbvbHedavbxQ
https://securityheaders.com/?q=https://5247.br.com/
https://md.darmstadt.ccc.de/s/16gHpPsJLI
https://www.pdc.edu/?URL=https://5247.br.com/
https://ask.mallaky.com/?qa=user/5247brcom
https://www.depechemode.cz/?URL=https://5247.br.com/
https://staroetv.su/go?https://5247.br.com/
https://road-to-eden.com/index.php?5247brcom
https://www.pintradingdb.com/forum/member.php?action=profile&uid=152621
https://pledgeme.co.nz/profiles/352850/
https://www.templepurohit.com/forums/users/KlompienLeef/
https://hedgedoc.logilab.fr/s/Srg2ZMslG
https://entre-vos-mains.alsace.eu/profiles/5247brcom
https://ixawiki.com/link.php?url=https://5247.br.com/
https://game8.jp/users/523389
https://www.vid419.com/home.php?mod=space&uid=3501463
http://jobboard.piasd.org/author/5247brcom/
https://www.okaywan.com/home.php?mod=space&uid=827545
http://tkdlab.com/wiki/index.php?5247brcom
https://volleypedia.org/index.php?qa=user&qa_1=5247brcom
http://pcsq28.com/home.php?mod=space&uid=2336679
https://bbs.airav.cc/home.php?mod=space&uid=4802224
https://pad.funkwhale.audio/s/tIlVUmQrD
https://forum.dfwmas.org/index.php?members/5247brcom.210566/
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=535253
https://bbs.darkml.net/home.php?mod=space&uid=226391
https://www.play56.net/home.php?mod=space&uid=6389200
Your comment is awaiting moderation.
https://www.youtube.com/@5247brcom
https://x.com/5247brcom
https://tooter.in/5247brcom
https://wakelet.com/@5247brcom
https://gravatar.com/5247brcom
https://shareyoursocial.com/5247brcom
https://500px.com/p/5247brcom
https://www.instapaper.com/p/5247brcom
https://protocol.ooo/ja/users/5247brcom
https://audiomack.com/5247brcom
https://hackaday.io/5247brcom
https://fyers.in/community/member/ddPWZ14zJR
https://leetcode.com/u/5247brcom/
https://www.notebook.ai/@5247brcom
https://www.halaltrip.com/user/profile/370049/5247brcom/
https://forums.jetphotos.com/member/56586-5247brcom/about
https://medibang.com/author/28792728/
https://www.blockdit.com/5247brcom
https://portfolium.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://topsitenet.com/profile/5247brcom/2174847/
https://akniga.org/profile/1447271-5247brcom/
https://jobs.suncommunitynews.com/profiles/8601629-casa-de-apostas-5247
https://www.speedrun.com/users/5247brcom
https://pbase.com/5247brcom
https://www.gta5-mods.com/users/5247brcom
https://www.nicovideo.jp/user/144858970
https://www.jigsawplanet.com/5247brcom
https://bit.ly/m/5247brcom
https://5247brcom.blogspot.com/2026/07/5247brcom.html
https://bookmeter.com/users/1748186
https://files.fm/5247brcom/info
https://startupxplore.com/en/person/5247brcom
https://m.xtutti.com/user/profile/497637
https://postr.blog/profile/5247brcom
https://5247brcom.stck.me/profile
https://www.chichi-pui.com/users/5247brcom/
https://www.mellow-fan.com/user/d7ezkk845ni5vwlxr56h/about
https://freeimage.host/5247brcom
https://motion-gallery.net/users/1016085
https://biomolecula.ru/authors/166395
https://www.callupcontact.com/b/businessprofile/5247brcom/10165976
https://www.growkudos.com/profile/casa_de_apostas_5247
https://blender.community/5247brcom/
https://doselect.com/@d6bd4a0d630391041c39b6319
https://matkafasi.com/user/5247brcom
https://allmyfaves.com/5247brcom
https://muare.vn/shop/casa-de-apostas-5247/914390
https://pads.zapf.in/s/ofSdJ9I8cG
https://barcelonadema-participa.cat/profiles/5247brcom/activity
https://pad.libreon.fr/s/xiydzgjOd
https://forum.dmec.vn/index.php?members/5247brcom.210079/#info
https://igli.me/5247brcom
http://delphi.larsbo.org/user/5247brcom
https://oye.participer.lyon.fr/profiles/5247brcom/activity
https://timdaily.vn/members/5247brcom.142372/#about
https://iszene.com/user-363435.html
https://www.theyeshivaworld.com/coffeeroom/users/5247brcom
https://desksnear.me/users/5247brcom
https://www.itchyforum.com/en/member.php?398851-5247brcom
https://able2know.org/user/5247brcom/
http://www.biblesupport.com/user/866066-5247brcom/
https://golosknig.com/profile/5247brcom/
https://awan.pro/forum/user/198307/
https://fortunetelleroracle.com/profile/5247brcom
https://fabble.cc/5247brcom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2580541
https://www.sythe.org/members/5247brcom.2073831/
https://potofu.me/5247brcom
https://transfur.com/Users/a5247brcom
https://github.com/klompie5247brcomnleef-eng
https://hedgedoc.stusta.de/s/RQwMylDIi
https://website.informer.com/5247.br.com
https://notes.stuve.fau.de/s/w2Lyd8nFAo
https://en.islcollective.com/portfolio/12969199
https://velog.io/@5247brcom/about
https://mez.ink/5247brcom
https://www.techbang.com/users/5247brcom
https://freeicons.io/profile/957152
https://onlinesequencer.net/members/294605
https://inkbunny.net/5247brcom
https://www.japaaan.com/user/110718
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5247
https://beatsaver.com/playlists/1235493
https://nyccharterschools.jobboard.io/employers/4255039-5247brcom
https://egl.circlly.com/users/5247brcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319989
https://acomics.ru/-5247brcom
https://www.criminalelement.com/members/5247brcom/profile/
https://hanson.net/users/5247brcom
https://expatguidekorea.com/profile/5247brcom/
https://www.heavyironjobs.com/profiles/8606538-casa-de-apostas-5247
https://git.disroot.org/5247brcom
https://song.link/5247brcom
https://idol.st/user/200813/5247brcom/
https://jobs.windomnews.com/profiles/8606530-casa-de-apostas-5247
https://hoaxbuster.com/redacteur/5247brcom
https://www.givey.com/5247brcom
https://zerosuicidetraining.edc.org/user/profile.php?id=593140
https://jobs.westerncity.com/profiles/8606563-casa-de-apostas-5247
https://www.thetriumphforum.com/members/5247brcom.74091/
https://album.link/5247brcom
http://forum.cncprovn.com/members/437103-5247brcom
https://forum.aigato.vn/user/5247brcom
https://rapidapi.com/user/5247brcom
https://www.skool.com/@casa-de-apostas-2260
http://www.invelos.com/UserProfile.aspx?alias=5247brcom
https://www.rwaq.org/users/5247brcom/
https://www.grepmed.com/5247brcom
https://espritgames.com/members/51952861/
https://www.haikudeck.com/presentations/5247brcom
https://hi-fi-forum.net/profile/1182898
https://te.legra.ph/5247brcom-07-17
https://undrtone.com/5247brcom
https://marshallyin.com/members/5247brcom/
https://gravesales.com/author/5247brcom/
https://belgaumonline.com/profile/5247brcom/
https://savelist.co/my-lists/users/5247brcom
https://zzb.bz/5247brcom
https://www.themeqx.com/forums/users/5247brcom/
http://newdigital-world.com/members/5247brcom.html
https://activepages.com.au/profile/5247brcom
https://snippet.host/fczvkq
https://tudomuaban.com/chi-tiet-rao-vat/2968769/5247brcom.html
https://phijkchu.com/a/5247brcom/video-channels
https://lifeinsys.com/user/5247brcom
https://kaeuchi.jp/forums/users/5247brcom/
https://www.claimajob.com/profiles/8607011-casa-de-apostas-5247
https://protospielsouth.com/user/155253
https://theafricavoice.com/profile/5247brcom
https://www.brownbook.net/business/55324163/5247brcom
https://app.hellothematic.com/creator/profile/1167649
https://hackmd.okfn.de/s/rky9tLPEfl
https://manylink.co/@5247brcom
https://www.akaqa.com/question/q19192717303-5247brcom
https://www.threadless.com/@5247brcom/activity
https://maxforlive.com/profile/user/5247brcom?tab=about
https://mathlog.info/users/fleJrzFiDzfiANlcuNO1IT0ZyS33
https://nous.malakoff.fr/profiles/5247brcom/activity
https://fora.babinet.cz/profile.php?section=personal&id=136400
https://www.shippingexplorer.net/en/user/5247brcom/314247
https://www.sunlitcentrekenya.co.ke/author/5247brcom/
https://www.lingvolive.com/en-us/profile/c2d4aa44-bd42-4b44-8fec-f46d638af526/translations
https://www.zubersoft.com/mobilesheets/forum/user-152400.html
https://md.coredump.ch/s/YigPY8RIC
https://aprenderfotografia.online/usuarios/5247brcom/profile/
https://hackmd.hub.yt/s/7riUvbwna
https://lqdoj.edu.vn/user/5247brcom
https://sciencemission.com/profile/5247brcom
https://www.wvhired.com/profiles/8608508-casa-de-apostas-5247
https://formulamasa.com/elearning/members/5247brcom/?v=96b62e1dce57
https://eilo.org/users-view.php?id=92233
https://backloggd.com/u/5247brcom/
https://forums.alliedmods.net/member.php?u=489457
http://forum.modulebazaar.com/forums/user/5247brcom/
https://viblo.asia/u/5247brcom/contact
https://brain-market.com/u/5247brcom
https://www.prosebox.net/book/120497/
https://www.fw-follow.com/forum/topic/162571/5247brcom
https://www.navacool.com/forum/topic/533381/5247brcom
https://www.driedsquidathome.com/forum/topic/192362/5247brcom
https://www.nongkhaempolice.com/forum/topic/196751/5247brcom
https://www.bestloveweddingstudio.com/forum/topic/118595/5247brcom
https://www.natthadon-sanengineering.com/forum/topic/147876/5247brcom
https://www.rueanmaihom.net/forum/topic/134707/5247brcom
https://www.ttlxshipping.com/forum/topic/533382/5247brcom
http://worldchampmambo.com/UserProfile/tabid/42/UserID/507470/Default.aspx
https://www.horticulturaljobs.com/employers/4255976-5247brcom
https://jobs.siliconflorist.com/employers/4255977-5247brcom
https://jobs.nefeshinternational.org/employers/4255978-5247brcom
https://forum.issabel.org/u/5247brcom
https://doc.anagora.org/s/Sleaw9pdD
https://profile.sampo.ru/a5247brcom
https://www.ekdarun.com/forum/topic/190801/5247brcom
https://fanclove.jp/profile/wyWeNgMEB0
https://www.d-ushop.com/forum/topic/192471/5247brcom
https://findaspring.org/members/5247brcom/
https://ketcau.com/member/135620-5247brcom/activities
https://library.zortrax.com/members/5247brcom/
https://pets4friends.com/profile-1665303
https://participa.aytojaen.es/profiles/5247brcom/activity
https://linkmix.co/57351495
https://www.maanation.com/5247brcom
https://janitorai.com/profiles/40bc3155-3ec0-4481-8a64-0040a1a3ae01_profile-of-5247-brcom
https://www.buymusic.club/user/5247brcom
http://iawbs.com/home.php?mod=space&uid=971405
https://participation.bordeaux.fr/profiles/5247brcom/activity
http://genina.com/user/editDone/5475210.page
https://pad.lescommuns.org/s/nblnOWkkL
https://chanylib.ru/ru/forum/user/36587/
https://producerbox.com/users/5247brcom
https://skrolli.fi/keskustelu/users/KlompienLeef/
https://www.thehockeypaper.co.uk/forums/users/5247brcom
https://zbrushcentral.jp/user/5247brcom
https://www.mapleprimes.com/users/5247brcom
https://guitarmaking.co.uk/members/5247brcom/
https://scrapbox.io/5247brcom/5247brcom
https://qiita.com/5247brcom
https://www.annuncigratuititalia.it/author/5247brcom/
https://lite.link/5247brcom
http://www.brenkoweb.com/user/102367/profile
https://www.rossoneriblog.com/author/5247brcom/
https://anunt-imob.ro/user/profile/868311
https://destaquebrasil.com/saopaulo/author/5247brcom/
https://bhmtsff.com/space-uid-99259.html
https://blog.sighpceducation.acm.org/wp/forums/users/5247brcom/
https://pad.libreon.fr/s/d4uET4d2b
https://vc.ru/id6045985
https://artist.link/5247brcom
https://backloggery.com/5247brcom
http://palangshim.com/space-uid-5356578.html
https://etextpad.com/osr0o41ikr
https://app.talkshoe.com/user/5247brcom
https://sfx.thelazy.net/users/u/5247brcom/
https://www.skypixel.com/users/djiuser-o63vncakbyxd
https://pictureinbottle.com/r/2dhuqx6j
https://md.openbikesensor.org/s/iYcH2P7HML
https://pad.codefor.fr/s/jTmrpReIcs
https://www.hogwartsishere.com/profile/1856655/
https://www.plotterusati.it/user/5247brcom
https://linqto.me/about/5247brcom
https://partecipa.poliste.com/profiles/5247brcom/activity
https://hedgedoc.stusta.de/s/9lKLPbutG
https://pad.codefor.fr/s/TAOr9Vq1Kt
https://pad.fablab-siegen.de/s/Dvg1Xq76zE
https://referrallist.com/profile/5247brcom/
https://pad.darmstadt.social/s/iogWv5UiVx
https://www.iglinks.io/KlompienLeef-zr7
https://homepage.ninja/5247brcom
https://md.rappet.xyz/s/dQJT1-41mf
https://md.sebastians.dev/s/iv4lFiWM-
https://controlc.com/lagcucn0
https://justpaste.it/u/5247brcom
https://www.pozible.com/profile/casa-de-apostas-5247
https://strikefans.com/forum/users/5247brcom/
https://experiment.com/users/5247brcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5247brcom/
https://doc.anagora.org/s/maPB95_YL
https://www.grabcaruber.com/members/5247brcom/profile/
https://bike-forum.cz/profil/u/5247brcom
https://galleria.emotionflow.com/196984/profile.html
https://www.myget.org/users/5247brcom
https://app.brancher.ai/user/7wKHr1JHHapQ
https://forum.aceinna.com/user/5247brcom
https://www.giveawayoftheday.com/forums/profile/2003569?updated=true
https://uiverse.io/profile/casadeapos_9437
https://cofacts.tw/user/5247brcom
https://vcook.jp/users/108579
https://pumpyoursound.com/u/user/1654786
https://doc.adminforge.de/s/Fl7LgoVLdz
https://tabelog.com/rvwr/034748578/prof/
https://app.parler.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://gamblingtherapy.org/forum/users/5247brcom/
https://marshmallow-qa.com/43ian8u2sjtb1tz
https://us.enrollbusiness.com/BusinessProfile/7884072/5247brcom
https://its-my.link/@5247brcom
https://writeablog.net/bopeaqv8vb
https://cointr.ee/5247brcom
https://aniworld.to/user/profil/5247brcom
https://hedgedoc.dezentrale.space/s/CWlysrHpc
https://official.link/5247brcom
https://www.czporadna.cz/user/5247brcom/wall
https://tealfeed.com/brcom5247
https://expathealthseoul.com/profile/5247brcom/
https://www.rctech.net/forum/members/5247brcom-560430.html
https://www.mateball.com/brcom5247
https://ofuse.me/e/390987
http://kjtr.grrr.jp/kjtr/?5247brcom
https://raovat.nhadat.vn/members/5247brcom-332484.html
https://advego.com/profile/5247brcom/
https://bio.site/5247brcom
https://www.vnbadminton.com/members/5247brcom.89774/
https://gourmet-calendar.com/users/5247brcom
https://www.sunemall.com/board/board_topic/8431232/8679443.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8679449.htm
https://cars.yclas.com/user/5247brcom
https://calgarybusinesses.ca/dashboard/reviews/5247brcom/
https://www.sciencebee.com.bd/qna/user/5247brcom
https://www.biblicaleldership.com/forums/users/5247brcom/
https://luvly.co/users/5247brcom
https://spinninrecords.com/profile/5247brcom
https://zenwriting.net/1pq4u67k1e
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8679459.htm
https://www.tai-ji.net/board/board_topic/4160148/8679578.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8679590.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8679595.htm
https://kheotay.com.vn/forums/users/KlompienLeef
https://alfounder.com/forums/users/5247brcom/
https://crazyservice.by/forum/user/18015/
https://rsfpost.com/forums/users/5247brcom/
https://www.ontime.co.th/forum/topic/874483/5247brcom
https://forum.gettinglost.ca/user/5247brcom
https://zepodcast.com/forums/users/5247brcom/
http://jobs.emiogp.com/author/5247brcom/
https://wikimapia.org/external_link?url=https://5247.br.com/
https://monviet88.com/profile/5247brcom/
https://onlinevetjobs.com/author/5247brcom/
https://rush1989.rash.jp/pukiwiki/index.php?5247brcom
https://www.fuelly.com/driver/5247brcom
https://www.beamng.com/members/5247brcom.811968/
https://www.spacedesk.net/support-forum/profile/5247brcom/
https://log.concept2.com/profile/3004932
https://playlist.link/5247brcom
https://pods.link/5247brcom
https://mylink.page/5247brcom
https://md.coredump.ch/s/6IYxrZ6JK
https://ctxt.io/3/odsUrJuQE
https://5247brcom.gitbook.io/5247brcom-docs/
https://6a5a368b1f7d2.site123.me/
https://casadeapostas5247.website3.me/
https://onespotsocial.com/5247brcom
https://www.scener.com/@5247brcom
https://amaz0ns.com/forums/users/5247brcom/
https://hostndobezi.com/5247brcom
https://nilechronicles.com/profile/5247brcom
https://paper.wf/5247brcom/5247brcom
https://devfolio.co/@5247brcom/readme-md
https://wibki.com/5247brcom
https://www.renderosity.com/users/id:1880858
https://eo-college.org/members/5247brcom/
https://ivpaste.com/v/rudQsj1MfZ
https://www.moshpyt.com/user/5247brcom
https://www.racerjobs.com/profiles/8610980-casa-de-apostas-5247
https://www.instructorsnearme.com/author/5247brcom/
https://www.yumpu.com/user/5247brcom
https://ferrariformula1.hu/community/profile/5247brcom/
http://koloboklinks.com/site?url=5247.br.com
https://biolinky.co/5247-brcom
https://md.chaospott.de/s/KT9bKF0si-
https://allmy.bio/5247brcom
https://whatson.plus/5247brcom
https://www.aviacionargentina.net/user/5247brcom
https://ac.db0.company/user/23498/5247brcom/
https://forum.hiv.plus/user/5247brcom
https://www.adminer.org/redirect/?lang=en&url=https://5247.br.com/
https://aboutcasemanagerjobs.com/author/5247brcom/
https://fr.islcollective.com/portfolio/12969199
https://es.islcollective.com/portafolio/12969199
https://www.minecraft-servers-list.org/details/5247brcom/
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://5247.br.com/
https://baskadia.com/user/h6va
https://decidim.calafell.cat/profiles/5247brcom/activity
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://5247.br.com/
https://vs.cga.gg/user/247939
https://www.fitlynk.com/ed5823912
https://bsky.app/profile/5247brcom.bsky.social
https://www.xmonsta.com/forums/users/5247brcom/
https://mail.londonchinese.com/home.php?mod=space&uid=628765&do=index
https://pimrec.pnu.edu.ua/members/5247brcom/profile/
https://www.hostboard.com/forums/members/5247brcom.html
https://forum.euro-pvp.com/user/593683-5247brcom/
http://byltz.com/home.php?mod=space&uid=484260
https://buyandsellhair.com/author/5247brcom/
https://sighpceducation.hosting.acm.org/wp/forums/users/5247brcom/
https://nogu.org.uk/forum/profile/5247brcom/
https://gitflic.ru/user/5247brcom
https://cornucopia.se/author/5247brcom/
http://mura.hitobashira.org/index.php?5247brcom
https://foss.heptapod.net/5247brcom
https://www.empregosaude.pt/en/author/5247brcom/
https://www.euskalmarket.com/author/5247brcom/
https://doingbusiness.eu/profile/5247brcom/
https://portfolium.com.au/5247brcom
https://www.tizmos.com/5247brcom/
https://jobs.lajobsportal.org/profiles/8611331-casa-de-apostas-5247
https://gamelet.online/user/114696621103424895842@google/about
https://www.facer.io/u/5247brcom
https://www.cryptoispy.com/forums/users/5247brcom/
https://forum.cnnr.fr/user/5247brcom
https://usabbs.org/home.php?mod=space&uid=91093
https://jobs.host-panel.com/author/5247brcom/
https://lankadevelopers.lk/user/5247brcom
https://sistacafe.com/user/620144
http://bbs.medicalforum.cn/home.php?mod=space&uid=2415033
https://www.hardmcasual.net/user/2370/
https://www.camtation.com/leden/5247brcom/profile/
http://www.webclap.com/php/jump.php?url=https://5247.br.com/
https://fueler.io/5247brcom
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=4021420
https://paidforarticles.in/author/5247brcom
https://biashara.co.ke/author/5247brcom/
https://feyenoord.supporters.nl/profiel/165057/5247brcom
https://zb3.org/5247brcom/5247brcom
https://everbookforever.com/share/profile/5247brcom/
https://shorturl.at/kQ1gy
https://hashnode.com/@5247brcom
https://nhattao.com/members/user7010750.7010750/
https://morguefile.com/creative/5247brcom
https://edabit.com/user/GKqACMbvbHedavbxQ
https://securityheaders.com/?q=https://5247.br.com/
https://md.darmstadt.ccc.de/s/16gHpPsJLI
https://www.pdc.edu/?URL=https://5247.br.com/
https://ask.mallaky.com/?qa=user/5247brcom
https://www.depechemode.cz/?URL=https://5247.br.com/
https://staroetv.su/go?https://5247.br.com/
https://road-to-eden.com/index.php?5247brcom
https://www.pintradingdb.com/forum/member.php?action=profile&uid=152621
https://pledgeme.co.nz/profiles/352850/
https://www.templepurohit.com/forums/users/KlompienLeef/
https://hedgedoc.logilab.fr/s/Srg2ZMslG
https://entre-vos-mains.alsace.eu/profiles/5247brcom
https://ixawiki.com/link.php?url=https://5247.br.com/
https://game8.jp/users/523389
https://www.vid419.com/home.php?mod=space&uid=3501463
http://jobboard.piasd.org/author/5247brcom/
https://www.okaywan.com/home.php?mod=space&uid=827545
http://tkdlab.com/wiki/index.php?5247brcom
https://volleypedia.org/index.php?qa=user&qa_1=5247brcom
http://pcsq28.com/home.php?mod=space&uid=2336679
https://bbs.airav.cc/home.php?mod=space&uid=4802224
https://pad.funkwhale.audio/s/tIlVUmQrD
https://forum.dfwmas.org/index.php?members/5247brcom.210566/
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=535253
https://bbs.darkml.net/home.php?mod=space&uid=226391
https://www.play56.net/home.php?mod=space&uid=6389200
Your comment is awaiting moderation.
https://www.youtube.com/@5247brcom
https://x.com/5247brcom
https://tooter.in/5247brcom
https://wakelet.com/@5247brcom
https://gravatar.com/5247brcom
https://shareyoursocial.com/5247brcom
https://500px.com/p/5247brcom
https://www.instapaper.com/p/5247brcom
https://protocol.ooo/ja/users/5247brcom
https://audiomack.com/5247brcom
https://hackaday.io/5247brcom
https://fyers.in/community/member/ddPWZ14zJR
https://leetcode.com/u/5247brcom/
https://www.notebook.ai/@5247brcom
https://www.halaltrip.com/user/profile/370049/5247brcom/
https://forums.jetphotos.com/member/56586-5247brcom/about
https://medibang.com/author/28792728/
https://www.blockdit.com/5247brcom
https://portfolium.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://topsitenet.com/profile/5247brcom/2174847/
https://akniga.org/profile/1447271-5247brcom/
https://jobs.suncommunitynews.com/profiles/8601629-casa-de-apostas-5247
https://www.speedrun.com/users/5247brcom
https://pbase.com/5247brcom
https://www.gta5-mods.com/users/5247brcom
https://www.nicovideo.jp/user/144858970
https://www.jigsawplanet.com/5247brcom
https://bit.ly/m/5247brcom
https://5247brcom.blogspot.com/2026/07/5247brcom.html
https://bookmeter.com/users/1748186
https://files.fm/5247brcom/info
https://startupxplore.com/en/person/5247brcom
https://m.xtutti.com/user/profile/497637
https://postr.blog/profile/5247brcom
https://5247brcom.stck.me/profile
https://www.chichi-pui.com/users/5247brcom/
https://www.mellow-fan.com/user/d7ezkk845ni5vwlxr56h/about
https://freeimage.host/5247brcom
https://motion-gallery.net/users/1016085
https://biomolecula.ru/authors/166395
https://www.callupcontact.com/b/businessprofile/5247brcom/10165976
https://www.growkudos.com/profile/casa_de_apostas_5247
https://blender.community/5247brcom/
https://doselect.com/@d6bd4a0d630391041c39b6319
https://matkafasi.com/user/5247brcom
https://allmyfaves.com/5247brcom
https://muare.vn/shop/casa-de-apostas-5247/914390
https://pads.zapf.in/s/ofSdJ9I8cG
https://barcelonadema-participa.cat/profiles/5247brcom/activity
https://pad.libreon.fr/s/xiydzgjOd
https://forum.dmec.vn/index.php?members/5247brcom.210079/#info
https://igli.me/5247brcom
http://delphi.larsbo.org/user/5247brcom
https://oye.participer.lyon.fr/profiles/5247brcom/activity
https://timdaily.vn/members/5247brcom.142372/#about
https://iszene.com/user-363435.html
https://www.theyeshivaworld.com/coffeeroom/users/5247brcom
https://desksnear.me/users/5247brcom
https://www.itchyforum.com/en/member.php?398851-5247brcom
https://able2know.org/user/5247brcom/
http://www.biblesupport.com/user/866066-5247brcom/
https://golosknig.com/profile/5247brcom/
https://awan.pro/forum/user/198307/
https://fortunetelleroracle.com/profile/5247brcom
https://fabble.cc/5247brcom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2580541
https://www.sythe.org/members/5247brcom.2073831/
https://potofu.me/5247brcom
https://transfur.com/Users/a5247brcom
https://github.com/klompie5247brcomnleef-eng
https://hedgedoc.stusta.de/s/RQwMylDIi
https://website.informer.com/5247.br.com
https://notes.stuve.fau.de/s/w2Lyd8nFAo
https://en.islcollective.com/portfolio/12969199
https://velog.io/@5247brcom/about
https://mez.ink/5247brcom
https://www.techbang.com/users/5247brcom
https://freeicons.io/profile/957152
https://onlinesequencer.net/members/294605
https://inkbunny.net/5247brcom
https://www.japaaan.com/user/110718
https://www.launchgood.com/user/newprofile#!/user-profile/profile/casa.de.apostas.5247
https://beatsaver.com/playlists/1235493
https://nyccharterschools.jobboard.io/employers/4255039-5247brcom
https://egl.circlly.com/users/5247brcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=319989
https://acomics.ru/-5247brcom
https://www.criminalelement.com/members/5247brcom/profile/
https://hanson.net/users/5247brcom
https://expatguidekorea.com/profile/5247brcom/
https://www.heavyironjobs.com/profiles/8606538-casa-de-apostas-5247
https://git.disroot.org/5247brcom
https://song.link/5247brcom
https://idol.st/user/200813/5247brcom/
https://jobs.windomnews.com/profiles/8606530-casa-de-apostas-5247
https://hoaxbuster.com/redacteur/5247brcom
https://www.givey.com/5247brcom
https://zerosuicidetraining.edc.org/user/profile.php?id=593140
https://jobs.westerncity.com/profiles/8606563-casa-de-apostas-5247
https://www.thetriumphforum.com/members/5247brcom.74091/
https://album.link/5247brcom
http://forum.cncprovn.com/members/437103-5247brcom
https://forum.aigato.vn/user/5247brcom
https://rapidapi.com/user/5247brcom
https://www.skool.com/@casa-de-apostas-2260
http://www.invelos.com/UserProfile.aspx?alias=5247brcom
https://www.rwaq.org/users/5247brcom/
https://www.grepmed.com/5247brcom
https://espritgames.com/members/51952861/
https://www.haikudeck.com/presentations/5247brcom
https://hi-fi-forum.net/profile/1182898
https://te.legra.ph/5247brcom-07-17
https://undrtone.com/5247brcom
https://marshallyin.com/members/5247brcom/
https://gravesales.com/author/5247brcom/
https://belgaumonline.com/profile/5247brcom/
https://savelist.co/my-lists/users/5247brcom
https://zzb.bz/5247brcom
https://www.themeqx.com/forums/users/5247brcom/
http://newdigital-world.com/members/5247brcom.html
https://activepages.com.au/profile/5247brcom
https://snippet.host/fczvkq
https://tudomuaban.com/chi-tiet-rao-vat/2968769/5247brcom.html
https://phijkchu.com/a/5247brcom/video-channels
https://lifeinsys.com/user/5247brcom
https://kaeuchi.jp/forums/users/5247brcom/
https://www.claimajob.com/profiles/8607011-casa-de-apostas-5247
https://protospielsouth.com/user/155253
https://theafricavoice.com/profile/5247brcom
https://www.brownbook.net/business/55324163/5247brcom
https://app.hellothematic.com/creator/profile/1167649
https://hackmd.okfn.de/s/rky9tLPEfl
https://manylink.co/@5247brcom
https://www.akaqa.com/question/q19192717303-5247brcom
https://www.threadless.com/@5247brcom/activity
https://maxforlive.com/profile/user/5247brcom?tab=about
https://mathlog.info/users/fleJrzFiDzfiANlcuNO1IT0ZyS33
https://nous.malakoff.fr/profiles/5247brcom/activity
https://fora.babinet.cz/profile.php?section=personal&id=136400
https://www.shippingexplorer.net/en/user/5247brcom/314247
https://www.sunlitcentrekenya.co.ke/author/5247brcom/
https://www.lingvolive.com/en-us/profile/c2d4aa44-bd42-4b44-8fec-f46d638af526/translations
https://www.zubersoft.com/mobilesheets/forum/user-152400.html
https://md.coredump.ch/s/YigPY8RIC
https://aprenderfotografia.online/usuarios/5247brcom/profile/
https://hackmd.hub.yt/s/7riUvbwna
https://lqdoj.edu.vn/user/5247brcom
https://sciencemission.com/profile/5247brcom
https://www.wvhired.com/profiles/8608508-casa-de-apostas-5247
https://formulamasa.com/elearning/members/5247brcom/?v=96b62e1dce57
https://eilo.org/users-view.php?id=92233
https://backloggd.com/u/5247brcom/
https://forums.alliedmods.net/member.php?u=489457
http://forum.modulebazaar.com/forums/user/5247brcom/
https://viblo.asia/u/5247brcom/contact
https://brain-market.com/u/5247brcom
https://www.prosebox.net/book/120497/
https://www.fw-follow.com/forum/topic/162571/5247brcom
https://www.navacool.com/forum/topic/533381/5247brcom
https://www.driedsquidathome.com/forum/topic/192362/5247brcom
https://www.nongkhaempolice.com/forum/topic/196751/5247brcom
https://www.bestloveweddingstudio.com/forum/topic/118595/5247brcom
https://www.natthadon-sanengineering.com/forum/topic/147876/5247brcom
https://www.rueanmaihom.net/forum/topic/134707/5247brcom
https://www.ttlxshipping.com/forum/topic/533382/5247brcom
http://worldchampmambo.com/UserProfile/tabid/42/UserID/507470/Default.aspx
https://www.horticulturaljobs.com/employers/4255976-5247brcom
https://jobs.siliconflorist.com/employers/4255977-5247brcom
https://jobs.nefeshinternational.org/employers/4255978-5247brcom
https://forum.issabel.org/u/5247brcom
https://doc.anagora.org/s/Sleaw9pdD
https://profile.sampo.ru/a5247brcom
https://www.ekdarun.com/forum/topic/190801/5247brcom
https://fanclove.jp/profile/wyWeNgMEB0
https://www.d-ushop.com/forum/topic/192471/5247brcom
https://findaspring.org/members/5247brcom/
https://ketcau.com/member/135620-5247brcom/activities
https://library.zortrax.com/members/5247brcom/
https://pets4friends.com/profile-1665303
https://participa.aytojaen.es/profiles/5247brcom/activity
https://linkmix.co/57351495
https://www.maanation.com/5247brcom
https://janitorai.com/profiles/40bc3155-3ec0-4481-8a64-0040a1a3ae01_profile-of-5247-brcom
https://www.buymusic.club/user/5247brcom
http://iawbs.com/home.php?mod=space&uid=971405
https://participation.bordeaux.fr/profiles/5247brcom/activity
http://genina.com/user/editDone/5475210.page
https://pad.lescommuns.org/s/nblnOWkkL
https://chanylib.ru/ru/forum/user/36587/
https://producerbox.com/users/5247brcom
https://skrolli.fi/keskustelu/users/KlompienLeef/
https://www.thehockeypaper.co.uk/forums/users/5247brcom
https://zbrushcentral.jp/user/5247brcom
https://www.mapleprimes.com/users/5247brcom
https://guitarmaking.co.uk/members/5247brcom/
https://scrapbox.io/5247brcom/5247brcom
https://qiita.com/5247brcom
https://www.annuncigratuititalia.it/author/5247brcom/
https://lite.link/5247brcom
http://www.brenkoweb.com/user/102367/profile
https://www.rossoneriblog.com/author/5247brcom/
https://anunt-imob.ro/user/profile/868311
https://destaquebrasil.com/saopaulo/author/5247brcom/
https://bhmtsff.com/space-uid-99259.html
https://blog.sighpceducation.acm.org/wp/forums/users/5247brcom/
https://pad.libreon.fr/s/d4uET4d2b
https://vc.ru/id6045985
https://artist.link/5247brcom
https://backloggery.com/5247brcom
http://palangshim.com/space-uid-5356578.html
https://etextpad.com/osr0o41ikr
https://app.talkshoe.com/user/5247brcom
https://sfx.thelazy.net/users/u/5247brcom/
https://www.skypixel.com/users/djiuser-o63vncakbyxd
https://pictureinbottle.com/r/2dhuqx6j
https://md.openbikesensor.org/s/iYcH2P7HML
https://pad.codefor.fr/s/jTmrpReIcs
https://www.hogwartsishere.com/profile/1856655/
https://www.plotterusati.it/user/5247brcom
https://linqto.me/about/5247brcom
https://partecipa.poliste.com/profiles/5247brcom/activity
https://hedgedoc.stusta.de/s/9lKLPbutG
https://pad.codefor.fr/s/TAOr9Vq1Kt
https://pad.fablab-siegen.de/s/Dvg1Xq76zE
https://referrallist.com/profile/5247brcom/
https://pad.darmstadt.social/s/iogWv5UiVx
https://www.iglinks.io/KlompienLeef-zr7
https://homepage.ninja/5247brcom
https://md.rappet.xyz/s/dQJT1-41mf
https://md.sebastians.dev/s/iv4lFiWM-
https://controlc.com/lagcucn0
https://justpaste.it/u/5247brcom
https://www.pozible.com/profile/casa-de-apostas-5247
https://strikefans.com/forum/users/5247brcom/
https://experiment.com/users/5247brcom
https://commoncause.optiontradingspeak.com/index.php/community/profile/5247brcom/
https://doc.anagora.org/s/maPB95_YL
https://www.grabcaruber.com/members/5247brcom/profile/
https://bike-forum.cz/profil/u/5247brcom
https://galleria.emotionflow.com/196984/profile.html
https://www.myget.org/users/5247brcom
https://app.brancher.ai/user/7wKHr1JHHapQ
https://forum.aceinna.com/user/5247brcom
https://www.giveawayoftheday.com/forums/profile/2003569?updated=true
https://uiverse.io/profile/casadeapos_9437
https://cofacts.tw/user/5247brcom
https://vcook.jp/users/108579
https://pumpyoursound.com/u/user/1654786
https://doc.adminforge.de/s/Fl7LgoVLdz
https://tabelog.com/rvwr/034748578/prof/
https://app.parler.com/5247brcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2C4780A86A587D020A495ECF@AdobeID
https://gamblingtherapy.org/forum/users/5247brcom/
https://marshmallow-qa.com/43ian8u2sjtb1tz
https://us.enrollbusiness.com/BusinessProfile/7884072/5247brcom
https://its-my.link/@5247brcom
https://writeablog.net/bopeaqv8vb
https://cointr.ee/5247brcom
https://aniworld.to/user/profil/5247brcom
https://hedgedoc.dezentrale.space/s/CWlysrHpc
https://official.link/5247brcom
https://www.czporadna.cz/user/5247brcom/wall
https://tealfeed.com/brcom5247
https://expathealthseoul.com/profile/5247brcom/
https://www.rctech.net/forum/members/5247brcom-560430.html
https://www.mateball.com/brcom5247
https://ofuse.me/e/390987
http://kjtr.grrr.jp/kjtr/?5247brcom
https://raovat.nhadat.vn/members/5247brcom-332484.html
https://advego.com/profile/5247brcom/
https://bio.site/5247brcom
https://www.vnbadminton.com/members/5247brcom.89774/
https://gourmet-calendar.com/users/5247brcom
https://www.sunemall.com/board/board_topic/8431232/8679443.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8679449.htm
https://cars.yclas.com/user/5247brcom
https://calgarybusinesses.ca/dashboard/reviews/5247brcom/
https://www.sciencebee.com.bd/qna/user/5247brcom
https://www.biblicaleldership.com/forums/users/5247brcom/
https://luvly.co/users/5247brcom
https://spinninrecords.com/profile/5247brcom
https://zenwriting.net/1pq4u67k1e
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8679459.htm
https://www.tai-ji.net/board/board_topic/4160148/8679578.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8679590.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8679595.htm
https://kheotay.com.vn/forums/users/KlompienLeef
https://alfounder.com/forums/users/5247brcom/
https://crazyservice.by/forum/user/18015/
https://rsfpost.com/forums/users/5247brcom/
https://www.ontime.co.th/forum/topic/874483/5247brcom
https://forum.gettinglost.ca/user/5247brcom
https://zepodcast.com/forums/users/5247brcom/
http://jobs.emiogp.com/author/5247brcom/
https://wikimapia.org/external_link?url=https://5247.br.com/
https://monviet88.com/profile/5247brcom/
https://onlinevetjobs.com/author/5247brcom/
https://rush1989.rash.jp/pukiwiki/index.php?5247brcom
https://www.fuelly.com/driver/5247brcom
https://www.beamng.com/members/5247brcom.811968/
https://www.spacedesk.net/support-forum/profile/5247brcom/
https://log.concept2.com/profile/3004932
https://playlist.link/5247brcom
https://pods.link/5247brcom
https://mylink.page/5247brcom
https://md.coredump.ch/s/6IYxrZ6JK
https://ctxt.io/3/odsUrJuQE
https://5247brcom.gitbook.io/5247brcom-docs/
https://6a5a368b1f7d2.site123.me/
https://casadeapostas5247.website3.me/
https://onespotsocial.com/5247brcom
https://www.scener.com/@5247brcom
https://amaz0ns.com/forums/users/5247brcom/
https://hostndobezi.com/5247brcom
https://nilechronicles.com/profile/5247brcom
https://paper.wf/5247brcom/5247brcom
https://devfolio.co/@5247brcom/readme-md
https://wibki.com/5247brcom
https://www.renderosity.com/users/id:1880858
https://eo-college.org/members/5247brcom/
https://ivpaste.com/v/rudQsj1MfZ
https://www.moshpyt.com/user/5247brcom
https://www.racerjobs.com/profiles/8610980-casa-de-apostas-5247
https://www.instructorsnearme.com/author/5247brcom/
https://www.yumpu.com/user/5247brcom
https://ferrariformula1.hu/community/profile/5247brcom/
http://koloboklinks.com/site?url=5247.br.com
https://biolinky.co/5247-brcom
https://md.chaospott.de/s/KT9bKF0si-
https://allmy.bio/5247brcom
https://whatson.plus/5247brcom
https://www.aviacionargentina.net/user/5247brcom
https://ac.db0.company/user/23498/5247brcom/
https://forum.hiv.plus/user/5247brcom
https://www.adminer.org/redirect/?lang=en&url=https://5247.br.com/
https://aboutcasemanagerjobs.com/author/5247brcom/
https://fr.islcollective.com/portfolio/12969199
https://es.islcollective.com/portafolio/12969199
https://www.minecraft-servers-list.org/details/5247brcom/
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://5247.br.com/
https://baskadia.com/user/h6va
https://decidim.calafell.cat/profiles/5247brcom/activity
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://5247.br.com/
https://vs.cga.gg/user/247939
https://www.fitlynk.com/ed5823912
https://bsky.app/profile/5247brcom.bsky.social
https://www.xmonsta.com/forums/users/5247brcom/
https://mail.londonchinese.com/home.php?mod=space&uid=628765&do=index
https://pimrec.pnu.edu.ua/members/5247brcom/profile/
https://www.hostboard.com/forums/members/5247brcom.html
https://forum.euro-pvp.com/user/593683-5247brcom/
http://byltz.com/home.php?mod=space&uid=484260
https://buyandsellhair.com/author/5247brcom/
https://sighpceducation.hosting.acm.org/wp/forums/users/5247brcom/
https://nogu.org.uk/forum/profile/5247brcom/
https://gitflic.ru/user/5247brcom
https://cornucopia.se/author/5247brcom/
http://mura.hitobashira.org/index.php?5247brcom
https://foss.heptapod.net/5247brcom
https://www.empregosaude.pt/en/author/5247brcom/
https://www.euskalmarket.com/author/5247brcom/
https://doingbusiness.eu/profile/5247brcom/
https://portfolium.com.au/5247brcom
https://www.tizmos.com/5247brcom/
https://jobs.lajobsportal.org/profiles/8611331-casa-de-apostas-5247
https://gamelet.online/user/114696621103424895842@google/about
https://www.facer.io/u/5247brcom
https://www.cryptoispy.com/forums/users/5247brcom/
https://forum.cnnr.fr/user/5247brcom
https://usabbs.org/home.php?mod=space&uid=91093
https://jobs.host-panel.com/author/5247brcom/
https://lankadevelopers.lk/user/5247brcom
https://sistacafe.com/user/620144
http://bbs.medicalforum.cn/home.php?mod=space&uid=2415033
https://www.hardmcasual.net/user/2370/
https://www.camtation.com/leden/5247brcom/profile/
http://www.webclap.com/php/jump.php?url=https://5247.br.com/
https://fueler.io/5247brcom
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=4021420
https://paidforarticles.in/author/5247brcom
https://biashara.co.ke/author/5247brcom/
https://feyenoord.supporters.nl/profiel/165057/5247brcom
https://zb3.org/5247brcom/5247brcom
https://everbookforever.com/share/profile/5247brcom/
https://shorturl.at/kQ1gy
https://hashnode.com/@5247brcom
https://nhattao.com/members/user7010750.7010750/
https://morguefile.com/creative/5247brcom
https://edabit.com/user/GKqACMbvbHedavbxQ
https://securityheaders.com/?q=https://5247.br.com/
https://md.darmstadt.ccc.de/s/16gHpPsJLI
https://www.pdc.edu/?URL=https://5247.br.com/
https://ask.mallaky.com/?qa=user/5247brcom
https://www.depechemode.cz/?URL=https://5247.br.com/
https://staroetv.su/go?https://5247.br.com/
https://road-to-eden.com/index.php?5247brcom
https://www.pintradingdb.com/forum/member.php?action=profile&uid=152621
https://pledgeme.co.nz/profiles/352850/
https://www.templepurohit.com/forums/users/KlompienLeef/
https://hedgedoc.logilab.fr/s/Srg2ZMslG
https://entre-vos-mains.alsace.eu/profiles/5247brcom
https://ixawiki.com/link.php?url=https://5247.br.com/
https://game8.jp/users/523389
https://www.vid419.com/home.php?mod=space&uid=3501463
http://jobboard.piasd.org/author/5247brcom/
https://www.okaywan.com/home.php?mod=space&uid=827545
http://tkdlab.com/wiki/index.php?5247brcom
https://volleypedia.org/index.php?qa=user&qa_1=5247brcom
http://pcsq28.com/home.php?mod=space&uid=2336679
https://bbs.airav.cc/home.php?mod=space&uid=4802224
https://pad.funkwhale.audio/s/tIlVUmQrD
https://forum.dfwmas.org/index.php?members/5247brcom.210566/
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=535253
https://bbs.darkml.net/home.php?mod=space&uid=226391
https://www.play56.net/home.php?mod=space&uid=6389200
Great wordpress blog here.. It’s hard to find quality writing like yours these days. I really appreciate people like you! take care
Hello, i feel that i saw you visited my blog so i got here to “go back the want”.I’m trying to to find issues to enhance my web site!I assume its good enough to use some of your ideas!!
Good write-up, I’m normal visitor of one’s website, maintain up the excellent operate, and It’s going to be a regular visitor for a long time.
I’ve been exploring for a little for any high-quality articles or weblog posts on this kind of space . Exploring in Yahoo I eventually stumbled upon this web site. Reading this information So i am happy to convey that I’ve a very just right uncanny feeling I found out exactly what I needed. I such a lot for sure will make certain to don’t put out of your mind this site and provides it a look regularly.
Thank you for the sensible critique. Me & my neighbor were just preparing to do a little research on this. We got a grab a book from our local library but I think I learned more clear from this post. I am very glad to see such excellent information being shared freely out there.
I really enjoy looking at on this internet site, it has wonderful posts. “Beware lest in your anxiety to avoid war you obtain a master.” by Demosthenes.
I like what you guys tend to be up too. This sort of clever work and reporting! Keep up the good works guys I’ve included you guys to my personal blogroll.
Thanks for the sensible critique. Me & my neighbor were just preparing to do some research about this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such wonderful information being shared freely out there.
Some truly nice and useful info on this internet site, also I conceive the design and style contains great features.
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
Thanks for any other informative blog. Where else may I get that kind of information written in such an ideal means? I’ve a mission that I’m simply now running on, and I have been at the glance out for such info.
I enjoy your work, appreciate it for all the great blog posts.
You have mentioned very interesting details ! ps decent internet site.
Howdy! Do you know if they make any plugins to help with SEO? I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good success. If you know of any please share. Thank you!
I too believe thus, perfectly composed post! .
I am only writing to make you be aware of what a fine encounter my cousin’s daughter experienced reading yuor web blog. She came to find too many details, which included what it is like to have an awesome helping nature to have other folks really easily master some tricky topics. You really did more than people’s desires. Thanks for displaying these great, healthy, educational and in addition easy thoughts on this topic to Emily.
My coder is trying to persuade me to move to .net from PHP. I have always disliked the idea because of the costs. But he’s tryiong none the less. I’ve been using Movable-type on various websites for about a year and am nervous about switching to another platform. I have heard very good things about blogengine.net. Is there a way I can transfer all my wordpress content into it? Any help would be greatly appreciated!
An interesting discussion is worth comment. I think that you should write more on this topic, it might not be a taboo subject but generally people are not enough to speak on such topics. To the next. Cheers
Very interesting points you have noted, regards for putting up. “Above all be true to yourself, and if you can not put your heart in it, take yourself out of it.” by Hardy D. Jackson.
I have been absent for some time, but now I remember why I used to love this web site. Thanks , I’ll try and check back more often. How frequently you update your website?
An fascinating dialogue is value comment. I think that you need to write extra on this subject, it won’t be a taboo topic but usually persons are not sufficient to talk on such topics. To the next. Cheers
Its fantastic as your other articles : D, regards for putting up.
I like this post, enjoyed this one thanks for posting. “The difference between stupidity and genius is that genius has its limits.” by Albert Einstein.
I am often to blogging and i really appreciate your content. The article has really peaks my interest. I am going to bookmark your site and keep checking for new information.
I have to express my thanks to the writer for rescuing me from such a predicament. After looking out throughout the online world and obtaining concepts which were not powerful, I believed my entire life was done. Being alive devoid of the solutions to the problems you have sorted out all through your main guideline is a crucial case, and ones that might have in a wrong way affected my career if I hadn’t come across your web page. Your ability and kindness in controlling almost everything was valuable. I’m not sure what I would have done if I hadn’t discovered such a thing like this. I’m able to at this time relish my future. Thanks for your time very much for your high quality and result oriented help. I will not be reluctant to propose your site to any person who needs support about this area.
I will immediately grasp your rss feed as I can not in finding your e-mail subscription hyperlink or newsletter service. Do you have any? Please let me recognise in order that I could subscribe. Thanks.
Everything is very open and very clear explanation of issues. was truly information. Your website is very useful. Thanks for sharing.
Some genuinely nice and utilitarian info on this site, besides I conceive the layout has great features.
Thank you for sharing with us, I believe this website genuinely stands out :D.
Enjoyed reading this, very good stuff, appreciate it.
This design is incredible! You certainly know how to keep a reader entertained. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job. I really loved what you had to say, and more than that, how you presented it. Too cool!
You have observed very interesting points! ps decent internet site. “Wisdom is the supreme part of happiness.” by Sophocles.
Luar biasa! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan yang luar biasa!
Ini adalah tips yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
Benar-benar bersih website, salam untuk posting ini.
Wow! Ini bisa jadi salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Luar biasa. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
Saya senang menjadi salah satu dari beberapa pengunjung di situs web hebat ini (:, terimakasih telah mengunggah.
Definitely imagine that which you stated. Your favourite reason seemed to be at the web the easiest factor to take into accout of. I say to you, I certainly get annoyed while people think about concerns that they just do not know about. You managed to hit the nail upon the highest and also outlined out the entire thing without having side-effects , folks could take a signal. Will likely be back to get more. Thanks
Sangat fantastis info dapat ditemukan di web blog.
Youre so cool! I dont suppose Ive read anything like this before. So nice to seek out anyone with some authentic ideas on this subject. realy thanks for starting this up. this web site is one thing that is wanted on the internet, someone with a bit of originality. useful job for bringing something new to the internet!
hello there and thanks in your information – I’ve definitely picked up anything new from right here. I did on the other hand expertise several technical issues the usage of this website, as I skilled to reload the web site lots of instances previous to I could get it to load properly. I had been wondering if your web hosting is OK? Not that I am complaining, but sluggish loading instances instances will very frequently impact your placement in google and could damage your high-quality score if ads and ***********|advertising|advertising|advertising and *********** with Adwords. Well I am including this RSS to my e-mail and could glance out for a lot more of your respective exciting content. Ensure that you replace this again very soon..
Lovely website! I am loving it!! Will come back again. I am taking your feeds also
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang sangat bagus!
Saya perlu mengatakan, ini adalah salah satu posting terbaik yang pernah saya baca dalam waktu yang lama. Informasi yang sangat berguna. Terima kasih telah berbagi.
Wow, superb weblog format! How long have you been running a blog for? you made blogging look easy. The total glance of your web site is magnificent, as well as the content!
Hebat blog yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan pendapat dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Terima kasih!
Sangat menarik detail yang Anda catat, salam telah mengunggah.
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan berterima kasih kepada Anda.
Kami mungkin memiliki hyperlink alternatif perjanjian di antara kita!
You have observed very interesting points! ps nice web site.
Whats Taking place i am new to this, I stumbled upon this I’ve discovered It absolutely useful and it has aided me out loads. I am hoping to contribute & assist different customers like its aided me. Great job.
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Perdamaian, perdagangan, dan persahabatan yang jujur dengan semua bangsa, tanpa aliansi yang mengikat.” oleh Thomas Jefferson.
Isi yang luar biasa! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Saya tidak sering berkomentar tetapi saya harus mengakui hargai untuk posting yang satu ini : D.
Ini adalah blog yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar hebat!
I got what you mean ,saved to my bookmarks, very nice web site.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Saya amat beruntung menemukan situs ini di Bing, persis seperti yang saya cari : D pula sudah saya simpan ke bookmark.
Ya menyimpan ini bukanlah keputusan yang spekulatif pos yang luar biasa! .
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
I think that is one of the so much vital information for me. And i am happy reading your article. However should commentary on some common things, The website taste is wonderful, the articles is truly excellent :D. Excellent task, cheers
Terima kasih, saya baru-baru ini menelusuri informasi tentang topik ini sudah lama dan milik Anda adalah yang terbaik yang saya ketahui sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda pasti tentang sumber tersebut?
Wohh baru saja apa yang saya cari, salam atas unggahan.
Saya tidak bisa menahan diri untuk berkomentar
Great site. Plenty of useful information here. I am sending it to some friends ans also sharing in delicious. And naturally, thanks for your sweat!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
This website is my inspiration , really excellent pattern and perfect subject material.
I have been absent for some time, but now I remember why I used to love this website. Thank you, I will try and check back more frequently. How frequently you update your website?
Saya senang menjadi salah satu dari beberapa pengunjung di situs hebat ini (:, sangat dihargai telah mengunggah.
Bagaimanapun, terima kasih untuk artikel yang fantastis ini dan meskipun saya tidak benar-benar sepakat sepenuhnya, saya menghargai pandangan.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
Isi yang hebat! Gaya penulisan Anda jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca konten lainnya.
Hey there would you mind stating which blog platform you’re using? I’m going to start my own blog in the near future but I’m having a difficult time making a decision between BlogEngine/Wordpress/B2evolution and Drupal. The reason I ask is because your design and style seems different then most blogs and I’m looking for something unique. P.S My apologies for being off-topic but I had to ask!
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Saya senang menjadi pengunjung dari blog paripurna ini!, sangat dihargai atas informasi langka ini!
I got what you intend,saved to my bookmarks, very nice internet site.
I must voice my affection for your kindness for men and women who have the need for help on this important situation. Your special dedication to passing the solution all around appeared to be exceedingly powerful and have really empowered girls like me to realize their pursuits. Your new warm and helpful facts denotes a lot to me and additionally to my fellow workers. Many thanks; from everyone of us.
Ребята, заметил интересную закономерность: сейчас почти все жаждут мгновенно подняться, хотя не учитывают, что нервы — это главный барьер в игре. Мой опыт не первый год придерживаюсь логичной позиции: проще забирать малый профит, чем спускать абсолютно весь баланс в попытках джекпота. Раз уж возникает потребность малость зайти в слот, обязательно разумно проверить https://intered.help-on.org/blog/index.php?entryid=203724 для выбора свежей информации на сайтах. Дополнительно заметил очередное убеждение, что выдержка сильнее любую пруху на длинной дистанции. Ряд людей считают, что казино — это просто рандом, но толковый взгляд неизменно обеспечивает крутые перспективы. Интересно, а через что сообщество сглаживаете с тильтом после серии минусов? Возможно ли вообще оставаться в стабильном состоянии, если сегодня рандом не прет?
Can you tell us more about this? I’d like to find out some additional information.
I think this is among the most vital info
for me. And i’m glad reading your article. But wanna remark on few general
things, The website style is wonderful, the articles is really
excellent : D. Good job, cheers
You made some nice points there. I did a search on the topic and found most persons will agree with your website.
Some truly wonderful posts on this site, appreciate it for contribution. “I finally know what distinguishes man from other beasts financial worries. – Journals” by Jules Renard.
Saya senang menjadi salah satu dari banyak pengunjung di situs web luar biasa ini (:, salam telah memposting.
I like this web site very much, Its a really nice situation to read and incur information. “Never contend with a man who has nothing to lose.” by Baltasar Gracian.
I’ve learn some just right stuff here. Certainly worth bookmarking for revisiting. I wonder how so much effort you place to make such a magnificent informative site.
Of course, what a magnificent website and instructive posts, I definitely will bookmark your blog.Have an awsome day!
That is really attention-grabbing, You are a very skilled blogger. I have joined your feed and stay up for in quest of extra of your fantastic post. Additionally, I’ve shared your site in my social networks!
I’ve been surfing online more than 3 hours these days, yet I never found any fascinating article like yours. It’s beautiful worth sufficient for me. Personally, if all site owners and bloggers made excellent content as you did, the internet shall be a lot more useful than ever before.
Thank you, I’ve recently been searching for info about this topic for ages and yours is the greatest I have discovered so far. But, what about the bottom line? Are you sure about the source?
I wanted to write you that tiny remark in order to give thanks yet again for the unique ideas you have provided on this website. It’s incredibly open-handed with people like you to offer unhampered what exactly some people might have offered for sale as an e book to help make some cash for themselves, notably since you could possibly have done it if you ever desired. The creative ideas also served to become a great way to recognize that other people online have a similar desire just like mine to figure out very much more with regard to this matter. I know there are thousands of more pleasant times ahead for many who see your website.
Hi there very nice site!! Man .. Excellent .. Superb .. I’ll bookmark your blog and take the feeds alsoKI am glad to find a lot of helpful info right here in the submit, we want work out extra techniques on this regard, thanks for sharing. . . . . .
Would you be interested in exchanging hyperlinks?
This is very interesting, You’re an excessively professional blogger. I’ve joined your feed and look ahead to looking for extra of your fantastic post. Also, I’ve shared your web site in my social networks!
Isi yang luar biasa! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
This design is wicked! You certainly know how to keep a reader entertained. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Fantastic job. I really loved what you had to say, and more than that, how you presented it. Too cool!
With havin so much content and articles do you ever run into any issues of plagorism or copyright violation? My website has a lot of unique content I’ve either authored myself or outsourced but it seems a lot of it is popping it up all over the web without my agreement. Do you know any techniques to help prevent content from being ripped off? I’d genuinely appreciate it.
It is actually a great and useful piece of information. I am satisfied that you shared this helpful information with us. Please stay us up to date like this. Thank you for sharing.
This really answered my problem, thank you!
Pretty! This was a really wonderful post. Thank you for your provided information.
Saya sangat menghargai usaha yang Anda curahkan untuk membuat artikel ini. Konten yang berguna. Terima kasih banyak!
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup posting yang bagus.
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
Great amazing issues here. I am very glad to look your article. Thanks a lot and i am having a look ahead to contact you. Will you please drop me a e-mail?
I have been surfing online greater than 3 hours these days, yet I never discovered any interesting article like yours. It is pretty value enough for me. In my opinion, if all website owners and bloggers made good content as you probably did, the internet will be much more useful than ever before.
Good day! This is my first visit to your blog! We are a collection of volunteers and starting a new initiative in a community in the same niche. Your blog provided us beneficial information to work on. You have done a outstanding job!
You are a very capable person!
You are my inspiration, I possess few web logs and often run out from brand :). “No opera plot can be sensible, for people do not sing when they are feeling sensible.” by W. H. Auden.
WONDERFUL Post.thanks for share..extra wait .. …
Berharga informasi. Beruntung saya menemukan situs web Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Biasanya saya tidak membaca posting di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup artikel yang bagus.
Wonderful web site. Lots of useful info here. I am sending it to several friends ans also sharing in delicious. And of course, thanks for your sweat!
Some genuinely nice stuff on this internet site, I love it.
Great line up. We will be linking to this great article on our site. Keep up the good writing.
Thank you for some other informative site. The place else may just I get that kind of info written in such a perfect approach? I have a challenge that I am just now running on, and I have been at the look out for such info.
Halo di sana, saya menemukan blog Anda melalui Google ketika mencari topik yang serupa, situs Anda muncul di hasil teratas. Saya harus mengatakan bahwa saya terkejut betapa bagus pengaturannya. Saya sangat menyukai menelusuri ini dan saya pasti akan kembali untuk membaca konten lainnya. Terima kasih banyak!
Saya terkesan dengan website ini, amat saya adalah penggemar berat.
Today, while I was at work, my cousin stole my iPad and tested to see if it can survive a forty foot drop, just so she can be a youtube sensation. My apple ipad is now broken and she has 83 views. I know this is completely off topic but I had to share it with someone!
A powerful share, I just given this onto a colleague who was doing somewhat evaluation on this. And he in truth purchased me breakfast as a result of I found it for him.. smile. So let me reword that: Thnx for the deal with! However yeah Thnkx for spending the time to discuss this, I really feel strongly about it and love studying more on this topic. If doable, as you grow to be experience, would you thoughts updating your blog with more details? It’s highly useful for me. Huge thumb up for this weblog submit!
I like this website because so much useful material on here :D.
I love it when people come together and share opinions, great blog, keep it up.
In the awesome design of things you actually receive a B- with regard to effort. Exactly where you actually lost me personally was first on all the particulars. As people say, details make or break the argument.. And it could not be much more true right here. Having said that, let me inform you what exactly did deliver the results. The writing is definitely extremely convincing which is most likely why I am taking an effort in order to opine. I do not really make it a regular habit of doing that. Second, whilst I can notice a leaps in reason you make, I am not necessarily confident of exactly how you appear to unite your points which make the actual final result. For right now I shall yield to your issue but wish in the foreseeable future you actually connect the facts better.
I like what you guys are up too. Such intelligent work and reporting! Keep up the excellent works guys I have incorporated you guys to my blogroll. I think it will improve the value of my site 🙂
Great, I should definitely pronounce, impressed with your website. I had no trouble navigating through all the tabs as well as related info ended up being truly easy to do to access. I recently found what I hoped for before you know it in the least. Quite unusual. Is likely to appreciate it for those who add forums or something, website theme . a tones way for your client to communicate. Nice task.
Heya i am for the first time here. I came across this board and I find It truly useful & it helped me out much. I hope to give something back and help others like you aided me.
This is really interesting, You’re a very skilled blogger. I’ve joined your feed and look forward to seeking more of your magnificent post. Also, I have shared your site in my social networks!
Great post, I believe website owners should acquire a lot from this web site its really user pleasant.
Amat baik info dapat ditemukan di website.
Isi yang berguna dan disajikan dengan sangat baik. Saya tentu akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
I have been absent for some time, but now I remember why I used to love this website. Thanks, I’ll try and check back more frequently. How frequently you update your website?
Menghargai usaha yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
I actually wanted to jot down a simple comment to be able to express gratitude to you for all the great secrets you are sharing here. My time consuming internet search has now been paid with extremely good insight to talk about with my great friends. I would suppose that many of us visitors are definitely blessed to exist in a useful place with many outstanding professionals with very helpful techniques. I feel pretty happy to have encountered the web pages and look forward to so many more pleasurable times reading here. Thank you again for all the details.
Today, I went to the beach front with my children. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is totally off topic but I had to tell someone!
I have been examinating out many of your posts and i can state clever stuff. I will definitely bookmark your blog.
Keep up the fantastic work, I read few blog posts on this site and I conceive that your site is real interesting and has got bands of wonderful info .
Thank you for another excellent article. Where else could anyone get that type of information in such a perfect way of writing? I have a presentation next week, and I’m on the look for such information.
I have been absent for some time, but now I remember why I used to love this web site. Thanks , I’ll try and check back more frequently. How frequently you update your website?
I really like your writing style, great info , regards for posting :D.
With every thing that seems to be building inside this specific subject matter, many of your opinions happen to be very radical. Nonetheless, I beg your pardon, but I can not give credence to your entire suggestion, all be it exhilarating none the less. It seems to everyone that your remarks are actually not completely justified and in actuality you are yourself not even totally confident of the point. In any case I did enjoy examining it.
I as well think so , perfectly composed post! .
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Situs ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Some truly fantastic articles on this website , thanks for contribution.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya perlu mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca dalam waktu yang lama. Konten yang sangat berguna. Terima kasih telah berbagi.
very nice post, i actually love this web site, keep on it
Halo semua, saya menjumpai blog Anda lewat Google saat menelusuri topik yang serupa, blog Anda tampil di bagian atas. Saya perlu mengatakan bahwa saya kagum betapa baik penulisannya. Saya benar-benar menyukai menelusuri ini dan saya akan kembali untuk membaca konten lainnya. Terima kasih!
Saya tidak sangat bagus dalam bahasa Inggris tetapi saya menyadari ini sangat santai untuk diterjemahkan.
Saya tanpa henti memikirkan hal ini, sangat dihargai telah memposting.
Artikel ini penuh informasi. Saya sangat menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan berterima kasih kepada Anda.
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
Fantastis website yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan saran dari orang-orang yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Banyak terima kasih!
Keep functioning ,splendid job!
Seseorang secara esensial membantu untuk membuat secara kritis artikel saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan hingga kini? Saya terkejut dengan riset yang Anda lakukan untuk membuat posting luar biasa ini. Pekerjaan yang mengagumkan!
Menikmati mempelajari ini, sangat bagus, terima kasih.
Hore google adalah raja saya yang menolong saya menemukan website yang hebat! .
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya mendapatkan info yang bagus dari blog Anda.
Saya sungguh puas menemukan situs internet ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke fav.
so much great info on here, :D.
Thanks for the sensible critique. Me & my neighbor were just preparing to do some research on this. We got a grab a book from our area library but I think I learned more from this post. I am very glad to see such magnificent information being shared freely out there.
Seseorang pada dasarnya membantu untuk membuat sangat posting saya mungkin katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga sekarang? Saya terkejut dengan analisis yang Anda lakukan untuk membuat posting menakjubkan ini. Aktivitas yang mengagumkan!
Thank you a bunch for sharing this with all folks you actually know what you are talking about! Bookmarked. Kindly additionally visit my website =). We will have a hyperlink change arrangement among us!
Wow! Terima kasih! Saya terus-menerus ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan fragmen dari posting Anda ke blog saya?
Artikel yang sangat bagus. Ini memberikan saya gambaran yang lebih jelas tentang topik ini. Teruskan pekerjaan yang luar biasa!
F*ckin’ tremendous issues here. I’m very glad to see your post. Thank you so much and i’m having a look forward to contact you. Will you please drop me a e-mail?
Postingan yang sangat membantu. Saya baru menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi.
Konten yang bermanfaat dan disajikan dengan sangat baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Some genuinely fantastic content on this website, thank you for contribution. “It is not often that someone comes along who is a true friend and a good writer.” by E. B. White.
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada cara Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Hello, I do think your site may be having internet browser compatibility problems.
When I take a look at your web site in Safari,
it looks fine however, if opening in Internet Explorer, it has some overlapping
issues. I merely wanted to provide you with a quick heads up!
Aside from that, great site!
Terima kasih untuk posting sangat baik tambahan. Di mana lagi siapa pun dapat mendapatkan tipe info seperti itu dengan metode penulisan yang ideal? Saya punya presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Saya secara tidak sengaja menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
I would like to thnkx for the efforts you have put in writing this blog. I am hoping the same high-grade site post from you in the upcoming also. Actually your creative writing abilities has inspired me to get my own website now. Really the blogging is spreading its wings fast. Your write up is a great example of it.
Hey there would you mind sharing which blog platform you’re using? I’m planning to start my own blog soon but I’m having a tough time making a decision between BlogEngine/Wordpress/B2evolution and Drupal. The reason I ask is because your design and style seems different then most blogs and I’m looking for something unique. P.S Apologies for getting off-topic but I had to ask!
I like this post, enjoyed this one thankyou for putting up.
hey there and thanks on your information – I have definitely picked up something new from right here. I did then again experience a few technical issues the usage of this site, since I skilled to reload the website a lot of times prior to I could get it to load correctly. I have been brooding about if your web hosting is OK? Now not that I’m complaining, but slow loading instances times will very frequently have an effect on your placement in google and could damage your high quality ranking if ads and ***********|advertising|advertising|advertising and *********** with Adwords. Well I am adding this RSS to my email and could look out for a lot extra of your respective interesting content. Ensure that you update this again soon..
I think other website proprietors should take this site as an model, very clean and magnificent user friendly style and design, let alone the content. You’re an expert in this topic!
Wonderful website you have here but I was wondering if you knew of any user discussion forums that cover the same topics talked about in this article? I’d really like to be a part of online community where I can get comments from other knowledgeable people that share the same interest. If you have any recommendations, please let me know. Bless you!
Saya perlu mengatakan, ini adalah salah satu artikel paling bagus yang pernah saya baca belakangan ini. Konten yang sangat berguna. Terima kasih telah berbagi.
Hey very cool site!! Man .. Excellent .. Amazing .. I’ll bookmark your web site and take the feeds also…I am happy to find numerous useful information here in the post, we need develop more strategies in this regard, thanks for sharing. . . . . .
Informasi yang berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Your comment is awaiting moderation.
https://www.youtube.com/@kliveaeorg
https://x.com/kliveaeorg
https://tooter.in/kliveaeorg
https://wakelet.com/@kliveaeorg
https://safechat.com/u/kliveaeorg
https://gravatar.com/kliveaeorg
https://www.pinterest.com/kliveaeorg/
https://shareyoursocial.com/kliveaeorg
https://myspace.com/kliveaeorg
https://500px.com/p/kliveaeorg
https://www.instapaper.com/p/kliveaeorg
https://protocol.ooo/ja/users/kliveaeorg
https://www.reddit.com/user/kliveaeorg/
https://audiomack.com/kliveaeorg
https://hackaday.io/kliveaeorg
https://fyers.in/community/member/qjfanBYUO7
https://leetcode.com/kliveaeorg/
https://swag.live/en/u/kliveaeorg
https://www.halaltrip.com/user/profile/366705/kliveaeorg/
https://medibang.com/author/28736037/
https://www.blockdit.com/kliveaeorg
https://portfolium.com/klive3
https://www.twitch.tv/kliveaeorg/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:F48581A26A4C588C0A495E7A@AdobeID
https://profile.hatena.ne.jp/kliveaeorg/profile
https://docs.google.com/presentation/d/1U8KXYI5fKZWdForFHUlMY22lihL8sxwhbBCE62bWO00/edit?usp=sharing
https://issuu.com/kliveaeorg
https://www.behance.net/kliveaeorg
https://www.reverbnation.com/artist/kliveaeorg
https://www.myminifactory.com/users/kliveaeorg
https://www.investagrams.com/Profile/kliveaeorg
https://gifyu.com/kliveaeorg
https://www.walkscore.com/people/117653056299/kliveaeorg
https://topsitenet.com/profile/kliveaeorg/2130219/
https://akniga.org/profile/1443444-klive/
https://disqus.com/by/kliveaeorg/about/
https://jobs.suncommunitynews.com/profiles/8542551-klive
https://www.speedrun.com/users/kliveaeorg
https://www.fanart-central.net/user/kliveaeorg/profile
https://www.aicrowd.com/participants/kliveaeorg
https://www.bitchute.com/channel/YcMQUUZGYhM9
https://pbase.com/kliveaeorg
https://hub.docker.com/u/kliveaeorg
https://www.gta5-mods.com/users/kliveaeorg
https://heylink.me/dalesandalphon/
https://pixabay.com/users/kliveaeorg-56593570/
http://nicovideo.jp/user/144767675
https://www.jigsawplanet.com/kliveaeorg
https://3dwarehouse.sketchup.com/by/kliveaeorg
https://robertsspaceindustries.com/en/citizens/kliveaeorg
https://bit.ly/m/kliveaeorg
https://allmylinks.com/kliveaeorg
https://www.tumblr.com/kliveaeorg
https://sites.google.com/view/kliveaeorg/
https://www.slideshare.net/dalesandalphon?tab=about
https://web.bikemap.net/u/kliveaeorg
https://www.xiuwushidai.com/home.php?mod=space&uid=2785517
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6716882
https://forum.dboglobal.to/wsc/index.php?user/153853-kliveaeorg/#about
https://rb.gy/pfstmk
https://files.fm/kliveaeorg/info
https://www.mynbest.info/profile/dalesandalphon52579/profile
https://jasa-seo.mn.co/members/40470580
https://creativemarket.com/users/kliveaeorg
https://www.zazzle.co.uk/mbr/238677052994275198
https://maps.arosalenzerheide.swiss/en/member/klive-nha-cai/345791844/
https://luma.com/user/kliveaeorg
https://www.africangenesis-101.org/profile/dalesandalphon82384/profile
https://www.proko.com/@klive_3/activity
https://www.miseducationofmotherhood.com/profile/dalesandalphon55315/profile
https://www.housedumonde.com/profile/dalesandalphon30250/profile
https://t.ly/ZAQJI
https://m.xtutti.com/user/profile/496427
https://postr.blog/profile/kliveaeorg
https://kliveaeorg.stck.me/
https://surli.cc/dcgbmn
https://joy.link/kliveaeorg
https://connect.garmin.com/app/profile/3bbc322b-98b2-4b47-bd74-49efdd83370e
https://b.hatena.ne.jp/kliveaeorg/bookmark
https://www.chichi-pui.com/users/kliveaeorg/
https://www.mellow-fan.com/user/kliveaeorg/about
https://routinehub.co/user/kliveaeorg
https://pxhere.com/en/photographer-me/5065880
https://teletype.in/@kliveaeorg
https://www.checkli.com/kliveaeorg#/a/process
https://www.nintendo-master.com/profil/kliveaeorg
https://freeimage.host/kliveaeorg
https://motion-gallery.net/users/1010448
https://linkin.bio/kliveaeorg/
https://biomolecula.ru/authors/162792
https://talk.plesk.com/members/kliveaeorg.520209/#about
https://www.callupcontact.com/b/businessprofile/orgklive/10154264
https://www.growkudos.com/profile/nha_klive
https://blender.community/klive29/
https://doselect.com/@f167ac4c45fd7573a9e2358d1
https://matkafasi.com/user/kliveaeorg
https://allmyfaves.com/kliveaeorg
https://www.notebook.ai/users/1393048
https://www.abclinuxu.cz/lide/kliveaeorg
https://muare.vn/shop/klive-28/912996
https://lookingforclan.com/user/kliveaeorg
https://forum.dmec.vn/index.php?members/kliveaeorg.206912/
https://igli.me/kliveaeorg
http://delphi.larsbo.org/user/kliveaeorg
https://timdaily.vn/members/kliveaeorg.141524/#about
https://app.readthedocs.org/profiles/kliveaeorg/
https://www.dibiz.com/dalesandalphon
https://iszene.com/user-361522.html
https://www.theyeshivaworld.com/coffeeroom/users/kliveaeorg
https://desksnear.me/users/kliveaeorg
https://www.itchyforum.com/en/member.php?397947-kliveaeorg
https://www.roton.com/forums/users/dalesandalphon/
https://able2know.org/user/kliveaeorg/
http://www.biblesupport.com/user/860416-kliveaeorg/
https://golosknig.com/profile/kliveaeorg/
https://wallhaven.cc/user/kliveaeorg
https://bandori.party/user/1358211/kliveaeorg/
https://schoolido.lu/user/kliveaeorg/
https://awan.pro/forum/user/194618/
https://fortunetelleroracle.com/profile/kliveaeorg
https://fabble.cc/kliveaeorg
https://pad.stuve.de/s/BUFH6fn_L
https://pad.geolab.space/s/9wcUOz7tG
https://www.sythe.org/members/kliveaeorg.2070530/
https://about.me/kliveaeorg/
https://www.equinenow.com/farm/klive-1342409.htm
https://wefunder.com/kliveaeorg/about
https://potofu.me/kliveaeorg
https://transfur.com/Users/kliveaeorg
https://github.com/kliveaeorg
https://qna.habr.com/user/kliveaeorg
https://website.informer.com/klive.ae.org
https://lightroom.adobe.com/u/kliveaeorg
https://en.islcollective.com/portfolio/12961693
https://www.xosothantai.com/members/kliveaeorg.626329/
https://velog.io/@kliveaeorg/about
https://iplogger.com/2Hm4R5
https://mez.ink/kliveaeorg
https://notionpress.com/author/1549850
https://digiphoto.techbang.com/users/kliveaeorg
https://leakedmodels.com/forum/members/kliveaeorg.726716/#about
https://freeicons.io/profile/952629
https://onlinesequencer.net/members/291805
https://inkbunny.net/kliveaeorg
https://www.japaaan.com/user/108925/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/dalesandalphon
https://beatsaver.com/playlists/1230830
https://apptuts.bio/kliveaeorg-274513
https://www.storenvy.com/kliveaeorg
https://forums.maxperformanceinc.com/forums/member.php?u=255958
https://egl.circlly.com/users/kliveaeorg
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=317382
https://acomics.ru/-kliveaeorg
https://www.criminalelement.com/members/kliveaeorg/profile/
https://writexo.com/share/6a4e7ae120d6
https://expatguidekorea.com/profile/kliveaeorg/
https://www.heavyironjobs.com/profiles/8544072-klive
https://pad.degrowth.net/s/0w2do_vwx
https://forum.skullgirlsmobile.com/members/kliveaeorg.241307/#about
https://jobs.landscapeindustrycareers.org/profiles/8544797-klive
https://phatwalletforums.com/user/kliveaeorg/
https://song.link/kliveaeorg
https://idol.st/user/196529/kliveaeorg/
https://jobs.windomnews.com/profiles/8544817-klive
https://hoaxbuster.com/redacteur/kliveaeorg
https://www.givey.com/kliveaeorg
https://zerosuicidetraining.edc.org/user/profile.php?id=588487
https://www.hobowars.com/game/linker.php?url=https://klive.ae.org/
https://jobs.westerncity.com/profiles/8544852-klive
https://www.thetriumphforum.com/members/kliveaeorg.72640/
https://album.link/nvbskbqjn9rgd
https://dev.muvizu.com/Profile/kliveaeorg/Latest
https://chaloke.com/forums/users/kliveaeorg/
https://buckeyescoop.com/community/members/outstanding-lavender-blue-kitsune.69063/#about
http://forum.cncprovn.com/members/435398-kliveaeorg
https://forum.aigato.vn/user/kliveaeorg
https://rapidapi.com/user/dalesandalphon
https://www.skool.com/@nha-cai-klive-2967
https://learningapps.org/watch?v=pkdo39gzj26
https://www.invelos.com/UserProfile.aspx?alias=kliveaeorg
https://www.video-bookmark.com/bookmark/7172498/kliveaeorg/
https://gitlab.vuhdo.io/kliveaeorg
https://poipiku.com/13973542/
https://www.rwaq.org/users/kliveaeorg
https://www.fundable.com/nha-cai-klive-1
https://www.grepmed.com/kliveaeorg
https://classificados.acheiusa.com/profile/a2tLNmRuODEySUdhazhCQXZCSUNvUldpRXc0VlE1R1A5blpESVh2Vm8rRT0=
https://espritgames.com/members/51823020/
https://www.haikudeck.com/presentations/kliveaeorg
https://hi-fi-forum.net/profile/1176818
https://undrtone.com/kliveaeorg
https://marshallyin.com/members/kliveaeorg/
https://www.atozed.com/forums/user-90153.html
https://gravesales.com/author/kliveaeorg/
https://belgaumonline.com/profile/kliveaeorg/
https://zzb.bz/kliveaeorg
https://www.themeqx.com/forums/users/kliveaeorg/
http://newdigital-world.com/members/kliveaeorg.html
https://www.xen-factory.com/index.php?members/kliveaeorg.174373/#about
https://forums.servethehome.com/index.php?members/kliveaeorg.257720/#about
https://www.blackhatprotools.info/member.php?300901-kliveaeorg
https://snippet.host/saxhax
https://tudomuaban.com/chi-tiet-rao-vat/2958510/kliveaeorg.html
https://phijkchu.com/a/kliveaeorg/video-channels
https://lifeinsys.com/user/kliveaeorg
https://kaeuchi.jp/forums/users/kliveaeorg/
https://www.claimajob.com/profiles/8545239-klive
https://protospielsouth.com/user/149254
https://theafricavoice.com/profile/kliveaeorg
https://support.bitspower.com/support/user/kliveaeorg
https://www.brownbook.net/business/55286679/klive
https://hackmd.okfn.de/s/ryEa4I9mfe
https://manylink.co/@kliveaeorg
https://anyflip.com/homepage/cdnts#About
https://www.akaqa.com/question/q19192714061-Kliveaeorg
https://www.threadless.com/@kliveaeorg/activity
https://civitai.com/user/kliveaeorg
https://www.spigotmc.org/members/kliveaeorg.2569472/
https://hoo.be/kliveaeorg
https://maxforlive.com/profile/user/kliveaeorg?tab=about
https://mathlog.info/users/wikBRn6ZqKX4m90yVz8PbJPc8O02
https://my.bio/ketquanet30com
https://fora.babinet.cz/profile.php?id=134726
https://www.shippingexplorer.net/en/user/kliveaeorg/310169
https://connect.gt/user/kliveaeorg
https://www.weddingbee.com/members/kliveaeorg/
https://kumu.io/kliveaeorg/kliveaeorg#untitled-map
https://www.sunlitcentrekenya.co.ke/author/kliveaeorg/
https://www.rcuniverse.com/forum/members/kliveaeorg.html
https://www.huntingnet.com/forum/members/kliveaeorg.html
https://vimeo.com/kliveaeorg
https://www.symbaloo.com/mix/klive
https://www.bricklink.com/aboutMe.asp?u=kliveaeorg
https://www.trackyserver.com/profile/264657
https://www.zubersoft.com/mobilesheets/forum/user-149771.html
https://md.coredump.ch/s/54X5VKxdf
https://aprenderfotografia.online/usuarios/kliveaeorg/profile/
https://hackmd.hub.yt/s/6KCBAVPFF
https://sciencemission.com/profile/kliveaeorg
https://www.wvhired.com/profiles/8545478-klive
https://formulamasa.com/elearning/members/kliveaeorg/?v=96b62e1dce57
https://chyoa.com/user/kliveaeorg
https://www.royalroad.com/profile/1017686
https://backloggd.com/u/kliveaeorg/
https://forums.alliedmods.net/member.php?u=487755
https://viblo.asia/u/kliveaeorg/contact
https://hype4.academy/profile/kliveaeorg
https://brain-market.com/u/kliveaeorg
https://ikanakama.ink/users/344192
https://www.prosebox.net/book/118809/
https://redirect.camfrog.com/redirect/?url=https://klive.ae.org/
https://www.fw-follow.com/forum/topic/157048/kliveaeorg
https://www.navacool.com/forum/topic/517426/kliveaeorg
https://www.driedsquidathome.com/forum/topic/185822/kliveaeorg
https://www.nongkhaempolice.com/forum/topic/186335/kliveaeorg
https://www.bestloveweddingstudio.com/forum/topic/113499/kliveaeorg
https://www.natthadon-sanengineering.com/forum/topic/142398/kliveaeorg
https://www.rueanmaihom.net/forum/topic/129721/kliveaeorg
https://www.ttlxshipping.com/forum/topic/517431/kliveaeorg
http://worldchampmambo.com/UserProfile/tabid/42/userId/504688/Default.aspx
http://forum.modulebazaar.com/forums/user/kliveaeorg/
https://www.rcmx.net/userinfo.php?uid=22358
https://eilo.org/user/kliveaeorg
https://lqdoj.edu.vn/user/kliveaeorg
https://indiestorygeek.com/user/kliveaeorg
https://www.bandlab.com/kliveaeorg
https://forum.issabel.org/u/kliveaeorg
https://www.easyhits4u.com/profile.cgi?login=kliveaeorg
https://doc.anagora.org/s/MzPT9LCDV
https://profile.sampo.ru/kliveaeorg
https://www.ekdarun.com/forum/topic/186067/kliveaeorg
https://fanclove.jp/profile/nK20GY1bBo
https://www.d-ushop.com/forum/topic/184095/kliveaeorg
https://ketcau.com/member/134455-kliveaeorg
https://fengshuidirectory.com/dashboard/listings/kliveaeorg/
https://library.zortrax.com/members/kliveaeorg/
https://pets4friends.com/profile-1654970
https://participa.aytojaen.es/profiles/kliveaeorg/activity
https://linkmix.co/56955329
https://muckrack.com/klive-aeorg/bio
http://linoit.com/users/kliveaeorg/canvases/kliveaeorg
https://www.myconcertarchive.com/en/user_home?id=137081
https://forum.jatekok.hu/User-kliveaeorg
https://www.buymusic.club/user/kliveaeorg
https://forum.freero.org/space-uid-26859.html
http://genina.com/user/editDone/5454519.page
https://wikifab.org/wiki/Utilisateur:Kliveaeorg
https://pad.lescommuns.org/s/EO-OFKrsB
https://rant.li/kliveaeorg/kliveaeorg
https://chanylib.ru/ru/forum/user/35049/
https://producerbox.com/users/kliveaeorg
https://skrolli.fi/keskustelu/users/dalesandalphon/
https://www.thehockeypaper.co.uk/forums/users/kliveaeorg
https://www.11plus.co.uk/users/dalesandalphon/
https://opaseke.com/users/17091
https://www.newgenstravel.com/forum/topic/67664/kliveaeorg
https://zbrushcentral.jp/user/kliveaeorg
https://www.mapleprimes.com/users/kliveaeorg
https://noti.st/kliveaeorg
https://www.adpost.com/u/dalesandalphon/
https://guitarmaking.co.uk/members/kliveaeorg/activity/196667/
https://scrapbox.io/kliveaeorg/kliveaeorg
https://circle-book.com/circles/73771
https://qiita.com/kliveaeorg
https://www.annuncigratuititalia.it/author/kliveaeorg/
https://lite.link/kliveaeorg
http://www.brenkoweb.com/user/100650/profile
https://hedgedoc.faimaison.net/s/iRG681ip46
https://www.townscript.com/o/kliveaeorg
https://www.scamadviser.com/check-website/klive.ae.org
https://adplist.org/members/dalesandalphongmailcom-mrbgl0mm
https://novel.daysneo.com/author/kliveaeorg/
https://destaquebrasil.com/saopaulo/author/kliveaeorg/
https://www.adsfare.com/kliveaeorg
https://bhmtsff.com/space-uid-99049.html
https://blog.sighpceducation.acm.org/wp/forums/users/kliveaeorg/
https://www.tacter.com/@kliveaeorg
https://vc.ru/id6035523
https://l2top.co/forum/members/kliveaeorg.204452/
https://artist.link/nvbskbqjn9rgd
https://dreevoo.com/profile_info.php?pid=2022524
https://www.passes.com/kliveaeorg
https://backloggery.com/kliveaeorg
http://palangshim.com/space-uid-5332017.html
https://etextpad.com/hn4obfzdos
https://app.talkshoe.com/user/kliveaeorg
https://m.wibki.com/kliveaeorg
https://pinshape.com/users/9004448-kliveaeorg
https://sfx.thelazy.net/users/u/kliveaeorg/
https://www.skypixel.com/users/djiuser-5eecm7pqdua2
https://pictureinbottle.com/r/kliveaeorg
https://forum.epicbrowser.com/profile.php?id=168889
https://hedgedoc.eclair.ec-lyon.fr/s/LEpmLtM5j
https://www.socialbookmarkssite.com/bookmark/6282575/kliveaeorg/
https://www.hogwartsishere.com/profile/1853829/
https://linqto.me/about/kliveaeorg
https://www.managementpedia.com/members/kliveaeorg.1126375/#about
https://partecipa.poliste.com/profiles/kliveaeorg/activity
https://hedgedoc.stusta.de/s/ed9kPGmUS
https://pad.codefor.fr/s/AETsJjk0ju
https://pad.fablab-siegen.de/s/P880hiy51l
https://hedgedoc.dezentrale.space/s/obzY2blXK
https://pad.darmstadt.social/s/snzEUd2AAR
https://referrallist.com/profile/kliveaeorg/
https://md.chaosdorf.de/s/oxnDmvpYVh
https://telegra.ph/kliveaeorg-07-08
https://runtrip.jp/users/809297
https://www.bonback.com/forum/topic/518498/kliveaeorg
https://www.pathumratjotun.com/forum/topic/220502/kliveaeorg
https://www.iglinks.io/dalesandalphon-lq0
https://www.bidhub.com/profiles/show/23936
https://www.dokkan-battle.fr/forums/users/kliveaeorg/
https://homepage.ninja/kliveaeorg
https://boss.why3s.cc/boss/home.php?mod=space&uid=288652
https://www.foriio.com/kliveaeorg
https://md.rappet.xyz/s/CCcWeU6tl-
https://md.sebastians.dev/s/rArJe3CDA
https://controlc.com/p93toect
https://justpaste.it/u/kliveaeorg
https://www.pozible.com/profile/kliveaeorg
https://www.elephantjournal.com/profile/kliveaeorg/
https://forum.allkpop.com/suite/user/323085-kliveaeorg/#about
https://strikefans.com/forum/users/kliveaeorg/
https://swat-portal.com/forum/wcf/user/56859-kliveaeorg/#about
https://experiment.com/users/kkliveaeorg
https://forum-foxess.pro/community/profile/kliveaeorg/
http://julia4tied.de/member.php?action=profile&uid=254378
https://mercadodinamico.com.br/author/kliveaeorg/
https://www.grabcaruber.com/members/kliveaeorg/profile/
https://bioqoo.com/kliveaeorg
https://turcia-tours.ru/forum/profile/kliveaeorg/
https://bike-forum.cz/profil/u/kliveaeorg
https://galleria.emotionflow.com/195270/profile.html
https://www.myget.org/users/kliveaeorg
https://app.brancher.ai/user/LEi_tTDV4zHe
https://confengine.com/user/kliveaeorg
https://mygamedb.com/profile/kliveaeorg
https://forum.aceinna.com/user/kliveaeorg
https://www.giveawayoftheday.com/forums/profile/1984760
https://uiverse.io/profile/klive_4575
https://cofacts.tw/user/kliveaeorg
https://vcook.jp/users/106179
https://www.efunda.com/members/people/show_people.cfm?Usr=kliveaeorg
https://pumpyoursound.com/u/user/1642105
https://usdinstitute.com/forums/users/kliveaeorg/
https://congdongx.com/thanh-vien/kliveaeorg.56403/#about
https://www.intensedebate.com/people/kliveaeor
https://tabelog.com/rvwr/kliveaeorg/prof/
https://app.parler.com/kliveaeorg
https://gitlab.com/kliveaeorg
https://gamblingtherapy.org/forum/users/kliveaeorg/
https://www.diigo.com/user/kliveaeorg
http://marshmallow-qa.com/3cxqf73v3ae0uik
https://us.enrollbusiness.com/BusinessProfile/7870966/kliveaeorg
https://link4u.cc/@kliveaeorg
https://its-my.link/@kliveaeorg
https://truckymods.io/user/519652
https://iplogger.org/vn/logger/a0XU5WnlVaCk/
https://www.iniuria.us/forum/member.php?698272-kliveaeorg
https://cointr.ee/kliveaeorg
https://indian-tv.cz/u/kliveaeorg
https://hedgedoc.envs.net/s/xQlBG-vuu
https://illust.daysneo.com/illustrator/kliveaeorg/
https://aniworld.to/user/profil/kliveaeorg
https://www.hentai-foundry.com/user/kliveaeorg/profile
http://teletype.link/kliveaeorg
https://hubb.link/kliveaeorg/
https://www.czporadna.cz/user/kliveaeorg
https://tutorialslink.com/member/kliveundefined/108967
https://expathealthseoul.com/profile/kliveaeorg/
https://www.goodreads.com/user/show/202493541-kliveaeorg
https://www.weddingvendors.com/directory/profile/45682/
https://uno-en-ligne.com/profile.php?user=431178
https://www.letsdobookmark.com/user/nLrFujMOS6n8
https://hub.vroid.com/en/users/127588432
https://www.mateball.com/kliveaeorg
https://gitlab.mpi-sws.org/kliveaeorg
https://ofuse.me/kliveaeorg
https://raovat.nhadat.vn/members/kliveaeorg-331315.html
https://advego.com/profile/kliveaeorg/
https://bio.site/kliveaeorg
https://www.vnbadminton.com/members/kliveaeorg.89070/
https://www.myebook.com/user_profile.php?id=ketquanet30com
https://gourmet-calendar.com/users/kliveaeorg
https://www.sunemall.com/board/board_topic/8431232/8659695.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8659696.htm
https://graph.org/kliveaeorg-07-13
https://cars.yclas.com/user/kliveaeorg
https://scanverify.com/siteverify.php?site=klive.ae.org
https://naijamatta.com/kliveaeorg
https://play-uno.com/profile.php?user=431178
https://www.fcc.gov/fcc-bin/bye?https://klive.ae.org/
https://calgarybusinesses.ca/dashboard/reviews/kliveaeorg/
https://www.sciencebee.com.bd/qna/user/kliveaeorg
https://www.notariosyregistradores.com/web/forums/usuario/kliveaeorg/
https://luvly.co/users/kliveaeorg
https://www.aipictors.com/users/cd69a3d4-1f5c-46e5-dee8-a355d3df3773
https://campsite.bio/kliveaeorg
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8659761.htm
https://www.tai-ji.net/board/board_topic/4160148/8659774.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8659773.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8659772.htm
https://kheotay.com.vn/forums/users/dalesandalphon
https://alfounder.com/forums/users/kliveaeorg/
https://zepodcast.com/forums/users/kliveaeorg/
Your comment is awaiting moderation.
https://www.youtube.com/@kliveaeorg
https://x.com/kliveaeorg
https://tooter.in/kliveaeorg
https://wakelet.com/@kliveaeorg
https://safechat.com/u/kliveaeorg
https://gravatar.com/kliveaeorg
https://www.pinterest.com/kliveaeorg/
https://shareyoursocial.com/kliveaeorg
https://myspace.com/kliveaeorg
https://500px.com/p/kliveaeorg
https://www.instapaper.com/p/kliveaeorg
https://protocol.ooo/ja/users/kliveaeorg
https://www.reddit.com/user/kliveaeorg/
https://audiomack.com/kliveaeorg
https://hackaday.io/kliveaeorg
https://fyers.in/community/member/qjfanBYUO7
https://leetcode.com/kliveaeorg/
https://swag.live/en/u/kliveaeorg
https://www.halaltrip.com/user/profile/366705/kliveaeorg/
https://medibang.com/author/28736037/
https://www.blockdit.com/kliveaeorg
https://portfolium.com/klive3
https://www.twitch.tv/kliveaeorg/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:F48581A26A4C588C0A495E7A@AdobeID
https://profile.hatena.ne.jp/kliveaeorg/profile
https://docs.google.com/presentation/d/1U8KXYI5fKZWdForFHUlMY22lihL8sxwhbBCE62bWO00/edit?usp=sharing
https://issuu.com/kliveaeorg
https://www.behance.net/kliveaeorg
https://www.reverbnation.com/artist/kliveaeorg
https://www.myminifactory.com/users/kliveaeorg
https://www.investagrams.com/Profile/kliveaeorg
https://gifyu.com/kliveaeorg
https://www.walkscore.com/people/117653056299/kliveaeorg
https://topsitenet.com/profile/kliveaeorg/2130219/
https://akniga.org/profile/1443444-klive/
https://disqus.com/by/kliveaeorg/about/
https://jobs.suncommunitynews.com/profiles/8542551-klive
https://www.speedrun.com/users/kliveaeorg
https://www.fanart-central.net/user/kliveaeorg/profile
https://www.aicrowd.com/participants/kliveaeorg
https://www.bitchute.com/channel/YcMQUUZGYhM9
https://pbase.com/kliveaeorg
https://hub.docker.com/u/kliveaeorg
https://www.gta5-mods.com/users/kliveaeorg
https://heylink.me/dalesandalphon/
https://pixabay.com/users/kliveaeorg-56593570/
http://nicovideo.jp/user/144767675
https://www.jigsawplanet.com/kliveaeorg
https://3dwarehouse.sketchup.com/by/kliveaeorg
https://robertsspaceindustries.com/en/citizens/kliveaeorg
https://bit.ly/m/kliveaeorg
https://allmylinks.com/kliveaeorg
https://www.tumblr.com/kliveaeorg
https://sites.google.com/view/kliveaeorg/
https://www.slideshare.net/dalesandalphon?tab=about
https://web.bikemap.net/u/kliveaeorg
https://www.xiuwushidai.com/home.php?mod=space&uid=2785517
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6716882
https://forum.dboglobal.to/wsc/index.php?user/153853-kliveaeorg/#about
https://rb.gy/pfstmk
https://files.fm/kliveaeorg/info
https://www.mynbest.info/profile/dalesandalphon52579/profile
https://jasa-seo.mn.co/members/40470580
https://creativemarket.com/users/kliveaeorg
https://www.zazzle.co.uk/mbr/238677052994275198
https://maps.arosalenzerheide.swiss/en/member/klive-nha-cai/345791844/
https://luma.com/user/kliveaeorg
https://www.africangenesis-101.org/profile/dalesandalphon82384/profile
https://www.proko.com/@klive_3/activity
https://www.miseducationofmotherhood.com/profile/dalesandalphon55315/profile
https://www.housedumonde.com/profile/dalesandalphon30250/profile
https://t.ly/ZAQJI
https://m.xtutti.com/user/profile/496427
https://postr.blog/profile/kliveaeorg
https://kliveaeorg.stck.me/
https://surli.cc/dcgbmn
https://joy.link/kliveaeorg
https://connect.garmin.com/app/profile/3bbc322b-98b2-4b47-bd74-49efdd83370e
https://b.hatena.ne.jp/kliveaeorg/bookmark
https://www.chichi-pui.com/users/kliveaeorg/
https://www.mellow-fan.com/user/kliveaeorg/about
https://routinehub.co/user/kliveaeorg
https://pxhere.com/en/photographer-me/5065880
https://teletype.in/@kliveaeorg
https://www.checkli.com/kliveaeorg#/a/process
https://www.nintendo-master.com/profil/kliveaeorg
https://freeimage.host/kliveaeorg
https://motion-gallery.net/users/1010448
https://linkin.bio/kliveaeorg/
https://biomolecula.ru/authors/162792
https://talk.plesk.com/members/kliveaeorg.520209/#about
https://www.callupcontact.com/b/businessprofile/orgklive/10154264
https://www.growkudos.com/profile/nha_klive
https://blender.community/klive29/
https://doselect.com/@f167ac4c45fd7573a9e2358d1
https://matkafasi.com/user/kliveaeorg
https://allmyfaves.com/kliveaeorg
https://www.notebook.ai/users/1393048
https://www.abclinuxu.cz/lide/kliveaeorg
https://muare.vn/shop/klive-28/912996
https://lookingforclan.com/user/kliveaeorg
https://forum.dmec.vn/index.php?members/kliveaeorg.206912/
https://igli.me/kliveaeorg
http://delphi.larsbo.org/user/kliveaeorg
https://timdaily.vn/members/kliveaeorg.141524/#about
https://app.readthedocs.org/profiles/kliveaeorg/
https://www.dibiz.com/dalesandalphon
https://iszene.com/user-361522.html
https://www.theyeshivaworld.com/coffeeroom/users/kliveaeorg
https://desksnear.me/users/kliveaeorg
https://www.itchyforum.com/en/member.php?397947-kliveaeorg
https://www.roton.com/forums/users/dalesandalphon/
https://able2know.org/user/kliveaeorg/
http://www.biblesupport.com/user/860416-kliveaeorg/
https://golosknig.com/profile/kliveaeorg/
https://wallhaven.cc/user/kliveaeorg
https://bandori.party/user/1358211/kliveaeorg/
https://schoolido.lu/user/kliveaeorg/
https://awan.pro/forum/user/194618/
https://fortunetelleroracle.com/profile/kliveaeorg
https://fabble.cc/kliveaeorg
https://pad.stuve.de/s/BUFH6fn_L
https://pad.geolab.space/s/9wcUOz7tG
https://www.sythe.org/members/kliveaeorg.2070530/
https://about.me/kliveaeorg/
https://www.equinenow.com/farm/klive-1342409.htm
https://wefunder.com/kliveaeorg/about
https://potofu.me/kliveaeorg
https://transfur.com/Users/kliveaeorg
https://github.com/kliveaeorg
https://qna.habr.com/user/kliveaeorg
https://website.informer.com/klive.ae.org
https://lightroom.adobe.com/u/kliveaeorg
https://en.islcollective.com/portfolio/12961693
https://www.xosothantai.com/members/kliveaeorg.626329/
https://velog.io/@kliveaeorg/about
https://iplogger.com/2Hm4R5
https://mez.ink/kliveaeorg
https://notionpress.com/author/1549850
https://digiphoto.techbang.com/users/kliveaeorg
https://leakedmodels.com/forum/members/kliveaeorg.726716/#about
https://freeicons.io/profile/952629
https://onlinesequencer.net/members/291805
https://inkbunny.net/kliveaeorg
https://www.japaaan.com/user/108925/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/dalesandalphon
https://beatsaver.com/playlists/1230830
https://apptuts.bio/kliveaeorg-274513
https://www.storenvy.com/kliveaeorg
https://forums.maxperformanceinc.com/forums/member.php?u=255958
https://egl.circlly.com/users/kliveaeorg
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=317382
https://acomics.ru/-kliveaeorg
https://www.criminalelement.com/members/kliveaeorg/profile/
https://writexo.com/share/6a4e7ae120d6
https://expatguidekorea.com/profile/kliveaeorg/
https://www.heavyironjobs.com/profiles/8544072-klive
https://pad.degrowth.net/s/0w2do_vwx
https://forum.skullgirlsmobile.com/members/kliveaeorg.241307/#about
https://jobs.landscapeindustrycareers.org/profiles/8544797-klive
https://phatwalletforums.com/user/kliveaeorg/
https://song.link/kliveaeorg
https://idol.st/user/196529/kliveaeorg/
https://jobs.windomnews.com/profiles/8544817-klive
https://hoaxbuster.com/redacteur/kliveaeorg
https://www.givey.com/kliveaeorg
https://zerosuicidetraining.edc.org/user/profile.php?id=588487
https://www.hobowars.com/game/linker.php?url=https://klive.ae.org/
https://jobs.westerncity.com/profiles/8544852-klive
https://www.thetriumphforum.com/members/kliveaeorg.72640/
https://album.link/nvbskbqjn9rgd
https://dev.muvizu.com/Profile/kliveaeorg/Latest
https://chaloke.com/forums/users/kliveaeorg/
https://buckeyescoop.com/community/members/outstanding-lavender-blue-kitsune.69063/#about
http://forum.cncprovn.com/members/435398-kliveaeorg
https://forum.aigato.vn/user/kliveaeorg
https://rapidapi.com/user/dalesandalphon
https://www.skool.com/@nha-cai-klive-2967
https://learningapps.org/watch?v=pkdo39gzj26
https://www.invelos.com/UserProfile.aspx?alias=kliveaeorg
https://www.video-bookmark.com/bookmark/7172498/kliveaeorg/
https://gitlab.vuhdo.io/kliveaeorg
https://poipiku.com/13973542/
https://www.rwaq.org/users/kliveaeorg
https://www.fundable.com/nha-cai-klive-1
https://www.grepmed.com/kliveaeorg
https://classificados.acheiusa.com/profile/a2tLNmRuODEySUdhazhCQXZCSUNvUldpRXc0VlE1R1A5blpESVh2Vm8rRT0=
https://espritgames.com/members/51823020/
https://www.haikudeck.com/presentations/kliveaeorg
https://hi-fi-forum.net/profile/1176818
https://undrtone.com/kliveaeorg
https://marshallyin.com/members/kliveaeorg/
https://www.atozed.com/forums/user-90153.html
https://gravesales.com/author/kliveaeorg/
https://belgaumonline.com/profile/kliveaeorg/
https://zzb.bz/kliveaeorg
https://www.themeqx.com/forums/users/kliveaeorg/
http://newdigital-world.com/members/kliveaeorg.html
https://www.xen-factory.com/index.php?members/kliveaeorg.174373/#about
https://forums.servethehome.com/index.php?members/kliveaeorg.257720/#about
https://www.blackhatprotools.info/member.php?300901-kliveaeorg
https://snippet.host/saxhax
https://tudomuaban.com/chi-tiet-rao-vat/2958510/kliveaeorg.html
https://phijkchu.com/a/kliveaeorg/video-channels
https://lifeinsys.com/user/kliveaeorg
https://kaeuchi.jp/forums/users/kliveaeorg/
https://www.claimajob.com/profiles/8545239-klive
https://protospielsouth.com/user/149254
https://theafricavoice.com/profile/kliveaeorg
https://support.bitspower.com/support/user/kliveaeorg
https://www.brownbook.net/business/55286679/klive
https://hackmd.okfn.de/s/ryEa4I9mfe
https://manylink.co/@kliveaeorg
https://anyflip.com/homepage/cdnts#About
https://www.akaqa.com/question/q19192714061-Kliveaeorg
https://www.threadless.com/@kliveaeorg/activity
https://civitai.com/user/kliveaeorg
https://www.spigotmc.org/members/kliveaeorg.2569472/
https://hoo.be/kliveaeorg
https://maxforlive.com/profile/user/kliveaeorg?tab=about
https://mathlog.info/users/wikBRn6ZqKX4m90yVz8PbJPc8O02
https://my.bio/ketquanet30com
https://fora.babinet.cz/profile.php?id=134726
https://www.shippingexplorer.net/en/user/kliveaeorg/310169
https://connect.gt/user/kliveaeorg
https://www.weddingbee.com/members/kliveaeorg/
https://kumu.io/kliveaeorg/kliveaeorg#untitled-map
https://www.sunlitcentrekenya.co.ke/author/kliveaeorg/
https://www.rcuniverse.com/forum/members/kliveaeorg.html
https://www.huntingnet.com/forum/members/kliveaeorg.html
https://vimeo.com/kliveaeorg
https://www.symbaloo.com/mix/klive
https://www.bricklink.com/aboutMe.asp?u=kliveaeorg
https://www.trackyserver.com/profile/264657
https://www.zubersoft.com/mobilesheets/forum/user-149771.html
https://md.coredump.ch/s/54X5VKxdf
https://aprenderfotografia.online/usuarios/kliveaeorg/profile/
https://hackmd.hub.yt/s/6KCBAVPFF
https://sciencemission.com/profile/kliveaeorg
https://www.wvhired.com/profiles/8545478-klive
https://formulamasa.com/elearning/members/kliveaeorg/?v=96b62e1dce57
https://chyoa.com/user/kliveaeorg
https://www.royalroad.com/profile/1017686
https://backloggd.com/u/kliveaeorg/
https://forums.alliedmods.net/member.php?u=487755
https://viblo.asia/u/kliveaeorg/contact
https://hype4.academy/profile/kliveaeorg
https://brain-market.com/u/kliveaeorg
https://ikanakama.ink/users/344192
https://www.prosebox.net/book/118809/
https://redirect.camfrog.com/redirect/?url=https://klive.ae.org/
https://www.fw-follow.com/forum/topic/157048/kliveaeorg
https://www.navacool.com/forum/topic/517426/kliveaeorg
https://www.driedsquidathome.com/forum/topic/185822/kliveaeorg
https://www.nongkhaempolice.com/forum/topic/186335/kliveaeorg
https://www.bestloveweddingstudio.com/forum/topic/113499/kliveaeorg
https://www.natthadon-sanengineering.com/forum/topic/142398/kliveaeorg
https://www.rueanmaihom.net/forum/topic/129721/kliveaeorg
https://www.ttlxshipping.com/forum/topic/517431/kliveaeorg
http://worldchampmambo.com/UserProfile/tabid/42/userId/504688/Default.aspx
http://forum.modulebazaar.com/forums/user/kliveaeorg/
https://www.rcmx.net/userinfo.php?uid=22358
https://eilo.org/user/kliveaeorg
https://lqdoj.edu.vn/user/kliveaeorg
https://indiestorygeek.com/user/kliveaeorg
https://www.bandlab.com/kliveaeorg
https://forum.issabel.org/u/kliveaeorg
https://www.easyhits4u.com/profile.cgi?login=kliveaeorg
https://doc.anagora.org/s/MzPT9LCDV
https://profile.sampo.ru/kliveaeorg
https://www.ekdarun.com/forum/topic/186067/kliveaeorg
https://fanclove.jp/profile/nK20GY1bBo
https://www.d-ushop.com/forum/topic/184095/kliveaeorg
https://ketcau.com/member/134455-kliveaeorg
https://fengshuidirectory.com/dashboard/listings/kliveaeorg/
https://library.zortrax.com/members/kliveaeorg/
https://pets4friends.com/profile-1654970
https://participa.aytojaen.es/profiles/kliveaeorg/activity
https://linkmix.co/56955329
https://muckrack.com/klive-aeorg/bio
http://linoit.com/users/kliveaeorg/canvases/kliveaeorg
https://www.myconcertarchive.com/en/user_home?id=137081
https://forum.jatekok.hu/User-kliveaeorg
https://www.buymusic.club/user/kliveaeorg
https://forum.freero.org/space-uid-26859.html
http://genina.com/user/editDone/5454519.page
https://wikifab.org/wiki/Utilisateur:Kliveaeorg
https://pad.lescommuns.org/s/EO-OFKrsB
https://rant.li/kliveaeorg/kliveaeorg
https://chanylib.ru/ru/forum/user/35049/
https://producerbox.com/users/kliveaeorg
https://skrolli.fi/keskustelu/users/dalesandalphon/
https://www.thehockeypaper.co.uk/forums/users/kliveaeorg
https://www.11plus.co.uk/users/dalesandalphon/
https://opaseke.com/users/17091
https://www.newgenstravel.com/forum/topic/67664/kliveaeorg
https://zbrushcentral.jp/user/kliveaeorg
https://www.mapleprimes.com/users/kliveaeorg
https://noti.st/kliveaeorg
https://www.adpost.com/u/dalesandalphon/
https://guitarmaking.co.uk/members/kliveaeorg/activity/196667/
https://scrapbox.io/kliveaeorg/kliveaeorg
https://circle-book.com/circles/73771
https://qiita.com/kliveaeorg
https://www.annuncigratuititalia.it/author/kliveaeorg/
https://lite.link/kliveaeorg
http://www.brenkoweb.com/user/100650/profile
https://hedgedoc.faimaison.net/s/iRG681ip46
https://www.townscript.com/o/kliveaeorg
https://www.scamadviser.com/check-website/klive.ae.org
https://adplist.org/members/dalesandalphongmailcom-mrbgl0mm
https://novel.daysneo.com/author/kliveaeorg/
https://destaquebrasil.com/saopaulo/author/kliveaeorg/
https://www.adsfare.com/kliveaeorg
https://bhmtsff.com/space-uid-99049.html
https://blog.sighpceducation.acm.org/wp/forums/users/kliveaeorg/
https://www.tacter.com/@kliveaeorg
https://vc.ru/id6035523
https://l2top.co/forum/members/kliveaeorg.204452/
https://artist.link/nvbskbqjn9rgd
https://dreevoo.com/profile_info.php?pid=2022524
https://www.passes.com/kliveaeorg
https://backloggery.com/kliveaeorg
http://palangshim.com/space-uid-5332017.html
https://etextpad.com/hn4obfzdos
https://app.talkshoe.com/user/kliveaeorg
https://m.wibki.com/kliveaeorg
https://pinshape.com/users/9004448-kliveaeorg
https://sfx.thelazy.net/users/u/kliveaeorg/
https://www.skypixel.com/users/djiuser-5eecm7pqdua2
https://pictureinbottle.com/r/kliveaeorg
https://forum.epicbrowser.com/profile.php?id=168889
https://hedgedoc.eclair.ec-lyon.fr/s/LEpmLtM5j
https://www.socialbookmarkssite.com/bookmark/6282575/kliveaeorg/
https://www.hogwartsishere.com/profile/1853829/
https://linqto.me/about/kliveaeorg
https://www.managementpedia.com/members/kliveaeorg.1126375/#about
https://partecipa.poliste.com/profiles/kliveaeorg/activity
https://hedgedoc.stusta.de/s/ed9kPGmUS
https://pad.codefor.fr/s/AETsJjk0ju
https://pad.fablab-siegen.de/s/P880hiy51l
https://hedgedoc.dezentrale.space/s/obzY2blXK
https://pad.darmstadt.social/s/snzEUd2AAR
https://referrallist.com/profile/kliveaeorg/
https://md.chaosdorf.de/s/oxnDmvpYVh
https://telegra.ph/kliveaeorg-07-08
https://runtrip.jp/users/809297
https://www.bonback.com/forum/topic/518498/kliveaeorg
https://www.pathumratjotun.com/forum/topic/220502/kliveaeorg
https://www.iglinks.io/dalesandalphon-lq0
https://www.bidhub.com/profiles/show/23936
https://www.dokkan-battle.fr/forums/users/kliveaeorg/
https://homepage.ninja/kliveaeorg
https://boss.why3s.cc/boss/home.php?mod=space&uid=288652
https://www.foriio.com/kliveaeorg
https://md.rappet.xyz/s/CCcWeU6tl-
https://md.sebastians.dev/s/rArJe3CDA
https://controlc.com/p93toect
https://justpaste.it/u/kliveaeorg
https://www.pozible.com/profile/kliveaeorg
https://www.elephantjournal.com/profile/kliveaeorg/
https://forum.allkpop.com/suite/user/323085-kliveaeorg/#about
https://strikefans.com/forum/users/kliveaeorg/
https://swat-portal.com/forum/wcf/user/56859-kliveaeorg/#about
https://experiment.com/users/kkliveaeorg
https://forum-foxess.pro/community/profile/kliveaeorg/
http://julia4tied.de/member.php?action=profile&uid=254378
https://mercadodinamico.com.br/author/kliveaeorg/
https://www.grabcaruber.com/members/kliveaeorg/profile/
https://bioqoo.com/kliveaeorg
https://turcia-tours.ru/forum/profile/kliveaeorg/
https://bike-forum.cz/profil/u/kliveaeorg
https://galleria.emotionflow.com/195270/profile.html
https://www.myget.org/users/kliveaeorg
https://app.brancher.ai/user/LEi_tTDV4zHe
https://confengine.com/user/kliveaeorg
https://mygamedb.com/profile/kliveaeorg
https://forum.aceinna.com/user/kliveaeorg
https://www.giveawayoftheday.com/forums/profile/1984760
https://uiverse.io/profile/klive_4575
https://cofacts.tw/user/kliveaeorg
https://vcook.jp/users/106179
https://www.efunda.com/members/people/show_people.cfm?Usr=kliveaeorg
https://pumpyoursound.com/u/user/1642105
https://usdinstitute.com/forums/users/kliveaeorg/
https://congdongx.com/thanh-vien/kliveaeorg.56403/#about
https://www.intensedebate.com/people/kliveaeor
https://tabelog.com/rvwr/kliveaeorg/prof/
https://app.parler.com/kliveaeorg
https://gitlab.com/kliveaeorg
https://gamblingtherapy.org/forum/users/kliveaeorg/
https://www.diigo.com/user/kliveaeorg
http://marshmallow-qa.com/3cxqf73v3ae0uik
https://us.enrollbusiness.com/BusinessProfile/7870966/kliveaeorg
https://link4u.cc/@kliveaeorg
https://its-my.link/@kliveaeorg
https://truckymods.io/user/519652
https://iplogger.org/vn/logger/a0XU5WnlVaCk/
https://www.iniuria.us/forum/member.php?698272-kliveaeorg
https://cointr.ee/kliveaeorg
https://indian-tv.cz/u/kliveaeorg
https://hedgedoc.envs.net/s/xQlBG-vuu
https://illust.daysneo.com/illustrator/kliveaeorg/
https://aniworld.to/user/profil/kliveaeorg
https://www.hentai-foundry.com/user/kliveaeorg/profile
http://teletype.link/kliveaeorg
https://hubb.link/kliveaeorg/
https://www.czporadna.cz/user/kliveaeorg
https://tutorialslink.com/member/kliveundefined/108967
https://expathealthseoul.com/profile/kliveaeorg/
https://www.goodreads.com/user/show/202493541-kliveaeorg
https://www.weddingvendors.com/directory/profile/45682/
https://uno-en-ligne.com/profile.php?user=431178
https://www.letsdobookmark.com/user/nLrFujMOS6n8
https://hub.vroid.com/en/users/127588432
https://www.mateball.com/kliveaeorg
https://gitlab.mpi-sws.org/kliveaeorg
https://ofuse.me/kliveaeorg
https://raovat.nhadat.vn/members/kliveaeorg-331315.html
https://advego.com/profile/kliveaeorg/
https://bio.site/kliveaeorg
https://www.vnbadminton.com/members/kliveaeorg.89070/
https://www.myebook.com/user_profile.php?id=ketquanet30com
https://gourmet-calendar.com/users/kliveaeorg
https://www.sunemall.com/board/board_topic/8431232/8659695.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8659696.htm
https://graph.org/kliveaeorg-07-13
https://cars.yclas.com/user/kliveaeorg
https://scanverify.com/siteverify.php?site=klive.ae.org
https://naijamatta.com/kliveaeorg
https://play-uno.com/profile.php?user=431178
https://www.fcc.gov/fcc-bin/bye?https://klive.ae.org/
https://calgarybusinesses.ca/dashboard/reviews/kliveaeorg/
https://www.sciencebee.com.bd/qna/user/kliveaeorg
https://www.notariosyregistradores.com/web/forums/usuario/kliveaeorg/
https://luvly.co/users/kliveaeorg
https://www.aipictors.com/users/cd69a3d4-1f5c-46e5-dee8-a355d3df3773
https://campsite.bio/kliveaeorg
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8659761.htm
https://www.tai-ji.net/board/board_topic/4160148/8659774.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8659773.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8659772.htm
https://kheotay.com.vn/forums/users/dalesandalphon
https://alfounder.com/forums/users/kliveaeorg/
https://zepodcast.com/forums/users/kliveaeorg/
Postingan yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi.
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang sangat bagus!
We’re a group of volunteers and starting a new scheme in our community. Your web site offered us with valuable info to work on. You’ve done a formidable job and our entire community will be grateful to you.
I’ve recently started a website, the information you provide on this website has helped me greatly. Thanks for all of your time & work.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Terima kasih atas tulisan yang baik. Faktanya ini sebelumnya adalah sebuah materi hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita bisa tetap berkomunikasi?
Sangat bagus situs yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin menjadi bagian dari komunitas di mana saya bisa mendapatkan masukan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Pekerjaan yang luar biasa!
Your comment is awaiting moderation.
https://www.youtube.com/@klivebid/about
https://x.com/klivebid
https://tooter.in/klivebid
https://wakelet.com/@klivebid1655
https://safechat.com/u/nha.cai.klive
https://gravatar.com/valiantly69480d0818
https://www.blogger.com/profile/09951647480826549274
https://www.pinterest.com/klivebid/
https://shareyoursocial.com/klivebid
https://500px.com/p/klivebid
https://www.instapaper.com/p/klivebid
https://www.band.us/band/103438190/post
https://protocol.ooo/ja/users/klivebid
https://www.reddit.com/user/klivebid/
https://audiomack.com/jermelshanley977
https://hackaday.io/klivebid?saved=true
https://fyers.in/community/member/CuzPBpbXqd
https://leetcode.com/u/klivebid/
https://swag.live/en/u/klivebid
https://www.halaltrip.com/user/profile/366515/klivebid/
https://medibang.com/author/28731609/
https://www.blockdit.com/users/6a4b7f6d6b689fc53d1a7b6c
https://portfolium.com/klivebid
https://www.twitch.tv/klivebid/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:D388819C6A4B81680A495C60@AdobeID
https://profile.hatena.ne.jp/klivebid/profile
https://docs.google.com/presentation/d/1LwEZxOgcMfiT7g8uOMkUitD6_D_cgNQP2ZPUqp6o7nI/edit?usp=sharing
https://issuu.com/klivebid
https://www.behance.net/nhciklive1
https://www.reverbnation.com/klivebid
https://www.myminifactory.com/users/klivebid
https://www.investagrams.com/Profile/klivebid
https://gifyu.com/klivebid
https://www.chordie.com/forum/profile.php?id=2585789
https://www.walkscore.com/people/338479699746/klive
https://topsitenet.com/profile/klivebid/2128902/
https://akniga.org/profile/1443285-klivebid/
https://disqus.com/by/klivebid/about/
https://jobs.suncommunitynews.com/profiles/8540124-nha-cai-klive
https://www.speedrun.com/users/klivebid
https://www.fanart-central.net/user/klivebid/profile
https://www.aicrowd.com/participants/klivebid
https://www.bitchute.com/channel/zgz2Pcz2UqWd
https://pbase.com/klivebid/image/176408964
https://hub.docker.com/u/klivebid
https://www.gta5-mods.com/users/klivebid
https://heylink.me/klivebid/
https://pixabay.com/users/klivebid-56588278/
https://www.nicovideo.jp/user/144763988
https://www.jigsawplanet.com/klivebid
https://3dwarehouse.sketchup.com/by/klivebid
https://robertsspaceindustries.com/en/citizens/klivebid
https://bit.ly/m/klivebid
https://allmylinks.com/klivebid
https://www.tumblr.com/klivebid
https://sites.google.com/view/klivebid/home
https://groups.google.com/g/klivebid/c/D7MYxJyuhoM
https://klivebid.blogspot.com/2026/07/nha-cai-klive.html
https://hashnode.com/@klivebid
https://medium.com/@jermelshanley977/about
https://www.slideshare.net/jermelshanley977?tab=about
https://soundcloud.com/klivebid
https://www.rehashclothes.com/klivebid
https://klivebid.mypixieset.com/
https://web.bikemap.net/u/klivebid
https://www.xiuwushidai.com/home.php?mod=space&uid=2784926
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6714734
https://bookmeter.com/users/1743711
https://party.biz/index.php/profile/389065?tab=541
https://files.fm/klivebid/info
https://startupxplore.com/en/person/klivebid
https://www.mynbest.info/profile/jermelshanley97782981/profile
https://jasa-seo.mn.co/members/40464437
https://www.zazzle.com/mbr/238158691581456632
https://maps.arosalenzerheide.swiss/en/member/klivebid/345770399/
https://luma.com/zy6q0nzg
https://www.africangenesis-101.org/profile/jermelshanley97726597/profile
https://www.proko.com/@klivebid/activity
https://sitereport.netcraft.com/?url=https://klive.bid/
https://www.miseducationofmotherhood.com/profile/jermelshanley97721609/profile
https://www.housedumonde.com/profile/jermelshanley97772530/profile
https://m.xtutti.com/user/profile/496405
https://postr.blog/profile/klivebid
https://jobs.dfw501c.com/profiles/8542411-nha-cai-klive
https://architecture-jobs.architizer.com/profiles/8542414-nha-cai-klive
https://www.webmastersun.com/members/klivebid.172059/#about
https://klivebid.stck.me/profile
https://surli.cc/hohhad
https://joy.link/klivebid
https://connect.garmin.com/app/profile/b5b138f6-1a25-4164-ad75-604813e4c421
https://b.hatena.ne.jp/klivebid/bookmark
https://www.chichi-pui.com/users/klivebid/
https://www.mellow-fan.com/user/dmb9x6640320bfvrmqqy/about
https://unityroom.com/users/39ecqhpuktzdwyimvr84
https://routinehub.co/user/klivebid
https://pxhere.com/en/photographer-me/5065676
https://www.checkli.com/klivebid#/a/process
https://www.nintendo-master.com/profil/klivebid
https://freeimage.host/klivebid
https://motion-gallery.net/users/1010300
https://linkin.bio/klivebid/
https://biomolecula.ru/authors/162712
https://talk.plesk.com/members/klivebid.520149/#about
https://www.callupcontact.com/b/businessprofile/nh_ci_klive/10153989
https://www.growkudos.com/profile/klive_bid
https://blender.community/klivebid/
https://doselect.com/@623249ef840aed7da2dccdbce
https://matkafasi.com/user/klivebid
https://allmyfaves.com/klivebid
https://www.notebook.ai/users/1392921
https://www.abclinuxu.cz/lide/klivebid
https://muare.vn/shop/klivebid/912955
https://musikersuche.musicstore.de/profil/klivebid/
https://lookingforclan.com/user/klivebid
https://forum.dmec.vn/index.php?members/klivebid.206859/
https://igli.me/klivebid
http://delphi.larsbo.org/user/klivebid
https://www.aseeralkotb.com/en/profiles/klivebid-110411559291122544423
https://timdaily.vn/members/klivebid.141498/#about
https://app.readthedocs.org/profiles/klivebid/
https://iszene.com/user-361476.html
https://www.theyeshivaworld.com/coffeeroom/users/klivebid
https://desksnear.me/users/klivebid
https://www.itchyforum.com/en/member.php?397922-klivebid
https://www.roton.com/forums/users/jermelshanley977/
https://able2know.org/user/klivebid/
http://www.biblesupport.com/user/860330-klivebid/
https://golosknig.com/profile/klivebid/
https://wallhaven.cc/user/klivebid
https://bandori.party/user/1357201/klivebid/
https://schoolido.lu/user/klivebid/
https://awan.pro/forum/user/194543/
https://fortunetelleroracle.com/profile/klivebid
https://fabble.cc/klivebid
https://pad.geolab.space/s/B8d8G4NXN
https://pad.stuve.de/s/qpX8FdDrcf
https://www.sythe.org/members/klivebid.2070459/
https://about.me/klivebid
https://www.gaiaonline.com/profiles/klivebid/51685714/
https://wefunder.com/nhciklive
https://potofu.me/klivebid
https://transfur.com/Users/klivebid
https://xtremepape.rs/members/klivebid.691438/#about
https://github.com/klivebid
https://qna.habr.com/user/klivebid
https://website.informer.com/klive.bid/
https://lightroom.adobe.com/u/nhciklive1
https://en.islcollective.com/portfolio/12961552
https://www.xosothantai.com/members/klivebid.626268/
https://velog.io/@klivebid/about
https://violet.vn/user/show/id/15331980
https://iplogger.org/logger/DRZU5ye7Xr3k/
https://mez.ink/klivebid
https://notionpress.com/author/1549745
https://www.edna.cz/uzivatele/klivebid/
https://www.techbang.com/users/klivebid
https://leakedmodels.com/forum/members/klivebid.726680/#about
https://freeicons.io/profile/952560
https://onlinesequencer.net/members/291762
https://inkbunny.net/klivebid
https://www.japaaan.com/user/108888
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.klive
https://beatsaver.com/profile/379446
https://apptuts.bio/klivebid-274468
https://participacion.cabildofuer.es/profiles/klivebid/activity?locale=en
https://forums.maxperformanceinc.com/forums/member.php?u=255926
https://egl.circlly.com/users/klivebid
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=317333
https://acomics.ru/-klivebid
https://www.criminalelement.com/members/klivebid/profile/
https://hanson.net/users/klivebid
https://writexo.com/share/cc6ae1c0064d
https://expatguidekorea.com/profile/nha-cai-klive/
https://www.heavyironjobs.com/profiles/8543061-nha-cai-klive
https://pad.degrowth.net/s/q00RNigrj
https://forum.skullgirlsmobile.com/members/klivebid.241196/#about
https://jobs.landscapeindustrycareers.org/profiles/8543075-nha-cai-klive
https://phatwalletforums.com/user/klivebid/
https://song.link/klivebid
https://idol.st/user/196417/klivebid/
https://gockhuat.net/member.php?u=440606
https://jobs.windomnews.com/profiles/8543139-nha-cai-klive
https://hoaxbuster.com/redacteur/klivebid
https://www.givey.com/klivebid
https://zerosuicidetraining.edc.org/user/profile.php?id=588375
https://www.hobowars.com/game/linker.php?url=https://klive.bid/
https://jobs.westerncity.com/profiles/8543177-nha-cai-klive
https://www.thetriumphforum.com/members/klivebid.72579/
https://album.link/klivebid
https://dev.muvizu.com/Profile/klivebid/Latest
https://chaloke.com/forums/users/klivebid/
https://buckeyescoop.com/community/members/klivebid.69028/#about
http://forum.cncprovn.com/members/435355-klivebid
https://forum.aigato.vn/user/klivebid
https://rapidapi.com/user/jermelshanley977
https://www.skool.com/@nha-cai-klive-9321
https://learningapps.org/watch?v=p3d1uxtoa26
https://www.invelos.com/UserProfile.aspx?Alias=klivebid
https://www.video-bookmark.com/bookmark/7172187/nh%C3%A0-c%C3%A1i-klive/
https://gitlab.vuhdo.io/klivebid
https://poipiku.com/13972826/
https://www.rwaq.org/users/klivebid
https://www.fitday.com/fitness/forums/members/klivebid.html
https://www.fundable.com/klive-bid
https://www.grepmed.com/klivebid
https://classificados.acheiusa.com/profile/NGdBL2hGS2pwMisrajQweDU3OWc4eks3dENNMkdNNkFmVGtBUDhadElvdz0=
https://espritgames.com/members/51820998/
https://www.haikudeck.com/presentations/cSsQYoLfRV
https://hi-fi-forum.net/profile/1176722
https://undrtone.com/klivebid
https://marshallyin.com/members/klivebid/
https://www.atozed.com/forums/user-90146.html
https://gravesales.com/author/klivebid/
https://belgaumonline.com/profile/klivebid/
https://savelist.co/my-lists/users/klivebid
https://zzb.bz/gPpZ37
https://www.themeqx.com/forums/users/klivebid/
http://newdigital-world.com/members/klivebid.html
https://www.xen-factory.com/index.php?members/klivebid.174360/#about
https://www.blackhatprotools.info/member.php?300892-klivebid
https://activepages.com.au/profile/klivebid
https://snippet.host/hwgeph
https://tudomuaban.com/chi-tiet-rao-vat/2958474/nha-cai-klive.html
https://phijkchu.com/a/klivebid/video-channels
https://lifeinsys.com/user/klivebid
https://kaeuchi.jp/forums/users/klivebid/
https://www.claimajob.com/profiles/8545138-nha-cai-klive
https://protospielsouth.com/user/149241
https://theafricavoice.com/profile/klivebid
https://support.bitspower.com/support/user/klivebid
https://www.brownbook.net/business/55286545/klivebid
https://hackmd.okfn.de/s/rkA_fI9Qzl
https://manylink.co/@klivebid
https://anyflip.com/homepage/bqqrs#About
https://www.akaqa.com/question/q19192714057-Nh-ci-klive
https://www.threadless.com/@klivebid/activity
https://civitai.com/user/klivebid
https://hoo.be/klivebid
https://maxforlive.com/profile/user/klivebid?tab=about
https://3dtoday.ru/blogs/klivebid/nha-cai-klive
https://mathlog.info/users/zLHLnLOGOwPnCmzJ4wsHfwXjcgi1
https://my.bio/klivebid
https://fora.babinet.cz/profile.php?id=134761
https://www.shippingexplorer.net/en/user/klivebid/310237
https://connect.gt/user/klivebid/
https://www.weddingbee.com/members/klivebid/
https://kumu.io/klivebid/jermelshanley977#nha-cai-klive
https://www.sunlitcentrekenya.co.ke/author/klivebid/
https://www.rcuniverse.com/forum/members/klivebid.html
https://www.huntingnet.com/forum/members/klivebid.html
https://vimeo.com/klivebid
https://www.symbaloo.com/mix/nha-cai-klive
https://www.bricklink.com/aboutMe.asp?u=klivebid
https://www.trackyserver.com/profile/264702
https://www.zubersoft.com/mobilesheets/forum/user-149824.html
https://md.coredump.ch/s/vhcpAb4em
https://aprenderfotografia.online/usuarios/klivebid/profile/
https://hackmd.hub.yt/s/r23JKKYp-
https://sciencemission.com/profile/klivebid
https://www.wvhired.com/profiles/8546987-nha-cai-klive
https://formulamasa.com/elearning/members/klivebid/
https://backloggd.com/u/klivebid/
https://forums.alliedmods.net/member.php?u=487793
https://community.jmp.com/t5/user/viewprofilepage/user-id/105213
https://viblo.asia/u/klivebid/contact
https://www.thesims3.com/mypage/klivebid/myBlog
https://brain-market.com/u/klivebid
https://ikanakama.ink/users/344202
https://www.prosebox.net/book/118849/
https://www.fw-follow.com/forum/topic/157186/nha-cai-klive
https://www.navacool.com/forum/topic/518046/nha-cai-klive
https://www.driedsquidathome.com/forum/topic/186041/nha-cai-klive
https://www.nongkhaempolice.com/forum/topic/186694/nha-cai-klive
https://www.natthadon-sanengineering.com/forum/topic/142579/nha-cai-klive
https://www.rueanmaihom.net/forum/topic/129891/nha-cai-klive
https://www.ttlxshipping.com/forum/topic/518072/nha-cai-klive
http://worldchampmambo.com/UserProfile/tabid/42/UserID/504666/Default.aspx
http://forum.modulebazaar.com/forums/user/klivebid/
https://www.rcmx.net/userinfo.php?uid=22356
https://eilo.org/user/klivebid
https://lqdoj.edu.vn/user/klivebid
https://indiestorygeek.com/user/klivebid
https://www.bandlab.com/klivebid
https://forum.issabel.org/u/klivebid
https://kvisit.com/Q_7wC
https://www.easyhits4u.com/profile.cgi?login=klivebid&view_as=1
https://doc.anagora.org/s/JRggdYzMA
https://profile.sampo.ru/klivebid
https://www.ekdarun.com/forum/topic/186064/nha-cai-klive
https://fanclove.jp/profile/ypWDe4r6Be
https://www.d-ushop.com/forum/topic/184088/nha-cai-klive
https://lustyweb.live/members/klivebid.155382/#about
https://findaspring.org/members/klivebid/
https://ketcau.com/member/134454-klivebid
https://fengshuidirectory.com/dashboard/listings/klivebid/
https://library.zortrax.com/members/nha-cai-klive/
https://pets4friends.com/profile-1654969
https://participa.aytojaen.es/profiles/klivebid/activity
https://linkmix.co/56955169
https://klivebid.amebaownd.com/pages/9873237/page_202607080825
https://janitorai.com/profiles/2c73fdd9-d63d-4926-856b-b2bd099876cb_profile-of-klivebid
https://muckrack.com/klive-bid/bio
http://linoit.com/users/klivebid/canvases/klivebid
https://www.myconcertarchive.com/en/user_home?id=137082
https://buymusicclub.vercel.app/user/klivebid
https://forum.freero.org/space-uid-26860.html
http://genina.com/user/profile/5454529.page
https://wikifab.org/wiki/Utilisateur:Klivebid
https://pad.lescommuns.org/s/RycBL3Bwd
https://rant.li/klivebid/klive-la-trang-xem-bong-da-truc-tuyen-danh-cho-nguoi-ham-mo-muon-theo-doi-cac
https://chanylib.ru/ru/forum/user/35051/
https://skrolli.fi/keskustelu/users/jermelshanley977/
https://www.thehockeypaper.co.uk/forums/users/klivebid
https://www.11plus.co.uk/users/JermelShanley977/
https://opaseke.com/users/17092
https://www.newgenstravel.com/forum/topic/67668/nha-cai-klive
https://zbrushcentral.jp/user/klivebid/
https://forum.rexygen.com/user/klivebid
https://www.mapleprimes.com/users/klivebid
https://noti.st/klivebid
https://www.adpost.com/u/jermelshanley977/
https://scrapbox.io/klivebid/nha_cai_klive
https://circle-book.com/circles/73774
https://qiita.com/klivebid
https://www.annuncigratuititalia.it/author/klivebid/
https://lite.link/klivebid
http://www.brenkoweb.com/user/100652/profile
https://hedgedoc.faimaison.net/s/gm0WrMceJH
https://www.rossoneriblog.com/author/klivebid/
https://www.scamadviser.com/check-website/klive.bid
https://video.fc2.com/account/87434275
https://adplist.org/members/jermelshanley977gmailcom-mrbhffxe
https://novel.daysneo.com/author/klivebid/
https://anunt-imob.ro/user/profile/866838
https://destaquebrasil.com/saopaulo/author/klivebid/
https://www.adsfare.com/klivebid
https://makerworld.com/en/@klivebid
https://bhmtsff.com/space-uid-99050.html
https://blog.sighpceducation.acm.org/wp/forums/users/klivebid/
https://congdongmassage.com/members/klivebid.161854/#about
https://www.tacter.com/@klivebid
https://vc.ru/id6035543
https://l2top.co/forum/members/klivebid.204464/
https://artist.link/klivebid
https://dreevoo.com/profile_info.php?pid=2022697
https://www.passes.com/klivebid
https://backloggery.com/klivebid
https://que.u.nosv.org/profile?user=klivebid
http://palangshim.com/space-uid-5332098.html
https://etextpad.com/iqcodazlmv
https://app.talkshoe.com/user/klivebid
https://m.wibki.com/klivebid
https://pinshape.com/users/9004484-klivebid?tab=designs
https://sfx.thelazy.net/users/u/klivebid/
https://www.skypixel.com/users/djiuser-i9zddus6hmgm
https://klivebid.notepin.co/
https://pictureinbottle.com/r/klivebid
https://forum.epicbrowser.com/profile.php?id=168897
https://hedgedoc.eclair.ec-lyon.fr/s/_pxIOC7RM
https://www.socialbookmarkssite.com/bookmark/6282580/nh-c-i-klive/
https://www.hogwartsishere.com/profile/1853836/
https://makeagif.com/user/klivebid?ref=omYXFU
https://www.plotterusati.it/user/nha-cai-klive
https://linqto.me/about/klivebid
https://www.managementpedia.com/members/klivebid.1126379/#about
https://partecipa.poliste.com/profiles/klivebid/activity
https://hedgedoc.stusta.de/s/RCYp0q_wb
https://pad.codefor.fr/s/_P6uhDK164
https://pad.fablab-siegen.de/s/4EhO2qSVjc
https://hedgedoc.dezentrale.space/s/F3NcCflhC
https://pad.darmstadt.social/s/Kk3uU-IJFT
https://referrallist.com/profile/nha-cai-klive/
https://md.chaosdorf.de/s/hpUnjRCu73
https://smallseo.tools/website-checker/klive.bid/
https://telegra.ph/klivebid-07-08
https://runtrip.jp/users/809322
https://www.bonback.com/forum/topic/518528/nha-cai-klive
https://www.pathumratjotun.com/forum/topic/220518/nha-cai-klive
https://www.iglinks.io/JermelShanley977-ovi
https://www.bidhub.com/profiles/show/23937
https://www.dokkan-battle.fr/forums/users/klivebid/
https://homepage.ninja/klivebid
https://boss.why3s.cc/boss/home.php?mod=space&uid=288679
https://www.gabitos.com/catalunyauniversal/template.php?nm=1783484735
https://www.foriio.com/klivebid
https://maiotaku.com/p/klivebid/info
https://md.rappet.xyz/s/U2_PaIoaBH
https://md.sebastians.dev/s/ChVeUHZVE
https://controlc.com/zgrxjh9m
https://justpaste.it/u/klivebid
https://www.pozible.com/profile/nha-cai-klive
https://www.elephantjournal.com/profile/jermelshanley977/
https://forum.allkpop.com/suite/user/323098-klivebid/#about
https://strikefans.com/forum/users/klivebid/
https://swat-portal.com/forum/wcf/user/56866-klivebid/#about
https://experiment.com/users/klivebid
https://forum-foxess.pro/community/profile/klivebid/
http://julia4tied.de/member.php?action=profile&uid=254383
https://stocktwits.com/klivebid
https://commoncause.optiontradingspeak.com/index.php/community/profile/klivebid/
https://booklog.jp/users/klivebid/profile
https://mercadodinamico.com.br/author/klivebid/
https://www.grabcaruber.com/members/klivebid/profile/
https://www.magcloud.com/user/klivebid
https://bioqoo.com/klivebid
https://turcia-tours.ru/forum/profile/klivebid/
https://bike-forum.cz/profil/u/klivebid
https://galleria.emotionflow.com/195293/profile.html
https://www.myget.org/users/klivebid
https://app.brancher.ai/user/ffvFJ7Qqew42
https://confengine.com/user/klivebid
https://mygamedb.com/profile/klivebid
https://forum.aceinna.com/user/klivebid
https://www.giveawayoftheday.com/forums/profile/1984967
https://uiverse.io/profile/klivebid_6329
https://cofacts.tw/user/klivebid
https://vcook.jp/users/107539
https://www.efunda.com/members/people/show_people.cfm?Usr=klivebid
https://pumpyoursound.com/u/user/1644376
https://illust.daysneo.com/illustrator/klivebid/
Your comment is awaiting moderation.
https://www.youtube.com/@klivebid/about
https://x.com/klivebid
https://tooter.in/klivebid
https://wakelet.com/@klivebid1655
https://safechat.com/u/nha.cai.klive
https://gravatar.com/valiantly69480d0818
https://www.blogger.com/profile/09951647480826549274
https://www.pinterest.com/klivebid/
https://shareyoursocial.com/klivebid
https://500px.com/p/klivebid
https://www.instapaper.com/p/klivebid
https://www.band.us/band/103438190/post
https://protocol.ooo/ja/users/klivebid
https://www.reddit.com/user/klivebid/
https://audiomack.com/jermelshanley977
https://hackaday.io/klivebid?saved=true
https://fyers.in/community/member/CuzPBpbXqd
https://leetcode.com/u/klivebid/
https://swag.live/en/u/klivebid
https://www.halaltrip.com/user/profile/366515/klivebid/
https://medibang.com/author/28731609/
https://www.blockdit.com/users/6a4b7f6d6b689fc53d1a7b6c
https://portfolium.com/klivebid
https://www.twitch.tv/klivebid/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:D388819C6A4B81680A495C60@AdobeID
https://profile.hatena.ne.jp/klivebid/profile
https://docs.google.com/presentation/d/1LwEZxOgcMfiT7g8uOMkUitD6_D_cgNQP2ZPUqp6o7nI/edit?usp=sharing
https://issuu.com/klivebid
https://www.behance.net/nhciklive1
https://www.reverbnation.com/klivebid
https://www.myminifactory.com/users/klivebid
https://www.investagrams.com/Profile/klivebid
https://gifyu.com/klivebid
https://www.chordie.com/forum/profile.php?id=2585789
https://www.walkscore.com/people/338479699746/klive
https://topsitenet.com/profile/klivebid/2128902/
https://akniga.org/profile/1443285-klivebid/
https://disqus.com/by/klivebid/about/
https://jobs.suncommunitynews.com/profiles/8540124-nha-cai-klive
https://www.speedrun.com/users/klivebid
https://www.fanart-central.net/user/klivebid/profile
https://www.aicrowd.com/participants/klivebid
https://www.bitchute.com/channel/zgz2Pcz2UqWd
https://pbase.com/klivebid/image/176408964
https://hub.docker.com/u/klivebid
https://www.gta5-mods.com/users/klivebid
https://heylink.me/klivebid/
https://pixabay.com/users/klivebid-56588278/
https://www.nicovideo.jp/user/144763988
https://www.jigsawplanet.com/klivebid
https://3dwarehouse.sketchup.com/by/klivebid
https://robertsspaceindustries.com/en/citizens/klivebid
https://bit.ly/m/klivebid
https://allmylinks.com/klivebid
https://www.tumblr.com/klivebid
https://sites.google.com/view/klivebid/home
https://groups.google.com/g/klivebid/c/D7MYxJyuhoM
https://klivebid.blogspot.com/2026/07/nha-cai-klive.html
https://hashnode.com/@klivebid
https://medium.com/@jermelshanley977/about
https://www.slideshare.net/jermelshanley977?tab=about
https://soundcloud.com/klivebid
https://www.rehashclothes.com/klivebid
https://klivebid.mypixieset.com/
https://web.bikemap.net/u/klivebid
https://www.xiuwushidai.com/home.php?mod=space&uid=2784926
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6714734
https://bookmeter.com/users/1743711
https://party.biz/index.php/profile/389065?tab=541
https://files.fm/klivebid/info
https://startupxplore.com/en/person/klivebid
https://www.mynbest.info/profile/jermelshanley97782981/profile
https://jasa-seo.mn.co/members/40464437
https://www.zazzle.com/mbr/238158691581456632
https://maps.arosalenzerheide.swiss/en/member/klivebid/345770399/
https://luma.com/zy6q0nzg
https://www.africangenesis-101.org/profile/jermelshanley97726597/profile
https://www.proko.com/@klivebid/activity
https://sitereport.netcraft.com/?url=https://klive.bid/
https://www.miseducationofmotherhood.com/profile/jermelshanley97721609/profile
https://www.housedumonde.com/profile/jermelshanley97772530/profile
https://m.xtutti.com/user/profile/496405
https://postr.blog/profile/klivebid
https://jobs.dfw501c.com/profiles/8542411-nha-cai-klive
https://architecture-jobs.architizer.com/profiles/8542414-nha-cai-klive
https://www.webmastersun.com/members/klivebid.172059/#about
https://klivebid.stck.me/profile
https://surli.cc/hohhad
https://joy.link/klivebid
https://connect.garmin.com/app/profile/b5b138f6-1a25-4164-ad75-604813e4c421
https://b.hatena.ne.jp/klivebid/bookmark
https://www.chichi-pui.com/users/klivebid/
https://www.mellow-fan.com/user/dmb9x6640320bfvrmqqy/about
https://unityroom.com/users/39ecqhpuktzdwyimvr84
https://routinehub.co/user/klivebid
https://pxhere.com/en/photographer-me/5065676
https://www.checkli.com/klivebid#/a/process
https://www.nintendo-master.com/profil/klivebid
https://freeimage.host/klivebid
https://motion-gallery.net/users/1010300
https://linkin.bio/klivebid/
https://biomolecula.ru/authors/162712
https://talk.plesk.com/members/klivebid.520149/#about
https://www.callupcontact.com/b/businessprofile/nh_ci_klive/10153989
https://www.growkudos.com/profile/klive_bid
https://blender.community/klivebid/
https://doselect.com/@623249ef840aed7da2dccdbce
https://matkafasi.com/user/klivebid
https://allmyfaves.com/klivebid
https://www.notebook.ai/users/1392921
https://www.abclinuxu.cz/lide/klivebid
https://muare.vn/shop/klivebid/912955
https://musikersuche.musicstore.de/profil/klivebid/
https://lookingforclan.com/user/klivebid
https://forum.dmec.vn/index.php?members/klivebid.206859/
https://igli.me/klivebid
http://delphi.larsbo.org/user/klivebid
https://www.aseeralkotb.com/en/profiles/klivebid-110411559291122544423
https://timdaily.vn/members/klivebid.141498/#about
https://app.readthedocs.org/profiles/klivebid/
https://iszene.com/user-361476.html
https://www.theyeshivaworld.com/coffeeroom/users/klivebid
https://desksnear.me/users/klivebid
https://www.itchyforum.com/en/member.php?397922-klivebid
https://www.roton.com/forums/users/jermelshanley977/
https://able2know.org/user/klivebid/
http://www.biblesupport.com/user/860330-klivebid/
https://golosknig.com/profile/klivebid/
https://wallhaven.cc/user/klivebid
https://bandori.party/user/1357201/klivebid/
https://schoolido.lu/user/klivebid/
https://awan.pro/forum/user/194543/
https://fortunetelleroracle.com/profile/klivebid
https://fabble.cc/klivebid
https://pad.geolab.space/s/B8d8G4NXN
https://pad.stuve.de/s/qpX8FdDrcf
https://www.sythe.org/members/klivebid.2070459/
https://about.me/klivebid
https://www.gaiaonline.com/profiles/klivebid/51685714/
https://wefunder.com/nhciklive
https://potofu.me/klivebid
https://transfur.com/Users/klivebid
https://xtremepape.rs/members/klivebid.691438/#about
https://github.com/klivebid
https://qna.habr.com/user/klivebid
https://website.informer.com/klive.bid/
https://lightroom.adobe.com/u/nhciklive1
https://en.islcollective.com/portfolio/12961552
https://www.xosothantai.com/members/klivebid.626268/
https://velog.io/@klivebid/about
https://violet.vn/user/show/id/15331980
https://iplogger.org/logger/DRZU5ye7Xr3k/
https://mez.ink/klivebid
https://notionpress.com/author/1549745
https://www.edna.cz/uzivatele/klivebid/
https://www.techbang.com/users/klivebid
https://leakedmodels.com/forum/members/klivebid.726680/#about
https://freeicons.io/profile/952560
https://onlinesequencer.net/members/291762
https://inkbunny.net/klivebid
https://www.japaaan.com/user/108888
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.klive
https://beatsaver.com/profile/379446
https://apptuts.bio/klivebid-274468
https://participacion.cabildofuer.es/profiles/klivebid/activity?locale=en
https://forums.maxperformanceinc.com/forums/member.php?u=255926
https://egl.circlly.com/users/klivebid
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=317333
https://acomics.ru/-klivebid
https://www.criminalelement.com/members/klivebid/profile/
https://hanson.net/users/klivebid
https://writexo.com/share/cc6ae1c0064d
https://expatguidekorea.com/profile/nha-cai-klive/
https://www.heavyironjobs.com/profiles/8543061-nha-cai-klive
https://pad.degrowth.net/s/q00RNigrj
https://forum.skullgirlsmobile.com/members/klivebid.241196/#about
https://jobs.landscapeindustrycareers.org/profiles/8543075-nha-cai-klive
https://phatwalletforums.com/user/klivebid/
https://song.link/klivebid
https://idol.st/user/196417/klivebid/
https://gockhuat.net/member.php?u=440606
https://jobs.windomnews.com/profiles/8543139-nha-cai-klive
https://hoaxbuster.com/redacteur/klivebid
https://www.givey.com/klivebid
https://zerosuicidetraining.edc.org/user/profile.php?id=588375
https://www.hobowars.com/game/linker.php?url=https://klive.bid/
https://jobs.westerncity.com/profiles/8543177-nha-cai-klive
https://www.thetriumphforum.com/members/klivebid.72579/
https://album.link/klivebid
https://dev.muvizu.com/Profile/klivebid/Latest
https://chaloke.com/forums/users/klivebid/
https://buckeyescoop.com/community/members/klivebid.69028/#about
http://forum.cncprovn.com/members/435355-klivebid
https://forum.aigato.vn/user/klivebid
https://rapidapi.com/user/jermelshanley977
https://www.skool.com/@nha-cai-klive-9321
https://learningapps.org/watch?v=p3d1uxtoa26
https://www.invelos.com/UserProfile.aspx?Alias=klivebid
https://www.video-bookmark.com/bookmark/7172187/nh%C3%A0-c%C3%A1i-klive/
https://gitlab.vuhdo.io/klivebid
https://poipiku.com/13972826/
https://www.rwaq.org/users/klivebid
https://www.fitday.com/fitness/forums/members/klivebid.html
https://www.fundable.com/klive-bid
https://www.grepmed.com/klivebid
https://classificados.acheiusa.com/profile/NGdBL2hGS2pwMisrajQweDU3OWc4eks3dENNMkdNNkFmVGtBUDhadElvdz0=
https://espritgames.com/members/51820998/
https://www.haikudeck.com/presentations/cSsQYoLfRV
https://hi-fi-forum.net/profile/1176722
https://undrtone.com/klivebid
https://marshallyin.com/members/klivebid/
https://www.atozed.com/forums/user-90146.html
https://gravesales.com/author/klivebid/
https://belgaumonline.com/profile/klivebid/
https://savelist.co/my-lists/users/klivebid
https://zzb.bz/gPpZ37
https://www.themeqx.com/forums/users/klivebid/
http://newdigital-world.com/members/klivebid.html
https://www.xen-factory.com/index.php?members/klivebid.174360/#about
https://www.blackhatprotools.info/member.php?300892-klivebid
https://activepages.com.au/profile/klivebid
https://snippet.host/hwgeph
https://tudomuaban.com/chi-tiet-rao-vat/2958474/nha-cai-klive.html
https://phijkchu.com/a/klivebid/video-channels
https://lifeinsys.com/user/klivebid
https://kaeuchi.jp/forums/users/klivebid/
https://www.claimajob.com/profiles/8545138-nha-cai-klive
https://protospielsouth.com/user/149241
https://theafricavoice.com/profile/klivebid
https://support.bitspower.com/support/user/klivebid
https://www.brownbook.net/business/55286545/klivebid
https://hackmd.okfn.de/s/rkA_fI9Qzl
https://manylink.co/@klivebid
https://anyflip.com/homepage/bqqrs#About
https://www.akaqa.com/question/q19192714057-Nh-ci-klive
https://www.threadless.com/@klivebid/activity
https://civitai.com/user/klivebid
https://hoo.be/klivebid
https://maxforlive.com/profile/user/klivebid?tab=about
https://3dtoday.ru/blogs/klivebid/nha-cai-klive
https://mathlog.info/users/zLHLnLOGOwPnCmzJ4wsHfwXjcgi1
https://my.bio/klivebid
https://fora.babinet.cz/profile.php?id=134761
https://www.shippingexplorer.net/en/user/klivebid/310237
https://connect.gt/user/klivebid/
https://www.weddingbee.com/members/klivebid/
https://kumu.io/klivebid/jermelshanley977#nha-cai-klive
https://www.sunlitcentrekenya.co.ke/author/klivebid/
https://www.rcuniverse.com/forum/members/klivebid.html
https://www.huntingnet.com/forum/members/klivebid.html
https://vimeo.com/klivebid
https://www.symbaloo.com/mix/nha-cai-klive
https://www.bricklink.com/aboutMe.asp?u=klivebid
https://www.trackyserver.com/profile/264702
https://www.zubersoft.com/mobilesheets/forum/user-149824.html
https://md.coredump.ch/s/vhcpAb4em
https://aprenderfotografia.online/usuarios/klivebid/profile/
https://hackmd.hub.yt/s/r23JKKYp-
https://sciencemission.com/profile/klivebid
https://www.wvhired.com/profiles/8546987-nha-cai-klive
https://formulamasa.com/elearning/members/klivebid/
https://backloggd.com/u/klivebid/
https://forums.alliedmods.net/member.php?u=487793
https://community.jmp.com/t5/user/viewprofilepage/user-id/105213
https://viblo.asia/u/klivebid/contact
https://www.thesims3.com/mypage/klivebid/myBlog
https://brain-market.com/u/klivebid
https://ikanakama.ink/users/344202
https://www.prosebox.net/book/118849/
https://www.fw-follow.com/forum/topic/157186/nha-cai-klive
https://www.navacool.com/forum/topic/518046/nha-cai-klive
https://www.driedsquidathome.com/forum/topic/186041/nha-cai-klive
https://www.nongkhaempolice.com/forum/topic/186694/nha-cai-klive
https://www.natthadon-sanengineering.com/forum/topic/142579/nha-cai-klive
https://www.rueanmaihom.net/forum/topic/129891/nha-cai-klive
https://www.ttlxshipping.com/forum/topic/518072/nha-cai-klive
http://worldchampmambo.com/UserProfile/tabid/42/UserID/504666/Default.aspx
http://forum.modulebazaar.com/forums/user/klivebid/
https://www.rcmx.net/userinfo.php?uid=22356
https://eilo.org/user/klivebid
https://lqdoj.edu.vn/user/klivebid
https://indiestorygeek.com/user/klivebid
https://www.bandlab.com/klivebid
https://forum.issabel.org/u/klivebid
https://kvisit.com/Q_7wC
https://www.easyhits4u.com/profile.cgi?login=klivebid&view_as=1
https://doc.anagora.org/s/JRggdYzMA
https://profile.sampo.ru/klivebid
https://www.ekdarun.com/forum/topic/186064/nha-cai-klive
https://fanclove.jp/profile/ypWDe4r6Be
https://www.d-ushop.com/forum/topic/184088/nha-cai-klive
https://lustyweb.live/members/klivebid.155382/#about
https://findaspring.org/members/klivebid/
https://ketcau.com/member/134454-klivebid
https://fengshuidirectory.com/dashboard/listings/klivebid/
https://library.zortrax.com/members/nha-cai-klive/
https://pets4friends.com/profile-1654969
https://participa.aytojaen.es/profiles/klivebid/activity
https://linkmix.co/56955169
https://klivebid.amebaownd.com/pages/9873237/page_202607080825
https://janitorai.com/profiles/2c73fdd9-d63d-4926-856b-b2bd099876cb_profile-of-klivebid
https://muckrack.com/klive-bid/bio
http://linoit.com/users/klivebid/canvases/klivebid
https://www.myconcertarchive.com/en/user_home?id=137082
https://buymusicclub.vercel.app/user/klivebid
https://forum.freero.org/space-uid-26860.html
http://genina.com/user/profile/5454529.page
https://wikifab.org/wiki/Utilisateur:Klivebid
https://pad.lescommuns.org/s/RycBL3Bwd
https://rant.li/klivebid/klive-la-trang-xem-bong-da-truc-tuyen-danh-cho-nguoi-ham-mo-muon-theo-doi-cac
https://chanylib.ru/ru/forum/user/35051/
https://skrolli.fi/keskustelu/users/jermelshanley977/
https://www.thehockeypaper.co.uk/forums/users/klivebid
https://www.11plus.co.uk/users/JermelShanley977/
https://opaseke.com/users/17092
https://www.newgenstravel.com/forum/topic/67668/nha-cai-klive
https://zbrushcentral.jp/user/klivebid/
https://forum.rexygen.com/user/klivebid
https://www.mapleprimes.com/users/klivebid
https://noti.st/klivebid
https://www.adpost.com/u/jermelshanley977/
https://scrapbox.io/klivebid/nha_cai_klive
https://circle-book.com/circles/73774
https://qiita.com/klivebid
https://www.annuncigratuititalia.it/author/klivebid/
https://lite.link/klivebid
http://www.brenkoweb.com/user/100652/profile
https://hedgedoc.faimaison.net/s/gm0WrMceJH
https://www.rossoneriblog.com/author/klivebid/
https://www.scamadviser.com/check-website/klive.bid
https://video.fc2.com/account/87434275
https://adplist.org/members/jermelshanley977gmailcom-mrbhffxe
https://novel.daysneo.com/author/klivebid/
https://anunt-imob.ro/user/profile/866838
https://destaquebrasil.com/saopaulo/author/klivebid/
https://www.adsfare.com/klivebid
https://makerworld.com/en/@klivebid
https://bhmtsff.com/space-uid-99050.html
https://blog.sighpceducation.acm.org/wp/forums/users/klivebid/
https://congdongmassage.com/members/klivebid.161854/#about
https://www.tacter.com/@klivebid
https://vc.ru/id6035543
https://l2top.co/forum/members/klivebid.204464/
https://artist.link/klivebid
https://dreevoo.com/profile_info.php?pid=2022697
https://www.passes.com/klivebid
https://backloggery.com/klivebid
https://que.u.nosv.org/profile?user=klivebid
http://palangshim.com/space-uid-5332098.html
https://etextpad.com/iqcodazlmv
https://app.talkshoe.com/user/klivebid
https://m.wibki.com/klivebid
https://pinshape.com/users/9004484-klivebid?tab=designs
https://sfx.thelazy.net/users/u/klivebid/
https://www.skypixel.com/users/djiuser-i9zddus6hmgm
https://klivebid.notepin.co/
https://pictureinbottle.com/r/klivebid
https://forum.epicbrowser.com/profile.php?id=168897
https://hedgedoc.eclair.ec-lyon.fr/s/_pxIOC7RM
https://www.socialbookmarkssite.com/bookmark/6282580/nh-c-i-klive/
https://www.hogwartsishere.com/profile/1853836/
https://makeagif.com/user/klivebid?ref=omYXFU
https://www.plotterusati.it/user/nha-cai-klive
https://linqto.me/about/klivebid
https://www.managementpedia.com/members/klivebid.1126379/#about
https://partecipa.poliste.com/profiles/klivebid/activity
https://hedgedoc.stusta.de/s/RCYp0q_wb
https://pad.codefor.fr/s/_P6uhDK164
https://pad.fablab-siegen.de/s/4EhO2qSVjc
https://hedgedoc.dezentrale.space/s/F3NcCflhC
https://pad.darmstadt.social/s/Kk3uU-IJFT
https://referrallist.com/profile/nha-cai-klive/
https://md.chaosdorf.de/s/hpUnjRCu73
https://smallseo.tools/website-checker/klive.bid/
https://telegra.ph/klivebid-07-08
https://runtrip.jp/users/809322
https://www.bonback.com/forum/topic/518528/nha-cai-klive
https://www.pathumratjotun.com/forum/topic/220518/nha-cai-klive
https://www.iglinks.io/JermelShanley977-ovi
https://www.bidhub.com/profiles/show/23937
https://www.dokkan-battle.fr/forums/users/klivebid/
https://homepage.ninja/klivebid
https://boss.why3s.cc/boss/home.php?mod=space&uid=288679
https://www.gabitos.com/catalunyauniversal/template.php?nm=1783484735
https://www.foriio.com/klivebid
https://maiotaku.com/p/klivebid/info
https://md.rappet.xyz/s/U2_PaIoaBH
https://md.sebastians.dev/s/ChVeUHZVE
https://controlc.com/zgrxjh9m
https://justpaste.it/u/klivebid
https://www.pozible.com/profile/nha-cai-klive
https://www.elephantjournal.com/profile/jermelshanley977/
https://forum.allkpop.com/suite/user/323098-klivebid/#about
https://strikefans.com/forum/users/klivebid/
https://swat-portal.com/forum/wcf/user/56866-klivebid/#about
https://experiment.com/users/klivebid
https://forum-foxess.pro/community/profile/klivebid/
http://julia4tied.de/member.php?action=profile&uid=254383
https://stocktwits.com/klivebid
https://commoncause.optiontradingspeak.com/index.php/community/profile/klivebid/
https://booklog.jp/users/klivebid/profile
https://mercadodinamico.com.br/author/klivebid/
https://www.grabcaruber.com/members/klivebid/profile/
https://www.magcloud.com/user/klivebid
https://bioqoo.com/klivebid
https://turcia-tours.ru/forum/profile/klivebid/
https://bike-forum.cz/profil/u/klivebid
https://galleria.emotionflow.com/195293/profile.html
https://www.myget.org/users/klivebid
https://app.brancher.ai/user/ffvFJ7Qqew42
https://confengine.com/user/klivebid
https://mygamedb.com/profile/klivebid
https://forum.aceinna.com/user/klivebid
https://www.giveawayoftheday.com/forums/profile/1984967
https://uiverse.io/profile/klivebid_6329
https://cofacts.tw/user/klivebid
https://vcook.jp/users/107539
https://www.efunda.com/members/people/show_people.cfm?Usr=klivebid
https://pumpyoursound.com/u/user/1644376
https://illust.daysneo.com/illustrator/klivebid/
Konten yang luar biasa! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
In the great pattern of things you secure an A just for hard work. Where you lost us was on your particulars. As as the maxim goes, the devil is in the details… And it couldn’t be more accurate here. Having said that, let me reveal to you just what exactly did do the job. The text can be pretty persuasive and that is probably why I am making an effort to opine. I do not really make it a regular habit of doing that. Second, although I can certainly notice the leaps in reason you make, I am not confident of just how you seem to unite the points which inturn produce your final result. For right now I will, no doubt yield to your point however trust in the future you link the dots better.
Konten yang sangat berguna. Saya baru saja mencari hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Thank you for sharing with us, I think this website really stands out :D.
Artikel yang luar biasa. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
Terima kasih, saya baru saja menelusuri informasi sekitar topik ini sudah lama dan milik Anda adalah yang paling hebat yang saya ketahui hingga sekarang. Tapi, bagaimana dengan inti permasalahan? Apakah Anda pasti tentang asal tersebut?
Terima kasih atas posting yang luar biasa. Saya benar-benar menyukai membaca ini dan menemukan banyak sekali informasi yang berguna. Teruskan pekerjaan yang hebat!
I saw a lot of website but I believe this one contains something special in it in it
There’s noticeably a bundle to know about this. I assume you made certain nice points in features also.
A person essentially assist to make severely posts I might state. This is the first time I frequented your website page and to this point? I surprised with the research you made to create this actual put up extraordinary. Wonderful job!
Hi my loved one! I wish to say that this post is amazing, great written and come with approximately all vital infos. I’d like to peer extra posts like this .
I was just searching for this info for a while. After 6 hours of continuous Googleing, at last I got it in your web site. I wonder what’s the lack of Google strategy that don’t rank this type of informative sites in top of the list. Usually the top web sites are full of garbage.
As soon as I noticed this website I went on reddit to share some of the love with them.
Hi there would you mind letting me know which webhost you’re using? I’ve loaded your blog in 3 completely different browsers and I must say this blog loads a lot quicker then most. Can you suggest a good internet hosting provider at a honest price? Kudos, I appreciate it!
you are actually a just right webmaster. The website loading pace is amazing. It seems that you are doing any unique trick. Furthermore, The contents are masterpiece. you have done a magnificent process in this subject!
You completed various fine points there. I did a search on the matter and found nearly all people will go along with with your blog.
Also visit my blog … http://tyamada.s1008.xrea.com/cgi-bin/blog.cgi?entryid=FibonacciTriangular-j
It’s really a cool and useful piece of info. I’m satisfied that you simply shared this useful information with us. Please stay us up to date like this. Thanks for sharing.
Thanks for every other wonderful article. Where else may just anyone get that type of info in such a perfect means of writing? I’ve a presentation subsequent week, and I’m on the look for such info.
Very interesting topic, regards for posting.
I am thankful that I observed this website, precisely the right info that I was looking for! .
Outstanding post, I believe people should learn a lot from this site its very user friendly.
Heya just wanted to give you a quick heads up and let you know a few of the images aren’t loading properly. I’m not sure why but I think its a linking issue. I’ve tried it in two different browsers and both show the same results.
Wonderful goods from you, man. I’ve consider your stuff previous to and you are just extremely fantastic. I really like what you’ve bought right here, certainly like what you are stating and the way in which wherein you are saying it. You’re making it entertaining and you continue to take care of to keep it smart. I cant wait to read much more from you. This is really a tremendous site.
Once I originally commented I clicked the -Notify me when new comments are added- checkbox and now every time a remark is added I get four emails with the same comment. Is there any way you’ll be able to take away me from that service? Thanks!
you have got an awesome blog here! would you like to make some invite posts on my weblog?
Thanks a lot for sharing this with all folks you really understand what you’re talking about! Bookmarked. Please additionally seek advice from my site =). We will have a link trade arrangement among us!
You completed several good points there. I did a search on the topic and found mainly people will consent with your blog.
I like this site because so much useful material on here :D.
Thank you for the auspicious writeup. It in fact was a amusement account it. Look advanced to far added agreeable from you! However, how could we communicate?
Ini adalah situs yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Ya menyimpan ini bukanlah penentuan yang spekulatif pos yang luar biasa! .
Hey, you used to write wonderful, but the last few posts have been kinda boring… I miss your great writings. Past few posts are just a little out of track! come on!
Thanks for all your efforts that you have put in this. very interesting info .
I have recently started a website, the info you offer on this web site has helped me tremendously. Thanks for all of your time & work.
Pretty section of content. I just stumbled upon your blog and in accession capital to assert that I acquire actually enjoyed account your blog posts. Anyway I’ll be subscribing to your feeds and even I achievement you access consistently rapidly.
Your comment is awaiting moderation.
https://www.youtube.com/@net88brandcom
https://x.com/net88brandcom
https://tooter.in/net88brandcom
https://wakelet.com/@net88brandcom
https://safechat.com/u/net88brandcom
https://gravatar.com/net88brandcom
https://www.blogger.com/profile/17592068677331420571
https://www.mymeetbook.com/net88brandcom
https://www.pinterest.com/net88brandcom/
https://shareyoursocial.com/net88brandcom
https://500px.com/p/net88brandcom
https://www.instapaper.com/p/net88brandcom
https://protocol.ooo/ja/users/net88brandcom
https://www.reddit.com/user/net88brandcom/
https://audiomack.com/net88brandcom
https://hackaday.io/net88brandcom
https://fyers.in/community/member/PtVS8SM1G8
https://leetcode.com/u/net88brandcom/
https://swag.live/en/u/net88brandcom
https://www.halaltrip.com/user/profile/362770/net88brandcom/
https://medibang.com/author/28650989/
https://www.blockdit.com/net88brandcom
https://portfolium.com/net88brandcom
https://www.twitch.tv/net88brandcom/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:0534815F6A3CD2120A495CB0@AdobeID
https://profile.hatena.ne.jp/net88brandcom/
https://docs.google.com/presentation/d/13-6XDZ94Hbumvmzk5GRi80WaI-SepQw5VGcHCbpvjJU/edit?usp=sharing
https://issuu.com/net88brandcom
https://www.behance.net/net88brandcom
https://www.reverbnation.com/artist/net88brandcom
https://www.myminifactory.com/users/net88brandcom
https://www.investagrams.com/Profile/net88brandcom
https://gifyu.com/net88brandcom
https://www.chordie.com/forum/profile.php?section=about&id=2575301
https://www.walkscore.com/people/308084743908/net88brandcom
https://topsitenet.com/profile/net88brandcom/2078071/
https://akniga.org/profile/1438772-net88brandcom/
https://disqus.com/by/net88brandcom/about/
https://jobs.suncommunitynews.com/profiles/8476059-nha-cai-net88
https://www.speedrun.com/users/net88brandcom
https://www.fanart-central.net/user/net88brandcom/profile
https://www.aicrowd.com/participants/net88brandcom
https://www.bitchute.com/channel/net88brandcom
https://pbase.com/net88brandcom/
https://hub.docker.com/u/net88brandcom
https://spiderum.com/nguoi-dung/net88brandcom
https://www.gta5-mods.com/users/net88brandcom
https://heylink.me/net88brandcom/
https://pixabay.com/users/net88brandcom-56444631/
https://www.nicovideo.jp/user/144667591
https://www.jigsawplanet.com/net88brandcom
https://3dwarehouse.sketchup.com/by/net88brandcom
https://robertsspaceindustries.com/en/citizens/net88brandcom
https://bit.ly/m/net88brandcom
https://www.tumblr.com/net88brandcom
https://scholar.google.com/citations?hl=en&view_op=list_works&gmla=ACrTK9WgMGMQT_eNAtmRlSEvRWaGy3NmvjlIZU6FKDhFQRsOTJKYSA8NJvFr11K6Ti-ebt2gZchUr3bOG8Ytjg&user=3Ym86dIAAAAJ
https://sites.google.com/view/net88brandcom/home
https://www.rehashclothes.com/net88brandcom
https://www.xiuwushidai.com/home.php?mod=space&uid=2764765
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6667840
https://bookmeter.com/users/1738878
https://files.fm/net88brandcom/info
https://www.mynbest.info/profile/net88brandcom/profile
https://jasa-seo.mn.co/members/40307860
https://www.zazzle.pt/mbr/238359667316955033
https://maps.arosalenzerheide.swiss/en/member/nha-cai-net88/344860466/
https://www.africangenesis-101.org/profile/net88brandcom/profile
https://sitereport.netcraft.com/?url=https://net88brand.com/
https://www.miseducationofmotherhood.com/profile/net88brandcom/profile
https://www.housedumonde.com/profile/net88brandcom/profile
https://t.ly/p5PeN
https://m.xtutti.com/user/profile/495112
https://postr.blog/profile/net88brandcom
https://www.webmastersun.com/members/net88brandcom.170815/#about
https://net88brandcom.stck.me
https://surl.li/zasubc
https://joy.link/net88brandcom
https://connect.garmin.com/app/profile/85af8aed-b7bf-44db-8ece-d4c3d7afb7ca
https://b.hatena.ne.jp/net88brandcom/bookmark
https://www.chichi-pui.com/users/net88brandcom/
https://www.openrec.tv/user/ibl0ket8355lnt02zzye/about
https://routinehub.co/user/net88brandcom
https://pxhere.com/en/photographer-me/5055488
https://teletype.in/@net88brandcom
https://www.checkli.com/net88brandcom#/a/process
https://www.nintendo-master.com/profil/net88brandcom
https://freeimage.host/net88brandcom
https://motion-gallery.net/users/1003870
https://linkin.bio/net88brandcom
https://biomolecula.ru/authors/159133
https://talk.plesk.com/members/netbrandcom.517210/#about
https://www.callupcontact.com/b/businessprofile/nh_ci_net88/10141120
https://www.growkudos.com/profile/nha_caj_net88
https://blender.community/net88brandcom/
https://doselect.com/@ae8051ce3fc3e2facb528c920
https://matkafasi.com/user/net88brandcom
https://allmyfaves.com/net88brandcom
https://www.notebook.ai/users/1383662
https://www.abclinuxu.cz/lide/net88brandcom
https://muare.vn/shop/net88brandcom/911577
https://musikersuche.musicstore.de/profil/net88brandcom/
https://lookingforclan.com/user/net88brandcom
https://forum.dmec.vn/index.php?members/net88brandcom.203717/
https://igli.me/net88brandcom
http://delphi.larsbo.org/user/net88brandcom
https://www.aseeralkotb.com/en/profiles/net88brandcom
https://timdaily.vn/members/net88brandcom.140531/#about
https://app.readthedocs.org/profiles/net88brandcom/
https://www.dibiz.com/freudenbergertemenujka
https://iszene.com/user-359504.html
https://www.theyeshivaworld.com/coffeeroom/users/net88brandcom
https://desksnear.me/users/net88brandcom
https://www.itchyforum.com/en/member.php?396783-net88brandcom
https://www.roton.com/forums/users/freudenbergertemenujka/
https://able2know.org/user/net88brandcom/
http://www.biblesupport.com/user/855397-net88brandcom/
https://golosknig.com/profile/net88brandcom/
https://wallhaven.cc/user/net88brandcom
https://bandori.party/user/1286246/net88brandcom/
https://schoolido.lu/user/net88brandcom/
https://awan.pro/forum/user/190212/
http://fortunetelleroracle.com/profile/net88brandcom
https://fabble.cc/net88brandcom
https://pad.geolab.space/s/foMLtwFyp
https://pad.stuve.de/s/K7SEmcP6L
https://www.sythe.org/members/net88brandcom.2066710/
https://about.me/net88brandcom
https://wefunder.com/net88brandcom
https://potofu.me/net88brandcom
https://transfur.com/Users/net88brandcom
https://github.com/net88brandcom
https://qna.habr.com/user/net88brandcom
https://website.informer.com/net88brand.com
https://lightroom.adobe.com/u/net88brandcom?
https://en.islcollective.com/portfolio/12954073
https://www.xosothantai.com/members/net88brandcom.623139/
https://velog.io/@net88brandcom/about
https://violet.vn/user/show/id/15330577
https://iplogger.com/2fExz6
https://mez.ink/net88brandcom
https://notionpress.com/author/1544396
https://www.edna.cz/uzivatele/net88brandcom/
https://digiphoto.techbang.com/users/net88brandcom
https://leakedmodels.com/forum/members/net88brandcom.724146/#about
https://freeicons.io/profile/948223
https://onlinesequencer.net/members/287535
https://inkbunny.net/net88brandcom
https://www.japaaan.com/user/107123
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.net8820
https://apptuts.bio/net88brandcom-272063
https://www.storenvy.com/net88brandcom
https://participacion.cabildofuer.es/profiles/net88brandcom/activity
https://forums.maxperformanceinc.com/forums/member.php?u=254554
https://egl.circlly.com/users/net88brandcom
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=314576
https://acomics.ru/-net88brandcom
https://www.criminalelement.com/members/net88brandcom/profile/
https://hanson.net/users/net88brandcom
https://writexo.com/share/1e468af1bbc8
https://expatguidekorea.com/profile/net88brandcom/
https://www.heavyironjobs.com/profiles/8478148-nha-cai-net88
https://pad.degrowth.net/s/4ppWUOJcu
http://fort-raevskiy.ru/community/profile/net88brandcom/
https://forum.skullgirlsmobile.com/members/net88brandcom.237641/#about
https://jobs.landscapeindustrycareers.org/profiles/8478189-nha-cai-net88
https://phatwalletforums.com/user/net88brandcom/
https://song.link/net88brandcom
https://idol.st/user/192043/net88brandcom/
https://www.bmwpower.lv/user.php?u=net88brandcom
https://gockhuat.net/member.php?u=440149
https://jobs.windomnews.com/profiles/8478191-nha-cai-net88
https://hoaxbuster.com/redacteur/net88brandcom
https://www.givey.com/net88brandcom
https://zerosuicidetraining.edc.org/user/profile.php?id=583632
https://jobs.westerncity.com/profiles/8478237-nha-cai-net88
https://www.thetriumphforum.com/members/net88brandcom.71098/
https://album.link/net88brandcom
https://dev.muvizu.com/Profile/net88brandcom/Latest
https://www.deafvideo.tv/net88brandcom
https://chaloke.com/forums/users/net88brandcom/
https://buckeyescoop.com/community/members/net88brandcom.68125/#about
http://forum.cncprovn.com/members/433660-net88brandcom
https://forum.aigato.vn/user/net88brandcom
https://rapidapi.com/user/freudenbergertemenujka
https://www.skool.com/@nha-cai-net-1805
https://learningapps.org/display?v=pmk3ceuv526
http://www.invelos.com/UserProfile.aspx?alias=net88brandcom
https://www.video-bookmark.com/bookmark/7170976/nh%C3%A0-c%C3%A1i-net88/
https://gitlab.vuhdo.io/net88brandcom
https://poipiku.com/13905414/
https://www.fundable.com/user-1334641
https://www.grepmed.com/net88brandcom
https://espritgames.com/members/51680327/
https://www.haikudeck.com/presentations/net88brandcom
https://scenarch.com/userpages/43548
https://undrtone.com/net88brandcom
https://marshallyin.com/members/net88brandcom/
https://www.atozed.com/forums/user-88010.html
https://gravesales.com/author/net88brandcom/
https://belgaumonline.com/profile/net88brandcom/
https://savelist.co/my-lists/users/net88brandcom
https://zzb.bz/5jyx04
https://www.themeqx.com/forums/users/net88brandcom/
https://forums.servethehome.com/index.php?members/net88brandcom.254500/#about
https://www.blackhatprotools.info/member.php?298681-net88brandcom
https://activepages.com.au/profile/net88brandcom
https://snippet.host/hdthva
https://tudomuaban.com/chi-tiet-rao-vat/2947821/net88brandcom.html
https://phijkchu.com/a/net88brandcom/video-channels
https://lifeinsys.com/user/net88brandcom
https://kaeuchi.jp/forums/users/net88brandcom/
https://www.claimajob.com/profiles/8478876-nha-cai-net88
https://protospielsouth.com/user/144956
https://theafricavoice.com/profile/net88brandcom
https://support.bitspower.com/support/user/net88brandcom
https://www.brownbook.net/business/55246363/net88brandcom
https://app.hellothematic.com/creator/profile/1161694
https://hackmd.okfn.de/s/S1IKKRqMzl
https://manylink.co/@net88brandcom
https://anyflip.com/homepage/kfhgu
https://www.threadless.com/@net88brandcom/activity
https://civitai.com/user/net88brandcom
https://www.spigotmc.org/members/net88brandcom.2562782/
https://hoo.be/net88brandcom
https://maxforlive.com/profile/user/net88brandcom?tab=about
https://mathlog.info/users/04YeVce3VaYQa5BSaKOLsFtc3e43
https://community.cloudera.com/t5/user/viewprofilepage/user-id/158567
https://fora.babinet.cz/profile.php?section=personal&id=133175
https://www.shippingexplorer.net/en/user/net88brandcom/306196
https://connect.gt/user/net88brandcom/
https://www.weddingbee.com/members/net88brandcom/
https://www.sunlitcentrekenya.co.ke/author/net88brandcom/
https://www.huntingnet.com/forum/members/net88brandcom.html
https://www.rcuniverse.com/forum/members/net88brandcom.html
https://vimeo.com/net88brandcom
https://www.trackyserver.com/profile/262043
https://www.zubersoft.com/mobilesheets/forum/user-147198.html
https://www.mindomo.com/mindmap/649da4cedebb43728ab0758784b99f49
https://md.coredump.ch/s/LA80q0dyj
https://aprenderfotografia.online/usuarios/net88brandcom/profile/
https://hackmd.hub.yt/s/7sqqaID3a
https://www.degreeforum.net/mybb/User-net88brandcom
https://sciencemission.com/profile/net88brandcom
https://www.wvhired.com/profiles/8483355-nha-cai-net88
https://formulamasa.com/elearning/members/net88brandcom/?v=96b62e1dce57
https://chyoa.com/user/net88brandcom
https://www.royalroad.com/profile/1009019
https://backloggd.com/u/net88brandcom/
https://forums.alliedmods.net/member.php?u=485976
https://community.jmp.com/t5/user/viewprofilepage/user-id/103999
https://viblo.asia/u/net88brandcom/contact
https://brain-market.com/u/net88brandcom
https://www.prosebox.net/book/117196/
https://www.fw-follow.com/forum/topic/150929/net88brandcom
https://www.navacool.com/forum/topic/499759/net88brandcom
https://www.driedsquidathome.com/forum/topic/179195/net88brandcom
https://www.nongkhaempolice.com/forum/topic/176388/net88brandcom
https://www.bestloveweddingstudio.com/forum/topic/108458/net88brandcom
https://www.natthadon-sanengineering.com/forum/topic/136686/net88brandcom
https://www.rueanmaihom.net/forum/topic/124516/net88brandcom
https://www.ttlxshipping.com/forum/topic/499762/net88brandcom
http://worldchampmambo.com/UserProfile/tabid/42/userId/502729/Default.aspx
http://forum.modulebazaar.com/forums/user/net88brandcom/
https://eilo.org/user/net88brandcom
https://lqdoj.edu.vn/user/net88brandcom
https://indiestorygeek.com/user/net88brandcom
https://forum.issabel.org/u/net88brandcom
https://www.easyhits4u.com/profile.cgi?login=net88brandcom
https://doc.anagora.org/s/Z95P9gCJX
https://profile.sampo.ru/net88brandcom
https://www.ekdarun.com/forum/topic/180454/net88brandcom
https://fanclove.jp/profile/8N2YQqRg2L
https://www.d-ushop.com/forum/topic/174741/net88brandcom
https://findaspring.org/members/net88brandcom/
https://ketcau.com/member/133327-net88brand
https://library.zortrax.com/members/net88brandcom/
https://pets4friends.com/profile-1646759
https://participa.aytojaen.es/profiles/net88brandcom/activity
https://linkmix.co/56452076
https://www.maanation.com/net88brandcom
https://janitorai.com/profiles/15d9084c-6a13-4b99-93e4-98f587bb1bd8_profile-of-net-88-brandcom
http://linoit.com/users/net88brandcom/canvases/net88brandcom
https://nortabs.net/user/17090/
https://www.myconcertarchive.com/en/user_home?id=136430
https://buymusicclub.vercel.app/user/net88brandcom
https://forum.freero.org/space-uid-26480.html
http://genina.com/user/editDone/5433595.page
https://wikifab.org/wiki/Utilisateur:Net88brandcom
https://pad.lescommuns.org/s/f6Zml1lgf
https://rant.li/net88brandcom/net88brandcom
https://chanylib.ru/ru/forum/user/33357/
https://producerbox.com/users/net88brandcom
https://skrolli.fi/keskustelu/users/freudenbergertemenujka/
https://www.thehockeypaper.co.uk/forums/users/net88brandcom
https://www.11plus.co.uk/users/freudenbergertemenujka/
https://opaseke.com/users/16798
https://imaginaria.ru/profile/net88brandcom/
https://nicheless.blog/author/nh-301
https://www.newgenstravel.com/forum/topic/63075/net88brandcom
https://zbrushcentral.jp/user/net88brandcom
https://www.mapleprimes.com/users/net88brandcom
https://noti.st/net88brandcom
https://www.adpost.com/u/net88brandcom/
https://scrapbox.io/net88brandcom/net88brandcom
https://forum.opnsense.org/index.php?action=profile;u=70168
https://qiita.com/net88brandcom
https://www.annuncigratuititalia.it/author/net88brandcom/
https://lite.link/net88brandcom
http://www.brenkoweb.com/user/98494/profile
https://hedgedoc.faimaison.net/s/AAokUw9LJ7
https://www.rossoneriblog.com/author/net88brandcom/
https://www.scamadviser.com/check-website/net88brand.com
https://video.fc2.com/account/44076672
https://www.mikocon.com/home.php?mod=space&uid=298864
https://novel.daysneo.com/author/net88brandcom/
https://anunt-imob.ro/user/profile/865086
https://destaquebrasil.com/saopaulo/author/net88brandcom/
https://www.adsfare.com/net88brandcom
https://makerworld.com/fr/@net88brandcom
https://bhmtsff.com/space-uid-98744.html
https://blog.sighpceducation.acm.org/wp/forums/users/net88brandcom/
https://congdongmassage.com/members/net88brandcom.159602/#about
https://www.tacter.com/@net88brandcom
https://vc.ru/id6021749
https://l2top.co/forum/members/net88brandcom.197757/
https://artist.link/net88brandcom
https://dreevoo.com/profile_info.php?pid=1958192
https://www.passes.com/net88brandcom
https://backloggery.com/net88brandcom
https://que.u.nosv.org/profile?user=net88brandcom
http://palangshim.com/space-uid-5310264.html
https://etextpad.com/qjza42lgdv
https://app.talkshoe.com/user/net88brandcom
https://m.wibki.com/net88brandcom
https://pinshape.com/users/8996477-net88brandcom?tab=designs
https://sfx.thelazy.net/users/u/net88brandcom/
https://www.skypixel.com/users/djiuser-hzkvrxoml89w
https://pictureinbottle.com/r/net88brandcom
https://forum.epicbrowser.com/profile.php?section=essentials&id=166030
https://hedgedoc.eclair.ec-lyon.fr/s/JIhtcpdqB
https://www.hogwartsishere.com/profile/1850969/
https://www.plotterusati.it/user/net88brandcom
https://linqto.me/about/net88brandcom
https://www.managementpedia.com/members/net88brandcom.1125541/#about
https://hedgedoc.stusta.de/s/bBT0uYb6I
https://pad.codefor.fr/s/Rhib1lzGzH
https://pad.fablab-siegen.de/s/zxUy1XUIl-
https://hedgedoc.dezentrale.space/s/E6EHFjR8Q
https://pad.darmstadt.social/s/Z0uUG4fF27
https://referrallist.com/profile/net88brandcom/
https://md.chaosdorf.de/s/F_WZHne0e3
https://smallseo.tools/website-checker/net88brand.com
https://telegra.ph/net88brandcom-06-26
https://www.bonback.com/forum/topic/499037/net88brandcom
https://www.pathumratjotun.com/forum/topic/212628/net88brandcom
https://www.iglinks.io/FreudenbergerTemenujka-1dc?preview=true
https://www.dokkan-battle.fr/forums/users/net88brandcom/
https://homepage.ninja/net88brandcom
https://boss.why3s.cc/boss/home.php?mod=space&uid=283586
https://www.foriio.com/net88brandcom
https://md.rappet.xyz/s/p3hxEslQED
https://md.sebastians.dev/s/rNLrmvJPF
https://controlc.com/ec6efudo
https://justpaste.it/u/net88brandcom
https://www.pozible.com/profile/net88brandcom
https://www.elephantjournal.com/profile/freudenbergertemenujka/
https://forum.allkpop.com/suite/user/320974-net88brandcom/#about
https://strikefans.com/forum/users/net88brandcom/
https://swat-portal.com/forum/wcf/user/55468-net88brandcom/#about
https://experiment.com/users/nnet88brandcom
http://julia4tied.de/member.php?action=profile&uid=252650
https://commoncause.optiontradingspeak.com/index.php/community/profile/net88brandcom/
https://booklog.jp/users/net88brandcom/profile
https://mercadodinamico.com.br/author/net88brandcom/
https://www.grabcaruber.com/members/net88brandcom/profile/
https://www.magcloud.com/user/net88brandcom
https://bioqoo.com/net88brandcom
https://galleria.emotionflow.com/193184/profile.html
https://www.myget.org/users/net88brandcom
https://app.brancher.ai/user/UH0AIZZURihY
https://mygamedb.com/profile/freudenbergertemenujka
https://forum.aceinna.com/user/net88brandcom
https://www.giveawayoftheday.com/forums/profile/1962190
https://uiverse.io/profile/net88brand_2083
https://cofacts.tw/user/net88brandcom
https://vcook.jp/users/103468
https://pumpyoursound.com/u/user/1638006
https://usdinstitute.com/forums/users/net88brandcom/
https://www.intensedebate.com/people/net88brandcomm
https://tabelog.com/rvwr/net88brandcom/prof/
https://www.tkaraoke.com/forums/profile/net88brandcom/
https://app.parler.com/net88brandcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:0534815F6A3CD2120A495CB0@AdobeID
https://gamblingtherapy.org/forum/users/net88brandcom/
https://svetelektro.com/clenovia/net88brandcom/
https://www.diigo.com/item/note/bvx7a/62d3?k=ec07109942025ec89dcc1e44c3444844
https://marshmallow-qa.com/z48d1v2vtl5mh91
https://us.enrollbusiness.com/BusinessProfile/7857249/net88brandcom
https://link4u.cc/@net88brandcom
https://its-my.link/@net88brandcom
https://truckymods.io/user/513850
https://iplogger.com/2fDAz6
https://cointr.ee/net88brandcom
https://indian-tv.cz/u/net88brandcom
https://hedgedoc.envs.net/s/xJjuVjpJX
https://www.hentai-foundry.com/user/net88brandcom/profile
https://teletype.link/net88brandcom
https://hubb.link/net88brandcom/
https://www.czporadna.cz/user/net88brandcom
https://tutorialslink.com/member/net88brandcomundefined/107373
https://expathealthseoul.com/profile/net88brandcom/
https://www.plurk.com/net88brandcom
https://malt-orden.info/userinfo.php?uid=470854
https://www.weddingvendors.com/directory/profile/44801/
https://www.abookmarking.com/story/net88-3
https://www.letsdobookmark.com/story/net88-23
https://hub.vroid.com/en/users/127280346
https://www.mateball.com/net88brandcom
https://ofuse.me/net88brandcom
https://photouploads.com/net88brandcom
https://raovat.nhadat.vn/members/net88brandcom-326566.html
https://advego.com/profile/net88brandcom/
https://bio.site/net88brandcom
https://www.vnbadminton.com/members/net88brandcom.86034/
https://www.myebook.com/user_profile.php?id=net88brandcom
https://gourmet-calendar.com/users/net88brandcom
https://shootinfo.com/ru/author/net88brandcom/?pt=ads
https://www.sunemall.com/board/board_topic/8431232/8566613.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8566621.htm
https://graph.org/net88brandcom-06-26-2
https://cars.yclas.com/user/net88brandcom
https://armchairjournal.com/forums/users/net88brandcom/edit/?updated=true
https://rmmedia.ru/members/186295/#about
https://calgarybusinesses.ca/dashboard/reviews/net88brandcom/
https://www.sciencebee.com.bd/qna/user/net88brandcom
https://www.notariosyregistradores.com/web/forums/usuario/net88brandcom/
https://www.biblicaleldership.com/forums/users/net88brandcom/
https://luvly.co/users/net88brandcom
https://spinninrecords.com/profile/net88brandcom
http://onlineboxing.net/jforum/user/profile/472725.page
https://www.aipictors.com/en/users/be049da5-3907-818e-eb00-b28ad5e011fe
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8566830.htm
https://www.tai-ji.net/board/board_topic/4160148/8566823.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8567149.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8567152.htm
https://www.uscgq.com/forum/posts.php?forum=general&id=711655
https://kheotay.com.vn/forums/users/freudenbergertemenujka
https://alfounder.com/forums/users/net88brandcom/
https://crazyservice.by/forum/user/17104/
https://rsfpost.com/forums/users/net88brandcom/
https://exceldemy.com/forum/members/net88brandcom.5864/#about
https://house.karuizawa.co.jp/forums/users/guest_net88brandcom/
https://www.ontime.co.th/forum/topic/862340/net88brandcom
https://forum.gettinglost.ca/user/net88brandcom
https://zepodcast.com/forums/users/net88brandcom/
https://www.portotheme.com/forums/users/net88brandcom/
https://brazcanchamber.org/forums/users/net88brandcom/
https://www.elitepvpers.com/forum/members/9063283-net88brandcom.html?simple=1#aboutme
https://monviet88.com/profile/net88brandcom/
https://www.frenchwomenorg.com/net88brandcom
https://oto-hui.com/members/netbrandcom.436700/about
https://www.fuelly.com/driver/net88brandcom
https://www.beamng.com/members/net88brandcom.806079/
https://www.stylevore.com/user/net88brandcom
https://alumni.mgimo.ru/page/adaptive/id397179/
https://pods.link/net88brandcom
https://mylink.page/net88brandcom
https://ctxt.io/2/AAAEep16Fg
https://www.ameba.jp/profile/general/net88brandcom/
https://onespotsocial.com/net88brandcom
https://www.scener.com/@net88brandcom
https://amaz0ns.com/forums/users/net88brandcom/
https://hostndobezi.com/net88brandcom
https://nilechronicles.com/profile/net88brandcom
https://paper.wf/net88brandcom/net88brandcom
https://aphorismsgalore.com/users/net88brandcom
https://www.renderosity.com/users/id:1873591
https://www.moshpyt.com/user/net88brandcom
https://www.racerjobs.com/profiles/8483785-nha-cai-net88
https://help.orrs.de/user/net88brandcom
https://www.instructorsnearme.com/author/net88brandcom/
https://pastelink.net/eccu4fgl
https://ferrariformula1.hu/community/profile/net88brandcom/
https://en.cofacts.tw/user/net88brandcom
https://www.pebforum.com/members/net88brandcom.257249/#about
http://koloboklinks.com/site?url=net88brandcom
https://justpaste.me/d7I4
https://jali.me/net88brandcom
https://biolinky.co/net-88-brandcom
https://freudenberger.gumroad.com/
https://allmy.bio/net88brandcom
https://user.qoo-app.com/102783702
https://whatson.plus/net88brandcom
https://www.aviacionargentina.net/user/net88brandcom
https://ac.db0.company/user/16122/net88brandcom
https://failiem.lv/net88brandcom/info
https://www.youyooz.com/profile/net88brandcom/
https://forum.hiv.plus/user/net88brandcom
https://www.youbiz.com/profile/net88brandcom/
https://affariat.com/user/profile/186557
https://theexplorers.com/user?id=3969c7ac-a6b8-4843-8651-aa70ca4af822
https://aiforkids.in/qa/user/net88brandcom+1
https://ja.cofacts.tw/user/net88brandcom
http://fr.islcollective.com/portfolio/12954073
https://es.islcollective.com/portafolio/12954073
https://www.minecraft-servers-list.org/details/net88brandcom/
https://blog.ulifestyle.com.hk/net88brandcom
https://baskadia.com/user/h29g
https://buyerseller.xyz/user/net88brandcom/
https://artelis.pl/autor/profil/241098
https://www.democracylab.org/user/50823
https://vs.cga.gg/user/245886
https://youslade.com/net88brandcom
https://www.fitlynk.com/net88brandcom
https://bsky.app/profile/net88brandcom.bsky.social
https://app.nft.nyc/wallet/6a3e97725061661e625c3089
https://www.xmonsta.com/forums/users/net88brandcom/
https://www.green-collar.com/forums/users/net88brandcom/
https://www.hostboard.com/forums/members/net88brandcom.html
https://ticketme.io/account/net88brandcom
https://infinitebacklog.net/users/net88brandcom
https://www.coh2.org/user/177719/net88brandcom
https://joy.bio/net88brandcom1
https://quangcaoso.vn/net88brandcom/gioithieu.html
https://raovatonline.org/author/net88brandcom/
I love your writing style truly enjoying this web site.
whoah this weblog is fantastic i love studying your articles. Keep up the good work! You recognize, many persons are hunting around for this information, you could aid them greatly.
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
My brother recommended I might like this blog. He was entirely right. This post actually made my day. You cann’t imagine just how much time I had spent for this information! Thanks!
I was looking at some of your articles on this site and I believe this internet site is rattling instructive! Continue putting up.
Sangat menarik poin yang Anda utarakan, salam telah memposting. “Hebatlah seni memulai, tetapi lebih hebat lagi seni mengakhiri.” oleh Henry Wadsworth Longfellow.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Postingan yang sangat baik. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
I don’t even know how I ended up here, but I thought this post was good. I do not know who you are but certainly you are going to a famous blogger if you aren’t already 😉 Cheers!
Saya terkesan dengan situs web ini, amat saya adalah penggemar.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar layak. Konten yang luar biasa dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Website ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Postingan yang sangat bagus. Saya benar-benar menikmati cara Anda menyampaikan gagasan-gagasan ini. Teruskan kerja yang hebat!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I dugg some of you post as I cogitated they were handy handy
Unquestionably believe that which you stated. Your favorite reason appeared to be on the net the easiest thing to be aware of. I say to you, I definitely get irked while people consider worries that they plainly do not know about. You managed to hit the nail upon the top and defined out the whole thing without having side-effects , people can take a signal. Will likely be back to get more. Thanks
Informasi yang berguna. Saya baru menelusuri hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
I always was concerned in this topic and stock still am, thanks for posting.
It is appropriate time to make a few plans for the long run and it’s time to be happy. I have learn this put up and if I could I desire to recommend you some fascinating things or suggestions. Perhaps you can write subsequent articles relating to this article. I desire to read more issues approximately it!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Ya menyimpan ini bukanlah kesimpulan yang buruk pos yang hebat! .
Saya selalu peduli dengan subjek ini dan tetap masih demikian, salam telah memposting.
Terima kasih untuk blog informatif tambahan. Di mana lagi saya memperoleh informasi seperti itu yang ditulis dengan gaya yang sempurna? Saya punya sebuah misi yang saya tengah kerjakan sekarang, dan saya telah mencari informasi seperti ini.
Saya biasanya tidak menulis komentar, tetapi yang satu ini benar-benar pantas. Konten yang hebat dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Ini adalah saran yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Konten yang bermanfaat dan disajikan dengan sangat baik. Saya pasti akan membagikan ini kepada teman-teman. Terima kasih telah berbagi.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Kami bisa memiliki tautan perubahan kesepakatan di antara kita!
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
You are so awesome! I don’t believe I’ve truly read something
like this before. So nice to discover someone with some genuine thoughts
on this topic. Seriously.. many thanks for starting this up.
This site is something that is required on the web, someone with
a bit of originality!
I like the helpful information you provide for your articles. I will bookmark your blog and take a look at once more right here frequently. I’m rather certain I’ll learn many new stuff right right here! Good luck for the following!
I was actively looking for a new gambling site, and betsuna absolutely blew me away. The variety of casino titles is massive, and the promos are truly player-friendly. What really caught me is the instant payout time. If you want a legit site to game, definitely check it out.
I would like to thnkx for the efforts you have put in writing this blog. I am hoping the same high-grade blog post from you in the upcoming as well. In fact your creative writing abilities has inspired me to get my own blog now. Really the blogging is spreading its wings quickly. Your write up is a good example of it.
I genuinely enjoy reading on this internet site, it holds superb blog posts. “Do what you fear, and the death of fear is certain.” by Anthony Robbins.
Pretty! This was a really wonderful post. Thank you for your provided information.
Well I truly enjoyed reading it. This information provided by you is very effective for correct planning.
Sangat bagus website yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan pendapat dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
Terima kasih atas tulisan yang baik. Faktanya ini dulunya adalah sebuah materi hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berhubungan?
Terima kasih, saya baru saja mencari informasi tentang topik ini sudah lama dan milik Anda adalah yang paling hebat yang saya jumpai sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang asal tersebut?
Menghargai dedikasi yang Anda curahkan ke website Anda dan informasi mendalam yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Kerja yang sangat baik!
Some genuinely wonderful info , Sword lily I detected this.
I too conceive therefore, perfectly written post! .
Saya mengunjungi banyak website tetapi saya anggap yang satu ini mengandung sesuatu yang ekstra di dalamnya
Seseorang secara esensial menolong untuk membuat secara kritis posting saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun publikasi istimewa ini. Kerja yang hebat!
Saya umumnya tidak menulis komentar, tetapi yang satu ini benar-benar layak. Isi yang hebat dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Spot on with this write-up, I truly assume this web site needs far more consideration. I’ll in all probability be once more to read way more, thanks for that info.
Saya secara terus melihat online untuk tips yang dapat memfasilitasi saya. Terima kasih!
Some truly marvelous work on behalf of the owner of this website , absolutely outstanding subject matter.
Saya selamanya memikirkan hal ini, terimakasih telah memposting.
Seiring dengan semua hal yang tampak sedang berkembang di dalam topik spesifik ini, sebagian besar pandangan Anda cenderung sangat menstimulasi. Di sisi lain, saya memohon maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh ide Anda, meskipun menggairahkan. Terlihat bagi semua orang bahwa ulasan Anda tidak sepenuhnya benar-benar rasional dan pada faktanya Anda sendiri tidak benar-benar sepenuhnya pasti terhadap argumen tersebut. Dalam hal apa pun saya menghargai membacanya.
Terima kasih untuk artikel fantastis tambahan. Di mana lagi siapa pun mungkin bisa mendapatkan tipe info seperti itu dengan metode penulisan yang ideal? Saya memiliki presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Menghargai usaha yang Anda curahkan ke situs Anda dan informasi mendalam yang Anda tawarkan. Sangat bagus menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Konten yang berguna. Saya baru mencari hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Halo semua, kamu sudah melakukan kerja yang fantastis. Saya tentu akan mem-bookmark ini dan kembali untuk melihat lebih banyak. Terima kasih!
Kami mungkin memiliki hyperlink pertukaran kesepakatan di antara kita!
Meski begitu, terima kasih untuk artikel yang luar biasa ini dan walaupun saya tidak setuju sepenuhnya, saya menghormati perspektif.
An impressive share, I just given this onto a colleague who was doing a little analysis on this. And he in fact bought me breakfast because I found it for him.. smile. So let me reword that: Thnx for the treat! But yeah Thnkx for spending the time to discuss this, I feel strongly about it and love reading more on this topic. If possible, as you become expertise, would you mind updating your blog with more details? It is highly helpful for me. Big thumb up for this blog post!
Excellent post but I was wanting to know if you could write a litte more on this subject? I’d be very grateful if you could elaborate a little bit further. Kudos!
I conceive other website owners should take this web site as an model, very clean and great user friendly design.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Hei, saya sekadar ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini merupakan tepat tipe informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
I always was interested in this subject and still am, appreciate it for putting up.
I have been absent for a while, but now I remember why I used to love this blog. Thanks, I will try and check back more often. How frequently you update your website?
Wow! Ini bisa jadi salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Fantastis. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami kerja keras Anda.
Kemarin, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu baik. Bye
Artikel yang luar biasa. Ini memberikan saya pemahaman yang lebih jelas tentang subjek ini. Teruskan kerja yang luar biasa!
I think that is among the most vital info for me. And i am glad studying your article. However should remark on few common things, The web site taste is wonderful, the articles is truly great :D. Excellent job, cheers
Saya biasanya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang sangat baik dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Postingan yang sangat baik. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Sangat bersih situs, hargai untuk pos ini.
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Terima kasih banyak atas posting yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak sekali informasi yang bermanfaat. Teruskan kerja yang bagus!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya sangat bersyukur menemukan situs ini di Bing, persis seperti yang saya telusuri : D juga sudah saya simpan di bookmark saya.
Saya selamanya memikirkan hal ini, sangat dihargai telah memposting.
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang sangat baik dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Thanks for sharing superb informations. Your site is so cool. I’m impressed by the details that you’ve on this blog. It reveals how nicely you perceive this subject. Bookmarked this web page, will come back for extra articles. You, my pal, ROCK! I found simply the info I already searched all over the place and just could not come across. What an ideal website.
Good info. Lucky me I reach on your website by accident, I bookmarked it.
Hey! This is kind of off topic but I need some advice from an established blog. Is it very difficult to set up your own blog? I’m not very techincal but I can figure things out pretty quick. I’m thinking about setting up my own but I’m not sure where to start. Do you have any points or suggestions? Many thanks
Great post. I am facing a couple of these problems.
You have brought up a very superb details, regards for the post.
You really make it seem so easy with your presentation but I find this topic to be really something which I think I would never understand. It seems too complex and very broad for me. I am looking forward for your next post, I will try to get the hang of it!
Some truly interesting info , well written and generally user friendly.
I am really enjoying the theme/design of your blog. Do you ever run into any internet browser compatibility problems? A couple of my blog audience have complained about my website not operating correctly in Explorer but looks great in Safari. Do you have any recommendations to help fix this issue?
Saya selamanya memikirkan hal ini, sangat dihargai telah mengunggah.
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah detail kontak Anda?
Luar biasa! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
Nearly all of what you claim happens to be supprisingly appropriate and that makes me ponder the reason why I hadn’t looked at this with this light before. This piece really did switch the light on for me personally as far as this subject matter goes. However at this time there is actually one factor I am not too comfortable with and whilst I attempt to reconcile that with the actual main theme of your issue, permit me observe just what the rest of the visitors have to point out.Very well done.
Saya terkesan dengan situs ini, amat saya adalah penggemar.
Konten yang bermanfaat dan ditulis dengan sangat baik. Saya tentu akan membagikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Hore google adalah raja saya yang membantu saya menemukan situs internet yang luar biasa! .
After examine a number of of the blog posts in your web site now, and I actually like your means of blogging. I bookmarked it to my bookmark web site checklist and will be checking again soon. Pls check out my website as effectively and let me know what you think.
I’d have to examine with you here. Which isn’t one thing I normally do! I enjoy studying a submit that can make folks think. Also, thanks for allowing me to remark!
I love your blog.. very nice colors & theme. Did you create this website yourself? Plz reply back as I’m looking to create my own blog and would like to know wheere u got this from. thanks
Thanks so much for giving everyone an extremely pleasant chance to read from this web site. It is always so pleasurable and as well , jam-packed with a great time for me and my office peers to search your blog really 3 times in 7 days to learn the newest secrets you have. And of course, I am at all times motivated concerning the unique opinions you give. Some 2 ideas in this post are certainly the finest we have all ever had.
Thank you a bunch for sharing this with all people you actually recognize what you’re talking about! Bookmarked. Kindly additionally visit my web site =). We can have a link exchange agreement among us!
Respect to article author, some fantastic information .
I’ve read some good stuff here. Certainly worth bookmarking for revisiting. I surprise how much effort you put to make such a magnificent informative web site.
I like what you guys are up also. Such clever work and reporting! Keep up the superb works guys I’ve incorporated you guys to my blogroll. I think it will improve the value of my site 🙂
Once I initially commented I clicked the -Notify me when new comments are added- checkbox and now every time a comment is added I get four emails with the same comment. Is there any way you possibly can take away me from that service? Thanks!
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
Terima kasih banyak atas posting yang hebat. Saya benar-benar menikmati membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan kerja yang hebat!
Menikmati menelaah ini, sangat bagus, terima kasih.
Mengagumi waktu dan tenaga yang Anda curahkan ke website Anda dan informasi terperinci yang Anda berikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Saya senang menjadi pengunjung dari web blog sempurna ini!, terimakasih atas informasi langka ini!
I’ve been surfing online more than three hours today, yet I never found any interesting article like yours. It’s pretty worth enough for me. Personally, if all website owners and bloggers made good content as you did, the net will be a lot more useful than ever before.
Postingan yang fantastis. Saya sungguh menikmati gaya Anda menyampaikan ide-ide ini. Teruskan pekerjaan yang hebat!
Ini adalah tips yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Menghargai dedikasi yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda tawarkan. Sangat baik menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Sangat menarik poin yang Anda catat, sangat menghargai telah mengunggah. “Saya telah membuat beberapa kesalahan yang ingin saya ulangi.” oleh Jerry Coleman.
Your comment is awaiting moderation.
https://www.youtube.com/@dn88pokercom
https://x.com/dn88pokercom
https://tooter.in/dn88pokercom
https://wakelet.com/@dn88pokercom
https://safechat.com/u/dn88pokercom
https://gravatar.com/dn88pokercom
https://www.blogger.com/profile/09676506695966520507
https://www.mymeetbook.com/dn88pokercom
https://www.pinterest.com/dn88pokercom/
https://shareyoursocial.com/dn88pokercom
https://myspace.com/dn88pokercom
https://500px.com/p/dn88pokercom
https://www.instapaper.com/p/dn88pokercom
https://protocol.ooo/ja/users/dn88pokercom
https://audiomack.com/dn88pokercom
https://hackaday.io/dn88pokercom
https://fyers.in/community/member/A5ZndKdEAH
https://leetcode.com/u/dn88pokercom/
https://swag.live/en/u/dn88pokercom
https://www.halaltrip.com/user/profile/365923/dn88pokercom/
https://medibang.com/author/28719623/
https://www.blockdit.com/dn88pokercom
https://portfolium.com/dn88pokercom
https://www.twitch.tv/dn88pokercom/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:9B3981A96A48FBEE0A495FD6@AdobeID
https://profile.hatena.ne.jp/dn88pokercom/profile
https://issuu.com/dn88pokercom
https://www.behance.net/dn88pokercom
https://www.reverbnation.com/artist/dn88pokercom
https://www.myminifactory.com/users/dn88pokercom
https://www.investagrams.com/Profile/dn88pokercom
https://gifyu.com/dn88pokercom
https://www.chordie.com/forum/profile.php?id=2584177
https://www.walkscore.com/people/544485812983/dn88pokercom
https://akniga.org/profile/1442678-dn88pokercom/
https://jobs.suncommunitynews.com/profiles/8530996-nha-cai-dn88
https://www.speedrun.com/users/dn88pokercom
https://www.fanart-central.net/user/dn88pokercom/profile
https://www.aicrowd.com/participants/dn88pokercom
https://www.bitchute.com/channel/IlbOJCA6hJOX
https://pbase.com/dn88pokercom
https://hub.docker.com/u/dn88pokercom
https://www.gta5-mods.com/users/dn88pokercom
https://heylink.me/dn88pokercom/
https://www.nicovideo.jp/user/144748260
https://www.jigsawplanet.com/dn88pokercom
https://3dwarehouse.sketchup.com/by/dn88pokercom
https://robertsspaceindustries.com/en/citizens/dn88pokercom
https://bit.ly/m/dn88pokercom
https://allmylinks.com/dn88pokercom
https://sites.google.com/view/dn88pokercom/home
https://groups.google.com/g/dn88pokercom/c/Nna6zzMWKDg
https://hashnode.com/@dn88pokercom
https://medium.com/@dn88pokercom/about
https://soundcloud.com/dn88pokercom
https://www.rehashclothes.com/dn88pokercom
https://www.xiuwushidai.com/home.php?mod=space&uid=2782147
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6709609
https://bookmeter.com/users/1742917
https://startupxplore.com/en/person/dn88pokercom
https://www.mynbest.info/profile/dn88pokercom/profile
https://jasa-seo.mn.co/members/40443819
https://www.zazzle.pt/mbr/238124038588608576
https://www.africangenesis-101.org/profile/dn88pokercom/profile
https://www.miseducationofmotherhood.com/profile/dn88pokercom/profile
https://www.housedumonde.com/profile/dn88pokercom/profile
https://m.xtutti.com/user/profile/496168
https://postr.blog/profile/dn88pokercom
https://www.webmastersun.com/members/dn88pokercom.171858/#about
https://dn88pokercom.stck.me/
https://joy.link/dn88pokercom
https://connect.garmin.com/app/profile/2fe77dfb-7a6c-468b-873e-2513e054ae22
https://www.chichi-pui.com/users/dn88pokercom/
https://www.openrec.tv/user/dn88pokercom/about
https://routinehub.co/user/dn88pokercom
https://pxhere.com/en/photographer-me/5063698
https://teletype.in/@dn88pokercom
https://www.checkli.com/dn88pokercom
https://www.nintendo-master.com/profil/dn88pokercom
https://freeimage.host/dn88pokercom
https://motion-gallery.net/users/1009472
https://linkin.bio/dn88pokercom/
https://biomolecula.ru/authors/162290
https://www.callupcontact.com/b/businessprofile/dn88pokercom/10152535
https://www.growkudos.com/profile/nh%C3%A0_c%C3%A1i_dn88_3
https://blender.community/dn88pokercom/
https://doselect.com/@ecb08c04489d62def5da515b5
https://matkafasi.com/user/dn88pokercom
https://allmyfaves.com/dn88pokercom
https://www.notebook.ai/users/1391900
https://www.abclinuxu.cz/lide/dn88pokercom
https://muare.vn/shop/dn88pokercom/912776
https://musikersuche.musicstore.de/profil/dn88pokercom/
https://lookingforclan.com/user/dn88pokercom
https://forum.dmec.vn/index.php?members/dn88pokercom.206440/
https://igli.me/dn88pokercom
http://delphi.larsbo.org/user/dn88pokercom
https://www.aseeralkotb.com/en/profiles/dn88pokercom
https://timdaily.vn/members/dn88pokercom.141355/#about
https://app.readthedocs.org/profiles/dn88pokercom/
https://www.dibiz.com/rinarubi206
https://iszene.com/user-361193.html
https://www.theyeshivaworld.com/coffeeroom/users/dn88pokercom
https://desksnear.me/users/dn88pokercom
https://www.itchyforum.com/en/member.php?397772-dn88pokercom
https://www.roton.com/forums/users/rinarubi206/
https://able2know.org/user/dn88pokercom/
http://www.biblesupport.com/user/859624-dn88pokercom/
https://golosknig.com/profile/dn88pokercom/
https://wallhaven.cc/user/dn88pokercom
https://bandori.party/user/1348119/dn88pokercom/
https://schoolido.lu/user/dn88pokercom/
https://awan.pro/forum/user/194016/
https://fortunetelleroracle.com/profile/dn88pokercom
https://fabble.cc/dn88pokercom
https://pad.geolab.space/s/nMHF4SgMB
https://pad.stuve.de/s/bwqrxkANgM
https://www.sythe.org/members/dn88pokercom.2069915/
https://about.me/dn88pokercom
https://wefunder.com/dn88pokercom
https://transfur.com/Users/dn88pokercom
https://xtremepape.rs/members/dn88pokercom.690921/#about
https://github.com/dn88pokercom
https://qna.habr.com/user/dn88pokercom
https://lightroom.adobe.com/u/dn88pokercom
https://en.islcollective.com/portfolio/12960367
https://www.xosothantai.com/members/dn88pokercom.625780/
https://velog.io/@dn88pokercom/about
https://mez.ink/dn88pokercom
https://notionpress.com/author/1549054
https://digiphoto.techbang.com/users/dn88pokercom
https://leakedmodels.com/forum/members/dn88pokercom.726346/#about
https://onlinesequencer.net/members/291318
https://inkbunny.net/dn88pokercom
https://www.japaaan.com/user/108618
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.dn8811
https://beatsaver.com/playlists/1229555
https://apptuts.bio/dn88pokercom
https://www.storenvy.com/dn88pokercom
https://participacion.cabildofuer.es/profiles/dn88pokercom/activity?locale=en
https://forums.maxperformanceinc.com/forums/member.php?u=255714
https://egl.circlly.com/users/dn88pokercom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=316956
https://acomics.ru/-dn88pokercom
https://hanson.net/users/dn88pokercom
https://writexo.com/share/d5bab3961ef3
https://expatguidekorea.com/profile/dn88pokercom/
https://www.heavyironjobs.com/profiles/8533994-nha-cai-dn88
https://pad.degrowth.net/s/bob_OKu8D
https://forum.skullgirlsmobile.com/members/dn88pokercom.240696/#about
https://jobs.landscapeindustrycareers.org/profiles/8534009-nha-cai-dn88
https://phatwalletforums.com/user/dn88pokercom
https://song.link/dn88pokercom
https://idol.st/user/195820/dn88pokercom/
https://jobs.windomnews.com/profiles/8534052-nha-cai-dn88
https://hoaxbuster.com/redacteur/dn88pokercom
https://www.givey.com/dn88pokercom
https://zerosuicidetraining.edc.org/user/profile.php?id=587715
https://jobs.westerncity.com/profiles/8534078-nha-cai-dn88
https://www.thetriumphforum.com/members/dn88pokercom.72365/
https://album.link/dn88pokercom
https://dev.muvizu.com/Profile/dn88pokercom/Latest
https://chaloke.com/forums/users/dn88pokercom/
https://buckeyescoop.com/community/members/dn88pokercom.68891/#about
http://forum.cncprovn.com/members/435109-dn88pokercom
https://forum.aigato.vn/user/dn88pokercom
https://rapidapi.com/user/dn88pokercom
https://www.skool.com/@nha-cai-dn-6169
https://learningapps.org/watch?v=p8j4n5mga26
https://www.invelos.com/UserProfile.aspx?Alias=dn88pokercom
https://gitlab.vuhdo.io/dn88pokercom
https://poipiku.com/13964278/
https://www.rwaq.org/users/dn88pokercom
https://www.fundable.com/nha-cai-dn88-10
https://www.grepmed.com/dn88pokercom
https://classificados.acheiusa.com/profile/OWRicHdsRFhRYTVoT004dmp0TGlVUmNsWUxqSkZhRTNMcVdZdGJuRTBhbz0=
https://espritgames.com/members/51803518/
https://www.haikudeck.com/presentations/dn88pokercom
https://hi-fi-forum.net/profile/1175522
https://scenarch.com/userpages/45961
https://undrtone.com/dn88pokercom
https://marshallyin.com/members/dn88pokercom/
https://www.atozed.com/forums/user-89788.html
https://gravesales.com/author/dn88pokercom/
https://belgaumonline.com/profile/dn88pokercom/
https://savelist.co/my-lists/users/dn88pokercom
https://www.themeqx.com/forums/users/dn88pokercom/
http://newdigital-world.com/members/dn88pokercom.html
https://www.xen-factory.com/index.php?members/dn88pokercom.173952/#about
https://forums.servethehome.com/index.php?members/dn88pokercom.257264/#about
https://www.blackhatprotools.info/member.php?300542-dn88pokercom
https://activepages.com.au/profile/dn88pokercom
https://snippet.host/ppkaoc
https://tudomuaban.com/chi-tiet-rao-vat/2956675/dn88pokercom.html
https://phijkchu.com/a/dn88pokercom/video-channels
https://lifeinsys.com/user/dn88pokercom
https://kaeuchi.jp/forums/users/dn88pokercom/
https://www.claimajob.com/profiles/8534289-nha-cai-dn88
https://protospielsouth.com/user/147792
https://theafricavoice.com/profile/dn88pokercom
https://support.bitspower.com/support/user/dn88pokercom
https://www.brownbook.net/business/55272658/dn88pokercom
https://hackmd.okfn.de/s/SJQqsWO7Me
https://manylink.co/@dn88pokercom
https://anyflip.com/homepage/yagrj#About
https://www.akaqa.com/question/q19192713555-Dn88pokercom
https://www.threadless.com/@dn88pokercom/activity
https://civitai.com/user/dn88pokercom
https://www.spigotmc.org/members/dn88pokercom.2568488/
https://hoo.be/dn88pokercom
https://maxforlive.com/profile/user/dn88pokercom?tab=about
https://mathlog.info/users/01uKpqts4iNz9B8LmOrBOrIlRhm1
https://my.bio/dn88pokercom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/160127
https://www.slmath.org/people/119951
https://fora.babinet.cz/profile.php?section=personal&id=134452
https://www.shippingexplorer.net/en/user/dn88pokercom/309371
https://connect.gt/user/dn88pokercom
https://www.weddingbee.com/members/dn88pokercom/
https://www.rcuniverse.com/forum/members/dn88pokercom.html
https://www.huntingnet.com/forum/members/dn88pokercom.html
https://www.trackyserver.com/profile/264216
https://www.zubersoft.com/mobilesheets/forum/user-149350.html
https://www.mindomo.com/mindmap/f302d05d103e4e36aabb5100bf56adfa
https://md.coredump.ch/s/Io0xJEr5c
https://aprenderfotografia.online/usuarios/dn88pokercom/profile/
https://hackmd.hub.yt/s/YuHjucBdA
https://sciencemission.com/profile/dn88pokercom
https://www.wvhired.com/profiles/8534521-nha-cai-dn88
https://formulamasa.com/elearning/members/dn88pokercom/?v=96b62e1dce57
https://chyoa.com/user/dn88pokercom
https://www.royalroad.com/profile/1016217
https://backloggd.com/u/dn88pokercom/
https://forums.alliedmods.net/member.php?u=487445
https://community.jmp.com/t5/user/viewprofilepage/user-id/104976
https://viblo.asia/u/dn88pokercom/contact
https://www.thesims3.com/myBlog.html?persona=dn88pokercom&showBlogMasterPopup=false
https://hype4.academy/profile/dn88pokercom
https://brain-market.com/u/dn88pokercom
https://www.prosebox.net/book/118521/
https://www.fw-follow.com/forum/topic/156119/dn88pokercom
https://www.navacool.com/forum/topic/514556/dn88pokercom
https://www.driedsquidathome.com/forum/topic/184795/dn88pokercom
https://www.nongkhaempolice.com/forum/topic/184766/dn88pokercom
https://www.bestloveweddingstudio.com/forum/topic/112657/dn88pokercom
https://www.natthadon-sanengineering.com/forum/topic/141483/dn88pokercom
https://www.rueanmaihom.net/forum/topic/128870/dn88pokercom
https://www.ttlxshipping.com/forum/topic/514557/dn88pokercom
http://worldchampmambo.com/UserProfile/tabid/42/userId/504261/Default.aspx
http://forum.modulebazaar.com/forums/user/dn88pokercom/
https://eilo.org/user/dn88pokercom
https://lqdoj.edu.vn/user/dn88pokercom
https://indiestorygeek.com/user/dn88pokercom
https://www.bandlab.com/dn88pokercom
https://forum.issabel.org/u/dn88pokercom
https://www.keepandshare.com/discuss2/48989/dn88
https://www.easyhits4u.com/profile.cgi?login=dn88pokercom
https://doc.anagora.org/s/H8yjKi99J
https://profile.sampo.ru/dn88pokercom
https://www.ekdarun.com/forum/topic/185001/dn88pokercom
https://fanclove.jp/profile/z0JR4eEXBp
https://www.d-ushop.com/forum/topic/182135/dn88pokercom
https://findaspring.org/members/dn88pokercom/
https://fengshuidirectory.com/dashboard/listings/dn88pokercom/
https://library.zortrax.com/members/dn88pokercom/
https://pets4friends.com/profile-1652578
https://participa.aytojaen.es/profiles/dn88pokercom/activity
https://linkmix.co/56858873
https://dn88pokercom.amebaownd.com/
https://janitorai.com/profiles/70024561-a7a6-40ad-a85d-19267853124b_profile-of-dn-88-pokercom
https://muckrack.com/nha-cai-dn88-4/bio
http://linoit.com/users/dn88pokercom/canvases/dn88pokercom
https://nortabs.net/user/17359/
https://www.myconcertarchive.com/en/user_home?id=136902
https://forum.jatekok.hu/User-dn88pokercom
https://www.buymusic.club/user/dn88pokercom
https://forum.freero.org/space-uid-26784.html
http://genina.com/user/edit/5448974.page
https://wikifab.org/wiki/Utilisateur:Dn88pokercom
https://pad.lescommuns.org/s/-jNCujL1Q
https://rant.li/dn88pokercom/dn88
https://chanylib.ru/ru/forum/user/34694/
https://skrolli.fi/keskustelu/users/rinarubi206/
https://www.thehockeypaper.co.uk/forums/users/dn88pokercom
https://www.11plus.co.uk/users/rinarubi206/
https://imaginaria.ru/profile/dn88pokercom/
https://www.newgenstravel.com/forum/topic/66803/dn88pokercom
https://zbrushcentral.jp/user/dn88pokercom
https://www.mapleprimes.com/users/dn88pokercom
https://noti.st/dn88pokercom
https://www.adpost.com/u/dn88pokercom/
https://guitarmaking.co.uk/members/dn88pokercom/
https://scrapbox.io/dn88pokercom/DN88
https://circle-book.com/circles/73603
https://forum.opnsense.org/index.php?action=profile;u=70496
https://qiita.com/dn88pokercom
https://www.annuncigratuititalia.it/author/dn88pokercom/
https://lite.link/dn88pokercom
http://www.brenkoweb.com/user/100191/profile
https://hedgedoc.faimaison.net/s/-V3_BNJYVq
https://www.rossoneriblog.com/author/dn88pokercom/
https://video.fc2.com/account/88699015
https://adplist.org/members/rinarubi206gmailcom-mr8eww3a
https://novel.daysneo.com/author/dn88pokercom/
https://anunt-imob.ro/user/profile/866470
https://destaquebrasil.com/saopaulo/author/dn88pokercom/
https://www.adsfare.com/dn88pokercom
https://makerworld.com/fr/@dn88pokercom
https://bhmtsff.com/space-uid-98996.html
https://blog.sighpceducation.acm.org/wp/forums/users/dn88pokercom/
https://congdongmassage.com/members/dn88pokercom.161414/#about
https://www.tacter.com/@dn88pokercom
https://vc.ru/id6032840
https://l2top.co/forum/members/dn88pokercom.203179/
https://artist.link/dn88pokercom
https://dreevoo.com/profile.php?pid=2010036
https://www.passes.com/dn88pokercom
https://backloggery.com/dn88pokercom
https://que.u.nosv.org/profile?user=dn88pokercom
http://palangshim.com/space-uid-5329457.html
https://etextpad.com/yplyrsley8
https://app.talkshoe.com/user/dn88pokercom
https://m.wibki.com/dn88pokercom
https://pinshape.com/users/9002381-rinarubi206?tab=designs
https://sfx.thelazy.net/users/u/dn88pokercom/
https://www.skypixel.com/users/djiuser-weu2mf3feew2
https://pictureinbottle.com/r/dn88pokercom
https://forum.epicbrowser.com/profile.php?id=168379
https://hedgedoc.eclair.ec-lyon.fr/s/GThVWvVqzm
https://www.hogwartsishere.com/profile/1853228/
https://www.plotterusati.it/user/dn88pokercom
https://linqto.me/about/dn88pokercom
https://www.managementpedia.com/members/dn88pokercom.1126228/#about
https://partecipa.poliste.com/profiles/dn88pokercom/activity
https://hedgedoc.stusta.de/s/IXc76OO8R
https://pad.codefor.fr/s/UfU-3Uk4Qd
https://pad.fablab-siegen.de/s/6kjb3D0Diy
https://hedgedoc.dezentrale.space/s/WQLJ3gADM
https://pad.darmstadt.social/s/hIbYP8Sqti
https://referrallist.com/profile/dn88pokercom/
https://md.chaosdorf.de/s/PTwwxWJyFs
https://telegra.ph/dn88pokercom-07-05
https://runtrip.jp/users/808310
https://www.bonback.com/forum/topic/514580/dn88pokercom
https://www.pathumratjotun.com/forum/topic/219486/dn88pokercom
https://www.iglinks.io/rinarubi206-toz?preview=true
https://www.dokkan-battle.fr/forums/users/dn88pokercom/
https://homepage.ninja/dn88pokercom
https://boss.why3s.cc/boss/home.php?mod=space&uid=287708
https://www.foriio.com/dn88pokercom
https://maiotaku.com/p/dn88pokercom/info
https://md.rappet.xyz/s/wKzidOY5Pf
https://md.sebastians.dev/s/0q2pICUaI
https://justpaste.it/u/dn88pokercom
https://www.pozible.com/profile/dn88pokercom
https://www.elephantjournal.com/profile/dn88pokercom/
https://forum.allkpop.com/suite/user/322652-dn88pokercom/#about
https://strikefans.com/forum/users/dn88pokercom/
https://swat-portal.com/forum/wcf/user/56570-dn88pokercom/#about
https://experiment.com/users/dn88pokercom
http://julia4tied.de/member.php?action=profile&uid=254127
https://commoncause.optiontradingspeak.com/index.php/community/profile/dn88pokercom/
https://mercadodinamico.com.br/author/dn88pokercom/
https://bioqoo.com/dn88pokercom
https://turcia-tours.ru/forum/profile/dn88pokercom/
https://bike-forum.cz/profil/u/dn88pokercom
https://galleria.emotionflow.com/194849/
https://www.myget.org/users/dn88pokercom
https://app.brancher.ai/user/2Z5HbV6-LcLj
https://confengine.com/user/dn88pokercom
https://mygamedb.com/profile/dn88pokercom
https://forum.aceinna.com/user/dn88pokercom
https://www.giveawayoftheday.com/forums/profile/1980793
https://uiverse.io/profile/nhci_9593
https://cofacts.tw/user/dn88pokercom
https://vcook.jp/users/105690
https://www.efunda.com/members/people/show_people.cfm?Usr=dn88pokercom
https://pumpyoursound.com/u/user/1641355
https://congdongx.com/thanh-vien/dn88pokercom.56114/#about
https://www.intensedebate.com/people/dn88pokercom1
https://tabelog.com/rvwr/dn88pokercom/prof/
https://www.tkaraoke.com/forums/profile/rinarubi206gmail-com/
https://app.parler.com/dn88pokercom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:C93C81976A4B3D6D0A495CC8@AdobeID
https://gitlab.com/dn88pokercom
https://gamblingtherapy.org/forum/users/dn88pokercom/
https://svetelektro.com/clenovia/dn88pokercom/
https://www.diigo.com/profile/dn88pokercom
https://marshmallow-qa.com/uc7xbc8n1lidmd7
https://us.enrollbusiness.com/BusinessProfile/7868372/dn88pokercom
https://link4u.cc/@dn88pokercom
https://its-my.link/@dn88pokercom
https://truckymods.io/user/518634
https://www.iniuria.us/forum/member.php?697573-dn88pokercom
https://cointr.ee/dn88pokercom
https://indian-tv.cz/u/dn88pokercom
https://hedgedoc.envs.net/s/DIZSPdeub
https://illust.daysneo.com/illustrator/dn88pokercom/
https://aniworld.to/user/profil/dn88pokercom
https://www.hentai-foundry.com/user/dn88pokercom/profile
https://teletype.link/dn88pokercom
https://hubb.link/dn88pokercom/
https://official.link/dn88pokercom
https://www.czporadna.cz/user/dn88pokercom
https://tealfeed.com/dn88pokercom
https://expathealthseoul.com/profile/dn88pokercom/
https://commu.nosv.org/p/dn88pokercom
https://www.weddingvendors.com/directory/profile/45497/
https://www.abookmarking.com/story/dn88-8
https://www.letsdobookmark.com/story/dn88-12
https://hub.vroid.com/en/users/127541166
https://www.mateball.com/dn88pokercom
https://ofuse.me/my/posts/386212
https://photouploads.com/dn88pokercom
https://raovat.nhadat.vn/members/dn88pokercom-329216.html
https://advego.com/profile/dn88pokercom/
https://bio.site/dn88pokercom
https://www.vnbadminton.com/members/dn88pokercom.87710/
https://www.myebook.com/user_profile.php?id=dn88pokercom
https://gourmet-calendar.com/users/dn88pokercom
https://www.sunemall.com/board/board_topic/8431232/8614535.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8614541.htm
https://graph.org/dn88pokercom-07-06
https://boards.rossmanngroup.com/members/dn88pokercom.95707/
https://naijamatta.com/dn88pokercom
https://rmmedia.ru/members/186663/#about
https://calgarybusinesses.ca/dashboard/reviews/dn88pokercom/
https://www.sciencebee.com.bd/qna/user/dn88pokercom
https://luvly.co/users/dn88pokercom
https://spinninrecords.com/profile/dn88pokercom
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8614569.htm
https://www.tai-ji.net/board/board_topic/4160148/8614576.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8614578.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8614580.htm
https://kheotay.com.vn/forums/users/rinarubi206
https://crazyservice.by/forum/user/17486/
https://rsfpost.com/forums/users/dn88pokercom/
https://exceldemy.com/forum/members/dn88pokercom.6104/#about
https://house.karuizawa.co.jp/forums/users/guest_nhacaidn88/
https://www.ontime.co.th/forum/topic/867466/dn88pokercom
https://zepodcast.com/forums/users/dn88pokercom/
https://www.elitepvpers.com/forum/members/9066825-dn88pokercom.html
https://monviet88.com/profile/dn88pokercom/
https://www.frenchwomenorg.com/dn88pokercom
https://www.beamng.com/members/dn88pokercom.808874/
https://www.physicsoverflow.org/user/dn88pokercom
https://pods.link/dn88pokercom
https://mylink.page/dn88pokercom
https://trakteer.id/dn88pokercom
https://ctxt.io/2/AAAE6jp5Ew
https://onespotsocial.com/dn88pokercom
https://www.scener.com/@dn88pokercom
https://amaz0ns.com/forums/users/dn88pokercom/
https://hostndobezi.com/dn88pokercom
https://nilechronicles.com/profile/dn88pokercom
https://paper.wf/dn88pokercom/dn88pokercom
https://devfolio.co/@dn88pokercom/readme-md
https://wibki.com/dn88pokercom
https://aphorismsgalore.com/users/dn88pokercom
https://comicvine.gamespot.com/profile/dn88pokercom/
https://www.renderosity.com/users/id:1876749
https://eo-college.org/members/dn88pokercom/
https://www.moshpyt.com/user/dn88pokercom
https://www.racerjobs.com/profiles/8537996-nha-cai-dn88
https://www.instructorsnearme.com/author/dn88pokercom/
https://en.cofacts.tw/user/dn88pokercom
https://www.pebforum.com/members/dn88pokercom.259739/#about
http://koloboklinks.com/site?url=dn88poker.com
https://www.doorkeeper.jp/users/dn88pokercom?locale=en
http://freestyler.ws/user/674053/dn88pokercom
https://jali.me/dn88pokercom
https://pastebin.com/u/dn88pokercom
https://www.swap-bot.com/user:dn88pokercom
https://whatson.plus/dn88pokercom
https://www.aviacionargentina.net/user/dn88pokercom
https://ac.db0.company/user/17425/dn88pokercom/
https://forum.hiv.plus/user/dn88pokercom
https://theexplorers.com/user?id=73a02a09-4f40-4fd8-9ffb-0fa0caec1632
https://www.thitrungruangclinic.com/forum/topic/185416/dn88pokercom
https://ja.cofacts.tw/user/dn88pokercom
https://www.minecraft-servers-list.org/details/dn88pokercom/
https://buyerseller.xyz/user/dn88pokercom/
https://www.democracylab.org/user/52230
https://vs.cga.gg/user/246736
https://youslade.com/dn88pokercom
https://www.fitlynk.com/dn88pokercom
https://www.vevioz.com/dn88pokercom
https://www.xmonsta.com/forums/users/dn88pokercom/
https://www.green-collar.com/forums/users/dn88pokercom/
https://quangcaoso.vn/dn88pokercom/gioithieu.html
https://vasep.vn/members/dn88pokercom.5878/#about
https://sighpceducation.hosting.acm.org/wp/forums/users/dn88pokercom/
https://raovatonline.org/author/dn88pokercom/
https://topkif.nvinio.com/dn88pokercom
https://gitflic.ru/user/dn88pokercom
https://www.themirch.com/blog/author/dn88pokercom/
https://mail.protospielsouth.com/user/147792
https://www.euskalmarket.com/author/dn88pokercom/
https://doingbusiness.eu/profile/dn88pokercom/
https://umczdt.ru/forum/?PAGE_NAME=profile_view&UID=160442
https://ic-info.ru/forum/user/226741/
https://stardust.run/user/176679/dn88pokercom/
/
https://md.darmstadt.ccc.de/s/_e17VfX4Mg
https://forum.reallusion.com/Users/3292013/dn88pokercom
https://webanketa.com/forms/6mw3edhq6cqpas1j6grk0rb4/
https://www.pdc.edu/?URL=https://dn88poker.com/
https://ask.mallaky.com/?qa=user/dn88pokercom
https://www.depechemode.cz/?URL=https://dn88poker.com/
https://userstyles.world/user/dn88pokercom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=16242
https://pledgeme.co.nz/profiles/349727
https://forum.herozerogame.com/index.php?/user/174566-dn88pokercom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2569200
https://hedgedoc.logilab.fr/s/dWF94VbJp
https://entre-vos-mains.alsace.eu/profiles/dn88pokercom/activity
https://zealy.io/cw/dn88pokercom/questboard/
https://www.france-ioi.org/user/perso.php?sLogin=dn88pokercom
https://ixawiki.com/link.php?url=https://dn88poker.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=151388
https://forum.ct8.pl/member.php?action=profile&uid=130380
https://www.okaywan.com/home.php?mod=space&uid=825152
http://tkdlab.com/wiki/index.php?dn88pokercom
https://volleypedia.org/index.php?qa=user&qa_1=dn88pokercom
http://pcsq28.com/home.php?mod=space&uid=2288235
https://bbs.airav.cc/home.php?mod=space&uid=4767036
https://pad.funkwhale.audio/s/zpah6_60E
https://pad.flipdot.org/s/eRuIWWCLU7
https://md.opensourceecology.de/s/gnQLEITJGw
https://md.chaospott.de/s/Qbi4OfkGuZ
https://doc.adminforge.de/s/7uCY8V63fp
https://wikimapia.org/external_link?url=https://dn88poker.com/
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://dn88poker.com/
https://playlist.link/dn88pokercom
https://odesli.co/dn88pokercom
Wow! Ini bisa jadi salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Hebat. Saya juga seorang ahli dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Sangat menarik info !Sempurna persis seperti yang saya cari!
good post.Ne’er knew this, thankyou for letting me know.
Postingan yang hebat. Ini memberi saya gambaran yang lebih baik tentang subjek ini. Teruskan kerja yang luar biasa!
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada pendekatan Anda dapat menghapus saya dari layanan itu? Terima kasih!
Postingan yang sangat bagus. Ini memberi saya gambaran yang lebih baik tentang subjek ini. Teruskan kerja yang luar biasa!
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Saya terkesan dengan website ini, sangat saya adalah penggemar.
you’re in reality a just right webmaster. The web site loading speed is amazing. It sort of feels that you are doing any distinctive trick. In addition, The contents are masterpiece. you have performed a wonderful job in this topic!
I’m not sure where you’re getting your information, but good topic. I needs to spend some time learning more or understanding more. Thanks for wonderful info I was looking for this info for my mission.
It’s hard to find knowledgeable people on this topic, but you sound like you know what you’re talking about! Thanks
I like this weblog so much, saved to bookmarks. “To hold a pen is to be at war.” by Francois Marie Arouet Voltaire.
Awsome post and straight to the point. I am not sure if this is truly the best place to ask but do you people have any thoughts on where to hire some professional writers? Thanks 🙂
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
Your style is really unique compared to other folks I have
read stuff from. Thank you for posting when you’ve got the
opportunity, Guess I’ll just bookmark this web site.
I have been absent for a while, but now I remember why I used to love this web site. Thanks, I’ll try and check back more often. How frequently you update your web site?
I like what you guys are up also. Such smart work and reporting! Carry on the superb works guys I’ve incorporated you guys to my blogroll. I think it will improve the value of my web site 🙂
It’s really a nice and useful piece of info. I’m happy that you just shared this useful information with us. Please keep us up to date like this. Thanks for sharing.
Appreciate it for this post, I am a big fan of this site would like to go on updated.
You actually make it appear really easy together with your presentation however I to find this topic to be actually something which I think I might by no means understand. It sort of feels too complicated and extremely extensive for me. I’m taking a look forward to your subsequent publish, I’ll try to get the grasp of it!
Respect to post author, some fantastic information .
I like this post, enjoyed this one appreciate it for putting up.
Hey just wanted to give you a quick heads up. The words in your post seem to be running off the screen in Chrome. I’m not sure if this is a formatting issue or something to do with browser compatibility but I figured I’d post to let you know. The style and design look great though! Hope you get the problem resolved soon. Cheers
I’ve been exploring for a little bit for any high-quality articles or weblog posts in this sort of area . Exploring in Yahoo I eventually stumbled upon this site. Reading this information So i’m glad to express that I’ve a very just right uncanny feeling I found out exactly what I needed. I most for sure will make certain to don’t put out of your mind this site and give it a glance regularly.
Very nice post. I just stumbled upon your blog and wished to say that I’ve really enjoyed browsing your blog posts. After all I will be subscribing to your feed and I hope you write again soon!
Hello there, You’ve done a great job. I will certainly digg it and personally recommend to my friends. I am confident they will be benefited from this website.
I like your writing style genuinely loving this internet site.
Saya tidak biasanya berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang satu ini : D.
Konten yang bermanfaat. Saya baru saja menelusuri hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Saya mendapatkan info yang bagus dari blog Anda.
Rattling nice style and wonderful subject material, hardly anything else we want :D.
Hey! I know this is kinda off topic however , I’d figured I’d ask. Would you be interested in exchanging links or maybe guest writing a blog article or vice-versa? My blog addresses a lot of the same topics as yours and I think we could greatly benefit from each other. If you’re interested feel free to send me an e-mail. I look forward to hearing from you! Wonderful blog by the way!
Anda dapat jelas melihat antusiasme Anda di dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Halo di sana, hanya ingin mengatakan bahwa saya benar-benar menyukai membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa banyak wawasan yang sangat berguna. Terima kasih!
Wohh tepat apa yang saya telusuri, salam atas posting.
I have learn several just right stuff here. Certainly price bookmarking for revisiting. I wonder how much effort you put to create such a wonderful informative site.
I genuinely enjoy reading on this website , it contains superb blog posts.
Kemarin, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi tiga puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini merupakan persis tipe informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada rekan-rekan. Terima kasih banyak telah berbagi.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Hore google adalah ratu saya yang membantu saya menemukan website yang luar biasa! .
Saya tidak bisa menahan diri untuk berkomentar
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Luar biasa. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami usaha Anda.
Keep functioning ,remarkable job!
Seseorang pada dasarnya membantu membuat artikel yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Kerja yang sangat baik!
Ya menyimpan ini bukanlah keputusan yang berisiko pos yang luar biasa! .
I have recently started a website, the information you provide on this site has helped me greatly. Thanks for all of your time & work. “The achievements of an organization are the results of the combined effort of each individual.” by Vince Lombardi.
Terima kasih atas tulisan yang baik. Sebenarnya ini dulunya adalah sebuah konten hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita dapat menjaga kontak?
I really enjoy studying on this web site, it holds superb posts.
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali evaluasi tentang ini. Dan dia pada kenyataannya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika dapat dicapai, seiring Anda menjadi lebih ahli, apakah Anda keberatan memperbarui weblog Anda dengan lebih banyak rincian? Ini sangat berguna bagi saya. Jempol besar untuk posting weblog ini!
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang hebat!
Saya secara berkelanjutan melihat online untuk ide yang dapat menolong saya. Thx!
Konten yang berguna. Saya baru saja menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
I’m no longer positive where you’re getting your info, but great topic. I needs to spend a while learning more or understanding more. Thank you for magnificent information I was on the lookout for this information for my mission.
Artikel yang hebat. Saya sungguh menikmati cara Anda menyampaikan gagasan-gagasan ini. Teruskan kerja yang luar biasa!
Anda bisa jelas melihat keahlian Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
In this grand design of things you secure a B+ with regard to effort. Where you misplaced me was on all the details. As people say, the devil is in the details… And it could not be much more accurate right here. Having said that, let me tell you what exactly did give good results. The writing is highly convincing and that is most likely the reason why I am making the effort to opine. I do not really make it a regular habit of doing that. Second, whilst I can certainly notice the leaps in logic you make, I am not really convinced of just how you appear to unite the details which help to make your final result. For the moment I will, no doubt yield to your point however hope in the near future you link the facts better.
I’m really impressed with your writing skills as well as with the layout on your blog. Is this a paid theme or did you modify it yourself? Anyway keep up the nice quality writing, it’s rare to see a nice blog like this one these days..
Hai semua, saya menemukan blog Anda lewat Google ketika mencari subjek yang mirip, website Anda tampil di bagian atas. Saya harus mengakui bahwa saya terkejut seberapa bagus pengaturannya. Saya sangat menyukai membaca ini dan saya akan kembali untuk melihat lebih banyak. Terima kasih banyak!
I got good info from your blog
Hiya, I’m really glad I have found this information. Nowadays bloggers publish just about gossips and web and this is actually annoying. A good web site with interesting content, that’s what I need. Thank you for keeping this web-site, I will be visiting it. Do you do newsletters? Can not find it.
I have to point out my passion for your generosity giving support to those people that require help on this particular issue. Your special dedication to passing the message up and down had been definitely beneficial and have all the time enabled guys like me to reach their desired goals. Your new helpful guidelines can mean much a person like me and extremely more to my peers. With thanks; from all of us.
It’s the best time to make a few plans for the longer term and it is time to be happy. I have read this post and if I may I want to recommend you some interesting issues or advice. Perhaps you can write next articles referring to this article. I want to read more issues approximately it!
I’m impressed, I must say. Actually hardly ever do I encounter a blog that’s both educative and entertaining, and let me let you know, you may have hit the nail on the head. Your idea is excellent; the difficulty is one thing that not enough individuals are speaking intelligently about. I am very comfortable that I stumbled throughout this in my seek for one thing relating to this.
Berharga informasi. Untungnya saya menemukan website Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
I am pleased that I discovered this blog, precisely the right information that I was looking for! .
Piece of writing writing is also a fun, if you know
afterward you can write if not it is complex to write.
Feel free to visit my page … Veterans Widows Benefits
Good site! I truly love how it is simple on my eyes and the data are well written. I am wondering how I might be notified when a new post has been made. I’ve subscribed to your RSS feed which must do the trick! Have a great day!
Hi there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
Amat indah informasi dapat ditemukan di situs.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Artikel ini sangat berguna. Saya sangat menghargai waktu yang Anda curahkan untuk menulisnya. Terima kasih!
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Sangat menarik info !Sempurna persis seperti yang saya cari!
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Hore google adalah ratu saya yang membantu saya menemukan web site yang luar biasa! .
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
I really like your writing style, good info , thanks for putting up :D.
Great post. I am facing a couple of these problems.
Hai di sana, kamu sudah melakukan pekerjaan yang luar biasa. Saya tentu akan menandai ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Pekerjaan yang sangat baik!
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Enjoyed looking through this, very good stuff, thanks.
I think other site proprietors should take this site as an model, very clean and magnificent user genial style and design, let alone the content. You are an expert in this topic!
Saya mengunjungi banyak website tetapi saya percaya yang satu ini memiliki sesuatu yang spesial di dalamnya
Mengagumi dedikasi yang Anda curahkan ke website Anda dan informasi mendalam yang Anda berikan. Sangat luar biasa menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
What i do not realize is in fact how you’re now not really a lot more well-liked than you may be now. You are so intelligent. You realize thus considerably in the case of this subject, produced me for my part imagine it from numerous numerous angles. Its like women and men aren’t fascinated unless it’s one thing to accomplish with Lady gaga! Your own stuffs excellent. All the time care for it up!
I have been exploring for a bit for any high quality articles or weblog posts on this kind of space . Exploring in Yahoo I ultimately stumbled upon this website. Reading this info So i am glad to express that I have a very excellent uncanny feeling I found out just what I needed. I so much for sure will make certain to don’t put out of your mind this site and give it a look regularly.
Postingan yang luar biasa. Ini benar-benar ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
I am extremely impressed with your writing skills and also with the layout on your blog. Is this a paid theme or did you modify it yourself? Either way keep up the excellent quality writing, it’s rare to see a great blog like this one today..
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca dalam waktu yang lama. Informasi yang sangat berguna. Terima kasih telah berbagi.
I have been exploring for a bit for any high-quality articles or blog posts on this kind of area . Exploring in Yahoo I at last stumbled upon this website. Reading this info So i’m happy to convey that I have an incredibly good uncanny feeling I discovered just what I needed. I most certainly will make certain to do not forget this web site and give it a look on a constant basis.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Informasi yang bermanfaat. Saya baru menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
I am incessantly thought about this, regards for posting.
Thank you, I have just been searching for information approximately this topic for a long time and yours is the best I have discovered till now. But, what concerning the conclusion? Are you positive in regards to the source?
Thanks for the auspicious writeup. It in fact used to be a leisure account it. Glance advanced to far delivered agreeable from you! By the way, how could we keep up a correspondence?
I don’t even know how I ended up right here, but I assumed this publish used to be good. I don’t know who you are but definitely you’re going to a well-known blogger when you aren’t already 😉 Cheers!
Hey very nice website!! Man .. Excellent .. Amazing .. I’ll bookmark your site and take the feeds also…I am happy to find numerous useful information here in the post, we need develop more techniques in this regard, thanks for sharing. . . . . .
An interesting discussion is worth comment. I think that you should write more on this topic, it might not be a taboo subject but generally people are not enough to speak on such topics. To the next. Cheers
It’s actually a great and useful piece of information. I’m glad that you simply shared this helpful information with us. Please stay us up to date like this. Thanks for sharing.
Attractive section of content. I just stumbled upon your web site and in accession capital to assert that I get actually enjoyed account your blog posts. Anyway I will be subscribing to your augment and even I achievement you access consistently rapidly.
Halo, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah persis tipe informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
ข้อมูลชุดนี้ อ่านแล้วได้ความรู้เพิ่ม ครับ
ผม ไปอ่านเพิ่มเติมเกี่ยวกับ หัวข้อที่คล้ายกัน
สามารถอ่านได้ที่ ทางเข้า betflix285
สำหรับใครกำลังหาเนื้อหาแบบนี้
มีการยกตัวอย่างที่เข้าใจง่าย
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
จะรอติดตามเนื้อหาใหม่ๆ ต่อไป
Thanks for sharing excellent informations. Your site is very cool. I’m impressed by the details that you’ve on this web site. It reveals how nicely you perceive this subject. Bookmarked this web page, will come back for extra articles. You, my friend, ROCK! I found just the info I already searched all over the place and just couldn’t come across. What a great web-site.
Menikmati menelaah ini, sangat bagus, sangat menghargai.
Aku sungguh ingin menulis komentar singkat untuk mengucapkan terima kasih Anda atas seluruh saran luar biasa yang Anda tuliskan di website ini.
Wow! Terima kasih! Saya selalu ingin menulis di website saya sesuatu seperti itu. Bolehkah saya mengambil bagian dari posting Anda ke blog saya?
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan yang unggul!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Ya menyimpan ini bukanlah keputusan yang spekulatif pos yang hebat! .
Benar-benar luar biasa informasi dapat ditemukan di weblog.
Saya secara berkelanjutan mencari online untuk posting yang dapat menolong saya. Terima kasih!
Saya secara terus menjelajah online untuk artikel yang dapat membantu saya. Thx!
Good info. Lucky me I reach on your website by accident, I bookmarked it.
Terima kasih atas tulisan yang baik. Faktanya ini sebelumnya adalah sebuah materi hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat menjaga kontak?
Hai semua, hanya ingin mengatakan bahwa saya sangat menyukai membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak wawasan yang sangat berguna. Terima kasih!
My brother recommended I might like this website. He was entirely right. This post actually made my day. You cann’t imagine simply how much time I had spent for this info! Thanks!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Umumnya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup artikel yang bagus.
Aku benar-benar ingin mengirim pesan singkat untuk menghargai Anda atas seluruh informasi luar biasa yang Anda bagikan di situs ini.
Kami akan memiliki hyperlink alternatif kesepakatan antara kita!
Hey There. I found your blog using msn. This is a really well written article. I’ll make sure to bookmark it and come back to read more of your useful information. Thanks for the post. I’ll certainly return.
Sangat menarik poin yang Anda sebutkan, thankyou telah mengunggah.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Wow, fantastic blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your site is magnificent, let alone the content!
Everything is very open and very clear explanation of issues. was truly information. Your website is very useful. Thanks for sharing.
Hey very nice site!! Man .. Excellent .. Wonderful ..
I’ll bookmark your web site and take the feeds also?
I’m glad to search outt numerous useful information here in the post, we’d like
develop moore techniques onn this regard, thanks
for sharing. . . . . .
Ini adalah blog yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar hebat!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di mana detail kontak Anda?
Isi yang luar biasa! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
I just could not depart your web site prior to suggesting that I really enjoyed the usual information an individual supply on your visitors? Is going to be back incessantly to investigate cross-check new posts.
Saya tidak biasanya berkomentar tetapi saya harus mengakui hargai untuk posting yang luar biasa ini : D.
I would like to show my thanks to the writer for rescuing me from this type of matter. As a result of browsing through the the web and getting suggestions which were not pleasant, I figured my entire life was done. Being alive minus the answers to the issues you have fixed by means of your entire post is a critical case, and ones that would have in a wrong way affected my entire career if I had not come across your web site. Your actual competence and kindness in handling everything was valuable. I am not sure what I would’ve done if I hadn’t encountered such a thing like this. I’m able to now look forward to my future. Thanks for your time so much for your specialized and result oriented guide. I will not think twice to recommend the sites to any individual who needs to have guidance on this topic.
I really appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again
Postingan yang hebat. Ini memberikan saya pemahaman yang lebih baik tentang topik ini. Teruskan kerja yang luar biasa!
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan yang sangat bagus!
Saya secara tidak sengaja menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang bagus.
Saya mengunjungi banyak website tetapi saya percaya yang satu ini mengandung sesuatu yang ekstra di dalamnya
Saya mendapatkan info yang bagus dari blog Anda.
I’ve recently started a blog, the info you offer on this site has helped me greatly. Thank you for all of your time & work.
Hebat website yang Anda miliki, tapi saya ingin tahu apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin sekali menjadi bagian dari kelompok di mana saya bisa mendapatkan umpan balik dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Cheers!
Hei semua, saya menemukan blog Anda melalui Google ketika menelusuri topik yang sebanding, website Anda muncul di posisi atas. Saya harus mengatakan bahwa saya kagum betapa rapi penulisannya. Saya benar-benar menikmati membaca ini dan saya pasti akan kembali untuk melihat lebih banyak. Terima kasih!
Hi my loved one! I wish to say that this article is amazing, nice written and come with approximately all significant infos. I’d like to peer more posts like this .
Hei semua, hanya ingin mengatakan bahwa saya benar-benar menyukai membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan banyak informasi yang sangat berguna. Terima kasih!
I have recently started a site, the information you offer on this site has helped me tremendously. Thanks for all of your time & work.
Isi yang luar biasa! Gaya penulisan Anda jelas dan mudah dipahami. Saya tentu akan kembali untuk membaca konten lainnya.
I am not rattling great with English but I come up this rattling easygoing to read .
I’m no longer positive the place you’re getting your information, however good topic. I needs to spend some time finding out much more or figuring out more. Thanks for great info I used to be looking for this info for my mission.
Anda bisa jelas melihat keahlian Anda di dalam karya yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu kejar hati Anda.
Hore google adalah penguasa dunia saya yang membantu saya menemukan situs yang luar biasa! .
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Anda telah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan bersyukur kepada Anda.
Interesting discussion, looking forward to reading more replies.
Thanks for starting this discussion, definitely an interesting read.
Nice forum discussion, some really useful insights
being shared here.
Really good thread, I appreciate all the information being shared.
Good topic for discussion, I enjoyed reading through the replies.
my webpage; reddit.com/r/microgrowery HLVD infection confirmed: Mass-Hydro – 81 strains tested positive
Interesting discussion, looking forward to reading more replies.
Thanks for starting this discussion, definitely an interesting read.
Nice forum discussion, some really useful insights
being shared here.
Really good thread, I appreciate all the information being shared.
Good topic for discussion, I enjoyed reading through the replies.
my webpage; reddit.com/r/microgrowery HLVD infection confirmed: Mass-Hydro – 81 strains tested positive
Artikel yang hebat. Ini memberi saya pemahaman yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
Umumnya saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup artikel yang bagus.
Saya mendapatkan info yang bagus dari blog Anda.
Sangat menarik detail yang Anda amati, terima kasih telah memposting.
Saya terkesan dengan website ini, amat saya adalah penggemar berat.
Konten yang luar biasa! Gaya penulisan Anda jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca konten lainnya.
Ini adalah saran yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Postingan yang luar biasa. Ini memberikan saya gambaran yang lebih jelas tentang subjek ini. Teruskan kerja yang hebat!
Saya senang menjadi pengunjung dari website sempurna ini!, terimakasih atas info langka ini!
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi empat puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna desain yang hebat!
I have been absent for a while, but now I remember why I used to love this web site. Thank you, I’ll try and check back more frequently. How frequently you update your website?
I am sure this article has touched all the internet viewers, its really really good paragraph on building up new web site.
F*ckin’ awesome issues here. I’m very happy to peer your article. Thank you a lot and i’m looking ahead to touch you. Will you please drop me a mail?
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada jalan Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada sarana Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
mative. I’m bookmarking this to refer to later. Looking forward to more content like this. Nordic IPTV One
Usually I don’t read article on blogs, however I wish to say that this write-up very pressured me to try and do so! Your writing taste has been surprised me. Thanks, very nice post.
It’s hard to find knowledgeable people on this topic, but you sound like you know what you’re talking about! Thanks
Wohh persis apa yang saya cari, salam atas posting.
Regards for helping out, good info .
Very interesting subject, regards for putting up.
Hi, i think that i saw you visited my web site so i came to “return the favor”.I am trying
to find things to enhance my website!I suppose its ok to use a few of your ideas!!
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada pendekatan Anda dapat menghapus saya dari layanan itu? Terima kasih!
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me. Anyways, I’m definitely happy I found it and I’ll be book-marking and checking back frequently!
Hey! I could have sworn I’ve been to this blog before but after reading through some of the post I realized it’s new to me. Anyways, I’m definitely delighted I found it and I’ll be bookmarking and checking back often!
Hmm it appears like your website ate my first comment (it was extremely long) so I guess I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your blog. I as well am an aspiring blog writer but I’m still new to the whole thing. Do you have any points for beginner blog writers? I’d really appreciate it.
Terima kasih atas tulisan yang bagus. Faktanya ini sebelumnya adalah sebuah materi hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Terima kasih untuk artikel luar biasa yang lain. Di tempat mana lagi siapa pun bisa mendapatkan tipe informasi seperti itu dengan pendekatan penulisan yang sempurna? Saya memiliki presentasi minggu berikutnya, dan saya berada dalam pencarian informasi seperti ini.
Yay google is my world beater helped me to find this great website ! .
Terrific work! This is the type of info that should be shared around the net. Shame on Google for not positioning this post higher! Come on over and visit my web site . Thanks =)
Hi my family member! I want to say that this article is awesome, nice written and include approximately all vital infos. I’d like to see extra posts like this .
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya tidak bisa menahan diri untuk berkomentar
Terima kasih untuk posting luar biasa yang lain. Di tempat mana lagi siapa pun dapat mendapatkan jenis informasi seperti itu dengan pendekatan penulisan yang sempurna? Saya punya presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
I was reading some of your articles on this site and I conceive this web site is really informative! Continue posting.
I like this blog very much so much great info .
Saya selalu peduli dengan topik ini dan tetap masih demikian, sangat dihargai telah mengunggah.
Hmm apakah ada orang lain yang mengalami masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Saya terkesan dengan situs web ini, sungguh saya adalah penggemar.
I like the helpful info you provide in your articles. I’ll bookmark your blog and check again here regularly. I am quite certain I will learn plenty of new stuff right here! Best of luck for the next!
I always was interested in this topic and stock still am, appreciate it for putting up.
Good day! Would you mind if I share your blog with my twitter group?
There’s a lot of people that I think would really enjoy your content.
Please let me know. Thank you
I really like your writing style, excellent information, regards for putting up :D. “Silence is more musical than any song.” by Christina G. Rossetti.
Postingan yang luar biasa. Saya benar-benar menyukai cara Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang hebat!
Menghargai ketekunan yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
As I web site possessor I believe the content material here is rattling excellent , appreciate it for your hard work. You should keep it up forever! Best of luck.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Glad I found this thread, lots of useful information here.
Good conversation here, I’ve learned a few new things already.
Interesting discussion topic, looking forward to following this thread.
Thanks for sharing your thoughts here, this has been a useful discussion.
Good topic for discussion, I enjoyed reading through the replies.
Feel free to surf to my site; reddit.com/r/microgrowery HLVD infection confirmed: he Clone Foundry – 114 strains tested positive
Artikel ini sangat informatif. Saya menghargai waktu yang Anda curahkan untuk menulisnya. Terima kasih!
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna desain yang luar biasa!
Wow! Terima kasih! Saya secara terus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya mengambil fragmen dari posting Anda ke situs saya?
Saya mendapatkan info yang bagus dari blog Anda.
Hmm is anyone else experiencing problems with the pictures on this blog loading? I’m trying to determine if its a problem on my end or if it’s the blog. Any responses would be greatly appreciated.
I really like your blog.. very nice colors & theme. Did you make this website yourself or did you hire someone to do it for you? Plz respond as I’m looking to construct my own blog and would like to know where u got this from. appreciate it
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Umumnya saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat artikel yang bagus.
Saya senang menjadi salah satu pengunjung di situs hebat ini (:, sangat dihargai telah mengunggah.
Saya sungguh beruntung menemukan website ini di Bing, persis seperti yang saya telusuri : D begitu juga sudah saya simpan ke fav.
Menghargai waktu dan tenaga yang Anda curahkan ke website Anda dan informasi mendalam yang Anda tawarkan. Sangat luar biasa menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Saya secara tidak sengaja menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang luar biasa.
Saya selalu peduli dengan subjek ini dan masih demikian, sangat dihargai telah mengunggah.
Postingan yang hebat! Saya menghargai cara Anda menguraikan segala sesuatu dengan sangat jelas. Teruskan kerja yang bagus!
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
I like this post, enjoyed this one thankyou for posting.
Sangat hebat informasi dapat ditemukan di blog.
Mengagumi ketekunan yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda tawarkan. Sangat baik menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menandai situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
I like the helpful info you provide in your articles. I will bookmark your weblog and test once more right here regularly. I’m rather certain I’ll be told a lot of new stuff right right here! Best of luck for the next!
Wow, awesome blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your site is magnificent, as well as the content!
What’s Happening i’m new to this, I stumbled upon this I’ve found It absolutely useful and it has helped me out loads. I hope to contribute & help other users like its aided me. Great job.
Thanks – Enjoyed this article, can I set it up so I receive an email when you write a fresh post?
I do agree with all of the ideas you’ve introduced to your post. They are very convincing and can certainly work. Nonetheless, the posts are too quick for beginners. Could you please prolong them a bit from subsequent time? Thank you for the post.
I have recently started a site, the info you provide on this web site has helped me greatly. Thank you for all of your time & work.
I savour, result in I discovered just what I used to be looking for. You’ve ended my four day long hunt! God Bless you man. Have a great day. Bye
I really like your writing style, wonderful info , thanks for posting :D.
Thanks for all your efforts that you have put in this. very interesting information.
I like this post, enjoyed this one thanks for posting.
Great blog! Do you have any suggestions for aspiring writers? I’m planning to start my own blog soon but I’m a little lost on everything. Would you suggest starting with a free platform like WordPress or go for a paid option? There are so many choices out there that I’m totally overwhelmed .. Any ideas? Thanks a lot!
It is in point of fact a nice and helpful piece of information. I am happy that you shared this helpful information with us. Please keep us informed like this. Thanks for sharing.
I’m very happy to read this. This is the type of manual that needs to be given and not the random misinformation that is at the other blogs. Appreciate your sharing this greatest doc.
Dead indited articles, appreciate it for selective information.
คอนเทนต์นี้ น่าสนใจดี ค่ะ
ดิฉัน ไปเจอรายละเอียดของ หัวข้อที่คล้ายกัน
ดูต่อได้ที่ สล็อตออนไลน์ได้เงินจริง
เผื่อใครสนใจ
เพราะอธิบายไว้ละเอียด
ขอบคุณที่แชร์ ข้อมูลที่มีประโยชน์ นี้
และหวังว่าจะมีข้อมูลใหม่ๆ มาแบ่งปันอีก
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada jalan Anda akan bisa menghapus saya dari layanan itu? Terima kasih!
Artikel yang sangat bagus. Ini memberikan saya gambaran yang lebih baik tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Informasi yang sangat berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
What’s Going down i am new to this, I stumbled upon this I have found It absolutely helpful and it has aided me out loads. I hope to give a contribution & assist different customers like its aided me. Great job.
magnificent points altogether, you just gained a new reader. What would you suggest in regards to your post that you made a few days ago? Any positive?
Saya kebetulan menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang hebat.
Bernilai info. Beruntung saya menemukan website Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
Do you have a spam problem on this site; I also am a blogger, and I was wanting to know your situation; we have developed some nice methods and we are looking to trade methods with other folks, please shoot me an email if interested.
Glad to be one of several visitants on this awful web site : D.
Saya benar-benar ingin menulis pesan singkat untuk mengucapkan terima kasih Anda atas seluruh saran luar biasa yang Anda bagikan di website ini.
Some really howling work on behalf of the owner of this website , absolutely outstanding subject material.
I have learn a few just right stuff here. Certainly worth bookmarking for revisiting. I surprise how a lot effort you place to create this kind of wonderful informative web site.
Loving the info on this website , you have done great job on the articles.
I’ve recently started a web site, the info you provide on this website has helped me tremendously. Thank you for all of your time & work. “If you would know strength and patience, welcome the company of trees.” by Hal Borland.
Hi are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and create my own. Do you require any coding knowledge to make your own blog? Any help would be really appreciated!
Postingan yang luar biasa. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan pekerjaan yang hebat!
Sangat menarik info !Sempurna persis seperti yang saya cari!
Terima kasih atas tulisan yang baik. Faktanya ini dulunya adalah sebuah akun hiburan. Terlihat maju menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Good website! I truly love how it is simple on my eyes and the data are well written. I am wondering how I could be notified whenever a new post has been made. I’ve subscribed to your RSS which must do the trick! Have a nice day!
Wow! Ini bisa jadi salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Sebenarnya Sangat baik. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
Only wanna remark on few general things, The website style is perfect, the written content is very superb. “To imagine is everything, to know is nothing at all.” by Anatole France.
Saya tidak umumnya berkomentar tetapi saya harus mengakui salam untuk posting yang spesial ini : D.
Saya senang menjadi salah satu dari banyak pengunjung di situs web hebat ini (:, terimakasih telah mengunggah.
Postingan yang sangat bagus. Ini memberikan saya pemahaman yang lebih baik tentang subjek ini. Teruskan pekerjaan yang hebat!
Saya senang menjadi pengunjung dari situs murni ini!, salam atas info langka ini!
Artikel yang sangat berguna. Saya baru menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Menikmati menelusuri ini, sangat bagus, terima kasih.
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan pesan yang identik. Apakah ada sarana Anda dapat menghapus saya dari layanan itu? Terima kasih!
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi empat puluh kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Saya sangat menghargai waktu yang Anda luangkan untuk menyusun artikel ini. Informasi yang berguna. Terima kasih!
Postingan ini sangat informatif. Saya sangat menghargai waktu yang Anda curahkan untuk menulisnya. Terima kasih!
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca belakangan ini. Konten yang sangat berguna. Terima kasih telah berbagi.
Saya sangat menghargai usaha yang Anda luangkan untuk membuat artikel ini. Konten yang berguna. Terima kasih banyak!
Postingan yang fantastis. Saya sungguh menikmati cara Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang luar biasa!
Wonderful post! We are linking to this particularly great
post oon our website. Keep up the goid writing.
I was wondering if you ever considered changing the page layout of your blog? Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better. Youve got an awful lot of text for only having 1 or 2 images. Maybe you could space it out better?
Saya tidak sering berkomentar tetapi saya harus menyatakan terimakasih untuk posting yang sempurna ini : D.
Halo semua, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasa cukup banyak wawasan yang bermanfaat. Terima kasih!
Halo, saya sekadar ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini merupakan persis tipe informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada cara Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
Konten yang bermanfaat dan disajikan dengan sangat baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Anda dapat pasti melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Absolutely composed articles, thanks for entropy.
Dengan hampir semuanya yang mana terlihat sedang berkembang di dalam topik spesifik ini, banyak pandangan Anda cenderung agak radikal. Walaupun begitu, saya minta maaf, tetapi saya tidak dapat setuju sepenuhnya pada keseluruhan rencana Anda, meskipun menggairahkan. Tampaknya bagi semua orang bahwa ulasan Anda tidak sepenuhnya tervalidasi dan pada kenyataannya Anda sendiri tidak sepenuhnya percaya diri terhadap argumen tersebut. Dalam hal apa pun saya menikmati membaca.
Undeniably believe that which you stated. Your favorite reason seemed to be on the web the simplest thing to be aware of. I say to you, I certainly get annoyed while people think about worries that they just don’t know about. You managed to hit the nail upon the top and defined out the whole thing without having side effect , people can take a signal. Will probably be back to get more. Thanks
Halo, saya sekadar ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah persis jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar pantas. Konten yang sangat baik dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Good write-up, I’m regular visitor of one’s website, maintain up the excellent operate, and It’s going to be a regular visitor for a lengthy time.
Hei di sana, saya menemukan website Anda lewat Google saat menelusuri subjek yang mirip, blog Anda tampil di posisi atas. Saya perlu mengakui bahwa saya terkejut betapa bagus penyusunannya. Saya sangat menikmati menelusuri ini dan saya akan kembali untuk melihat lebih banyak. Terima kasih!
Terima kasih, saya baru saja menelusuri informasi sekitar subjek ini cukup lama dan milik Anda adalah yang terbaik yang saya ketahui sejauh ini. Namun, bagaimana dengan inti permasalahan? Apakah Anda pasti tentang asal tersebut?
I am not really wonderful with English but I come up this real easy to read .
Sangat menarik detail yang Anda catat, terima kasih telah mengunggah. “Kematian adalah nasihat ahli Alam untuk mendapatkan lebih banyak Kehidupan.” oleh Johann Wolfgang von Goethe.
Terima kasih, saya baru saja menelusuri informasi tentang subjek ini sudah lama dan milik Anda adalah yang terbaik yang saya temukan sejauh ini. Tapi, bagaimana dengan kesimpulan? Apakah Anda yakin tentang sumber tersebut?
Saya benar-benar ingin mengirim pesan singkat guna mengucapkan terima kasih Anda atas seluruh tips luar biasa yang Anda tuliskan di website ini.
Kami bisa memiliki hyperlink perubahan kesepakatan antara kita!
Magnificent beat ! I would like to apprentice while you amend your web site, how can i subscribe for a blog website? The account aided me a acceptable deal. I had been a little bit acquainted of this your broadcast offered bright clear idea
Hai di sana, saya menemukan situs Anda lewat Google saat mencari subjek yang serupa, blog Anda muncul di bagian atas. Saya harus mengakui bahwa saya kagum seberapa baik penyusunannya. Saya benar-benar menyukai menelusuri ini dan saya pasti akan kembali untuk melihat lebih banyak. Terima kasih banyak!
I am always looking online for articles that can help me. Thank you!
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
You should take part in a contest for one of the highest quality sites on the web.
I most certainly will highly recommend this site!
Saya mendapatkan info yang bagus dari blog Anda.
Saya mengunjungi banyak website tetapi saya pikir yang satu ini memiliki sesuatu yang ekstra di dalamnya
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
Artikel yang sangat bagus. Saya sungguh menikmati cara Anda menjelaskan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
Woah! I’m really digging the template/theme of this site. It’s simple, yet effective. A lot of times it’s challenging to get that “perfect balance” between usability and appearance. I must say that you’ve done a amazing job with this. Additionally, the blog loads super quick for me on Safari. Excellent Blog!
Saya menghargai waktu yang Anda luangkan untuk membuat posting ini. Konten yang bernilai. Terima kasih!
Saya tidak umumnya berkomentar tetapi saya harus mengatakan salam untuk posting yang sempurna ini : D.
Menikmati membaca keseluruhan ini, sangat bagus, terima kasih.
Anda bisa pasti melihat keahlian Anda di dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
I and also my buddies have been studying the excellent solutions found on your web page while suddenly came up with a horrible suspicion I had not thanked the website owner for them. Those guys ended up as a consequence glad to study them and now have pretty much been making the most of these things. We appreciate you genuinely well thoughtful as well as for finding this kind of great information millions of individuals are really eager to discover. My very own sincere regret for not saying thanks to you sooner.
Menikmati menelaah ini, sangat bagus, salam.
I conceive this website contains some really superb info for everyone. “There is nothing so disagreeable, that a patient mind cannot find some solace for it.” by Lucius Annaeus Seneca.
Heya! I just wanted to ask if you ever have any issues with hackers? My last blog (wordpress) was hacked and I ended up losing months of hard work due to no backup. Do you have any methods to protect against hackers?
I admire your work, appreciate it for all the great posts.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi luar biasa dibagikan secara bebas.
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me. Anyways, I’m definitely happy I found it and I’ll be book-marking and checking back frequently!
Benar-benar indah info dapat ditemukan di blog.
Umumnya saya tidak membaca posting di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup artikel yang bagus.
급하게 현금이 필요한 순간, 소액결제 현금화를 안전하게 이용하는 방법을 안내합니다. 실제 이용 기준으로 수수료, 절차, 주의사항까지 빠르게 확인하세요.
Wohh persis apa yang saya telusuri, terimakasih atas unggahan.
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
Hey there! Someone in my Myspace group shared this site with us so I came to take a look. I’m definitely enjoying the information. I’m book-marking and will be tweeting this to my followers! Superb blog and terrific style and design.
Saya terkesan dengan website ini, benar-benar saya adalah penggemar.
Saya tanpa henti memikirkan hal ini, terima kasih telah mengunggah.
I like thhe valuble informkation you provixe in your articles.
I will bookmark your weblog and check again here frequently.
I am quite sure I’ll learn plenty of new stuff right here!
Best of luck for the next!
There are some fascinating deadlines in this article but I don’t know if I see all of them center to heart. There is some validity however I will take maintain opinion until I look into it further. Good article , thanks and we wish extra! Added to FeedBurner as well
Thank you for the auspicious writeup. It in fact was a amusement account it. Look advanced to more added agreeable from you! However, how can we communicate?
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Hi would you mind letting me know which hosting company you’re utilizing? I’ve loaded your blog in 3 different internet browsers and I must say this blog loads a lot faster then most. Can you recommend a good hosting provider at a reasonable price? Many thanks, I appreciate it!
Terima kasih, saya baru-baru ini mencari informasi sekitar subjek ini cukup lama dan milik Anda adalah yang terbaik yang saya jumpai sejauh ini. Namun, bagaimana dengan kesimpulan? Apakah Anda yakin tentang asal tersebut?
Saya senang menjadi salah satu dari banyak pengunjung di situs luar biasa ini (:, salam telah memposting.
You could certainly see your skills in the work you write. The arena hopes for more passionate writers such as you who aren’t afraid to say how they believe. All the time follow your heart. “There are only two industries that refer to their customers as users.” by Edward Tufte.
Postingan yang sangat membantu. Saya baru menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
Saya selamanya memikirkan hal ini, terimakasih telah memposting.
Ten portal z recenzjami ułatwia sprawdzenie popularne strony z kasynami https://www.blindspotphoto.fi/uncategorized/hello-world-2/ pod kątem oferty.
Pretty section of content. I just stumbled upon your website and in accession capital to assert that I get actually enjoyed account your blog posts. Anyway I will be subscribing to your augment and even I achievement you access consistently rapidly.
Artikel yang sangat baik. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Umumnya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup posting yang bagus.
Saya selamanya memikirkan hal ini, sangat dihargai telah mengunggah.
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada cara Anda bisa menghapus saya dari layanan itu? Terima kasih!
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan bersyukur kepada Anda.
Meski begitu, terima kasih untuk artikel yang fantastis ini dan walaupun saya tidak setuju sepenuhnya, saya menghormati sudut pandang.
Situs ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
I really like your writing style, wonderful info, thanks for posting :D. “God save me from my friends. I can protect myself from my enemies.” by Claude Louis Hector de Villars.
Konten yang bermanfaat. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Awesome blog! Do you have any hints for aspiring writers? I’m planning to start my own website soon but I’m a little lost on everything. Would you propose starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m totally overwhelmed .. Any tips? Many thanks!
Hai di sana, Anda telah melakukan pekerjaan yang luar biasa. Saya pasti akan menandai ini dan kembali untuk melihat konten lainnya. Terima kasih!
I don’t even know how I ended up here, but I thought this post was great. I do not know who you are but certainly you’re going to a famous blogger if you aren’t already 😉 Cheers!
Hi, Neat post. There’s a problem with your site in internet explorer, would test this… IE still is the market leader and a big portion of people will miss your excellent writing due to this problem.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
I’ve read some good stuff here. Certainly worth bookmarking for revisiting. I wonder how much effort you put to make such a excellent informative site.
Your place is valueble for me. Thanks!…
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke situs saya?
I appreciate, cause I found exactly what I was looking for. You’ve ended my 4 day long hunt! God Bless you man. Have a nice day. Bye
Terima kasih untuk artikel fantastis yang lain. Di mana lagi seseorang dapat mendapatkan jenis informasi seperti itu dengan metode penulisan yang ideal? Saya memiliki presentasi minggu depan, dan saya sedang mencari informasi seperti ini.
Saya kebetulan menemukan website Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang luar biasa.
Hey There. I found your blog using msn. This is an extremely well written article. I’ll make sure to bookmark it and come back to read more of your useful information. Thanks for the post. I will certainly return.
Some really superb info , Glad I discovered this. “Love consists in this, that two solitudes protect and touch and greet each other.” by Rainer Maria Rilke.
Saya puas bahwa saya menemukan web blog ini, benar-benar info yang saya telusuri!
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang identik. Apakah ada cara Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Saya sangat menghargai usaha yang Anda luangkan untuk membuat posting ini. Informasi yang sangat berharga. Terima kasih!
Amat jelas web site, terima kasih untuk pos ini.
Kemarin, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Bagaimanapun, terima kasih untuk poin yang menonjol ini dan meskipun saya tidak setuju sepenuhnya, saya menilai pandangan.
Hi there! I just want to give a huge thumbs up for the great info you have got here on this post. I shall be coming back to your weblog for more soon.
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia pada kenyataannya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka membaca lebih banyak tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan tambahan rincian? Ini sangat berguna bagi saya. Jempol sangat besar untuk kiriman weblog ini!
Saya tidak sering berkomentar tetapi saya harus menyatakan hargai untuk posting yang sempurna ini : D.
Wow, hebat blog format! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Seluruh tampilan website Anda fantastis, serta kontennya!
I’m really enjoying the design and layout of your blog. It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did you hire out a designer to create your theme? Fantastic work!
Saya tidak benar-benar unggul dalam bahasa Inggris tetapi saya memperoleh ini amat mudah untuk diterjemahkan.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
I just couldn’t go away your site before suggesting that I extremely loved the standard info a person provide for your visitors? Is gonna be back ceaselessly to check up on new posts
I’ve been absent for some time, but now I remember why I used to love this website. Thanks , I’ll try and check back more often. How frequently you update your web site?
Your comment is awaiting moderation.
Good afternoon,
Dear Friends.
At the moment I would like to tell more about Great Ocean Road
tours from Melbourne
I think you in search of specifically about Great Ocean Road tours or perhaps you want
to find more about Great Ocean Road tours Australia?!
So this optimally up-to-date information about Great Ocean Road tours from Melbourne
will be the most useful for you.
On our site more more about Great Ocean Road tours Australia,
also information about Great Ocean Road tours from Melbourne.
more about Great Ocean Road tours Australia at https://ctm.kr/gboard/bbs/board.php?bo_table=dico&wr_id=167216
Our Tags: Great Ocean Road tours Australia, Great Ocean Road
tours, Great Ocean Road tours, Great Ocean Road tours Australia, Great Ocean Road tours from Melbourne,
Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great Ocean Road tours from
Melbourne, Great Ocean Road tours
Have a good day http://www.bwheater.co.kr/bbs/board.php?bo_table=free&wr_id=44924
Your comment is awaiting moderation.
Good afternoon,
Dear Friends.
At the moment I would like to tell more about Great Ocean Road tours from Melbourne
I think you in search of specifically about Great Ocean Road tours or perhaps you want to find
more about Great Ocean Road tours Australia?!
So this optimally up-to-date information about Great Ocean Road tours
from Melbourne will be the most useful for you.
On our site more more about Great Ocean Road tours Australia,
also information about Great Ocean Road tours from Melbourne.
more about Great Ocean Road tours Australia at https://ctm.kr/gboard/bbs/board.php?bo_table=dico&wr_id=167216
Our Tags: Great Ocean Road tours Australia, Great Ocean Road tours, Great Ocean Road tours,
Great Ocean Road tours Australia, Great Ocean Road tours
from Melbourne, Great Ocean Road tours from Melbourne,
Great Ocean Road tours from Melbourne, Great Ocean Road tours
from Melbourne, Great Ocean Road tours
Have a good day http://www.bwheater.co.kr/bbs/board.php?bo_table=free&wr_id=44924
Your comment is awaiting moderation.
Good afternoon,
Dear Friends.
At the moment I would like to tell more about Great Ocean Road tours from Melbourne
I think you in search of specifically about Great Ocean Road tours or perhaps you
want to find more about Great Ocean Road tours Australia?!
So this optimally up-to-date information about Great Ocean Road tours from Melbourne will
be the most useful for you.
On our site more more about Great Ocean Road tours Australia,
also information about Great Ocean Road tours from Melbourne.
more about Great Ocean Road tours Australia at https://ctm.kr/gboard/bbs/board.php?bo_table=dico&wr_id=167216
Our Tags: Great Ocean Road tours Australia, Great
Ocean Road tours, Great Ocean Road tours, Great Ocean Road tours Australia,
Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great Ocean Road
tours from Melbourne, Great Ocean Road tours
Have a good day http://www.bwheater.co.kr/bbs/board.php?bo_table=free&wr_id=44924
Your comment is awaiting moderation.
Good afternoon,
Dear Friends.
At the moment I would like to tell more about Great Ocean Road
tours from Melbourne
I think you in search of specifically about Great Ocean Road tours or perhaps you want to find more about
Great Ocean Road tours Australia?!
So this optimally up-to-date information about
Great Ocean Road tours from Melbourne will be the most useful for you.
On our site more more about Great Ocean Road tours Australia, also information about Great Ocean Road tours from Melbourne.
more about Great Ocean Road tours Australia at https://ctm.kr/gboard/bbs/board.php?bo_table=dico&wr_id=167216
Our Tags: Great Ocean Road tours Australia, Great Ocean Road tours, Great Ocean Road tours, Great
Ocean Road tours Australia, Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great Ocean Road tours from Melbourne, Great
Ocean Road tours
Have a good day https://uk.kme-berlin.de/index.php?title=Benutzer:Antje977485
Saya senang menjadi salah satu dari banyak pengunjung di situs internet luar biasa ini (:, terima kasih telah mengunggah.
Your comment is awaiting moderation.
Good afternoon,
Dear Friends.
Now I would like to tell a little about Great Ocean Road tours
I think you thinking specifically about Great Ocean Road tours
Australia or perhaps you desire to learn more about Great Ocean Road tours Australia?!
So this more up-to-date information about Great Ocean Road tours Australia will be the
most useful for you.
On our website a little more about Great Ocean Road
tours from Melbourne, also information about Great
Ocean Road tours.
more about Great Ocean Road tours from Melbourne at http://key-bone.com/bbs/board.php?bo_table=free&wr_id=365967
Our Tags: Great Ocean Road tours Australia, Great Ocean Road
tours from Melbourne, Great Ocean Road tours Australia, Great Ocean Road tours from Melbourne, Great Ocean Road
tours Australia, Great Ocean Road tours Australia, Great Ocean Road tours, Great Ocean Road tours Australia, Great
Ocean Road tours from Melbourne
Have a good day http://www.braiding.co.kr/gnuboard5/bbs/board.php?bo_table=free&wr_id=32009
Saya tidak umumnya berkomentar tetapi saya harus menyatakan terima kasih untuk posting yang luar biasa ini : D.
Rattling good info can be found on web blog.
You made some first rate factors there. I regarded on the internet for the issue and found most people will go together with together with your website.
I visited a lot of website but I conceive this one has got something special in it in it
Postingan yang luar biasa. Ini memberikan saya pemahaman yang lebih jelas tentang subjek ini. Teruskan kerja yang hebat!
Mengagumi usaha yang Anda curahkan ke blog Anda dan informasi terperinci yang Anda sajikan. Sangat luar biasa menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Halo di sana, kamu sudah melakukan pekerjaan yang mengagumkan. Saya pasti akan menyimpan ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Anda bisa jelas melihat keterampilan Anda di dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu kejar hati Anda.
Sangat menarik detail yang Anda amati, salam telah mengunggah. “Peluang jarang diberi label.” oleh John H. Shield.
Ini adalah saran yang sangat baik, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Terima kasih banyak atas artikel yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan kerja yang hebat!
Saya senang menjadi pengunjung dari web blog mutlak ini!, salam atas info langka ini!
Kami bisa memiliki hyperlink pertukaran perjanjian antara kita!
Saya perlu mengatakan, ini adalah salah satu posting terbaik yang pernah saya baca belakangan ini. Konten yang sangat berguna. Terima kasih telah berbagi.
Seiring dengan hampir semuanya yang mana tampak sedang berkembang sepanjang topik khusus ini, pandangan Anda cenderung relatif menarik. Di sisi lain, saya minta maaf, karena saya tidak dapat setuju sepenuhnya pada keseluruhan teori Anda, meskipun menyegarkan. Tampaknya bagi semua orang bahwa ulasan Anda tidak benar-benar dapat dibenarkan dan pada kenyataannya Anda diri Anda tidak benar-benar sepenuhnya yakin terhadap argumen tersebut. Dalam hal apa pun saya menikmati membacanya.
Saya senang menjadi pengunjung dari blog total ini!, terimakasih atas informasi langka ini!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Saya tidak bisa menahan diri untuk berkomentar
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan bersyukur kepada Anda.
Saya puas bahwa saya mengamati weblog ini, tepat informasi yang saya cari!
Isi yang berguna dan ditulis dengan baik. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Isi yang bermanfaat dan disajikan dengan baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Sangat bagus situs yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan pendapat dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Thank you for the sensible critique. Me and my neighbor were just preparing to do a little research about this. We got a grab a book from our local library but I think I learned more from this post. I am very glad to see such wonderful information being shared freely out there.
Umumnya saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup artikel yang bagus.
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang mantap!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
hi!,I like your writing very much! share we communicate more about your post on AOL? I need a specialist on this area to solve my problem. Maybe that’s you! Looking forward to see you.
Saya secara terus menjelajah online untuk artikel yang dapat membantu saya. Terima kasih!
Very clean web site, thanks for this post.
Anda dapat pasti melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
Saya selalu tertarik dengan topik ini dan tetap masih demikian, terimakasih telah mengunggah.
Saya senang menjadi salah satu pengunjung di website luar biasa ini (:, terima kasih telah mengunggah.
As a Newbie, I am permanently exploring online for articles that can aid me. Thank you
I’ve recently started a website, the info you offer on this website has helped me greatly. Thank you for all of your time & work.
Anda bisa jelas melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Saya mendapatkan info yang bagus dari blog Anda.
Saya bersyukur bahwa saya menemukan weblog ini, persis info yang saya telusuri!
I was suggested this blog by means of my cousin. I am not certain whether or not this submit is written by him as nobody else understand such designated approximately my difficulty. You’re amazing! Thanks!
Saya terkesan dengan situs internet ini, benar-benar saya adalah penggemar.
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get three emails with the same comment. Is there any way you can remove people from that service? Thanks!
Saya selamanya memikirkan hal ini, salam telah memposting.
Having read this I thought it was very informative. I appreciate you taking the time and effort to put this article together. I once again find myself spending way to much time both reading and commenting. But so what, it was still worth it!
I appreciate, cause I found exactly what I was looking for. You have ended my four day long hunt! God Bless you man. Have a great day. Bye
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Saya terkesan dengan situs internet ini, benar-benar saya adalah penggemar berat.
Saya gembira bahwa saya mengamati situs ini, benar-benar informasi yang saya cari!
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Saya senang menjadi salah satu dari banyak pengunjung di situs web hebat ini (:, salam telah memposting.
Saya selalu mencari online untuk posting yang dapat membantu saya. Thanks!
Some genuinely nice and utilitarian info on this website, besides I conceive the style contains wonderful features.
Hore google adalah penguasa dunia saya yang membantu saya menemukan web site yang hebat! .
Wow, menakjubkan weblog struktur! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Seluruh tampilan situs Anda sangat baik, belum lagi materinya!
Krótko mówiąc, jeśli ktoś szuka hasła najlepsze polskie kasyna online online ranking, taki portal z
recenzjami pomaga szybciej porównać dostępne
opcje.
Krótko mówiąc, jeśli ktoś szuka hasła najlepsze polskie kasyna online online ranking, taki portal z
recenzjami pomaga szybciej porównać dostępne
opcje.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I cherished as much as you’ll receive carried out right here. The caricature is tasteful, your authored material stylish. however, you command get got an nervousness over that you would like be turning in the following. in poor health for sure come more beforehand again as precisely the same nearly very steadily inside case you shield this hike.
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada jalan Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Good blog! I really love how it is simple on my eyes and the data are well written. I’m wondering how I could be notified whenever a new post has been made. I have subscribed to your RSS feed which must do the trick! Have a nice day!
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
I truly appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You have made my day! Thank you again
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Thanks everyone for sharing your thoughts and experiences here.
Interesting topic, curious to see what others think
about this.
Glad I came across this thread, very interesting conversation so far.
Interesting replies here, definitely an engaging discussion to read through.
Interesting conversation, thanks everyone for
contributing and sharing ideas.
Look into my blog Giveaway
Thanks everyone for sharing your thoughts and experiences here.
Interesting topic, curious to see what others think
about this.
Glad I came across this thread, very interesting conversation so far.
Interesting replies here, definitely an engaging discussion to read through.
Interesting conversation, thanks everyone for
contributing and sharing ideas.
Look into my blog Giveaway
I am extremely inspired with your writing talents and also with the format to your weblog. Is this a paid theme or did you modify it your self? Anyway stay up the nice high quality writing, it is rare to look a great weblog like this one these days..
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna desain yang unggul!
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di situs saya sesuatu seperti itu. Bolehkah saya menerapkan fragmen dari posting Anda ke blog saya?
Wow, menakjubkan weblog tata letak! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda mengagumkan, serta kontennya!
Sangat menarik detail yang Anda utarakan, sangat menghargai telah memposting. “Kematian adalah nasihat ahli Alam untuk mendapatkan lebih banyak Kehidupan.” oleh Johann Wolfgang von Goethe.
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan bersyukur kepada Anda.
Amat mantap informasi dapat ditemukan di web blog.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Ya menyimpan ini bukanlah keputusan yang buruk posting yang hebat! .
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Ya menyimpan ini bukanlah keputusan yang buruk pos yang hebat! .
I got good info from your blog
Excellent weblog here! Additionally your site a lot up very fast! What host are you using? Can I am getting your associate link for your host? I wish my site loaded up as fast as yours lol
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke blog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
obviously like your web site but you have to check the spelling on quite a few of your posts. A number of them are rife with spelling problems and I find it very troublesome to tell the truth nevertheless I will definitely come back again.
Ya menyimpan ini bukanlah keputusan yang buruk pos yang hebat! .
Terima kasih untuk situs web informatif lainnya. Di mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan cara yang sempurna? Saya memiliki sebuah inisiatif yang saya sedang kerjakan, dan saya sudah mengamati informasi seperti ini.
Hai semua, kamu sudah melakukan kerja yang mengagumkan. Saya tentu akan mem-bookmark ini dan kembali untuk membaca konten lainnya. Terima kasih!
Im now not sure the place you’re getting your info, but good topic. I needs to spend some time finding out more or working out more. Thank you for great info I used to be looking for this information for my mission.
I’m truly enjoying the design and layout of your site. It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did you hire out a developer to create your theme? Great work!
Enjoyed reading this, very good stuff, thanks.
Greetings from Carolina! I’m bored to tears at work so I decided to browse your website on my iphone during lunch break. I enjoy the information you present here and can’t wait to take a look when I get home. I’m surprised at how fast your blog loaded on my phone .. I’m not even using WIFI, just 3G .. Anyhow, very good blog!
I’m not sure why but this site is loading extremely slow for me. Is anyone else having this issue or is it a issue on my end? I’ll check back later on and see if the problem still exists.
What i don’t understood is actually how you’re not really much more well-liked than you may be now. You’re so intelligent. You realize thus significantly relating to this subject, produced me personally consider it from so many varied angles. Its like women and men aren’t fascinated unless it is one thing to do with Lady gaga! Your own stuffs nice. Always maintain it up!
I always was interested in this subject and stock still am, thankyou for putting up.
Real nice pattern and wonderful subject material, very little else we need :D.
magnificent points altogether, you simply gained a brand new reader. What would you recommend about your post that you made some days ago? Any positive?
This web page is known as a walk-by for all of the data you needed about this and didn’t know who to ask. Glimpse here, and also you’ll undoubtedly discover it.
Hey, you used to write excellent, but the last few posts have been kinda boring… I miss your great writings. Past few posts are just a bit out of track! come on!
There are some fascinating time limits in this article but I don’t know if I see all of them heart to heart. There is some validity but I will take maintain opinion till I look into it further. Good article , thanks and we would like more! Added to FeedBurner as nicely
very good post, i definitely love this website, carry on it
We’re a group of volunteers and opening a new scheme in our community. Your web site offered us with valuable info to work on. You’ve done an impressive job and our entire community will be grateful to you.
I have been browsing online more than 3 hours today, yet I never found any interesting article like yours. It is pretty worth enough for me. In my opinion, if all webmasters and bloggers made good content as you did, the internet will be a lot more useful than ever before.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Terima kasih atas posting yang hebat. Saya benar-benar menikmati membaca ini dan menemukan banyak informasi yang bermanfaat. Teruskan pekerjaan yang hebat!
My brother suggested I might like this website. He was entirely right. This post truly made my day. You cann’t imagine simply how much time I had spent for this info! Thanks!
Pretty section of content. I just stumbled upon your site and in accession capital to assert that I get in fact enjoyed account your blog posts. Any way I’ll be subscribing to your feeds and even I achievement you access consistently fast.
The very root of your writing while sounding reasonable originally, did not really work perfectly with me personally after some time. Someplace throughout the paragraphs you actually managed to make me a believer but only for a while. I nevertheless have got a problem with your leaps in logic and you would do nicely to fill in all those gaps. In the event that you actually can accomplish that, I could undoubtedly be impressed.
I’m not sure exactly why but this website is loading very slow for me. Is anyone else having this issue or is it a problem on my end? I’ll check back later on and see if the problem still exists.
Wow! Ini mungkin salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Pada dasarnya Luar biasa. Saya juga seorang ahli dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
you are really a good webmaster. The website loading velocity is incredible. It sort of feels that you are doing any unique trick. Furthermore, The contents are masterpiece. you have performed a excellent activity on this topic!
Meski begitu, terima kasih untuk artikel yang fantastis ini dan meskipun saya tidak benar-benar setuju sepenuhnya, saya menghargai perspektif.
Saya sangat menghargai waktu yang Anda luangkan untuk membuat posting ini. Informasi yang berguna. Terima kasih!
It’s really a great and useful piece of information. I’m glad that you shared this helpful info with us. Please keep us informed like this. Thank you for sharing.
Nice read, I just passed this onto a friend who was doing a little research on that. And he actually bought me lunch as I found it for him smile Thus let me rephrase that: Thanks for lunch!
I am not really good with English but I get hold this rattling leisurely to read .
I’ve been absent for a while, but now I remember why I used to love this website. Thank you, I will try and check back more frequently. How frequently you update your web site?
I want forgathering utile info, this post has got me even more info! .
I enjoy the efforts you have put in this, regards for all the great articles.
I don’t ordinarily comment but I gotta tell thankyou for the post on this one :D.
I am lucky that I discovered this web blog, just the right information that I was searching for! .
Can I simply say what a relief to find somebody who actually is aware of what theyre speaking about on the internet. You positively know tips on how to bring a problem to gentle and make it important. Extra folks must learn this and perceive this aspect of the story. I cant imagine youre no more common because you definitely have the gift.
You have brought up a very wonderful points, thanks for the post.
Aw, this was a really nice post. In idea I would like to put in writing like this additionally – taking time and precise effort to make a very good article… but what can I say… I procrastinate alot and not at all appear to get one thing done.
I want studying and I conceive this website got some genuinely utilitarian stuff on it! .
so much great information on here, :D.
Hi , I do believe this is an excellent blog. I stumbled upon it on Yahoo , i will come back once again. Money and freedom is the best way to change, may you be rich and help other people.
I believe this is one of the most significant information for me. And i am glad reading your article. However should observation on some normal things, The web site style is perfect, the articles is in point of fact excellent :D. Just right activity, cheers
Saya tidak benar-benar bagus dalam bahasa Inggris tetapi saya menganggap ini sungguh santai untuk diterjemahkan.
Really Appreciate this article, is there any way I can receive an email every time you publish a new post?
Saya perlu mengatakan, ini adalah salah satu posting terbaik yang yang pernah saya baca dalam waktu yang lama. Konten yang sangat berguna. Terima kasih telah berbagi.
Saya senang menjadi salah satu dari beberapa pengunjung di situs luar biasa ini (:, salam telah memposting.
Saya sangat menghargai waktu yang Anda curahkan untuk membuat posting ini. Informasi yang bernilai. Terima kasih!
I couldn’t resist commenting
Dengan segala sesuatu yang terlihat sedang berkembang di dalam topik khusus ini, banyak pandangan Anda cenderung agak menstimulasi. Meskipun demikian, saya memohon maaf, tetapi saya tidak dapat setuju sepenuhnya pada seluruh rencana Anda, meskipun menyegarkan. Sepertinya bagi semua orang bahwa ulasan Anda tidak sepenuhnya benar-benar dapat dibenarkan dan pada faktanya Anda diri Anda tidak benar-benar sepenuhnya percaya diri terhadap argumen tersebut. Dalam hal apa pun saya menikmati membaca.
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar layak. Isi yang sangat baik dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Hello There. I found your blog using msn. This is a really well written article. I’ll be sure to bookmark it and return to read more of your useful information. Thanks for the post. I will definitely return.
Mengagumi dedikasi yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda tawarkan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
I believe you have observed some very interesting points, regards for the post.
Wow, superb weblog tata letak! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Seluruh tampilan web site Anda fantastis, belum lagi kontennya!
Saya tanpa henti memikirkan hal ini, salam telah mengunggah.
Hello There. I found your blog using msn. This is a really well written article. I will be sure to bookmark it and return to read more of your useful info. Thanks for the post. I will definitely return.
Artikel yang luar biasa! Saya menghargai gaya Anda menguraikan semuanya dengan jelas. Teruskan pekerjaan yang bagus!
Saya tidak umumnya berkomentar tetapi saya harus menyatakan terimakasih untuk posting yang hebat ini : D.
Situs web ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Wohh persis apa yang saya cari, terimakasih atas unggahan.
Some truly wonderful information, Sword lily I found this. “Perfect valor is to behave, without witnesses, as one would act were all the world watching.” by La Rochefoucauld.
Does your site have a contact page? I’m having trouble locating it but, I’d like to send you an email. I’ve got some suggestions for your blog you might be interested in hearing. Either way, great website and I look forward to seeing it develop over time.
Amat jelas website, terima kasih untuk pos ini.
Sangat menarik detail yang Anda sebutkan, sangat menghargai telah mengunggah. “Ketidaktahuan adalah akar dan batang dari setiap kejahatan.” oleh Plato.
Website ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Saya senang menjadi salah satu dari beberapa pengunjung di situs web luar biasa ini (:, terimakasih telah mengunggah.
Saya biasanya tidak menulis komentar, tetapi yang satu ini benar-benar pantas. Isi yang sangat baik dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Enjoyed examining this, very good stuff, regards.
Saya sangat senang menemukan situs internet ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke favorit.
Saya mendapatkan info yang bagus dari blog Anda.
Informasi yang sangat berguna. Saya baru mencari hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Pretty great post. I just stumbled upon your blog and wished to say that I have truly loved browsing your weblog posts. After all I’ll be subscribing for your feed and I hope you write again very soon!
Postingan yang luar biasa! Saya menghargai gaya Anda menjelaskan segala sesuatu dengan jelas. Teruskan kerja yang hebat!
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Really great info can be found on site. “We should be eternally vigilant against attempts to check the expression of opinions that we loathe.” by Oliver Wendell Holmes.
Benar-benar luar biasa info dapat ditemukan di web blog.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Kerja yang mengagumkan!
I really appreciate this post. I’ve been looking all over for this! Thank goodness I found it on Bing. You’ve made my day! Thanks again
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Wow! Ini mungkin salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Sebenarnya Sangat baik. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami kerja keras Anda.
Amat fantastis informasi dapat ditemukan di blog.
Artikel yang sangat baik. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Saya menghargai usaha yang Anda luangkan untuk menyusun posting ini. Konten yang bernilai. Terima kasih!
Wohh persis apa yang saya cari, hargai atas posting.
Sangat menarik informasi!Sempurna persis seperti yang saya cari! “Energi adalah kekuatan yang menggerakkan setiap manusia. Energi tidak hilang karena digunakan, tetapi dipertahankan olehnya.” oleh Germaine Greer.
Wow! This can be one particular of the most beneficial blogs We have ever arrive across on this subject. Basically Fantastic. I am also a specialist in this topic therefore I can understand your hard work.
Ini adalah blog yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini adalah tepat jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
This blog is definitely rather handy since I’m at the moment creating an internet floral website – although I am only starting out therefore it’s really fairly small, nothing like this site. Can link to a few of the posts here as they are quite. Thanks much. Zoey Olsen
With every little thing which seems to be developing inside this subject material, many of your perspectives are generally quite radical. Nevertheless, I beg your pardon, but I do not subscribe to your whole strategy, all be it radical none the less. It appears to me that your opinions are generally not totally justified and in simple fact you are generally your self not really totally convinced of your assertion. In any case I did appreciate examining it.
Postingan yang sangat bagus. Ini memberi saya pemahaman yang lebih baik tentang subjek ini. Teruskan kerja yang hebat!
I absolutely love your blog and find many of your post’s to be just what I’m looking for. can you offer guest writers to write content for yourself? I wouldn’t mind writing a post or elaborating on many of the subjects you write related to here. Again, awesome web log!
Postingan yang sangat bagus. Ini memberi saya gambaran yang lebih jelas tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Ini adalah topik yang sangat penting di hati saya, cheers, tapi di mana detail kontak Anda?
Saya perlu mengatakan, ini adalah salah satu posting paling bagus yang yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
I think this is among the most vital info for me. And i’m glad reading your article. But should remark on some general things, The website style is great, the articles is really great :D. Good job, cheers
Wow! Ini bisa jadi salah satu blog paling membantu yang pernah kami temui tentang topik ini. Sebenarnya Luar biasa. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Artikel yang fantastis! Saya menghargai cara Anda menguraikan segala sesuatu dengan mudah dipahami. Teruskan kerja yang hebat!
Sangat baik situs yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan pendapat dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Salut!
Anda bisa jelas melihat keahlian Anda di dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Very nice post. I just stumbled upon your blog and wanted to mention that I have truly loved surfing around your weblog posts. After all I’ll be subscribing on your feed and I’m hoping you write again soon!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
In the great design of things you get a B+ with regard to effort. Where exactly you lost everybody ended up being in the details. You know, they say, the devil is in the details… And it couldn’t be more correct in this article. Having said that, allow me say to you just what exactly did work. The article (parts of it) is actually highly engaging and this is most likely why I am taking the effort in order to comment. I do not really make it a regular habit of doing that. Second, whilst I can certainly notice a jumps in reasoning you make, I am definitely not certain of just how you seem to connect your points which help to make your conclusion. For right now I will, no doubt yield to your issue but hope in the future you actually connect your dots better.
I like this site so much, saved to fav.
Great post, you have pointed out some excellent points, I as well believe this s a very wonderful website.
부산출장마사지란 전문 마사지 관리사가 고객이 있는 부산 지역 내 자택, 호텔, 숙소, 사무실 등 원하는 장소로 직접 방문하여 마사지를 제공하는 서비스(홈케어)
Appreciating the time and effort you put into your blog and detailed information you provide. It’s nice to come across a blog every once in a while that isn’t the same unwanted rehashed information. Wonderful read! I’ve bookmarked your site and I’m adding your RSS feeds to my Google account.
Postingan yang hebat. Saya sungguh menyukai gaya Anda menyampaikan gagasan-gagasan ini. Teruskan pekerjaan yang luar biasa!
Anda bisa jelas melihat keahlian Anda di dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Konten yang luar biasa! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Jika Anda gagal membesarkan anak-anak Anda, saya rasa apa pun yang Anda lakukan selain itu tidaklah penting.” oleh Jacqueline Lee Bouvier Kennedy Onassis.
Amat jelas situs, terimakasih untuk pos ini.
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Saya terkesan dengan situs internet ini, sangat saya adalah penggemar.
Loving the information on this internet site, you have done outstanding job on the content.
Hey there, I think your website might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, awesome blog!
You have brought up a very great points, thanks for the post.
Terrific work! This is the type of information that should be shared around the web. Shame on Google for not positioning this post higher! Come on over and visit my site . Thanks =)
Saya sangat gembira menemukan situs internet ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke fav.
Saya mengunjungi banyak website tetapi saya anggap yang satu ini mengandung sesuatu yang ekstra di dalamnya
Halo, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah persis tipe informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Artikel ini sangat berguna. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Wow! Terima kasih! Saya selalu membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya mengambil bagian dari posting Anda ke situs saya?
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang unggul!
Benar-benar bersih web site, salam untuk pos ini.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Konten yang luar biasa! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Kerja yang hebat!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Kerja yang hebat!
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada pendekatan Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
You’re so awesome! I do not believe I’ve read through a single thing like that before.
So nice to find someone with genuine thoughts on this topic.
Really.. many thanks for starting this up. This web site is something that is needed on the internet, someone with a
little originality!
Also visit my page; no kyc casinos
You’re so awesome! I do not believe I’ve read through a single thing like that before.
So nice to find someone with genuine thoughts on this topic.
Really.. many thanks for starting this up. This web site is something that is needed on the internet, someone with a
little originality!
Also visit my page; no kyc casinos
Artikel yang fantastis. Saya benar-benar menikmati cara Anda menyampaikan ide-ide ini. Teruskan pekerjaan yang hebat!
Hei di sana, saya menemukan blog Anda lewat Google saat mencari topik yang mirip, blog Anda muncul di hasil teratas. Saya harus mengatakan bahwa saya terkejut betapa bagus pengaturannya. Saya benar-benar menikmati menelusuri ini dan saya pasti akan kembali untuk melihat konten lainnya. Terima kasih!
Saya sangat menghargai usaha yang Anda luangkan untuk menyusun posting ini. Informasi yang bernilai. Terima kasih banyak!
you have a great blog here! would you like to make some invite posts on my blog?
Seseorang secara esensial menolong untuk membuat sangat artikel saya akan katakan. Itu adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga sekarang? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun posting luar biasa ini. Kerja yang luar biasa!
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang mantap!
Saya mendapatkan info yang bagus dari blog Anda.
Wow! Thank you! I constantly wanted to write on my site something like that. Can I include a fragment of your post to my website?
Hai, saya sekadar ingin mengatakan bahwa saya sangat menikmati membaca postingan blog Anda. Ini merupakan tepat jenis informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Postingan yang luar biasa! Saya sangat menghargai gaya Anda menjelaskan semuanya dengan sangat jelas. Teruskan kerja yang hebat!
Konten yang berguna dan ditulis dengan sangat baik. Saya tentu akan membagikan ini kepada teman-teman. Terima kasih telah berbagi.
Saya senang menjadi pengunjung dari situs web total ini!, terimakasih atas info langka ini!
Thanks, I’ve just been searching for info approximately this topic for a long time and yours is the greatest I have discovered so far. However, what about the conclusion? Are you sure in regards to the source?
Way cool, some valid points! I appreciate you making this article available, the rest of the site is also high quality. Have a fun.
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Postingan yang sangat berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi.
Informasi yang sangat berguna. Saya baru saja mencari hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada sarana Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
Great article and right to the point. I don’t know if this is in fact the best place to ask but do you people have any ideea where to hire some professional writers? Thx 🙂
Merely wanna remark on few general things, The website layout is perfect, the subject matter is real good. “Believe those who are seeking the truth. Doubt those who find it.” by Andre Gide.
Sangat jelas web site, terimakasih untuk posting ini.
Berharga info. Beruntung saya menemukan situs web Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Hei semua, Anda telah melakukan pekerjaan yang hebat. Saya tentu akan mem-bookmark ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
This design is wicked! You obviously know how to keep a reader amused. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Great job. I really loved what you had to say, and more than that, how you presented it. Too cool!
Nyata hebat informasi dapat ditemukan di web site.
Isi yang fantastis! Cara penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca konten lainnya.
Tetap saja, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak setuju sepenuhnya, saya menghormati perspektif.
Isi yang luar biasa! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Saya mengunjungi banyak website tetapi saya pikir yang satu ini memiliki sesuatu yang spesial di dalamnya
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar layak. Isi yang hebat dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Wow! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang hebat!
Saya tidak biasanya berkomentar tetapi saya harus menyatakan hargai untuk posting yang hebat ini : D.
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia pada kenyataannya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika bisa dilakukan, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui weblog Anda dengan tambahan detail? Ini sangat berguna bagi saya. Jempol sangat besar untuk kiriman weblog ini!
Konten yang fantastis! Cara penulisan Anda jelas dan mudah dipahami. Saya pasti akan kembali untuk melihat konten lainnya.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
I just like the helpful information you provide to your articles. I will bookmark your blog and test once more right here frequently. I am slightly sure I will be told lots of new stuff right here! Best of luck for the following!
Great web site. Lots of helpful information here. I am sending it to several buddies ans additionally sharing in delicious. And obviously, thank you for your effort!
I conceive this website has some rattling superb info for everyone :D. “The public will believe anything, so long as it is not founded on truth.” by Edith Sitwell.
certainly like your web-site however you have to test the spelling on several of your posts. Many of them are rife with spelling problems and I to find it very bothersome to inform the truth then again I will certainly come back again.
The next time I read a blog, I hope that it doesnt disappoint me as much as this one. I mean, I know it was my choice to read, but I actually thought youd have something interesting to say. All I hear is a bunch of whining about something that you could fix if you werent too busy looking for attention.
I very happy to find this website on bing, just what I was looking for : D besides saved to favorites.
Spot on with this write-up, I honestly think this website needs far more attention. I’ll probably be returning
to read through more, thanks for the advice!
Heya i’m for the first time here. I came across this board and I find It truly useful & it helped me out much. I am hoping to offer one thing back and aid others such as you helped me.
Mengagumi ketekunan yang Anda curahkan ke blog Anda dan informasi terperinci yang Anda tawarkan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
My developer is trying to persuade me to move to .net from PHP. I have always disliked the idea because of the costs. But he’s tryiong none the less. I’ve been using Movable-type on numerous websites for about a year and am concerned about switching to another platform. I have heard good things about blogengine.net. Is there a way I can import all my wordpress posts into it? Any help would be greatly appreciated!
I used to be more than happy to search out this net-site.I wanted to thanks for your time for this wonderful read!! I undoubtedly having fun with every little bit of it and I have you bookmarked to check out new stuff you weblog post.
Saya terkesan dengan situs web ini, amat saya adalah penggemar.
Really fantastic information can be found on web blog. “I know of no great men except those who have rendered great service to the human race.” by Francois Marie Arouet Voltaire.
Do you mind if I quote a couple of your articles as long as I provide credit and sources back to your website? My blog is in the very same area of interest as yours and my users would certainly benefit from some of the information you present here. Please let me know if this okay with you. Regards!
I dugg some of you post as I cogitated they were very helpful invaluable
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia sebenarnya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika bisa dilakukan, seiring Anda berkembang menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak rincian? Ini sangat membantu bagi saya. Jempol besar untuk unggahan blog ini!
Wow! Ini mungkin salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Pada dasarnya Mengagumkan. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
I have been examinating out a few of your articles and i must say nice stuff. I will make sure to bookmark your website.
Saya selalu tertarik dengan subjek ini dan masih demikian, terimakasih telah mengunggah.
Artikel yang sangat baik. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
My brother recommended I might like this website. He was entirely right. This post actually made my day. You can not imagine just how much time I had spent for this info! Thanks!
Saya senang bahwa saya menemukan kembali weblog ini, benar-benar informasi yang saya cari!
Its like you read my mind! You appear to know so much about this, like you wrote the book in it or something. I think that you could do with some pics to drive the message home a little bit, but instead of that, this is fantastic blog. A great read. I’ll certainly be back.
Saya terkesan dengan situs internet ini, amat saya adalah penggemar berat.
I know this if off topic but I’m looking into starting my own weblog and was wondering what all is required to get setup? I’m assuming having a blog like yours would cost a pretty penny? I’m not very web smart so I’m not 100 sure. Any recommendations or advice would be greatly appreciated. Many thanks
I am glad to be a visitant of this consummate website! , thanks for this rare info ! .
Artikel yang hebat. Ini memberi saya gambaran yang lebih baik tentang subjek ini. Teruskan pekerjaan yang luar biasa!
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Kerja yang luar biasa!
Terima kasih atas posting yang luar biasa. Saya sungguh menikmati membaca ini dan menemukan banyak sekali wawasan yang berguna. Teruskan kerja yang hebat!
Wow! Ini bisa jadi salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Pada dasarnya Sangat baik. Saya juga seorang ahli dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Kami bisa memiliki tautan pertukaran kontrak antara kita!
Nice blog here! Additionally your website loads up very fast! What web host are you the use of? Can I am getting your associate link for your host? I want my website loaded up as fast as yours lol
I have recently started a site, the information you provide on this website has helped me tremendously. Thank you for all of your time & work.
Hari ini, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Glad to be one of the visitors on this awing site : D.
Those are yours alright! . We at least need to get these people stealing images to start blogging! They probably just did a image search and grabbed them. They look good though!
Some really interesting info , well written and broadly user pleasant.
Terima kasih untuk situs web informatif lainnya. Di mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan cara yang ideal? Saya punya sebuah tantangan yang saya sedang kerjakan, dan saya telah mencari informasi seperti ini.
Terrific post however , I was wondering if you could write a litte more on this topic? I’d be very thankful if you could elaborate a little bit further. Appreciate it!
Saya secara berkelanjutan menyelidiki online untuk posting yang dapat mendukung saya. Thanks!
It’s perfect time to make some plans for the future and it is time to be happy. I have read this post and if I could I wish to suggest you few interesting things or advice. Perhaps you could write next articles referring to this article. I desire to read more things about it!
I like this website very much so much fantastic information.
Im now not sure the place you are getting your information, however good topic. I must spend a while finding out more or figuring out more. Thank you for fantastic information I used to be on the lookout for this info for my mission.
I’m not sure where you are getting your info, but good topic. I needs to spend some time learning more or understanding more. Thanks for fantastic info I was looking for this information for my mission.
As I web site possessor I believe the content matter here is rattling excellent , appreciate it for your efforts. You should keep it up forever! Good Luck.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Saya mendapatkan info yang bagus dari blog Anda.
You are my inhalation, I own few blogs and often run out from to brand : (.
You could definitely see your enthusiasm in the work you write. The world hopes for more passionate writers like you who are not afraid to say how they believe. Always go after your heart.
Isi yang luar biasa! Cara penulisan Anda jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca lebih banyak.
Heya i’m for the first time here. I came across this board and I to find It truly helpful & it helped me out much. I hope to give one thing back and aid others like you aided me.
A lot of thanks for all your valuable work on this blog. Kim loves conducting research and it’s obvious why. All of us notice all concerning the powerful mode you make both useful and interesting guidelines by means of the blog and even encourage participation from other ones on this matter plus my child is in fact understanding so much. Take advantage of the rest of the year. You’re performing a really great job.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I have been browsing online greater than three hours these days, but I by no means found any interesting article like yours. It’s lovely price enough for me. In my opinion, if all webmasters and bloggers made good content material as you did, the net will likely be much more helpful than ever before. “Where facts are few, experts are many.” by Donald R. Gannon.
Hello. remarkable job. I did not expect this. This is a excellent story. Thanks!
After examine a couple of of the blog posts in your website now, and I really like your approach of blogging. I bookmarked it to my bookmark website record and will likely be checking back soon. Pls check out my site as effectively and let me know what you think.
I do agree with all of the ideas you’ve presented on your post. They’re very convincing and can definitely work. Still, the posts are very quick for beginners. May just you please extend them a bit from subsequent time? Thanks for the post.
Saya senang menjadi salah satu dari banyak pengunjung di situs luar biasa ini (:, salam telah memposting.
I really like your writing style, excellent info , thanks for putting up :D.
Postingan yang sangat baik! Saya sangat menghargai cara Anda menjelaskan semuanya dengan sangat jelas. Teruskan kerja yang bagus!
Saya mendapatkan info yang bagus dari blog Anda.
I was just searching for this information for a while. After six hours of continuous Googleing, at last I got it in your site. I wonder what is the lack of Google strategy that do not rank this kind of informative web sites in top of the list. Normally the top web sites are full of garbage.
Sangat jelas web site, terimakasih untuk pos ini.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Benar-benar jelas situs internet, terimakasih untuk posting ini.
Thank you for the sensible critique. Me & my neighbor were just preparing to do some research about this. We got a grab a book from our local library but I think I learned more clear from this post. I’m very glad to see such great info being shared freely out there.
Great wordpress blog here.. It’s hard to find quality writing like yours these days. I really appreciate people like you! take care
Just a smiling visitor here to share the love (:, btw outstanding layout. “Competition is a painful thing, but it produces great results.” by Jerry Flint.
Really enjoying the discussion here, lots of interesting opinions.
Good conversation here, I’ve learned a few new things already.
Glad I came across this thread, very interesting conversation so far.
Good forum thread with a lot of helpful and interesting comments.
Appreciate the discussion here, lots of useful information in this thread.
Here is my webpage … marijuana clones for sale
Really enjoying the discussion here, lots of interesting opinions.
Good conversation here, I’ve learned a few new things already.
Glad I came across this thread, very interesting conversation so far.
Good forum thread with a lot of helpful and interesting comments.
Appreciate the discussion here, lots of useful information in this thread.
Here is my webpage … marijuana clones for sale
you’re really a good webmaster. The site loading speed is amazing. It seems that you’re doing any unique trick. In addition, The contents are masterpiece. you have done a great job on this topic!
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
Thanks, I have recently been looking for info about this subject for a while and yours is the best I’ve found out so far. But, what about the bottom line? Are you certain concerning the supply?
Hey there! I know this is somewhat off topic but I was wondering which blog platform are you using for this site? I’m getting sick and tired of WordPress because I’ve had issues with hackers and I’m looking at alternatives for another platform. I would be awesome if you could point me in the direction of a good platform.
Its such as you learn my thoughts! You seem to grasp so much about this,
like you wrote the e-book in it or something.
I believe that you just can do with a few p.c. to drive the message
house a little bit, however instead of that, that is great blog.
A fantastic read. I will definitely be back.
magnificent issues altogether, you simply received a logo new reader. What could you suggest in regards to your publish that you simply made a few days ago? Any sure?
Saya terkesan dengan situs web ini, amat saya adalah penggemar berat.
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
I went over this web site and I conceive you have a lot of superb information, saved to my bookmarks (:.
Some truly wonderful information, Gladiola I observed this. “The past is a guide post, not a hitching post.” by L. Thomas Holdcroft.
Wow, hebat blog struktur! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Seluruh tampilan web site Anda hebat, serta kontennya!
It’s hard to find knowledgeable people on this topic, but you sound like you know what you’re talking about! Thanks
Situs web ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
I just like the helpful information you supply in your articles. I’ll bookmark your weblog and test once more right here frequently. I am fairly sure I will be informed plenty of new stuff right right here! Best of luck for the next!
Saya senang bahwa saya menemukan weblog ini, benar-benar informasi yang saya telusuri!
Postingan ini penuh informasi. Saya sangat menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
F*ckin’ remarkable things here. I’m very glad to look your article. Thanks so much and i am taking a look ahead to touch you. Will you please drop me a mail?
Saya harus mengatakan, ini adalah salah satu posting terbaik yang pernah saya baca belakangan ini. Informasi yang sangat membantu. Terima kasih telah berbagi.
Saya senang menjadi salah satu dari beberapa pengunjung di website hebat ini (:, terima kasih telah memposting.
magnificent points altogether, you simply gained a new reader. What would you suggest about your post that you made a few days ago? Any positive?
Wohh baru saja apa yang saya telusuri, terima kasih atas unggahan.
Kami dapat memiliki tautan perdagangan kontrak antara kita!
Hi, Neat post. There’s a problem together with your site in web explorer, could check this?K IE still is the market chief and a good section of other folks will leave out your wonderful writing because of this problem.
I just could not depart your site before suggesting that I extremely enjoyed the standard information a person provide for your visitors? Is going to be back often in order to check up on new posts
Woah! I’m really enjoying the template/theme of this website. It’s simple, yet effective. A lot of times it’s tough to get that “perfect balance” between user friendliness and appearance. I must say that you’ve done a amazing job with this. Also, the blog loads extremely fast for me on Firefox. Superb Blog!
It is truly a nice and helpful piece of info. I’m satisfied that you simply shared this useful info with us. Please stay us informed like this. Thank you for sharing.
I have been checking out some of your articles and i must say pretty clever stuff. I will definitely bookmark your website.
Saya tidak bisa menahan diri untuk berkomentar
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi tiga puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Hei, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah persis tipe informasi yang sedang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
Saya mendapatkan info yang bagus dari blog Anda.
Artikel yang fantastis! Saya menghargai cara Anda menguraikan semuanya dengan sangat jelas. Teruskan kerja yang bagus!
Saya kebetulan menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang luar biasa.
Postingan yang hebat! Saya sangat menghargai cara Anda menjelaskan segala sesuatu dengan sangat jelas. Teruskan pekerjaan yang hebat!
Hi! This is my 1st comment here so I just wanted to give a quick shout out and tell you I genuinely enjoy reading your blog posts. Can you suggest any other blogs/websites/forums that cover the same subjects? Thank you!
Postingan yang bagus. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
I’ve been absent for a while, but now I remember why I used to love this web site. Thank you, I will try and check back more frequently. How frequently you update your web site?
My brother recommended I might like this web site. He was once totally right. This post actually made my day. You cann’t imagine just how so much time I had spent for this information! Thanks!
Halo di sana, sekadar ingin mengatakan bahwa saya sangat menikmati membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa cukup banyak informasi yang bermanfaat. Terima kasih!
I precisely had to say thanks again. I do not know the things that I could possibly have achieved in the absence of the strategies discussed by you on such theme. It was actually an absolute frustrating crisis for me, but encountering the well-written avenue you treated that took me to weep over delight. I’m thankful for this service and even hope you know what a great job you happen to be carrying out teaching the mediocre ones using your web blog. I am certain you haven’t got to know all of us.
Thanks for the sensible critique. Me and my neighbor were just preparing to do some research on this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such wonderful info being shared freely out there.
Saya kebetulan menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang hebat.
Do you have a spam issue on this website; I also am a blogger, and I was curious about your situation; we have created some nice practices and we are looking to trade solutions with other folks, be sure to shoot me an e-mail if interested.
I think this internet site contains very excellent written articles content.
Pretty! This was a really wonderful post. Thank you for your provided information.
It is really a nice and useful piece of information. I am satisfied that you shared this useful info with us. Please stay us up to date like this. Thank you for sharing.
Isi yang berguna dan ditulis dengan sangat baik. Saya tentu akan membagikan ini kepada orang lain. Terima kasih telah berbagi.
Konten yang berguna. Saya baru menelusuri hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Very interesting subject, regards for putting up.
Terima kasih atas tulisan yang baik. Faktanya ini dulunya adalah sebuah konten hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Postingan ini penuh informasi. Saya sangat menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Ini adalah saran yang sangat baik, terutama bagi mereka yang masih baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
You made some nice points there. I looked on the internet for the subject and found most persons will approve with your website.
Saya tidak sering berkomentar tetapi saya harus mengakui hargai untuk posting yang luar biasa ini : D.
Ini adalah blog yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Sangat menarik poin yang Anda catat, sangat menghargai telah memposting.
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Saya senang menjadi pengunjung dari situs mutlak ini!, terimakasih atas info langka ini!
Terima kasih atas tulisan yang bagus. Sebenarnya ini sebelumnya adalah sebuah akun hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berhubungan?
Saya biasanya tidak meninggalkan komentar, tetapi yang ini benar-benar pantas. Konten yang luar biasa dan sangat membantu. Terima kasih telah meluangkan waktu untuk menulis ini.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada jalan Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
I’ll immediately seize your rss feed as I can’t to find your email subscription link or e-newsletter service. Do you have any? Please let me understand so that I may subscribe. Thanks.
Regards for helping out, wonderful information. “Job dissatisfaction is the number one factor in whether you survive your first heart attack.” by Anthony Robbins.
Berharga informasi. Untungnya saya menemukan situs web Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
I adore looking at and I believe this website got some really useful stuff on it! .
Great, I should definitely pronounce, impressed with your website. I had no trouble navigating through all the tabs as well as related information ended up being truly easy to do to access. I recently found what I hoped for before you know it at all. Reasonably unusual. Is likely to appreciate it for those who add forums or anything, web site theme . a tones way for your customer to communicate. Excellent task.
you are truly a just right webmaster. The website loading pace is amazing. It sort of feels that you are doing any unique trick. In addition, The contents are masterwork. you’ve performed a excellent job on this subject!
Saya secara berkelanjutan menyelidiki online untuk posting yang dapat memfasilitasi saya. Thx!
Hey! I know this is kinda off topic nevertheless I’d figured I’d ask. Would you be interested in exchanging links or maybe guest authoring a blog article or vice-versa? My site goes over a lot of the same subjects as yours and I believe we could greatly benefit from each other. If you are interested feel free to shoot me an email. I look forward to hearing from you! Superb blog by the way!
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini sebelumnya adalah sebuah konten hiburan. Terlihat kompleks menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Real good information can be found on web site.
As I website owner I think the subject matter here is really superb, thankyou for your efforts.
I like this web blog very much, Its a very nice berth to read and get info .
I was just looking for this information for a while. After 6 hours of continuous Googleing, at last I got it in your site. I wonder what’s the lack of Google strategy that do not rank this type of informative sites in top of the list. Normally the top sites are full of garbage.
Having read this I thought it was very informative. I appreciate you taking the time and effort to put this article together. I once again find myself spending way to much time both reading and commenting. But so what, it was still worth it!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Your place is valueble for me. Thanks!…
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
Saya senang menjadi pengunjung dari website mutlak ini!, terimakasih atas info langka ini!
I like this post, enjoyed this one appreciate it for posting. “The basis of optimism is sheer terror.” by Oscar Wilde.
I like this site very much, Its a rattling nice spot to read and obtain information. “No one wants advice — only corroboration.” by John Steinbeck.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Pekerjaan yang mengagumkan!
I’ll right away take hold of your rss as I can’t in finding your e-mail subscription hyperlink or newsletter service. Do you have any? Please allow me recognize in order that I may just subscribe. Thanks.
Postingan yang sangat berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
What i don’t understood is actually how you’re not really much more well-liked than you might be right now. You are so intelligent. You realize therefore significantly relating to this subject, produced me personally consider it from a lot of varied angles. Its like women and men aren’t fascinated unless it is one thing to do with Lady gaga! Your own stuffs outstanding. Always maintain it up!
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya sangat senang melihat informasi sangat baik dibagikan secara bebas.
Anda bisa pasti melihat keterampilan Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
Saya tidak bisa menahan diri untuk berkomentar
you’re actually a good webmaster. The website loading speed is incredible. It sort of feels that you’re doing any unique trick. Moreover, The contents are masterwork. you have done a great activity in this topic!
Kami akan memiliki tautan pertukaran kontrak di antara kita!
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang sangat bagus!
Wow! Terima kasih! Saya secara terus ingin menulis di situs saya sesuatu seperti itu. Bolehkah saya menyertakan fragmen dari posting Anda ke blog saya?
I do believe all the ideas you have introduced on your post. They are very convincing and can certainly work. Nonetheless, the posts are too short for starters. May you please extend them a little from subsequent time? Thank you for the post.
Aw, this was a really nice post. In idea I wish to put in writing like this additionally – taking time and precise effort to make an excellent article… however what can I say… I procrastinate alot and on no account seem to get one thing done.
Ya menyimpan ini bukanlah keputusan yang spekulatif posting yang luar biasa! .
I like what you guys are up also. Such smart work and reporting! Carry on the excellent works guys I’ve incorporated you guys to my blogroll. I think it’ll improve the value of my website 🙂
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Kerja yang luar biasa!
Terima kasih atas tulisan yang baik. Pada kenyataannya ini sebelumnya adalah sebuah materi hiburan. Terlihat kompleks menjadi jauh lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat menjaga kontak?
I believe you have observed some very interesting details , thanks for the post.
Artikel yang hebat. Saya benar-benar menyukai gaya Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang luar biasa!
Saya terkesan dengan website ini, benar-benar saya adalah penggemar berat.
Excellent goods from you, man. I’ve understand your stuff previous to and you’re just too fantastic. I really like what you have acquired here, certainly like what you are stating and the way in which you say it. You make it entertaining and you still take care of to keep it smart. I can not wait to read far more from you. This is actually a wonderful site.
Saya secara tidak sengaja menemukan blog Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang bagus.
Nyata bersih web site, hargai untuk pos ini.
I am not positive the place you are getting your information, however good topic. I must spend a while finding out more or working out more. Thanks for magnificent info I used to be on the lookout for this info for my mission.
Anda telah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan berterima kasih kepada Anda.
Hore google adalah raja saya yang membantu saya menemukan website yang luar biasa! .
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Informasi yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
Saya menghargai waktu yang Anda luangkan untuk membuat posting ini. Informasi yang sangat berharga. Terima kasih!
Saya selalu tertarik dengan subjek ini dan masih demikian, terima kasih telah mengunggah.
I have been exploring for a little for any high quality articles or blog posts on this kind of area . Exploring in Yahoo I at last stumbled upon this site. Reading this info So i’m happy to convey that I have an incredibly good uncanny feeling I discovered exactly what I needed. I most certainly will make sure to don’t forget this web site and give it a glance on a constant basis.
Saya mendapatkan info yang bagus dari blog Anda.
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan daerah kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi megah dibagikan secara bebas.
Wow! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Saya tidak biasanya berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang luar biasa ini : D.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya benar-benar senang melihat informasi hebat dibagikan secara bebas.
Artikel yang luar biasa. Ini jelas ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Saya selalu menyelidiki online untuk posting yang dapat memfasilitasi saya. Terima kasih!
Your comment is awaiting moderation.
https://www.youtube.com/@sss8org
https://x.com/sss8org
https://tooter.in/sss8org
https://wakelet.com/@sss8org
https://safechat.com/u/sss8org
https://gravatar.com/sss8org
https://www.blogger.com/profile/15058852690630909046
https://www.mymeetbook.com/sss8org
https://www.pinterest.com/sss8org/
https://demo.wowonder.com/sss8org
https://500px.com/p/sss8org
https://instapaper.com/p/sss8org
https://www.band.us/band/102998220/intro
https://audiomack.com/sss8org
https://fyers.in/community/member/m9xLFBCFzN
https://medibang.com/author/28492537/
https://www.blockdit.com/sss8org
https://portfolium.com/sss8org
https://www.twitch.tv/sss8org/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:C3AE82F06A2171BE0A495FB5@AdobeID
https://profile.hatena.ne.jp/sss8org/
https://issuu.com/sss8org
https://www.investagrams.com/Profile/sss8org
https://gifyu.com/sss8org
https://www.chordie.com/forum/profile.php?id=2553174
https://www.walkscore.com/people/107769847844/sss8org
https://topsitenet.com/profile/sss8org/1942998/
https://akniga.org/profile/1432505-sss8org/
https://disqus.com/by/sss8org/about/
https://www.aicrowd.com/participants/sss8org
https://www.bitchute.com/channel/uklWk4HTgm45/
https://pbase.com/sss8org/sss8org
https://hub.docker.com/u/sss8org
https://spiderum.com/nguoi-dung/sss8org
https://www.gta5-mods.com/users/sss8org
https://www.nicovideo.jp/user/144490142
https://3dwarehouse.sketchup.com/by/sss8org
https://bit.ly/m/sss8org
https://allmylinks.com/sss8org
https://www.tumblr.com/sss8org
https://sites.google.com/view/sss8org/home
https://groups.google.com/g/sss8org
https://sss8org.blogspot.com/2026/06/u.html
https://hashnode.com/@sss8org
https://www.xiuwushidai.com/home.php?mod=space&uid=2735275&do=profile
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6602883
https://startupxplore.com/en/person/sss8org
https://www.proko.com/@sss8org/activity
https://m.xtutti.com/user/profile/493011
https://www.proko.com/@sss8org/activity
https://www.webmastersun.com/members/sss8org.168216/#about
https://sss8org.stck.me/profile
https://joy.link/sss8org
https://connect.garmin.com/app/profile/9d62c501-5f49-4a8d-8aab-9d4ad44208f1
https://pxhere.com/en/photographer-me/5038114
https://teletype.in/@sss8org
https://www.checkli.com/sss8org#/a/process
https://www.nintendo-master.com/profil/sss8org
https://freeimage.host/sss8org
https://motion-gallery.net/users/994549
https://linkin.bio/sss8org/
https://biomolecula.ru/authors/153821
https://talk.plesk.com/members/sssorg.512599/#about
https://www.callupcontact.com/b/businessprofile/sss8org/10114875
https://www.growkudos.com/profile/nh%C3%A0_c%C3%A1i_s8_4
https://blender.community/sss8org/
https://doselect.com/@2403015ff7734c1ebda824ab9
https://matkafasi.com/user/sss8org
https://allmyfaves.com/sss8org
https://www.notebook.ai/users/1371349
https://www.abclinuxu.cz/lide/sss8org
https://muare.vn/shop/sss8org/907772
https://musikersuche.musicstore.de/profil/sss8org/
https://forum.dmec.vn/index.php?members/sss8org.198462/
https://igli.me/sss8org
http://delphi.larsbo.org/user/sss8org
https://www.aseeralkotb.com/en/profiles/sss8org
https://timdaily.vn/members/sss8org.139056/#about
https://app.readthedocs.org/profiles/sss8org/
https://www.dibiz.com/tblerinda
https://iszene.com/user-356403.html
https://www.theyeshivaworld.com/coffeeroom/users/sss8org
https://desksnear.me/users/sss8org
https://www.itchyforum.com/en/member.php?394376-sss8org
https://www.roton.com/forums/users/tblerinda/
https://able2know.org/user/sss8org/
http://www.biblesupport.com/user/848246-sss8org/
https://golosknig.com/profile/sss8org/
https://wallhaven.cc/user/sss8org
https://bandori.party/user/1139997/sss8org/
https://schoolido.lu/user/sss8org/
https://awan.pro/forum/user/183022/
https://fortunetelleroracle.com/profile/sss8org
https://fabble.cc/sss8org
https://pad.geolab.space/s/pTx9gUnKv
https://pad.stuve.de/s/eJ_RMzxra
https://f319.com/members/sss8org.1120885/
https://potofu.me/sss8org
https://transfur.com/Users/sss8org
https://website.informer.com/sss8.org
https://lightroom.adobe.com/u/sss8org?
https://en.islcollective.com/portfolio/12938565
https://www.xosothantai.com/members/sss8org.618861/
https://velog.io/@sss8org/about
https://violet.vn/user/show/id/15283047
https://iplogger.org/logger/5QfY5M5VfVbz/
https://mez.ink/sss8org
https://www.edna.cz/uzivatele/sss8org/
https://digiphoto.techbang.com/users/sss8org
https://leakedmodels.com/forum/members/sss8org.719342/#about
https://inkbunny.net/sss8org
https://beatsaver.com/playlists/1215095
https://participacion.cabildofuer.es/profiles/sss8org/activity
https://www.criminalelement.com/members/sss8org/profile/
https://pad.degrowth.net/s/2sXkcryx9
http://fort-raevskiy.ru/community/profile/sss8org/
https://forum.skullgirlsmobile.com/members/sss8org.231242/#about
https://phatwalletforums.com/user/sss8org
https://idol.st/user/184423/sss8org/
https://www.givey.com/sss8org
https://zerosuicidetraining.edc.org/user/profile.php?id=575951
https://hobowars.com/game/linker.php?url=https://sss8.org/
https://album.link/sss8org
https://forum.pabbly.com/members/sss8org.124788/#about
https://forum.aigato.vn/user/sss8org
https://rapidapi.com/user/sss8org
https://www.skool.com/@nha-cai-s-5369
https://learningapps.org/watch?v=pof42k5zt26
https://www.invelos.com/UserProfile.aspx?alias=sss8org
https://www.video-bookmark.com/bookmark/7151544/sss8org/
https://www.fitday.com/fitness/forums/members/sss8org.html
https://www.fundable.com/sss8-org
https://www.grepmed.com/sss8org
https://espritgames.com/members/51421855/
https://hi-fi-forum.net/profile/1162843
https://scenarch.com/userpages/40013
https://undrtone.com/sss8org
https://marshallyin.com/members/sss8org/
https://gravesales.com/author/sss8org/
https://hukukevi.net/user/sss8org
https://savelist.co/my-lists/users/sss8org
https://zzb.bz/sss8org
https://www.themeqx.com/forums/users/sss8org/
https://www.udrpsearch.com/user/sss8org
https://www.xen-factory.com/index.php?members/sss8org.167170/#about
https://forums.servethehome.com/index.php?members/sss8org.249510/#about
https://activepages.com.au/profile/sss8org
https://snippet.host/tojaov
https://tudomuaban.com/chi-tiet-rao-vat/2927464/sss8org.html
https://phijkchu.com/a/sss8org/video-channels
https://lifeinsys.com/user/sss8org
https://kaeuchi.jp/forums/users/sss8org/
https://protospielsouth.com/user/140444
https://theafricavoice.com/profile/sss8org
https://www.brownbook.net/business/55175510/sss8org
https://hackmd.okfn.de/s/rk4Joh1Zze
https://beteiligung.hafencity.com/profile/sss8org/
https://anyflip.com/homepage/zuher
https://www.spigotmc.org/members/sss8org.2549579/
https://hoo.be/sss8org
https://maxforlive.com/profile/user/sss8org?tab=about
https://3dtoday.ru/blogs/sss8org
https://mathlog.info/users/utoeh0fiQHhe70d3dslLN8ft20s2
https://my.bio/sss8org
https://community.cloudera.com/t5/user/viewprofilepage/user-id/156380
https://fora.babinet.cz/profile.php?id=130543
https://www.shippingexplorer.net/en/user/sss8org/298159
https://shhhnewcastleswingers.club/forums/users/sss8org/
https://connect.gt/user/sss8org
https://www.sunlitcentrekenya.co.ke/author/sss8org/
https://vimeo.com/sss8org
https://www.symbaloo.com/mix/sss8org
https://www.lingvolive.com/en-us/profile/03ecfc39-f0c7-4547-aded-1596223a1bd3/translations
https://www.trackyserver.com/profile/257595
https://www.zubersoft.com/mobilesheets/forum/user-143706.html
https://md.coredump.ch/s/sWDUUZ4Wa
https://aprenderfotografia.online/usuarios/sss8org/profile/
https://hackmd.hub.yt/s/WK5lREYcV
https://sciencemission.com/profile/sss8org
https://beteiligung.tengen.de/profile/sss8org/
https://formulamasa.com/elearning/members/sss8org/
https://chyoa.com/user/sss8org
https://www.royalroad.com/profile/992313
https://community.jmp.com/t5/user/viewprofilepage/user-id/102056
https://viblo.asia/u/sss8org/contact
https://brain-market.com/u/sss8org
https://www.prosebox.net/book/114287/
https://redirect.camfrog.com/redirect/?url=https://sss8.org/
https://www.fw-follow.com/forum/topic/140080/sss8org
https://www.navacool.com/forum/topic/464464/sss8org
https://www.driedsquidathome.com/forum/topic/168250/sss8org
https://www.nongkhaempolice.com/forum/topic/159183/sss8org
https://www.bestloveweddingstudio.com/forum/topic/100305/sss8org
https://www.natthadon-sanengineering.com/forum/topic/126985/sss8org
https://www.rueanmaihom.net/forum/topic/116438/sss8org
https://www.ttlxshipping.com/forum/topic/464465/sss8org
http://worldchampmambo.com/UserProfile/tabid/42/UserID/498471/Default.aspx
http://forum.modulebazaar.com/forums/user/sss8org/
https://www.rcmx.net/userinfo.php?uid=19766
https://eilo.org/user/sss8org
https://forum.web-z.net/profile.php?userid=11061
https://www.bandlab.com/sss8org
https://forum.issabel.org/u/sss8org
https://www.easyhits4u.com/profile.cgi?login=sss8org
https://doc.anagora.org/s/ECWKWb8p6
https://profile.sampo.ru/sss8org
https://www.ekdarun.com/forum/topic/172220/sss8org
https://fanclove.jp/profile/vMBj87xEJe
https://www.d-ushop.com/forum/topic/160749/sss8org
https://findaspring.org/members/sss8org/
https://vietcurrency.vn/members/sss8org.243918/#about
https://fengshuidirectory.com/dashboard/listings/sss8org/
https://library.zortrax.com/members/sss8org/
https://participa.aytojaen.es/profiles/sss8org/activity
https://linkmix.co/55503047
http://linoit.com/users/sss8org/canvases/sss8org
https://www.myconcertarchive.com/en/user_home?id=134789
https://www.buymusic.club/user/sss8org
https://forum.freero.org/space-uid-25922.html
http://genina.com/user/edit/5398890.page
https://wikifab.org/wiki/Utilisateur:Sss8org
https://pad.lescommuns.org/s/eLJ1XetWD
https://rant.li/sss8org/sss8org
https://chanylib.ru/ru/forum/user/31069/
https://producerbox.com/users/sss8org
https://skrolli.fi/keskustelu/users/TBlerinda/
https://www.thehockeypaper.co.uk/forums/users/sss8org
https://www.11plus.co.uk/users/TBlerinda/
https://opaseke.com/users/16327
https://imaginaria.ru/profile/sss8org/
https://nicheless.blog/author/sss8org
https://www.newgenstravel.com/forum/topic/56013/sss8org
https://forum.rexygen.com/user/sss8org
https://www.mapleprimes.com/users/sss8org
https://noti.st/sss8org
https://guitarmaking.co.uk/members/sss8org/
https://scrapbox.io/sss8org/sss8org
https://circle-book.com/circles/71599
https://qiita.com/sss8org
https://www.annuncigratuititalia.it/author/sss8org/
https://nonon-centsnanna.com/members/sss8org/
https://lite.link/sss8org
http://www.brenkoweb.com/user/95265/profile
https://hedgedoc.faimaison.net/s/4L4FBr_1xm
https://www.rossoneriblog.com/author/sss8org/
https://video.fc2.com/a/account/83248037
https://adplist.org/members/sss8org-mpzj240c
https://novel.daysneo.com/author/sss8org/
https://anunt-imob.ro/user/profile/862292
https://congdongmassage.com/members/sss8org.155744/#about
https://vc.ru/id5997166
https://artist.link/sss8org
https://dreevoo.com/profile.php?pid=1834865
https://www.passes.com/sss8org
https://backloggery.com/sss8org
http://palangshim.com/space-uid-5242821.html
https://app.talkshoe.com/user/sss8org
https://m.wibki.com/sss8org
https://pinshape.com/users/8983475-tblerinda?tab=designs
https://sfx.thelazy.net/users/u/sss8org/
https://www.skypixel.com/users/djiuser-v5it2dktz7u1
https://pictureinbottle.com/r/sss8org
https://forum.epicbrowser.com/profile.php?id=161808
https://hedgedoc.eclair.ec-lyon.fr/s/o9oweFBS-
https://www.socialbookmarkssite.com/bookmark/6270313/sss8org/
https://www.plotterusati.it/user/sss8org
https://linqto.me/about/sss8org
https://www.managementpedia.com/members/sss8org.1123855/#about
https://partecipa.poliste.com/profiles/sss8org/activity
https://hedgedoc.stusta.de/s/kkMhUvegG
https://pad.codefor.fr/s/R4cYv_z6i7
https://pad.fablab-siegen.de/s/9Fw5xZlmFl
https://md.swk-web.com/s/zyRqeZOhV
https://hedgedoc.dezentrale.space/s/gglJiERDY
https://pad.darmstadt.social/s/-tLboFgsqJ
https://referrallist.com/profile/sss8org/
https://md.chaosdorf.de/s/83GSiQbeeU
https://telegra.ph/sss8org-06-04
https://runtrip.jp/users/795287
https://www.bonback.com/forum/topic/463734/sss8org
https://www.pathumratjotun.com/forum/topic/200362/sss8org
https://www.iglinks.io/TBlerinda-erv?preview=true
https://www.dokkan-battle.fr/forums/users/sss8org/
https://boss.why3s.cc/boss/home.php?mod=space&uid=274426
https://www.foriio.com/sss8org
https://md.rappet.xyz/s/-do6CdjzBu
https://md.sebastians.dev/s/nuRrIPXfP
https://justpaste.it/u/sss8org
https://www.pozible.com/profile/sss8org
https://www.elephantjournal.com/profile/sss8org/
https://forum.allkpop.com/suite/user/318660-sss8org/#about
https://strikefans.com/forum/users/sss8org/
https://swat-portal.com/forum/wcf/user/53441-sss8org/
https://experiment.com/users/sss8org
http://julia4tied.de/member.php?action=profile&uid=250405
https://commoncause.optiontradingspeak.com/index.php/community/profile/sss8org/
https://mercadodinamico.com.br/author/sss8org/
https://bike-forum.cz/profil/u/sss8org
https://galleria.emotionflow.com/190051/
https://www.myget.org/users/sss8org
https://app.brancher.ai/user/kijgC4BEdKPG
https://mygamedb.com/profile/sss8org
https://forum.aceinna.com/user/sss8org
https://www.giveawayoftheday.com/forums/profile/1913609
https://vcook.jp/users/96836
https://pumpyoursound.com/u/user/1630555
https://app.parler.com/sss8org
https://gitlab.com/sss8org
https://us.enrollbusiness.com/BusinessProfile/7831686/sss8org
https://link4u.cc/@sss8org
https://its-my.link/@sss8org
https://truckymods.io/user/505364
https://cointr.ee/sss8org
https://indian-tv.cz/u/sss8org
https://hedgedoc.envs.net/s/NgdhTRqqA
https://teletype.link/sss8org
https://hubb.link/sss8org/
https://tutorialslink.com/member/BlerindaTika/104722
https://tealfeed.com/sss8org
https://www.goodreads.com/user/show/201609442-sss8org
https://malt-orden.info/userinfo.php?uid=466913
https://www.abookmarking.com/story/sss8org
https://www.letsdobookmark.com/story/sss8org
https://www.mateball.com/sss8org
https://forum.delftship.net/Public/users/sss8org/
https://ofuse.me/my/posts/376372
https://photouploads.com/sss8org
https://raovat.nhadat.vn/members/sss8org-320824.html
https://advego.com/profile/sss8org/
https://bio.site/sss8org
https://www.vnbadminton.com/members/sss8org.82791/
https://gourmet-calendar.com/users/sss8org
https://shootinfo.com/ru/author/sss8org/?pt=ads
https://www.sunemall.com/board/board_topic/8431232/8466128.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8466131.htm
https://fact-finder.xyz/pukiwiki/?sss8org
https://graph.org/sss8org-06-04-2
https://naijamatta.com/63citcom
https://www.sakaseru.jp/mina/user/profile/320132
https://calgarybusinesses.ca/dashboard/reviews/sss8org/
https://www.sciencebee.com.bd/qna/user/sss8org
https://www.notariosyregistradores.com/web/forums/usuario/sss8org/
https://www.biblicaleldership.com/forums/users/sss8org/
https://luvly.co/users/sss8org
https://campsite.bio/sss8org
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8467900.htm
https://www.tai-ji.net/board/board_topic/4160148/8467901.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8467908.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8467914.htm
https://kheotay.com.vn/forums/users/tblerinda
https://crazyservice.by/forum/user/16573/
https://exceldemy.com/forum/members/sss8org.5506/#about
https://www.ontime.co.th/forum/topic/831857/sss8org
https://zepodcast.com/forums/users/sss8org/
https://www.nedrago.com/forums/users/sss8org/
https://www.portotheme.com/forums/users/sss8org/
https://monviet88.com/profile/sss8org/
https://leasedadspace.com/members/sss8org/
https://www.frenchwomenorg.com/sss8org
https://www.beamng.com/members/sss8org.801076/
https://freelance.ru/sss8org
https://alumni.mgimo.ru/page/adaptive/id396681/
https://pods.link/sss8org
https://mylink.page/sss8org
https://onespotsocial.com/sss8org
https://www.scener.com/@sss8org
https://amaz0ns.com/forums/users/sss8org/
https://hostndobezi.com/sss8org
https://paper.wf/sss8org/s8
https://wibki.com/sss8org
https://aphorismsgalore.com/users/sss8org
https://www.moshpyt.com/user/sss8org
https://www.racerjobs.com/profiles/8374478-nha-cai-s8
https://help.orrs.de/user/sss8org
https://www.instructorsnearme.com/author/sss8org/
https://www.yumpu.com/user/sss8org
https://ferrariformula1.hu/community/profile/sss8org/
https://www.pebforum.com/members/sss8org.251948/#about
http://freestyler.ws/user/664526/sss8org
https://justpaste.me/VNBg1
https://sss8org.gumroad.com/
https://allmy.bio/sss8org
https://www.swap-bot.com/user:sss8org
https://sss8org.themedia.jp/
https://whatson.plus/sss8org
https://www.fullhires.com/author/sss8org/
https://ac.db0.company/user/14045/sss8org/
https://www.youyooz.com/profile/sss8org/
https://forum.hiv.plus/user/sss8org
https://affariat.com/user/profile/184422
https://aiforkids.in/qa/user/sss8org
https://sss8org.shopinfo.jp/
https://www.thitrungruangclinic.com/forum/topic/159259/sss8org
https://www.minecraft-servers-list.org/details/sss8org/
https://www.joomla51.com/forum/profile/105938-sss8org
https://baskadia.com/user/gyba
https://www.democracylab.org/user/47401
https://vs.cga.gg/user/244674
https://youslade.com/sss8org
https://bsky.app/profile/sss8org.bsky.social
https://app.nft.nyc/wallet/6a2266435061666c8515f285
https://englishsharedfutures.uk/forums/users/sss8org/
https://www.xmonsta.com/forums/users/sss8org/
https://www.green-collar.com/forums/users/sss8org/
https://ticketme.io/account/XzyGkIL8A
https://forum.euro-pvp.com/user/573596-sss8org/
https://infinitebacklog.net/users/sss8org
https://quangcaoso.vn/sss8org
https://xmrbazaar.com/user/sss8org/
https://tuscl.net/member/894486
https://www.ironlifting.it/forum/member.php?u=433182
https://reactormag.com/members/sss8org/profile
https://gitflic.ru/user/sss8org
https://www.themirch.com/blog/author/sss8org/
https://reach.link/sss8org
https://www.euskalmarket.com/author/sss8org/
https://www.globalbusinesslisting.org/sss8org
https://doingbusiness.eu/profile/sss8org/
https://portfolium.com.au/sss8org
https://ic-info.ru/forum/user/225320/
https://stardust.run/user/174027/sss8org/#preferences
https://gamelet.online/user/sss8org
https://www.facer.io/u/sss8org
https://forum.cnnr.fr/user/sss8org
https://jobs.host-panel.com/author/sss8org/
https://lankadevelopers.lk/user/sss8org
https://www.simplexthailand.com/forum/topic/34153/sss8org
https://sistacafe.com/user/617557
https://www.bunyipclassifieds.com.au/pro/20260605221203
https://www.hardmcasual.net/user/1294/
https://zimexapp.co.zw/sss8org
https://triumph.srivenkateshwaraa.edu.in/profile/sss8org
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3993326
https://feyenoord.supporters.nl/profiel/156641/sss8org
https://propeller.hu/tagok/sss8org/adatlap
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=346294
https://cinderella.pro/user/281812/sss8org/#preferences
https://www.pesteam.it/forum/members/sss8org.98549/#about
https://www.pageorama.com/?p=sss8org
https://coolors.co/u/sss8org
https://camp-fire.jp/profile/sss8org
https://www.pearltrees.com/sss8org/item800310234
https://gesoten.com/profile/detail/12924755
https://edabit.com/user/KGkrtRuqgSRuzTB6R
https://ask.mallaky.com/?qa=user/sss8org
https://www.matrix-digi.com/forums/member.php?action=profile&uid=15257
https://pledgeme.co.nz/profiles/342070
https://forum.herozerogame.com/index.php?/user/169902-sss8org/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2532908
https://hedgedoc.logilab.fr/s/XzqYp7BnE
https://entre-vos-mains.alsace.eu/profiles/sss8org/activity
https://zealy.io/cw/sss8org/questboard?show-info=true
https://www.pintradingdb.com/forum/member.php?action=profile&uid=148356
https://www.vid419.com/home.php?mod=space&uid=3493773
https://www.goodolcomics.com/blog/profile/sss8org/
http://tkdlab.com/wiki/index.php?sss8org
https://volleypedia.org/index.php?qa=user&qa_1=sss8org
http://pcsq28.com/home.php?mod=space&uid=2175822
https://bbs.airav.cc/home.php?mod=space&uid=4691123
https://hker2uk.com/home.php?mod=space&uid=5620800
https://pad.funkwhale.audio/s/nRhWbZL32
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=514406
https://tilengine.org/forum/member.php?action=profile&uid=167909
https://bbs.darkml.net/home.php?mod=space&uid=186165
https://www.play56.net/home.php?mod=space&uid=6285479
https://pad.flipdot.org/s/6iCnIW2z9j
https://hack.allmende.io/s/xn6RUuJvNm
https://md.opensourceecology.de/s/s5y56bQSx
https://md.chaospott.de/s/bXAbTbojv5
http://jobboard.piasd.org/author/sss8org/
http://jobs.emiogp.com/author/sss8org/
https://doc.adminforge.de/s/CJMf8SDPmZ
https://onlinevetjobs.com/author/sss8org/
https://rush1989.rash.jp/pukiwiki/index.php?sss8org
https://log.concept2.com/profile/2970594
https://calaos.fr/forum/member.php?action=profile&uid=21026
https://www.vrwant.org/wb/home.php?mod=space&uid=5176590
https://usabbs.org/home.php?mod=space&uid=89257
http://byltz.com/home.php?mod=space&uid=483314
http://bbs.medicalforum.cn/home.php?mod=space&uid=2331711
https://www.templepurohit.com/forums/users/tblerinda/
https://cornucopia.se/author/sss8org/
https://kttm.club/members/sss8org.5845/#about
https://vnbit.org/members/sss8org.113243/#about
https://pads.zapf.in/s/ohJzpgYPrD
https://pad.libreon.fr/s/crrSDQi76
https://quomon.es/Profile/sss8org/
https://mm.tt/map/4020323336?t=sk5VMGMQ4P
https://www.blurb.com/user/sss8org?profile_preview=true
https://walling.app/n5b7eX1OxnIbnyU3LKFy/-
https://game8.jp/users/503286
http://mura.hitobashira.org/index.php?sss8org
https://dojour.us/u/sss8org
https://urlz.fr/vaZq
https://community.alexgyver.ru/members/sss8org.182729/#about
https://tinyurl.com/sss8org
https://www.toontrack.com/forums/users/sss8org/
https://amazingradio.com/profile/sss8org
https://www.empregosaude.pt/en/author/sss8org/
https://hkgay.net/member.php?action=profile&uid=530812
https://divisionmidway.org/jobs/author/sss8org/
https://sketchersunited.org/users/327690
https://profu.link/u/sss8org
https://newdayrp.com/members/sss8org.76043/#about
https://te.legra.ph/sss8org-06-05
https://chodaumoi247.com/members/sss8org.55092/#about
http://gojourney.xsrv.jp/index.php?sss8org
https://www.bangyaimaterial.com/forum/topic/160676/sss8org
https://myanimelist.net/profile/sss8org
https://playlist.link/sss8org
https://odesli.co/sss8org
https://suzuri.jp/sss8org
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=171202_pg4p78i6
https://ivpaste.com/v/H6PJXfUcbX
https://coinfolk.net/user/sss8org
http://iawbs.com/home.php?mod=space&uid=962958
https://sss8org.theblog.me/
https://forum.tkool.jp/index.php?members/sss8org.112484/#about
https://www.ganjingworld.com/channel/1ijf6q1kbhutdN2uSPJpxaSWR1k00c?tab=about
https://road-to-eden.com/index.php?sss8org
https://megalodon.jp/?url=https://sss8.org/
https://sss8org.storeinfo.jp/
https://slackcommunity.com/u/mwvmnk/#/about
https://es.stylevore.com/user/sss8org
https://www.ameba.jp/profile/general/sss8org/
https://www.adminer.org/redirect/?lang=en&url=https://sss8.org/
https://community.bemeapps.com/user/sss8org
https://www.inkitt.com/sss8org
https://stackoverflow.com/users/32803440/nh%c3%a0-c%c3%a1i-s8?tab=profile
https://www.lookingforjob.co/profile/sss8org
http://arahn.100webspace.net/profile.php?mode=viewprofile&u=251609
https://vietstock247.com/members/sss8org.1613/#about
https://www.menomoniechiro.com/profile/sss8org/profile
https://www.koreaequestrian.com/profile/sss8org/profile
https://www.eyalsflowers.com/profile/sss8org/profile
https://forums.digitalpool.com/member.php?action=profile&uid=15423
https://hackaday.io/sss8org
https://www.jigsawplanet.com/sss8org
https://surl.li/qtqmhh
https://github.com/sss8org
https://www.japaaan.com/user/99776
https://apptuts.bio/sss8org-268792
https://writexo.com/share/4acf781df548
https://song.link/sss8org
https://hoaxbuster.com/redacteur/sss8org
https://dev.muvizu.com/Profile/sss8org/Latest
http://forum.cncprovn.com/members/431152-sss8org
https://www.rwaq.org/users/sss8org
https://www.atozed.com/forums/user-85019.html
https://manylink.co/@sss8org
https://www.maanation.com/sss8org
https://destaquebrasil.com/saopaulo/author/sss8org/
https://www.adsfare.com/sss8org
https://l2top.co/forum/members/sss8org.189702/
https://www.intensedebate.com/people/sss8org1
https://diigo.com/012qo5i
https://commu.nosv.org/p/sss8org
https://www.weddingvendors.com/directory/profile/43466/
https://gitlab.mpi-sws.org/sss8org
http://onlineboxing.net/jforum/user/edit/464666.page
https://brazcanchamber.org/forums/users/sss8org/
https://biiut.com/sss8org
https://devfolio.co/@sss8org/readme-md
https://tawk.to/sss8org
https://www.inventoridigiochi.it/membri/sss8org/profile/
http://koloboklinks.com/site?url=sss8.org
https://theexplorers.com/user?id=a9599009-b605-4c16-8670-873d18e25b1f
https://nogu.org.uk/forum/profile/sss8org/
https://www.tizmos.com/sss8org?folder=Home
https://umczdt.ru/forum/?PAGE_NAME=profile_view&UID=159615
https://www.cryptoispy.com/forums/users/sss8org/
https://www.camtation.com/leden/sss8org/profile/
https://chillspot1.com/user/sss8org
https://aoezone.net/members/sss8org.193246/#about
https://blacksocially.com/sss8org
https://jerseyboysblog.com/forum/member.php?action=profile&uid=102667
https://akwatik.com/sss8org
https://pod.beautifulmathuncensored.de/people/d763ffe042de013f95da021877951523
https://www.bloggalot.com/profile/sss8org
https://photozou.jp/user/top/3455898
https://opencollective.com/nha-cai-s8-e22b9487
https://blooder.net/sss8org
https://md.edgar.bzh/s/UVE-SKJQL
https://s80-29.gitbook.io/s8-docs/
https://nhcis81780553026.website3.me/
https://cdn.muvizu.com/Profile/sss8org/Latest/
https://www.reddit.com/user/sss8org/
https://www.behance.net/nhcis815
https://soundcloud.com/sss8org
https://about.me/sss8org
https://6a218a17acd79.site123.me/
https://support.bitspower.com/support/user/sss8org
https://dongnairaovat.com/members/sss8org.78883.html
https://dentaltechnician.org.uk/community/profile/sss8org/
https://www.babelcube.com/user/nha-cai-s8-61
https://www.anibookmark.com/user/sss8org.html
https://www.aipictors.com/en/users/sss8org
https://kumu.io/sss8org/s8#s8
https://digiex.net/members/sss8org.148525/
https://diit.cz/profil/ipwigpzmjo
https://pixelfed.uno/sss8org
https://crypto.jobs/talent/profile/sss8org
https://www.party.biz/index.php/profile/387164?tab=541
https://www.diggerslist.com/sss8org/about
https://pad.koeln.ccc.de/s/rgUaQ8jzO
https://promosimple.com/ps/4a650/sss8org
https://whitehat.vn/members/sss8org.237077/#about
https://www.siasat.pk/members/sss8org.275962/#about
https://www.salejusthere.com/profile/0328974475
https://forum.gettinglost.ca/user/sss8orgz
http://catalog.drobak.com.ua/communication/forum/user/2852905/
https://forumketoan.com/members/sss8org.45703/#about
https://diendannhansu.com/members/sss8org.109775/#about
https://www.universe.com/users/nha-cai-s8-1JFHZY
https://www.telerik.com/forums/profile/44fcf05f-9410-41e4-8081-09632e94d229
https://nhattao.com/members/user6983973.6983973/
https://sss8org.therestaurant.jp/posts/58889182
https://i.techbang.com/users/8dayjpnet1
https://mforum2.cari.com.my/home.php?mod=space&uid=3407565&do=profile
https://slidehtml5.com/homepage/ajhx#About
https://twitback.com/sss8org
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=785572
https://postr.yruz.one/profile/sss8org
https://ncnews.co/profile/sss8org
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=269972&backurl=%2Fforum%2F%3FPAGE_NAME%3Drules
https://paste.toolforge.org/view/75a4ed83
https://www.codingame.com/profile/5d1da7fd58f43e02c932fc83d129b2600030237
https://sss8org.localinfo.jp/posts/58889208
https://seomotionz.com/member.php?action=profile&uid=137440
http://hkeverton.com/forumnew/home.php?mod=space&uid=660891
https://www.thetriumphforum.com/members/sss8org.68853/
https://ru.myanimeshelf.com/profile/sss8org
https://cloudburstmc.org/members/sss8org.82549/#about
https://uiverse.io/profile/blerinda_8681
https://huggingface.co/sss8org
https://gitea.com/sss8org
https://forum.codeigniter.com/member.php?action=profile&uid=241396
https://www.producthunt.com/@sss8org
https://securityheaders.com/?q=https://sss8.org/
https://infiniteabundance.mn.co/members/40036452
https://gitconnected.com/sss8org
https://roomstyler.com/users/sss8org
https://creator.nightcafe.studio/u/sss8org
https://postheaven.net/sss8org/sss8org
https://oye.participer.lyon.fr/profiles/sss8org/activity
https://writeablog.net/sss8org/sss8org
https://www.pexels.com/@nha-cai-s8-2162067349/
https://blogfreely.net/sss8org/sss8org
https://rebrickable.com/users/sss8org/mocs/photos/
https://www.rctech.net/forum/members/sss8org-554656.html
https://bbcovenant.guildlaunch.com/users/blog/6762169/?mode=view&gid=97523
https://kitsu.app/users/sss8org
https://jobs.siliconflorist.com/employers/4185508-sss8org
https://jobs.tdwi.org/employers/4185583-sss8org
https://jobs.lajobsportal.org/profiles/8372420-nha-cai-s8
https://swag.live/en/user/6a219e41f121b792905d454d
https://zb3.org/sss8org/s8
https://careers.coloradopublichealth.org/profiles/8375603-sss8org
https://www.mikocon.com/home.php?mod=space&uid=296121
https://dialogluzern.ch/profiles/sss8org/activity
https://www.harimajuku.com/profile/sss8org/profile
https://www.ltstesting.com/profile/sss8org/profile
https://www.africangenesis-101.org/profile/sss8org/profile
https://www.miseducationofmotherhood.com/profile/sss8org/profile
https://www.healthleadershipbraintrust.com/profile/sss8org/profile
https://supplyautonomy.com/sss8org.us
https://www.squadskates.com/profile/sss8org/profile
https://www.grioo.com/forum/profile.php?mode=viewprofile&u=5682686
https://start.me/w/xQ6KEw
https://www.chess.com/member/sss8org
https://tabelog.com/rvwr/sss8org/prof/
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1082658
https://backabuddy.co.za/campaign/sss8org
https://notionpress.com/author/1533501
https://md.yeswiki.net/s/tOOOHM1Fif
https://www.myebook.com/user_profile.php?id=sss8org
https://bytesize.me/sss8org
https://www.thethingsnetwork.org/u/sss8org
https://forums.hostsearch.com/member.php?290844-sss8org
https://urlscan.io/result/019e9762-94ac-7301-aab1-d6a7c85812d0/
https://www.motom.me/user/300599/profile?shared=true
https://www.bahamaslocal.com/userprofile/1/297766/sss8org.html
https://sangtac.waka.vn/author/s-gQKZVgeAPL
https://rekonise.com/u/sss8org
https://artelis.pl/autor/profil/240379
https://forum.korabli.su/profile/304351290-sss8org/?tab=field_core_pfield_12
https://mt2.org/uyeler/sss8org.42562/#about
http://www.library.sokal.lviv.ua/forum/profile.php?mode=viewprofile&u=19355&sid=7490afcc51bd7b50f121054b4d95fb66
https://consultas.saludisima.com/yo/sss8org
https://www.tkc-games.com/forums/users/tblerinda/
https://forum.maycatcnc.net/members/sss8org.6540/#about
https://lustyweb.live/members/sss8org.130907/#about
https://tlcworld.it/forum/members/sss8org.39155/#about
https://www.foundryvtt-hub.com/members/sss8org/
https://www.bookingblog.com/forum/users/sss8org/
https://raovat.vn/members/sss8org.146748/about
https://dawlish.com/user/details/53ad3ff6-dc8a-4117-9986-9555cd881c03
https://www.ibizaclubpt.com/members/sss8org.122927/#about
https://clan-warframe.fr/forums/users/sss8org/
https://www.teuko.com/user/sss8org
https://forum.m5stack.com/user/sss8org
http://www.jindousa.cn/bbs/home.php?mod=space&uid=368957
https://learndash.aula.edu.pe/miembros/sss8org/
https://input.scs.community/s/c44WYSw-0t
https://www.coh2.org/user/176305/sss8org
https://mjjcn.com/mjjcnforum/space-uid-1007651.html
https://www.dideadesign.com/forum/topic/56812/sss8org
https://www.hyperlabthailand.com/forum/topic/832251/sss8org
https://www.myaspenridge.com/board/board_topic/3180173/8470584.htm
https://www.emdr-training.net/forums/users/tblerinda/
https://pixbender.com/sss8org36
https://maiotaku.com/p/sss8org/info
https://mysound.ge/profile/sss8org
https://act4sdgs.org/profile/sss8org
https://joy.gallery/sss8org
https://www.donbla.co.jp/user/sss8org
http://www.grandisvietnam.com/members/sss8org.31982/#about
https://crypto4me.net/members/sss8org.33135/#about
https://www.grabcaruber.com/members/sss8org/profile/
https://hackmd.openmole.org/s/_7Wd_VW5M
https://iyinet.com/kullanici/sss8org.100532/#about
https://www.mshowto.org/forum/members/sss8org.html
https://virtuoart.com/sss8org
https://searchengines.bg/members/sss8org.29005/#about
https://support.super-resume.com/sss8org-td1646.html
http://dalle-elementari-all-universita-del-running.381.s1.nabble.com/sss8org-td6859.html
https://www.postman.com/sss8org
https://www.abitur-und-studium.de/Forum/News/s8-trang-chu-s8-com-cong-game-tham-gia-online-nhan-qua-ss-s8
https://tesera.ru/user/sss8org
https://webcamscenter.com/user/sss8org
https://skeptikon.fr/a/sss8org/video-channels
https://fotolibre.social/sss8org
https://pad.interhop.org/s/GMibKAR7mk
https://pad.karuka.tech.rexo.top/load.php?note=5217dd07
https://recash.wpsoul.net/members/sss8org/profile/
https://topkif.nvinio.com/sss8org
https://www.prodesigns.com/wordpress-themes/support/users/sss8org
https://webyourself.eu/sss8org
https://guestboard.co/events/s8-1/details
https://www.tacter.com/@sss8org
https://rsfpost.com/forums/users/sss8org/
https://mail.londonchinese.com/home.php?mod=space&uid=624749&do=profile
https://kabos.net/profile/sss8org/
https://ikanakama.ink/users/343004
https://nortabs.net/user/16469/
https://giloo.ist/member/sss8org/?mainTab=notes&subTab=my_notes
https://www.scamadviser.com/check-website/sss8.org
https://teratail.com/users/sss8org
https://www.warriorforum.com/members/sss8org.html
https://web.bikemap.net/u/sss8org
https://sitereport.netcraft.com/?url=https://sss8.org
https://stepik.org/users/1298005761/profile?auth=registration
https://www.domestika.org/en/sss8org
https://www.are.na/nha-cai-s8-c3_x36p5w0q/sss8org
https://shareyoursocial.com/sss8org
https://www.chichi-pui.com/users/sss8org/
https://kktix.com/user/9097825
https://jobs.windomnews.com/profiles/8376771-nha-cai-s8
https://www.adpost.com/u/sss8org/
https://egl.circlly.com/users/sss8org
https://www.openrec.tv/user/sss8org/about
https://etextpad.com/fndbqvtidr
https://protocol.ooo/ja/users/sss8org
https://pixabay.com/users/sss8org-56181698/
https://b.cari.com.my/home.php?mod=space&uid=3407565&do=profile
https://jobs.echinacities.com/user/center/blog_detail/2694904/27276
https://spoutible.com/sss8org
https://dynamicscommunities.com/community/members/tblerindagmail-com/
https://latinverge.com/profile/41933?tab=541
https://simblr.cc/user/9151-sss8org/
https://www.myminifactory.com/users/sss8org
https://leetcode.com/u/sss8org/
https://uk.gta5-mods.com/users/sss8org
https://www.heavyironjobs.com/profiles/8376871-nha-cai-s8
https://jobs.westerncity.com/profiles/8376876-nha-cai-s8
https://www.blackhatprotools.info/member.php?295623-sss8org
https://jobs.suncommunitynews.com/profiles/8376821-sss8org
https://civitai.com/user/sss8org
https://pantip.com/profile/9366416
https://www.speedrun.com/users/sss8org
https://jobs.landscapeindustrycareers.org/profiles/8376849-sss8org
https://www.wvhired.com/profiles/8376854-sss8org
https://www.weddingbee.com/members/sss8org/
https://routinehub.co/user/sss8org
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.s812
https://gitlab.vuhdo.io/sss8org
https://oyaschool.com/users/sss8org/
https://expathealthseoul.com/profile/sss8org/
https://expatguidekorea.com/profile/sss8org/
https://foss.heptapod.net/sss8org
https://forums.sonicretro.org/members/sss8org.75254/
https://codi.ide3.de/s/JGFJ3Gxx_
https://docs.copincha.org/s/tK_hHO-kx
https://docs.erraticbits.ca/s/dLZ_0Csi68
https://talkmarkets.com/profile/nh%C3%A0-c%C3%A1i-s8-260605-155755
https://www.wikidot.com/user:info/sss8org
https://onlinesequencer.net/members/281082
https://buckeyescoop.com/community/members/sss8org.66547/#about
https://www.onetap.com/members/sss8org.511466/#about
https://forumton.org/members/sss8org.38428/#about
https://www.fitlynk.com/sss8org
https://confengine.com/user/sss8org
https://heylink.me/sss8org
https://hub.vroid.com/en/users/126746763
https://cofacts.tw/user/sss8org
https://www.iniuria.us/forum/member.php?688846-sss8org
https://killtv.me/user/sss8org/
https://cgmood.com/sss8org
https://sss8org.webflow.io/
https://ques.noirandblanco.com/profile/sss8org/
https://www.ybookmarking.com/story/sss8org
https://www.aersia.net/members/sss8org.14707/
https://www.threadless.com/@sss8org/activity
https://kenhsinhvien.vn/m/sss8org.1171125/#about
https://official.link/sss8org
https://papers-please.info/?sss8org
http://www.in-almelo.com/users/sss8org
https://pad.deckenpfronn.info/s/mIl6dDLQz
https://dinosquadsuriku.com/?sss8org
https://codimd.syssec.org/s/tz9SHBKuA
https://wiki.lio-darmstadt.de/s/gOPEnQM1z
https://sparktv.net/sss8org
https://forum.flashphoner.com/members/sss8org.50210/#about
https://www.pixiv.net/en/users/126746763
https://fnote.net/notes/wb6yBL
https://line-monsterfarm.wiki/?sss8org
https://www.freewebmarks.com/user/HLORKS1MynIR
https://egamerprofile.com/player/sss8org
https://marshmallow-qa.com/g46dyjz8bcaet1t
https://doc.itkonzept.at/s/E_y6JRmOi
https://www.kingmods.net/en/profile/sss8org
https://doc.hkispace.com/s/cfrwZpbeY
https://doc.interscalar.eu/s/M5dX1g18m
https://shareshortcuts.com/u/sss8org/
https://app.wedonthavetime.org/profile/sss8org
https://www.newline.co/@sss8org
https://www.prshine.com/profile/sss8org
https://backloggd.com/u/sss8org/
https://thewion.com/sss8org
https://www.completefoods.co/diy/recipes/sss8org
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Wohh baru saja apa yang saya cari, terimakasih atas unggahan.
Kami akan memiliki tautan pertukaran kesepakatan antara kita!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah informasi kontak Anda?
Seiring dengan semua hal yang mana tampak sedang berkembang dalam topik spesifik ini, banyak pandangan Anda ternyata sangat menstimulasi. Namun, saya minta maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh ide Anda, meskipun menstimulasi. Terlihat bagi kami bahwa komentar Anda tidak sepenuhnya rasional dan pada faktanya Anda diri Anda tidak sepenuhnya yakin terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membacanya.
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini dulunya adalah sebuah akun hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa tetap berkomunikasi?
Isi yang luar biasa! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
Bersama dengan semua hal yang tampak sedang dibangun sepanjang topik spesifik ini, sebagian besar pandangan Anda adalah relatif menarik. Meskipun demikian, saya memohon maaf, tetapi saya tidak dapat setuju sepenuhnya pada seluruh strategi Anda, meskipun menggairahkan. Tampaknya bagi saya bahwa komentar Anda tidak sepenuhnya sepenuhnya rasional dan pada faktanya Anda diri Anda tidak sepenuhnya yakin terhadap poin tersebut. Dalam hal apa pun saya menghargai membaca.
Ya menyimpan ini bukanlah kesimpulan yang berisiko tinggi pos yang hebat! .
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Terima kasih untuk situs informatif tambahan. Di tempat mana lagi saya memperoleh info seperti itu yang ditulis dengan pendekatan yang sempurna? Saya memiliki sebuah proyek yang saya sedang kerjakan sekarang, dan saya telah mengamati informasi seperti ini.
Artikel yang sangat menarik dan informatif. Banyak pengguna di Indonesia mencari informasi terpercaya tentang viagra indonesia dan kesehatan pria.
Konten seperti ini sangat membantu pembaca memahami penggunaan yang aman dan efektif.
Terima kasih atas artikel yang bermanfaat ini. Topik viagra indonesia memang
banyak dicari saat ini, terutama bagi mereka yang ingin mendapatkan informasi kesehatan pria
secara aman dan tepat.
Konten yang bagus dan mudah dipahami. Informasi mengenai viagra indonesia sangat
relevan dan membantu banyak orang mendapatkan edukasi yang benar tentang kesehatan pria.
Hore google adalah ratu saya yang membantu saya menemukan web site yang hebat! .
Saya secara tidak sengaja menemukan situs Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang hebat.
Sangat menarik info !Sempurna persis seperti yang saya cari! “Saya sendiri tidak melakukan apa-apa. Roh Kudus melakukan segalanya melalui saya.” oleh William Blake.
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan daerah kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi hebat dibagikan secara bebas.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Website ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Terima kasih, saya baru-baru ini menelusuri informasi tentang topik ini dalam waktu yang panjang dan milik Anda adalah yang paling hebat yang saya ketahui sejauh ini. Namun, bagaimana dengan inti permasalahan? Apakah Anda positif tentang asal tersebut?
Amat fantastis informasi dapat ditemukan di website.
Terima kasih atas tulisan yang bagus. Faktanya ini sebelumnya adalah sebuah akun hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berhubungan?
Saya kebetulan menemukan website Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang luar biasa.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Saya perlu mengatakan, ini adalah salah satu artikel paling bagus yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada pendekatan Anda dapat menghapus saya dari layanan itu? Terima kasih!
Saya mendapatkan info yang bagus dari blog Anda.
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan bersyukur kepada Anda.
Regards for this tremendous post, I am glad I noticed this web site on yahoo.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Luar biasa situs yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan tanggapan dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
Saya mendapatkan info yang bagus dari blog Anda.
Ya menyimpan ini bukanlah kesimpulan yang buruk pos yang hebat! .
Anda bisa jelas melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Terima kasih untuk posting luar biasa tambahan. Di mana lagi siapa pun dapat mendapatkan tipe info seperti itu dengan metode penulisan yang ideal? Saya memiliki presentasi minggu berikutnya, dan saya berada dalam pencarian informasi seperti ini.
Isi yang fantastis! Gaya penulisan Anda sangat jelas dan mudah dipahami. Saya pasti akan kembali untuk membaca konten lainnya.
Saya gembira bahwa saya mendeteksi blog ini, benar-benar informasi yang saya cari!
Situs ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Postingan yang luar biasa! Saya sangat menghargai cara Anda menjelaskan semuanya dengan jelas. Teruskan kerja yang hebat!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Ini adalah situs yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
I have been exploring for a little bit for any high-quality articles or weblog posts on this sort of area . Exploring in Yahoo I at last stumbled upon this web site. Reading this info So i am happy to exhibit that I have a very excellent uncanny feeling I discovered exactly what I needed. I most surely will make certain to do not omit this site and give it a glance on a constant basis.
Kami mungkin memiliki tautan perdagangan kesepakatan antara kita!
Mengagumi waktu dan tenaga yang Anda curahkan ke website Anda dan informasi mendalam yang Anda berikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Saya sangat puas menemukan website ini di Bing, persis seperti yang saya telusuri : D begitu juga sudah saya bookmark.
Isi yang berguna dan ditulis dengan sangat baik. Saya pasti akan membagikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Ini adalah situs yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga hampir sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke website saya?
Saya secara tidak sengaja menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang bagus.
Isi yang fantastis! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
I think you have observed some very interesting points, thanks for the post.
Wow! Terima kasih! Saya secara terus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya menerapkan fragmen dari posting Anda ke blog saya?
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Berharga info. Untungnya saya menemukan situs Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak terjadi lebih awal! Saya menyimpannya.
Terima kasih, saya baru saja menelusuri informasi tentang topik ini cukup lama dan milik Anda adalah yang paling hebat yang saya jumpai sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang asal tersebut?
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna desain yang hebat!
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan berterima kasih kepada Anda.
Tetap saja, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak benar-benar setuju sepenuhnya, saya menghargai perspektif.
I love it when people come together and share opinions, great blog, keep it up.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada pendekatan Anda bisa menghapus saya dari layanan itu? Terima kasih!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah detail kontak Anda?
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Konten yang fantastis! Cara penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca konten lainnya.
Hello my loved one! I wish to say that this article is awesome, great written and come with approximately all important infos. I’d like to see extra posts like this.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke blog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Hei semua, saya menjumpai website Anda melalui Google saat menelusuri subjek yang serupa, blog Anda muncul di hasil teratas. Saya perlu mengatakan bahwa saya terkejut seberapa rapi penulisannya. Saya sangat menyukai membaca ini dan saya akan kembali untuk melihat konten lainnya. Terima kasih banyak!
Hore google adalah ratu saya yang membantu saya menemukan web site yang luar biasa! .
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
Isi yang hebat! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Pekerjaan yang fantastis!
I’ll right away clutch your rss feed as I can’t in finding your e-mail subscription link or e-newsletter service. Do you have any? Kindly let me know so that I may subscribe. Thanks.
Artikel yang hebat. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan kerja yang hebat!
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Kami bisa memiliki tautan perubahan kesepakatan di antara kita!
Greetings I am so grateful I found your web site, I really found you by error, while I was looking on Digg for something else, Anyhow I am here now and would just like to say thank you for a remarkable post and a all round thrilling blog (I also love the theme/design), I don’t have time to go through it all at the minute but I have saved it and also added in your RSS feeds, so when I have time I will be back to read much more, Please do keep up the fantastic work.
Hey! Would you mind if I share your blog with my myspace group? There’s a lot of people that I think would really appreciate your content. Please let me know. Thank you
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
After looking into a handful of the articles on your blog, I truly appreciate your way of writing a blog.
I saved as a favorite it to my bookmark website list and
will be checking back in the near future. Please visit my website as well and let me know your opinion.
My web site; jotform apps
I like what you guys are up too. Such clever work and reporting! Carry on the superb works guys I have incorporated you guys to my blogroll. I think it’ll improve the value of my site 🙂
Bernilai info. Untungnya saya menemukan website Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
You can definitely see your expertise in the work you write. The world hopes for more passionate writers like you who aren’t afraid to say how they believe. Always go after your heart.
I have learn several just right stuff here. Certainly price bookmarking for revisiting. I wonder how much effort you place to create one of these fantastic informative web site.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Spot on with this write-up, I really think this web site needs far more consideration. I’ll in all probability be again to read way more, thanks for that info.
Namun, terima kasih untuk artikel yang fantastis ini dan walaupun saya tidak benar-benar sepakat sepenuhnya, saya menilai pandangan.
Terima kasih untuk artikel megah lainnya. Di tempat mana lagi seseorang dapat mendapatkan jenis informasi seperti itu dengan cara penulisan yang sempurna? Saya memiliki presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Artikel yang sangat membantu. Saya baru saja menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang luar biasa!
Saya biasanya tidak menulis komentar, tetapi yang ini benar-benar layak. Konten yang sangat baik dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
It is really a great and helpful piece of information. I’m happy that you simply shared this useful info with us. Please stay us informed like this. Thank you for sharing.
I think other website owners should take this website as an model, very clean and superb user friendly style and design.
I reckon something truly interesting about your website so I saved to favorites.
Hi there! I know this is kinda off topic however , I’d figured I’d ask. Would you be interested in exchanging links or maybe guest writing a blog article or vice-versa? My website discusses a lot of the same topics as yours and I think we could greatly benefit from each other. If you’re interested feel free to shoot me an e-mail. I look forward to hearing from you! Terrific blog by the way!
great post, very informative. I wonder why the other specialists of this sector do not notice this. You should continue your writing. I am sure, you have a great readers’ base already!
Wow! This could be one particular of the most beneficial blogs We have ever arrive across on this subject. Actually Great. I am also an expert in this topic therefore I can understand your hard work.
I got what you mean , thankyou for posting.Woh I am glad to find this website through google. “Food is the most primitive form of comfort.” by Sheila Graham.
You made some decent factors there. I appeared on the web for the difficulty and located most individuals will associate with along with your website.
Hey! I simply wish to give an enormous thumbs up for the nice data you could have here on this post. I can be coming back to your blog for extra soon.
Terima kasih banyak atas artikel yang luar biasa. Saya sungguh menikmati membaca ini dan menemukan banyak informasi yang berguna. Teruskan pekerjaan yang hebat!
Sangat menarik detail yang Anda sebutkan, sangat menghargai telah memposting.
You made some respectable points there. I looked on the internet for the issue and located most people will go together with along with your website.
Postingan yang sangat baik. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Saya biasanya tidak meninggalkan komentar, tetapi yang satu ini benar-benar pantas. Konten yang luar biasa dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Saya tidak sering berkomentar tetapi saya harus mengakui salam untuk posting yang spesial ini : D.
I like this web blog very much so much superb information.
Wohh baru saja apa yang saya cari, hargai atas posting.
Thank you! I appreciate it.
Terima kasih, saya baru saja mencari informasi sekitar subjek ini sudah lama dan milik Anda adalah yang paling hebat yang saya ketahui hingga sekarang. Tapi, bagaimana dengan inti permasalahan? Apakah Anda positif tentang sumber tersebut?
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Hari ini, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Sangat bagus blog yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan saran dari orang-orang yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Cheers!
Saya senang menjadi salah satu dari beberapa pengunjung di situs internet luar biasa ini (:, sangat dihargai telah mengunggah.
Wohh persis apa yang saya cari, terimakasih atas posting.
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih ahli, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak detail? Ini sangat membantu bagi saya. Jempol besar untuk posting weblog ini!
You have mentioned very interesting points! ps nice site. “Every man over forty is a scoundrel.” by George Bernard Shaw.
I’m now not certain the place you are getting your information, but good topic. I needs to spend a while studying more or understanding more. Thank you for great info I was on the lookout for this information for my mission.
Terima kasih untuk posting hebat lainnya. Di tempat mana lagi seseorang bisa mendapatkan jenis informasi seperti itu dengan pendekatan penulisan yang sempurna? Saya punya presentasi minggu depan, dan saya sedang mencari informasi seperti ini.
Hey, you used to write fantastic, but the last few posts have been kinda boring?K I miss your tremendous writings. Past several posts are just a bit out of track! come on!
Terima kasih untuk website informatif tambahan. Di mana lagi saya bisa mendapatkan informasi seperti itu yang ditulis dengan cara yang sempurna? Saya punya sebuah misi yang saya tengah jalankan, dan saya sudah mencari informasi seperti ini.
I am really enjoying the theme/design of your website. Do you ever run into any internet browser compatibility issues? A handful of my blog readers have complained about my site not working correctly in Explorer but looks great in Firefox. Do you have any ideas to help fix this problem?
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Postingan yang sangat berguna. Saya baru saja menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Would you be inquisitive about exchanging links?
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan daerah kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi sangat baik dibagikan secara bebas.
Terima kasih, saya baru saja menelusuri informasi sekitar topik ini dalam waktu yang panjang dan milik Anda adalah yang terbaik yang saya temukan hingga sekarang. Tapi, bagaimana dengan inti permasalahan? Apakah Anda pasti tentang asal tersebut?
I got what you intend, regards for putting up.Woh I am glad to find this website through google. “The test and use of a man’s education is that he finds pleasure in the exercise of his mind.” by Carl Barzun.
This is really interesting, You are a very skilled blogger. I’ve joined your feed and look forward to seeking more of your excellent post. Also, I’ve shared your website in my social networks!
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar pantas. Isi yang sangat baik dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Saya sungguh ingin mengirim komentar singkat untuk mengucapkan terima kasih Anda atas seluruh saran luar biasa yang Anda tuliskan di situs ini.
Saya senang menjadi salah satu pengunjung di situs luar biasa ini (:, terima kasih telah mengunggah.
I have read a few good stuff here. Certainly worth bookmarking for revisiting. I wonder how much effort you put to make such a excellent informative website.
Postingan yang sangat baik! Saya menghargai cara Anda menguraikan segala sesuatu dengan sangat jelas. Teruskan kerja yang hebat!
Ya menyimpan ini bukanlah penentuan yang berisiko tinggi pos yang hebat! .
Postingan yang luar biasa. Saya benar-benar menikmati cara Anda menyampaikan gagasan-gagasan ini. Teruskan pekerjaan yang luar biasa!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan tambahan detail? Ini sangat berguna bagi saya. Jempol sangat besar untuk unggahan blog ini!
Konten yang hebat! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Aavant produces the best photography, event and theatre backdrops in the world and works for almost all the biggest players in the world. Being in backdrops industry for last two decades it is the largest player in the world, providing highest quality backdrops to every buyer from USA to Australia.
Hai, saya hanya ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini merupakan persis jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Artikel yang luar biasa. Ini memberi saya pemahaman yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
Aavant produces the best photography, event and theatre backdrops in the world and works for almost all the biggest players in the world. Being in backdrops industry for last two decades it is the largest player in the world, providing highest quality backdrops to every buyer from USA to Australia.
I like what you guys are up also. Such clever work and reporting! Carry on the excellent works guys I have incorporated you guys to my blogroll. I think it’ll improve the value of my site 🙂
You could definitely see your skills in the work you write. The sector hopes for more passionate writers like you who are not afraid to say how they believe. All the time follow your heart.
Hello! Quick question that’s completely off topic. Do you know how to make your site mobile friendly? My weblog looks weird when viewing from my iphone4. I’m trying to find a template or plugin that might be able to resolve this problem. If you have any suggestions, please share. Thanks!
Spot on with this write-up, I truly assume this web site needs way more consideration. I’ll most likely be once more to learn much more, thanks for that info.
For most recent news you have to pay a visit web and on the web I found this site
as a finest site for latest updates.
naturally like your website however you need to test the spelling on several of your posts.
Several of them are rife with spelling problems and I to find it very troublesome
to inform the truth nevertheless I will definitely come again again.
I have learn some good stuff here. Definitely price bookmarking for revisiting. I surprise how a lot effort you set to make one of these fantastic informative website.
We are a group of volunteers and starting a new scheme in our community. Your website offered us with valuable info to work on. You have done an impressive job and our entire community will be grateful to you.
Saya selalu melihat online untuk tips yang dapat mendukung saya. Thanks!
Saya mendapatkan info yang bagus dari blog Anda.
Excellent items from you, man. I’ve take into accout your stuff previous to and you are just too magnificent. I really like what you’ve obtained here, certainly like what you are stating and the way wherein you are saying it. You make it entertaining and you continue to take care of to stay it smart. I cant wait to read much more from you. That is really a wonderful website.
Saya puas bahwa saya mengamati situs web ini, persis info yang saya telusuri!
Saya harus mengatakan, ini adalah salah satu posting terbaik yang pernah saya baca dalam waktu yang lama. Konten yang sangat berguna. Terima kasih telah berbagi.
I always was interested in this topic and stock still am, appreciate it for putting up.
Terima kasih untuk artikel megah lainnya. Di tempat mana lagi siapa pun mungkin bisa mendapatkan tipe info seperti itu dengan cara penulisan yang ideal? Saya punya presentasi minggu depan, dan saya berada mencari informasi seperti ini.
Kami bisa memiliki tautan perubahan kesepakatan antara kita!
Saya senang menjadi salah satu dari banyak pengunjung di situs web luar biasa ini (:, salam telah mengunggah.
Artikel yang bagus. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
Your comment is awaiting moderation.
https://www.facebook.com/people/R%E1%BA%A1p-C%C6%B0%E1%BB%9Bi-H%E1%BA%A3i-Ph%C3%B2ng/61589547527248/
https://www.youtube.com/@rapcuoihaiphong
https://x.com/rapcuoihaiphong
https://tooter.in/rapcuoihaiphong
https://wakelet.com/@RapCuoiHaiPhongcom
https://safechat.com/u/rap.cuoi.hai.phong
https://www.blogger.com/profile/15053809838577729078
https://www.pinterest.com/rapcuoihaiphongcom/?invite_code=d0163f36f08e452b85fcc8bcef870813&sender=1133148093651834945
https://demo.wowonder.com/rapcuoihaiphongcom
https://shareyoursocial.com/rapcuoihaiphongcom
https://500px.com/p/rapcuoihaiphongcom
https://www.instapaper.com/p/rapcuoihaiphong/folder/5363696/r-p-c-i-h-i-ph-ng
https://protocol.ooo/ja/users/r-p-c-i-h-i-phong
https://www.tumblr.com/rapcuoihaiphongcom
https://www.reddit.com/user/Parking_Sell237/?solution=cbe6a126f876f1f5cbe6a126f876f1f5&js_challenge=1&token=bbbe4bf1c9a2b5160829c4be34da58614acd7c865eabdd22b1a03405de624143&jsc_orig_r=&utm_source=share&utm_medium=web3x&utm_name=web3xcss&utm_term=1&utm_content=share_button
https://audiomack.com/rapcuoihaiphongcom
https://leetcode.com/u/rapcuoihaiphongcom/
https://swag.live/user/6a09726eae95231837a05a12?utm_source=share&utm_campaign=userid_6a09726eae95231837a05a12&utm_content=profile_6a09726eae95231837a05a12
https://www.halaltrip.com/user/profile/350736/rapcuoihaiphong/
https://medibang.com/author/28318324/
https://www.blockdit.com/rapcuoihaiphong
https://portfolium.com/rapcuoihaiphongcom
https://www.twitch.tv/rapcuoihaiphongcom/about
https://profile.hatena.ne.jp/rapcuoihaiphongcom/profile
https://issuu.com/rapcuoihaiphongcom?ps=24
https://www.behance.net/rpcihiphng
https://gravatar.com/rapcuoihaiphongcom
https://www.reverbnation.com/rapcuoihaiphongcom
https://www.myminifactory.com/users/rapcuoihaiphong
https://www.investagrams.com/Profile/rapcuoihaiphongcom
https://gifyu.com/rapcuihaiphong
https://www.chordie.com/forum/profile.php?id=2535463
https://www.longisland.com/profile/rapcuoihaiphongcom
https://www.walkscore.com/people/154648310898/rapcuoihaiphongcom
https://topsitenet.com/profile/rapcuoihaiphongcom/1790398/
https://akniga.org/profile/1425736-rap-cuoi-hai-phng/
https://rapcuoihaiphongcom.bandcamp.com/album/r-p-c-i-h-i-ph-ng
https://jobs.suncommunitynews.com/profiles/8291833-r-p-c-i-h-i-phong
https://www.speedrun.com/users/rapcuoihaiphongcom
https://www.fanart-central.net/user/rapcuoihaiphongcom/profile
https://www.aicrowd.com/participants/rapcuoihaiphongcom
https://old.bitchute.com/channel/3uPKfswnOtJ6/
https://pbase.com/rapcuoihaiphongcom
https://hub.docker.com/u/rapcuoihaiphongcom
https://spiderum.com/nguoi-dung/rapcuoihaiphongcom
https://www.gta5-mods.com/users/rapcuoihaiphongcom
https://heylink.me/rapcuoihaiphongcom/
https://www.nicovideo.jp/user/144290493
https://3dwarehouse.sketchup.com/by/rapcuoihaiphong
https://robertsspaceindustries.com/en/citizens/RapCuoiHaiPhong
https://joy.bio/rapcuoihaiphongcom
https://connect.garmin.com/app/profile/6b7509f7-b9a3-47bc-bea8-c3ffe3a1d5fc
https://www.chichi-pui.com/users/rapcuoihaiphong/
https://pxhere.com/en/photographer-me/5018184
https://teletype.in/@rapcuoihaiphong
https://www.checkli.com/rapcuoihaiphongcom#/a/process
https://www.fuelly.com/driver/rapcuoihaiphongcom
https://www.nintendo-master.com/profil/rapcuoihaiphongcom
https://freeimage.host/rapcuoihaiphong
https://motion-gallery.net/users/982606
https://linkin.bio/rapcuoihaiphongcom
https://biomolecula.ru/authors/149396
https://talk.plesk.com/members/ellstromwandriezm24-g.508579/#about
https://www.callupcontact.com/b/businessprofile/rapcuoihaiphongcom/10092604
https://blender.community/rap_cuoi/
https://doselect.com/@70ac3c1a093f2f09026347766
https://sciter.com/forums/users/rapcuoihaiphongcom/
https://matkafasi.com/user/rapcuoihaiphongcom
https://allmyfaves.com/rapcuoihaiphongcom
https://conecta.bio/rapcuoihaiphongcom
https://doodleordie.com/profile/rapcuoihaiphongcom
https://www.intensedebate.com/people/rapcuoihaiphong
https://forum.dmec.vn/index.php?members/rapcuoihaiphongcom.194207/
https://igli.me/rapcuoihaiphongcom
http://delphi.larsbo.org/user/rapcuoihaiphongcom
https://timdaily.vn/members/rapcuoihp.137185/#about
https://app.readthedocs.org/profiles/rapcuoihaiphongcom/
https://www.dibiz.com/ellstromwandriezm24
https://iszene.com/user-353090.html
https://desksnear.me/users/rapcuoihaiphongcom
https://able2know.org/user/rapcuoihaiphongcom/
https://golosknig.com/profile/rapcuoihaiphongcom/
https://www.anibookmark.com/user/rapcuoihaiphongcom.html
https://forum.m5stack.com/user/rapcuoihaiphongcom
https://old.bitchute.com/channel/3uPKfswnOtJ6/
https://bandori.party/user/987442/rapcuoihaiphongcom/
https://community.m5stack.com/user/rapcuoihaiphongcom
https://schoolido.lu/user/rapcuoihaiphongcom/
https://awan.pro/forum/user/176195/
https://fabble.cc/rapcuoihaiphongcom
https://affariat.com/user/profile/182465
https://www.sythe.org/members/rapcuoihaiphongcom.2053448/
https://f319.com/members/rapcuoihaiphongcom.1111915/
https://about.me/rapcuoihaiphongcom
https://booklog.jp/users/rapcuoihaiphong/profile
https://www.equinenow.com/farm/rapcuoihaiphongcom.htm
https://wefunder.com/rapcuoihaiphongcom
https://potofu.me/rapcuoihaiphongcom
https://transfur.com/Users/rapcuoihaiphongcom
https://xtremepape.rs/members/rapcuoihaiphongcom.676254/#about
https://myanimelist.net/profile/rapcuoihaiphong
https://qna.habr.com/user/rapcuoihaiphongcom
https://en.islcollective.com/portfolio/12925364
https://www.xosothantai.com/members/rapcuoihaiphongcom.615274/
https://violet.vn/user/show/id/15277723
https://iplogger.org/vn/logger/8pRT5eFWJmKF/
https://mez.ink/rapcuoihaiphongcom
https://notionpress.com/author/1523906
https://www.edna.cz/uzivatele/rapcuoihaiphongcom/
https://digiphoto.techbang.com/users/rapcuoihaiphongcom
https://onlinesequencer.net/forum/user-275952.html
https://inkbunny.net/rapcuoihaiphongcom
https://www.japaaan.com/user/81334
https://spinninrecords.com/profile/rapcuoihaiphongcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/r%E1%BA%A1p.c%C6%B0%E1%BB%9Bi.h%E1%BA%A3i.ph%C3%B2ng
https://apptuts.bio/rapcuoihaiphongcom
https://dialog.eslov.se/profiles/rapcuoihaiphongcom/activity?locale=en
https://www.storenvy.com/rapcuoihaiphong
https://participacion.cabildofuer.es/profiles/rapcuoihaiphongcom/activity
https://egl.circlly.com/users/rapcuoihaiphongcom
https://goodandbadpeople.com/rapcuoihaiphongcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=306634
https://www.sciencebee.com.bd/qna/user/rapcuoihaiphongcom
https://acomics.ru/-rapcuoihaiphongcom
https://writexo.com/share/a41c356a2418
https://expatguidekorea.com/profile/rapcuoihaiphongcom/
https://www.laundrynation.com/community/profile/rapcuoihaiphongcom/
https://www.heavyironjobs.com/profiles/8295026-r-p-c-i-h-i-phong
https://pad.degrowth.net/s/LWUQcvh3t
http://fort-raevskiy.ru/community/profile/rapcuoihaiphongcom/
https://forum.skullgirlsmobile.com/members/rapcuoihaiphongcom.225506/#about
https://jobs.landscapeindustrycareers.org/profiles/8295077-r-p-c-i-h-i-phong
https://song.link/rapcuoihaiphongcom
https://idol.st/user/177528/rapcuoihaiphongcom/
https://violet.vn/user/show/id/15277723
https://www.bmwpower.lv/user.php?u=rapcuoihaiphongcom
https://jobs.windomnews.com/profiles/8295210-r-p-c-i-h-i-phong
https://pc.poradna.net/users/1212300674-rapcuoihaiphongcom
https://zerosuicidetraining.edc.org/user/profile.php?id=569601
https://aiplanet.com/profile/rapcuoihaiphongcom
https://beteiligung.amt-huettener-berge.de/profile/rapcuoihaiphongcom/
https://jobs.westerncity.com/profiles/8295349-r-p-c-i-h-i-phong
https://www.thetriumphforum.com/members/r%E1%BA%A1p-c%C6%B0%E1%BB%9Bi-h%E1%BA%A3i-ph%C3%B2ng.66734/
https://l2top.co/forum/members/r%E1%BA%A1p-c%C6%B0%E1%BB%9Bi-h%E1%BA%A3i-ph%C3%B2ng.182495/
http://www.askmap.net/location/7825046/vi%E1%BB%87t-nam/rapcuoihaiphongcom
https://app.brancher.ai/user/4FK7Wqwb_FjR
https://www.empregosaude.pt/en/author/rapcuoihaiphongcom/
https://confengine.com/user/rapcuoihaiphongcom
https://mygamedb.com/profile/ellstromwandriezm24
https://www.buckeyescoop.com/users/422835e9-50cb-4c20-a943-4d7199b94df5
https://forum.aceinna.com/user/rapcuoihaiphong
https://web-tourist.net/members/rapcuoihaiphongcom.54743/#about
https://forum.pabbly.com/members/rapcuoihaiphongcom.120164/#about
https://ncnews.co/profile/rapcuoihaiphongcom
https://dreevoo.com/profile.php?pid=1685277
https://forum.aigato.vn/user/rapcuoihaiphong
https://amaz0ns.com/forums/users/rapcuoihaiphongcom/
https://rapidapi.com/user/ellstromwandriezm24
https://www.skool.com/@rap-cuoi-hai-phong-9846
https://learningapps.org/watch?v=pihdb0yvk26
https://www.giveawayoftheday.com/forums/profile/1870513
http://onlineboxing.net/jforum/user/editDone/459389.page
https://tealfeed.com/rapcuoihaiphongcom/connect
https://www.invelos.com/UserProfile.aspx?Alias=rapcuoihaiphongcom
https://wibki.com/rapcuoihaiphongcom
https://aniworld.to/user/profil/rapcuoihaiphongcom
https://kktix.com/user/8978020
https://www.passes.com/rapcuoihaiphongcom
https://uiverse.io/profile/rpci_5507
https://cofacts.tw/user/rapcuoihaiphongcom
https://www.fitday.com/fitness/forums/members/rapcuoihaiphongcom.html
https://www.fundable.com/user-1320542
https://vcook.jp/users/93723
https://www.grepmed.com/rapcuoihaiphongcom
https://espritgames.com/members/51179655/
https://cgmood.com/rapcuoihaiphongcom
https://www.efunda.com/members/people/show_people.cfm?Usr=rapcuoihaiphongcom
https://backloggery.com/rapcuoihaiphong
https://www.moshpyt.com/user/rapcuoihaiphongcom
https://pumpyoursound.com/u/user/1624980
https://scenarch.com/userpages/37576
https://marshallyin.com/members/rapcuoihaiphongcom/
https://gram.social/rapcuoihaiphongcom
https://searchengines.bg/members/rapcuoihaiphongcom.27912/#about
https://luvly.co/users/rapcuoihaiphongcom
https://hukukevi.net/user/rapcuoihaiphongcom
https://savelist.co/profile/users/rapcuoihaiphongcom
https://www.apsense.com/user/rapcuoihaiphongcom
https://zzb.bz/zOBfT2
https://draft.blogger.com/profile/15053809838577729078
https://hack.allmende.io/s/HXl_QRd6Y
https://pad.codefor.fr/s/EoiwnoI2jg
https://hackmd.hub.yt/s/wV1Ega6Wu
https://www.themeqx.com/forums/users/rapcuoihaiphongcom/
https://www.udrpsearch.com/user/rapcuoihaiphongcom
http://newdigital-world.com/members/rapcuoihaiphongcom.html
https://www.xen-factory.com/index.php?members/rapcuoihaiphongcom.162573/#about
https://cointr.ee/rapcuoihaiphongcom
https://forums.servethehome.com/index.php?members/rapcuoihaiphongcom.245645/#about
https://jali.me/rapcuoihaiphongcom
https://www.blackhatprotools.info/member.php?292711-rapcuoihaiphongcom
https://activepages.com.au/profile/rapcuoihaiphongcom
https://snippet.host/yyeyhw
https://tudomuaban.com/chi-tiet-rao-vat/2910714/rap-cuoi-hai-phong.html
https://phijkchu.com/a/rapcuoihaiphongcom/video-channels
https://lifeinsys.com/user/rapcuoihaiphongcom
https://www.claimajob.com/profiles/8297416-r-p-c-i-h-i-phong
https://theafricavoice.com/profile/rapcuoihaiphongcom
http://palangshim.com/space-uid-5188149.html
https://www.africangenesis-101.org/profile/ellstromwandriezm2473337/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:4F9982E66A0983560A495F99@AdobeID
https://gravatar.com/rapcuoihaiphongcom
https://www.mixcloud.com/rapcuoihaiphongcom/
https://www.designspiration.com/ellstromwandriezm24/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=198460
https://www.pixiv.net/en/users/126302643
https://www.brownbook.net/business/55112877/rapcuoihaiphongcom
https://etextpad.com/uogx1xvxwt
https://app.hellothematic.com/creator/profile/1152604
https://www.babelcube.com/user/rap-cuoi-hai-phong
https://app.talkshoe.com/user/rapcuoihaiphongcom/about
https://golden-forum.com/memberlist.php?mode=viewprofile&u=232280
https://wibki.com/rapcuoihaiphongcom?tab=R%E1%BA%A1pC%C6%B0%E1%BB%9BiH%E1%BA%A3iPh%C3%B2ng
https://www.pageorama.com/?p=rapcuoihaiphongcom
https://bandsworksconcerts.info/index.php?HOME
https://jerseyboysblog.com/forum/member.php?action=profile&uid=97833
https://manylink.co/@rapcuoihaiphongcom
https://seomotionz.com/member.php?action=profile&uid=134020
https://anyflip.com/homepage/mbxkw
https://copynotes.be/shift4me/forum/user-57392.html
https://tabelog.com/rvwr/rapcuoihaiphongcom/prof/
https://prosinrefgi.wixsite.com/pmbpf/profile/ellstromwandriezm2412834/profile
https://coolors.co/u/rapcuoihaiphongcom
https://civitai.com/user/rapcuoihaiphongcom
https://www.spigotmc.org/members/rapcuoihaiphong.2539057/
https://camp-fire.jp/profile/rapcuoihaiphongcom
https://feyenoord.supporters.nl/profiel/153586/rapcuoihaiphongcom
https://www.pearltrees.com/rapcuoihaiphongcom/item797118898
https://gesoten.com/profile/detail/12854023
https://hashnode.com/@rapcuoihaiphongcom
https://hoo.be/rapcuoihaiphongcom
https://nhattao.com/members/user6973269.6973269/
https://maxforlive.com/profile/user/rapcuoihaiphongcom?tab=about
https://3dtoday.ru/blogs/rapcuoihaiphongcom
https://pinshape.com/users/8972632-ellstromwandriezm24?tab=designs
https://morguefile.com/creative/rapcuoihaiphongcom
https://edabit.com/user/bWHMBGrwGW7jww5fH
https://community.cloudera.com/t5/user/viewprofilepage/user-id/154385
https://sfx.thelazy.net/users/u/rapcuoihaiphongcom/
https://app.daily.dev/rapcuoihaiphongcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=265543
https://www.skypixel.com/users/djiuser-fzr5cvm9msmt
https://www.slmath.org/people/108596
https://userstyles.world/user/rapcuoihaiphongcom
https://www.shippingexplorer.net/en/user/rapcuoihaiphongcom/290579
https://rapcuoihaiphongcom.notepin.co/
https://forum.epicbrowser.com/profile.php?section=personal&id=158255
http://www.dungdong.com/home.php?mod=space&uid=3383723
https://www.squadskates.com/profile/ellstromwandriezm2497006/profile
https://forum.herozerogame.com/index.php?/user/167009-rapcuoihaiphongcom/
https://electroswingthing.com/profile/rapcuoihaiphongcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2507804
https://connect.gt/user/rapcuoihaiphongcom
https://forum.tkool.jp/index.php?members/rapcuoihaiphongcom.109815/#about
https://www.weddingbee.com/members/Rap%20Cuoi%20Hai%20Phong/
https://bioimagingcore.be/q2a/user/rapcuoihaiphongcom
https://www.sunlitcentrekenya.co.ke/author/rapcuoihaiphongcom/
https://www.livejournal.com/profile/?userid=102817572&t=I
https://entre-vos-mains.alsace.eu/profiles/rapcuoihaiphongcom/activity
https://www.rcuniverse.com/forum/members/rapcuoihaiphongcom.html
https://www.hogwartsishere.com/1843734/
https://makeagif.com/user/jfnf22p4szv?ref=QdHgUi
https://www.trackyserver.com/profile/253808
https://www.pintradingdb.com/forum/member.php?action=profile&uid=146617
https://www.zubersoft.com/mobilesheets/forum/user-140686.html
https://hackmd.openmole.org/s/VN3VEMBz9
https://md.chaosdorf.de/s/xbyJKm4gzZ
https://md.openbikesensor.org/s/ZyE7BORes3
https://www.plotterusati.it/user/rapcuoihaiphongcom
https://tutorialslink.com/member/R%C3%A1%C2%BA%C2%A1pC%C3%86%C2%B0%C3%A1%C2%BB%C2%9BiH%C3%A1%C2%BA%C2%A3iPh%C3%83%C2%B2ng/102566
https://linqto.me/n/rapcuoihaiphongcom
https://www.goodolcomics.com/blog/profile/rapcuoihaiphongcom/
https://www.managementpedia.com/members/ellstromwandriezm24-gmail.1122716/#about
https://partecipa.poliste.com/profiles/rapcuoihaiphongcom/activity
https://hker2uk.com/home.php?mod=space&uid=5581754
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=507060
https://aprenderfotografia.online/usuarios/rapcuoihaiphongcom/profile/
https://pads.zapf.in/s/L-yJ-kVEQw
https://md.swk-web.com/s/T2b-JGsj3
https://hedgedoc.dezentrale.space/s/ihQbqSZfO
https://ar.gravatar.com/rapcuoihaiphongcom
https://odesli.co/rapcuoihaiphongcom
https://wandb.ai/profile/rapcuoihaiphongcom
https://bbcovenant.guildlaunch.com/users/blog/6758677/?mode=view&gid=97523
http://jobboard.piasd.org/author/rapcuoihaiphongcom/
https://www.wvhired.com/profiles/8298761-r-p-c-i-h-i-phong
https://kenhrao.com/members/rapcuoihaiphongcom.123417/#about
http://jobs.emiogp.com/author/rapcuoihaiphongcom/
https://forumketoan.com/members/rapcuoihaiphongcom.45119/#about
https://onlinevetjobs.com/author/rapcuoihaiphongcom/
https://gl.gta5-mods.com/users/rapcuoihaiphongcom
https://formulamasa.com/elearning/members/rapcuoihaiphongcom/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1126534
https://forum.flashphoner.com/members/rapcuoihaiphongcom.48671/#about
https://backloggd.com/u/rapcuoihaiphong/
https://kenhsinhvien.vn/m/rapcuoihaiphongcom.1169613/#about
https://bwinglive.lighthouseapp.com/users/1998963
https://www.stylevore.com/user/ellstromwandriezm24
https://www.noff.gg/user/rapcuoihaiphongcom
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6536642
https://telegra.ph/rapcuoihaiphongcom-05-19
https://hype4.academy/profile/rapcuoihaiphongcom
https://reactormag.com/members/rapcuoihaiphongcom/
https://failiem.lv/ellstromwandriezm24
https://brain-market.com/u/rapcuoihaiphong
https://www.prosebox.net/box/83321/
http://forum.orangepi.org/home.php?mod=space&uid=6536642
https://beteiligung.hafencity.com/profile/rapcuoihaiphongcom/
https://adhocracy.plus/profile/rapcuoihaiphongcom/
https://beteiligung.stadtlindau.de/profile/rapcuoihaiphongcom/
Konten yang fantastis! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Artikel ini penuh informasi. Saya sangat menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
Aku sungguh ingin menulis pesan singkat guna mengucapkan terima kasih Anda atas seluruh tips luar biasa yang Anda tuliskan di situs ini.
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit analisis tentang ini. Dan dia pada kenyataannya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih ahli, apakah Anda berkenan memperbarui blog Anda dengan tambahan detail? Ini sangat berguna bagi saya. Jempol sangat besar untuk kiriman weblog ini!
Keep functioning ,terrific job!
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Hebat situs yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin sekali menjadi bagian dari kelompok di mana saya bisa mendapatkan saran dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Saya kebetulan menemukan blog Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang hebat.
I have read some good stuff here. Definitely worth bookmarking for revisiting. I surprise how a lot attempt you put to make this kind of fantastic informative web site.
Postingan yang luar biasa. Ini memberi saya gambaran yang lebih baik tentang subjek ini. Teruskan pekerjaan yang hebat!
Saya tidak sering berkomentar tetapi saya harus menyatakan terimakasih untuk posting yang sempurna ini : D.
You are my inspiration, I possess few web logs and rarely run out from post :). “Fiat justitia et pereat mundus.Let justice be done, though the world perish.” by Ferdinand I.
Hmm is anyone else having problems with the pictures on this blog loading? I’m trying to figure out if its a problem on my end or if it’s the blog. Any feedback would be greatly appreciated.
Bersama dengan semua hal yang tampak sedang dibangun dalam topik ini, banyak pandangan Anda umumnya relatif menarik. Walaupun begitu, saya maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh rencana Anda, meskipun radikal. Sepertinya bagi semua orang bahwa pendapat Anda tidak benar-benar rasional dan pada faktanya Anda sendiri tidak sepenuhnya pasti terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membacanya.
Isi yang luar biasa! Gaya penulisan Anda sangat jelas dan mudah dipahami. Saya tentu akan kembali untuk membaca lebih banyak.
Saya mendapatkan info yang bagus dari blog Anda.
Kami bisa memiliki tautan perdagangan perjanjian antara kita!
References:
Online casino biz https://https://favpress.site/item/hit-prospekt-n-chste-woche-ab-26-05-2026/item/hit-prospekt-n-chste-woche-ab-26-05-2026
Your comment is awaiting moderation.
https://www.facebook.com/llwinvncom
https://issuu.com/llwinvncom
https://www.tumblr.com/llwinvncom
https://500px.com/p/llwinvncom?view=photos
https://gravatar.com/llwinvncom
https://www.youtube.com/@llwinvncom
https://shareyoursocial.com/llwinvncom
https://tooter.in/llwinvncom
https://demo.wowonder.com/1779512073452159_555822
https://band.us/band/102834788/post/1
https://wakelet.com/@llwinvncom
https://www.behance.net/llwinvncom
https://profile.hatena.ne.jp/llwinvncom/profile
https://scholar.google.com/citations?view_op=list_works&hl=en&authuser=1&user=tX9qtdEAAAAJ
https://graph.org/LLWIN-05-23
https://dongnairaovat.com/members/llwinvncom.77847.html
https://www.nintendo-master.com/profil/llwinvncom
https://www.intensedebate.com/people/llwinvncom1
https://forum.aceinna.com/user/llwinvncom1
https://www.vnbadminton.com/members/llwinvncom.80997/
https://participacion.cabildofuer.es/profiles/llwinvncom/activity?locale=en
https://hub.vroid.com/en/users/126403579
https://hukukevi.net/user/llwinvncom
https://www.gta5-mods.com/users/llwinvncom
https://supplyautonomy.com/llwin11.vn
https://fileforums.com/member.php?u=300557
https://www.adsfare.com/llwinvncom
https://profile.sampo.ru/llwinvncom
https://phijkchu.com/a/llwinvncom/video-channels
http://forum.vodobox.com/profile.php?section=personal&id=73850
https://www.fw-follow.com/forum/topic/133735/llwinvncom
https://pinshape.com/users/8975701
https://3dtoday.ru/blogs/llwinvncom
https://www.chichi-pui.com/users/llwinvncom/
https://en.islcollective.com/portfolio/12929621
https://www.driedsquidathome.com/forum/topic/161108/llwinvncom
https://sciencemission.com/profile/llwinvncom
https://malt-orden.info/userinfo.php?uid=464973
https://egl.circlly.com/users/llwinvncom
https://www.trackyserver.com/profile/254841
https://theafricavoice.com/profile/llwinvncom
https://audiomack.com/llwinvncom
https://raovat.nhadat.vn/members/llwinvncom-316960.html
https://www.hyperlabthailand.com/forum/topic/817861/llwinvncom
https://seomotionz.com/member.php?action=profile&uid=135169
https://freeimage.host/llwinvncom
https://www.nongkhaempolice.com/forum/topic/148976/llwinvncom
https://swat-portal.com/forum/wcf/user/52287-llwinvncom/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=147108
https://www.video-bookmark.com/bookmark/7139948/llwin/
https://www.newgenstravel.com/forum/topic/51781/llwinvncom
https://posteezy.com/llwin
https://belgaumonline.com/profile/llwinvncom/
https://www.magcloud.com/user/llwinvncom
https://www.lwn3d.com/forum/topic/71000/llwinvncom
https://chillspot1.com/user/llwinvncom
https://pixelfed.uno/llwinvncom
http://freestyler.ws/user/661405/llwinvncom
https://www.freelistingusa.com/listings/llwin-24
https://forum.epicbrowser.com/profile.php?section=personal&id=159276
https://www.thitrungruangclinic.com/forum/topic/148977/llwinvncom
https://www.tizmos.com/llwinvncom?folder=Home
https://nicheless.blog/author/llwin-1
https://official.link/llwinvncom
https://www.renderosity.com/users/id:1862387
https://www.giveawayoftheday.com/forums/profile/1881240
https://expatguidekorea.com/profile/llwinvncom/
https://latinverge.com/profile/40059?tab=541
https://4irdeveloper.com/index.php/forums/view_forumtopic_details/60512
https://shorturl.ly/zTOCB
https://snippet.host/uqfsun
https://sfx.thelazy.net/users/u/llwinvncom/
https://scrapbox.io/llwinvncom/LLWIN
https://l2top.co/forum/members/llwinvncom.184975/
https://www.navacool.com/forum/topic/444576/llwinvncom
https://unityroom.com/users/ce4g0fd8y1oajs7q9uxw
https://backloggery.com/llwinvncom
https://protocol.ooo/ja/users/llwinvncom
https://www.annuncigratuititalia.it/author/llwinvncom/
https://forum.delftship.net/Public/users/llwinvncom/
https://www.simplexthailand.com/forum/topic/30168/llwinvncom
https://allmyfaves.ca/llwinvncom
https://pets4friends.com/profile-1608783
https://sciter.com/forums/users/llwinvncom/
https://www.natthadon-sanengineering.com/forum/topic/120591/llwinvncom
https://guestboard.co/events/llwin-1/details#show-features
https://dentaltechnician.org.uk/community/profile/llwinvncom/
https://www.ybookmarking.com/user/dgAZHkqRcCgF
https://egamerprofile.com/player/llwinvncom
https://www.passes.com/llwinvncom
https://webcamscenter.com/user/llwinvncom
https://www.ttlxshipping.com/forum/topic/444577/llwinvncom
https://marshmallow-qa.com/c4ru7x3teu4kn5g
https://www.freewebmarks.com/user/xFBa9GeDBvaR
https://nonon-centsnanna.com/members/llwinvncom/
https://mysound.ge/profile/llwinvncom
https://xmrbazaar.com/user/llwinvncom/
https://lankadevelopers.lk/user/llwinvncom1
https://www.bestloveweddingstudio.com/forum/topic/95322/llwinvncom
https://jpeg.ly/Jewu4
https://www.democracylab.org/user/44445
https://www.xen-factory.com/index.php?members/llwinvncom.163803/#about
https://user.linkdata.org/user/llwinvncom/work
https://spoutible.com/llwinvncom
https://act4sdgs.org/profile/llwin_9
https://cboj.ca/user/llwinvncom
https://www.pesteam.it/forum/members/llwinvncom.97670/#about
https://simblr.cc/user/8680-llwinvncom/
https://link4u.cc/@llwinvncom
https://vote.easypolls.net/6a1126d5de4083005f4ca79d
https://bbs.superbuy.com/forum.php?mod=viewthread&tid=778789&extra=
https://bwinglive.lighthouseapp.com/users/2000593
https://triumph.srivenkateshwaraa.edu.in/profile/llwinvncom
https://zimexapp.co.zw/llwinvncom
https://devpost.com/llwinvncom
https://jerseyboysblog.com/forum/member.php?action=profile&uid=99552
https://ibit.ly/WIKnp
https://www.letsdobookmark.com/user/ql7NPyCL2VXy
http://gojourney.xsrv.jp/index.php?llwinvncom
https://walling.app/b7JiQpnoSa3cVl8aE7cs/llwin
http://jobboard.piasd.org/author/llwinvncom/
https://coolors.co/u/llwinvncom
https://www.diigo.com/item/note/bulnt/sxpy?k=39e241f683c3c952f27de4289e8e2d8e
https://qiita.com/llwinvncom
https://poipiku.com/13698506/
https://www.socialbookmarkssite.com/bookmark/6261315/llwin/
https://stepik.org/users/1287772090
https://tinyurl.com/llwinvncom
https://hype4.academy/profile/llwinvncom
https://mikropragmata.lifo.gr/meli/llwinvncom/profile/
https://niflheim.world/members/llwinvncom.55768/about
https://www.townscript.com/o/llwinvncom-200232
https://t.ly/jWPz0
https://www.mecanique-bateau.com/community/profile/llwinvncom
https://about.me/llwinvncom
https://www.bonback.com/forum/topic/444723/llwinvncom
https://www.freelistinguk.com/listings/llwin
https://www.freelistingindia.in/listings/llwin
https://www.diggerslist.com/llwinvncom/about
http://www.brenkoweb.com/user/93593/profile
https://forum-foxess.pro/community/profile/llwinvncom/
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=474765&sid=585f3e9ddd2f8a13689d9bfecb22a2fb
https://jali.me/llwinvncom
https://jaga.link/llwinvncom
https://biolinku.co/llwinvncom
https://bioqoo.com/llwinvncom
https://qoolink.co/llwinvncom
https://ngel.ink/llwinvncom
https://doodleordie.com/profile/llwinvncom
https://app.readthedocs.org/profiles/llwinvncom/
https://disqus.com/by/disqus_CblaQ9wphy/about/
https://www.mixcloud.com/llwinvncom/
https://www.speedrun.com/users/llwinvncom
https://leetcode.com/u/llwinvncom/
https://hub.docker.com/u/llwinvncom
https://gifyu.com/llwinvncom
https://justpaste.it/u/LLWIN7
https://uiverse.io/profile/llwinvncom_7116
https://www.skypixel.com/users/djiuser-bykophpihgab
http://www.genina.com/user/editDone/5374462.page
https://skitterphoto.com/photographers/2769117/llwin
https://www.skool.com/@ll-win-2752
https://www.adpost.com/u/mistyakhter3662/
https://photouploads.com/llwinvncom
https://feyenoord.supporters.nl/profiel/154456/llwinvncom
https://dreevoo.com/profile.php?pid=1727928
https://techplanet.today/member/llwinvncom
https://www.scener.com/@llwinvncom
https://www.vid419.com/home.php?mod=space&uid=3491755
https://pumpyoursound.com/u/user/1626653
https://mygamedb.com/profile/mistyakhter3662
https://onespotsocial.com/llwinvncom
https://akniga.org/profile/1427852-llwin
https://www.longisland.com/profile/llwinvncom
http://palangshim.com/space-uid-5202222.html
https://lifeinsys.com/user/llwinvncom
https://devfolio.co/@llwinvncom
https://pantip.com/profile/9356039
https://tutorialslink.com/member/llwinvncomundefined/103175
https://circleten.org/a/409581?postTypeId=whatsNew
https://partecipa.poliste.com/profiles/llwinvncom/activity
https://forum.aigato.vn/user/llwinvncom
https://wikifab.org/wiki/Utilisateur:Llwinvncom
https://www.udrpsearch.com/user/llwinvncom
https://www.fitlynk.com/83423ae9e
https://teratail.com/users/llwinvncom
https://topkif.nvinio.com/llwinvncom
https://www.claimajob.com/profiles/8317445-llwin
https://www.pozible.com/profile/llwin-28
https://elovebook.com/llwinvncom
https://pastebin.com/u/llwinvncom
https://zeroone.art/profile/llwinvncom
https://galgame.dev/user/llwinvncom
https://gourmet-calendar.com/users/llwinvncom
https://www.iniuria.us/forum/member.php?685137-llwinvncom
https://smartprogress.do/goal/436265/
https://hcgdietinfo.com/hcgdietforums/members/llwinvncom/
https://bandori.party/user/1034816/llwinvncom/
https://www.blackhatprotools.info/member.php?293613-llwinvncom
https://acomics.ru/-llwinvncom
https://armchairjournal.com/forums/users/llwinvncom/
http://fort-raevskiy.ru/community/profile/llwinvncom/
https://imgur.com/user/llwinvncom1/about
https://manylink.co/@llwinvncom
https://xtremepape.rs/members/llwinvncom.678113/#about
https://projectnoah.org/users/llwin-3
https://www.goodreads.com/user/show/201286413-llwin
https://kenhrao.com/members/llwinvncom.123747/#about
https://praca.uxlabs.pl/author/llwinvncom/
https://www.biblegrove.org/profile/meadowchan8205649783/profile
https://www.ganjingworld.com/channel/1iiedge6ibb4WrfCinPzO7QEn1160c?tab=about
https://aboutpharmacistjobs.com/author/llwinvncom/
http://kjtr.grrr.jp/kjtr/?llwinvncom
https://hkgay.net/member.php?action=profile&uid=530243
http://pcsq28.com/home.php?mod=space&uid=2110774
https://jobs.lajobsportal.org/profiles/8318211-llwin
https://www.xiuwushidai.com/home.php?mod=space&uid=2713977
https://hker2uk.com/home.php?mod=space&uid=5594866
https://wall.page/QNgjqM
https://userstyles.world/user/llwinvncom
https://chomikuj.pl/meadowchan820564
https://pastewall.com/sticker/643324ece81e4c25baf46f4d24c35c3c
http://qa.doujiju.com/index.php?qa=user&qa_1=llwinvncom
https://rush1989.rash.jp/pukiwiki/index.php?llwinvncom
https://matters.town/me/drafts/RHJhZnQ6MTcxMjQwOQ
https://tempel.in/view/i8acJG5
https://www.rappad.co/users/llwinvncom
https://www.d3jsp.org/profile.php?mode=viewprofile&u=61786
https://culturesbook.com/llwinvncom
https://www.highpriceddatinguk.com/llwinvncom
https://rnmanagers.com/author/llwinvncom/
https://to-portal.com/llwinvncom
https://dialogluzern.ch/profiles/llwinvncom/activity
https://altacucina.co/profile/llwinvncom
https://freeglobalclassifiedads.com/user/profile/557245
http://iawbs.com/home.php?mod=space&uid=960935
https://searchengines.guru/ru/users/2237967
https://www.squadskates.com/profile/musakond6050509/profile
https://medium.com/@llwinvncom
https://challonge.com/llwinvncom
https://hearthis.at/group/544582/llwinvncom/
https://giphy.com/channel/llwinvncom
https://openwhyd.org/u/6a1121ac2294fc435c116073
https://www.thebostoncalendar.com/user/169792
https://www.questmetaldetectors.com/members-area/musakond608228/profile
https://tinhte.vn/members/llwinvncom.3392621/
https://www.are.na/nha-cai-llwin-liq-yjwlrgq/llwin-qgq8wed6ziy
https://www.atlasobscura.com/users/llwinvncom
https://www.blurb.com/user/llwinvncom?profile_preview=true
https://www.mightycause.com/profile/LLWIN
https://www.noteflight.com/profile/935cb8950da0448406e956cd24efb0bfecaebd50
https://www.ted.com/profiles/51629649
https://luma.com/user/llwinvncom
https://meta.decidim.org/profiles/llwinvncom/activity
https://fairygodboss.com/users/profile/Skc-Hfhjm9/llwinvncom
https://comunitat.canodrom.barcelona/profiles/llwinvncom/activity?locale=en
https://community.atlassian.com/user/profile/1b851085-3f09-48bb-b800-bb68a9986375
https://fyers.in/community/member/1pmLen6HaH
https://findpenguins.com/58nnhehoftbbp
https://www.gamerlaunch.com/community/users/blog/6759499/?mode=view&gid=535
https://chatclub.mn.co/members/39843407
https://dinosquadsuriku.com/?llwinvncom
https://careers.coloradopublichealth.org/profiles/8318453-llwin
https://idol.st/user/179419/llwinvncom/
https://beteiligung.tengen.de/profile/llwinvncom/
https://undrtone.com/llwinvncom
https://hackmd.okfn.de/s/H1RVssR1Me
https://rant.li/ea88csh/
https://aboutcasemanagerjobs.com/author/llwinvncom/
http://mura.hitobashira.org/index.php?llwinvncom
https://barcelonadema-participa.cat/profiles/llwinvncom/activity
https://marshallyin.com/members/llwinvncom/
https://jobs.nefeshinternational.org/employers/4167470-llwin
https://jobs.siliconflorist.com/employers/4167471-llwin
https://jobs.landscapeindustrycareers.org/profiles/8318479-llwin
https://bandsworksconcerts.info/index.php?llwinvncom
https://telegra.ph/LLWIN-05-23-2
https://www.investagrams.com/Profile/llwinv4248648
https://app.talkshoe.com/user/llwinvncom
https://civitai.com/user/llwinvncom
https://zumvu.com/llwinvncom/
https://affariat.com/user/profile/183157
https://pastelink.net/28kh8d0g
https://newdayrp.com/members/llwinvncom.74546/#about
https://vhearts.net/llwinvncom
https://rentry.co/qr26tb8g
https://te.legra.ph/LLWIN-05-23-3
https://activepages.com.au/profile/llwinvncom
https://fliphtml5.com/home/llwinvncom
https://wirtube.de/a/llwinvncom/video-channels
https://f319.com/members/llwinvncom.1114927/
https://expathealthseoul.com/profile/llwinvncom/
https://baskadia.com/user/gwaq
https://m.xtutti.com/user/profile/491703
https://desksnear.me/users/llwin-cbed97
https://talkmarkets.com/profile/nh%C3%A0-c%C3%A1i-llwin-260523-045612
https://www.openrec.tv/user/eur6hc9w6jcflhj8unjg
https://fabble.cc/llwinvncom
https://decidim.santcugat.cat/profiles/llwinvncom/activity
https://experiment.com/users/llwinvncom
https://classificados.acheiusa.com/profile/MDZPNmwrM2laM1VQdzNvS3hkZzh5TDJReXBqSEpNQXI3WE1vNW52SnRDQT0=
https://app.brancher.ai/user/rxZER1z2uj2W
http://delphi.larsbo.org/user/llwinvncom
https://llwinvncom.stck.me/profile
https://nilechronicles.com/profile/llwinvncom
https://londonchinese.com/home.php?mod=space&uid=623637&do=profile
https://hypothes.is/users/llwinvncom
https://forums.alliedmods.net/member.php?u=481474
https://cointr.ee/llwinvncom
https://biomolecula.ru/authors/150908
https://flipboard.social/@llwinvncom
https://aiforkids.in/qa/user/llwinvncom
https://www.aicrowd.com/participants/llwinvncom
https://theamberpost.com/member/llwinvncom
https://tokemonkey.com/afe7f3d5e/activities
https://www.flyingv.cc/users/1459757
https://www.motiondesignawards.com/profile/22434
https://www.inkitt.com/llwinvncom
https://www.arriba420.com/profile/mistyakhter366233190/profile
https://www.gamingtop100.net/server/58094/llwin
https://www.shippingexplorer.net/en/user/llwinvncom/292626
https://www.chordie.com/forum/profile.php?id=2542201
https://tealfeed.com/llwinvncom
https://pxhere.com/en/photographer-me/5024654
https://participa.aytojaen.es/profiles/llwinvncom
https://volleypedia.org/index.php?qa=user&qa_1=llwinvncom
https://fotolibre.social/llwinvncom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=232875
https://participation.touraine.fr/profiles/llwinvncom/activity
https://nhattao.com/members/user6976025.6976025/
https://ncnews.co/profile/llwinvncom1
https://galleria.emotionflow.com/188359/profile.html
https://electroswingthing.com/profile/llwinvncom/
https://pod.beautifulmathuncensored.de/people/7f47f3b0388d013f95da021877951523
https://medibulletin.com/author/llwinvncom/
https://leakedmodels.com/forum/members/llwinvncom.716853/#about
https://chodilinh.com/members/llwinvncom.309735/#about
https://www.laundrynation.com/community/profile/llwinvncom/
https://krachelart.com/UserProfile/tabid/43/userId/1347834/Default.aspx
https://log.concept2.com/profile/2952249
https://espritgames.com/members/51241046/
https://forum.pabbly.com/members/llwinvncom.121541/#about
https://cinderella.pro/user/278885/llwinvncom/#preferences
https://hackmd.io/@vomM5D5sRGegn7_RgT5gjw/B1EkbnA1zg
https://confengine.com/user/llwinvncom
https://doc.interscalar.eu/s/XakdH-pQq
https://forum.risingko.net/members/llwinvncom.86709/#about
https://nhatkythuthuat.com/members/llwinvncom.71130/#about
https://road-to-eden.com/index.php?llwinvncom
https://www.rwaq.org/users/llwinvncom
https://www.siasat.pk/members/llwinvncom.274625/#about
https://hedgedoc.envs.net/s/iROIBFg5C
https://www.dokkan-battle.fr/forums/users/llwinvncom/
https://www.kingmods.net/en/profile/llwinvncom
https://socialsocial.social/user/llwinvncom/
https://www.bookingblog.com/forum/users/llwinvncom/
https://doc.itkonzept.at/s/0syYh6MbW
https://zb3.org/s3myr7gx4s
https://linkdirectorynet.com/listings13590282/llwin
https://www.yourquote.in/llwinvncom-d3qx3/quotes
https://sistacafe.com/user/617128
https://fortunetelleroracle.com/profile/llwinvncom
https://www.invelos.com/UserProfile.aspx?alias=llwinvncom
https://hostndobezi.com/1779501574230423_51980
https://www.brownbook.net/business/55133288/llwin
https://rapidapi.com/user/llwinvncom
https://hashnode.com/@llwinvncom
https://www.speedway-world.pl/forum/member.php?action=profile&uid=489124
https://booklog.jp/users/llwinvncom/profile
https://ffm.bio/bxzkmpq
https://ask.mallaky.com/?qa=user/llwinvncom
https://www.gaiaonline.com/profiles/llwinvncom/51674751/
https://domain.opendns.com/llwinvn.com
https://formulamasa.com/elearning/members/llwinvncom/?v=96b62e1dce57
https://www.growkudos.com/profile/llwinvn_com
https://mathlog.info/users/8rt0P49b5JbW6MgPt1xErcb5q3H3
https://wibki.com/llwinvncom
https://bresdel.com/llwinvncom
https://tabelog.com/rvwr/034204854/prof/
https://backloggd.com/u/llwinvncom/
https://www.reverbnation.com/artist/llwinvncom
https://decide.enguera.es/profiles/llwinvncom/activity
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.llwin5
https://www.royalroad.com/profile/981892
https://filesharingtalk.com/members/638770-llwinvncom
https://zepodcast.com/forums/users/llwinvncom/
https://velog.io/@llwinvncom/about
https://www.rossoneriblog.com/author/llwinvncom/
https://faithlife.com/posts/6339475
https://worstgen.alwaysdata.net/forum/members/llwinvncom.178645/#about
https://www.stylevore.com/user/llwinvncom
https://congdongx.com/thanh-vien/llwinvncom.52339/#about
https://amazingradio.com/profile/llwinvncom
https://www.myget.org/users/llwinvncom
https://vishalbharat.in/llwinvncom
https://makerworld.com/en/@llwinvncom
https://www.frenchwomenorg.com/llwinvncom
https://support.bitspower.com/support/user/llwinvncom
http://forum.cncprovn.com/members/429570-llwinvncom
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=199121
https://camp-fire.jp/profile/llwinvncom
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=508810
https://diit.cz/profil/ruqqaxd2qc/llwinvncom
https://twitback.com/82725d006
https://www.tm-town.com///translators/llwinvncom
https://6a1118f632432.site123.me/
https://thewion.com/llwinvncom
https://shareshortcuts.com/u/llwinvncom/
https://giloo.ist/member/_v60vvab88/?mainTab=notes&subTab=my_notes
https://app.wedonthavetime.org/profile/llwinvncom
https://www.prshine.com/profile/llwinvncom
https://www.retailandwholesalebuyer.com/profile/llwinvncom
https://blogosm.com/profile/llwinvncom
https://logicmastersindia.com/forum/view-profile.asp?action=view&uid=41701
https://zbrushcentral.jp/user/llwinvncom
https://tannda.net/llwinvncom
https://divinguniverse.com/user/llwinvncom
https://www.sakaseru.jp/mina/user/profile/317484
https://janitorai.com/profiles/9d573798-11cd-40da-ac92-125e69d11493_profile-of-llwinvncom
https://www.lookingforjob.co/profile/llwinvncom
https://englishsharedfutures.uk/forums/users/llwinvncom/
https://gamelet.online/user/llwinvncom/about
https://ac.db0.company/user/12972/llwinvncom/
https://bizidex.com/en/llwin-agriculture-963518
https://www.devglan.com/user/public/mistyakhter36624
https://tapas.io/llwinvncom
https://www.awwwards.com/llwinvncom/
https://quomon.es/Profile/llwinvncom/
https://newspicks.com/user/12495966/
https://startupxplore.com/en/services/educational/llwin-3
https://creator.nightcafe.studio/u/llwinvncom
https://qurspiqp.forms.app/
https://www.spoonflower.com/profiles/llwinvncom?sub_action=shop
https://www.atozed.com/forums/user-83164.html
https://allmylinks.com/llwinvncom
https://www.proko.com/@llwinvncom/activity
https://trakteer.id/llwinvncom
https://aoezone.net/members/llwinvncom.191279/#about
https://teletype.in/@llwinvncom
http://app.gxbs.net/home.php?mod=space&uid=1878317
https://racetime.gg/user/5JlzyB7d2Z3V4GED/llwin
https://apptuts.bio/llwin-266778
https://rekonise.com/u/llwinvncom
https://ionpron.net/profile.php?mode=viewprofile&u=1633923
https://timdaily.vn/members/llwinvncom.137847/#about
https://mt2.org/uyeler/llwinvncom.41671/#about
https://www.bandlab.com/llwinvncom
https://findnerd.com/profile/publicprofile/llwinvncom/161005
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=266563
https://quangcaoso.vn/llwinvncom
http://www.biblesupport.com/user/843362-llwinvncom/
http://bbs.medicalforum.cn/home.php?mod=space&uid=2300272
https://www.betmma.tips/mma_handicapper.php?ID=184812
https://www.plotterusati.it/user/llwin-14
https://www.betting-forum.com/members/llwinvncom.163189/#about
https://www.databaze-her.cz/uzivatele/llwinvncom/
http://arahn.100webspace.net/profile.php?mode=viewprofile&u=249114
https://linkmix.co/54981098
https://www.swap-bot.com/user:llwinvncom
http://artutor.teiemt.gr/el/user/llwinvncom/
https://forum.norbrygg.no/members/llwinvncom.152922/#about
https://mez.ink/llwinvncom
https://app.hellothematic.com/creator/profile/1153624
https://illust.daysneo.com/illustrator/llwinvncom/
https://www.deafvideo.tv/vlogger/llwinvncom
https://in.enrollbusiness.com/BusinessProfile/7818161/llwinvncom
https://maxforlive.com/profile/user/llwinvncom?tab=about
https://jobs.westerncity.com/profiles/8318141-llwin
https://www.mateball.com/llwinvncom
https://shootinfo.com/author/llwinvncom/?pt=ads
https://www.halaltrip.com/user/profile/352819/llwinvncom/
https://www.physicsoverflow.org/user/llwinvncom
https://www.bookemon.com/member-home/llwinvncom/1150890
https://spiderum.com/nguoi-dung/llwinvncom
https://www.wantedly.com/id/llwinvncom
https://referrallist.com/profile/llwinvncom
https://guides.co/g/llwinvncom/768915
https://www.xosothantai.com/members/llwinvncom.616422/#info
https://gamejolt.com/@llwinvncom
http://galeria.farvista.net/member.php?action=showprofile&user_id=79706
https://www.completefoods.co/diy/recipes/llwinvncom
http://www.in-almelo.com/users/-llwinvncom
https://codap.concord.org/forums/users/llwinvncom/
https://www.storenvy.com/llwinvncom
https://www.rcuniverse.com/forum/members/llwinvncom.html?simple=1#aboutme
https://bbs.theviko.com/home.php?mod=space&uid=4710388
https://www.huntingnet.com/forum/members/llwinvncom.html?simple=1#aboutme
https://peatix.com/user/29690985/view
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=783443
https://allods.my.games/forum/index.php?page=User&userID=253236
https://circle-book.com/circles/66871
https://forums.maxperformanceinc.com/forums/member.php?u=251036&tab=aboutme&simple=1
https://builtbybit.com/members/llwinvncom.818329/#about
https://amvnews.ru/forum/profile.php?mode=viewprofile&u=106261
https://www.pearltrees.com/llwinvncom/item798066649
https://forum.mbprinteddroids.com/member.php?action=profile&uid=638588
https://www.kwlt.net/profile/llwinvncom/profile
https://postr.yruz.one/profile/llwinvncom
https://magazin.orgsoft.ru/communication/forum/index.php?PAGE_NAME=profile_view&UID=237828
https://forum.tkool.jp/index.php?members/llwinvncom.110462/#about
https://hoaxbuster.com/redacteur/llwinvncom
https://ekcochat.com/llwinvncom
https://www.bark.com/en/gb/company/llwin/ozjNXJ/
https://www.webmastersun.com/members/llwinvncom.166893/#about
https://www.dcfever.com/users/profile.php?id=1279281
https://www.pioneer2.net/community/members/llwinvncom.14711/#about
https://www.question2answer.rexo.top/index.php?qa=user&qa_1=llwinvncom
https://hosted.weblate.org/user/llwinvncom/
https://say.la/llwinvncom
https://www.dailymotion.com/user/llwinvncom
https://slides.com/llwinvncom
https://www.cbmstuff.com/forum/member.php?action=profile&uid=12522
http://www.place123.net/place/llwin0000-h%E1%BB%93-ch%C3%AD-minh-vietnam
https://casualgamerevolution.com/user/llwinvncom
https://photozou.jp/user/top/3454213
https://community.bemeapps.com/user/llwinvncom
https://social.vivaldi.net/@llwinvncom
https://www.gifthero.com/list/c92a8145-0cb0-4fff-8c1e-3662779574f1
https://colorswall.com/users/34489
https://ko-fi.com/llwinvncom
https://community.cisco.com/t5/user/viewprofilepage/user-id/2078864
https://www.designnominees.com/profile/llwin
https://careers.mntech.org/profiles/8318380-llwin
https://aboutnurseassistantjobs.com/author/llwinvncom/
https://diaperedanime.com/forum/member.php?u=76583&tab=aboutme&simple=1
https://www.outdooractive.com/en/member/nha-cai-llwin/341870764/
https://www.wattpad.com/user/llwinvncom
https://xoops.ec-cube.net/userinfo.php?uid=351602
https://www.tractorbynet.com/forums/members/llwinvncom.432113/#about
https://fitinline.com/profile/llwinvncom/about/
https://www.leadworksprojects.com/profile/llwinvncom/profile
https://www.realityofchoice.com/profile/llwinvncom/profile
https://igli.me/llwinvncom
https://www.iglinks.io/llwinvncom-3y7
https://onne.link/llwinvncom
https://www.redbubble.com/people/llwinvncom/shop?anchor=profile&asc=u
https://metaldevastationradio.com/llwinvncom
https://bbarlock.com/index.php/User_talk:Llwinvncom
https://anunt-imob.ro/user/profile/860479
https://anyflip.com/homepage/bszjl#About
https://blender.community/meadow/
https://freeicons.io/profile/935915
https://jobs.suncommunitynews.com/profiles/8318079-meadowchan820564-gmail-com
https://motion-gallery.net/users/985305
https://potofu.me/llwinvncom
https://pubhtml5.com/homepage/dhbws/
https://www.czporadna.cz/user/llwinvncom
https://schoolido.lu/user/llwinvncom/
https://www.moshpyt.com/user/llwinvncom
https://youslade.com/llwinvncom
https://www.freelistingaustralia.com/listings/llwin-12
https://skrolli.fi/keskustelu/users/meadowchan820564/
https://doc.anagora.org/s/IuybzOUcG
https://www.euskalmarket.com/author/llwinvncom/
https://www.fanart-central.net/user/llwinvncom/profile
https://cofacts.tw/user/llwinvncom
https://bookmeter.com/users/1725730
https://www.blockdit.com/llwinvncom
https://www.aersia.net/members/llwinvncom.14061/
https://www.podchaser.com/users/mistyakhter3662
https://buyerseller.xyz/user/llwinvncom/
https://songdew.com/mistyakhter3662gmailcom-178090
https://vozer.net/members/llwinvncom.91616/#about
https://iplogger.org/logger/CALT5mICJWOt/
https://boards.rossmanngroup.com/members/llwinvncom.93709/#about
https://prosinrefgi.wixsite.com/pmbpf/profile/mistyakhter366246953/profile
https://www.horticulturaljobs.com/employers/4167486-llwin
https://www.stephhalllcsw.com/profile/mistyakhter366276030/profile
https://www.guidedground.com/profile/mistyakhter366259418/profile
https://www.null-scripts.net/members/llwinvnco.121534/#about
https://app.roll20.net/users/18008638/orange-travel
https://social.kubo.chat/rajluxmisweets
https://cornucopia.se/author/llwinvncom/
https://www.sonorancareerlink.com/employers/4167501-llwin
https://www.tripadvisor.com/Profile/llwinvncom
https://www.zazzle.ca/mbr/238822118696475819
https://www.madglassmob.com/profile/mistyakhter366218370/profile
https://www.doggies911.com/profile/mistyakhter366239184/profile
https://fnote.me/edit/GQ2RKv?t=true
https://unsplash.com/@llwinvncom
https://definedictionarymeaning.com/user/llwinvncom
https://www.codingame.com/profile/59e4b854620cb883cb3613d59a4162aa4799927
https://www.maanation.com/llwinvncom
https://gitlab.haskell.org/llwinvncom1
https://www.thepartyservicesweb.com/board/board_topic/3929364/8402437.htm
https://japaneseclass.jp/notes/open/115979
https://dawlish.com/user/details/2036a5f8-8016-487f-a1b6-9ed6c50cf628
https://www.australianwinner.com/AuWinner/profile.php?mode=viewprofile&u=llwinvncom
https://iyinet.com/kullanici/llwinvncom.100002/#about
https://hedgedoc.stusta.de/s/93vDHIavp
https://www.bahamaslocal.com/userprofile/1/295407/llwinvncom.html
http://rareconnect.org/en/user/llwinvncom/network
https://www.thesims3.com/myBlog.html?persona=llwinvncom&showBlogMasterPopup=false
https://stackshare.io/meadowchan820564/llwin
https://www.buymusic.club/user/llwinvncom
https://www.myminifactory.com/users/meadowchan
https://www.notebook.ai/users/1363845
https://www.coffeesix-store.com/board/board_topic/7560063/8402462.htm
https://www.telix.pl/profile/llwinvncom/
https://mantis.batterystaplegames.com/view.php?id=8095
https://tlcworld.it/forum/members/llwinvncom.38330/#about
https://remoteok.com/@llwinvncom
https://www.leetchi.com/fr/c/llwin-4903134?utm_source=copylink&utm_medium=social_sharing
https://scenarch.com/userpages/38311
https://hubb.link/llwinvncom/
https://www.joomla51.com/forum/profile/105504-llwinvncom
https://beteiligung.amt-huettener-berge.de/profile/llwinvncom/
https://writexo.com/share/79629ae4f981
https://www.wvhired.com/profiles/8318094-llwin
https://savelist.co/my-lists/users/llwinvncom
https://doselect.com/@f15add7f241b4eab5f05146c3
https://naijamatta.com/llwinvncom
https://medibang.com/author/28376530/
https://zzb.bz/WKFsNV
https://papers-please.info/?llwinvncom
https://recash.wpsoul.net/members/llwinvncom/profile/
https://www.heavyironjobs.com/profiles/8318107-llwin
https://chyoa.com/user/llwinvncom
https://jobs.windomnews.com/profiles/8318111-llwin
https://iszene.com/user-354281.html
https://www.checkli.com/llwinvncom#/a/process
https://beteiligung.hafencity.com/profile/llwinvncom/
https://paper.wf/llwinvncom/pa-href-llwinvn-com-target-blank-rel-nofollowllwin-aandnbsp-thu-handuacute-t
https://forum.issabel.org/u/llwinvncom
http://jobs.emiogp.com/author/llwinvncom
https://forum.skullgirlsmobile.com/members/llwinvncom.227130/#about
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=307591
http://www.muzikspace.com/profiledetails.aspx?profileid=143439
https://topsitenet.com/profile/llwinvncom/1839756/
https://axe.rs/forum/members/llwinvncom.13434118/#about
https://help.orrs.de/user/llwinvncom
https://vnbit.org/members/llwinvncom.110178/#about
https://codimd.communecter.org/s/Thl2uUufQ
https://jobs.host-panel.com/author/llwinvncom/
https://destaquebrasil.com/saopaulo/author/llwinvncom/
https://willysforsale.com/author/llwinvncom/
https://kktix.com/user/8994413
https://pub41.bravenet.com/forum/static/show.php?usernum=3501574107&frmid=26&msgid=1037297&cmd=show
https://www.finders-english.com/profile/meadowchan82056452415/profile
https://www.klynt.net/members/llwinvncom/
https://www.ad-links.org/https://llwinvncom/_375533.html
https://www.beegdirectory.com/https://llwinvncom/_495527.html
https://apk.tw/space-uid-7340436.html
https://www.bat-safe.com/profile/meadowchan82056424308/profile
https://www.kidsofagape.com/profile/meadowchan8205645830/profile
https://www.veteranscup.org/profile/meadowchan82056492437/profile
https://www.saltlakeladyrebels.com/profile/meadowchan82056453334/profile
https://www.mexicanmadness.com/profile/meadowchan82056450481/profile
https://www.aquarius-dir.com/https://llwinvncom/_521356.html
https://www.apeopledirectory.com/https://llwinvncom/_419308.html
https://www.bedirectory.com/https://llwinvncom/_452985.html
https://www.interesting-dir.com/details.php?id=445291
https://www.addirectory.org/details.php?id=482961
https://www.alive-directory.com/https://llwinvncom/_728648.html
https://www.ecodir.net/https://llwinvncom/_341227.html
https://www.ask-dir.org/https://llwinvncom/_386863.html
https://uno-en-ligne.com/profile.php?user=426767
https://skeptikon.fr/a/llwinvncom/video-channels
https://www.craigslistdir.org/https://llwinvncom/_417067.html
https://www.macke-bornauw.com/profile/meadowchan82056420878/profile
https://jsfiddle.net/qaoscfkw/
https://www.free-weblink.com/https://llwinvncom/_280360.html
https://bbs.airav.cc/home.php?mod=space&uid=4650931
http://www.jbt4.com/home.php?mod=space&uid=8673699
https://git.disroot.org/llwinvncom
https://dutrai.com/members/llwinvncom.37758/#about
https://anotepad.com/notes/fwbr445k
https://aboutnursepractitionerjobs.com/author/llwinvncom/
https://chaloke.com/forums/users/llwinvncom/
http://nao.earth/index.php?llwinvncom
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6557336
https://paste.lightcast.com/view/9bba126a
https://www.housedumonde.com/profile/meadowchan82056460962/profile
https://www.harimajuku.com/profile/meadowchan82056496494/profile
https://www.ltstesting.com/profile/meadowchan82056484516/profile
https://www.happycampersmontessori.com/profile/meadowchan82056477609/profile
https://aboutsnfjobs.com/author/llwinvncom/
https://sub4sub.net/forums/users/llwinvncom/
https://github.com/llwinvncom
https://tudomuaban.com/chi-tiet-rao-vat/2915781/llwinvncom.html
https://www.france-ioi.org/user/perso.php?sLogin=llwinvncom
https://etextpad.com/i1tmaymgkn
https://pixabay.com/users/llwinvncom-55989404/
https://linqto.me/about/llwinvncom
http://newdigital-world.com/members/llwinvncom.html
https://ofuse.me/e/372632
https://www.walkscore.com/people/194220263671/llwin
https://kumu.io/llwinvncom/llwin#untitled-map
https://aphorismsgalore.com/users/llwinvncom
https://transfur.com/Users/llwinvncom
https://aprenderfotografia.online/usuarios/llwinvncom/profile/
https://activeprospect.fogbugz.com/default.asp?168055_ub2b3u93
https://forums.megalith-games.com/member.php?action=profile&uid=1471030
https://jobs.echinacities.com/user/center/blog_detail/2689138/27100
https://producerbox.com/users/llwinvncom
https://collectednotes.com/llwinvncom/unknown/
https://forum.ircam.fr/profile/llwinvncom/
https://muare.vn/shop/llwinvncom/906600
https://wefunder.com/llwinvncom
https://www.printables.com/@llwinvncom_4888777
https://edabit.com/user/mEuwR8t2bsyM6Lw68
https://www.mynbest.info/profile/mistyakhter366236872/profile
https://gesoten.com/profile/detail/12872539
https://suzuri.jp/llwinvncom
https://www.producthunt.com/@llwinvncom
https://participationcitoyenne.rillieuxlapape.fr/profiles/llwinvncom/activity
https://www.luzsantomauro.com/profile/mistyakhter366211128/profile
https://morguefile.com/creative/llwinvncom
https://participer.loire-atlantique.fr/profiles/llwinvncom/activity
https://www.dek-o-block.com/profile/mistyakhter366266799/profile
https://myanimelist.net/profile/llwinvncom1
https://co-roma.openheritage.eu/profiles/llwinvncom/activity
https://dynamicscommunities.com/community/members/mistyakhter3662gmail-com/
https://gratisafhalen.be/author/llwinvncom/
https://bsky.app/profile/llwinvncom.bsky.social
https://coub.com/llwinvncom
https://3dwarehouse.sketchup.com/user/279c6846-b906-40bb-bdae-d1408029d9ca
https://biiut.com/llwinvncom
https://www.jointcorners.com/llwinvncom
https://substack.com/@llwinvncom
https://www.clickasnap.com/profile/llwinvncom
https://jobs.tdwi.org/employers/4168200-llwin
https://all4.vip/p/page/view-persons-profile?id=127365
https://inkbunny.net/llwinvncom
https://routinehub.co/user/Resourceful-Bear-2605
http://belobog1.freehostia.com/phpBB2/profile.php?mode=viewprofile&u=214811
https://www.foriio.com/llwinvncom
https://www.mymeetbook.com/llwinvncom
https://www.aseeralkotb.com/ar/profiles/llwinvncom-106377569164332061590
https://slackcommunity.com/u/mvaw33/#/about
https://www.watershedwellness.net/profile/llwinvncom/profile
https://foss.heptapod.net/llwinvncom
https://sketchersunited.org/users/325402
https://gitea.com/llwinvncom
https://maphub.net/llwinvncom
https://code.datasciencedojo.com/google_106377569164332061590
https://protospielsouth.com/user/137899
https://gitlab.com/llwinvncom
https://coinfolk.net/user/llwinvncom
https://v.gd/create.php
https://runtrip.jp/courses/tokyo/13101/51542
https://www.futurelearn.com/profiles/23184973
https://www.rcmx.net/userinfo.php?uid=18965
https://www.c8ke.co/influencer/onboarding/index.html
https://phatwalletforums.com/user/llwinvncom
https://ctxt.io/2/AAAEDEhQFA
https://www.mapleprimes.com/users/llwinvncom
https://divisionmidway.org/jobs/author/llwinvncom/
https://swdteam.com/profile/llwinvncom
https://www.racerjobs.com/employers/4168232-llwin
https://www.dibiz.com/mistyakhter3662
https://www.weddingbee.com/members/llwinvncom/
http://xline.vc/index.php?llwinvncom
https://fact-finder.xyz/pukiwiki/?llwinvncom
https://line-monsterfarm.wiki/?llwinvncom
https://dq10wiki.net/wiki/?llwinvncom
https://gpd.wiki/index.php?llwinvncom
https://sf6wiki.com/?llwinvncom
https://www.bloggalot.com/profile/llwinvncom
https://orcid.org/0009-0000-6179-2011
https://decidim.calafell.cat/profiles/llwinvncom/activity
https://www.slideshare.net/mistyakhter3662?tab=about
https://controlc.com/72sj1t80
https://filmfreeway.com/llwinvncomNone
https://seedly.sg/profile/llwin/
https://businesslistingplus.com/profile/llwinvncom/
https://thefeedfeed.com/coconut8650
https://www.planetminecraft.com/member/llwinvncom/
https://musikersuche.musicstore.de/profil/llwinvncom/
https://paste.toolforge.org/view/f7a605ec
https://www.davidrio.com/profile/llwinvncom/profile
https://www.claimingthecorner.net/profile/llwinvncom/profile
https://www.lytekids.com/members-area/llwinvncom/profile
https://www.seasidestones.com/profile/llwinvncom/profile
https://www.celsocarvalho.com/profile/llwinvncom/profile
https://letterboxd.com/llwinvncom/
https://virtualdj.com/user/user32645653/index.html
https://aboutnursernjobs.com/author/llwinvncom/
https://failiem.lv/llwinvncom/info
https://www.jigsawplanet.com/llwinvncom
https://myanimeshelf.com/profile/llwinvncom
https://www.themeqx.com/forums/users/llwinvncom/
https://bbs.bee-link.com/u/16820
https://kotob4all.com/profile/llwinvncom
https://findaspring.org/members/llwinvncom/
https://www.abclinuxu.cz/lide/llwinvncom
https://sdelai.ru/members/llwinvncom/
https://www.slmath.org/people/109108
https://www.ibizaclubpt.com/members/llwinvncom.122785/#about
https://www.airportcitygame.com/members/llwinvncom.37453/#about
https://vietcurrency.vn/members/llwinvncom.242716/#about
https://www.hentai-foundry.com/user/llwinvncom/profile
https://forum.dmec.vn/index.php?members/llwinvncom.195794/
https://onlinesequencer.net/forum/user-277639.html
https://thaicpe.com/members/llwinvncom.15198/#about
https://forumton.org/members/llwinvncom.37780/#about
https://www.onetap.com/members/llwinvncom.510732/#about
https://amaz0ns.com/forums/users/llwinvncom/
https://hi-fi-forum.net/profile/1158035
https://longbets.org/user/llwinvncom/
https://www.zubersoft.com/mobilesheets/forum/user-141701.html
https://www.youyooz.com/profile/llwinvncom/
https://www.threadless.com/@llwinvncom/activity
https://xwikiplayground.org/xwiki/bin/view/XWiki/llwinvncom
https://mokum.place/llwinvncom
https://nyccharterschools.jobboard.io/employers/4168211-llwin
https://adhocracy.plus/profile/llwinvncom/
https://monopinion.namur.be/profiles/llwinvncom/activity
https://www.getlisteduae.com/listings/llwin-22
https://vimeo.com/llwinvncom
https://openlibrary.org/people/llwinvncom
https://omiyou.com/llwinvncom
https://forum.cnnr.fr/user/llwinvncom
https://observablehq.com/user/@llwinvncom
https://go.famuse.co/llwinvncom
https://www.buzzfeed.com/llwinvncom
https://www.cameraftp.com/cameraftp/publish/PublicProfile.aspx/UserID79925932
https://writeupcafe.com/author/55ddappnet
https://www.globalbusinesslisting.org/llwin-10
https://archive.org/details/@llwinvncom
https://www.remotehub.com/llwinvncom
https://forum.uookle.com/home.php?mod=space&uid=1494375
https://www.funsocio.com/llwinvncom
https://www.thetriumphforum.com/members/llwinvncom.67433/
https://www.jmriascos.space/profile/llwinvncom/profile
https://onlyfans.com/llwinvncom
https://www.healthleadershipbraintrust.com/profile/llwinvncom/profile
https://www.goodolcomics.com/blog/profile/llwinvncom
https://outdoor.surselva.info/en/member/nha-cai-llwin/341870764/
https://www.floodzonebrewery.com/profile/llwinvncom/profile
https://bkk.tips/forums/users/llwinvncom
https://www.bridgescdc.com/profile/llwinvncom/profile
https://www.leonidastacticalss.com/profile/llwinvncom/profile
https://turcia-tours.ru/forum/profile/llwinvncom
https://lospec.com/llwinvncom
http://linoit.com/users/55ddappnet/canvases/LLWIN
https://www.mindomo.com/mindmap/b4db173b9fbf4102a50b3db7050dad87
https://www.aipictors.com/en/users/c21cc426-2bef-8eeb-1ed2-809aa7a0ff04
http://tkdlab.com/wiki/index.php?llwinvncom
https://fairebruxellessamen.be/profiles/llwinvncom
https://radio.immo/user/1-7977-LLWIN
https://www.insanelymac.com/forum/profile/2750811-llwinvncom/?tab=field_core_pfield_13
https://www.fullhires.com/author/llwinvncom/
https://www.japaaan.com/user/82392
https://www.40billion.com/profile/212086518
https://brain-market.com/u/llwinvncom
https://market360.vn/page/78053
https://atthehive.com/user/llwinvncom/
https://www.rueanmaihom.net/forum/topic/111168/llwin
https://www.skillshot.pl/users/27392
https://rumble.com/user/llwinvncom/about
https://kick.com/llwinvncom/about
https://mylittlebookmark.com/story7305302/llwin
http://www49.atwiki.org/fateextraccc/index.php?llwinvncom
https://promosimple.com/ps/49cec/https-llwinvn-com
https://roomstyler.com/users/llwinvncom
https://speakerdeck.com/llwinvncom
https://www.yakuza.wiki/?llwinvncom
https://slideslive.com/llwinvncom?tab=about
https://www.scienceuniverse.org/profile/mistyakhter366267542/profile
https://www.chess.com/member/llwinvncom
http://mikraite.559.s1.nabble.com/llwinvncom-td6856.html
https://www.apsense.com/user/llwinvncom
https://listium.com/@llwinvncom
https://www.myvidster.com/profile/mistyakhter3662
https://darksteam.net/direct-messages/llwin.20842/
https://community.silabs.com/s/profile/005Vm00000EOE9p
https://opensea.io/llwinvncom
https://directory4search.com/listings13606249/llwin
https://www.opleague.pro/user/53125-llwinvncom
https://webanketa.com/forms/6mw36e1r60qkcr9q61jkee1m/
https://cannabis.net/user/231969
https://justnock.com/llwinvncom
https://www.experts123.com/portal/u/llwinvncom
https://socialcompare.com/en/member/llwinvncom-8jy95axm
https://pad.karuka.tech.rexo.top/load.php?note=0e4f1cbf
https://pixelfed.tokyo/llwinvncom
https://jali.pro/llwinvncom
https://www.wowonder.xyz/llwinvncom
https://allmyfaves.com/llwinvncom
https://pledgeme.co.nz/profiles/339125
https://b.cari.com.my/home.php?mod=space&uid=3405245&do=profile
https://justpaste.me/Qdk02
https://pimrec.pnu.edu.ua/members/llwinvncom/profile/
https://www.sciencebee.com.bd/qna/user/llwinvncom
http://catalog.drobak.com.ua/communication/forum/user/2852505/
https://fnote.net/notes/4mS2Wb
Saya tidak bisa menahan diri untuk berkomentar
Saya sangat menghargai usaha yang Anda curahkan untuk membuat posting ini. Informasi yang berguna. Terima kasih!
Terima kasih untuk posting hebat lainnya. Di mana lagi seseorang mungkin bisa mendapatkan jenis info seperti itu dengan gaya penulisan yang ideal? Saya punya presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Saya kebetulan menemukan blog Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang luar biasa.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan bersyukur kepada Anda.
Ini adalah topik yang sangat dekat di hati saya, salam, tapi di manakah informasi kontak Anda?
Anda bisa pasti melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Menikmati melihat ini, sangat bagus, terima kasih.
Mengagumi usaha yang Anda curahkan ke website Anda dan informasi mendalam yang Anda tawarkan. Sangat baik menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang fantastis! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Isi yang fantastis! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
Amat hebat info dapat ditemukan di weblog.
Saya melihat banyak website tetapi saya percaya yang satu ini punya sesuatu yang spesial di dalamnya
Saya tidak bisa menahan diri untuk berkomentar
Luar biasa blog yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin menjadi bagian dari kelompok di mana saya bisa mendapatkan umpan balik dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Terima kasih!
I every time spent my half an hour to read this weblog’s posts
daily along with a cup of coffee.
Postingan ini sangat berguna. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di situs saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke blog saya?
Saya senang menjadi pengunjung dari weblog murni ini!, salam atas informasi langka ini!
Saya selalu peduli dengan topik ini dan tetap masih demikian, terima kasih telah memposting.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Hebat. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami kerja keras Anda.
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Ini adalah topik yang sangat dekat di hati saya, salam, tapi di manakah detail kontak Anda?
Hai, saya hanya ingin mengatakan bahwa saya sangat menikmati membaca postingan blog Anda. Ini adalah persis jenis informasi yang saya cari. Saya akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Terima kasih atas tulisan yang baik. Faktanya ini sebelumnya adalah sebuah akun hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Terima kasih atas tulisan yang baik. Faktanya ini dulunya adalah sebuah akun hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Howdy! I’m at work browsing your blog from my
new iphone 4! Just wanted to say I love reading through your blog and
look forward to all your posts! Keep up the fantastic work!
Menghargai dedikasi yang Anda curahkan ke website Anda dan informasi terperinci yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Terima kasih, saya baru saja menelusuri informasi sekitar subjek ini cukup lama dan milik Anda adalah yang terbaik yang saya ketahui hingga sekarang. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang asal tersebut?
Rattling nice pattern and great subject material, nothing at all else we require :D.
Spot on with this write-up, I actually think this website needs far more consideration. I’ll in all probability be again to learn far more, thanks for that info.
you’re really a good webmaster. The site loading speed is incredible. It seems that you’re doing any unique trick. Moreover, The contents are masterwork. you’ve done a excellent job on this topic!
Heya are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and set up my own. Do you require any coding knowledge to make your own blog? Any help would be greatly appreciated!
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
I will right away grab your rss feed as I can’t find your email subscription link or newsletter service. Do you’ve any? Please let me know in order that I could subscribe. Thanks.
I was recommended this website by way of my cousin. I’m not sure whether or not this put up is written by way of him as no one else recognize such certain about my difficulty. You are amazing! Thanks!
Wow that was strange. I just wrote an really long comment but after I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyway, just wanted to say wonderful blog!
Good, I should definitely pronounce, impressed with your website. I had no trouble navigating through all tabs as well as related info ended up being truly easy to do to access. I recently found what I hoped for before you know it in the least. Quite unusual. Is likely to appreciate it for those who add forums or anything, web site theme . a tones way for your client to communicate. Excellent task.
Nice post. I learn something more challenging on different blogs everyday. It will always be stimulating to read content from other writers and practice a little something from their store. I’d prefer to use some with the content on my blog whether you don’t mind. Natually I’ll give you a link on your web blog. Thanks for sharing.
This website online can be a stroll-through for the entire information you needed about this and didn’t know who to ask. Glimpse here, and you’ll undoubtedly uncover it.
I enjoy what you guys are up too. This sort of clever work and coverage! Keep up the very good works guys I’ve incorporated you guys to our blogroll.
whoah this blog is magnificent i really like studying your articles. Stay up the good paintings! You understand, a lot of people are hunting around for this info, you can help them greatly.
Very efficiently written post. It will be supportive to anybody who employess it, as well as yours truly :). Keep up the good work – i will definitely read more posts.
Currently it seems like BlogEngine is the preferred blogging platform out there right now. (from what I’ve read) Is that what you are using on your blog?
I like the helpful info you provide in your articles. I’ll bookmark your weblog and check again here regularly. I am quite sure I will learn plenty of new stuff right here! Good luck for the next!
I am often to blogging and i really appreciate your content. The article has really peaks my interest. I am going to bookmark your site and keep checking for new information.
I’ve been exploring for a bit for any high quality articles or blog posts on this kind of area . Exploring in Yahoo I eventually stumbled upon this web site. Studying this information So i am satisfied to convey that I have an incredibly excellent uncanny feeling I found out just what I needed. I most unquestionably will make certain to do not omit this site and give it a look on a relentless basis.
naturally like your web site but you need to check the spelling on quite a few of your posts. A number of them are rife with spelling problems and I find it very troublesome to tell the truth nevertheless I’ll certainly come back again.
Hi! This is kind of off topic but I need some help from an established blog. Is it difficult to set up your own blog? I’m not very techincal but I can figure things out pretty fast. I’m thinking about setting up my own but I’m not sure where to start. Do you have any tips or suggestions? With thanks
Good write-up, I’m normal visitor of one’s site, maintain up the nice operate, and It is going to be a regular visitor for a lengthy time.
I’ve recently started a site, the info you provide on this website has helped me tremendously. Thanks for all of your time & work.
I just couldn’t go away your site before suggesting that I actually loved the usual information an individual provide for your visitors? Is gonna be back often in order to inspect new posts.
Along with the whole thing which seems to be building throughout this particular subject matter, a significant percentage of viewpoints happen to be rather exciting. Nonetheless, I am sorry, because I can not subscribe to your entire idea, all be it refreshing none the less. It looks to everyone that your commentary are generally not completely justified and in actuality you are generally yourself not thoroughly confident of the point. In any event I did appreciate examining it.
Hi, i feel that i noticed you visited my blog thus i got here to “go back the choose”.I’m trying to in finding things to enhance my site!I guess its adequate to make use of a few of your ideas!!
Hore google adalah penguasa dunia saya yang menolong saya menemukan web site yang luar biasa! .
Saya tidak umumnya berkomentar tetapi saya harus mengakui hargai untuk posting yang satu ini : D.
I’ve read some excellent stuff here. Definitely price bookmarking for revisiting. I surprise how so much attempt you set to make such a magnificent informative site.
Hore google adalah ratu saya yang membantu saya menemukan situs yang luar biasa! .
Hey! I’m at work browsing your blog from my new iphone 4! Just wanted to say I love reading through your blog and look forward to all your posts! Carry on the great work!
Saya terkesan dengan situs ini, amat saya adalah penggemar.
I always was concerned in this subject and stock still am, appreciate it for putting up.
excellent put up, very informative. I’m wondering why the opposite specialists of this sector don’t understand this. You must continue your writing. I’m confident, you have a great readers’ base already!
Hebat situs yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan masukan dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Terima kasih banyak!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di mana informasi kontak Anda?
That is the suitable blog for anybody who wants to find out about this topic. You understand so much its nearly exhausting to argue with you (not that I truly would need…HaHa). You definitely put a new spin on a topic thats been written about for years. Great stuff, just great!
Great site! I am loving it!! Will be back later to read some more. I am bookmarking your feeds also
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
Terima kasih untuk posting hebat yang lain. Di mana lagi siapa pun mungkin bisa mendapatkan tipe info seperti itu dengan cara penulisan yang ideal? Saya memiliki presentasi minggu berikutnya, dan saya sedang dalam pencarian informasi seperti ini.
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
Thanks a bunch for sharing this with all of us you actually know what you are talking about! Bookmarked. Kindly also visit my web site =). We could have a link exchange agreement between us!
Good post. I be taught something tougher on totally different blogs everyday. It’s going to at all times be stimulating to read content material from other writers and follow just a little one thing from their store. I’d choose to use some with the content on my weblog whether or not you don’t mind. Natually I’ll offer you a hyperlink on your web blog. Thanks for sharing.
I was just looking for this info for a while. After six hours of continuous Googleing, at last I got it in your web site. I wonder what is the lack of Google strategy that do not rank this kind of informative websites in top of the list. Normally the top web sites are full of garbage.
Nyata baik info dapat ditemukan di web site.
Wow! Terima kasih! Saya senantiasa membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke situs saya?
Very interesting details you have noted, thankyou for posting. “Jive Lady Just hang loose blood. She gonna handa your rebound on the med side.” by Airplane.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Thankyou for helping out, wonderful info .
I simply couldn’t go away your website before suggesting that I actually enjoyed the standard information an individual provide to your visitors? Is gonna be again frequently to inspect new posts
Greetings from Idaho! I’m bored at work so I decided to check out your blog on my iphone during lunch break. I love the knowledge you present here and can’t wait to take a look when I get home. I’m surprised at how fast your blog loaded on my cell phone .. I’m not even using WIFI, just 3G .. Anyhow, very good blog!
Wow, hebat weblog tata letak! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan web site Anda sangat baik, serta kontennya!
Hei, saya hanya ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini merupakan persis tipe informasi yang saya cari. Saya akan merekomendasikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Hmm it seems like your blog ate my first comment (it was extremely long) so I guess I’ll just sum it up what I submitted and say, I’m thoroughly enjoying your blog. I too am an aspiring blog writer but I’m still new to everything. Do you have any helpful hints for inexperienced blog writers? I’d certainly appreciate it.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Hello just wanted to give you a quick heads up. The words in your article seem to be running off the screen in Safari. I’m not sure if this is a format issue or something to do with internet browser compatibility but I figured I’d post to let you know. The style and design look great though! Hope you get the issue resolved soon. Thanks
I was reading some of your blog posts on this internet site and I believe this internet site is rattling instructive! Continue posting.
Very interesting information!Perfect just what I was looking for!
You could definitely see your skills in the work you write. The world hopes for even more passionate writers like you who aren’t afraid to say how they believe. Always follow your heart.
Ini benar-benar menjawab masalah saya, terima kasih!
Saya senang menjadi salah satu pengunjung di situs web hebat ini (:, terima kasih telah memposting.
Only wanna remark on few general things, The website design is perfect, the content is really excellent. “By following the concept of ‘one country, two systems,’ you don’t swallow me up nor I you.” by Deng Xiaoping.
I’ve been exploring for a bit for any high quality articles or blog posts in this sort of house . Exploring in Yahoo I finally stumbled upon this website. Studying this information So i’m glad to show that I’ve an incredibly excellent uncanny feeling I came upon exactly what I needed. I such a lot indisputably will make certain to do not fail to remember this website and give it a glance on a constant basis.
Hai di sana, hanya ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan cukup banyak wawasan yang sangat berguna. Terima kasih!
Regards for this post, I am a big fan of this site would like to continue updated.
Anda dapat jelas melihat keahlian Anda di dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Thanks a bunch for sharing this with all of us you actually know what you’re talking about! Bookmarked. Kindly also visit my site =). We could have a link exchange contract between us!
whoah this blog is magnificent i love reading your articles. Keep up the great work! You know, many people are looking around for this information, you can aid them greatly.
Appreciating the hard work you put into your site and detailed information you present. It’s good to come across a blog every once in a while that isn’t the same outdated rehashed material. Wonderful read! I’ve saved your site and I’m adding your RSS feeds to my Google account.
Yeah bookmaking this wasn’t a high risk conclusion great post! .
Informasi yang bermanfaat. Saya baru menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Greetings from Idaho! I’m bored to death at work so I decided to check out your website on my iphone during lunch break. I enjoy the knowledge you provide here and can’t wait to take a look when I get home. I’m surprised at how quick your blog loaded on my cell phone .. I’m not even using WIFI, just 3G .. Anyhow, great site!
Postingan ini sangat informatif. Saya menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
I like the helpful information you provide in your articles.
I will bookmark your blog and check again here frequently.
I’m quite sure I’ll learn many new stuff right here!
Good luck for the next!
Berharga informasi. Beruntung saya menemukan website Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Just what I was searching for, appreciate it for posting.
Hai di sana, hanya ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa banyak informasi yang bermanfaat. Terima kasih!
Thanks for the sensible critique. Me & my neighbor were just preparing to do some research on this. We got a grab a book from our local library but I think I learned more from this post. I am very glad to see such excellent information being shared freely out there.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Saya senang menjadi pengunjung dari situs web total ini!, sangat dihargai atas informasi langka ini!
At this time it appears like Expression Engine is the best blogging
platform out there right now. (from what I’ve read) Is that what you are using on your blog?
Your comment is awaiting moderation.
dog house slot
https://dog-house.sbs
dog house megaways игровой автомат на iphone
https://dog-house.sbs
the dog house сайт
https://dog-house.sbs
dog house demo megaways дог хаус слот
https://dog-house.sbs
the dog house megaways играть онлайн
https://dog-house.sbs
dog-house.sbs
Hari ini, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Terima kasih atas tulisan yang baik. Sebenarnya ini dulunya adalah sebuah materi hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berhubungan?
Saya menghargai usaha yang Anda curahkan untuk menyusun artikel ini. Konten yang sangat berharga. Terima kasih banyak!
Ini adalah blog yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
I conceive this web site has got very good pent written content content.
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You obviously know what youre talking about, why waste your intelligence on just posting videos to your blog when you could be giving us something enlightening to read?
Saya mendapatkan info yang bagus dari blog Anda.
F*ckin’ amazing things here. I am very glad to see your article. Thanks a lot and i am looking forward to contact you. Will you kindly drop me a e-mail?
Normally I do not learn article on blogs, but I would like to say that this write-up very forced me to check out and do so! Your writing style has been amazed me. Thank you, very great post.
Artikel yang sangat berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi.
Thank you for another informative web site. Where else could I get that type of info written in such a perfect way? I have a project that I’m just now working on, and I’ve been on the look out for such info.
Saya tidak benar-benar mahir dalam bahasa Inggris tetapi saya menemukan ini amat ringan untuk dipahami.
Terima kasih banyak atas artikel yang sangat baik. Saya benar-benar menyukai membaca ini dan menemukan banyak sekali informasi yang bermanfaat. Teruskan pekerjaan yang bagus!
I’ve read several good stuff here. Certainly value bookmarking for revisiting. I surprise how a lot attempt you place to make any such magnificent informative website.
Bagaimanapun, terima kasih untuk artikel yang istimewa ini dan walaupun saya tidak sepakat sepenuhnya, saya menilai sudut pandang.
WOW just what I was searching for. Came here
by searching for scammer site
Farming setup on nomiswap — stake LP tokens, monitor NMX rewards, claim threshold logic, compound cycle — practical nomiswap yield workflow.
Very instructive and superb anatomical structure of written content, now that’s user pleasant (:.
Farming setup on nomiswap — stake LP tokens, monitor NMX rewards, claim threshold logic, compound cycle — practical nomiswap yield workflow.
Enjoyed reading through this, very good stuff, appreciate it. “Golf isn’t a game, it’s a choice that one makes with one’s life.” by Charles Rosin.
Stableswap pool advantages on how to use nomiswap — low-slippage swaps, capital efficiency, peg-stability pairs — beginner-friendly nomiswap intro for stablecoin holders.
Isi yang fantastis! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
An impressive share, I just given this onto a colleague who was doing a little analysis on this. And he in fact bought me breakfast because I found it for him.. smile. So let me reword that: Thnx for the treat! But yeah Thnkx for spending the time to discuss this, I feel strongly about it and love reading more on this topic. If possible, as you become expertise, would you mind updating your blog with more details? It is highly helpful for me. Big thumb up for this blog post!
Wow! Terima kasih! Saya secara terus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke blog saya?
Ini adalah topik yang sangat dekat di hati saya, cheers, tapi di manakah informasi kontak Anda?
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Very interesting topic, regards for posting. “The reason people sweat is so they won’t catch fire when making love.” by Don Rose.
It’s hard to find knowledgeable people on this topic, but you sound like you know what you’re talking about! Thanks
Kami akan memiliki tautan alternatif kesepakatan di antara kita!
Sangat bersih situs, salam untuk posting ini.
Saya secara berkelanjutan menjelajah online untuk tips yang dapat memberi manfaat saya. Thanks!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Kerja yang fantastis!
Saya senang menjadi salah satu dari beberapa pengunjung di situs web hebat ini (:, sangat dihargai telah mengunggah.
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
Artikel yang sangat baik. Ini benar-benar ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Saya secara terus mencari online untuk tips yang dapat menolong saya. Thx!
Aku benar-benar ingin mengirim komentar singkat untuk mengucapkan terima kasih Anda atas semua informasi luar biasa yang Anda bagikan di situs ini.
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Aw, this was a really nice post. In thought I wish to put in writing like this additionally – taking time and actual effort to make an excellent article… however what can I say… I procrastinate alot and in no way seem to get one thing done.
Situs web ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
This site is my aspiration, really fantastic layout and perfect subject matter.
Konten yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
I have been checking out a few of your posts and it’s clever stuff. I will definitely bookmark your site.
Terima kasih untuk website informatif tambahan. Di tempat mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan cara yang sempurna? Saya memiliki sebuah tantangan yang saya sedang kerjakan, dan saya sudah mengamati informasi seperti ini.
Saya benar-benar tertarik menemukan situs internet ini di Bing, persis seperti yang saya telusuri : D begitu juga sudah saya simpan ke favorit.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Artikel yang bagus. Ini benar-benar ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Kami akan memiliki hyperlink perdagangan perjanjian antara kita!
Saya selalu mencari online untuk artikel yang dapat memberi manfaat saya. Terima kasih!
Saya secara terus menjelajah online untuk artikel yang dapat menolong saya. Terima kasih!
Sangat jelas website, terima kasih untuk pos ini.
Great blog! Do you have any tips and hints for aspiring writers? I’m planning to start my own blog soon but I’m a little lost on everything. Would you recommend starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m completely confused .. Any ideas? Appreciate it!
Saya menghargai usaha yang Anda curahkan untuk menyusun posting ini. Informasi yang bernilai. Terima kasih!
Very interesting information!Perfect just what I was searching for!
Artikel yang luar biasa. Ini memberi saya gambaran yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
With every thing that seems to be building throughout this particular subject material, all your points of view are actually relatively exciting. On the other hand, I appologize, because I can not give credence to your entire suggestion, all be it stimulating none the less. It appears to us that your commentary are generally not totally validated and in actuality you are your self not really completely convinced of the point. In any case I did enjoy examining it.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada pendekatan Anda bisa menghapus saya dari layanan itu? Terima kasih!
Hebat blog yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan umpan balik dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih banyak!
Saya tidak sangat hebat dalam bahasa Inggris tetapi saya memperoleh ini benar-benar ringan untuk dibaca .
Postingan ini sangat informatif. Saya sangat menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Good write-up, I am normal visitor of one’s site, maintain up the nice operate, and It is going to be a regular visitor for a lengthy time.
Some truly interesting details you have written.Aided me a lot, just what I was searching for :D.
Whats up very cool website!! Guy .. Beautiful .. Superb .. I will bookmark your blog and take the feeds additionally…I am satisfied to seek out so many useful info right here within the submit, we need work out more techniques in this regard, thanks for sharing. . . . . .
Wonderful work! This is the type of info that should be shared around the internet. Shame on the search engines for not positioning this post higher! Come on over and visit my site . Thanks =)
What a material of un-ambiguity and preserveness of precious know-how about unpredicted feelings.
Informative article, just what I wanted to find.
Heya! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing a few months of hard work due to no backup. Do you have any solutions to protect against hackers?
I just like the helpful info you provide for your articles. I will bookmark your weblog and take a look at once more right here frequently. I am relatively sure I will be told many new stuff proper here! Best of luck for the next!
Its great as your other articles : D, thanks for posting. “To be able to look back upon ones life in satisfaction, is to live twice.” by Kahlil Gibran.
The core of your writing while sounding agreeable in the beginning, did not work perfectly with me personally after some time. Someplace within the paragraphs you managed to make me a believer but just for a short while. I however have got a problem with your leaps in logic and you would do nicely to fill in those gaps. When you can accomplish that, I could surely end up being impressed.
Good info. Lucky me I reach on your website by accident, I bookmarked it.
Artikel yang sangat bagus. Ini memberikan saya pemahaman yang lebih baik tentang topik ini. Teruskan kerja yang luar biasa!
Informasi yang berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
Luar biasa blog yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan masukan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Salut!
Saya mendapatkan info yang bagus dari blog Anda.
Superb, what a website it is! This web site gives
helpful information to us, keep it up.
Konten yang fantastis! Cara penulisan Anda jelas dan mudah dimengerti. Saya pasti akan kembali untuk membaca konten lainnya.
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca belakangan ini. Informasi yang sangat membantu. Terima kasih telah berbagi.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri! “Hari yang paling sia-sia adalah hari di mana kita tidak tertawa.” oleh Sbastien-Roch Nicolas de Chamfort.
Terima kasih atas tulisan yang bagus. Faktanya ini sebelumnya adalah sebuah konten hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Seseorang secara esensial menolong untuk membuat secara kritis posting saya akan katakan. Itu adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga sekarang? Saya terkagum dengan riset yang Anda lakukan untuk menyusun kiriman luar biasa ini. Pekerjaan yang mengagumkan!
Some truly nice and useful information on this website , as well I believe the style has got excellent features.
Magnificent goods from you, man. I’ve be mindful your stuff previous to and
you’re just too fantastic. I really like what you have obtained here, certainly
like what you’re stating and the way in which
through which you are saying it. You are making
it entertaining and you still take care of to stay it smart.
I can’t wait to learn much more from you. This is really a wonderful site.
I have read several just right stuff here. Definitely value bookmarking for revisiting. I surprise how much effort you set to make this type of excellent informative web site.
I’m impressed, I must say. Really not often do I encounter a blog that’s both educative and entertaining, and let me let you know, you’ve gotten hit the nail on the head. Your thought is outstanding; the problem is something that not sufficient individuals are talking intelligently about. I’m very completely satisfied that I stumbled throughout this in my seek for one thing referring to this.
Thank you for some other informative site. Where else may just I am getting that kind of info written in such an ideal means? I have a mission that I’m simply now operating on, and I have been at the look out for such information.
Saya selamanya memikirkan hal ini, sangat dihargai telah mengunggah.
Saya tidak umumnya berkomentar tetapi saya harus menyatakan terima kasih untuk posting yang luar biasa ini : D.
I haven’t checked in here for some time because I thought it was getting boring, but the last several posts are good quality so I guess I will add you back to my daily bloglist. You deserve it my friend 🙂
Postingan yang bagus. Ini jelas ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Aku sungguh ingin menulis komentar singkat guna menghargai Anda atas semua saran luar biasa yang Anda tuliskan di website ini.
Have you ever thought about adding a little bit more than just your articles? I mean, what you say is important and all. But think of if you added some great visuals or videos to give your posts more, “pop”! Your content is excellent but with images and videos, this site could definitely be one of the very best in its niche. Wonderful blog!
Saya selalu peduli dengan topik ini dan masih demikian, terima kasih telah mengunggah.
Regards for this wondrous post, I am glad I observed this web site on yahoo.
Ya menyimpan ini bukanlah penentuan yang spekulatif pos yang hebat! .
Konten yang berguna. Saya baru menelusuri hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Saya tidak sering berkomentar tetapi saya harus mengakui terima kasih untuk posting yang satu ini : D.
so much superb info on here, :D.
Hi my friend! I wish to say that this article is awesome, nice written and include almost all important infos. I would like to see more posts like this.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
You made some first rate points there. I looked on the internet for the difficulty and located most individuals will go together with together with your website.
Sangat menarik info !Sempurna persis seperti yang saya cari!
Postingan yang sangat baik! Saya menghargai cara Anda menjelaskan segala sesuatu dengan sangat jelas. Teruskan pekerjaan yang bagus!
Can I simply say what a relief to discover somebody who actually understands what they are discussing online.
You definitely understand how to bring a problem to light
and make it important. More people need to look at this
and understand this side of the story. I was surprised you aren’t more popular since you definitely possess the gift.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Sangat menarik informasi!Sempurna persis seperti yang saya cari! “Kita dibentuk dan dipahat oleh apa yang kita cintai.” oleh Johann von Goethe.
Saya tidak benar-benar bagus dalam bahasa Inggris tetapi saya menganggap ini sungguh mudah untuk dibaca .
Terima kasih untuk website informatif lainnya. Di mana lagi saya memperoleh info seperti itu yang ditulis dengan metode yang ideal? Saya memiliki sebuah proyek yang saya tengah kerjakan, dan saya telah mengamati informasi seperti ini.
I have been reading out a few of your posts and i can state pretty good stuff. I will make sure to bookmark your blog.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Ya menyimpan ini bukanlah penentuan yang berisiko posting yang luar biasa! .
Wonderful work! This is the kind of info that are meant to be shared across the web. Shame on Google for not positioning this post upper! Come on over and seek advice from my site . Thank you =)
Benar-benar bersih website, terimakasih untuk posting ini.
Menghargai waktu dan tenaga yang Anda curahkan ke website Anda dan informasi mendalam yang Anda tawarkan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang sangat baik! Saya sudah menandai situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Hai di sana, sekadar ingin mengatakan bahwa saya sangat menikmati membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan banyak informasi yang bermanfaat. Terima kasih!
I’ve been browsing online greater than three hours lately, yet I by no means discovered any attention-grabbing article like yours. It’s beautiful value enough for me. In my view, if all website owners and bloggers made excellent content material as you did, the web might be much more useful than ever before. “Baseball is 90 percent mental. The other half is physical.” by Lawrence Peter Berra.
Heya i am for the first time here. I found this board and I find It really helpful & it helped me out a lot. I am hoping to give something again and help others such as you helped me.
I like this web site so much, saved to bookmarks.
Wow, awesome blog layout! How long have you been blogging for? you make blogging look easy. The overall look of your website is wonderful, as well as the content!
I saw a lot of website but I believe this one holds something special in it in it
What’s Happening i’m new to this, I stumbled upon this I’ve found It absolutely helpful and it has aided me out loads. I hope to contribute & assist other users like its aided me. Good job.
Generally I do not read post on blogs, however I wish to say
that this write-up very compelled me to try and do so!
Your writing taste has been surprised me. Thanks, very nice post.
superb post.Never knew this, thankyou for letting me know.
It’s hard to search out knowledgeable people on this subject, however you sound like you recognize what you’re speaking about! Thanks
Appreciate it for helping out, great information.
I got what you intend, thanks for putting up.Woh I am delighted to find this website through google. “Spare no expense to make everything as economical as possible.” by Samuel Goldwyn.
You can certainly see your enthusiasm in the work you write. The world hopes for more passionate writers like you who aren’t afraid to say how they believe. Always go after your heart.
he blog was how do i say it… relevant, finally something that helped me. Thanks
These are in fact fantastic ideas in concerning blogging.
You have touched some good things here. Any way keep up wrinting.
Some truly select posts on this web site, saved to bookmarks.
Keep working ,great job!
Discover how SBLC and Bank Guarantee monetization works in trade finance, including liquidity access, structured funding, risk management, and global trade financing solutions.
Bagian yang kuat, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia sebenarnya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka membaca lebih banyak tentang topik ini. Jika dapat dicapai, seiring Anda berkembang menjadi lebih ahli, apakah Anda berkenan memperbarui blog Anda dengan tambahan rincian? Ini sangat membantu bagi saya. Jempol besar untuk posting blog ini!
Thankyou for helping out, fantastic information.
Amat bersih situs internet, hargai untuk pos ini.
I’d forever want to be update on new blog posts on this web site, bookmarked! .
Terima kasih atas tulisan yang baik. Pada kenyataannya ini sebelumnya adalah sebuah materi hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat tetap berhubungan?
Postingan yang sangat baik! Saya sangat menghargai cara Anda menguraikan semuanya dengan mudah dipahami. Teruskan kerja yang bagus!
Saya perlu mengatakan, ini adalah salah satu artikel paling bagus yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Menikmati mempelajari ini, sangat bagus, terima kasih.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Saya sungguh bersyukur menemukan situs internet ini di Bing, persis seperti yang saya cari : D juga sudah saya simpan ke bookmark.
You actually make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand. It seems too complex and very broad for me. I am looking forward for your next post, I’ll try to get the hang of it!
Wow, awesome blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your web site is fantastic, as well as the content!
Hello would you mind stating which blog platform you’re using? I’m looking to start my own blog in the near future but I’m having a difficult time choosing between BlogEngine/Wordpress/B2evolution and Drupal. The reason I ask is because your design seems different then most blogs and I’m looking for something completely unique. P.S My apologies for getting off-topic but I had to ask!
I see something genuinely special in this internet site.
Saya selamanya memikirkan hal ini, salam telah mengunggah.
Your comment is awaiting moderation.
Dark web market Western Union services usually require fake ID to pick up, adds another layer of complexity.
Darknet market
https://darkweb-market.com
https://darkweb-market.com
https://darkweb-market.com
Saya benar-benar senang menemukan situs web ini di Bing, persis seperti yang saya cari : D begitu juga sudah saya bookmark.
Hore google adalah raja saya yang menolong saya menemukan web site yang luar biasa! .
Benar-benar hebat info dapat ditemukan di situs.
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
Terima kasih atas tulisan yang baik. Sebenarnya ini sebelumnya adalah sebuah materi hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat tetap berhubungan?
Konten yang luar biasa! Gaya penulisan Anda sangat jelas dan mudah dimengerti. Saya pasti akan kembali untuk melihat lebih banyak.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Very fantastic visual appeal on this internet site, I’d rate it 10 10.
I love your blog.. very nice colors & theme. Did you create this website yourself? Plz reply back as I’m looking to create my own blog and would like to know wheere u got this from. thanks
It is the best time to make a few plans for the longer term and it is time to be happy. I’ve read this publish and if I may I want to counsel you few fascinating issues or tips. Maybe you could write next articles relating to this article. I want to read more things about it!
Your comment is awaiting moderation.
https://www.facebook.com/fly88no1com/
https://x.com/fly88183185
https://www.youtube.com/@fly88no1com
https://www.pinterest.com/fly88no1com/
https://gravatar.com/fly88no1com
https://www.notebook.ai/users/1357977
https://pixabay.com/users/fly88no1com-55848196/
https://www.twitch.tv/fly88no1com/about
https://wakelet.com/@fly88no1com
https://profile.hatena.ne.jp/fly88no1com/
https://500px.com/p/fly88no1com
https://files.fm/fly88no1com/info
https://fliphtml5.com/home/fly88no1com
https://leetcode.com/u/fly88no1com/
https://savelist.co/profile/users/fly88no1com
https://jobs.windomnews.com/profiles/8273580-fly88
https://www.magcloud.com/user/fly88no1com
https://linkin.bio/fly88no1com/
https://jobs.landscapeindustrycareers.org/profiles/8273602-fly88
https://jobs.westerncity.com/profiles/8273609-fly88
https://wefunder.com/fly88no1com/about
http://freestyler.ws/user/657980/fly88no1com
https://jobs.tdwi.org/employers/4153483-fly88
https://www.minecraft-servers-list.org/details/fly88no1com/
https://lifeinsys.com/user/fly88no1com
https://www.directorylib.com/domain/fly88-no1.com
https://forums.alliedmods.net/member.php?u=479847
https://forums.maxperformanceinc.com/forums/member.php?u=249646
https://www.aviacionargentina.net/user/fly88no1com
https://road-to-eden.com/index.php?fly88no1com
https://line-monsterfarm.wiki/?fly88no1com
https://teletype.in/@fly88no1com
https://www.fw-follow.com/forum/topic/127971/fly88
https://www.getlisteduae.com/listings/fly88-27
https://www.nongkhaempolice.com/forum/topic/139780/fly88
https://www.anibookmark.com/user/fly88no1com.html
http://newdigital-world.com/members/fly88no1com.html
https://www.bitchute.com/channel/Gk0QOlVWmf6u
https://vocal.media/authors/fly88-qke6l0du8
https://www.wvhired.com/profiles/8274966-fly88
https://www.claimajob.com/profiles/8274965-fly88
https://golosknig.com/profile/fly88no1com/
https://motion-gallery.net/users/980846
https://www.passes.com/fly88no1com
https://www.reverbnation.com/artist/fly88no1com
https://www.checkli.com/fly88no1com#/a/process
https://forum.delftship.net/Public/users/fly88no1com/
https://homepage.ninja/fly88no1com
https://www.equinenow.com/farm/fly88-1334419.htm
https://advego.com/profile/fly88no1com/
https://backloggery.com/fly88no1com
https://www.designspiration.com/fly88no1com/saves/
https://protocol.ooo/ja/users/fly88no1com
http://fort-raevskiy.ru/community/profile/fly88no1com/
https://joy.link/fly88no1com
https://pxhere.com/en/photographer/5013682
https://fanclove.jp/profile/jpJLjPzrBa
https://www.speedrun.com/users/fly88no1com
https://www.iglinks.io/mepupeteye20-ira?preview=true
https://www.tizmos.com/fly88no1com
https://feyenoord.supporters.nl/profiel/152555/fly88no1com
https://www.iniuria.us/forum/member.php?682119-fly88no1com
https://www.dibiz.com/mepupeteye20
https://doodleordie.com/profile/fly88no1com
https://anyflip.com/homepage/cakqc/preview
https://cointr.ee/fly88no1com
https://www.nintendo-master.com/profil/fly88no1com
https://www.band.us/band/102712070/post
https://allmylinks.com/fly88no1com
https://connect.gt/user/fly88no1com
https://hub.docker.com/u/fly88no1com
https://f319.com/members/fly88no1com.1109821/
https://rapidapi.com/user/fly88no1com
https://www.skool.com/@nha-cai-fly-5318
https://www.aicrowd.com/participants/fly88no1com
https://activepages.com.au/profile/fly88no1com
https://zzb.bz/XN1You
https://beteiligung.tengen.de/profile/fly88no1com/
https://sciencemission.com/profile/fly88no1com
https://naijamatta.com/fly88no1com
https://cdn.muvizu.com/Profile/fly88no1com/Latest/
http://forum.vodobox.com/profile.php?section=personal&id=72435
https://help.orrs.de/user/fly88no1com
https://dev.muvizu.com/Profile/fly88no1com/Latest/
https://pimrec.pnu.edu.ua/members/fly88no1com/profile/
https://community.cisco.com/t5/user/viewprofilepage/user-id/2075739
https://kotob4all.com/profile/fly88no1com
https://www.dideadesign.com/forum/topic/47849/fly88
https://killtv.me/user/fly88no1com/
https://l2top.co/forum/members/fly88no1com.180099/
https://pubhtml5.com/homepage/zjcly/preview
https://transfur.com/Users/fly88no1com
https://dojour.us/u/fly88no1com
https://www.wattpad.com/user/fly88no1com
https://chodaumoi247.com/members/fly88no1com.52953/#about
https://www.11plus.co.uk/users/mepupeteye20/
https://stardust.run/user/172694/fly88no1com/#preferences
https://congdongmassage.com/members/fly88no1com.151655/
https://onespotsocial.com/fly88no1com
http://iawbs.com/home.php?mod=space&uid=959342
https://en.islcollective.com/portfolio/12922690
https://classificados.acheiusa.com/profile/Z0M0d1lIVXR3UCswMjdzUUNtQllQNGJZa25ENUltK0VpTytKTU1nUGRCND0=
https://dreevoo.com/profile_info.php?pid=1640284
https://raovat.nhadat.vn/members/fly88no1com-313726.html
https://www.callupcontact.com/b/businessprofile/fly88/10087955
https://myget.org/users/fly88no1com
http://delphi.larsbo.org/user/fly88no1com
https://www.joomla51.com/forum/profile/105086-fly88no1com
https://support.bitspower.com/support/user/fly88no1com
https://www.maanation.com/neko96
https://belgaumonline.com/profile/fly88no1com/
https://speakerdeck.com/fly88no1com
https://www.flyingv.cc/users/1457250
https://www.outdooractive.com/en/member/nha-cai-fly88/341132479/
https://www.wowonder.xyz/fly88no1com
https://demo.wowonder.com/fly88no1com
https://letterboxd.com/fly88no1com/
https://www.hyperlabthailand.com/forum/topic/813656/fly88
http://qa.doujiju.com/index.php?qa=user&qa_1=fly88no1com
https://biashara.co.ke/author/fly88no1com/
https://soundcloud.com/fly88no1com
https://sub4sub.net/forums/users/fly88no1com/
https://userstyles.world/user/fly88no1com
https://businessbookmark.com/story7052330/fly88
https://www.slideshare.net/mepupeteye20?tab=about
https://wirtube.de/a/fly88no1com/video-channels
https://participation.bordeaux.fr/profiles/fly88no1com/activity
https://collectednotes.com/fly88no1com/unknown
https://www.mikocon.com/home.php?mod=space&uid=293505
https://nous.malakoff.fr/profiles/fly88no1com/activity
https://community.alexgyver.ru/members/fly88no1com.178033/#about
https://www.producthunt.com/@fly88no1com
https://hu.gravatar.com/fly88no1com
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=264452
https://fr.quora.com/profile/Fly88-42
https://ncnews.co/profile/fly88no1com
https://mitwirken.stadt-zuerich.ch/profiles/fly88no1com/activity?locale=en
https://openwhyd.org/u/6a0557d090a8660442cdee7c
https://independent.academia.edu/fly88no1com
https://notionpress.com/author/1521452
https://rnmanagers.com/author/fly88no1com/
https://jobs.nefeshinternational.org/employers/4154057-fly88
https://www.tripadvisor.in/Profile/fly88no1com
https://www.akaqa.com/question/q19192681788-Fly88no1com
https://www.play56.net/home.php?mod=space&uid=6214079
https://www.fanart-central.net/user/fly88no1com/profile
https://bbs.mofang.com.tw/home.php?mod=space&uid=2501482
https://stepik.org/users/1274032893/profile
https://peatix.com/user/29610490/view
https://market360.vn/page/77334
https://digiex.net/members/fly88no1com.146718/
https://www.aipictors.com/en/users/2297920f-5034-e271-7205-cb897c37d6c8
https://writeupcafe.com/author/fly88no1com
https://mepupeteye20.wixstudio.com/my-site
https://forums.desmume.org/profile.php?section=personal&id=421508
https://cv.viblo.asia/preview-cv/dacc1220-a302-4958-87ec-f2fa3f63a5ab
http://bbs.medicalforum.cn/home.php?mod=space&uid=2272965
http://prsync.com/flynocom/
https://viblo.asia/p/fly88-1XVOWMqZVMz
https://blacksocially.com/fly88no1com
https://www.codingame.com/profile/a17799a4766b2376434c8a1602be12989899827
https://www.foriio.com/fly88no1com
https://able2know.org/topic/596213-1
https://xoops.ec-cube.net/userinfo.php?uid=350752
https://www.awwwards.com/fly88no1com/
https://maps.arosalenzerheide.swiss/en/member/nha-cai-fly88/341132479/
https://congdongx.com/thanh-vien/fly88no1com.51137/#about
https://www.highpriceddatinguk.com/fly88no1com
https://unityroom.com/users/g4yo785kn9dwexvurts3
https://shootinfo.com/ru/author/fly88no1com/?pt=ads
https://www.buckeyescoop.com/users/88dbf587-138e-4a8b-89b9-a089e7122a50
https://upuge.com/fly88no1com
https://manylink.co/@fly88no1com
https://kooperation.winterthur.ch/profiles/fly88no1com/activity
https://mforum.cari.com.my/home.php?mod=space&uid=3402947&do=profile
https://www.euskalmarket.com/author/fly88no1com/
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:EFC283CF6A041EC50A495FBF@AdobeID
https://www.airportcitygame.com/members/fly88no1com.37000/#about
https://challonge.com/fly88no1com
https://dinosquadsuriku.com/?fly88no1com
https://mel-assessment.com/members/fly88no1com/profile/
https://www.onetap.com/members/fly88no1com.510200/#about
https://dialogluzern.ch/profiles/fly88no1com/activity
https://www.pebforum.com/members/fly88no1com.245602/#about
https://sv.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://kr.pinterest.com/fly88no1com/
https://buyerseller.xyz/user/fly88no1com/
https://dongnairaovat.com/members/fly88no1com.76693.html
https://www.tacter.com/@fly88no1com
https://vi.gravatar.com/fly88no1com
https://mathlog.info/users/oENb0aOheSU9t1Dr0kcOsRZcRQx1
https://partecipa.poliste.com/profiles/fly88no1com/activity
https://forum.pabbly.com/members/fly88no1com.118707/#about
https://www.vid419.com/home.php?mod=space&uid=3490002
http://forum.orangepi.org/home.php?mod=space&uid=6506877
https://forum.dmec.vn/index.php?members/fly88no1com.193058/
https://ofuse.me/fly88no1com
https://ztndz.com/story28504494/fly88no1com
https://www.scener.com/@fly88no1com
https://hostndobezi.com/fly88no1com
https://pt.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://marshallyin.com/members/fly88no1com/
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=165112_5fnlo3i9
https://community.m5stack.com/user/fly88no1com
https://www.bestloveweddingstudio.com/forum/topic/90822/fly88no1com
https://allmy.bio/fly88no1com
https://www.laundrynation.com/community/profile/fly88no1com/
https://jali.me/fly88no1com
https://jaga.link/fly88no1com
https://www.rcmx.net/userinfo.php?op=avatarform&uid=18151
https://bd.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://www.fundable.com/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a
https://biolinku.co/fly88no1com
https://undrtone.com/fly88no1com
https://b.cari.com.my/home.php?mod=space&uid=3402947&do=profile
https://paper.wf/fly88no1com/nguoi-choi-co-the-tham-gia-fly88-de-kham-pha-he-sinh-thai-game-truc-tuyen-voi
http://palangshim.com/space-uid-5171055.html
https://topsitenet.com/profile/fly88no1com/1753949/
https://fortunetelleroracle.com/profile/fly88no1com
https://www.annuncigratuititalia.it/author/fly88no1com/
https://hukukevi.net/user/fly88no1com
https://zeroone.art/profile/fly88no1com
https://gt.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://devfolio.co/@7f4de393cb604b2/readme-md
https://phatwalletforums.com/user/fly88no1com
https://divisionmidway.org/jobs/author/fly88no1com/
https://audiomack.com/fly88no1com
https://biiut.com/fly88no1com
https://its-my.link/@fly88no1com
https://coub.com/fly88no1com
https://qoolink.co/fly88no1com
https://mx.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://jali.pro/fly88no1com
https://ngel.ink/fly88no1com
https://www.floodzonebrewery.com/profile/fly88no1com/profile
https://hk.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://pastelink.net/834duaf4
https://matters.town/@fly88no1com
https://photouploads.com/fly88no1com
https://profile.sampo.ru/fly88no1com
https://pbase.com/fly88no1com/root
http://www.askmap.net/location/7822392/vietnam/fly88-trang-ch%E1%BB%A7-nh%C3%A0-c%C3%A1i-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-uy-t%C3%ADn-s%E1%BB%91-1-ch%C3%A2u-%C3%A1
https://etextpad.com/dwtqga2mmj
https://www.ttlxshipping.com/forum/topic/427605/fly88no1com
https://www.chichi-pui.com/users/fly88no1com/
https://ie.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://www.moshpyt.com/user/fly88no1com
https://mygamedb.com/profile/fly88no1com
https://robertsspaceindustries.com/en/citizens/fly88no1com
https://bioqoo.com/fly88no1com
https://br.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://phijkchu.com/a/fly88no1com/video-channels
https://www.freelistingusa.com/listings/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a
https://www.brownbook.net/business/55097338/fly88-trang-ch%E1%BB%A7-nh%C3%A0-c%C3%A1i-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-uy-t%C3%ADn-s%E1%BB%91-1-ch%C3%A2u-%C3%A1
https://forum.codeigniter.com/member.php?action=profile&uid=237685
https://myanimelist.net/profile/fly88no1com
https://www.weddingbee.com/members/fly88no1com/
https://community.jmp.com/t5/user/viewprofilepage/user-id/99900
https://sciter.com/forums/users/fly88no1com/
http://galeria.farvista.net/member.php?action=showprofile&user_id=78730
https://dirstop.com/story28501975/fly88no1com
https://myanimeshelf.com/profile/fly88no1com
https://www.1001fonts.com/users/fly88no1com/
https://fora.babinet.cz/profile.php?section=personal&id=127251
http://www.dungdong.com/home.php?mod=space&uid=3380243
https://old.bitchute.com/channel/Gk0QOlVWmf6u/
http://web.symbol.rs/forum/member.php?action=profile&uid=1288492
https://tempel.in/view/G4vMKNUC
https://www.horticulturaljobs.com/employers/4153937-nha-cai-fly88
https://www.hentai-foundry.com/user/fly88no1com/profile
https://aboutcasemanagerjobs.com/author/fly88no1com/
https://londonchinese.com/home.php?mod=space&uid=622718&do=profile
https://boss.why3s.cc/boss/home.php?mod=space&uid=266020
https://rush1989.rash.jp/pukiwiki/index.php?cmd=read&page=fly88no1com&refer=neko96
https://us.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://findaspring.org/members/fly88/
https://pl.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://www.bridgescdc.com/profile/fly88no1com/profile
https://gourmet-calendar.com/users/fly88no1com
https://www.elephantjournal.com/profile/fly88no1com/
https://kyourc.com/fly88no1com
https://www.leonidastacticalss.com/profile/fly88no1com/profile
https://www.miseducationofmotherhood.com/profile/fly88no1com/profile
https://www.guidedground.com/profile/fly88no1com/profile
https://webspeed.intensys.pl/wyniki/219505/
https://devpost.com/fly88no1com
https://www.thatjessedenis.com/profile/fly88no1com/profile
https://hedgedoc.k8s.rexo.top/load.php?note=22e1012a
https://hedge.f.rexo.top/load.php?note=d6111ccb
https://www.stephhalllcsw.com/profile/fly88no1com/profile
https://redirect.camfrog.com/redirect/?url=https://fly88-no1.com/
https://website.informer.com/fly88-no1.com
https://hcgdietinfo.com/hcgdietforums/members/fly88no1com/
https://www.adsfare.com/fly88no1com
https://www.lytekids.com/members-area/fly88no1com/profile?disableScrollToTop=true
https://www.celsocarvalho.com/profile/fly88no1com/profile
https://www.claimingthecorner.net/profile/fly88no1com/profile
https://v.gd/dS8bGm
https://creator.nightcafe.studio/u/fly88no1com
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=197670
https://zealy.io/cw/fly88no1com
https://www.bat-safe.com/profile/fly88no1com/profile
https://skrolli.fi/keskustelu/users/mepupeteye20/
https://www.ixawiki.com/link.php?url=https://fly88-no1.com/
https://socialcreditu.com/fly88no1com
https://defence.pk/members/fly88no1com.241927/#about
https://www.kwlt.net/profile/fly88no1com/profile
https://www.leadworksprojects.com/profile/fly88no1com/profile
https://www.davidrio.com/profile/fly88no1com/profile
https://securityheaders.com/?q=https%3A%2F%2Ffly88-no1.com%2F&followRedirects=on
https://fairygodboss.com/users/profile/skMu458ati/fly88no1com
http://vintagemachinery.org/members/detail.aspx?id=168224
https://boosty.to/fly88no1com
https://community.poco.in/post/28327
https://fotolibre.social/fly88no1com
https://www.bloggalot.com/profile/fly88no1com
https://gloobalnews.com/profile/fly88no1com
https://www.watershedwellness.net/profile/fly88no1com/profile
https://outdoor.surselva.info/en/member/nha-cai-fly88/341132479/
https://allmyfaves.ca/fly88no1com
https://adhocracy.plus/profile/fly88no1com/
https://www.fullhires.com/author/fly88no1com/
https://www.goldposter.com/members/fly88no1com/profile/
https://amvnews.ru/forum/profile.php?mode=viewprofile&u=105689
https://goodandbadpeople.com/fly88no1com
https://nilechronicles.com/profile/fly88no1com
https://www.komoot.com/pt-br/user/5771600029951
https://coinfolk.net/user/fly88no1com
https://app.reczee.com/talenthub/fly88no1com
https://www.blockdit.com/fly88no1com
https://beteiligung.stadtlindau.de/profile/fly88no1com/
https://gitlab.vuhdo.io/fly88no1com
https://iszene.com/user-352079.html
https://muare.vn/shop/lucien/905146
https://www.facer.io/u/fly88no1com
https://www.telix.pl/profile/Lucien/
https://es.stylevore.com/user/fly88no1com
https://www.rcuniverse.com/forum/members/fly88no1com.html
https://igli.me/fly88no1com
https://blog.sighpceducation.acm.org/wp/forums/users/fly88no1com/
https://filesharingtalk.com/members/637881-fly88no1com
https://forum.issabel.org/u/fly88no1com
https://hanson.net/users/fly88no1com
https://kktix.com/user/8958399
https://hi-fi-forum.net/profile/1153304
https://www.chordie.com/forum/profile.php?section=about&id=2530607
https://www.mecanique-bateau.com/community/profile/fly88no1com
https://iplogger.org/logger/Q3jT5aduUxdS/
https://www.themeqx.com/forums/users/fly88no1com/
http://www.genina.com/user/edit/5359490.page
https://longbets.org/user/fly88no1com/
https://www.siasat.pk/members/fly88no1com.273436/#about
https://bbs.t-firefly.com/home.php?mod=space&uid=694534
https://theenergyprofessor.net/community/profile/fly88no1com/
https://sfx.thelazy.net/users/u/fly88no1com/
https://www.prosebox.net/book/110906/
https://dq10wiki.net/wiki/?fly88no1com
https://participa.aytojaen.es/profiles/fly88no1com/activity
https://www.techbang.com/users/fly88no1com
https://cboj.ca/user/fly88no1com
https://awan.pro/forum/user/173533/
https://forum.euro-pvp.com/user/565126-fly88no1com/
https://novel.daysneo.com/author/fly88no1com/
https://formulamasa.com/elearning/members/fly88no1com/
https://sdelai.ru/members/fly88no1com/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/fly88no1.com
https://video.fc2.com/account/76189697
https://te.legra.ph/fly88-05-13
http://www.grandisvietnam.com/members/fly88no1com.30679/#about
https://gb.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://b.hatena.ne.jp/fly88no1com/
https://bio.site/fly88no1com
https://cloudburstmc.org/members/fly88no1com.79872/#about
https://www.rankone.global/fly88no1com
https://vn.enrollbusiness.com/BusinessProfile/7806642/fly88
https://fly88no1com.blogkoo.com/fly88-60960250
https://beteiligung.hafencity.com/profile/fly88no1com/
https://fly88no1com.stck.me/profile
https://www.pexels.com/@nha-cai-fly88-2161574074/
https://blogosm.com/profile/fly88no1com
https://tealfeed.com/fly88no1com
https://vishalbharat.in/fly88no1com
https://cornucopia.se/author/fly88no1com/
http://www.fromeyes.cn/bbs/home.php?mod=space&uid=64013
https://hashnode.com/@fly88no1com
https://aboutpharmacistjobs.com/author/fly88no1com/
http://kjtr.grrr.jp/kjtr/
https://www.spoofee.com/forums/members/fly88no1com.111679/#about
https://www.okaywan.com/home.php?mod=space&uid=804462
https://sedowiki.com/?fly88no1com
https://www.bandsworksconcerts.info/index.php?fly88no1com
https://kitsu.app/users/fly88no1com
https://fly88no1com.ampblogs.com/fly88-78215371
https://pod.beautifulmathuncensored.de/people/887a50a0318c013f95dc021877951523
https://www.gamerlaunch.com/community/users/blog/6757819?gl_user=6757819&gid=535
https://www.socialbookmarkssite.com/bookmark/6254607/fly88/
https://learningapps.org/display?v=p428ea38k26
https://gitlab.haskell.org/fly88no1com
https://www.weddingvendors.com/directory/profile/41566/
https://www.99freelas.com.br/user/fly88no1com
https://www.efunda.com/members/people/show_people.cfm?Usr=fly88no1com
https://hangoutshelp.net/user/fly88no1com
https://newspicks.com/user/12470838/
https://savee.com/fly88no1com/
https://muabanhaiduong.com/members/fly88no1com.89977/#about
https://atthehive.com/user/fly88no1com/
https://www.livecleo.xxx/community/profile/fly88no1com/
https://estar.jp/users/2043362189
https://www.clashfarmer.com/forum/member.php?action=profile&uid=81640
https://ru.myanimeshelf.com/profile/fly88no1com
https://kenhrao.com/members/fly88no1com.123000/#about
https://fly88no1com.blogkoo.com/fly88no1com-60969324
https://fly88no1com.national-wiki.com/2356470/fly88no1com
https://giphy.com/channel/fly88no1com
https://community.hpe.com/t5/user/ViewProfilePage/user-id/2486194
https://comicvine.gamespot.com/profile/fly88no1com/
https://neodb.social/article/6P3lWjAcquDvxRRjviaaIt
https://all4.vip/p/page/view-persons-profile?id=125891
https://www.veteranscup.org/profile/fly88no1com/profile
https://participer.loire-atlantique.fr/profiles/fly88no1com/activity
https://www.ltstesting.com/profile/fly88no1com/profile
https://www.housedumonde.com/profile/fly88no1com/profile
https://oyaschool.com/users/fly88no1com/
https://www.luzsantomauro.com/profile/fly88no1com/profile
https://galgame.dev/user/fly88no1com
https://dumagueteinfo.com/author/fly88no1com/
https://magic.ly/fly88no1com
https://www.squadskates.com/profile/fly88no1com/profile
https://www.saltlakeladyrebels.com/profile/fly88no1com/profile
https://slides.com/fly88no1com
https://opencollective.com/fly88no1com1
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=229824&tab=field_core_pfield_13
https://3ddd.ru/users/fly88no1com
https://tannda.net/fly88no1com
https://thewion.com/fly88no1com
https://meta.decidim.org/profiles/fly88no1com/activity
https://bbs.airav.cc/home.php?mod=space&uid=4618446
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=781771
https://www.plotterusati.it/user/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a
https://forum.aceinna.com/user/fly88no1com
https://jobs.lajobsportal.org/profiles/8273433-fly88
http://bbs.sdhuifa.com/home.php?mod=space&uid=1123071
https://www.xen-factory.com/index.php?members/fly88no1com.161099/#about
https://fly88no1com.jasperwiki.com/7673619/fly88
https://qiita.com/fly88no1com
https://walling.app/IwJY9uumQ9z5A3LHjfpD/-
https://www.freelistingindia.in/listings/fly88
https://praca.uxlabs.pl/author/fly88no1com/
https://beta.cent.co/fly88no1com/+jz6qb4
https://www.frenchwomenorg.com/fly88no1com
https://guestboard.co/events/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a/details
https://app.wedonthavetime.org/profile/fly88
https://modx.pro/users/fly88no1com
https://shareshortcuts.com/u/fly88no1com/
https://promosimple.com/ps/493d4/fly88
https://www.newline.co/@fly88no1com
https://www.vitalpilze.de/board/woltlab/user/39148-fly88no1com/#about
https://logicmastersindia.com/forum/view-profile.asp?action=view&uid=41325
https://interestpin.com/user/118124/fly88no1com
https://inkbunny.net/fly88no1com
https://www.fitday.com/fitness/forums/members/fly88no1com.html
https://lookingforclan.com/user/fly88no1com
https://trakteer.id/fly88no1com
https://gravesales.com/author/fly88no1com/
https://www.project1999.com/forums/member.php?u=337393
https://axe.rs/forum/members/fly88no1com.13430450/#about
https://www.rueanmaihom.net/forum/topic/106582/fly88
https://runtrip.jp/users/783877
https://anh135689999.violet.vn/user/show/id/15276287
https://www.diggerslist.com/fly88no1com/about
https://www.lookingforjob.co/profile/fly88no1com
https://englishsharedfutures.uk/forums/users/fly88no1com/
https://tulieu.violet.vn/user/show/id/15276287
https://artelis.pl/autor/profil/239654
https://snabaynetworking.com/profile/18107/
https://giaoan.violet.vn/user/show/id/15276287
https://ja.cofacts.tw/user/fly88no1com
https://startupxplore.com/en/person/fly88-17
https://violet.vn/user/show/id/15276287
https://circleten.org/a/408010?postTypeId=whatsNew
https://www.symbaloo.com/mix/fly88no1com
https://participacion.cabildofuer.es/profiles/fly88no1com/activity?locale=en
https://muckrack.com/fly88no1-com/bio
https://sighpceducation.hosting.acm.org/wp/forums/users/fly88no1com/
https://www.empregosaude.pt/en/author/fly88no1com/
https://hoaxbuster.com/redacteur/fly88no1com
https://fly88no1com.stck.me/
https://www.mapleprimes.com/users/fly88no1com
https://que.u.nosv.org/profile?user=fly88no1com
https://affariat.com/user/profile/181824
https://commoncause.optiontradingspeak.com/index.php/community/profile/fly88no1com/
https://www.youyooz.com/profile/fly88no1com/
https://www.thetriumphforum.com/members/fly88no1com.66004/
https://manga-no.com/@fly88no1com/profile
https://tutorialslink.com/member/fly88undefined/101688
https://www.rwaq.org/users/fly88no1com
https://boldomatic.com/view/writer/fly88no1com
https://www.vnbadminton.com/members/fly88no1com.79183/
https://cofacts.tw/user/fly88no1com
https://galleria.emotionflow.com/186637/profile.html
https://www.mymeetbook.com/fly88no1com
https://beteiligung.amt-huettener-berge.de/profile/fly88no1com/
https://fly88trangchnhciccctrctuynuytns1.website3.me/
https://projectnoah.org/users/fly88no1com
https://musikersuche.musicstore.de/profil/fly88no1com/
https://www.abclinuxu.cz/lide/fly88no1com.
https://skitterphoto.com/photographers/2679382/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a
https://www.theyeshivaworld.com/coffeeroom/users/fly88no1com
https://desksnear.me/users/fly88-trang-ch-nha-cai-ca-c-c-tr-c-tuy-n-uy-tin-s-1-chau-a
http://www.biblesupport.com/user/839371-fly88no1com/
https://www.invelos.com/UserProfile.aspx?Alias=fly88no1com
https://www.lingvolive.com/en-us/profile/6b8fced9-b699-4d31-bc57-263a3523e116/translations
https://doselect.com/@38fb7037033696e4d807c89df
https://dentaltechnician.org.uk/community/profile/fly88no1com/
https://linkmix.co/54535625
https://www.investagrams.com/Profile/fly88no1com
https://www.blackhatprotools.info/member.php?291539-fly88no1com
https://aprenderfotografia.online/usuarios/fly88no1com/profile/
https://wibki.com/fly88no1com?tab=fly88no1com
https://chyoa.com/user/fly88no1com
https://forum.cnnr.fr/user/fly88no1com
https://malt-orden.info/userinfo.php?uid=462990
https://scenarch.com/userpages/36681
https://forum.hiv.plus/user/fly88no1com
https://www.apsense.com/user/fly88no1com
https://zimexapp.co.zw/fly88no1com
https://www.navacool.com/forum/topic/427196/fly88no1com
https://velog.io/@fly88no1com/posts
https://qna.alpharegiment.com/profile/fly88no1com/
https://protospielsouth.com/user/135209
https://allmyfaves.com/fly88no1com
https://www.notariosyregistradores.com/web/forums/usuario/fly88no1com/
https://www.sunlitcentrekenya.co.ke/author/fly88no1com/
https://www.natthadon-sanengineering.com/forum/topic/114018/fly88no1com
https://imaginaria.ru/profile/fly88no1com/
https://nicheless.blog/author/fly88-6
https://learn.mystudyseries.co.nz/members/fly88no1com/
https://forum.m5stack.com/user/fly88no1com
https://jobs.suncommunitynews.com/profiles/8272176-nha-cai-fly88
https://www.cardanocube.com/community/fly88no1com
https://matkafasi.com/user/fly88no1com
https://talkmarkets.com/profile/nh%C3%A0-c%C3%A1i-fly88-260513-121343
https://searchengines.guru/ru/users/2236718
https://blender.community/fly88no1com/
https://app.talkshoe.com/user/fly88no1com
https://www.tai-ji.net/members/profile/3727067/fly88no1com.htm
https://webcamscenter.com/user/fly88no1com
https://www.threadless.com/@fly88no1com/activity
https://civitai.com/user/fly88no1com
https://zepodcast.com/forums/users/fly88no1com/
https://bandori.party/user/943870/fly88no1com/
https://triumph.srivenkateshwaraa.edu.in/profile/fly88no1com
https://www.greencarpetcleaningprescott.com/members/profile/3727185/fly88no1com.htm
https://app.brancher.ai/user/29qdLI_Teoh0
https://www.stylevore.com/user/fly88no1com
https://californiafilm.ning.com/profile/FLY88TrangChuNhaCaiCaCoc
https://recash.wpsoul.net/members/fly88no1com/profile/
https://bbs.mikocon.com/home.php?mod=space&uid=293505
https://justpaste.me/NCfR2
https://vs.cga.gg/user/243118
https://freeimage.host/fly88no1com
https://www.ironlifting.it/forum/member.php?u=431222
https://janitorai.com/profiles/6ecf375a-401f-4e38-8210-ca9176bae396_profile-of-fly-88-no-1-com
https://the22koreanwar.org/members/fly88no1com/profile/
https://www.halaltrip.com/user/profile/349275/fly88no1com/
https://www.democracylab.org/user/42810
https://www.pathumratjotun.com/forum/topic/188026/fly88no1com
https://www.muvizu.com/Profile/fly88no1com/Latest
https://www.jk-green.com/forum/topic/119987/fly88no1com
https://www.mateball.com/fly88no1com
https://aphorismsgalore.com/users/fly88no1com
https://pastebin.com/u/fly88no1com
https://searchengines.bg/members/fly88no1com.27517/#about
https://issuu.com/fly88no1com
https://tophatsec.com/forum/member.php?action=profile&uid=16148
https://destaquebrasil.com/saopaulo/author/fly88no1com/
https://pets4friends.com/profile-1595010
https://linqto.me/about/fly88no1com
https://vc.ru/id5967666
https://pumpyoursound.com/u/user/1623085
https://tuscl.net/member/890333
https://mikropragmata.lifo.gr/meli/fly88no1com/profile/
https://www.giveawayoftheday.com/forums/profile/1859768
https://www.adpost.com/u/fly88no1com/
https://disqus.com/by/fly88no1com/about/
https://youslade.com/fly88no1com
https://lankadevelopers.lk/user/fly88no1com
https://www.newgenstravel.com/forum/topic/48588/fly88no1com
https://forum.herozerogame.com/index.php?/user/166017-fly88no1com/
https://chanylib.ru/ru/forum/user/28290/
https://www.czporadna.cz/user/fly88no1com
https://shareyoursocial.com/fly88no1com
https://opensea.io/fly88no1com
https://bike-forum.cz/profil/u/fly88no1com
https://www.goodreads.com/user/show/201057374-fly88-no1com
https://luvly.co/users/fly88no1com
https://www.tkaraoke.com/forums/profile/fly88no1com/
https://aiti.edu.vn/members/fly88no1com.47890/
https://www.camtation.com/leden/fly88no1com/profile/
https://vn.ekademia.com/@fly88no1com
https://m.twitch.tv/fly88no1com/home
https://bresdel.com/fly88no1com
https://www.pozible.com/profile/fly88-73
https://swat-portal.com/forum/wcf/user/51144-fly88no1com/#about
https://www.quora.com/profile/Fly88-42
https://edabit.com/user/vDSdfpLAFQFCCQPn4
https://forum.tkool.jp/index.php?members/fly88no1com.109045/#about
https://git.disroot.org/fly88no1com
https://propterest.com.au/user/84005/fly88no1com
https://amaz0ns.com/forums/users/fly88no1com/
https://songdew.com/fly88no1com
https://www.pintradingdb.com/forum/member.php?action=profile&uid=146023
https://fly88no1com.mssg.me/
https://www.sonorancareerlink.com/employers/4154137-fly88no1com
http://app.gxbs.net/home.php?mod=space&uid=1850441
https://raovatonline.org/author/fly88no1com/
https://swdteam.com/profile/fly88no1com#posts
https://decidim.santcugat.cat/profiles/fly88no1com/activity
https://hkgay.net/member.php?action=profile&uid=529706
http://tkdlab.com/wiki/index.php?fly88no1com
https://pledgeme.co.nz/profiles/336787
https://decidim.calafell.cat/profiles/fly88no1com/activity
https://www.clickasnap.com/profile/fly88no1com
https://www.retailandwholesalebuyer.com/profile/fly88no1com
https://expatguidekorea.com/profile/fly88no1com/
http://pcsq28.com/home.php?mod=space&uid=2059525
https://www.sciencebee.com.bd/qna/user/fly88no1com
https://www.vaingloryfire.com/profile/fly88no1com/bio?profilepage
https://quomon.es/Profile/fly88no1com
https://rentry.co/ywswredw
https://xtremepape.rs/members/fly88no1com.674935/#about
http://jobs.emiogp.com/author/fly88no1com/
https://onlinevetjobs.com/author/fly88no1com/
https://www.xiuwushidai.com/home.php?mod=space&uid=2698494
https://vhearts.net/fly88no1com
https://chatclub.mn.co/members/39712676
https://slideslive.com/fly88no1com?tab=about
https://careers.coloradopublichealth.org/profiles/8276470-mepupeteye20-gmail-com-fly88
https://aboutnursepractitionerjobs.com/author/fly88no1com/
https://aboutsnfjobs.com/author/fly88no1com/
https://decide.enguera.es/profiles/fly88no1com/activity
http://hkeverton.com/forumnew/home.php?mod=space&uid=647846
https://rndirectors.com/author/fly88no1com/
http://xline.vc/index.php?fly88no1com
https://participation.touraine.fr/profiles/fly88no1com/activity
http://bbs.yongrenqianyou.com/home.php?mod=space&uid=4371016&do=profile
https://forum.skullgirlsmobile.com/members/fly88no1com.224098/#about
https://www.betting-forum.com/members/fly88no1com.161446/#about
https://forums.mybb.rexo.top/member.php?action=profile&uid=365
https://controlc.com/de0dcqok
https://www.fitlynk.com/fly88no1com
https://nhatkythuthuat.com/members/fly88no1com.70270/#about
https://bsky.app/profile/fly88no1com.bsky.social
http://www.muzikspace.com/profiledetails.aspx?profileid=138936
https://chodilinh.com/members/fly88no1com.307040/#about
https://log.concept2.com/profile/2945367
https://medium.com/@fly88no1com/about
https://3dwarehouse.sketchup.com/by/fly88no1com
https://poipiku.com/13626715/
https://www.simplexthailand.com/forum/topic/27357/fly88
https://www.milliescentedrocks.com/board/board_topic/2189097/8327478.htm
https://www.ekdarun.com/forum/topic/163013/fly88no1com
https://forum.aigato.vn/user/fly88no1com
https://www.zumvu.com/fly88no1com/
https://www.myebook.com/user_profile.php?id=fly88no1com
https://www.udrpsearch.com/user/fly88no1com
https://www.skypixel.com/users/djiuser-tribsgdjmjgj
https://www.bmwpower.lv/user.php?u=fly88no1com
https://pinshape.com/users/8969376-fly88no1com?tab=designs
https://pika-network.net/members/fly88no1com.413373/#about
https://sketchersunited.org/users/323321
http://www49.atwiki.org/fateextraccc/index.php?fly88no1com
https://booklog.jp/users/fly88no1com/profile
https://library.zortrax.com/members/fly88-73/
https://pixelfed.uno/fly88no1com
https://makerworld.com/en/@fly88no1com
https://biomolecula.ru/authors/148258
https://www.harimajuku.com/profile/fly88no1com/profile
https://expathealthseoul.com/profile/fly88no1com/
https://niflheim.world/members/fly88no1com.55271/about
https://gifyu.com/fly88no1com
https://zerosuicidetraining.edc.org/user/profile.php?id=567946
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8322326.htm?page=1
https://justpaste.it/u/fly88no1com
https://www.thitrungruangclinic.com/forum/topic/139504/fly88no1com
https://www.thepartyservicesweb.com/board/board_topic/3929364/8322513.htm?page=1
https://www.fuelly.com/driver/fly88no1com
https://www.bonback.com/forum/topic/427812/fly88no1com
https://fabble.cc/fly88no1com
http://onlineboxing.net/jforum/user/editDone/457773.page
https://www.beamng.com/members/fly88-trang-ch%E1%BB%A7-nh%C3%A0.795262/
https://vietcurrency.vn/members/fly88no1com.241547/#about
https://www.arriba420.com/profile/fly88no1com/profile
https://writexo.com/share/88743c76e386
https://www.themirch.com/blog/author/fly88no1com/
https://www.d-ushop.com/forum/topic/143862/fly88no1com
https://www.coffeesix-store.com/board/board_topic/7560063/8322658.htm?page=1
https://www.driedsquidathome.com/forum/topic/154712/fly88no1com
https://fact-finder.xyz/pukiwiki/?fly88no1com
https://idol.st/user/175564/fly88no1com/
https://giloo.ist/member/fly88no1com/?mainTab=notes&subTab=my_notes
https://www.sunemall.com/board/board_topic/8431232/8322732.htm?page=1
https://www.grepmed.com/fly88no1com
https://acomics.ru/-fly88no1com
http://jobboard.piasd.org/author/fly88no1com/
https://act4sdgs.org/profile/fly88_trang_ch_nha_cai_ca_c_c_tr_c_tuy_n_uy_tin_s_1_chau_a
https://bit.ly/m/fly88no1com
https://ac.db0.company/user/12094/fly88no1com/
https://www.intensedebate.com/people/fly88no1com1
https://pictureinbottle.com/r/fly88no1com
https://heylink.me/fly88no1com/
https://www.proko.com/@fly88no1com/activity
https://www.green-collar.com/forums/users/neko96/
https://bbs.theviko.com/home.php?mod=space&uid=4693248
https://www.trackyserver.com/profile/252555
https://www.ganjingworld.com/channel/1iho7jockm732D3JXtoDsBoxG1hd0c?subTab=all&tab=about&subtabshowing=latest&q=
https://tooter.in/fly88no1com
https://theafricavoice.com/profile/https:fly88-no1.com
https://zbrushcentral.jp/user/fly88no1com
https://www.simplexthailand.com/forum/topic/27297/fly88no1com
https://nogu.org.uk/forum/profile/fly88no1com/
https://www.instructorsnearme.com/author/fly88no1com/
https://cinderella.pro/user/276829/fly88no1com/#preferences
https://gitlab.com/fly88no1com
https://www.gta5-mods.com/users/fly88no1com
https://jo-el.es/user/fly88no1com
https://portfolium.com/mepupeteye20
https://app.readthedocs.org/profiles/fly88no1com/
https://sklad-slabov.ru/forum/user/46498/
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=305862
https://www.shippingexplorer.net/en/user/fly88no1com/288663
https://fiat-freemont-club.ru/profile.php?section=about&id=14125
https://copynotes.be/shift4me/forum/user-55934.html
https://www.heavyironjobs.com/profiles/8276855-fly88
https://mail.protospielsouth.com/user/135209
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=504949
https://www.ekdarun.com/forum/topic/162986/fly88
https://fly88no1com.tistory.com/1
https://mez.ink/fly88no1com
https://www.sythe.org/members/fly88no1com.2051567/
https://blogfreely.net/fly88no1com/
https://postheaven.net/fly88no1com/
https://telegra.ph/fly88-05-14
https://fly88no1com.webflow.io/
https://pad.degrowth.net/s/gRkn-peVx
https://schoolido.lu/user/fly88no1com/
https://www.nicovideo.jp/user/144230393
https://md.chaosdorf.de/s/69ZtuuQ9M0
https://www.renderosity.com/users/id:1858954
https://pad.codefor.fr/s/zw5e9_yLlz
https://safechat.com/u/fly88.trang.chu.nha.cai.ca.cuoc.truc.tuyen.uy.tin.so.1.chau.a
https://6a058df747902.site123.me/articles/fly88-trang-ch%E1%BB%A7-nh%C3%A0-c%C3%A1i-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-uy-t%C3%ADn-s%E1%BB%91-1-ch%C3%A2u-%C3%81
https://doc.adminforge.de/s/jPIM5zMiMZ
https://fly88no1com.notepin.co/
https://pad.flipdot.org/s/-BcFfOE6Bw
https://www.montessorijobsuk.co.uk/author/fly88no1com/
https://pad.libreon.fr/s/WQyvg2Iwah
https://anotepad.com/notes/mir25t27
https://md.chaospott.de/s/WNUCTv-Y2n
https://telescope.ac/fly88no1com/o461wzrchwxtsitl04h5b8
https://fly88no1com.mystrikingly.com/
https://experiment.com/users/fly88no1com
https://hackmd.io/@fly88no1com/fly88no1com
https://padlet.com/mepupeteye20/fly88-xveuhk7149tcr92n/wish/YDgnZe1obd1oZwrA
https://diigo.com/012l42r
https://confengine.com/user/fly88no1com
https://espritgames.com/members/51120446/
https://tudomuaban.com/chi-tiet-rao-vat/2906137/fly88no1com.html
https://flipboard.social/@fly88no1com
https://paste.lightcast.com/view/b9226b1a
https://www.telerik.com/forums/profile/26892b96-3c23-4af6-b2ff-519e2a6a0d05
https://chillspot1.com/user/fly88no1com
https://supplyautonomy.com/7db238a1ec980d53e9e17e209fbe4ab72c308e6c.vn
http://worldchampmambo.com/UserProfile/tabid/42/userId/491649/Default.aspx
https://onlinesequencer.net/members/274748
http://gojourney.xsrv.jp/index.php?fly88no1com
https://www.racerjobs.com/profiles/8276440-fly88
https://bookmarkport.com/story24277671/fly88
https://slackcommunity.com/u/mpzeve/#/about
https://www.funsocio.com/fly88no1com
https://www.dailymotion.com/user/fly88no1com
https://krachelart.com/UserProfile/tabid/43/userId/1346393/Default.aspx
https://builtbybit.com/members/fly88no1com.810300/#about
https://www.noteflight.com/profile/4291c3c7109b247fe7182782b4b668e87cb39b99
https://bizidex.com/en/fly88-apartments-949205
http://nao.earth/index.php?fly88no1com
https://www.lwn3d.com/forum/topic/68734/fly88
https://topkif.nvinio.com/fly88no1com
https://fly88no1com.blogpayz.com/41588730/fly88
https://ask.mallaky.com/?qa=user/fly88no1com
https://www.huntingnet.com/forum/members/fly88no1com.html
https://papers-please.info/?fly88no1com
https://www.vrwant.org/wb/home.php?mod=space&uid=5136137
https://www.codementor.io/@mepupeteye20
http://www.daojianchina.com/home.php?mod=space&uid=1107864
http://mura.hitobashira.org/index.php?fly88no1com
https://www.spoonflower.com/profiles/fly88no1com?sub_action=shop
https://bbs.darkml.net/home.php?mod=space&uid=165801
https://www.webmastersun.com/members/fly88no1com.165888/#about
https://www.demilked.com/author/fly88no1com/
https://www.jointcorners.com/fly88no1com
https://www.babelcube.com/user/fly88-trang-chu-nha-cai-ca-cuoc-truc-tuyen-uy-tin-so-1-chau-a
https://www.deviantart.com/fly88no1com
https://seomotionz.com/member.php?action=profile&uid=132056
https://www.prshine.com/profile/fly88no1com
https://www.inkitt.com/fly88no1com
https://ko-fi.com/fly88no1com
https://forum.uookle.com/home.php?mod=space&uid=1464145
https://nhattao.com/members/user6970522.6970522/
https://expressafrica.net/fly88no1com
https://entre-vos-mains.alsace.eu/profiles/fly88no1com/activity
https://friendtalk.mn.co/members/39711288
https://infiniteabundance.mn.co/members/39711197
https://truckymods.io/user/495904
https://www.popdaily.com.tw/user/535157
http://julia4tied.de/member.php?action=profile&uid=248522
https://bpa-mastery.mn.co/members/39715163
https://hker2uk.com/home.php?mod=space&uid=5566102
https://foss.heptapod.net/fly88no1com
https://anunt-imob.ro/user/profile/858877
https://in.enrollbusiness.com/BusinessProfile/7806642/FLY88
https://linkmate.mn.co/members/39715147
https://volleypedia.org/index.php?qa=user&qa_1=fly88no1com
https://armchairjournal.com/forums/users/fly88no1com/
https://bbcovenant.guildlaunch.com/users/blog/6757819/2524298/fly88/?gid=97523
https://globalaffairs.mn.co/members/39715169
https://videos.muvizu.com/Profile/fly88no1com/Latest/
https://participationcitoyenne.rillieuxlapape.fr/profiles/fly88no1com/activity
https://forums.servethehome.com/index.php?members/fly88no1com.244621/#about
https://socialvias.com/fly88no1com
https://maxforlive.com/profile/user/fly88no1com?tab=about
https://eo-college.org/members/fly88no1com/
https://eternagame.org/players/622291
https://www.dokkan-battle.fr/forums/users/fly88no1com/
https://www.video-bookmark.com/bookmark/7131127/fly88/
https://culturesbook.com/fly88no1com
https://jszst.com.cn/home.php?mod=space&uid=6919295
https://faceout.mn.co/members/39715159
https://www.rctech.net/forum/members/fly88no1com-551632.html
https://comunitat.canodrom.barcelona/profiles/fly88no1com/activity?locale=en
https://maiotaku.com/p/fly88no1com
Saya tertarik bahwa saya menemukan situs web ini, tepat informasi yang saya cari!
Saya biasanya tidak menulis komentar, tetapi yang satu ini benar-benar pantas. Isi yang luar biasa dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya selalu mencari online untuk tips yang dapat membantu saya. Terima kasih!
Saya tidak sering berkomentar tetapi saya harus mengakui salam untuk posting yang spesial ini : D.
Hey there excellent blog! Does running a blog like this take a lot of work?
I’ve no expertise in computer programming
however I was hoping to start my own blog in the near future.
Anyways, should you have any recommendations or tips for new blog owners
please share. I know this is off subject however I simply had to ask.
Cheers!
Undeniably believe that which you said. Your favorite reason appeared to be on the internet the easiest thing to be aware of. I say to you, I certainly get irked while people consider worries that they plainly don’t know about. You managed to hit the nail upon the top as well as defined out the whole thing without having side effect , people could take a signal. Will probably be back to get more. Thanks
Halo di sana, saya menjumpai blog Anda lewat Google saat mencari subjek yang mirip, website Anda muncul di posisi atas. Saya perlu mengatakan bahwa saya terkejut betapa rapi pengaturannya. Saya benar-benar menikmati membaca ini dan saya pasti akan kembali untuk melihat konten lainnya. Terima kasih banyak!
Bernilai informasi. Beruntung saya menemukan situs Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Luar biasa! Blog ini terlihat tepat seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang luar biasa!
Wow! Terima kasih! Saya senantiasa membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya mengambil sebagian dari posting Anda ke situs saya?
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Postingan yang sangat berguna. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Saya selalu tertarik dengan topik ini dan masih demikian, terima kasih telah memposting.
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi luar biasa dibagikan secara bebas.
Hi, Neat post. There’s an issue together with your site in web explorer, could test thisK IE still is the market leader and a large component of folks will omit your magnificent writing because of this problem.
Wow, superb weblog struktur! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan web site Anda hebat, belum lagi kontennya!
Saya melihat banyak website tetapi saya percaya yang satu ini memiliki sesuatu yang spesial di dalamnya
Having read this I thought it was very informative. I appreciate you taking the time and effort to put this article together. I once again find myself spending way to much time both reading and commenting. But so what, it was still worth it!
Mengagumi usaha yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda sajikan. Sangat bagus menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Saya secara berkelanjutan melihat online untuk tips yang dapat memberi manfaat saya. Terima kasih!
Saya mengunjungi banyak website tetapi saya anggap yang satu ini memiliki sesuatu yang ekstra di dalamnya
Saya tidak biasanya berkomentar tetapi saya harus mengakui salam untuk posting yang sempurna ini : D.
You are my inhalation, I possess few web logs and rarely run out from post :). “Analyzing humor is like dissecting a frog. Few people are interested and the frog dies of it.” by E. B. White.
As I website possessor I think the written content here is rattling wonderful, thankyou for your efforts.
It is appropriate time to make some plans for the future and it’s time to be happy. I have read this post and if I could I wish to suggest you few interesting things or tips. Perhaps you can write next articles referring to this article. I wish to read more things about it!
I think the admin of this site is in fact working hard for his web page, since here every stuff is quality based stuff.
I believe this site has got some real superb info for everyone :D.
This design is wicked! You obviously know how to keep a reader entertained. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Fantastic job. I really loved what you had to say, and more than that, how you presented it. Too cool!
Wow that was strange. I just wrote an incredibly long comment but after I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyhow, just wanted to say excellent blog!
dating+coach+Dating+Coach+LA+is+a+well-known+dating+coaching+provider+in+Los+Angeles+CA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
I visited a lot of website but I believe this one has got something special in it in it
Simply wish to say your article is as amazing. The clearness in your
submit is simply nice and that i could assume you’re an expert in this subject.
Fine along with your permission allow me to snatch your feed to stay updated with coming
near near post. Thank you a million and please
carry on the rewarding work.
Hi! I realize this is somewhat off-topic however I needed to ask.
Does building a well-established website like yours take a massive amount work?
I’m brand new to running a blog however I do write in my journal everyday.
I’d like to start a blog so I can easily share my own experience and views
online. Please let me know if you have any ideas or tips for brand new aspiring blog
owners. Appreciate it!
Real excellent visual appeal on this site, I’d rate it 10 10.
I’ve been surfing on-line greater than three hours as of late, but I by no means found any attention-grabbing article like yours. It is lovely value sufficient for me. In my opinion, if all website owners and bloggers made excellent content as you probably did, the internet shall be a lot more useful than ever before. “No nation was ever ruined by trade.” by Benjamin Franklin.
I gotta favorite this website it seems very useful invaluable
Sangat indah info dapat ditemukan di web blog.
Mengagumi kerja keras yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda berikan. Sangat hebat menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
fantastic points altogether, you just gained a new reader. What may you recommend in regards to your post that you just made some days in the past? Any certain?
Wow! Terima kasih! Saya secara terus membutuhkan menulis di situs saya sesuatu seperti itu. Bolehkah saya menerapkan bagian dari posting Anda ke situs saya?
Normally I don’t learn article on blogs, but I would like to say that this write-up very compelled me to take a look at and do so! Your writing style has been surprised me. Thanks, quite nice article.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Saya selalu tertarik dengan subjek ini dan tetap masih demikian, terima kasih telah mengunggah.
Hello, There’s no doubt that your blog may be having browser compatibility problems.
When I take a look at your website in Safari, it looks fine however, when opening in IE, it has some overlapping issues.
I simply wanted to provide you with a quick heads
up! Besides that, excellent website!
Sangat menarik poin yang Anda amati, thankyou telah mengunggah.
Saya amat bersyukur menemukan situs ini di Bing, persis seperti yang saya telusuri : D selain itu sudah saya simpan di bookmark saya.
What’s up friends, fastidious post and good urging commented at this place, I am really enjoying
by these.
I consider something truly special in this website .
I absolutely love your blog and find the majority of your post’s to be just what I’m looking for. Does one offer guest writers to write content for yourself? I wouldn’t mind composing a post or elaborating on some of the subjects you write concerning here. Again, awesome weblog!
Postingan yang hebat! Saya menghargai gaya Anda menguraikan semuanya dengan sangat jelas. Teruskan kerja yang hebat!
Menikmati mempelajari ini, sangat bagus, terima kasih.
Some times its a pain in the ass to read what people wrote but this website is very user friendly! .
Konten yang bermanfaat dan ditulis dengan sangat baik. Saya pasti akan membagikan ini kepada orang lain. Terima kasih telah berbagi.
dating+coach+Dating+Coach+LA+is+a+established+dating+coach+provider+in+Los+Angeles+CA+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Dating Coach LA provides skilled dating guidance in Los Angeles, CA.
Dating Coach LA enables clients to establish their dating goals.
The Dating Coach LA from Dating Coach LA offers personalized therapy to handle dating issues.
Dating Coach LA supports individuals in finding love with confidence.
The Dating Coach LA at Dating Coach LA delivers helpful feedback on dating apps.
Dating Coach LA simplifies workshops to boost confidence when attracting potential partners.
The Dating Coach LA from Dating Coach LA assists clients to understand dating psychology.
Dating Coach LA offers an authentic approach to dating
coaching. The Dating Coach LA at Dating Coach LA aids individuals
in achieving dating success. Dating Coach LA enables clients
to navigate the dating scene in Los Angeles,
CA. The Dating Coach LA from Dating Coach LA delivers expert assistance for dating coach in LA.
Dating Coach LA offers resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA supports clients in setting realistic dating expectations.
Dating Coach LA facilitates the development of effective dating strategies.
The Dating Coach LA from Dating Coach LA enables clients to achieve their
dating goals. Dating Coach LA delivers guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA offers comprehensive
coaching services to clients in Los Angeles, CA.
Hello. splendid job. I did not anticipate this. This is a great story. Thanks!
This is the right blog for anyone who wants to find out about this topic. You realize so much its almost hard to argue with you (not that I actually would want…HaHa). You definitely put a new spin on a topic thats been written about for years. Great stuff, just great!
Dating Coach LA provides skilled dating advice in Los Angeles,
CA. Dating Coach LA allows clients to establish their dating goals.
The Dating Coach LA from Dating Coach LA delivers personalized therapy to handle dating
issues. Dating Coach LA supports individuals in finding love
with confidence. The Dating Coach LA at Dating Coach LA provides valuable feedback on dating apps.
Dating Coach LA facilitates workshops to boost confidence when attracting potential partners.
The Dating Coach LA from Dating Coach LA assists clients to understand dating psychology.
Dating Coach LA provides an authentic approach to dating coaching.
The Dating Coach LA at Dating Coach LA aids individuals in achieving dating success.
Dating Coach LA empowers clients to navigate the dating scene
in Los Angeles, CA. The Dating Coach LA from
Dating Coach LA offers expert assistance for dating coach in LA.
Dating Coach LA delivers resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA assists clients in setting realistic dating expectations.
Dating Coach LA facilitates the development of effective dating
strategies. The Dating Coach LA from Dating Coach LA enables clients
to achieve their dating goals. Dating Coach LA provides guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA delivers thorough
coaching services to clients in Los Angeles, CA.
You really make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand.
It seems too complicated and very broad for me. I am looking forward for your next post,
I will try to get the hang of it!
Saya sangat menghargai waktu yang Anda luangkan untuk menyusun posting ini. Konten yang berguna. Terima kasih!
Nyata jelas web site, terima kasih untuk posting ini.
Terima kasih, saya baru saja menelusuri informasi tentang subjek ini sudah lama dan milik Anda adalah yang paling hebat yang saya jumpai hingga sekarang. Tapi, bagaimana dengan inti permasalahan? Apakah Anda positif tentang sumber tersebut?
Isi yang bermanfaat dan disajikan dengan baik. Saya tentu akan membagikan ini kepada rekan-rekan. Terima kasih telah berbagi.
I have been exploring for a little for any high-quality articles or blog posts on this sort of area . Exploring in Yahoo I at last stumbled upon this web site. Reading this information So i am happy to convey that I’ve a very good uncanny feeling I discovered exactly what I needed. I most certainly will make sure to do not forget this web site and give it a glance on a constant basis.
I do enjoy the way you have framed this particular difficulty plus it does indeed offer me some fodder for consideration. Nonetheless, through just what I have personally seen, I just simply hope as the commentary stack on that people today keep on point and don’t start on a soap box involving the news du jour. Still, thank you for this outstanding point and whilst I do not really agree with this in totality, I respect the viewpoint.
Fantastic goods from you, man. I’ve have in mind your stuff prior to and you’re simply too magnificent. I actually like what you’ve got right here, certainly like what you are saying and the way in which wherein you assert it. You are making it enjoyable and you still care for to stay it sensible. I can’t wait to learn far more from you. This is actually a great site.
Halo semua, kamu sudah melakukan pekerjaan yang hebat. Saya tentu akan menandai ini dan kembali untuk membaca konten lainnya. Terima kasih!
It genuinely surprised me when I stumbled onto a fresh online casino site that had an atmosphere that pulled me
in emotionally.
Honestly, I was skeptical, but the crazy number of titles — so many
that scrolling felt endless — kept me exploring.
The welcome offer felt like a real push, and as soon as I
activated it, I finally understood why people talk about good bonuses.
The requirements weren’t exactly relaxed, but I just treated it like part of the experience.
What really caught me emotionally was how smooth the withdrawals were.
A day or two later, I saw the payout confirmed, and that moment felt reassuring.
The VIP program was another unexpected thing.
I never cared much for VIP stuff, but the gradual rewards actually added
real value.
Getting back regular cashback packages made my sessions less stressful, and I actually enjoyed the
grind.
The game variety overwhelmed me at first — in a good way.
Every session felt different because the library was massive.
Other times I’d hunt for higher-RTP options, and there was always something new to try.
What also surprised me was how many payment methods they supported.
For me, waiting kills enthusiasm, so the crypto support made the sessions
start without delay.
Of course, it wasn’t perfect.
Some game info wasn’t detailed.
And I had to search around for regulatory info.
But emotionally?
Despite the flaws, I kept coming back.
If you’re reading this because you’re curious, from my own experience
— this platform gave me some of the most memorable
gaming moments I’ve had online.
And yes, there’s a link in the comment, so give it a look if you’re curious.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Ini benar-benar menjawab masalah saya, terima kasih!
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang luar biasa dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Sangat menarik detail yang Anda sebutkan, sangat menghargai telah mengunggah.
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini merupakan tepat jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
This is very fascinating, You are a very professional blogger.
I’ve joined your feed and look forward to in quest of extra of your great
post. Also, I’ve shared your website in my social networks
Wow! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang hebat!
Seseorang secara esensial menolong untuk membuat secara signifikan artikel saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman web Anda dan sampai saat ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat unggahan menakjubkan ini. Proses yang luar biasa!
Saya kebetulan menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang hebat.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Konten yang hebat! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
After checking out a handful of the blog articles on your site, I really
appreciate your way of writing a blog. I book marked it to my bookmark site list and
will be checking back soon. Take a look at my website too and
let me know how you feel.
Seseorang secara esensial membantu untuk membuat secara signifikan posting saya mungkin katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga sekarang? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi menakjubkan ini. Pekerjaan yang sangat baik!
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang hebat!
Ya menyimpan ini bukanlah kesimpulan yang spekulatif pos yang hebat! .
I am not very good with English but I find this rattling easy to translate.
I like the efforts you have put in this, appreciate it for all the great blog posts.
I like this blog so much, saved to my bookmarks. “American soldiers must be turned into lambs and eating them is tolerated.” by Muammar Qaddafi.
Terima kasih atas artikel yang hebat. Saya benar-benar menikmati membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan pekerjaan yang bagus!
Wohh baru saja apa yang saya cari, terima kasih atas posting.
You are a very intelligent person!
Saya senang menjadi salah satu dari beberapa pengunjung di website luar biasa ini (:, salam telah mengunggah.
Wow! Terima kasih! Saya selalu membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke website saya?
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi sangat baik dibagikan secara bebas.
Saya tidak sering berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang hebat ini : D.
Absolutely indited subject material, thankyou for selective information.
This web site is my intake, rattling fantastic design and perfect content.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Mengagumkan. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Saya tertarik bahwa saya menemukan kembali blog ini, tepat info yang saya cari!
Kami dapat memiliki hyperlink perubahan perjanjian antara kita!
dating+coach+Dating+Coach+LA+is+trusted+by+dating+coaches+people+in+Los+Angeles+California+Dating+Coach+LA+355+S+Grand+Ave+%23469%2C+Los+Angeles%2C+CA+90071%2C+United+States
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar pantas. Konten yang hebat dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Artikel yang sangat baik. Ini jelas ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
When I initially commented I clicked the -Notify me when new feedback are added- checkbox and now each time a comment is added I get 4 emails with the same comment. Is there any way you possibly can take away me from that service? Thanks!
Great post. I am facing a couple of these problems.
Saya terkesan dengan situs ini, sangat saya adalah penggemar berat.
Nyata fantastis informasi dapat ditemukan di web blog.
Saya sangat menghargai waktu yang Anda curahkan untuk menyusun posting ini. Konten yang sangat berharga. Terima kasih banyak!
It’s appropriate time to make some plans for the long run and it’s time to be happy. I’ve learn this put up and if I may I wish to counsel you few attention-grabbing issues or advice. Perhaps you can write next articles relating to this article. I wish to learn even more issues approximately it!
Ya menyimpan ini bukanlah penentuan yang spekulatif posting yang hebat! .
I reckon something genuinely interesting about your website so I saved to bookmarks.
Saya tidak biasanya berkomentar tetapi saya harus menyatakan terimakasih untuk posting yang spesial ini : D.
Artikel yang luar biasa. Saya sungguh menikmati cara Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang hebat!
Saya senang menjadi salah satu dari banyak pengunjung di website hebat ini (:, terima kasih telah mengunggah.
Saya senang menjadi pengunjung dari blog total ini!, terima kasih atas informasi langka ini!
Konten yang bermanfaat dan disajikan dengan baik. Saya tentu akan membagikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
F*ckin’ amazing issues here. I’m very satisfied to see your post. Thank you so much and i’m having a look ahead to contact you. Will you kindly drop me a e-mail?
As I web-site possessor I believe the content matter here is rattling wonderful , appreciate it for your hard work. You should keep it up forever! Best of luck.
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar pantas. Konten yang hebat dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Wohh baru saja apa yang saya telusuri, terimakasih atas unggahan.
Hai di sana, Anda telah melakukan pekerjaan yang fantastis. Saya tentu akan mem-bookmark ini dan kembali untuk melihat konten lainnya. Terima kasih banyak!
Isi yang bermanfaat dan ditulis dengan baik. Saya pasti akan membagikan ini kepada rekan-rekan. Terima kasih banyak telah berbagi.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Informasi yang berguna. Saya baru mencari hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Can I just say what a reduction to find somebody who truly is aware of what theyre speaking about on the internet. You undoubtedly know the right way to convey a difficulty to mild and make it important. More folks have to learn this and perceive this facet of the story. I cant believe youre not more common because you undoubtedly have the gift.
Good day! I know this is kinda off topic but I’d figured I’d ask. Would you be interested in exchanging links or maybe guest authoring a blog post or vice-versa? My blog covers a lot of the same topics as yours and I feel we could greatly benefit from each other. If you’re interested feel free to shoot me an e-mail. I look forward to hearing from you! Fantastic blog by the way!
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan berterima kasih kepada Anda.
fantastic post, very informative. I wonder why the other specialists of this sector don’t notice this. You must continue your writing. I’m confident, you’ve a great readers’ base already!
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada metode Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Saya terkesan dengan situs internet ini, amat saya adalah penggemar berat.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
This is really interesting, You’re a very skilled blogger.
I’ve joined your rss feed and look forward to seeking more of your
excellent post. Also, I have shared your website
in my social networks!
Ini adalah blog yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga hampir sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar hebat!
I’ve been absent for a while, but now I remember why I used to love this website. Thanks , I will try and check back more often. How frequently you update your web site?
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
I would like to thnkx for the efforts you’ve put in writing this site. I am hoping the same high-grade site post from you in the upcoming also. Actually your creative writing abilities has inspired me to get my own blog now. Actually the blogging is spreading its wings rapidly. Your write up is a great example of it.
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Saya tidak sangat fantastis dalam bahasa Inggris tetapi saya menganggap ini benar-benar ringan untuk diterjemahkan.
Simply wanna admit that this is invaluable, Thanks for taking your time to write this.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
I’m really enjoying the design and layout of your site. It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did you hire out a designer to create your theme? Fantastic work!
Saya senang menjadi salah satu dari banyak pengunjung di website hebat ini (:, salam telah mengunggah.
Saya mengunjungi banyak website tetapi saya pikir yang satu ini punya sesuatu yang spesial di dalamnya
Ini adalah blog yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga hampir sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
I’m curious to find out what blog platform you are using? I’m having some minor security problems with my latest website and I would like to find something more risk-free. Do you have any recommendations?
Bernilai info. Beruntung saya menemukan website Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Saya mendapatkan info yang bagus dari blog Anda.
You are my aspiration, I have few blogs and occasionally run out from to post : (.
Your comment is awaiting moderation.
https://www.facebook.com/ao88yucom/
https://www.youtube.com/@ao88yucom
https://x.com/ao88yucom
https://wakelet.com/@ao88yucom
https://safechat.com/u/ao88yucom
https://www.blogger.com/profile/15185449343016861003
https://www.pinterest.com/ao88yucom/
https://community.wongcw.com/ao88yucom
https://demo.wowonder.com/ao88yucom
https://shareyoursocial.com/ao88yucom
https://500px.com/p/ao88yucom
https://magic.ly/ao88yucom
https://hackaday.io/ao88yucom
https://leetcode.com/u/ao88yucom/
https://audiomack.com/ao88yucom
https://protocol.ooo/ja/users/ao88yucom
https://portfolium.com/ao88yucom
https://www.blockdit.com/ao88yucom
https://www.tumblr.com/ao88yucom
https://gravatar.com/ao88yucom
https://www.instapaper.com/p/ao88yucom1
https://swag.live/en/user/69f73737bbd85c200da811cf
https://www.halaltrip.com/user/profile/345173/ao88yucom1/
https://medibang.com/author/28231558/
https://opensea.io/ao88yucom1
https://groups.google.com/g/ao88yucom1/c/QXaaJMv_i5E
https://www.twitch.tv/ao88yucom1/about
https://profile.hatena.ne.jp/ao88yucom1/
https://issuu.com/ao88yucom1
https://www.behance.net/ao88yucom1
https://www.reverbnation.com/ao88yucom1
https://www.myminifactory.com/users/ao88yucom1
https://www.investagrams.com/Profile/ao88yucom1
https://gifyu.com/ao88yucom1
https://www.chordie.com/forum/profile.php?id=2521488
https://skitterphoto.com/photographers/2664831/ao88
https://www.walkscore.com/people/650389447888/ao88
https://akniga.org/profile/1420249-ao88/
https://disqus.com/by/ao88yucom1/about/
https://jobs.suncommunitynews.com/profiles/8225830-trang-ch-ao88
https://www.speedrun.com/users/ao88yucom1
https://slides.com/ao88yucom1
https://www.aicrowd.com/participants/ao88yucom1
https://www.bitchute.com/channel/sjJBtVOg8zRT
https://hub.docker.com/u/ao88yucom1
https://spiderum.com/nguoi-dung/ao88yucom1
https://www.gta5-mods.com/users/ao88yucom
https://heylink.me/ao88yucom1
https://pixabay.com/users/ao88yucom1-55710649/
https://www.nicovideo.jp/user/144132481
https://3dwarehouse.sketchup.com/by/ao88yucom1
https://robertsspaceindustries.com/en/citizens/ao88yucom1
https://bit.ly/3QXSTva
https://joy.bio/ao88yucom1
https://connect.garmin.com/app/profile/b0b6e704-42a8-49e5-9eab-11343c5bbc48
https://b.hatena.ne.jp/ao88yucom1/bookmark
https://www.chichi-pui.com/users/ao88yucom1/
https://www.openrec.tv/user/ao88yucom1
https://unityroom.com/users/ao88yucom1
https://pxhere.com/en/photographer-me/5002888
https://teletype.in/@ao88yucom1
https://www.nintendo-master.com/profil/ao88yucom1
https://freeimage.host/ao88yucom1
https://motion-gallery.net/users/976579
https://linkin.bio/ao88yucom1/
https://talk.plesk.com/members/aoyucom.505367/#about
https://www.callupcontact.com/b/businessprofile/Trang_ch_AO88/10077513
https://blender.community/ao88yucom1/
https://doselect.com/@8d4490c19fbd960049e90ce0f
https://sciter.com/forums/users/ao88yucom1/
https://matkafasi.com/user/ao88yucom1
https://allmyfaves.com/ao88yucom
https://www.notebook.ai/@ao88yucom1
https://www.abclinuxu.cz/lide/ao88yucom1
https://dumagueteinfo.com/author/ao88yucom1/
https://muare.vn/shop/landon-henning/904080
https://doodleordie.com/profile/ao88yucom1
https://www.intensedebate.com/people/ao88yucom1
https://igli.me/ao88yucom1
http://delphi.larsbo.org/user/ao88yucom1
https://www.aseeralkotb.com/en/profiles/ao88yucom1
https://timdaily.vn/members/ao88yucom1.135654/#about
https://app.readthedocs.org/profiles/ao88yucom1/
https://iszene.com/user-350481.html
https://www.roton.com/forums/users/henninglandon735/
https://able2know.org/user/ao88yucom/
https://chuanmen.edu.vn/members/ao88yucom.30376/
https://www.bls.gov/bls/exit_BLS.htm?url=https://ao88-yu.com/
https://pad.fablab-siegen.de/s/bdvNZYP17F
https://pad.darmstadt.social/s/Uq2MpFDGfP
https://md.opensourceecology.de/s/TIQGok8gu
http://www.biblesupport.com/user/835714-ao88yucom/
https://golosknig.com/profile/ao88yucom/
https://www.anibookmark.com/user/ao88yucom.html
https://www.inventoridigiochi.it/membri/ao88yucom/profile/
https://forum.m5stack.com/user/ao88yucom
https://ngel.ink/ao88yucom
https://jali.pro/ao88yucom
https://qoolink.co/ao88yucom
https://bioqoo.com/ao88yucom
https://jaga.link/ao88yucom
https://biolinku.co/ao88yucom
https://jali.me/ao88yucom
https://alumni.skema.edu/global/redirect.php?url=https://ao88-yu.com/
https://bandori.party/user/885190/ao88yucom
https://community.m5stack.com/user/ao88yucom
https://schoolido.lu/user/ao88yucom/
https://fortunetelleroracle.com/profile/ao88yucom
https://fabble.cc/ao88yucom
https://scripts.mit.edu/trac/search?aff-387363&q=https://ao88-yu.com/
https://vozer.net/members/ao88yucom.90543/#about
https://affariat.com/user/profile/180654
https://community.cisco.com/t5/user/viewprofilepage/user-id/2072231
https://kr.pinterest.com/ao88yucom/
https://pt.gravatar.com/ao88yucom
https://th.gravatar.com/ao88yucom
https://violet.vn/user/show/id/15271913
https://tulieu.violet.vn/user/show/id/15271913
https://beteiligung.amt-huettener-berge.de/profile/ao88yucom/
https://app.brancher.ai/user/KKbucQF4uDyZ
https://ctxt.io/2/AAAEcOVKFQ
https://www.newgenstravel.com/forum/topic/45213/ao88yucom
https://www.dideadesign.com/forum/topic/44324/ao88yucom
https://justpaste.me/Jdkk4
https://de.pinterest.com/ao88yucom/
https://co.pinterest.com/ao88yucom/
https://cl.pinterest.com/ao88yucom/
https://f319.com/members/ao88yucom.1103951/
https://about.me/ao88yucom
https://booklog.jp/users/ao88yucom/profile
https://www.equinenow.com/farm/ao88yucom.htm
https://wefunder.com/ao88yucom
https://potofu.me/ao88yucom
https://transfur.com/Users/ao88yucom
https://xtremepape.rs/members/ao88yucom.670594/#about
https://myanimelist.net/profile/ao88yucom
https://qna.habr.com/user/ao88yucom
https://pad.itiv.kit.edu/s/YQwWA2wPl
https://doc.anagora.org/s/ypkGTC-Z9
https://tutos.cemea.org/s/QRRmiYA1q
https://uk.pinterest.com/ao88yucom/
https://website.informer.com/ao88-yu.com
https://beacons.ai/ao88yucom
https://en.islcollective.com/portfolio/12914195
https://www.xosothantai.com/members/ao88yucom.611802/
https://velog.io/@ao88yucom/posts
https://iplogger.org/vn/logger/VG1T58tCrlqN/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3962613
https://mez.ink/ao88yucom
https://se.pinterest.com/ao88yucom/
https://mx.pinterest.com/ao88yucom/
https://es.pinterest.com/ao88yucom/
https://notionpress.com/author/1515945
https://www.edna.cz/uzivatele/ao88yucom/
https://digiphoto.techbang.com/users/ao88yucom
https://i.techbang.com/users/ao88yucom
https://leakedmodels.com/forum/members/ao88yucom.712131/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1071110
https://freeicons.io/profile/926734
https://id.pinterest.com/ao88yucom/
https://jobs.westerncity.com/profiles/8226699-nha-cai-ao88
https://www.thepartyservicesweb.com/board/board_topic/3929364/8259681.htm
https://ph.pinterest.com/ao88yucom/
https://pt.pinterest.com/ao88yucom/
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8259677.htm
https://www.crossroadsbaitandtackle.com/board/board_topic/9053260/8259678.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8259679.htm
https://inkbunny.net/ao88yucom
https://www.japaaan.com/user/78805
https://spinninrecords.com/profile/ao88yucom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.ao8813
https://beatsaver.com/playlists/1194667
https://apptuts.bio/ao88yucom-262737
https://dialog.eslov.se/profiles/ao88yucom/activity
https://www.storenvy.com/ao88yucom
https://participacion.cabildofuer.es/profiles/ao88yucom/activity
https://forums.maxperformanceinc.com/forums/member.php?u=248207
https://egl.circlly.com/users/ao88yucom
https://goodandbadpeople.com/ao88yucom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=303520
https://www.sciencebee.com.bd/qna/user/ao88yucom
https://acomics.ru/-ao88yucom
https://nl.pinterest.com/ao88yucom/
https://au.pinterest.com/ao88yucom/
https://ca.pinterest.com/ao88yucom/
https://forums.ashesofthesingularity.com/user/7665436
https://forums.wincustomize.com/user/7665436
https://md.coredump.ch/s/RBO4eq5JY
https://md.un-hack-bar.de/s/4Sl18NXy4_
https://hedgedoc.dezentrale.space/s/C1PnaIj2Y
https://hanson.net/users/ao88yucom
https://www.northwestu.edu/?URL=https://ao88-yu.com/
https://writexo.com/share/6d8b6a2a1612
https://expatguidekorea.com/profile/ao88yucom/
https://www.laundrynation.com/community/profile/ao88yucom/
https://www.heavyironjobs.com/profiles/8226641-nha-cai-ao88
https://pad.degrowth.net/s/xy1tiYYu8
http://fort-raevskiy.ru/community/profile/ao88yucom/
https://forums.galciv4.com/user/7665436
https://forums.stardock.com/user/7665436
https://www.tai-ji.net/members/profile/3715714/ao88yucom.htm
https://forum.skullgirlsmobile.com/members/ao88yucom.220116/#about
https://jobs.landscapeindustrycareers.org/profiles/8226640-nha-cai-ao88
https://phatwalletforums.com/user/ao88yucom
https://jobs.njota.org/employers/4137787-ao88yucom
https://dk.pinterest.com/ao88yucom/
https://it.pinterest.com/ao88yucom/
https://fr.pinterest.com/ao88yucom/
https://www.vhs80.com/board/board_topic/6798823/8259682.htm
https://www.coffeesix-store.com/board/board_topic/7560063/8259683.htm
https://okmen.edu.vn/members/ao88yucom1.30194/
https://batdongsan24h.edu.vn/members/ao88yucom1.21086/
https://www.milliescentedrocks.com/board/board_topic/2189097/8259685.htm
https://www.greencarpetcleaningprescott.com/members/profile/3715713/ao88yucom.htm
https://forums.galciv3.com/user/7665436
https://forums.sinsofasolarempire2.com/user/7665436
https://idol.st/user/170733/ao88yucom/
https://www.bmwpower.lv/user.php?u=ao88yucom
https://jobs.windomnews.com/profiles/8226697-nha-cai-ao88
https://hedgedoc.stusta.de/s/f19KJctp2
https://md.chaospott.de/s/XRvTcjvNW0
https://pandora.nla.gov.au/external.html?link=https://ao88-yu.com/
https://login.ezproxy.lib.lehigh.edu/login?url=https://ao88-yu.com/
https://hoaxbuster.com/redacteur/ao88yucom
https://www.givey.com/ao88yucom
https://talkmarkets.com/profile/ao88yucom
https://pc.poradna.net/users/1197732154-ao88yucom
https://zerosuicidetraining.edc.org/user/profile.php?id=564735
https://www.telix.pl/forums/users/Landon-Henning/
https://www.thetriumphforum.com/members/ao88yucom.64591/
https://l2top.co/forum/members/ao88yucom.176975/
http://www.askmap.net/location/7814446/h%E1%BB%93-ch%C3%AD-minh/ao88yucom
https://graphcommons.com/graphs/f59ab844-f5df-49ff-ae4f-e0535f56a84e
https://galleria.emotionflow.com/184999/profile.html
https://www.deafvideo.tv/vlogger/ao88yucom
https://www.empregosaude.pt/en/author/ao88yucom/
https://confengine.com/user/ao88yucom
https://mygamedb.com/profile/ao88yucom
https://buckeyescoop.com/community/members/ao88yucom.63609/#about
https://forum.aceinna.com/user/ao88yucom
https://www.mateball.com/ao88yucom
https://toirscript.com/user/ao88yucom
https://forum.pabbly.com/members/ao88yucom.116223/#about
http://forum.cncprovn.com/members/426351-ao88yucom
https://ncnews.co/profile/ao88yucom
https://dreevoo.com/profile_info.php?pid=1598248
https://forum.aigato.vn/user/ao88yucom
https://amaz0ns.com/forums/users/ao88yucom/
https://rapidapi.com/user/ao88yucom
https://www.skool.com/@nha-cai-ao-4469
https://learningapps.org/watch?v=p4df0qvp326
https://subscribe.ru/author/32301355
https://www.giveawayoftheday.com/forums/profile/1841434
http://onlineboxing.net/jforum/user/editDone/453843.page
https://tealfeed.com/ao88yucom_829217
https://www.invelos.com/UserProfile.aspx?Alias=ao88yucom
https://www.video-bookmark.com/bookmark/7121692/ao88yucom/
https://wibki.com/ao88yucom
https://krachelart.com/UserProfile/tabid/43/userId/1344667/Default.aspx
https://gitlab.vuhdo.io/ao88yucom
https://aniworld.to/user/profil/ao88yucom
https://s.id/ao88yucom
https://worldvectorlogo.com/ar/profile/ao88yucom
https://kktix.com/user/8822194
https://www.passes.com/ao88yucom
https://uiverse.io/profile/landon_6431
https://www.fitday.com/fitness/forums/members/ao88yucom.html
https://www.fundable.com/nha-cai-ao88-10
https://vcook.jp/users/90190
https://www.grepmed.com/ao88yucom
https://classificados.acheiusa.com/profile/dTZYbVUvWWVYUE5wNE40Vm0zNEF1MElIaWZ6TFpuUXhmbFVJbE9Na2l5OD0=
https://espritgames.com/members/51010087/
https://cgmood.com/ao88yucom
https://www.efunda.com/members/people/show_people.cfm?Usr=ao88yucom
https://diit.cz/profil/qv69sktkvq
https://backloggery.com/ao88yucom
https://raovat.nhadat.vn/members/ao88yucom-310304.html
https://www.moshpyt.com/user/ao88yucom
https://www.koi-s.id/member.php?332647-ao88yucom
https://pumpyoursound.com/u/user/1618406
https://que.u.nosv.org/profile?user=ao88yucom
https://secondstreet.ru/profile/ao88yucom/
https://forum.fakeidvendors.com/user/ao88yucom
https://scenarch.com/userpages/35145
https://undrtone.com/ao88yucom
https://marshallyin.com/members/ao88yucom/
https://us.enrollbusiness.com/BusinessProfile/7796133/ao88yucom
https://www.atozed.com/forums/user-79527.html
https://www.tizmos.com/ao88yucom
https://gravesales.com/author/ao88yucomao88yucom/
https://luvly.co/users/ao88yucom
https://www.soshified.com/forums/user/666620-ao88yucom/
https://hukukevi.net/user/ao88yucom
https://savelist.co/profile/users/ao88yucom
https://www.apsense.com/user/ao88yucom
https://etextpad.com/rlnewhnnqg
https://zzb.bz/QKTwoy
https://www.pdc.edu/?URL=https://ao88-yu.com/
https://www.depechemode.cz/?URL=https://ao88-yu.com/
https://iplog.link/wsBIux
https://flii.by/eqSRUI
https://ixawiki.com/link.php?url=https://ao88-yu.com/
https://hackmd.openmole.org/s/xqw-K07P3
https://md.chaosdorf.de/s/1qfxoF4MsY
https://doc.adminforge.de/s/8kbgRJbzTJ
https://www.plotterusati.it/user/ao88-7
https://qoo.by/MTsiTM
https://goo.by/bfUQYQ
https://hack.allmende.io/s/aKClaIVQH
https://vi.gravatar.com/ao88yucom
https://www.claimajob.com/profiles/8227620-nha-cai-ao88
https://pad.codefor.fr/s/JlV3zmnF55
https://www.montessorijobsuk.co.uk/author/ao88yucom/
https://hackmd.hub.yt/s/C73IZ_nXo
https://draft.blogger.com/profile/15185449343016861003
https://boldomatic.com/view/writer/ao88yucom
https://www.themeqx.com/forums/users/ao88yucom/
https://www.udrpsearch.com/user/ao88yucom
https://www.inseparabile.it/forum/member.php?u=48176
https://www.xen-factory.com/index.php?members/ao88yucom.158362/#about
https://cointr.ee/ao88yucom
https://raovatquynhon.com/thiet-bi-dien-tu-4/ao88yucom124-20531
https://b.io/ao88yucomao88yucom
https://www.blackhatprotools.info/member.php?289828-ao88yucom
https://activepages.com.au/profile/ao88yucom
https://snippet.host/xwsfqs
https://tudomuaban.com/chi-tiet-rao-vat/2896381/ao88yucom.html
https://phijkchu.com/a/ao88yucom/video-channels
https://lifeinsys.com/user/ao88yucom
https://kaeuchi.jp/forums/users/ao88yucom/
https://protospielsouth.com/user/132992
https://theafricavoice.com/profile/ao88yucom
http://palangshim.com/space-uid-5144024.html
https://www.africangenesis-101.org/profile/henninglandon73515558/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:9C8181E769F76C160A495FA3@AdobeID
https://www.mixcloud.com/ao88yucom/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=196262
https://www.pixiv.net/en/users/125958906
https://hub.vroid.com/en/users/125958906
https://support.bitspower.com/support/user/ao88yucom
https://www.brownbook.net/user-profile/6304038
https://blog.ulifestyle.com.hk/ao88yucom
https://app.talkshoe.com/user/ao88yucomao88yucom
https://www.babelcube.com/user/nha-cai-ao88-3
https://golden-forum.com/memberlist.php?mode=viewprofile&u=230701
https://www.pageorama.com/?p=ao88yucom
https://bandsworksconcerts.info/index.php?ao88yucom
https://bbs.mikocon.com/home.php?mod=space&uid=292187
https://www.mikocon.com/home.php?mod=space&uid=292187
https://jerseyboysblog.com/forum/member.php?action=profile&uid=93885
https://manylink.co/@ao88yucom
https://seomotionz.com/member.php?action=profile&uid=130401
https://anyflip.com/homepage/ddhin#About
https://www.akaqa.com/question/q19192677386-Ao88yucom
https://londonchinese.com/home.php?mod=space&uid=621677&do=profile
https://copynotes.be/shift4me/forum/user-54247.html
https://scholar.google.com/citations?hl=en&user=WIyYkXkAAAAJ
https://tabelog.com/rvwr/ao88yucom/prof/
https://prosinrefgi.wixsite.com/pmbpf/profile/henninglandon73581624/profile
https://coolors.co/u/ao88yucom
https://civitai.com/user/ao88yucom
https://camp-fire.jp/profile/ao88yucom
https://feyenoord.supporters.nl/profiel/151075/ao88yucom
https://www.pearltrees.com/ao88yucom/item794952911
https://gesoten.com/profile/detail/12805177
https://hashnode.com/@ao88yucom
https://hoo.be/ao88yucom
https://nhattao.com/members/user6964724.6964724/
https://maxforlive.com/profile/user/ao88yucom?tab=about
https://3dtoday.ru/blogs/ao88yucom
https://my.bio/ao88yucom
https://ask.mallaky.com/?qa=user/ao88yucom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=80962
https://bresdel.com/ao88yucom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=14183
https://ao88yucom.notepin.co/
http://www.dungdong.com/home.php?mod=space&uid=3375172&do=profile
https://www.squadskates.com/profile/henninglandon73593905/profile
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=91399
https://mylinks.ai/ao88yucom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2490645
https://forum.tkool.jp/index.php?members/ao88yucom.107768/#about
https://ao88yucom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/ao88yucom/activity
https://uccle.monopinion.belgium.be/profiles/ao88yucom/activity
https://makeagif.com/user/ao88yucom?ref=GgYRba
https://mt2.org/uyeler/ao88yucom.40148/#about
https://partecipa.poliste.com/profiles/ao88yucom/activity
http://www.jbt4.com/home.php?mod=space&uid=8671932
https://www.vid419.com/home.php?mod=space&uid=3488712
https://forum.ct8.pl/member.php?action=profile&uid=123599
https://devfolio.co/@ao88yucom/readme-md
https://www.pintradingdb.com/forum/member.php?action=profile&uid=145007
https://www.mindomo.com/mindmap/3a160aca6c524e45ba8d7a092c531e4a
https://www.okaywan.com/home.php?mod=space&uid=801659
https://www.goodolcomics.com/blog/profile/ao88yucom/
http://techou.jp/index.php?ao88yucom
http://tkdlab.com/wiki/index.php?ao88yucom
https://www.managementpedia.com/members/ao88yucom.1121527/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=636208
https://volleypedia.org/index.php?qa=user&qa_1=ao88yucom
http://pcsq28.com/home.php?mod=space&uid=2023341
https://bbs.airav.cc/home.php?mod=space&uid=4601397
https://partecipa.poliste.com/profiles/ao88yucom/activity
https://hker2uk.com/home.php?mod=space&uid=5538314
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=500193
https://aprenderfotografia.online/usuarios/ao88yucom/profile/
http://galeria.farvista.net/member.php?action=showprofile&user_id=77920
https://tilengine.org/forum/member.php?action=profile&uid=165198
https://bbs.darkml.net/home.php?mod=space&uid=158942
https://www.play56.net/home.php?mod=space&uid=6187459
https://wandb.ai/profile/ao88yucom
https://bio.site/ao88yucom
https://wikimapia.org/external_link?url=https://ao88-yu.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6455335
https://pads.zapf.in/s/AAWQLUvQon
http://www.webclap.com/php/jump.php?url=https://ao88-yu.com/
https://md.swk-web.com/s/JUyJP0Cvb
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://ao88-yu.com/
https://redirect.camfrog.com/redirect/?url=https://ao88-yu.com/
https://beteiligung.hafencity.com/profile/ao88yucom/
https://adhocracy.plus/profile/ao88yucom/
https://www.hobowars.com/game/linker.php?url=https://ao88-yu.com/
https://beteiligung.stadtlindau.de/profile/ao88yucom/
https://www.fw-follow.com/forum/topic/122450/ao88yucom
https://www.jk-green.com/forum/topic/115002/ao88yucom
https://www.navacool.com/forum/topic/412241/ao88yucom
https://www.bonback.com/forum/topic/412242/ao88yucom
https://www.driedsquidathome.com/forum/topic/148879/ao88yucom
https://www.nongkhaempolice.com/forum/topic/131396/ao88yucom
https://www.bestloveweddingstudio.com/forum/topic/86662/ao88yucom
https://www.natthadon-sanengineering.com/forum/topic/108951/ao88yucom
https://www.rueanmaihom.net/forum/topic/102164/ao88yucom
https://www.ttlxshipping.com/forum/topic/412244/ao88yucom
https://www.pathumratjotun.com/forum/topic/182111/ao88yucom
https://beteiligung.tengen.de/profile/ao88yucom/
https://ar.gravatar.com/ao88yucom
https://divisionmidway.org/jobs/author/ao88yucom/
http://jobs.emiogp.com/author/ao88yucom/
https://onlinevetjobs.com/author/ao88yucom/
https://v.gd/4nl6VM
https://gl.gta5-mods.com/users/ao88yucom
http://jobboard.piasd.org/author/ao88yucom/
https://bbcovenant.guildlaunch.com/users/blog/6755874/?mode=view&gid=97523
https://www.youbiz.com/profile/ao88yucom
https://www.wowonder.xyz/ao88yucom
https://sciencemission.com/profile/ao88yucom
https://www.wvhired.com/profiles/8236178-nha-cai-ao88
https://kenhrao.com/members/ao88yucom.122205/#about
https://ismschools.com.au/forums/users/ao88yucom/
https://forumketoan.com/members/ao88yucom.44599/#about
https://xoops.ec-cube.net/userinfo.php?uid=349801
http://www.wmhelp.cz/html/modules.php?name=Forums&file=profile&mode=viewprofile&u=601777
https://formulamasa.com/elearning/members/ao88yucom/?v=96b62e1dce57
http://bbs.sdhuifa.com/home.php?mod=space&uid=1118031
https://quangcaoso.vn/ao88yucom-412905.html
https://forum.flashphoner.com/members/ao88yucom.47359/#about
https://backloggd.com/u/ao88yucom/
https://www.warriorforum.com/members/Landon%20Henning.html?utm_source=internal&utm_medium=user-menu&utm_campaign=user-profile
https://community.jmp.com/t5/user/viewprofilepage/user-id/98846
https://rush1989.rash.jp/pukiwiki/index.php?ao88yucom
https://calaos.fr/forum/member.php?action=profile&uid=20246
https://www.vrwant.org/wb/home.php?mod=space&uid=5118394
https://www.speedway-world.pl/forum/member.php?action=profile&uid=479938
http://forum.orangepi.org/home.php?mod=space&uid=6455335
http://byltz.com/home.php?mod=space&uid=482165
http://bbs.medicalforum.cn/home.php?mod=space&uid=2261142
https://forum.enscape3d.com/wcf/index.php?user/139311-ao88yucom/#about
https://usabbs.org/home.php?mod=space&uid=88073
https://forums.sinsofasolarempire.com/user/7665436
https://forums.stardock.net/user/7665436
https://www.d-ushop.com/forum/topic/137030/ao88yucom
https://aboutcasemanagerjobs.com/author/ao88yucom/
https://lustyweb.live/members/ao88yucom.125430/#about
https://findaspring.org/members/ao88yucom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=779806
https://careers.coloradopublichealth.org/profiles/8222975-nha-cai-ao88
https://crowdsourcer.io/profile/bHwWKW3M
https://gorillasocialwork.com/user/ao88yucom
https://homepage.ninja/ao88yucom
https://propeller.hu/tagok/ao88yucom/adatlap
https://cuadepviet.com/members/13323-ao88yuco.html
https://datcang.vn/memberlist.php?mode=viewprofile&u=52534
https://dienbd.violet.vn/user/show/id/15271913
https://www.ixawiki.com/link.php?url=https://ao88-yu.com/
https://www.shinobi.jp/etc/goto.html?https://ao88-yu.com/
https://decide.enguera.es/profiles/ao88yucom/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345969
https://axe.rs/forum/members/ao88yucom.13428081/#about
https://co-roma.openheritage.eu/profiles/ao88yucom/activity
https://openlibrary.org/people/landon_henning
https://www.bookingblog.com/forum/users/ao88yucom/
https://www.motiondesignawards.com/profile/21203
https://pad.stuve.de/s/BYEl6MMht
https://pad.libreon.fr/s/8iCnW1St_
https://chodaumoi247.com/members/ao88yucom.51661/
https://aiti.edu.vn/members/ao88yucom.45314/
https://tinhte.vn/members/ao88yucom.3390102/
https://md.rappet.xyz/s/f9hhwq6jTK
https://wall.page/bMpOTU
https://www.ad-links.org/https://ao88-yucom/_373777.html
https://www.reddit-directory.com/ao88yucom_711904.html
https://www.beegdirectory.com/https://ao88-yucom/_492953.html
https://www.aquarius-dir.com/https://ao88-yucom/_518857.html
https://www.apeopledirectory.com/https://ao88-yucom/_417328.html
https://www.bedirectory.com/https://ao88-yucom/_449898.html
https://www.alive-directory.com/https://ao88-yucom/_726845.html
https://www.craigslistdir.org/https://ao88-yucom/_415860.html
https://www.ecodir.net/https://ao88-yucom/_339509.html
https://www.ask-dir.org/https://ao88-yucom/_385157.html
https://www.bestbuydir.com/https://ao88-yucom/_456107.html
https://www.free-weblink.com/ao88yucom_278200.html
http://depechemode.cz/?URL=https://ao88-yu.com/
https://www.buckeyescoop.com/users/0241b28e-6804-434f-ab51-0b69f91c4a1b
https://jp.pinterest.com/ao88yucom/
https://de.gta5-mods.com/users/ao88yucom
https://urlscan.io/result/019deab0-66cd-7258-8f2f-3e39f30411f9/
https://jobs.host-panel.com/author/ao88yucom/
https://syosetu.org/?mode=url_jump&url=https://ao88-yu.com/
https://aboutsnfjobs.com/author/ao88yucom/
https://mk.gta5-mods.com/users/ao88yucom
https://tr.gta5-mods.com/users/ao88yucom
https://bs.gravatar.com/ao88yucom
https://community.perchcms.com/user/31531-ao88yucom/#about
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ao88-yu.com/
https://giaoan.violet.vn/user/show/id/15271913
https://anh135689999.violet.vn/user/show/id/15271913
https://hu.gta5-mods.com/users/ao88yucom
https://uk.gta5-mods.com/users/ao88yucom
https://sl.gta5-mods.com/users/ao88yucom
https://at.pinterest.com/ao88yucom/
https://newdayrp.com/members/ao88yucom.72365/#about
https://in.pinterest.com/ao88yucom/
https://doc.anagora.org/s/7ElVgLE2O
https://song.link/ao88yucom
https://album.link/ao88yucom
https://artist.link/ao88yucom
https://pods.link/ao88yucom
https://playlist.link/ao88yucom
https://mylink.page/ao88yucom
https://odesli.co/ao88yucom
https://portfolium.com.au/ao88yucom
https://aboutnursepractitionerjobs.com/author/ao88yucom/
https://jpeg.ly/zr33T
https://jobs.tdwi.org/profiles/8227899-nha-cai-ao88
https://aboutpharmacistjobs.com/author/ao88yucom/
https://blog.ss-blog.jp/_pages/mobile/step/index?u=https://ao88-yu.com/
https://shorturl.ly/3V7gZ
https://nyccharterschools.jobboard.io/employers/4138361-ao88yucom
https://aboutnursernjobs.com/author/ao88yucom/
https://www.sunemall.com/board/board_topic/8431232/8254977.htm
https://ibit.ly/UHjPc
https://t.ly/2khgD
https://profile.sampo.ru/ao88yucom
https://mail.londonchinese.com/home.php?mod=space&uid=621677&do=profile
https://videos.muvizu.com/Profile/ao88yucom/Latest/
https://www.ulearnnow.net/profile/henninglandon73531594/profile
https://dev.muvizu.com/Profile/ao88yucom/Latest
https://cdn.muvizu.com/Profile/ao88yucom/Latest
https://www.muvizu.com/Profile/ao88yucom/Latest
https://urlz.fr/v8m4
https://jobs.lajobsportal.org/profiles/8227665-nha-cai-ao88
https://www.bidhub.com/profiles/show/21707
https://baigiang.violet.vn/user/show/id/15271913
https://forums.starcontrol.com/user/7665436
https://forums.offworldgame.com/user/7665436
https://www.ekdarun.com/forum/topic/158553/ao88yucom
https://nl.gravatar.com/ao88yucom
https://nb.gravatar.com/ao88yucom
https://ms.gravatar.com/ao88yucom
https://us.pinterest.com/ao88yucom/
https://lt.gravatar.com/ao88yucom
https://kn.gravatar.com/ao88yucom
https://memmai.com/index.php?members/ao88yucom1.42532/#about
https://vn-zom.com/members/ao88yucom.5848/
https://vietcurrency.vn/members/ao88yucom.240762/#about
https://vnbit.org/members/ao88yucom.105605/#about
https://boss.why3s.cc/boss/home.php?mod=space&uid=264494
https://participa.aytojaen.es/profiles/ao88yucom/activity
https://www.interesting-dir.com/details.php?id=444031
https://www.addirectory.org/details.php?id=480506
https://dialogluzern.ch/profiles/ao88yucom/activity
http://mura.hitobashira.org/index.php?ao88yucom
https://decidim.santcugat.cat/profiles/ao88yucom/activity
https://fr.slideshare.net/henninglandon735?tab=about
https://janitorai.com/profiles/d222eeff-3964-448d-be57-172799f09486_profile-of-ao-88-yucom
https://www.akiba-online.com/members/ao88yucom.1356299/#about
https://barcelonadema-participa.cat/profiles/ao88yucom/activity
https://worstgen.alwaysdata.net/forum/members/ao88yucom.175876/#about
https://defence.pk/members/ao88yucom.241077/#about
https://wiki.armello.com/index.php/User:Ao88yucom
https://da.gta5-mods.com/users/ao88yucom
https://el.gta5-mods.com/users/ao88yucom
https://no.gta5-mods.com/users/ao88yucom
https://forum.freero.org/space-uid-25072.html
https://forum.biblepay.org/index.php?action=profile;area=forumprofile;u=43459
https://www.cbmstuff.com/forum/member.php?action=profile&uid=11994
https://forum.vgatemall.com/member.php?action=profile&uid=526125
https://www.freebeg.com/forum/member.php?action=profile&uid=136450
https://www.forum-joyingauto.com/member.php?action=profile&uid=125118
http://julia4tied.de/member.php?action=profile&uid=247703
https://altered.ajordat.com/it/profiles/b800a115-1bfb-4d09-8592-3b3f5a55c12d/
https://gspanel.net/member.php?action=profile&uid=17700
https://muabanhaiduong.com/members/ao88yucom.88762/#about
https://monopinion.namur.be/profiles/ao88yucom/activity
https://www.fiferosdevenezuela.com/foro/member.php?action=profile&uid=12780
https://www.mycast.io/users/ao88yucom
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=229139&tab=field_core_pfield_13
https://br.gravatar.com/ao88yucom
https://www.xiuwushidai.com/home.php?mod=space&uid=2688639
https://bbs.theviko.com/home.php?mod=space&uid=4675016
http://app.gxbs.net/home.php?mod=space&uid=1826265
https://www.saltlakeladyrebels.com/profile/henninglandon73523536/profile
https://pastewall.com/59308/sticker/2e79d81ce9bf4583addcf2d8e8a19978
https://www.veteranscup.org/profile/henninglandon73563657/profile
https://www.biblegrove.org/profile/henninglandon73536006/profile
https://careers.mntech.org/profiles/8238109-nha-cai-ao88
https://nous.malakoff.fr/profiles/ao88yucom/activity
https://slackcommunity.com/u/mrzkm9/#/about
https://walling.app/tEU9B8NO0JJCFYdqVJYm/ao88yucom
https://racetime.gg/user/5K9rm360JyWq1aOX/ao88yucom
https://ca.gravatar.com/ao88yucom
http://gojourney.xsrv.jp/index.php?ao88yucom
https://magazin.orgsoft.ru/communication/forum/index.php?PAGE_NAME=profile_view&UID=237244
https://gl.gravatar.com/ao88yucom
https://builtbybit.com/members/ao88yucom.803775/#about
https://www.webmastersun.com/members/ao88yucom.165005/#about
https://www.pioneer2.net/community/members/aoyucom.14580/#about
https://forum.norbrygg.no/members/ao88yucom.151650/#about
https://allmylinks.com/ao88yucom
https://sk.gravatar.com/ao88yucom
https://congdongx.com/thanh-vien/ao88yucom.50089/#about
https://mel-assessment.com/members/ao88yucom/profile/
https://www.leonidastacticalss.com/profile/henninglandon7357056/profile
https://www.bridgescdc.com/profile/henninglandon73544411/profile
https://boards.rossmanngroup.com/members/ao88yucom.92763/#about
https://paste.toolforge.org/view/e3fcdf5f
https://participation.touraine.fr/profiles/ao88yucom/activity
https://zh-tw.gravatar.com/ao88yucom
https://chodilinh.com/members/ao88yucom.304934/#about
https://www.hostboard.com/forums/members/ao88yucom.html
https://videos.benjaminbrady.ie/accounts/ao88yucom/about
https://forum.uookle.com/home.php?mod=space&uid=1439363
https://participer.loire-atlantique.fr/profiles/ao88yucom/activity
https://po.gravatar.com/ao88yucom
http://hkeverton.com/forumnew/home.php?mod=space&uid=643164
https://www.siasat.pk/members/ao88yucom.272634/#about
https://forums.sorcererking.com/user/7665436
https://forums.galciv2.com/user/7665436
https://forums.gamersbillofrights.com/user/7665436
https://forums.littletinyfrogs.com/user/7665436
https://bn.gravatar.com/ao88yucom
https://scanverify.com/siteverify.php?site=https://ao88-yu.com/
https://thaicpe.com/members/ao88yucom.14539/#about
https://www.onetap.com/members/ao88yucom.509771/#about
https://forums.politicalmachine.com/user/7665436
https://forumton.org/members/ao88yucom.36808/#about
http://www.grandisvietnam.com/members/ao88yucom.30300/#about
https://www.airportcitygame.com/members/ao88yucom.36721/#about
https://www.zophar.net/forums/index.php?members/ao88yucom.136192/#about
https://congdongmassage.com/members/ao88yucom.150096/#about
http://web.symbol.rs/forum/member.php?action=profile&uid=1280983
https://hu.gravatar.com/ao88yucom
https://jeparticipe.ville-montlouis-loire.fr/profiles/ao88yucom/activity
https://fr.gta5-mods.com/users/ao88yucom
https://pad.deckenpfronn.info/s/iTQEZib9M
https://zh.gta5-mods.com/users/ao88yucom
https://www.harimajuku.com/profile/henninglandon73534406/profile
https://www.happycampersmontessori.com/profile/henninglandon73546311/profile
https://www.miseducationofmotherhood.com/profile/henninglandon73596309/profile
https://independent.academia.edu/LandonHenning1
https://vnseo.edu.vn/members/ao88yucom.485703.html
https://www.newdirectionchildcarefacility.com/profile/henninglandon7358506/profile
https://start.me/u/ogPD6k/ao88yucom
https://ieee-dataport.org/authors/trangchu-ao
https://tuscl.net/member/888944
https://f.gvn.co/members/ao88.1820991/#about
https://linqto.me/about/ao88yucom
https://ro.gta5-mods.com/users/ao88yucom
https://sighpceducation.hosting.acm.org/wp/forums/users/ao88yucom1/
https://www.suamusica.com.br/landonhenning
https://bmw-sg.com/forums/members/ao88yucom.113368/#about
https://vipcorel.com/members/ao88yucom.50359/#about
https://congdongketoan.vn/members/ao88yucom.34769/#about
https://diendanit.net/members/ao88yucom.44001/#about
https://forum.edu.vn/members/ao88yucom.1862/#about
https://nhanxetdanhgia.vn/members/ao88yucom.63243/#about
https://vn-z.vn/members/ao88yucom.353235/#about
https://www.otosaigon.com/members/ao88yucom.427034/#about
https://raovat.trumbansi.net/members/ao88yucom.1916/#about
https://yeupet.vn/thanh-vien/ao88yucom.1150/#about
https://designerviet.com/members/ao88yucom.100558/#about
http://web.symbol.rs/forum/member.php?action=profile&uid=1280983
https://fr.slideshare.net/henninglandon735?tab=about
https://www.tractorbynet.com/forums/members/ao88yucom.431489/#about
https://commoncause.optiontradingspeak.com/index.php/community/profile/ao88yucom/
https://reduser.net/members/ao88yucom.230358/#about
https://forum.splashteck.com/member.php?action=profile&uid=5129
https://board.playzo.de/index.php?user/9910-ao88yucom/&editOnInit=1#about
https://forum.laborcraft.net/members/ao88yucom.27297/#about
https://www.ibizaclubpt.com/members/ao88yucom.122445/#about
https://devbest.com/members/ao88yucom.153795/#about
https://vi.gta5-mods.com/users/ao88yucom
https://bbs.darkml.net/home.php?mod=space&uid=158942
https://3ddd.ru/users/ao88yucom
https://www.pebforum.com/members/ao88yucom.243606/#about
https://participez.villeurbanne.fr/profiles/ao88yucom/activity
https://pt.gta5-mods.com/users/ao88yucom
https://community.alexgyver.ru/members/ao88yucom.176275/#about
https://ivpaste.com/v/836DdmQvm4
https://forums.demigodgame.com/user/7665436
https://forums.elementalgame.com/user/7665436
https://pl.gta5-mods.com/users/ao88yucom
https://participation.bordeaux.fr/profiles/ao88yucom/activity
http://www.daojianchina.com/home.php?mod=space&uid=1088507
http://qa.doujiju.com/index.php?qa=user&qa_1=ao88yucom
https://www.ted.com/profiles/51551130
https://to-portal.com/ao88yucom
https://docs.google.com/document/d/1uzpmjV1mxYZBY2hOr1ZBHh4ANFnZtXzlvDrIyrQ0Uuk/edit?usp=sharing
https://www.questmetaldetectors.com/members-area/henninglandon73516460/profile
https://vozer.net/members/ao88yucom.90543/#about
https://www.rappad.co/users/ao88yucom
https://comunitat.canodrom.barcelona/profiles/ao88yucom/activity?locale=en
https://rnmanagers.com/author/ao88yucom/
https://www.floodzonebrewery.com/profile/henninglandon73554080/profile
https://participa.gijon.es/profiles/ao88yucom/activity
https://clusterbusters.org/forums/profile/35756-ao88yucom1/?tab=field_core_pfield_11
https://joy.bio/ao88yucom1
https://joyrulez.com/ao88yucom1
https://pets4friends.com/profile-1591091
https://bsky.app/profile/ao88yucom1.bsky.social
https://www.clickasnap.com/profile/ao88yucom1
https://soundcloud.com/ao88yucom1
https://fliphtml5.com/vi/home/ao88yucom1
https://newspicks.com/user/12458566/
https://biolinku.co/ao88yucom
https://linkmix.co/54435053
https://land-book.com/ao88yucom1
https://ko-fi.com/ao88yucom1
https://jali.me/ao88yucom
https://jii.li/ao88yucom1
https://kitsu.app/users/ao88yucom1
https://giphy.com/channel/ao88yucom1
https://www.awwwards.com/ao88yucom1/
https://fairygodboss.com/users/profile/elxW-U4Rh_/Landon-Henning
https://stepik.org/users/1268791737/profile?auth=registration
https://rentry.co/nvew7uxq
https://www.demilked.com/author/landonhenning/
https://www.pozible.com/profile/ao88-19
https://community.atlassian.com/user/profile/0590e115-dffd-4065-a857-9902857c13fd
https://manifold.markets/ao88yucom1
https://game8.jp/users/495080
https://tempel.in/view/8yIncV
https://www.maanation.com/ao88yucom1
https://peatix.com/user/29585808/view
https://odysee.com/@ao88yucom1:3
Bersama dengan semua hal yang mana tampak sedang dibangun dalam topik khusus ini, sebagian besar pandangan Anda ternyata sangat menarik. Meskipun demikian, saya maaf, tetapi saya tidak dapat memberikan kepercayaan pada keseluruhan ide Anda, meskipun menarik. Tampaknya bagi kami bahwa komentar Anda tidak sepenuhnya benar-benar tervalidasi dan pada kenyataannya Anda sendiri tidak benar-benar sepenuhnya percaya diri terhadap poin tersebut. Dalam hal apa pun saya menikmati membaca.
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Hello! Someone in my Facebook group shared this website with us so I came to check it out. I’m definitely loving the information. I’m book-marking and will be tweeting this to my followers! Wonderful blog and amazing design and style.
Can I just say what a aid to find somebody who actually is aware of what theyre speaking about on the internet. You definitely know learn how to convey a difficulty to light and make it important. Extra folks have to read this and perceive this aspect of the story. I cant imagine youre no more common because you positively have the gift.
We are a group of volunteers and starting a new scheme in our community.
Your web site provided us with valuable info to work on. You have done
a formidable job and our entire community will be grateful to you.
Terima kasih atas tulisan yang baik. Sebenarnya ini sebelumnya adalah sebuah materi hiburan. Terlihat kompleks menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
This web site can be a walk-through for all the information you needed about this and didn’t know who to ask. Glimpse right here, and also you’ll undoubtedly uncover it.
Hai, saya sekadar ingin mengatakan bahwa saya sangat menikmati membaca postingan blog Anda. Ini merupakan tepat jenis informasi yang saya cari. Saya akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Oh my goodness! an incredible article dude. Thanks Nevertheless I am experiencing concern with ur rss . Don’t know why Unable to subscribe to it. Is there anyone getting equivalent rss problem? Anyone who knows kindly respond. Thnkx
Excellent beat ! I wish to apprentice while you amend your website, how could i subscribe for a blog web site? The account helped me a acceptable deal. I had been a little bit acquainted of this your broadcast offered bright clear idea
Saya mendapatkan info yang bagus dari blog Anda.
It’s a pity you don’t have a donate button! I’d certainly donate to this excellent blog! I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account. I look forward to brand new updates and will share this blog with my Facebook group. Talk soon!
Wohh tepat apa yang saya cari, salam atas unggahan.
I’d incessantly want to be update on new content on this site, saved to bookmarks! .
As soon as I found this web site I went on reddit to share some of the love with them.
Bagaimanapun, terima kasih untuk poin yang istimewa ini dan walaupun saya tidak sepakat sepenuhnya, saya menilai sudut pandang.
The heart of your writing while appearing agreeable originally, did not really settle well with me after some time. Somewhere throughout the paragraphs you managed to make me a believer unfortunately only for a very short while. I nevertheless have got a problem with your jumps in logic and one would do nicely to help fill in all those breaks. In the event that you actually can accomplish that, I could definitely be amazed.
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, sangat posting yang bagus.
Very interesting points you have observed, regards for putting up. “These days an income is something you can’t live without–or within.” by Tom Wilson.
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan bersyukur kepada Anda.
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup artikel yang bagus.
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan pesan yang sama. Apakah ada sarana Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan bersyukur kepada Anda.
Very interesting points you have noted, appreciate it for putting up. “Never call an accountant a credit to his profession a good accountant is a debit to his profession.” by Charles J. C. Lyall.
Postingan yang sangat membantu. Saya baru saja menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Have you ever thought about adding a little bit more than just your articles? I mean, what you say is fundamental and all. But imagine if you added some great pictures or video clips to give your posts more, “pop”! Your content is excellent but with pics and videos, this site could definitely be one of the best in its field. Excellent blog!
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang hebat!
Nyata bersih situs internet, terimakasih untuk pos ini.
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Saya tidak bisa menahan diri untuk berkomentar
Those are yours alright! . We at least need to get these people stealing images to start blogging! They probably just did a image search and grabbed them. They look good though!
Im now not certain the place you are getting your info, but great topic. I needs to spend some time finding out much more or figuring out more. Thank you for excellent info I used to be in search of this info for my mission.
Informasi yang bermanfaat. Saya baru saja menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Kami dapat memiliki hyperlink perdagangan kontrak antara kita!
I have not checked in here for a while as I thought it was getting boring, but the last few posts are great quality so I guess I will add you back to my everyday bloglist. You deserve it my friend 🙂
Ini adalah blog yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Hello, I think your blog might be having browser compatibility issues. When I look at your website in Ie, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, superb blog!
Mengagumi kerja keras yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda sajikan. Sangat baik menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Saya senang bahwa saya menemukan situs ini, benar-benar informasi yang saya telusuri!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
Hai semua, hanya ingin mengatakan bahwa saya benar-benar menyukai membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak wawasan yang sangat berguna. Terima kasih!
Thank you, I’ve just been looking for information approximately this subject for a while and yours is the greatest I’ve found out till now. But, what concerning the bottom line? Are you certain concerning the source?
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada cara Anda akan bisa menghapus saya dari layanan itu? Terima kasih!
Saya sungguh puas menemukan situs web ini di Bing, persis seperti yang saya cari : D pula sudah saya simpan ke fav.
I believe other website owners should take this site as an example , very clean and good user pleasant style.
Saya tidak sering berkomentar tetapi saya harus menyatakan salam untuk posting yang spesial ini : D.
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah tepat tipe informasi yang saya cari. Saya akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
I know this if off topic but I’m looking into starting my own blog and was curious what all is needed to get setup? I’m assuming having a blog like yours would cost a pretty penny? I’m not very internet smart so I’m not 100 positive. Any recommendations or advice would be greatly appreciated. Many thanks
Pretty section of content. I just stumbled upon your web site and in accession capital to assert that I get in fact enjoyed account your blog posts. Any way I will be subscribing to your augment and even I achievement you access consistently fast.
Saya secara tidak sengaja menemukan website Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang bagus.
Saya selalu memikirkan hal ini, terima kasih telah memposting.
What i don’t understood is in reality how you’re no longer really much more well-liked than you might be right now. You are so intelligent. You understand therefore significantly with regards to this subject, made me in my opinion imagine it from a lot of varied angles. Its like men and women aren’t involved until it is something to accomplish with Lady gaga! Your personal stuffs nice. All the time maintain it up!
Menikmati menelaah ini, sangat bagus, sangat menghargai.
Hey I know this is off topic but I was wondering if you knew of
any widgets I could add to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was hoping
maybe you would have some experience with something like
this. Please let me know if you run into anything. I truly enjoy reading your blog and I
look forward to your new updates.
Nyata jelas situs internet, terimakasih untuk pos ini.
Saya sangat menghargai waktu yang Anda curahkan untuk menyusun artikel ini. Informasi yang berguna. Terima kasih banyak!
Thanks a bunch for sharing this with all of us you actually know what you’re talking about! Bookmarked. Kindly also visit my website =). We could have a link exchange contract between us!
Anda bisa pasti melihat antusiasme Anda di dalam karya yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Terima kasih atas tulisan yang baik. Pada kenyataannya ini dulunya adalah sebuah konten hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita bisa tetap berhubungan?
Wow! Terima kasih! Saya secara terus ingin menulis di situs saya sesuatu seperti itu. Bolehkah saya menerapkan sebagian dari posting Anda ke blog saya?
Isi yang fantastis! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Your place is valueble for me. Thanks!…
It’s hard to search out educated folks on this matter, however you sound like you realize what you’re talking about! Thanks
Having read this I thought it was very informative. I appreciate you taking the time and effort to put this article together. I once again find myself spending way to much time both reading and commenting. But so what, it was still worth it!
I want to show some appreciation to you for rescuing me from this type of scenario. As a result of looking out through the world wide web and meeting notions which were not productive, I assumed my entire life was gone. Living without the answers to the difficulties you’ve sorted out all through your entire posting is a crucial case, and the ones that could have negatively affected my entire career if I had not come across your web site. The knowledge and kindness in taking care of all the pieces was crucial. I’m not sure what I would have done if I had not discovered such a step like this. It’s possible to at this time look ahead to my future. Thanks so much for the professional and effective help. I will not be reluctant to recommend the blog to any person who should have assistance about this matter.
Hi there! Do you know if they make any plugins to help with SEO?
I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good success.
If you know of any please share. Appreciate it!
My site – Use any others you think will help it rank.
Saya tanpa henti memikirkan hal ini, sangat dihargai telah memposting.
Hey there would you mind stating which blog platform you’re using? I’m planning to start my own blog in the near future but I’m having a hard time deciding between BlogEngine/Wordpress/B2evolution and Drupal. The reason I ask is because your layout seems different then most blogs and I’m looking for something unique. P.S Apologies for being off-topic but I had to ask!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Hi! This is kind of off topic but I need some advice from an established blog. Is it tough to set up your own blog? I’m not very techincal but I can figure things out pretty fast. I’m thinking about making my own but I’m not sure where to start. Do you have any points or suggestions? Appreciate it
Saya secara tidak sengaja menemukan website Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang luar biasa.
Very interesting info !Perfect just what I was looking for! “If you could choose one characteristic that would get you through life, choose a sense of humor.” by Jennifer Jones.
Saya secara tidak sengaja menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang hebat.
Artikel yang sangat baik. Ini benar-benar disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
I always was interested in this topic and still am, regards for putting up.
Sangat fantastis info dapat ditemukan di weblog.
Menghargai komitmen yang Anda curahkan ke website Anda dan informasi mendalam yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Bacaan yang fantastis! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
The next time I read a blog, I hope that it doesnt disappoint me as much as this one. I mean, I know it was my choice to read, but I actually thought youd have something interesting to say. All I hear is a bunch of whining about something that you could fix if you werent too busy looking for attention.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Terima kasih banyak atas posting yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak sekali informasi yang bermanfaat. Teruskan pekerjaan yang bagus!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Saya tidak sering berkomentar tetapi saya harus menyatakan terima kasih untuk posting yang hebat ini : D.
Terima kasih untuk situs informatif lainnya. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan gaya yang ideal? Saya memiliki sebuah inisiatif yang saya tengah kerjakan sekarang, dan saya telah mencari informasi seperti ini.
Menikmati membaca ini, sangat bagus, terima kasih.
Saya secara tidak sengaja menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang hebat.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I am glad to be one of many visitants on this great internet site (:, appreciate it for putting up.
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
It’s amazing designed for me to have a web page, which is beneficial designed for my knowledge.
thanks admin
Dead pent articles, Really enjoyed examining.
Terima kasih untuk posting fantastis lainnya. Di mana lagi siapa pun bisa mendapatkan tipe informasi seperti itu dengan gaya penulisan yang ideal? Saya punya presentasi minggu berikutnya, dan saya berada dalam pencarian informasi seperti ini.
Seseorang pada dasarnya membantu membuat artikel yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Pekerjaan yang mengagumkan!
Wow! This blog looks exactly like my old one! It’s on a completely different topic but it has pretty much the same page layout and design. Great choice of colors!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Dengan hampir semuanya yang mana tampak sedang berkembang dalam topik khusus ini, semua pandangan Anda adalah cukup menarik. Walaupun begitu, saya maaf, tetapi saya tidak memberikan kepercayaan pada keseluruhan teori Anda, meskipun menyegarkan. Tampaknya bagi semua orang bahwa pendapat Anda tidak sepenuhnya sepenuhnya tervalidasi dan pada kenyataannya Anda sendiri tidak benar-benar sepenuhnya pasti terhadap poin tersebut. Dalam hal apa pun saya menghargai membaca.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas akan bersyukur kepada Anda.
Saya tidak bisa menahan diri untuk berkomentar
Artikel yang hebat. Ini memberi saya pemahaman yang lebih jelas tentang topik ini. Teruskan pekerjaan yang luar biasa!
Sangat menarik info !Sempurna persis seperti yang saya cari!
Hi , I do believe this is an excellent blog. I stumbled upon it on Yahoo , i will come back once again. Money and freedom is the best way to change, may you be rich and help other people.
I genuinely value your piece of work, Great post.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Saya terus memikirkan hal ini, terima kasih telah memposting.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Halo semua, sekadar ingin mengatakan bahwa saya sangat menyukai membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan banyak informasi yang sangat berguna. Terima kasih!
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna desain yang hebat!
Saya senang menjadi pengunjung dari situs web abadi ini!, terimakasih atas informasi langka ini!
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Saya selamanya memikirkan hal ini, salam telah memposting.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
I genuinely treasure your work, Great post.
Saya terus-menerus melihat online untuk artikel yang dapat membantu saya. Thanks!
Ya menyimpan ini bukanlah keputusan yang berisiko posting yang luar biasa! .
Saya benar-benar ingin mengirim pesan singkat guna mengucapkan terima kasih Anda atas semua tips luar biasa yang Anda tuliskan di website ini.
Terima kasih atas artikel yang luar biasa. Saya sungguh menikmati membaca ini dan menemukan banyak sekali wawasan yang bermanfaat. Teruskan pekerjaan yang hebat!
Konten yang fantastis! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
Hebat situs yang Anda miliki, tapi saya penasaran apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan tanggapan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Banyak terima kasih!
Mengagumi dedikasi yang Anda curahkan ke blog Anda dan informasi terperinci yang Anda berikan. Sangat baik menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang luar biasa! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Berharga info. Untungnya saya menemukan situs web Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menandainya.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Your comment is awaiting moderation.
https://www.facebook.com/kp88store
https://youtube.com/@kp88store
https://x.com/kp88store
https://wakelet.com/@kp88store
https://www.blogger.com/profile/12405097171515636248
https://pinterest.com/kp88store/
https://shareyoursocial.com/kp88store
https://500px.com/p/kp88store?view=photos
https://www.instapaper.com/p/kp88store
https://band.us/@kp88store
https://protocol.ooo/ja/users/kp88store
https://www.tumblr.com/kp88store
https://www.reddit.com/user/kp88store/
https://audiomack.com/andreahariharan623
https://hackaday.io/kp88store?saved=true
https://vocal.media/authors/kp88store
https://leetcode.com/u/kp88store/
https://www.halaltrip.com/user/profile/345126/kp88store/
https://medibang.com/author/28231068/
https://www.blockdit.com/users/69f711f905194c8dde009add
https://portfolium.com/andreahariharan623
https://groups.google.com/g/kp88store
https://www.twitch.tv/kp88store/about
https://profile.hatena.ne.jp/kp88store/profile
https://issuu.com/kp88store
https://www.behance.net/andreahariharan
https://gravatar.com/kp88store
https://www.reverbnation.com/artist/kp88store
https://www.myminifactory.com/users/kp88store
https://www.investagrams.com/Profile/kp88store
https://gifyu.com/kp88store
https://www.chordie.com/forum/profile.php?id=2521280
https://www.longisland.com/profile/kp88store
https://topsitenet.com/profile/kp88store/1714048/
https://akniga.org/profile/1420105-kp88store/
https://bandcamp.com/kp88store
https://disqus.com/by/kp88store/about/
https://jobs.suncommunitynews.com/profiles/8224359-kp88-nha-cai
https://www.speedrun.com/users/kp88store
https://www.aicrowd.com/participants/kp88store
https://old.bitchute.com/channel/Crw5BWLP21Sq/
https://pbase.com/kp88store/root
https://hub.docker.com/u/kp88store
https://spiderum.com/nguoi-dung/kp88store
https://www.gta5-mods.com/users/kp88store
https://heylink.me/andreahariharan623/
https://www.nicovideo.jp/user/144121042
https://3dwarehouse.sketchup.com/user/f865077b-5b3d-4fa6-a2e2-de82588e2cd6
https://joy.bio/kp88store
https://connect.garmin.com/app/profile/471fa2e9-5151-4134-99a2-26ac09640ced
https://b.hatena.ne.jp/kp88store/hotentry
https://b.hatena.ne.jp/kp88store/hotentry
https://unityroom.com/users/0r6wzgctuqeohpyndkx8
https://routinehub.co/user/kp88store
https://pxhere.com/en/photographer/5001730
https://teletype.in/@kp88store
https://www.checkli.com/kp88store#/a/process
https://www.fuelly.com/driver/kp88store
https://www.nintendo-master.com/profil/kp88store
https://freeimage.host/kp88store
https://motion-gallery.net/users/975984
https://linkin.bio/kp88store
https://biomolecula.ru/authors/145274
https://blender.community/kp88store/
https://doselect.com/@7e998877690c23aeeefc1b526
https://matkafasi.com/user/kp88store
https://allmyfaves.com/kp88store
https://conecta.bio/kp88store
https://www.abclinuxu.cz/lide/kp88store
https://muare.vn/shop/andrea-hariharan/903791
https://www.intensedebate.com/people/kp88store1
https://forum.dmec.vn/index.php?members/kp88store.190209/
https://igli.me/kp88store
http://delphi.larsbo.org/user/kp88store
https://app.readthedocs.org/profiles/kp88store/
https://www.dibiz.com/andreahariharan623
https://iszene.com/user-349865.html
https://desksnear.me/users/kp88store
https://www.roton.com/forums/users/andreahariharan623/
https://able2know.org/user/kp88store/
http://www.biblesupport.com/user/835888-kp88store/
https://golosknig.com/profile/kp88store/
https://www.inventoridigiochi.it/membri/kp88store/profile/
https://forum.m5stack.com/user/kp88store
https://www.bitchute.com/channel/yQNErkclWOxg
https://bandori.party/user/880152/kp88store/
https://community.m5stack.com/user/kp88store1
https://schoolido.lu/user/kp88store/
https://awan.pro/forum/user/169684/
https://fabble.cc/kp88store
https://kr.pinterest.com/kp88store/
https://pt.gravatar.com/kp88store
https://th.gravatar.com/kp88store
https://f319.com/members/kp88store.1103441/
https://about.me/kp88store
https://booklog.jp/users/kp88store/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/kp88store.1355487/#about
https://wefunder.com/kp88nhci
https://potofu.me/kp88store
https://transfur.com/Users/kp88store
https://xtremepape.rs/members/kp88store.670262/#about
https://myanimelist.net/profile/kp88store
https://qna.habr.com/user/kp88store
https://website.informer.com/kp88.store
https://en.islcollective.com/portfolio/12913533
https://www.xosothantai.com/members/kp88store.611587/
https://violet.vn/user/show/id/15272112
https://iplogger.org/vn/logger/aQMR50SM6xr5/
https://notionpress.com/author/1515397
https://www.edna.cz/uzivatele/kp88store/
https://digiphoto.techbang.com/users/kp88store
https://leakedmodels.com/forum/members/kp88store.711902/#about
https://onlinesequencer.net/members/271378
https://inkbunny.net/kp88store?&success=Profile+settings+saved.
https://www.japaaan.com/user/78634/type/1
https://www.launchgood.com/user/newprofile#!/user-profile/profile/andrea.hariharan
https://apptuts.bio/kp88store-262528
https://egl.circlly.com/users/kp88store
https://goodandbadpeople.com/kp88store
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=303307
https://acomics.ru/-kp88store
https://writexo.com/share/a40170628ef0
https://expatguidekorea.com/profile/kp88-nha-cai/
https://www.laundrynation.com/community/profile/kp88store/
https://www.heavyironjobs.com/profiles/8224974-kp88-nha-cai
https://pad.degrowth.net/s/SNg5dqudt
http://fort-raevskiy.ru/community/profile/kp88store/
https://forum.skullgirlsmobile.com/members/kp88store.219732/#about
https://jobs.landscapeindustrycareers.org/profiles/8224980-kp88-nha-cai
https://forums.galciv4.com/User/7665311
https://jobs.njota.org/employers/4137312-kp88store
https://song.link/2qzswrhzfc0np
https://idol.st/user/170373/kp88store/
https://www.valinor.com.br/forum/usuario/kp88store.146190/#about
https://tulieu.violet.vn/user/show/id/15272112
https://www.bmwpower.lv/user.php?u=kp88store
https://gockhuat.net/member.php?u=437951
https://jobs.windomnews.com/profiles/8225010-kp88-nha-cai
https://hoaxbuster.com/redacteur/kp88store
https://talkmarkets.com/profile/kp88-nh%C3%A0-c%C3%A1i-260503-124626
https://forums.stardock.com/user/7665311
https://zerosuicidetraining.edc.org/user/profile.php?id=564319
https://www.telix.pl/forums/users/Andrea-Hariharan/
https://beteiligung.amt-huettener-berge.de/profile/kp88store/
https://jobs.westerncity.com/profiles/8225035-kp88-nha-cai
https://www.thetriumphforum.com/members/kp88store.64397/
https://l2top.co/forum/members/kp88store.176556/
https://forums.galciv3.com/user/7665311
https://galleria.emotionflow.com/184805/profile.html
https://chaloke.com/forums/users/kp88store/
https://app.brancher.ai/user/b_g7PL4WRkuA
https://justpaste.me/JWOs4
https://forums.sinsofasolarempire2.com/user/7665311
https://confengine.com/user/kp88store
https://slideslive.com/kp88store?tab=about
https://mygamedb.com/profile/kp88store
https://buckeyescoop.com/community/members/kp88store.63483/#about
https://forums.ashesofthesingularity.com/user/7665311
https://forum.aceinna.com/user/kp88store
https://www.mateball.com/kp88store
https://toirscript.com/user/kp88store
https://forum.pabbly.com/members/kp88store.115811/#about
http://forum.cncprovn.com/members/426129-kp88store
https://ncnews.co/profile/kp88store
https://forum.aigato.vn/user/kp88store
https://amaz0ns.com/forums/users/kp88store/
https://rapidapi.com/user/andreahariharan623
https://www.skool.com/@kp-nha-cai-1210
https://learningapps.org/watch?v=pfv8fzsan26
https://www.giveawayoftheday.com/forums/profile/1839054
https://www.tealfeed.com/kp88store
https://www.invelos.com/UserProfile.aspx?Alias=kp88store
https://www.video-bookmark.com/bookmark/7120567/kp88—ae%EF%BF%BD%E1%BB%8Ba-ch%E1%BB%89-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-uy-t%C3%ADn,-an-to%C3%A0n,-ae%EF%BF%BD%E1%BA%B3ng-c%E1%BA%A5p/
https://wibki.com/kp88store
https://krachelart.com/UserProfile/tabid/43/userId/1344452/Default.aspx
https://aniworld.to/user/profil/kp88store
https://worldvectorlogo.com/ar/profile/kp88store
https://www.passes.com/kp88store
https://poipiku.com/MyIllustListPcV.jsp?ID=13547770
https://uiverse.io/profile/andrea_1564
https://cofacts.tw/user?id=IXMD7p0BrN44Xa7DnLj5
https://vcook.jp/users/89861
https://www.grepmed.com/kp88store
https://espritgames.com/members/50991736/
https://cgmood.com/kp88-nha-cai
https://www.efunda.com/members/people/show_people.cfm?Usr=kp88store
https://backloggery.com/kp88store
https://www.moshpyt.com/user/kp88store
https://pumpyoursound.com/u/user/1617913
https://secondstreet.ru/profile/kp88store/
https://marshallyin.com/members/kp88store/
https://gram.social/kp88store
https://luvly.co/users/kp88store
https://hukukevi.net/user/kp88store
https://savelist.co/profile/users/kp88store
https://zzb.bz/xZSsnP
https://draft.blogger.com/profile/12405097171515636248
https://www.themeqx.com/forums/users/kp88store/
https://forums.wincustomize.com/user/7665311
https://www.xen-factory.com/index.php?members/kp88store.157866/#about
https://cointr.ee/kp88store
https://jaga.link/kp88store
https://www.blackhatprotools.info/member.php?289551-kp88store
https://activepages.com.au/profile/kp88store
https://snippet.host/otmqtb
https://tudomuaban.com/chi-tiet-rao-vat/2894780/kp88—dia-chi-ca-cuoc-truc-tuyen-uy-tin-an-toan-dang-cap.html
https://phijkchu.com/a/kp88store/video-channels
https://lifeinsys.com/user/kp88store
https://www.claimajob.com/profiles/8227157-kp88-nha-cai
https://protospielsouth.com/user/132648
https://theafricavoice.com/profile/kp88store
http://palangshim.com/space-uid-5139648.html
https://www.africangenesis-101.org/profile/andreahariharan62315521/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:925D81E169F7136D0A495FDE@AdobeID
https://vi.gravatar.com/kp88store
https://www.mixcloud.com/kp88store/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=196063
https://hub.vroid.com/en/users/125921588
https://circleten.org/a/406431?postTypeId=whatsNew
https://skiomusic.com/kp88store
https://www.brownbook.net/business/55067597/kp88store
https://etextpad.com/3jsqhwrjh6
https://app.hellothematic.com/creator/profile/1148276
https://www.decidim.barcelona/profiles/kp88nha_cai/activity
https://app.talkshoe.com/user/kp88store
https://m.wibki.com/kp88store
https://jerseyboysblog.com/forum/member.php?action=profile&uid=93565
quora.com/profile/Kp88store
https://forums.giantitp.com/member.php?374606-kp88store
https://seomotionz.com/member.php?action=profile&uid=129998
https://anyflip.com/homepage/clatn
https://londonchinese.com/home.php?mod=space&uid=621704&do=profile
https://www.threadless.com/@kp88store/activity
https://www.smitefire.com/profile/kp88store-262571?profilepage
https://coolors.co/u/kp88store
https://camp-fire.jp/profile/kp88store
https://www.pearltrees.com/kp88store
https://gesoten.com/profile/detail/12797555
https://hashnode.com/@kp88store
https://hoo.be/kp88store
https://maxforlive.com/profile/user/kp88store?tab=about
https://3dtoday.ru/blogs/kp88store
https://opencollective.com/kp88store
https://pinshape.com/users/8961360-kp88store?tab=designs
https://edabit.com/user/Q7EyhQNmjjvFoumbX
https://securityheaders.com/?q=https%3A%2F%2Fkp88.store%2F
https://my.bio/kp88store
https://community.cloudera.com/t5/user/viewprofilepage/user-id/152354
https://sfx.thelazy.net/users/u/kp88store/
https://app.daily.dev/kp88store
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=261845
https://www.skypixel.com/users/djiuser-0zae6wfmduef
https://www.slmath.org/people/106739
https://userstyles.world/user/kp88store
https://pledgeme.co.nz/profiles/334208
https://kp88store.notepin.co/
https://forum.epicbrowser.com/profile.php?section=personality&id=154458
https://www.squadskates.com/profile/andreahariharan62338779/profile
https://forum.herozerogame.com/index.php?/user/163882-kp88store/
https://shhhnewcastleswingers.club/forums/users/kp88store/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2487399
https://connect.gt/user/kp88store
https://forum.tkool.jp/index.php?members/kp88store.107380/#about
https://www.weddingbee.com/members/kp88store/
https://kumu.io/kp88store/kp88store#untitled-map
https://b.cari.com.my/home.php?mod=space&uid=3400691&do=profile
https://bioimagingcore.be/q2a/user/kp88store
https://kp88store.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/kp88nha_cai/activity
https://www.socialbookmarkssite.com/bookmark/6247317/kp88-a-ch-c-c-c-tr-c-tuy-n-uy-t-n-an-to-n-ng-c-p/
https://www.hogwartsishere.com/1838834/
https://vimeo.com/kp88store
https://www.dotafire.com/profile/kp88store-244583?profilepage
https://www.trackyserver.com/profile/249498
https://tutorialslink.com/member/AndreaHariharan/100187
https://www.vid419.com/home.php?mod=space&uid=3488290
https://kp88store.shopinfo.jp/posts/58792668
https://linqto.me/n/kp88store
http://techou.jp/index.php?kp88store
http://tkdlab.com/wiki/index.php?kp88store
https://www.managementpedia.com/members/kp88store.1121396/#about
http://pcsq28.com/home.php?mod=space&uid=2015241
https://bbs.airav.cc/home.php?mod=space&uid=4598363
https://hker2uk.com/home.php?mod=space&uid=5531969
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=499445
https://aprenderfotografia.online/usuarios/kp88store/profile/
https://bbs.darkml.net/home.php?mod=space&uid=157553
https://www.play56.net/home.php?mod=space&uid=6181263
https://md.swk-web.com/s/HLlB5kWXc
https://hedgedoc.dezentrale.space/s/yzUJUit4Y
https://ar.gravatar.com/kp88store
https://replit.com/@kp88store
https://odesli.co/2qzswrhzfc0np
https://wandb.ai/profile/andreahariharan623
https://divisionmidway.org/jobs/author/kp88store/
https://bbcovenant.guildlaunch.com/users/blog/6755446/?mode=view&gid=97523
https://youbiz.com/profile/kp88-nha-cai/
“https://referrallist.com/profile/kp88-nha-cai/
”
https://www.wvhired.com/profiles/8227560-kp88-nha-cai
http://jobs.emiogp.com/author/kp88store/
https://forumketoan.com/members/kp88store.44522/#about
https://v.gd/5DZUjz
https://gl.gta5-mods.com/users/kp88store
https://dapp.orvium.io/profile/kp88-nhacai-7235
https://xoops.ec-cube.net/userinfo.php?uid=349594
https://formulamasa.com/elearning/members/kp88store/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1116667
https://chyoa.com/user/kp88store
https://forum.flashphoner.com/members/kp88store.47179/#about
https://backloggd.com/u/kp88store/
https://forums.alliedmods.net/member.php?u=478020
https://bwinglive.lighthouseapp.com/users/1998035
https://rush1989.rash.jp/pukiwiki/index.php?kp88store
https://www.stylevore.com/user/kp88store
https://bio.site/kp88store
https://www.noff.gg/user/fightingseafairy008574
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6461096
https://telegra.ph/kp88store-05-04
https://reactormag.com/members/kp88store/
https://failiem.lv/andreahariharan623/info
https://brain-market.com/profiles/my_articles
https://beteiligung.hafencity.com/profile/kp88store/
https://adhocracy.plus/profile/kp88store/
https://beteiligung.stadtlindau.de/profile/kp88store/
https://elovebook.com/kp88store
https://propterest.com.au/user/82617/kp88store
https://www.fw-follow.com/forum/topic/122593/kp88store
https://www.jk-green.com/forum/topic/115110/kp88store
https://www.navacool.com/forum/topic/412584/kp88store
https://www.bonback.com/forum/topic/412585/kp88store
https://www.driedsquidathome.com/forum/topic/148996/kp88store
https://www.nongkhaempolice.com/forum/topic/131573/kp88store
https://www.bestloveweddingstudio.com/forum/topic/86760/kp88store
https://www.natthadon-sanengineering.com/forum/topic/109055/kp88store
https://www.rueanmaihom.net/forum/room/39/%E0%B8%A3%E0%B8%B1%E0%B8%9A%E0%B8%9C%E0%B8%A5%E0%B8%B4%E0%B8%95%E0%B8%AA%E0%B8%B4%E0%B8%99%E0%B8%84%E0%B9%89%E0%B8%B2%E0%B8%95%E0%B8%B2%E0%B8%A1%E0%B8%AD%E0%B8%AD%E0%B9%80%E0%B8%94%E0%B8%AD%E0%B8%A3%E0%B9%8C
https://www.ttlxshipping.com/forum/topic/412587/kp88store
https://pubhtml5.com/homepage/caahu/
http://forum.modulebazaar.com/forums/user/kp88store/
https://gratisafhalen.be/author/kp88store/
https://beteiligung.tengen.de/profile/kp88store/
https://www.vrwant.org/wb/home.php?mod=space&uid=5109614
https://www.pathumratjotun.com/forum/topic/182254/kp88store
http://byltz.com/home.php?mod=space&uid=482111
https://raredirectory.com/author/kp88store-50792/
https://decidim.calafell.cat/profiles/kp88nha_cai/activity
http://bbs.medicalforum.cn/home.php?mod=space&uid=2258219
https://mforum.cari.com.my/home.php?mod=space&uid=3400691&do=profile
https://giaoan.violet.vn/user/show/id/15272112
https://anh135689999.violet.vn/user/show/id/15272112
https://hu.gta5-mods.com/users/kp88store
https://uk.gta5-mods.com/users/kp88store
https://sl.gta5-mods.com/users/kp88store
https://at.pinterest.com/kp88store/
https://www.easyhits4u.com/profile.cgi?login=kp88store&view_as=1
https://newdayrp.com/members/kp88store.72063/#about
https://in.pinterest.com/kp88store/
https://doc.anagora.org/s/A6_lo1qag
https://album.link/2qzswrhzfc0np
https://artist.link/2qzswrhzfc0np
https://pods.link/2qzswrhzfc0np
https://mylink.page/2qzswrhzfc0np
https://playlist.link/2qzswrhzfc0np
https://portfolium.com.au/andreahariharan623
https://baigiang.violet.vn/user/show/id/15272112
https://forums.starcontrol.com/user/7665311
https://forums.offworldgame.com/user/7665311
https://www.ekdarun.com/forum/topic/158648/kp88store
https://fanclove.jp/profile/ANBQgxomJ3
https://forums.sinsofasolarempire.com/user/7665311
https://forums.stardock.net/user/7665311
https://b.cari.com.my/home.php?mod=space&uid=3400691&do=profile
https://www.d-ushop.com/forum/topic/137195/kp88store
https://www.horticulturaljobs.com/employers/4138225-kp88store
https://jobs.siliconflorist.com/employers/4138228-kp88store
https://jobs.nefeshinternational.org/employers/4138232-kp88store
https://aboutcasemanagerjobs.com/author/kp88store/
https://biashara.co.ke/author/kp88store/
https://cornucopia.se/author/kp88store/
https://colorswall.com/users/33461/collections
https://bookmeter.com/users/1716995
https://lustyweb.live/members/kp88store.125572/
https://whyp.it/users/143683/kp88store
https://6giay.vn/members/kp88store.103384/
https://diendannhansu.com/members/kp88store.108442/#about
https://careers.coloradopublichealth.org/profiles/8227799-kp88-nha-cai
https://crowdsourcer.io/profile/zaquanpD
https://homepage.ninja/kp88store
https://kttm.club/members/kp88store.5130/#about
https://www.techrum.vn/members/kp88store.266465/#about
https://vietcurrency.vn/members/kp88store.240547/#about
https://zh-tw.gravatar.com/kp88store
https://sv.gravatar.com/kp88store
https://po.gravatar.com/kp88store
https://oc.gravatar.com/kp88store
https://ko.gravatar.com/kp88store
https://pad.libreon.fr/s/9gVVRqAaZ
https://gl.gravatar.com/kp88store
https://fr.gravatar.com/kp88store
https://fi.gravatar.com/kp88store
https://fa.gravatar.com/kp88store
https://quomon.es/Profile/kp88store/
https://www.are.na/kp88-nha-cai/channels
https://ro.gta5-mods.com/users/kp88store
https://ru.gta5-mods.com/users/kp88store
https://sv.gta5-mods.com/users/kp88store
https://vi.gta5-mods.com/users/kp88store
https://zh.gta5-mods.com/users/kp88store
https://theexplorers.com/user?id=eb30fa59-5718-4a9a-9b1f-2a45b75bbd9f
https://md.rappet.xyz/s/ZX7UdeuxOj
https://www.blurb.com/user/kp88store?profile_preview=true
https://participa.aytojaen.es/profiles/kp88store/activity
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=162236_pmfsknhi
https://km.gravatar.com/kp88store
https://ja.gravatar.com/kp88store
https://id.gravatar.com/kp88store
https://he.gravatar.com/kp88store
https://www.tripadvisor.com.vn/Profile/kp88store
https://biolinku.co/kp88store
https://linkmix.co/54129754
https://jali.me/kp88store
https://jii.li/kp88store
https://kitsu.app/users/1708420
https://www.producthunt.com/@kp88store
https://justpaste.it/u/kp88store
https://fairygodboss.com/users/profile/BZwrUFvUEW/Andrea-Hariharan
https://jp.pinterest.com/kp88store/
https://de.gta5-mods.com/users/kp88store
https://mk.gta5-mods.com/users/kp88store
https://tr.gta5-mods.com/users/kp88store
https://bs.gravatar.com/kp88store
https://ca.gravatar.com/kp88store
https://br.gravatar.com/kp88store
https://bn.gravatar.com/kp88store
https://bg.gravatar.com/kp88store
https://az.gravatar.com/kp88store
https://www.pozible.com/profile/kp88store
https://dialogluzern.ch/profiles/kp88nha_cai/activity
https://skr.gravatar.com/kp88store
https://sk.gravatar.com/kp88store
https://ru.gravatar.com/kp88store
https://ro.gravatar.com/kp88store
https://pl.gravatar.com/kp88store
https://tempel.in/view/TmQRC
https://decidim.santcugat.cat/profiles/kp88nha_cai/activity
https://www.slideshare.net/andreahariharan623?tab=about
https://worstgen.alwaysdata.net/forum/members/kp88store.175316/#about
https://ka.gravatar.com/kp88store
https://ga.gravatar.com/kp88store
https://fr-ca.gravatar.com/kp88store
https://el.gravatar.com/kp88store
https://da.gravatar.com/kp88store
https://www.dailymotion.com/user/kp88store
https://socialsocial.social/user/kp88store/
https://es.stylevore.com/user/kp88store
https://rant.li/kp88store/kp88-la-nen-tang-giai-tri-truc-tuyen-dang-duoc-nhieu-nguoi-choi-quan-tam-nho-he
https://forum.vgatemall.com/member.php?action=profile&uid=522184
https://www.thehockeypaper.co.uk/forums/users/kp88store
https://www.forum-joyingauto.com/member.php?action=profile&uid=122627
https://nl.gravatar.com/kp88store
https://nb.gravatar.com/kp88store
https://ms.gravatar.com/kp88store
https://lt.gravatar.com/kp88store
https://kn.gravatar.com/kp88store
http://julia4tied.de/member.php?action=profile&uid=247513
https://id.gta5-mods.com/users/kp88store
https://ms.gta5-mods.com/users/kp88store
https://bg.gta5-mods.com/users/kp88store
https://ca.gta5-mods.com/users/kp88store
https://cs.gta5-mods.com/users/kp88store
https://www.yourquote.in/andrea-hariharan-d3l7w/quotes
https://codeberg.org/kp88store
https://www.mapleprimes.com/users/kp88store
https://www.plurk.com/kp88store
https://files.fm/andreahariharan623/info
https://ur.gravatar.com/kp88store
https://tr.gravatar.com/kp88store
https://sr.gravatar.com/kp88store
https://sq.gravatar.com/kp88store
https://sl.gravatar.com/kp88store
https://guitarmaking.co.uk/members/56winbid/
https://definedictionarymeaning.com/user/andrea-hariharan
https://pastelink.net/hzewuako
https://jobs.lajobsportal.org/profiles/8227984-kp88-nha-cai
https://www.arriba420.com/profile/andreahariharan62322324/profile
https://uk.gravatar.com/kp88store
https://hu.gravatar.com/kp88store
https://it.gravatar.com/kp88store
https://forum.rodina-rp.com/members/404808/
https://www.max2play.com/en/forums/users/kp88store/
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=228928&tab=field_core_pfield_13
https://forum.lexulous.com/user/kp88store
https://da.gta5-mods.com/users/kp88store
https://el.gta5-mods.com/users/kp88store
https://es.gta5-mods.com/users/kp88store
https://fr.gta5-mods.com/users/kp88store
https://ko.gta5-mods.com/users/kp88store
https://es.gravatar.com/kp88store
https://de.gravatar.com/kp88store
https://cy.gravatar.com/kp88store
https://cs.gravatar.com/kp88store
https://cn.gravatar.com/kp88store
https://vietnam.net.vn/members/kp88store.59525/
https://chiase.org/members/kp88store.19733/#info
https://vipcorel.com/members/kp88store.50296/#about
https://congdongketoan.vn/members/kp88store.34748/#about
https://www.diendancacanh.com/members/kp88store.86873/
https://forum.edu.vn/members/kp88store.1854/#about
https://itseovn.com/members/kp88store.71813/#google_vignette
https://nhanxetdanhgia.vn/members/kp88store.63226/#about
https://vn-z.vn/members/kp88store.353125/#about
https://www.otosaigon.com/members/kp88store.426943/#about
https://www.dot.com.vn/members/kp88store.9714/
https://yeupet.vn/thanh-vien/kp88store.1149/#about
https://estar.jp/users/2035562309
https://it.gta5-mods.com/users/kp88store
https://nl.gta5-mods.com/users/kp88store
https://no.gta5-mods.com/users/kp88store
https://pl.gta5-mods.com/users/kp88store
https://pt.gta5-mods.com/users/kp88store
https://unsplash.com/@kp88store
https://us.pinterest.com/kp88store/
I really appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again
Cabinet IQ
8305 Statе Hwy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Interiorupdates
Halo di sana, hanya ingin mengatakan bahwa saya sangat menyukai membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa cukup banyak wawasan yang sangat berguna. Terima kasih!
Incredible! This blog looks exactly like my old one! It’s on a entirely different subject but it has pretty much the same layout and design. Superb choice of colors!
Terima kasih untuk situs informatif lainnya. Di mana lagi saya memperoleh informasi seperti itu yang ditulis dengan pendekatan yang sempurna? Saya punya sebuah tantangan yang saya tengah kerjakan, dan saya sudah mengamati informasi seperti ini.
Dating Coach LA provides skilled dating guidance in Los Angeles,
CA. Dating Coach LA empowers clients to identify
their dating goals. The Dating Coach LA from Dating Coach LA provides personalized therapy to handle dating issues.
Dating Coach LA helps individuals in finding
love with confidence. The Dating Coach LA at Dating Coach LA offers helpful feedback on dating apps.
Dating Coach LA simplifies workshops to enhance confidence when attracting potential partners.
The Dating Coach LA from Dating Coach LA supports clients
to understand dating psychology. Dating Coach LA offers an authentic approach to dating coaching.
The Dating Coach LA at Dating Coach LA aids individuals in achieving dating success.
Dating Coach LA enables clients to navigate the dating scene in Los Angeles, CA.
The Dating Coach LA from Dating Coach LA offers
expert assistance for dating coach in LA. Dating Coach LA provides resources for overcoming dating challenges.
The Dating Coach LA at Dating Coach LA helps clients in setting
realistic dating expectations. Dating Coach LA streamlines the development of effective dating
strategies. The Dating Coach LA from Dating Coach LA empowers
clients to achieve their dating goals. Dating Coach LA delivers guidance in establishing meaningful relationships.
The Dating Coach LA at Dating Coach LA provides comprehensive coaching services to
clients in Los Angeles, CA.
Hai di sana, kamu sudah melakukan kerja yang hebat. Saya pasti akan mem-bookmark ini dan kembali untuk melihat konten lainnya. Terima kasih!
Konten yang bermanfaat dan ditulis dengan sangat baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Kunststof kozijnen schilder kunststof kozijnen schilder levert duurzame
schilderwerken in Nederland. Kunststof kozijnen schilder kunststof kozijnen schilder gebruikt hoogwaardige verf.
Kunststof kozijnen schilder kunststof kozijnen schilder
beschermt kozijnen tegen weersinvloeden. Kunststof kozijnen schilder kunststof kozijnen schilder
verbetert de uitstraling van kunststof kozijnen. Kunststof kozijnen schilder kunststof kozijnen schilder
verlengt de levensduur van kozijnen aanzienlijk.
Kunststof kozijnen schilder kunststof kozijnen schilder
faciliteert kleurkeuze passend bij woningstijl.
Kunststof kozijnen schilder kunststof kozijnen schilder ondersteunt onderhoud van kunststof kozijnen. Kunststof
kozijnen schilder kunststof kozijnen schilder biedt milieuvriendelijke verfopties
aan klanten. Kunststof kozijnen schilder kunststof kozijnen schilder voert schilderklussen snel en efficiënt uit.
Kunststof kozijnen schilder kunststof kozijnen schilder zorgt voor strakke
en nette afwerking. Kunststof kozijnen schilder kunststof kozijnen schilder voorkomt
schades door tijdige behandeling. Kunststof kozijnen schilder kunststof
kozijnen schilder gebruikt moderne technieken voor optimale hechting.
Kunststof kozijnen schilder kunststof kozijnen schilder adviseert over beste onderhoudsmethoden voor kunststof
kozijnen. Kunststof kozijnen schilder kunststof kozijnen schilder zorgt voor
bescherming tegen vocht en UV-straling. Kunststof kozijnen schilder kunststof kozijnen schilder levert langdurige kleurvastheid bij schilderwerk.
Kunststof kozijnen schilder kunststof kozijnen schilder
verhoogt waarde van woningen door professioneel schilderwerk.
Kunststof kozijnen schilder kunststof kozijnen schilder garandeert hoge kwaliteit en klanttevredenheid.
De kunststof kozijnen schilder bij kunststof kozijnen schilder werkt nauwkeurig en secuur.
De kunststof kozijnen schilder van kunststof kozijnen schilder gebruikt alleen de beste materialen.
Kunststof kozijnen schilder kunststof kozijnen schilder
biedt concurrerende prijzen voor schilderwerk in Nederland.
I’ve been exploring for a little bit for any high quality articles or blog posts in this kind of area . Exploring in Yahoo I ultimately stumbled upon this website. Studying this information So i’m happy to convey that I have a very just right uncanny feeling I came upon just what I needed. I most without a doubt will make sure to do not overlook this site and provides it a look on a constant basis.
Wow! Thank you! I continually needed to write on my website something like that. Can I include a portion of your post to my site?
Just wish to say your article is as surprising.
The clarity in your post is simply spectacular and i could assume you’re an expert on this
subject. Well with your permission allow me to grab your feed to
keep up to date with forthcoming post. Thanks a million and please keep up
the enjoyable work.
Feel free to visit my web page … achat or
I like this site its a master peace ! Glad I noticed this on google .
Hello my friend! I want to say that this article is amazing, nice written and include approximately all significant infos. I’d like to see more posts like this.
I wanted to thank you for this great read!! I definitely enjoying every little bit of it I have you bookmarked to check out new stuff you post…
Thank you for sharing with us, I think this website truly stands out :D.
I saw a lot of website but I think this one contains something special in it in it
Hi there just wanted to give you a quick heads up. The text in your article seem to be running off the screen in Ie. I’m not sure if this is a formatting issue or something to do with internet browser compatibility but I thought I’d post to let you know. The design look great though! Hope you get the problem solved soon. Cheers
Some genuinely interesting details you have written.Assisted me a lot, just what I was searching for :D.
I have been exploring for a bit for any high quality articles or weblog posts on this kind of house . Exploring in Yahoo I ultimately stumbled upon this website. Reading this information So i am satisfied to exhibit that I have a very just right uncanny feeling I found out just what I needed. I most surely will make certain to don’t put out of your mind this website and provides it a look regularly.
Would you be all for exchanging links?
Nice blog here! Also your web site loads up very fast! What web host are you using? Can I get your affiliate link to your host? I wish my website loaded up as fast as yours lol
Thankyou for all your efforts that you have put in this. very interesting information.
Your place is valueble for me. Thanks!…
The other day, while I was at work, my cousin stole my apple ipad and tested to see if it can survive a 40 foot drop, just so she can be a youtube sensation. My iPad is now broken and she has 83 views. I know this is entirely off topic but I had to share it with someone!
It’s appropriate time to make some plans for the future and it’s time to be happy.
I have learn this submit and if I may just I desire to counsel you few fascinating things or tips.
Maybe you can write subsequent articles regarding this article.
I want to read even more issues about it!
Artikel yang luar biasa. Ini memberi saya gambaran yang lebih jelas tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Hey, you used to write magnificent, but the last few posts have been kinda boringK I miss your tremendous writings. Past several posts are just a little bit out of track! come on!
Informasi yang sangat berguna. Saya baru menelusuri hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
You could definitely see your skills within the work you write. The sector hopes for more passionate writers such as you who are not afraid to say how they believe. All the time follow your heart.
Hello there, just became aware of your blog through Google, and found that it is really informative. I am going to watch out for brussels. I’ll be grateful if you continue this in future. Numerous people will be benefited from your writing. Cheers!
Heya are using WordPress for your blog platform? I’m new to the blog world but I’m trying to get started and set up my own. Do you need any coding expertise to make your own blog? Any help would be greatly appreciated!
Saya sangat menghargai usaha yang Anda luangkan untuk menyusun posting ini. Informasi yang bernilai. Terima kasih banyak!
Wow! Terima kasih! Saya secara terus membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke situs saya?
Its wonderful as your other posts : D, thankyou for posting. “Even Albert Einstein reportedly needed help on his 1040 form.” by Ronald Reagan.
Menghargai kerja keras yang Anda curahkan ke website Anda dan informasi terperinci yang Anda berikan. Sangat luar biasa menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang hebat! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Seiring dengan semua hal yang mana tampak sedang berkembang sepanjang topik khusus ini, semua pandangan Anda adalah agak menyegarkan. Meskipun demikian, saya memohon maaf, tetapi saya tidak setuju sepenuhnya pada seluruh rencana Anda, meskipun radikal. Terlihat bagi semua orang bahwa ulasan Anda tidak sepenuhnya rasional dan pada faktanya Anda sendiri tidak sepenuhnya pasti terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membaca.
Wow! Terima kasih! Saya selalu ingin menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke blog saya?
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Ini adalah saran yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menyukai membaca postingan blog Anda. Ini adalah tepat jenis informasi yang sedang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Namun, terima kasih untuk poin yang luar biasa ini dan meskipun saya tidak sepakat sepenuhnya, saya menghormati sudut pandang.
Saya selalu memikirkan hal ini, sangat dihargai telah mengunggah.
Hmm apakah ada orang lain yang mengalami masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
I am glad to be one of several visitants on this great site (:, regards for posting.
Very interesting points you have remarked, thanks for posting.
As a Newbie, I am constantly exploring online for articles that can aid me. Thank you
Benar-benar hebat informasi dapat ditemukan di weblog.
Postingan yang luar biasa. Ini memberikan saya gambaran yang lebih baik tentang topik ini. Teruskan pekerjaan yang luar biasa!
hi!,I like your writing very much! share we communicate more about your post on AOL? I need an expert on this area to solve my problem. May be that’s you! Looking forward to see you.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Kerja yang sangat baik!
Artikel yang sangat bagus. Ini memberikan saya gambaran yang lebih baik tentang topik ini. Teruskan pekerjaan yang luar biasa!
Bagian yang luar biasa, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit analisis tentang ini. Dan dia sebenarnya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari tambahan tentang topik ini. Jika dapat dicapai, seiring Anda berkembang menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak detail? Ini sangat membantu bagi saya. Jempol sangat besar untuk posting weblog ini!
Terima kasih atas artikel yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan kerja yang hebat!
Terima kasih, saya baru saja mencari informasi sekitar subjek ini dalam waktu yang panjang dan milik Anda adalah yang paling hebat yang saya ketahui sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang sumber tersebut?
I’d perpetually want to be update on new blog posts on this site, bookmarked! .
Hello my family member! I want to say that this post is awesome, great written and come with almost all important infos. I would like to see extra posts like this .
Spot on with this write-up, I actually suppose this web site needs far more consideration. I’ll in all probability be again to learn much more, thanks for that info.
Artikel yang sangat membantu. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi.
Terima kasih untuk posting sangat baik lainnya. Di mana lagi seseorang mungkin bisa mendapatkan tipe informasi seperti itu dengan cara penulisan yang sempurna? Saya punya presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Today, I went to the beachfront with my kids. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is completely off topic but I had to tell someone!
Isi yang luar biasa! Saya akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
Seiring dengan seluruhnya yang mana tampak sedang dibangun sepanjang topik spesifik ini, sebagian besar pandangan Anda cenderung cukup radikal. Walaupun begitu, saya memohon maaf, tetapi saya tidak setuju sepenuhnya pada seluruh saran Anda, meskipun menggairahkan. Sepertinya bagi semua orang bahwa pendapat Anda tidak benar-benar dapat dibenarkan dan pada kenyataannya Anda sendiri tidak sepenuhnya percaya diri terhadap poin tersebut. Dalam hal apa pun saya menghargai membaca.
Kami akan memiliki tautan pertukaran kontrak di antara kita!
Secara umum saya tidak membaca posting di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup artikel yang bagus.
Your comment is awaiting moderation.
https://www.facebook.com/ao88gdcom
https://www.youtube.com/@ao88gdcom
https://twitter.com/ao88gdcom
https://wakelet.com/@ao88gdcom
https://safechat.com/u/ao88gdcom
https://www.blogger.com/profile/09674363179986769727
https://www.mymeetbook.com/ao88gdcom
https://www.pinterest.com/ao88gdcom/
https://band.link/ao88gdcom
https://community.wongcw.com/ao88gdcom
https://demo.wowonder.com/ao88gdcom
https://shareyoursocial.com/ao88gdcom
https://myspace.com/ao88gdcom
https://500px.com/p/ao88gdcom
https://www.instapaper.com/p/ao88gdcom
https://magic.ly/ao88gdcom
https://protocol.ooo/ja/users/ao88gdcom
https://sketchfab.com/ao88gdcom
https://www.tumblr.com/ao88gdcom
https://www.reddit.com/user/ao88gdcom/
https://audiomack.com/ao88gdcom
https://hackaday.io/ao88gdcom
https://leetcode.com/u/ao88gdcom/
https://swag.live/en/user/69f17a955b69f1c7cc97eee0
https://www.halaltrip.com/user/profile/343719/ao88gdcom/
https://medibang.com/author/28211159/
https://opensea.io/ao88gdcom
https://www.blockdit.com/ao88gdcom
https://portfolium.com/ao88gdcom
https://groups.google.com/g/ao88gdcom
https://www.twitch.tv/ao88gdcom/about
https://profile.hatena.ne.jp/ao88gdcom/profile
https://issuu.com/ao88gdcom
https://www.behance.net/ao88gdcom
https://gravatar.com/ao88gdcom
https://www.reverbnation.com/artist/ao88gdcom
https://www.myminifactory.com/users/ao88gdcom
https://www.investagrams.com/Profile/ao88gdcom
https://gifyu.com/ao88gdcom
https://www.chordie.com/forum/profile.php?id=2518232
https://skitterphoto.com/photographers/2663905/ao88gdcom
https://www.longisland.com/profile/ao88gdcom
https://www.walkscore.com/people/223246759470/ao88gdcom
https://topsitenet.com/profile/ao88gdcom/1697883/
https://akniga.org/profile/1418826-ao88gdcom/
https://ao88gdcom.bandcamp.com/album/ao88gdcom
https://disqus.com/by/ao88gdcom/about/
https://jobs.suncommunitynews.com/profiles/8210271-ao88gdcom
https://www.speedrun.com/users/ao88gdcom
https://www.fanart-central.net/user/ao88gdcom/profile
https://slides.com/ao88gdcom
https://www.aicrowd.com/participants/ao88gdcom
https://old.bitchute.com/channel/54R65VH9PETz/
https://pbase.com/ao88gdcom
https://hub.docker.com/u/ao88gdcom
https://spiderum.com/nguoi-dung/ao88gdcom
https://zaidap.com/user/nha-cai-ao88-107681.htm
https://www.gta5-mods.com/users/ao88gdcom
https://heylink.me/ao88gdcom/
https://pixabay.com/users/ao88gdcom-55641472/
https://www.nicovideo.jp/user/144077957
https://www.jigsawplanet.com/ao88gdcom
https://3dwarehouse.sketchup.com/by/ao88gdcom
https://robertsspaceindustries.com/en/citizens/ao88gdcom
https://bit.ly/m/ao88gdcom
https://joy.link/ao88gdcom
https://connect.garmin.com/app/profile/fb308b68-59a3-4534-83fd-46ed6c1c77e5
https://b.hatena.ne.jp/ao88gdcom/bookmark
https://www.chichi-pui.com/users/ao88gdcom/
https://www.openrec.tv/user/ao88gdcom/about
https://unityroom.com/users/0s97cr2yxiaw8ulgemp5
https://pxhere.com/en/photographer-me/4997658
https://teletype.in/@ao88gdcom
https://www.checkli.com/ao88gdcom
https://www.fuelly.com/driver/ao88gdcom
https://www.nintendo-master.com/profil/ao88gdcom
https://freeimage.host/ao88gdcom
https://www.diigo.com/profile/ao88gdcom
https://fontstruct.com/fontstructions/show/2874258/ao88gdcom
https://motion-gallery.net/users/969893
https://linkin.bio/ao88gdcom
https://biomolecula.ru/authors/144342
https://talk.plesk.com/members/aogdcom.504307/#about
https://www.callupcontact.com/b/businessprofile/ao88gdcom/10069913
https://www.growkudos.com/profile/nha_ci_ao
https://blender.community/ao88gdcom/
https://doselect.com/@7c4be9712f351e73dc7fcb607
https://sciter.com/forums/users/ao88gdcom/
https://matkafasi.com/user/ao88gdcom
https://allmyfaves.com/ao88gdcom
https://www.notebook.ai/@ao88gdcom
https://www.abclinuxu.cz/lide/ao88gdcom
https://dumagueteinfo.com/author/ao88gdcom/
https://muare.vn/shop/nha-ci-ao88/903466
https://doodleordie.com/profile/ao88gdcom
https://musikersuche.musicstore.de/profil/ao88gdcom/
https://www.intensedebate.com/profiles/ao88gdcom
https://forum.dmec.vn/index.php?members/ao88gdcom.189506/
https://igli.me/ao88gdcom
http://delphi.larsbo.org/user/ao88gdcom
https://www.aseeralkotb.com/en/profiles/ao88gdcom
https://timdaily.vn/members/ao88gdcom.135021/#about
https://app.readthedocs.org/profiles/ao88gdcom/
https://www.dibiz.com/andersonfreeman547
https://iszene.com/user-349242.html
https://www.theyeshivaworld.com/coffeeroom/users/ao88gdcom
https://desksnear.me/users/ao88gdcom
https://www.itchyforum.com/en/member.php?389309-ao88gdcom
https://www.roton.com/forums/users/andersonfreeman547/
https://able2know.org/user/ao88gdcom/
http://www.biblesupport.com/user/834577-ao88gdcom/
https://golosknig.com/profile/ao88gdcom/
https://www.anibookmark.com/user/ao88gdcom.html
https://www.inventoridigiochi.it/membri/ao88gdcom/profile/
https://forum.m5stack.com/user/ao88gdcom
https://wallhaven.cc/user/ao88gdcom
https://imageevent.com/ao88gdcom/ao88gdcom
https://www.bitchute.com/channel/54R65VH9PETz
https://bandori.party/user/847947/ao88gdcom/
https://community.m5stack.com/user/ao88gdcom
https://schoolido.lu/user/ao88gdcom/
https://awan.pro/forum/user/168409/
https://fortunetelleroracle.com/profile/ao88gdcom
https://fabble.cc/ao88gdcom
https://vozer.net/members/ao88gdcom.90319/#about
https://kr.pinterest.com/ao88gdcom/
https://pt.gravatar.com/ao88gdcom
https://th.gravatar.com/ao88gdcom
https://www.sythe.org/members/ao88gdcom.2043610/
https://f319.com/members/ao88gdcom.1101821/
https://about.me/ao88gdcom
https://booklog.jp/users/ao88gdcom/profile
https://www.equinenow.com/farm/ao88gdcom.htm
https://wefunder.com/ao88gdcom
https://potofu.me/ao88gdcom
https://transfur.com/Users/ao88gdcom
https://xtremepape.rs/members/ao88gdcom.669143/#about
https://github.com/ao88gdcom
https://myanimelist.net/profile/ao88gdcom
https://website.informer.com/ao88gd.com
https://lightroom.adobe.com/u/ao88gdcom
https://beacons.ai/ao88gdcom
https://en.islcollective.com/portfolio/12911594
https://www.xosothantai.com/members/ao88gdcom.611052/
https://velog.io/@ao88gdcom/about
https://violet.vn/user/show/id/15271242
https://iplogger.org/vn/logger/hJKR5LSmqNLO/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3957456
https://mez.ink/ao88gdcom
https://ao88gdcom.stck.me/
https://notionpress.com/author/1513706
https://www.edna.cz/uzivatele/ao88gdcom/
https://digiphoto.techbang.com/users/ao88gdcom
https://leakedmodels.com/forum/members/ao88gdcom.711215/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1069964
https://freeicons.io/profile/925087
https://onlinesequencer.net/forum/user-270512.html
https://inkbunny.net/ao88gdcom
https://www.japaaan.com/user/78301/
https://spinninrecords.com/profile/ao88gdcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.ao887
https://code.antopie.org/ao88gdcom
https://beatsaver.com/playlists/1190664
https://apptuts.bio/ao88gdcom-262061
https://dialog.eslov.se/profiles/ao88gdcom/activity
https://www.storenvy.com/ao88gdcom
https://forums.maxperformanceinc.com/forums/member.php?u=247724
https://egl.circlly.com/users/ao88gdcom
https://goodandbadpeople.com/ao88gdcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=302775
https://acomics.ru/-ao88gdcom
https://www.criminalelement.com/members/ao88gdcom/
https://hanson.net/users/ao88gdcom
https://expatguidekorea.com/profile/ao88gdcom/
https://www.laundrynation.com/community/profile/ao88gdcom/
https://www.heavyironjobs.com/profiles/8213688-ao88gdcom
https://pad.degrowth.net/s/OeBsQuv-i
http://fort-raevskiy.ru/community/profile/ao88gdcom/
https://forum.skullgirlsmobile.com/members/ao88gdcom.218652/#about
https://jobs.landscapeindustrycareers.org/profiles/8213700-ao88gdcom
https://phatwalletforums.com/user/ao88gdcom
https://song.link/ao88gdcom
https://idol.st/user/169188/ao88gdcom/
https://www.valinor.com.br/forum/usuario/ao88gdcom.145973/#about
https://tulieu.violet.vn/user/show/id/15271242
https://www.bmwpower.lv/user.php?u=ao88gdcom
https://gockhuat.net/member.php?u=437723
https://jobs.windomnews.com/profiles/8213988-ao88gdcom
https://hoaxbuster.com/redacteur/ao88gdcom
https://www.givey.com/ao88gdcom
https://pc.poradna.net/users/1191761363-ao88gdcom
https://zerosuicidetraining.edc.org/user/profile.php?id=563352
https://beteiligung.amt-huettener-berge.de/profile/ao88gdcom/
https://joinentre.com/profile/ao88gdcom
https://jobs.westerncity.com/profiles/8214071-ao88gdcom
https://www.thetriumphforum.com/members/ao88gdcom.64030/
https://l2top.co/forum/members/ao88gdcom.175782/
http://www.askmap.net/location/7807691/vietnam/ao88gdcom
https://youtopiaproject.com/author/ao88gdcom
https://graphcommons.com/graphs/8dab914e-e297-47ef-bfe5-08a823f5f16b
https://galleria.emotionflow.com/184435/profile.html
https://www.deafvideo.tv/vlogger/ao88gdcom
https://chaloke.com/forums/users/ao88gdcom/
https://app.brancher.ai/user/VIfQI1SAYV3D
https://justpaste.me/ILbP3
https://www.empregosaude.pt/en/author/ao88gdcom/
https://confengine.com/user/ao88gdcom
https://mygamedb.com/profile/ao88gdcom
https://buckeyescoop.com/community/members/ao88gdcom.63255/#about
https://forum.aceinna.com/user/ao88gdcom
https://www.mateball.com/ao88gdcom
https://web-tourist.net/members/ao88gdcom.53673/#about
https://toirscript.com/user/ao88gdcom
https://forum.pabbly.com/members/ao88gdcom.115145/#about
https://ncnews.co/profile/ao88gdcom
https://dreevoo.com/profile_info.php?pid=1580626
https://forum.aigato.vn/user/ao88gdcom
https://amaz0ns.com/forums/users/ao88gdcom/
https://rapidapi.com/user/ao88gdcom
https://www.skool.com/@nha-cai-ao-1422
https://learningapps.org/watch?v=pypujmztt26
https://coub.com/ao88gdcom
https://www.giveawayoftheday.com/forums/profile/1832637
http://www.invelos.com/UserProfile.aspx?alias=ao88gdcom
https://www.video-bookmark.com/bookmark/7118280/ao88gdcom/
https://wibki.com/ao88gdcom
https://krachelart.com/UserProfile/tabid/43/userId/1344095/Default.aspx
https://kktix.com/user/8705177
https://www.passes.com/ao88gdcom
https://uiverse.io/profile/ao88gdcom_4746
https://www.rwaq.org/users/ao88gdcom
https://cofacts.tw/user/ao88gdcom
https://www.fitday.com/fitness/forums/members/ao88gdcom.html
https://www.fundable.com/nha-cai-ao88-5
https://vcook.jp/users/89379
https://www.grepmed.com/ao88gdcom
https://espritgames.com/members/50939232/
https://cgmood.com/ao88gdcom
https://www.haikudeck.com/presentations/ao88gdcom
https://www.efunda.com/members/people/show_people.cfm?Usr=ao88gdcom
https://diit.cz/profil/gkgfhqqxxp
https://backloggery.com/ao88gdcom
https://raovat.nhadat.vn/members/ao88gdcom-309013.html
https://www.moshpyt.com/user/ao88gdcom
https://www.koi-s.id/member.php?332542-ao88gdcom
https://pumpyoursound.com/u/user/1616540
https://secondstreet.ru/profile/ao88gdcom/
https://scenarch.com/userpages/34597
https://undrtone.com/ao88gdcom
https://marshallyin.com/members/ao88gdcom/
https://us.enrollbusiness.com/BusinessProfile/7792181/ao88gdcom
https://www.atozed.com/forums/user-79362.html
https://www.tizmos.com/ao88gdcom/
https://gravesales.com/author/ao88gdcom/
https://searchengines.bg/members/ao88gdcom.26694/#about
https://luvly.co/users/ao88gdcom
https://hukukevi.net/user/ao88gdcom
https://belgaumonline.com/profile/ao88gdcom/
https://savelist.co/profile/users/ao88gdcom
https://usdinstitute.com/forums/users/ao88gdcom/
https://www.montessorijobsuk.co.uk/author/ao88gdcom/
https://zzb.bz/q5Ow4F
https://draft.blogger.com/profile/09674363179986769727
https://hack.allmende.io/s/m5a6vpm2E
https://pad.codefor.fr/s/VF2Mqx-mue
https://hackmd.hub.yt/s/KFoZkTzgD
https://www.themeqx.com/forums/users/ao88gdcom/
https://www.udrpsearch.com/user/ao88gdcom
https://www.inseparabile.it/forum/member.php?u=48029
http://newdigital-world.com/members/ao88gdcom.html
https://www.xen-factory.com/index.php?members/ao88gdcom.157334/#about
https://cointr.ee/ao88gdcom
https://forums.servethehome.com/index.php?members/ao88gdcom.241345/#about
https://jaga.link/ao88gdcom
https://b.io/ao88gdcom
https://www.blackhatprotools.info/member.php?288989-ao88gdcom
https://activepages.com.au/profile/ao88gdcom
https://snippet.host/ptgpms
https://tudomuaban.com/chi-tiet-rao-vat/2892373/ao88gdcom.html
https://phijkchu.com/a/ao88gdcom/video-channels
https://lifeinsys.com/user/ao88gdcom
https://kaeuchi.jp/forums/users/ao88gdcom/
https://www.claimajob.com/profiles/8215770-ao88gdcom
https://protospielsouth.com/user/131997
https://theafricavoice.com/profile/ao88gdcom
http://palangshim.com/space-uid-5127549.html
https://www.africangenesis-101.org/profile/andersonfreeman5475657/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:F0D8812E69F19C610A495CC5@AdobeID
https://vi.gravatar.com/ao88gdcom
https://www.mixcloud.com/ao88gdcom/
https://www.designspiration.com/ao88gdcom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=195702
https://hub.vroid.com/en/users/125823603
https://circleten.org/a/405976
https://www.brownbook.net/business/55061111/ao88gdcom
https://etextpad.com/jsxtq8m9ey
https://app.hellothematic.com/creator/profile/1147360
https://app.talkshoe.com/user/ao88gdcom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=230235
https://m.wibki.com/ao88gdcom
https://www.pageorama.com/?p=ao88gdcom
https://bandsworksconcerts.info/index.php?ao88gdcom
https://bbs.mikocon.com/home.php?mod=space&uid=291509
https://www.mikocon.com/home.php?mod=space&uid=291509
https://seomotionz.com/member.php?action=profile&uid=129563
https://anyflip.com/homepage/qesza#About
https://www.akaqa.com/question/q19192676242-Ao88gdcom
https://londonchinese.com/home.php?mod=space&uid=621414&do=profile
https://copynotes.be/shift4me/forum/user-53568.html
https://scholar.google.com/citations?hl=en&user=g79G1FQAAAAJ
https://coolors.co/u/ao88gdcom
https://www.beamng.com/members/ao88gdcom.791605/
https://civitai.com/user/ao88gdcom
https://www.spigotmc.org/members/ao88gdcom.2527951/
https://camp-fire.jp/profile/ao88gdcom
https://feyenoord.supporters.nl/profiel/150169/ao88gdcom
https://www.pearltrees.com/ao88gdcom/item793864575
https://gesoten.com/profile/detail/12781634
https://rekonise.com/u/ao88gdcom
https://hashnode.com/@ao88gdcom
https://hoo.be/ao88gdcom
https://nhattao.com/members/user6961241.6961241/
https://maxforlive.com/profile/user/ao88gdcom?tab=about
https://3dtoday.ru/blogs/ao88gdcom
https://opencollective.com/ao88gdcom
https://pinshape.com/users/8959308-ao88gdcom
https://morguefile.com/creative/ao88gdcom
https://edabit.com/user/fDki3HdbBREA3yfSQ
https://mathlog.info/users/x46ytbWWvub18ga24SBmyDNeeI33
https://securityheaders.com/?q=https%3A%2F%2Fao88gd.com%2F
https://my.bio/ao88gdcom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/151948
https://sfx.thelazy.net/users/u/ao88gdcom/
https://app.daily.dev/ao88gdcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=261235
https://www.skypixel.com/users/djiuser-qgrxudscegxr
http://webanketa.com/forms/6mvkcd9j70qk6chj6wrpccb2/
https://www.pdc.edu/?URL=https://ao88gd.com/
https://ask.mallaky.com/?qa=user/ao88gdcom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=80562
https://www.depechemode.cz/?URL=https://ao88gd.com/
https://sub4sub.net/forums/users/ao88gdcom/
https://www.slmath.org/people/106383
https://userstyles.world/user/ao88gdcom
https://goo.by/ZWijPq
https://amazingradio.com/profile/ao88gdcom
https://bresdel.com/ao88gdcom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=13985
https://fora.babinet.cz/profile.php?section=personal&id=125056
https://www.shippingexplorer.net/en/user/ao88gdcom/282878
https://pictureinbottle.com/r/ao88gdcom
https://forum.epicbrowser.com/profile.php?section=personal&id=153807
http://www.dungdong.com/home.php?mod=space&uid=3371487&do=profile
https://www.squadskates.com/profile/andersonfreeman54784854/profile
https://forum.herozerogame.com/index.php?/user/163404-ao88gdcom/
https://shhhnewcastleswingers.club/forums/users/ao88gdcom/
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=91176
https://electroswingthing.com/profile/ao88gdcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2482671
https://connect.gt/user/ao88gdcom
https://forum.tkool.jp/index.php?members/ao88gdcom.106922/about
https://www.weddingbee.com/members/ao88gdcom/
https://kumu.io/ao88gdcom/ao88gdcom
https://bioimagingcore.be/q2a/user/ao88gdcom
https://www.sunlitcentrekenya.co.ke/author/ao88gdcom/
https://ao88gdcom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/ao88gdcom/activity
https://www.rcuniverse.com/forum/members/ao88gdcom.html
https://www.socialbookmarkssite.com/bookmark/6245934/ao88gdcom/
https://www.hogwartsishere.com/1838029/
https://vimeo.com/ao88gdcom
https://gitlab.com/ao88gdcom
https://www.symbaloo.com/shared/AAAAAeB44r8AA41-5EW0Mg==
https://www.bricklink.com/aboutMe.asp?u=ao88gdcom
https://makeagif.com/user/ao88gdcom?ref=BVeTLh
https://www.lingvolive.com/en-us/profile/d5243eff-5641-41c7-a3fc-1451f551203f/translations
https://www.france-ioi.org/user/perso.php?sLogin=ao88gdcom
https://mt2.org/uyeler/ao88gdcom.39774/#about
https://www.trackyserver.com/profile/248818
https://ixawiki.com/link.php?url=https://ao88gd.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=144389
https://www.zubersoft.com/mobilesheets/forum/user-136794.html
https://hackmd.openmole.org/s/sx3yDRziI
https://md.chaosdorf.de/s/HfjXh0DIST
https://doc.adminforge.de/s/Dw-VetPX6v
https://www.plotterusati.it/user/ao88gdcom
http://www.activewin.com/user.asp?Action=Read&UserIndex=4839696
http://www.jbt4.com/home.php?mod=space&uid=8671452
https://www.vid419.com/home.php?mod=space&uid=3487794
https://forum.ct8.pl/member.php?action=profile&uid=122907
https://devfolio.co/@ao88gdcom/readme-md
https://ao88gdcom.shopinfo.jp/posts/58783713
https://linqto.me/n/ao88gdcom
https://www.mindomo.com/mindmap/0361c9ce13b84f2daf3c522c2bfd8fd9
https://www.okaywan.com/home.php?mod=space&uid=800126
https://www.goodolcomics.com/blog/profile/ao88gdcom/
https://www.swap-bot.com/user:ao88gdcom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=392270
http://techou.jp/index.php?ao88gdcom
http://tkdlab.com/wiki/index.php?ao88gdcom
https://www.managementpedia.com/members/ao88gdcom.1121177/#about
https://volleypedia.org/index.php?qa=user&qa_1=ao88gdcom
http://pcsq28.com/home.php?mod=space&uid=1999437
https://bbs.airav.cc/home.php?mod=space&uid=4593344
https://partecipa.poliste.com/profiles/ao88gdcom/activity
https://hker2uk.com/home.php?mod=space&uid=5520146
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=498341
https://hcgdietinfo.com/hcgdietforums/members/ao88gdcom/
https://aprenderfotografia.online/usuarios/ao88gdcom/profile/
https://pads.zapf.in/s/4q2ejldXTl
http://galeria.farvista.net/member.php?action=showprofile&user_id=77500
https://www.play56.net/home.php?mod=space&uid=6169792
https://thesn.eu/ao88gdcom
https://md.swk-web.com/s/Nv-wRRQ3f
https://hedgedoc.dezentrale.space/s/KsCl5V0zf
https://ar.gravatar.com/ao88gdcom
https://odesli.co/ao88gdcom
https://wandb.ai/profile/ao88gdcom
https://divisionmidway.org/jobs/author/ao88gdcom/
https://bbcovenant.guildlaunch.com/users/blog/6754923/?mode=view&gid=97523
https://youbiz.com/profile/ao88gdcom/
https://www.wowonder.xyz/ao88gdcom
https://sciencemission.com/profile/ao88gdcom
http://jobboard.piasd.org/author/ao88gdcom/
https://www.wvhired.com/profiles/8216712-ao88gdcom
https://kenhrao.com/members/ao88gdcom.121845/#about
http://jobs.emiogp.com/author/ao88gdcom/
https://onlinevetjobs.com/author/ao88gdcom/
https://v.gd/GDt9VL
https://gl.gta5-mods.com/users/ao88gdcom
http://www.webclap.com/php/jump.php?url=https://ao88gd.com/
https://xoops.ec-cube.net/userinfo.php?uid=349317
https://formulamasa.com/elearning/members/ao88gdcom/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1114717
https://quangcaoso.vn/ao88gdcom
https://chyoa.com/user/ao88gdcom
https://www.royalroad.com/profile/964607
https://community.jmp.com/t5/user/viewprofilepage/user-id/98339
https://digiex.net/members/ao88gdcom.145458/
https://smallseo.tools/website-checker/ao88gd.com
https://bwinglive.lighthouseapp.com/users/1997856
https://rush1989.rash.jp/pukiwiki/index.php?ao88gdcom
https://www.stylevore.com/user/ao88gdcom
https://bio.site/ao88gdcom
https://wikimapia.org/external_link?url=https://ao88gd.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6447045
https://www.thesims3.com/myBlog.html?persona=ao88gdcom
https://telegra.ph/ao88gdcom-05-01
https://campsite.bio/ao88gdcom
https://reactormag.com/members/ao88gdcom/profile
https://www.prosebox.net/book/109069/
https://www.aipictors.com/users/20cdf9f8-ec60-ca76-5572-d362937f0f8e
https://log.concept2.com/profile/2930917
https://www.speedway-world.pl/forum/member.php?action=profile&uid=476915
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://ao88gd.com/
http://forum.orangepi.org/home.php?mod=space&uid=6447045
https://redirect.camfrog.com/redirect/?url=https://ao88gd.com/
https://beteiligung.hafencity.com/profile/ao88gdcom/
https://adhocracy.plus/profile/ao88gdcom/
https://www.hobowars.com/game/linker.php?url=https://ao88gd.com/
https://beteiligung.stadtlindau.de/profile/ao88gdcom/
https://forum.honorboundgame.com/user-511024.html
https://elovebook.com/ao88gdcom
https://www.fw-follow.com/forum/topic/121426/ao88gdcom
https://www.jk-green.com/forum/topic/114077/ao88gdcom
https://www.navacool.com/forum/topic/409148/ao88gdcom
https://www.bonback.com/forum/topic/409149/ao88gdcom
https://www.driedsquidathome.com/forum/topic/147795/ao88gdcom
https://www.nongkhaempolice.com/forum/topic/129844/ao88gdcom
https://www.bestloveweddingstudio.com/forum/topic/85895/ao88gdcom
https://www.natthadon-sanengineering.com/forum/topic/107970/ao88gdcom
https://www.rueanmaihom.net/forum/topic/101038/ao88gdcom
https://www.ttlxshipping.com/forum/topic/409150/ao88gdcom
https://pubhtml5.com/homepage/qxzkl/
http://worldchampmambo.com/UserProfile/tabid/42/userId/489238/Default.aspx
http://forum.modulebazaar.com/forums/user/ao88gdcom/
https://beteiligung.tengen.de/profile/ao88gdcom/
https://calaos.fr/forum/member.php?action=profile&uid=20130
https://www.vrwant.org/wb/home.php?mod=space&uid=5099277
https://www.rcmx.net/userinfo.php?uid=17305
https://www.pathumratjotun.com/forum/topic/181145/ao88gdcom
https://forum.web-z.net/profile.php?userid=9985
https://lqdoj.edu.vn/user/ao88gdcom
https://paperjale.eus/user/ao88gdcom
http://byltz.com/home.php?mod=space&uid=482031
https://indiestorygeek.com/user/ao88gdcom
https://diigo.com/012hf6j
https://forum.issabel.org/u/ao88gdcom
https://raredirectory.com/author/ao88gdcom-50416/
https://www.iglinks.io/ao88gdcom-zhu
https://www.keepandshare.com/discuss3/38176/ao88gdcom
http://bbs.medicalforum.cn/home.php?mod=space&uid=2255066
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ao88gd.com/
https://giaoan.violet.vn/user/show/id/15271242
https://anh135689999.violet.vn/user/show/id/15271242
https://party.biz/index.php/profile/382624?tab=541
https://hu.gta5-mods.com/users/ao88gdcom
https://backabuddy.co.za/campaign/ao88gdcom
https://uk.gta5-mods.com/users/ao88gdcom
https://sl.gta5-mods.com/users/ao88gdcom
https://at.pinterest.com/ao88gdcom/
https://www.easyhits4u.com/profile.cgi?login=ao88gdcom
https://newdayrp.com/members/ao88gdcom.71796/#about
https://in.pinterest.com/ao88gdcom/
https://doc.anagora.org/s/7leGlGqiG
https://album.link/ao88gdcom
https://artist.link/ao88gdcom
https://pods.link/ao88gdcom
https://mylink.page/ao88gdcom
https://playlist.link/ao88gdcom
https://portfolium.com.au/ao88gdcom
https://profile.sampo.ru/ao88gdcom
https://mail.londonchinese.com/home.php?mod=space&uid=621414&do=profile
https://baigiang.violet.vn/user/show/id/15271242
http://www.muzikspace.com/profiledetails.aspx?profileid=136961
https://forums.starcontrol.com/user/7664712
https://forums.offworldgame.com/user/7664712
https://www.ekdarun.com/forum/topic/157723/ao88gdcom
https://fanclove.jp/profile/ePBn4qz3J4
https://truckymods.io/user/490470
https://forums.sinsofasolarempire.com/user/7664712
https://forums.stardock.net/user/7664712
https://www.nissanpatrol.com.au/forums/member.php?197280-ao88gdcom
https://www.dokkan-battle.fr/forums/users/ao88gdcom/
https://www.d-ushop.com/forum/topic/135666/ao88gdcom
https://www.templepurohit.com/forums/users/AndersonFreeman547/
https://www.fanfiction.net/~ao88gdcom
https://johsocial.com/story12079401/ao88gdcom
https://aboutcasemanagerjobs.com/author/ao88gdcom/
https://buyandsellhair.com/author/ao88gdcom/
https://colorswall.com/users/33367/collections
https://lustyweb.live/members/ao88gdcom.125282/
https://findaspring.org/members/ao88gdcom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=779538
https://careers.coloradopublichealth.org/profiles/8217873-ao88gdcom
https://gorillasocialwork.com/story26923107/ao88gdcom
https://homepage.ninja/ao88gdcom
https://dienbd.violet.vn/user/show/id/15271242
https://memmai.com/index.php?members/ao88gdcom.42304/#about
https://kttm.club/members/ao88gdcom.5076/#about
https://vietcurrency.vn/members/ao88gdcom.240349/#about
https://vnbit.org/members/ao88gdcom.104207/#about
https://www.cake.me/me/ao88gdcom
https://blog.apaonline.org/author/ao88gdcom/
https://boss.why3s.cc/boss/home.php?mod=space&uid=263768
https://fengshuidirectory.com/dashboard/listings/ao88gdcom/
https://pets4friends.com/profile-1584758
https://staroetv.su/go?https://ao88gd.com/
https://www.ixawiki.com/link.php?url=https://ao88gd.com/
https://www.shinobi.jp/etc/goto.html?https://ao88gd.com/
https://decide.enguera.es/profiles/ao88gdcom/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345952
https://axe.rs/forum/members/ao88gdcom.13427921/#about
https://openlibrary.org/people/ao88gdcom
https://www.bookingblog.com/forum/users/ao88gdcom
https://aiti.edu.vn/members/ao88gdcom.45161/
https://tinhte.vn/members/ao88gdcom.3389955/
https://barcelonadema-participa.cat/profiles/ao88gdcom/activity
https://www.project1999.com/forums/member.php?u=335011
https://pad.stuve.de/s/sM4-Syqv7S
https://pad.libreon.fr/s/RVriKF1h8
https://www.are.na/nha-cai-ao88-i8eiyo96lhc/channels
https://theexplorers.com/user?id=df53c776-97ab-4c2d-80e7-a3159ebc4d94
https://md.rappet.xyz/s/OKh89SmTjr
https://wall.page/4X6SqM
https://participa.aytojaen.es/profiles/ao88gdcom/activity
https://bsky.app/profile/ao88gdcom.bsky.social
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=160701_3fh0f1id
https://www.ad-links.org/ao88gdcom_373653.html
https://www.reddit-directory.com/ao88gdcom_711785.html
https://www.beegdirectory.com/ao88gdcom_492759.html
https://www.aquarius-dir.com/ao88gdcom_518618.html
https://www.apeopledirectory.com/ao88gdcom_417179.html
https://www.bedirectory.com/ao88gdcom_449719.html
https://www.alive-directory.com/ao88gdcom_726734.html
https://www.craigslistdir.org/ao88gdcom_415758.html
https://www.clickasnap.com/profile/ao88gdcom
https://fliphtml5.com/home/ao88gdcom
https://newspicks.com/user/12431787/
https://jump.5ch.net/?https://ao88gd.com/
https://www.tm-town.com///translators/ao88gdcom
https://biolinku.co/ao88gdcom
https://linkmix.co/54032816
https://land-book.com/ao88gdcom
https://jali.me/ao88gdcom
https://www.interesting-dir.com/details.php?id=443655
https://www.addirectory.org/details.php?id=479850
https://kitsu.app/users/1707697
http://resurrection.bungie.org/forum/index.pl?profile=ao88gdcom
https://giphy.com/channel/ao88gdcom
https://www.awwwards.com/ao88gdcom/
https://rentry.co/qqzoqzy5
https://www.demilked.com/author/ao88gdcom/
https://depechemode.cz/?URL=https://ao88gd.com/
https://www.buckeyescoop.com/users/202f9ff1-02d4-459f-bb21-f003a69aaba1
https://jp.pinterest.com/ao88gdcom/
https://de.gta5-mods.com/users/ao88gdcom
https://mk.gta5-mods.com/users/ao88gdcom
https://tr.gta5-mods.com/users/ao88gdcom
https://bs.gravatar.com/ao88gdcom
https://www.pozible.com/profile/ao88gdcom
https://dialogluzern.ch/profiles/ao88gdcom/activity
https://game8.jp/users/489955
https://www.ecodir.net/ao88gdcom_339410.html
https://www.ask-dir.org/ao88gdcom_385011.html
https://tempel.in/view/7O7nsaF
https://quicknote.io/f4e53990-4541-11f1-b470-6fe4fcc93a56/
https://www.maanation.com/ao88gdcom
http://mura.hitobashira.org/index.php?ao88gdcom
https://peatix.com/user/29511125/view
https://padlet.com/ao88gdcom/ao88gdcom-6eevro2ehhvxftyb
https://www.elephantjournal.com/profile/ao88gdcom/
https://decidim.santcugat.cat/profiles/ao88gdcom/activity
https://mangahelpers.com/forum/members/ao88gdcom.261173/#about
https://www.akiba-online.com/members/ao88gdcom.1355400/#about
https://www.pickupforum.de/profile/248012-ao88gdcom/?tab=activity
http://linoit.com/users/ao88gdcom/canvases/ao88gdcom
https://nortabs.net/user/15201/
https://www.pickupforum.ru/index.php?showuser=6612018
https://dojour.us/u/ao88gdcom
https://www.myconcertarchive.com/en/user_home?id=130780
https://all4.vip/p/page/view-persons-profile?id=123733
https://ferrariformula1.hu/community/profile/ao88gdcom
https://strikefans.com/forum/users/ao88gdcom
https://swat-portal.com/forum/wcf/user/49527-ao88gdcom/#about
https://giloo.ist/member/ao88gdcom
https://defence.pk/members/ao88gdcom.240313/#about
https://forum.jatekok.hu/User-ao88gdcom
https://www.buymusic.club/user/ao88gdcom
https://wiki.armello.com/index.php/User:Ao88gdcom
https://histre.com/notes/andersonfreeman547/and3qm8i/?accesscode=7z7kdzVKMitr_ykO
https://forum.freero.org/space-uid-24936.html
https://oraclenana.com/MYBB3/user-42628.html
https://www.notariosyregistradores.com/web/forums/usuario/ao88gdcom/
https://experiment.com/users/aao88gdcom
https://www.facer.io/u/ao88gdcom
http://genina.com/user/editDone/5338854.page
https://wikifab.org/wiki/Utilisateur:Ao88gdcom
https://www.dailymotion.com/ao88gdcom
https://mysportsgo.com/profile/140500
https://www.sqlservercentral.com/forums/user/ao88gdcom
https://forum-foxess.pro/community/profile/ao88gdcom/
https://socialsocial.social/user/ao88gdcom/
https://huggingface.co/ao88gdcom
https://es.stylevore.com/user/ao88gdcom
https://rant.li/ao88gdcom/ao88gdcom
https://chanylib.ru/ru/forum/user/26307/
https://www.cbmstuff.com/forum/member.php?action=profile&uid=11820
https://producerbox.com/users/ao88gdcom
https://skrolli.fi/keskustelu/users/andersonfreeman547/
https://forum.vgatemall.com/member.php?action=profile&uid=514489
https://www.thehockeypaper.co.uk/articles/author/ao88gdcom
https://www.rankone.global/ao88gdcom
https://www.forum-joyingauto.com/member.php?action=profile&uid=118058
https://www.11plus.co.uk/users/ao88gdcom/
https://opaseke.com/users/15400
https://app.getfarmish.com/profile/ao88gdcom
https://www.freebeg.com/forum/member.php?action=profile&uid=135943
https://artconomy.com/profile/ao88gdcom/about/
https://nl.gravatar.com/ao88gdcom
https://nb.gravatar.com/ao88gdcom
https://ms.gravatar.com/ao88gdcom
https://lt.gravatar.com/ao88gdcom
https://kn.gravatar.com/ao88gdcom
https://nicheless.blog/post/ao88gdcom
https://www.newgenstravel.com/forum/topic/44402/ao88gdcom
https://zbrushcentral.jp/user/ao88gdcom
http://julia4tied.de/member.php?action=profile&uid=247143
https://gspanel.net/member.php?action=profile&uid=17437
https://forum.rexygen.com/user/ao88gdcom
https://www.yourquote.in/nha-ci-ao88-d3k3l/quotes
https://codeberg.org/ao88gdcom
https://www.mapleprimes.com/users/ao88gdcom
https://www.plurk.com/ao88gdcom
https://www.anobii.com/fr/0192d629e2a083724a/profile/activity
https://uno-en-ligne.com/profile.php?user=424107
https://c8ke.me/ao88gdcom
https://www.rossoneriblog.com/author/ao88gdcom/
https://hieuvetraitim.vn/members/ao88gdcom.127266/
https://www.discogs.com/fr/user/ao88gdcom
https://forum.giantbomb.com/user/ao88gdcom
https://vc.ru/id5928487
https://www.postman.com/ao88gdcom
https://www.penmai.com/community/members/56winbid.482415/#about
https://www.flyingsolo.com.au/members/ao88gdcom/
https://muabanhaiduong.com/members/ao88gdcom.88080/#about
https://noti.st/ao88gdcom
https://www.adpost.com/u/ao88gdcom/
https://guitarmaking.co.uk/members/ao88gdcom/
https://play-uno.com/profile.php?user=424107
https://ao88gdcom.shopinfo.jp/posts/58783713
https://definedictionarymeaning.com/user/ao88gdcom
https://fairebruxellessamen.be/profiles/ao88gdcom/activity
https://pastelink.net/5javnj65
https://archive.org/details/@ao88gdcom/collections
https://ao88gdcom.stck.me/profile
https://www.notion.so/AO88-352d144f17e18006968ecf3f0f22ee1a
https://cannabis.net/user/227824
https://videos.muvizu.com/Profile/ao88gdcom/Latest
https://dev.muvizu.com/Profile/ao88gdcom/Latest
https://cdn.muvizu.com/Profile/ao88gdcom/Latest
https://www.muvizu.com/Profile/ao88gdcom/Latest
https://sketchersunited.org/users/320148
http://disq.us/p/35mets9
https://jobs.lajobsportal.org/profiles/8214261-nha-cai-ao88
https://urlz.fr/v8fz
https://x.com/ao88gdcom
https://www.goldposter.com/members/ao88gdcom/profile/
https://scrapbox.io/ao88gdcom/AO88
https://circle-book.com/circles/57713
https://vrcmods.com/user/ao88gdcom
https://oyaschool.com/users/ao88gdcom/
https://www.fiferosdevenezuela.com/foro/member.php?action=profile&uid=12719
https://stackoverflow.com/users/32680184/ao88gdcom?tab=profile
https://comicvine.gamespot.com/profile/ao88gdcom/
https://forum.opnsense.org/index.php?action=profile;u=67862
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=228764&tab=field_core_pfield_13
https://www.mshowto.org/forum/members/ao88gdcom.html
https://www.ekademia.pl/@ao88gdcom
https://youbiz.com/profile/ao88gdcom/
https://ao88gdcom.mystrikingly.com//
https://ja.cofacts.tw/user/ao88gdcom
https://pslk.net/5javnj65
https://pste.link/5javnj65
https://ofuse.me/ao88gdcom
https://walling.app/Wr6Dqjm5hsnzThIZpj8X/ao88gdcom
https://in.enrollbusiness.com/BusinessProfile/7792181/ao88gdcom
https://ao88gdcomm.blogspot.com/2026/05/ao88gdcom.html
https://sites.google.com/view/ao88gdcom1/home
Kami dapat memiliki tautan pertukaran kontrak antara kita!
I just could not depart your web site before suggesting that I extremely enjoyed the standard information a person provide for your visitors? Is going to be back often in order to check up on new posts
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Postingan yang hebat! Saya sangat menghargai cara Anda menjelaskan segala sesuatu dengan jelas. Teruskan kerja yang bagus!
Whoa! This blog looks just like my old one! It’s on a entirely different topic but it has pretty much the same page layout
and design. Great choice of colors!
whoah this weblog is fantastic i love reading your posts.
Stay up the great work! You realize, lots of persons are searching round for this information, you can help them greatly.
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang hebat!
Terima kasih untuk posting megah lainnya. Di tempat mana lagi seseorang bisa mendapatkan tipe info seperti itu dengan gaya penulisan yang sempurna? Saya memiliki presentasi minggu depan, dan saya sedang dalam pencarian informasi seperti ini.
Informasi yang sangat berguna. Saya baru saja menelusuri hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Your comment is awaiting moderation.
https://www.youtube.com/@33win68comco
https://x.com/33win68comco
https://wakelet.com/@33win68comco
https://safechat.com/u/33win68comco
https://gravatar.com/33win68comco
https://www.pinterest.com/33win68comco/
https://demo.wowonder.com/33win68comco
https://shareyoursocial.com/33win68comco
https://500px.com/p/33win68comco
https://www.instapaper.com/p/33win68comco
https://www.band.us/band/102569910/post
https://protocol.ooo/ja/users/33win68comco
https://www.reddit.com/user/No_Weird_2833/
https://audiomack.com/33win68comco
https://hackaday.io/33win68comco
https://fyers.in/community/member/6VCc2TYZav
https://vocal.media/authors/33win68comco
https://leetcode.com/u/33win68comco/
https://swag.live/en/user/69f81f5387a3f029bd913482
https://www.halaltrip.com/user/profile/345364/33win68comco/
https://medibang.com/author/28234016/
https://www.blockdit.com/33win68comco
https://portfolium.com/nhci33win81
https://www.twitch.tv/33win68comco/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:AD7781EE69F8246A0A495CDD@AdobeID
https://profile.hatena.ne.jp/ba3win68comco/profile
https://issuu.com/33win68comco
https://www.behance.net/nhci33win80
https://www.reverbnation.com/33win68comco
https://www.myminifactory.com/users/33win68comco
https://www.investagrams.com/Profile/33win68comco
https://gifyu.com/33win68comco
https://www.chordie.com/forum/profile.php?id=2521993
https://www.walkscore.com/people/131815557766/33win68comco
https://topsitenet.com/profile/33win68comco/1716964/
https://akniga.org/profile/1420424-33win68comco/
https://disqus.com/by/33win68comco/about/
https://jobs.suncommunitynews.com/profiles/8227391-nha-cai-33win
https://www.speedrun.com/users/33win68comco
https://www.fanart-central.net/user/33win68comco/profile
https://www.aicrowd.com/participants/33win68comco
https://www.bitchute.com/channel/qyfkOubAREzn
https://pbase.com/33win68comco
https://hub.docker.com/u/33win68comco
https://spiderum.com/nguoi-dung/33win68comco
https://www.gta5-mods.com/users/33win68comco
https://pixabay.com/users/33win68comco-55707305/
https://www.nicovideo.jp/user/144129707
https://3dwarehouse.sketchup.com/by/33win68comco
https://robertsspaceindustries.com/en/citizens/33win68comco
https://bit.ly/m/33win68comco
https://allmylinks.com/33win68comco
https://www.tumblr.com/33win68comco
https://scholar.google.com/citations?hl=en&user=Ss4e2fkAAAAJ
https://sites.google.com/view/33win68comco/trang-ch%E1%BB%A7
https://www.slideshare.net/daobaotoan70?tab=about
https://www.scribd.com/user/979572937/33win68comco
https://soundcloud.com/33win68comco
https://hashnode.com/@33win68comco
https://web.bikemap.net/u/daobaotoan70
https://easymeals.qodeinteractive.com/forums/users/33win68comco/
https://bookmeter.com/users/1717049
https://bbs.theviko.com/home.php?mod=space&uid=4666078
https://www.xiuwushidai.com/home.php?mod=space&uid=2686473
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6461691
https://www.mynbest.info/profile/daobaotoan7063548/profile
https://matkafasi.com/user/33win68comco
https://allmyfaves.com/33win68comco
https://www.notebook.ai/@33win68comco
https://www.abclinuxu.cz/lide/33win68comco
https://teletype.in/@33win68comco
https://www.checkli.com/33win68comco#/a/process
https://www.nintendo-master.com/profil/33win68comco
https://freeimage.host/33win68comco
https://motion-gallery.net/users/976422
https://linkin.bio/33win68comco/
https://www.chichi-pui.com/users/33win68comco/
https://www.openrec.tv/user/33win68comco/about
https://unityroom.com/users/2b9aitse47p0z8goqvmr
https://forum.dmec.vn/index.php?members/33win68comco.190346/
https://igli.me/33win68comco
https://www.miseducationofmotherhood.com/profile/daobaotoan7077456/profile
https://www.housedumonde.com/profile/daobaotoan7021179/profile
https://pad.geolab.space/s/aAmnxYlVE
https://pad.stuve.de/s/33ZagxwwmA
https://www.sythe.org/members/33win68comco.2045443/#info
https://f319.com/members/33win68comco.1103791/
https://www.itchyforum.com/en/member.php?389818-33win68comco
https://www.roton.com/forums/users/daobaotoan70/
https://able2know.org/topic/596083-1
http://www.biblesupport.com/user/836196-33win68comco/
https://golosknig.com/profile/33win68comco/
https://blender.community/nha_cai276/
https://doselect.com/@7e43b52cd7f1021f9637deeec
https://maps.arosalenzerheide.swiss/en/member/nha-cai-33win/340423807/
https://bandori.party/user/884538/33win68comco/
https://schoolido.lu/user/33win68comco/
https://awan.pro/forum/user/169996/
https://fortunetelleroracle.com/profile/33win68comco
https://fabble.cc/33win68comco
https://www.theyeshivaworld.com/coffeeroom/users/33win68comco
http://delphi.larsbo.org/user/33win68comco
https://www.aseeralkotb.com/en/profiles/33win68comco
https://timdaily.vn/members/33win68comco.135414/#about
https://app.readthedocs.org/profiles/33win68comco/
https://www.dibiz.com/daobaotoan70
https://about.me/wincomco1
https://www.canadavisa.com/canada-immigration-discussion-board/members/33win68comco.1355626/#about
https://www.equinenow.com/farm/33win68comco.htm
https://www.gaiaonline.com/profiles/33win68comco/50669841/
https://wefunder.com/33win68comco/about
https://potofu.me/33win68comco
https://transfur.com/Users/win68comco
https://xtremepape.rs/members/33win68comco.670493/#about
https://gachmienbac.com/members/12922-33win68c.html
https://qna.habr.com/user/33win68comco
https://website.informer.com/33win68.com.co
https://velog.io/@33win68comco/about
https://en.islcollective.com/portfolio/12913978
https://www.xosothantai.com/members/33win68comco.611740/
https://velog.io/@33win68comco/about
https://violet.vn/user/show/id/15272409
https://xaydunghanoimoi.net/members/27953-33win68c.html
https://iplogger.com/2eXbk6
https://mez.ink/33win68comco
https://33win68comco.stck.me/profile
https://notionpress.com/author/1515787
https://www.edna.cz/uzivatele/33win68comco/
https://digiphoto.techbang.com/users/33win68comco
https://leakedmodels.com/forum/members/33win68comco.712091/#about
https://maychetao.com/members/21304-33win68c.html
https://onlinesequencer.net/members/271589
https://inkbunny.net/33win68comco
https://www.japaaan.com/user/78749
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.33win13
https://beatsaver.com/playlists/1194333
https://apptuts.bio/33win68comco-262681
https://www.storenvy.com/N33win68comco
https://participacion.cabildofuer.es/profiles/33win68comco/activity
https://forums.maxperformanceinc.com/forums/member.php?u=248173
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=303474
https://acomics.ru/-33win68comco
https://www.criminalelement.com/members/33win68comco/profile/
https://hanson.net/users/33win68comco
https://diendan.cuabenhvien.com/members/19867-33win68c.html
https://writexo.com/share/8157ff8c802f
https://expatguidekorea.com/profile/33win68comco/
https://www.heavyironjobs.com/profiles/8227535-nha-cai-33win
https://pad.degrowth.net/s/ZvgYFh1f9
http://fort-raevskiy.ru/community/profile/33win68comco/
https://forum.skullgirlsmobile.com/members/33win68comco.220003/#about
https://jobs.landscapeindustrycareers.org/profiles/8227592-nha-cai-33win
https://phatwalletforums.com/user/33win68comco
https://song.link/33win68comco
https://idol.st/user/170604/33win68comco/
https://www.bmwpower.lv/user.php?u=33win68comco
https://gockhuat.net/member.php?u=438000
https://jobs.windomnews.com/profiles/8227741-nha-cai-33win
https://hoaxbuster.com/redacteur/33win68comco
https://www.givey.com/33win68comco
https://zerosuicidetraining.edc.org/user/profile.php?id=564542
https://www.hobowars.com/game/linker.php?url=https://33win68.com.co/
https://jobs.westerncity.com/profiles/8227779-nha-cai-33win
https://www.thetriumphforum.com/members/33win68comco.64508/
https://album.link/33win68comco
https://dev.muvizu.com/Profile/33win68comco/Latest
https://chaloke.com/forums/users/33win68comco/
https://www.buckeyescoop.com/users/1d024c1f-7ddc-4f83-9659-ff3897d8e896
https://toirscript.com/user/33win68comco
https://forum.pabbly.com/members/33win68comco.116043/#about
http://forum.cncprovn.com/members/426246-33win68comco
https://forum.aigato.vn/user/33win68comco
https://rapidapi.com/user/33win68comco
https://www.skool.com/@nha-cai-babawin-7028
https://learningapps.org/watch?v=p8ejtnn6j26
https://www.invelos.com/UserProfile.aspx?alias=33win68comco
https://www.video-bookmark.com/bookmark/7121117/33win/
https://krachelart.com/UserProfile/tabid/43/userId/1344575/Default.aspx
https://gitlab.vuhdo.io/33win68comco
https://kktix.com/user/8775274
https://poipiku.com/13551492/
https://www.fitday.com/fitness/forums/members/33win68comco.html
https://www.grepmed.com/33win68comco
https://classificados.acheiusa.com/profile/OTAwZFFVelhjWXBIYkdKNXNwa2V4YVdTaWtpck9WR3Q5N0Y5TG1EcDNCZz0=
https://espritgames.com/members/51001357/
https://cgmood.com/nha-cai-33win-1852620855
https://secondstreet.ru/profile/33win68comco/
https://scenarch.com/userpages/35066
https://undrtone.com/33win68comco
https://marshallyin.com/members/33win68comco/
https://www.atozed.com/forums/user-79409.html
https://gravesales.com/author/33win68comco/
https://hukukevi.net/user/33win68comco
https://belgaumonline.com/profile/33win68comco/
https://savelist.co/my-lists/users/33win68comco
https://zzb.bz/frAHUi
https://www.themeqx.com/forums/users/33win68comco/
https://www.udrpsearch.com/user/33win68comco
https://www.xen-factory.com/index.php?members/33win68comco.157996/#about
https://forums.servethehome.com/index.php?members/33win68comco.242089/
https://b.io/33win68comco
https://www.blackhatprotools.info/member.php?289550-33win68comco
https://activepages.com.au/profile/33win68comco
https://snippet.host/hejwdk
https://tudomuaban.com/chi-tiet-rao-vat/2894786/33win68comco.html
https://phijkchu.com/a/33win68comco/video-channels
https://lifeinsys.com/user/33win68comco
https://kaeuchi.jp/forums/users/33win68comco/
https://www.claimajob.com/profiles/8227251-nha-cai-33win
https://protospielsouth.com/user/132659
https://theafricavoice.com/profile/33win68comco
https://support.bitspower.com/support/user/33win68comco
https://support.bitspower.com/support/user/33win68comco
https://www.brownbook.net/business/54947259/ketquanet30com
https://app.hellothematic.com/artist/profile/1148297
https://hackmd.okfn.de/s/r1_e8aSRZl
https://manylink.co/@33win68comco
https://beteiligung.hafencity.com/profile/33win68comco/
https://anyflip.com/homepage/zhgaa
https://www.akaqa.com/question/q19192677025-Nh-ci-33win
https://copynotes.be/shift4me/forum/user-54032.html
https://www.threadless.com/@33win68comco/activity
https://civitai.com/user/33win68comco
https://www.spigotmc.org/members/33win68comco.2530115/
https://hoo.be/33win68comco
https://maxforlive.com/profile/user/33win68comco?tab=about
https://3dtoday.ru/blogs/33win68comco
https://mathlog.info/users/EOgQM6UYEZgUVtrRVdltov1INW92
https://allmylinks.com/33win68comco
https://community.cloudera.com/t5/user/viewprofilepage/user-id/152380
https://www.shippingexplorer.net/en/user/33win68comco/283994
https://shhhnewcastleswingers.club/forums/users/33win68comco/
https://connect.gt/user/33win68comco/
https://www.weddingbee.com/members/33win68comco/
https://www.trackyserver.com/profile/249484
https://www.zubersoft.com/mobilesheets/forum/user-137377.html
https://www.mindomo.com/mindmap/aa029ea743a94438a905b85d5dd089e6
https://md.coredump.ch/s/zJlTR5J2z
https://aprenderfotografia.online/usuarios/33win68comco/profile/
https://hackmd.hub.yt/s/Rvl9HGqOt
https://sciencemission.com/profile/33win68comco
https://www.wvhired.com/profiles/8227183-33win-nha-cai
https://beteiligung.tengen.de/profile/33win68comco/
https://chyoa.com/user/33win68comco
https://www.royalroad.com/profile/966789
https://backloggd.com/u/33win68comco/
https://forums.alliedmods.net/member.php?u=478001
https://community.jmp.com/t5/user/viewprofilepage/user-id/98567
https://viblo.asia/u/33win68comco
https://hype4.academy/profile/33win68comco
https://brain-market.com/u/33win68comco
https://www.prosebox.net/box/80559/
https://www.fw-follow.com/forum/topic/122539/33win68comco
https://www.jk-green.com/forum/topic/115073/33win68comco
https://www.navacool.com/forum/topic/412483/33win68comco
https://www.driedsquidathome.com/forum/topic/148962/33win68comco
https://www.nongkhaempolice.com/forum/topic/131510/33win68comco
https://www.bestloveweddingstudio.com/forum/topic/86730/33win68comco
https://www.natthadon-sanengineering.com/forum/topic/109026/33win68comco
https://www.rueanmaihom.net/forum/topic/102239/33win68comco
https://www.ttlxshipping.com/forum/topic/412488/33win68comco
http://worldchampmambo.com/UserProfile/tabid/42/userId/489658/Default.aspx
http://forum.modulebazaar.com/forums/user/33win68comco/
https://www.rcmx.net/userinfo.php?uid=17428
https://eilo.org/user/33win68comco
https://forum.web-z.net/profile.php?userid=10033
https://lqdoj.edu.vn/user/33win68comco
https://indiestorygeek.com/user/33win68comco
https://forum.issabel.org/u/33win68comco
https://www.easyhits4u.com/profile.cgi?login=33win68comco
https://doc.anagora.org/s/-I87gaQtL
https://profile.sampo.ru/n33win68comco
https://www.ekdarun.com/forum/topic/158614/33win68comco
https://fanclove.jp/profile/ePBn4LboJ4
https://www.d-ushop.com/forum/topic/137127/33win68comco
https://lustyweb.live/members/33win68comco.125560/#about
https://findaspring.org/members/33win68comco/
https://ketcau.com/member/129062-33win68comco
https://fengshuidirectory.com/dashboard/listings/33win68comco/
https://library.zortrax.com/members/33win68comco/
https://pets4friends.com/profile-1586315
https://participa.aytojaen.es/profiles/33win68comco/activity
https://linkmix.co/54125316
https://www.maanation.com/33win68comco
https://janitorai.com/profiles/60c687a9-ec64-47df-9dc4-71a7043ec3a8_profile-of-33-win-68-comco
https://muckrack.com/33win68comco/bio
http://linoit.com/users/33win68comco/canvases/33win68comco
https://nortabs.net/user/15305/
https://www.myconcertarchive.com/en/user_home?id=130952
https://giloo.ist/member/33win68comco
https://defence.pk/members/33win68comco.240681/#about
https://www.buymusic.club/user/33win68comco
https://forum.freero.org/space-uid-25014.html
http://genina.com/user/editDone/5343865.page
https://wikifab.org/wiki/Utilisateur:33win68comco
https://pad.lescommuns.org/s/_-qZyCsJT
https://rant.li/33win68comco/33win68comco
https://chanylib.ru/ru/forum/user/26730/
https://skrolli.fi/keskustelu/users/daobaotoan70/
https://www.thehockeypaper.co.uk/forums/users/33win68comco
https://www.11plus.co.uk/users/daobaotoan70/
https://git.entryrise.com/33win68comco
https://app.getfarmish.com/profile/33win68comco
https://imaginaria.ru/profile/33win68comco/
https://nicheless.blog/author/33win68comco
https://www.newgenstravel.com/forum/topic/45276/33win68comco
https://zbrushcentral.jp/user/33win68comco
https://forum.rexygen.com/user/33win68comco
https://www.mapleprimes.com/users/33win68comco
https://noti.st/n33win68comco
https://www.adpost.com/u/33win68comco/
https://scrapbox.io/33win68comco/33win68comco
https://qiita.com/33win68comco
https://www.annuncigratuititalia.it/author/33win68comco/
https://lite.link/33win68comco
http://www.brenkoweb.com/user/90059/profile
https://hedgedoc.faimaison.net/s/mt14jRrh51
https://www.rossoneriblog.com/author/33win68comco/
https://www.scamadviser.com/check-website/33win68.com.co
https://adplist.org/members/33win68comco-moqugc91
https://novel.daysneo.com/author/33win68comco/
https://destaquebrasil.com/saopaulo/author/33win68comco/
http://adsfare.com/33win68comco
https://makerworld.com/en/@33win68comco
https://bhmtsff.com/space-uid-97616.html
https://congdongmassage.com/members/33win68comco.149542/#about
https://www.tacter.com/@33win68comco
https://www.vrcarena.com/users/f1d81ec2-4f8e-440a-84b4-caac5b898e17
https://artist.link/33win68comco
https://dreevoo.com/profile_info.php?pid=1596208
https://www.passes.com/33win68comco
https://backloggery.com/33win68comco
http://palangshim.com/space-uid-5140063.html
https://etextpad.com/1l0n4q7hoe
https://m.wibki.com/33win68comco
https://pinshape.com/users/8961471-33win68comco?tab=designs
https://sfx.thelazy.net/users/u/33win68comco/
https://www.skypixel.com/users/djiuser-yt4bc8oefs6t
https://33win68comco.notepin.co/
https://pictureinbottle.com/r/33win68comco
https://forum.epicbrowser.com/profile.php?id=154490
https://electroswingthing.com/profile/33win68comco/
https://stuv.othr.de/pad/s/qwKOLFXDm
https://hedgedoc.eclair.ec-lyon.fr/s/zBG9Yx2Kf
https://www.socialbookmarkssite.com/user/33win68comco/
https://www.hogwartsishere.com/1838874/
https://makeagif.com/user/33win68comco?ref=l6TidG
https://www.plotterusati.it/user/33win68comco
https://linqto.me/about/33win68comco
https://www.managementpedia.com/members/33win68comco.1121403/#about
https://partecipa.poliste.com/profiles/33win68comco/activity
https://hedgedoc.stusta.de/s/1gTVGqiLP
https://pad.codefor.fr/s/kvodngTzMr
https://pad.fablab-siegen.de/s/7F0mXAcv7u
https://md.swk-web.com/s/9aDAWZGBc
https://hedgedoc.dezentrale.space/s/RE4eKysnn
https://pad.darmstadt.social/s/ZeXcDY_xtm
https://referrallist.com/profile/33win68comco/
https://md.chaosdorf.de/s/q4v-92O1UX
https://smallseo.tools/website-checker/33win68.com.co
https://telegra.ph/33win-05-04-3
https://runtrip.jp/users/778920
https://www.bonback.com/forum/topic/412698/33win68comco
https://www.pathumratjotun.com/forum/topic/182287/33win68comco
https://www.iglinks.io/33win68comco-kic
https://homepage.ninja/33win68comco
https://www.noteflight.com/profile/69baa481d89b962bc0fc3f20c5e91e980e2652b4
https://www.gabitos.com/catalunyauniversal/template.php?nm=1777882259
https://www.foriio.com/33win68comco
https://controlc.com/1hgk87mu
https://justpaste.it/u/33win68comco
https://www.pozible.com/profile/33win68comco
https://www.elephantjournal.com/profile/33win68comco/
https://swat-portal.com/forum/wcf/user/49953-33win68comco/#about
https://stocktwits.com/33win68comco
https://mercadodinamico.com.br/author/33win68comco/
https://www.grabcaruber.com/members/33win68comco/profile/
https://www.magcloud.com/user/33win68comco
https://bioqoo.com/33win68comco
https://app.brancher.ai/user/lJGyDS9_LAYY
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345983
https://www.giveawayoftheday.com/forums/profile/1840573
https://uiverse.io/profile/nhci_8031
https://cofacts.tw/user/33win68comco
https://www.efunda.com/members/people/show_people.cfm?Usr=33win68comco
https://usdinstitute.com/forums/users/33win68comco/
https://sistacafe.com/user/616120
https://www.intensedebate.com/people/33win68comco1
https://tabelog.com/rvwr/33win68comco/prof/
https://app.parler.com/33win68comco
https://svetelektro.com/clenovia/33win68comco/
https://www.diigo.com/profile/n33win68comco
https://marshmallow-qa.com/2izjeu4emko06zu
https://us.enrollbusiness.com/BusinessProfile/7795495/33win68comco
https://link4u.cc/@33win68comco
https://www.iniuria.us/forum/member.php?678766-33win68comco
https://cointr.ee/33win68comco
https://indian-tv.cz/u/33win68comco
https://illust.daysneo.com/illustrator/33win68comco/
https://www.ironlifting.it/forum/member.php?u=430281
https://www.hentai-foundry.com/user/33win68comco/profile
https://www.mateball.com/k33win68comco
https://ofuse.me/e/365773
https://photouploads.com/33win68comco
https://advego.com/profile/33win68comco/
https://form.jotform.com/261232420859051
https://www.sunemall.com/board/board_topic/8431232/8257318.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8257324.htm
https://rmmedia.ru/members/184149/#about
https://calgarybusinesses.ca/dashboard/reviews/33win68comco/
https://www.notariosyregistradores.com/web/forums/usuario/33win68comco/
https://luvly.co/users/33win68comco
https://spinninrecords.com/profile/33win68comco
http://onlineboxing.net/jforum/user/profile/453632.page
https://www.aipictors.com/en/users/f5c9d701-de5d-7dac-3510-ae9f9963295d
https://campsite.bio/33win68comco
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8255991.htm
https://www.tai-ji.net/board/board_topic/4160148/8255988.htm
https://www.vhs80.com/board/board_topic/6798823/8255987.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8255985.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8255983.htm
https://kheotay.com.vn/forums/users/daobaotoan70
https://sklad-slabov.ru/forum/user/44697/
https://crazyservice.by/forum/user/15664/
https://rsfpost.com/forums/users/33win68comco/
https://exceldemy.com/forum/members/33win68comco.5058/
https://www.ontime.co.th/forum/topic/809355/33win68comco
https://forum.gettinglost.ca/user/33win68comco
https://zepodcast.com/forums/users/33win68comco/
https://md.rappet.xyz/s/d7evYKp4tI
https://md.sebastians.dev/s/IWSadXdSr
https://experiment.com/users/333win68comco
http://julia4tied.de/member.php?action=profile&uid=247508
https://booklog.jp/users/33win68comco/profile
https://turcia-tours.ru/forum/profile/33win68comco/
https://www.montessorijobsuk.co.uk/author/33win68comco/
https://gitlab.com/33win68comco
https://hedgedoc.envs.net/s/GSILiKzyH
https://hub.vroid.com/en/users/125925129
https://fact-finder.xyz/pukiwiki/?33win68comco
https://naijamatta.com/33win68comco
https://graph.org/33win68comco-05-04
https://cars.yclas.com/user/33win68comco
https://shootinfo.com/ru/author/33win68comco/?pt=ads
https://www.sciencebee.com.bd/qna/user/33win68comco
https://decidim.calafell.cat/profiles/33win68comco/activity
https://mail.londonchinese.com/home.php?mod=space&uid=621727&do=profile
https://mforum3.cari.com.my/home.php?mod=space&uid=3400721&do=profile
https://qna.alpharegiment.com/profile/33win68comco/
https://www.dokkan-battle.fr/forums/users/33win68comco/
https://boss.why3s.cc/boss/home.php?mod=space&uid=264113
https://www.horticulturaljobs.com/employers/4138349-33win68comco
https://jobs.siliconflorist.com/employers/4138352-33win68comco
https://jobs.nefeshinternational.org/employers/4138354-33win68comco
https://aboutcasemanagerjobs.com/author/33win68comco/
https://biashara.co.ke/author/33win68comco/
https://strikefans.com/forum/users/33win68comco/
https://galleria.emotionflow.com/184918/profile.html
https://www.myget.org/users/33win68comco
https://mygamedb.com/profile/33win68comco
https://forum.aceinna.com/user/33win68comco
https://vcook.jp/users/90064
https://pumpyoursound.com/u/user/1618167
https://congdongx.com/thanh-vien/33win68comco.49777/#about
https://doodleordie.com/profile/3win68comco
https://tuscl.net/member/888494
https://aniworld.to/user/profil/33win68comco
https://nogu.org.uk/forum/profile/33win68comco/
https://gitflic.ru/user/33win68comco
http://themirch.com/blog/author/33win68comco/
https://www.czporadna.cz/user/33win68comco
https://commu.nosv.org/p/33win68comco
https://www.euskalmarket.com/author/33win68comco/
https://www.vnbadminton.com/members/33win68comco.77322/
https://iszene.com/user-350089.html
https://forum.delftship.net/Public/users/33win68comco/
https://scenarch.com/userpages/35066
https://pad.funkwhale.audio/s/jbM08levW
http://jobs.emiogp.com/author/33win68comco/
https://is.gd/AV0bm0
https://33win68comco.amebaownd.com/posts/58792885
https://www.zazzle.co.jp/mbr/238234755925824015
https://www.adminer.org/redirect/?lang=en&url=https://33win68.com.co/
https://pastes.io/AsidN9ZY
https://biolinku.co/33win68comco
http://simp.ly/p/Z5LcpV
https://www.slideshare.net/daobaotoan70?tab=about
https://en.asg.to/bridgePage.html?url=https://33win68.com.co/
https://nyccharterschools.jobboard.io/employers/4138379-33win68comco
https://participation.touraine.fr/profiles/33win68comco/activity
https://www.4shared.com/u/bywqCK6V/daobaotoan70.html
https://www.popdaily.com.tw/user/533609
https://git.disroot.org/33win68comco
https://nous.malakoff.fr/profiles/33win68comco/activity
https://community.bemeapps.com/user/33win68comco
https://www.scienceuniverse.org/profile/33win68comco/profile
https://www.inkitt.com/33win68comco
https://www.healthleadershipbraintrust.com/profile/33win68comco/profile
https://www.pexels.com/@nha-cai-33win-2161344979/
https://aboutpharmacistjobs.com/author/33win68comco/
https://www.dek-o-block.com/profile/33win68comco/profile
https://www.yesflowers.ie/profile/33win68comco/profile
https://www.longisland.com/profile/33win68comco
https://www.squadskates.com/profile/33win68comco/profile
https://www.leonidastacticalss.com/profile/33win68comco/profile
https://www.questmetaldetectors.com/members-area/33win68comco/profile
https://www.twilightcreationsinc.com/profile/33win68comco/profile
https://www.floodzonebrewery.com/profile/33win68comco/profile
https://www.lookingforjob.co/profile/33win68comco
https://photozou.jp/user/top/3451634
https://jii.li/WwJvX
https://dec.2chan.net/bin/jump.php?https://33win68.com.co/
https://chatclub.mn.co/members/39562498
https://www.shabeenaam.com/profile/daobaotoan7026320/profile
http://bbs.sdhuifa.com/home.php?mod=space&uid=1116763
https://www.e-auto.global/profile/33win68comco/profile
http://nao.earth/index.php?33win68comco
https://www.newdirectionchildcarefacility.com/profile/33win68comco/profile
http://xline.vc/index.php?33win68comco
https://7tdmjpf5yuwu.jobboard.io/profiles/8228328-nha-cai-33win
Very interesting topic, appreciate it for posting. “Genius is of no country.” by Charles Churchill.
Hai di sana, saya menemukan blog Anda lewat Google saat menelusuri subjek yang serupa, situs Anda tampil di bagian atas. Saya perlu mengakui bahwa saya terkejut seberapa baik pengaturannya. Saya benar-benar menyukai menelusuri ini dan saya pasti akan kembali untuk melihat konten lainnya. Terima kasih!
Excellent read, I just passed this onto a colleague who was doing some research on that. And he just bought me lunch because I found it for him smile Therefore let me rephrase that: Thanks for lunch!
Ini adalah saran yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
Hebat website yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan pendapat dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Cheers!
I believe other website proprietors should take this site as an example , very clean and fantastic user pleasant design.
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini dulunya adalah sebuah konten hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita bisa menjaga kontak?
Wohh just what I was searching for, appreciate it for putting up.
Saya gembira bahwa saya mengamati situs ini, tepat info yang saya cari!
Saya beruntung bahwa saya menyadari blog ini, benar-benar info yang saya telusuri!
I gotta bookmark this site it seems very useful extremely helpful
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri! “Menjadi kaya adalah memiliki uang, menjadi sejahtera adalah memiliki waktu.” oleh Margaret Bonnano.
Hello! Someone in my Myspace group shared this website with us so I came
to take a look. I’m definitely enjoying the information. I’m book-marking and
will be tweeting this to my followers! Great blog and brilliant design.
I am now not sure the place you are getting your information, however good topic. I needs to spend a while studying more or understanding more. Thanks for great information I used to be looking for this info for my mission.
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali evaluasi tentang ini. Dan dia sebenarnya membeli saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika potensial, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui weblog Anda dengan tambahan rincian? Ini sangat membantu bagi saya. Jempol besar untuk posting blog ini!
Saya terus-menerus menyelidiki online untuk tips yang dapat membantu saya. Thx!
Thanks a bunch for sharing this with all folks you actually recognize what you’re talking about! Bookmarked. Please additionally discuss with my site =). We will have a link change agreement among us!
Saya perlu mengatakan, ini adalah salah satu posting terbaik yang yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Sangat menarik detail yang Anda sebutkan, sangat menghargai telah mengunggah. “Apa yang benar-benar dibutuhkan dunia adalah lebih banyak cinta dan lebih sedikit dokumen.” oleh Pearl Bailey.
Sangat menarik info !Sempurna persis seperti yang saya cari!
Luar biasa blog yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan tanggapan dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
Saya bersyukur bahwa saya menemukan kembali weblog ini, tepat info yang saya telusuri!
Saya mendapatkan info yang bagus dari blog Anda.
you have a great blog here! would you like to make some invite posts on my blog?
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi luar biasa dibagikan secara bebas.
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You definitely know what youre talking about, why waste your intelligence on just posting videos to your weblog when you could be giving us something enlightening to read?
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
I’m gone to say to my little brother, that he should also go to see this web site on regular basis to
obtain updated from hottest gossip.
I’ve learn a few just right stuff here. Certainly value bookmarking for revisiting. I wonder how a lot effort you place to create this type of wonderful informative web site.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Wow! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna desain yang hebat!
Seseorang pada dasarnya menolong untuk membuat secara serius posting saya mungkin katakan. Itu adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi luar biasa ini. Kerja yang luar biasa!
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang yang pernah saya baca dalam waktu yang lama. Konten yang sangat berguna. Terima kasih telah berbagi.
I really appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again!
Very nice post. I just stumbled upon your weblog and wanted to say that I’ve really enjoyed surfing around your blog posts. After all I’ll be subscribing to your feed and I hope you write again soon!
I was reading some of your articles on this website and I conceive this site is really instructive! Retain posting.
Kami akan memiliki hyperlink alternatif perjanjian di antara kita!
For most recent information you have to pay a visit world wide web and on internet I found this site as a
finest web page for latest updates.
I have recently started a site, the information you provide on this website has helped me greatly. Thank you for all of your time & work.
Your comment is awaiting moderation.
https://www.youtube.com/@u888vipapp1
https://x.com/u888vipapp1
https://wakelet.com/@u888vipapp1
https://safechat.com/u/u8887.191
https://gravatar.com/u888vipapp1
https://www.blogger.com/profile/09135520076440640988
https://www.mymeetbook.com/u888vipapp1
https://www.pinterest.com/u888vipapp1/
https://demo.wowonder.com/u888vipapp1/
https://shareyoursocial.com/u888vipapp1
https://500px.com/p/u888vipapp1
https://www.instapaper.com/p/u888vipapp1
https://band.us/@u888vipapp1
https://protocol.ooo/ja/users/u888vipapp1
https://www.reddit.com/user/u888vipapp1/
https://audiomack.com/u888vipapp1
https://hackaday.io/u888vipapp1
https://fyers.in/community/member/VFw5IsT6JV
https://vocal.media/authors/u888-drbad0xcy
https://swag.live/en/user/69f03adb602875dd470d0cf6
https://www.halaltrip.com/user/profile/343239/u888vipapp1/
https://forums.jetphotos.com/member/55633-u888vipapp1/about
https://www.blockdit.com/u888vipapp1
https://portfolium.com/u888vipapp1
https://www.twitch.tv/u888vipapp1/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:C166810769F03ECB0A495EE1@AdobeID
https://profile.hatena.ne.jp/u888vipapp1/
https://issuu.com/u888vipapp1
https://www.behance.net/nhacaiu8887
https://www.reverbnation.com/artist/u888vipapp1
https://www.myminifactory.com/users/u888vipapp1
https://www.investagrams.com/Profile/u888vipapp2
https://gifyu.com/u888vipapp1
https://www.chordie.com/forum/profile.php?id=2517189
https://www.walkscore.com/people/115298768366/u888vipapp1
https://akniga.org/profile/1418425-u888vipapp1/
https://disqus.com/by/u888vipapp1/about/
https://jobs.suncommunitynews.com/profiles/8206252-nha-cai-u888
https://www.speedrun.com/users/u888vipapp1
https://www.fanart-central.net/user/u888vipapp1/profile
https://www.aicrowd.com/participants/u888vipapp1
https://www.bitchute.com/channel/ZyvdUAJLuUoF
https://pbase.com/u888vipapp1/image/176262291
https://hub.docker.com/u/u888vipapp1
https://spiderum.com/nguoi-dung/u888vipapp2
https://www.nicovideo.jp/user/144067770
https://www.jigsawplanet.com/u888vipapp1
https://3dwarehouse.sketchup.com/by/u888vipapp1
https://robertsspaceindustries.com/en/citizens/u888vipapp1
https://bit.ly/m/u888vipapp1
https://allmylinks.com/u888vipapp1
https://sites.google.com/view/u888vipapp2/
https://u888vipapp1.blogspot.com/2026/04/u888.html
https://www.slideshare.net/kiemhohoan5?tab=about
https://web.bikemap.net/u/u888vipapp1
https://lamsn.com/home.php?mod=space&uid=1993978
http://www.activewin.com/user.asp?Action=Read&UserIndex=4839212
https://bbs.theviko.com/home.php?mod=space&uid=4644555
https://www.xiuwushidai.com/home.php?mod=space&uid=2680366
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6433252
https://forum.dboglobal.to/wsc/index.php?user/149032-u888vipapp1/#about
https://easymeals.qodeinteractive.com/forums/users/u888vipapp1/
https://bookmeter.com/users/1714405
https://party.biz/index.php/profile/382289
https://rb.gy/5naxtz
https://files.fm/u888vipapp1/info
https://www.mynbest.info/profile/u888vipapp1/profile
https://jasa-seo.mn.co/members/39476259
https://creativemarket.com/users/u888vipapp1
https://www.zazzle.pt/mbr/238121030642330441
https://www.africangenesis-101.org/profile/u888vipapp1/profile
https://www.proko.com/@u888vipapp1/activity
https://sitereport.netcraft.com/?url=https://u888vip.app
https://www.miseducationofmotherhood.com/profile/u888vipapp1/profile
https://www.housedumonde.com/profile/u888vipapp1/profile
https://www.macdermottmethod.com/members-area/u888vipapp1/profile
https://t.ly/OyrGt
https://m.xtutti.com/user/profile/488861
https://jobs.dfw501c.com/profiles/8206694-nha-cai-u888
https://architecture-jobs.architizer.com/profiles/8206697-nha-cai-u888
https://www.webmastersun.com/members/u888vipapp1.164059/#about
https://drivehud.com/forums/users/kiemhohoan5/
https://u888vipapp1.stck.me/
https://joy.link/u888vipapp2
https://joy.gallery/u888vipapp2
https://joy.bio/u888vipapp2
https://connect.garmin.com/app/profile/2fa98805-aa85-4ad7-a4fd-c77574d84e88
https://b.hatena.ne.jp/u888vipapp1/bookmark
https://www.chichi-pui.com/users/u888vipapp1/
https://www.openrec.tv/user/u888vipapp1/about
https://unityroom.com/users/euyv2cr10d4fx3gq5m7h
https://routinehub.co/user/u888vipapp1
https://pxhere.com/en/photographer/4996586
https://teletype.in/@u888vipapp1
https://www.checkli.com/u888vipapp1/
https://www.nintendo-master.com/profil/u888vipapp1
https://freeimage.host/u888vipapp1
https://motion-gallery.net/users/964671
https://linkin.bio/u888vipapp1/
https://talk.plesk.com/members/uvipapp.504068/#about
https://www.callupcontact.com/b/businessprofile/U888/10068402
https://www.growkudos.com/profile/nha_cai__u888_4
https://blender.community/u888153/
https://doselect.com/@b902734713cee389b0bdabe26
https://sciter.com/forums/users/u888vipapp1/
https://matkafasi.com/user/u888vipapp1
https://allmyfaves.com/u888vipapp1/
https://www.notebook.ai/users/1347809
https://heylink.me/u888vipapp1/
https://muare.vn/shop/u888vipapp1/903408
https://lookingforclan.com/user/u888vipapp1
https://forum.dmec.vn/index.php?members/u888vipapp1.189430/
https://igli.me/u888vipapp1
http://delphi.larsbo.org/user/u888vipapp1
https://www.aseeralkotb.com/en/profiles/u888vipapp1
https://timdaily.vn/members/uv_ipap1sa.135002/#about
https://app.readthedocs.org/profiles/u888vipapp1/
https://www.dibiz.com/kiemhohoan5
https://iszene.com/user-349179.html
https://desksnear.me/users/u888-b06096
https://www.itchyforum.com/en/member.php?389261-u888vipapp1
https://www.roton.com/forums/users/kiemhohoan5/
https://able2know.org/user/u888vipapp1/
http://www.biblesupport.com/user/834472-u888vipapp1/
https://golosknig.com/profile/u888vipapp1/
https://wallhaven.cc/user/u888vipapp1
https://bandori.party/user/844995/u888vipapp1/
https://schoolido.lu/user/u888vipapp1/
https://awan.pro/forum/user/168303/
https://fortunetelleroracle.com/profile/u888vipapp1
https://fabble.cc/u888vipapp1
https://pad.geolab.space/s/T2A5VZ1uM
https://pad.stuve.de/s/AWXGFrYGL
https://www.sythe.org/members/u888vipapp1.2043437/
https://f319.com/members/u888vipapp1.1101625/
https://about.me/u888vipapp1
https://wefunder.com/u888vipapp1
https://potofu.me/u888vipapp1
https://transfur.com/Users/u888vipapp1
https://xtremepape.rs/members/u888vipapp1.668988/#about
https://website.informer.com/u888vip.app
https://en.islcollective.com/portfolio/12910735
https://www.xosothantai.com/members/u888vipapp1.610904/
https://velog.io/@u888vipapp1/about
https://violet.vn/user/show/id/15270982
https://iplogger.com/2takt8
https://mez.ink/u888vipapp1
https://u888vipapp1.stck.me/profile
https://www.edna.cz/uzivatele/u888vipapp1/
https://digiphoto.techbang.com/users/u888vipapp1
https://leakedmodels.com/forum/members/u888vipapp1.710996/#about
https://freeicons.io/profile/924687
https://inkbunny.net/u888vipapp1
https://www.japaaan.com/user/78157
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.u8884
https://apptuts.bio/u888-261920
https://www.storenvy.com/u888vipapp1
https://egl.circlly.com/users/u888vipapp1
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=302589
https://acomics.ru/-u888vipapp1
https://hanson.net/users/u888vipapp1
https://writexo.com/share/44af4a03fb22
https://expatguidekorea.com/profile/u888vipapp1/
https://www.heavyironjobs.com/profiles/8209643-nha-cai-u888
https://pad.degrowth.net/s/I2bK0u85Y
http://fort-raevskiy.ru/community/profile/u888vipapp1/
https://forum.skullgirlsmobile.com/members/u888vipapp1.218364/#about
https://jobs.landscapeindustrycareers.org/profiles/8209655-nha-cai-u888
https://phatwalletforums.com/user/u888vipapp1
https://song.link/u888vipapp1
https://idol.st/user/168810/u888vipapp1/
https://www.bmwpower.lv/user.php?u=u888vipapp1
https://gockhuat.net/member.php?u=437643
https://jobs.windomnews.com/profiles/8209670-nha-cai-u888
https://hoaxbuster.com/redacteur/u888vipapp1
https://www.givey.com/u888vipapp1
https://zerosuicidetraining.edc.org/user/profile.php?id=563005
https://joinentre.com/profile/u888vipapp1
https://jobs.westerncity.com/profiles/8209685-nha-cai-u888
https://www.thetriumphforum.com/members/u888vipapp1.63880/
https://album.link/u888vipapp1
https://dev.muvizu.com/Profile/u888vipapp1/Latest
https://chaloke.com/forums/users/u888vipapp1/
https://buckeyescoop.com/community/members/successful-neon-pink-coyote.63181/#about
https://toirscript.com/user/u888vipapp1
https://forum.pabbly.com/members/u888vipapp1.114843/#about
http://forum.cncprovn.com/members/425611-u888vipapp1
https://forum.aigato.vn/user/u888vipapp1
https://rapidapi.com/user/u888vipapp1
https://www.skool.com/@nha-cai-u-7156
https://learningapps.org/watch?v=p56gwhgu226
https://www.invelos.com/UserProfile.aspx?alias=u888vipapp1
https://www.video-bookmark.com/bookmark/7116829/u888/
https://gitlab.vuhdo.io/u888vipapp1
https://kktix.com/user/8702614
https://poipiku.com/13528390/
https://www.rwaq.org/users/u888vipapp1
https://www.fitday.com/fitness/forums/members/u888vipapp1.html
https://www.grepmed.com/u888vipapp1
https://classificados.acheiusa.com/profile/N0FaT0JaME9oL0VXUGhTcERubkQzcVRSdmtlZjExRHBMbFpWUk4xanJnND0=
https://espritgames.com/members/50923548/
https://hi-fi-forum.net/profile/1147626
https://secondstreet.ru/profile/u888vipapp1/
https://scenarch.com/userpages/34485
https://undrtone.com/u888vipapp1
https://marshallyin.com/members/u888vipapp1/
https://www.atozed.com/forums/user-79205.html
https://gravesales.com/author/u888vipapp1/
https://hukukevi.net/user/u888vipapp1
https://savelist.co/my-lists/users/u888vipapp1
https://zzb.bz/wrFzSJ
https://www.themeqx.com/forums/users/u888vipapp1/
https://www.udrpsearch.com/user/u888vipapp1
https://www.xen-factory.com/index.php?members/u888vipapp1.157046/#about
https://b.io/nha-cai-u888-1777436989
https://www.blackhatprotools.info/member.php?288751-u888vipapp1
https://activepages.com.au/profile/u888vipapp1
https://tudomuaban.com/chi-tiet-rao-vat/2891045/u888vipapp1.html
https://phijkchu.com/a/u888vipapp1/video-channels
https://lifeinsys.com/user/u888vipapp1
https://kaeuchi.jp/forums/users/u888vipapp1/
https://www.claimajob.com/profiles/8209827-nha-cai-u888
https://protospielsouth.com/user/131679
https://theafricavoice.com/profile/u888vipapp1
https://www.brownbook.net/business/55055517/u888
https://app.hellothematic.com/creator/profile/1146965
https://hackmd.okfn.de/s/Syf22m10Wx
https://manylink.co/@u888vipapp1
https://beteiligung.hafencity.com/profile/u888vipapp1/
https://anyflip.com/homepage/qzqci
https://civitai.com/user/u888vipapp1
https://hoo.be/u888vipapp1
https://maxforlive.com/profile/user/u888vipapp1?tab=about
https://3dtoday.ru/blogs/u888vipapp1
https://mathlog.info/users/Y12j1pY2DXcpy00yDnOsB9SNNjq2
https://my.bio/u888vipapp1
https://community.cloudera.com/t5/user/viewprofilepage/user-id/151810
https://www.slmath.org/people/106227
https://fora.babinet.cz/profile.php?id=124879
https://www.shippingexplorer.net/en/user/u888vipapp1/282367
https://shhhnewcastleswingers.club/forums/users/u888vipapp1/
https://connect.gt/user/u888vipapp1
https://www.weddingbee.com/members/u888vipapp1/
https://kumu.io/u888vipapp1/u888#u888
https://www.sunlitcentrekenya.co.ke/author/u888vipapp1/
https://www.rcuniverse.com/forum/members/u888vipapp1.html
https://www.huntingnet.com/forum/members/u888vipapp1.html
https://vimeo.com/u888vipapp1
https://www.symbaloo.com/shared/AAAAA9gguz4AA41_W3O_aQ==
https://www.lingvolive.com/en-us/profile/7e66c07f-d956-45c3-b3d3-1eabd3eb64d3/translations
https://www.trackyserver.com/profile/248444
https://www.zubersoft.com/mobilesheets/forum/user-136534.html
https://www.mindomo.com/mindmap/e635d0a9c3d8410580dc35e76c0c63e9
https://md.coredump.ch/s/hyC8tGjSR
https://aprenderfotografia.online/usuarios/u888vipapp1/profile/
https://hackmd.hub.yt/s/HDAlB2M-G
https://sciencemission.com/profile/u888vipapp1
https://www.wvhired.com/profiles/8210477-nha-cai-u888
https://beteiligung.tengen.de/profile/u888vipapp1/
https://formulamasa.com/elearning/members/u888vipapp1/
https://chyoa.com/user/u888vipapp1
https://www.royalroad.com/profile/963415
https://backloggd.com/u/u888vipapp1/
https://forums.alliedmods.net/member.php?u=476507
https://community.jmp.com/t5/user/viewprofilepage/user-id/98190
https://viblo.asia/u/u888vipapp1/contact
https://brain-market.com/u/u888vipapp1
https://www.prosebox.net/book/108865/
https://forum.honorboundgame.com/user-510792.html
http://forum.modulebazaar.com/forums/user/u888vipapp1/
https://www.rcmx.net/userinfo.php?uid=17213
https://lqdoj.edu.vn/user/u888vipapp1
https://paperjale.eus/user/u888vipapp1
https://indiestorygeek.com/user/u888vipapp1
https://www.bandlab.com/u888vipapp1
https://www.keepandshare.com/discuss2/46499/u888
https://www.easyhits4u.com/profile.cgi?login=u888vipapp1
https://doc.anagora.org/s/bp1WCXKSn
https://profile.sampo.ru/u888vipapp1
https://fanclove.jp/profile/pv2xADa7JR
https://lustyweb.live/members/u888vipapp1.123852/
https://findaspring.org/members/u888vipapp1/
https://vietcurrency.vn/members/u888vipapp1.240214/#about
https://fengshuidirectory.com/dashboard/listings/u888vipapp1/
https://pets4friends.com/profile-1583628
https://participa.aytojaen.es/profiles/u888vipapp1/activity
https://linkmix.co/53967021
https://www.maanation.com/u888vipapp1
https://janitorai.com/profiles/86eff567-4c3d-406b-bbad-2d7c5f549dc6_profile-of-u-888-vipapp-1
http://linoit.com/users/u888vipapp1/canvases/U888
https://giloo.ist/member/u888vipapp1/
https://defence.pk/members/u888vipapp1.240256/#about
https://forum.jatekok.hu/User-u888vipapp1
https://www.buymusic.club/user/u888vipapp1
https://forum.freero.org/space-uid-24922.html
http://genina.com/user/editDone/5338330.page
https://rant.li/u888vipapp1/u888
https://chanylib.ru/ru/forum/user/26215/
https://producerbox.com/users/u888vipapp1
https://skrolli.fi/keskustelu/users/kiemhohoan5/
https://www.thehockeypaper.co.uk/forums/users/u888vipapp1
https://www.11plus.co.uk/users/kiemhohoan5/
https://opaseke.com/users/15376
https://app.getfarmish.com/profile/60516805-c6a3-42b9-b1f5-3d7739233843
https://nicheless.blog/author/u888vipapp1
https://zbrushcentral.jp/user/u888vipapp1
https://forum.rexygen.com/user/u888vipapp1
https://www.mapleprimes.com/users/u888vipapp1
https://www.adpost.com/u/u888vipapp1/
https://qiita.com/u888vipapp1
Postingan yang sangat membantu. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Hi there i am kavin, its my first time to commenting anywhere,
when i read this piece of writing i thought i could also create comment due to
this brilliant article.
I’m glad I gave this a full learn — it didn’t disappoint.
Postingan yang luar biasa. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Pretty component of content. I just stumbled upon your website and in accession capital to say that I get actually loved account your blog posts. Any way I will be subscribing to your augment and even I fulfillment you get admission to constantly fast.
Saya tidak umumnya berkomentar tetapi saya harus menyatakan hargai untuk posting yang luar biasa ini : D.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Saya menghargai usaha yang Anda curahkan untuk menyusun artikel ini. Informasi yang sangat berharga. Terima kasih!
Ini adalah blog yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Ini adalah topik yang sangat penting di hati saya, cheers, tapi di manakah detail kontak Anda?
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Namun, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak benar-benar setuju sepenuhnya, saya menilai perspektif.
Saya tidak amat luar biasa dalam bahasa Inggris tetapi saya menemukan ini sungguh ringan untuk diterjemahkan.
I couldn’t resist commenting. Perfectly written!
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi megah dibagikan secara bebas.
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Ini adalah situs yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Biasanya saya tidak membaca posting di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, sangat artikel yang bagus.
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Saya mendapatkan info yang bagus dari blog Anda.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Wow! Ini mungkin salah satu blog paling membantu yang pernah kami temui tentang topik ini. Sebenarnya Sangat baik. Saya juga seorang ahli dalam topik ini jadi saya dapat memahami usaha Anda.
Your comment is awaiting moderation.
https://www.youtube.com/@ao88mlcom
https://x.com/ao88mlcom
https://wakelet.com/@ao88mlcom
https://safechat.com/u/ao88mlcom
https://gravatar.com/ao88mlcom1
https://www.blogger.com/profile/03634287805600671326
https://www.pinterest.com/ao88mlcom/_profile/
https://demo.wowonder.com/ao88mlcom
https://shareyoursocial.com/ao88mlcom
https://myspace.com/ao88mlcom
https://500px.com/p/ao88mlcom
https://www.instapaper.com/p/ao88mlcom
https://band.us/band/102529476/post/1
https://protocol.ooo/ja/users/ao88mlcom
https://www.reddit.com/user/ao88mlcom/
https://audiomack.com/ao88mlcom
https://hackaday.io/ao88mlcom
https://fyers.in/community/member/a45q5jNDUV
https://vocal.media/authors/ao88mlcom
https://leetcode.com/u/ao88mlcom/
https://swag.live/en/user/69f45727ddfb2becc91d0727
https://www.halaltrip.com/user/profile/344536/ao88mlcom/
https://medibang.com/author/28222498/
https://www.blockdit.com/ao88mlcom
https://portfolium.com/ao88mlcom
https://www.twitch.tv/ao88mlcom/about
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:4AFC81D969F45AF60A495F8C@AdobeID
https://profile.hatena.ne.jp/ao88mlcom/
https://issuu.com/ao88mlcom
https://www.behance.net/ao88mlcom
https://www.reverbnation.com/artist/ao88mlcom
https://www.myminifactory.com/users/ao88mlcom
https://www.investagrams.com/Profile/ao88mlcom
https://gifyu.com/ao88mlcom
https://www.chordie.com/forum/profile.php?id=2520069
https://www.walkscore.com/people/278013786851/ao88
https://topsitenet.com/profile/ao88mlcom/1707368/
https://akniga.org/profile/1419534-ao88/
https://disqus.com/by/ao88mlcom/about/
https://jobs.suncommunitynews.com/profiles/8218023-nhacai-ao88
https://www.speedrun.com/users/ao88mlcom
https://www.fanart-central.net/user/ao88mlcom/profile
https://www.aicrowd.com/participants/ao88mlcom
https://www.bitchute.com/channel/bTeenJMaSVpb
https://pbase.com/ao88mlcom
https://hub.docker.com/u/ao88mlcom
https://spiderum.com/nguoi-dung/ao88mlcom
https://www.gta5-mods.com/users/ao88mlcom
https://heylink.me/ao88mlcom/
https://pixabay.com/users/ao88mlcom-55670034/
https://www.nicovideo.jp/user/144096096
https://tinyurl.com/ao88mlcom
https://www.jigsawplanet.com/ao88mlcom
https://3dwarehouse.sketchup.com/by/ao88mlcom
https://robertsspaceindustries.com/en/citizens/ao88mlcom
https://bit.ly/m/ao88mlcom
https://allmylinks.com/ao88mlcom
https://www.tumblr.com/ao88mlcom1
https://scholar.google.com/citations?hl=en&view_op=list_works&gmla=AIqSsVuDqCpgVY9VfmJ9LGVjXicR5ueNyhoJRIzo1Xv9A75eVQJUhEEtXuiK9riDkjdePE-5zcPUMVtd37VK4A&user=VDsiMIUAAAAJ
https://sites.google.com/view/ao88mlcom/
https://ao88mlcom1.blogspot.com/2026/05/ao88-trang-chu-ao88com-chinh-thuc-ang.html
https://ok.ru/profile/910467757099/statuses/159080523209515
https://ao88mlcom.hashnode.dev/
https://medium.com/@ao88mlcom/about
https://www.slideshare.net/tung264an?tab=about
https://soundcloud.com/ao88mlcom
https://ixawiki.com/link.php?url=https://ao88ml.com/
https://writexo.com/share/204ae7ac6479
https://newdayrp.com/members/ao88mlcom.71814/#about
https://web.bikemap.net/u/ao88mlcom
http://www.activewin.com/user.asp?Action=Read&UserIndex=4839806
https://construim.fedaia.org/profiles/ao88mlcom/activity
https://bbs.theviko.com/home.php?mod=space&uid=4655540
https://www.xiuwushidai.com/home.php?mod=space&uid=2684022
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6448885
https://imgur.com/a/MGhKbSH
https://easymeals.qodeinteractive.com/forums/users/ao88mlcom
https://bookmeter.com/users/1715785
https://rb.gy/5tbich
https://startupxplore.com/en/person/ao88-5
https://www.mynbest.info/profile/tung264an17179/profile
https://jasa-seo.mn.co/members/39526679
https://creativemarket.com/users/ao88mlcom
https://www.zazzle.pt/mbr/238611502928829746
https://maps.arosalenzerheide.swiss/en/member/nhacai-ao88/340125015/
https://luma.com/user/ao88mlcom
https://www.africangenesis-101.org/profile/tung264an35700/profile
https://sitereport.netcraft.com/?url=https://ao88ml.com/
https://www.miseducationofmotherhood.com/profile/tung264an71104/profile
https://www.housedumonde.com/profile/tung264an83243/profile
https://www.macdermottmethod.com/members-area/ao88mlcom/profile
https://antique-anaconda-841.notion.site/AO88-Trang-Ch-AO88-COM-Ch-nh-Th-c-ng-K-V-ng-Nh-p-Nh-n-u-i-100-353036b33918807e818dd372a87d0cde?pvs=73
https://quicknote.io/2816eef0-455e-11f1-9955-cf2afc450c48
https://t.ly/xy64D
https://m.xtutti.com/user/profile/489226
https://www.webmastersun.com/members/ao88mlcom.164471/#about
https://drivehud.com/forums/users/tung264an
https://ao88mlcom1.stck.me/profile
https://surli.cc/xaaaes
https://joy.link/ao88mlcom
https://connect.garmin.com/app/profile/1a91ff7c-8bec-4ecf-b583-2d7c935d8219
https://b.hatena.ne.jp/ao88mlcom/bookmark
https://www.chichi-pui.com/users/ao88mlcom/
https://www.openrec.tv/user/ao88mlcom/about
https://unityroom.com/users/ao88mlcom
https://routinehub.co/user/ao88mlcom
https://pxhere.com/en/photographer-me/5000154
https://teletype.in/@ao88mlcom
https://www.checkli.com/ao88mlcom#/a/process
https://www.nintendo-master.com/profil/ao88mlcom
https://freeimage.host/ao88mlcom
https://motion-gallery.net/users/975391
https://linkin.bio/ao88mlcom/
https://biomolecula.ru/authors/144853
https://talk.plesk.com/members/aomlcom.504742/#about
https://www.callupcontact.com/b/businessprofile/ao88mlcom/10073148
https://website.informer.com/ao88ml.com
https://blender.community/ao887/
https://doselect.com/@4618c5084f29d5dad0b0dc3e4
https://sciter.com/forums/users/ao88mlcom/
https://matkafasi.com/user/ao88mlcom
https://allmyfaves.com/ao88mlcom
https://www.notebook.ai/users/1349935
https://www.abclinuxu.cz/lide/ao88mlcom
https://muare.vn/shop/ao88mlcom/903631
https://musikersuche.musicstore.de/profil/ao88mlcom/
https://lookingforclan.com/user/ao88mlcom
https://forum.dmec.vn/index.php?members/ao88mlcom.189913/
https://igli.me/ao88mlcom
https://urlz.fr/v8h2
http://delphi.larsbo.org/user/ao88mlcom
https://www.aseeralkotb.com/en/profiles/ao88mlcom
https://timdaily.vn/members/ao88mlcom.135149/#about
https://app.readthedocs.org/profiles/ao88mlcom/
https://www.dibiz.com/tung264an
https://iszene.com/user-349554.html
https://www.theyeshivaworld.com/coffeeroom/users/ao88mlcom
https://desksnear.me/users/ao88-13451c
http://resurrection.bungie.org/forum/index.pl?profile=ao88mlcom
https://pad.lescommuns.org/s/92mrju-8c
https://www.itchyforum.com/en/member.php?389506-ao88mlcom
https://www.roton.com/forums/users/tung264an
https://able2know.org/user/ao88mlcom/
http://www.biblesupport.com/user/835228-ao88mlcom/
https://golosknig.com/profile/ao88mlcom/
https://wallhaven.cc/user/ao88mlcom
http://www.library.sokal.lviv.ua/forum/profile.php?mode=viewprofile&u=18564
https://bandori.party/user/865327/ao88mlcom/
https://schoolido.lu/user/ao88mlcom/
https://awan.pro/forum/user/168982/
https://fortunetelleroracle.com/profile/ao88mlcom
https://fabble.cc/ao88mlcom
https://www.zazzle.com/mbr/238611502928829746
https://tempel.in/view/AseyZsG
https://rentry.co/k859zpn8
https://pad.geolab.space/s/K7qSKONuD
https://pad.stuve.de/s/LOTgWEF_t4
https://www.sythe.org/members/ao88mlcom.2044305/
https://f319.com/members/ao88mlcom.1102629/
https://about.me/ao88mlcom/
https://www.canadavisa.com/canada-immigration-discussion-board/members/ao88mlcom.1355254/#about
https://www.equinenow.com/farm/profile69f46a763e08a.htm
https://www.gaiaonline.com/profiles/ao88mlcom/50668998/
https://participacion.cabildofuer.es/profiles/ao88mlcom/activity?locale=en
https://expatguidekorea.com/profile/ao88mlcom/
https://www.heavyironjobs.com/profiles/8218429-nha-cai-ao88
https://transfur.com/Users/ao88mlcom
https://xtremepape.rs/members/ao88mlcom.669763/#about
https://kooperation.winterthur.ch/profiles/ao88mlcom/activity
https://www.xosothantai.com/members/ao88mlcom.611267/
https://www.edna.cz/uzivatele/ao88mlcom/
https://www.invelos.com/UserProfile.aspx?alias=ao88mlcom
https://tudomuaban.com/chi-tiet-rao-vat/2892954/ao88mlcom.html
https://www.rcmx.net/userinfo.php?uid=17318
https://lqdoj.edu.vn/user/ao88mlcom1
https://paperjale.eus/user/ao88mlcom
https://fora.babinet.cz/profile.php?section=personal&id=125159
https://connect.gt/user/ao88mlcom
https://md.coredump.ch/s/0BhKxZS2R
https://participa.aytojaen.es/profiles/ao88mlcom/activity
https://forum.freero.org/space-uid-24962.html
https://te.legra.ph/ao88mlcom-05-01
https://md.un-hack-bar.de/s/FW-X_Fwybk
https://londonchinese.com/home.php?mod=space&uid=621482&do=profile
https://rant.li/ao88mlcom/a-href-ao88ml-com-ao88-a-la-mot-nen-tang-giai-tri-truc-tuyen-dang-thu-hut-su
https://chanylib.ru/ru/forum/user/26435/
https://skrolli.fi/keskustelu/users/tung264an/
https://www.11plus.co.uk/users/tung264an/
https://www.mikocon.com/home.php?mod=space&uid=291621
https://sklad-slabov.ru/forum/user/44405/
https://naijamatta.com/ao88mlcom
https://fact-finder.xyz/pukiwiki/?ao88mlcom
https://graph.org/ao88mlcom-05-01-2
https://cars.yclas.com/user/ao88mlcom
https://www.vnbadminton.com/members/ao88mlcom.76856/
https://shootinfo.com/ru/author/ao88mlcom/?pt=ads
https://truckymods.io/user/490580
https://aniworld.to/user/profil/ao88mlcom
https://hub.vroid.com/en/users/125849919
https://marshmallow-qa.com/vlcxrgm667bttby
https://sfx.thelazy.net/users/u/ao88mlcom/
https://turcia-tours.ru/forum/profile/ao88mlcom/
https://galleria.emotionflow.com/184596/profile.html
https://www.myget.org/users/ao88mlcom
https://stuv.othr.de/pad/s/HtHQ8mnnK
https://strikefans.com/forum/users/ao88mlcom/
https://experiment.com/users/ao88mlcom
https://forum-foxess.pro/community/profile/ao88mlcom/
http://julia4tied.de/member.php?action=profile&uid=247273
https://commoncause.optiontradingspeak.com/index.php/community/profile/ao88mlcom/
https://telegra.ph/ao88mlcom-05-01-3
https://www.dokkan-battle.fr/forums/users/ao88mlcom/
https://boss.why3s.cc/boss/home.php?mod=space&uid=263807
https://md.rappet.xyz/s/RNPwC7sHKJ
https://md.sebastians.dev/s/tIiYmG9b2
https://hedgedoc.eclair.ec-lyon.fr/s/89NY5KXFx
https://partecipa.poliste.com/profiles/ao88mlcom/activity
https://hedgedoc.stusta.de/s/HxDyG2otK
https://backloggery.com/ao88mlcom
http://palangshim.com/space-uid-5131109.html
https://forum.rexygen.com/user/ao88mlcom
https://zbrushcentral.jp/user/ao88mlcom
https://hcgdietinfo.com/hcgdietforums/members/ao88mlcom/
https://formulamasa.com/elearning/members/ao88mlcom/?v=96b62e1dce57
https://www.royalroad.com/profile/965017
https://backloggd.com/u/ao88mlcom/
https://careers.coloradopublichealth.org/profiles/8219262-nha-cai-ao88
https://aprenderfotografia.online/usuarios/ao88mlcom/profile/
https://www.horticulturaljobs.com/employers/4135237-ao88mlcom
https://jobs.lajobsportal.org/profiles/8219272-nha-cai-ao88
https://oye.participer.lyon.fr/profiles/ao88mlcom/activity
https://decidim.santcugat.cat/profiles/ao88mlcom/activity
https://jobs.siliconflorist.com/employers/4135245-ao88mlcom
https://jobs.nefeshinternational.org/employers/4135247-ao88mlcom
https://aboutcasemanagerjobs.com/author/ao88mlcom/
https://forum.issabel.org/u/ao88mlcomAO88
https://www.easyhits4u.com/profile.cgi?login=ao88mlcom
https://doc.anagora.org/s/LVIUroD5m
https://zenwriting.net/gpqv9jfzbr
https://writeablog.net/atw8fi9vvi
https://rush1989.rash.jp/pukiwiki/index.php?ao88mlcom
http://jobs.emiogp.com/author/ao88mlcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2483591
https://md.chaospott.de/s/PE9Ni04Iq9
https://md.opensourceecology.de/s/IVX46bLuB
http://jobboard.piasd.org/author/ao88mlcom/
https://hack.allmende.io/s/6j9d59oi-
https://bbs.darkml.net/home.php?mod=space&uid=155408
https://www.play56.net/home.php?mod=space&uid=6171601
https://hedgedoc.logilab.fr/s/39D7_6cEe
https://hker2uk.com/home.php?mod=space&uid=5521899
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=498611
https://pad.funkwhale.audio/s/m8ZRccLCv
http://pcsq28.com/home.php?mod=space&uid=2002593
https://bbs.airav.cc/home.php?mod=space&uid=4594185
https://forum.ct8.pl/member.php?action=profile&uid=122989
https://www.vid419.com/home.php?mod=space&uid=3487870
https://www.okaywan.com/home.php?mod=space&uid=800331
https://www.goodolcomics.com/blog/profile/ao88mlcom/
http://techou.jp/index.php?ao88mlcom
http://tkdlab.com/wiki/index.php?ao88mlcom
https://entre-vos-mains.alsace.eu/profiles/ao88mlcom/activity
https://www.france-ioi.org/user/perso.php?sLogin=ao88mlcom
https://divisionmidway.org/jobs/author/ao88mlcom/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=144452
https://ask.mallaky.com/?qa=user/ao88mlcom
https://hackmd.hub.yt/s/PaIU6PfYw
https://vietcurrency.vn/members/ao88mlcom.240373/#about
https://www.wvhired.com/profiles/8218538-nha-cai-ao88
https://www.sunlitcentrekenya.co.ke/author/ao88mlcom/
https://www.zubersoft.com/mobilesheets/forum/user-136962.html
https://www.weddingbee.com/members/ao88mlcom/
https://lifeinsys.com/user/ao88mlcom
https://kaeuchi.jp/forums/users/ao88mlcom/
https://www.claimajob.com/profiles/8218544-nha-cai-ao88
https://support.bitspower.com/support/user/ao88mlcom
https://www.spigotmc.org/members/ao88mlcom.2528495/
https://maxforlive.com/profile/user/ao88mlcom?tab=about
https://3dtoday.ru/blogs/ao88mlcom
https://theafricavoice.com/profile/ao88mlcom
https://hackmd.okfn.de/s/HyHDVrMRZl
https://krachelart.com/UserProfile/tabid/43/userId/1344254/Default.aspx
https://www.threadless.com/@ao88mlcom
https://www.xen-factory.com/index.php?members/ao88mlcom.157516/#about
https://forums.servethehome.com/index.php?members/ao88mlcom.241540/#about
https://www.blackhatprotools.info/member.php?289149-ao88mlcom
https://activepages.com.au/profile/ao88mlcom
https://www.fundable.com/nha-cai-ao88-6
https://espritgames.com/members/50961441/
https://www.udrpsearch.com/user/ao88mlcom
https://cgmood.com/ao88mlcom
https://scenarch.com/userpages/34733
https://undrtone.com/ao88mlcom
https://marshallyin.com/members/ao88mlcom/
https://www.atozed.com/forums/user-79562.html
https://gravesales.com/author/ao88mlcom/
https://www.themeqx.com/forums/users/ao88mlcom/
https://gitlab.vuhdo.io/ao88mlcom
https://digiphoto.techbang.com/users/ao88mlcom
https://leakedmodels.com/forum/members/ao88mlcom.711538/#about
https://freeicons.io/profile/925717
https://onlinesequencer.net/members/270928
https://inkbunny.net/ao88mlcom
https://www.japaaan.com/user/78455
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.ao8810
https://code.antopie.org/ao88mlcom
https://pad.degrowth.net/s/AOKEPWFUB
http://fort-raevskiy.ru/community/profile/ao88mlcom/
https://forum.skullgirlsmobile.com/members/ao88mlcom.219131/#about
https://jobs.landscapeindustrycareers.org/profiles/8218553-nha-cai-ao88
https://phatwalletforums.com/user/ao88mlcom
https://idol.st/user/169761/ao88mlcom/
https://www.bmwpower.lv/user.php?u=ao88mlcom
https://jobs.windomnews.com/profiles/8218999-nha-cai-ao88
https://hoaxbuster.com/redacteur/ao88mlcom
https://jobs.westerncity.com/profiles/8218556-nha-cai-ao88
https://www.thetriumphforum.com/members/ao88mlcom.64198/
https://buckeyescoop.com/community/members/ao88mlcom.63346/#about
https://toirscript.com/user/ao88mlcom
https://forum.pabbly.com/members/ao88mlcom.115440/#about
https://forum.aigato.vn/user/ao88mlcom
https://zepodcast.com/forums/users/ao88mlcom/
https://www.nedrago.com/forums/users/ao88mlcom/
https://www.beamng.com/members/ao88mlcom.791750/
https://beatsaver.com/playlists/1191605
https://apptuts.bio/ao88mlcom-262255
https://www.storenvy.com/ao88mlcom
https://diendan.bftvietnam.com/members/21704-ao88mlcom.html
https://forums.maxperformanceinc.com/forums/member.php?u=247871
https://egl.circlly.com/users/ao88mlcom
https://acomics.ru/-ao88mlcom
https://hanson.net/users/ao88mlcom
https://diendan.cuabenhvien.com/members/19842-ao88mlco.html
https://song.link/ao88mlcom
https://www.givey.com/ao88mlcom
https://zerosuicidetraining.edc.org/user/profile.php?id=563756
https://www.hobowars.com/game/linker.php?url=https://ao88ml.com/
https://album.link/ao88mlcom
https://dev.muvizu.com/Profile/ao88mlcom/Latest
https://www.skool.com/@nha-cai-ao-6061
https://learningapps.org/watch?v=p6fhyt9w526
https://www.video-bookmark.com/user/ao88mlcom
https://kktix.com/user/8710946
https://poipiku.com/13537759/
https://www.grepmed.com/ao88mlcom
https://classificados.acheiusa.com/profile/UHlTQm9kZ2xyZ2c3R21OTnk0VzV4MXY0V21QKytINExrYlhpUndJYndpRT0=
https://hi-fi-forum.net/profile/1148547
https://secondstreet.ru/profile/ao88mlcom/
https://hukukevi.net/user/ao88mlcom
https://belgaumonline.com/profile/ao88mlcom/
https://savelist.co/my-lists/users/ao88mlcom
https://zzb.bz/sFWtra
http://newdigital-world.com/members/ao88mlcom.html
https://b.io/ao88mlcom
https://snippet.host/fqesnt
https://phijkchu.com/a/ao88mlcom/video-channels
https://protospielsouth.com/user/132183
https://www.brownbook.net/business/55064727/ao88mlcom
https://app.hellothematic.com/creator/profile/1147608
https://manylink.co/@ao88mlcom
https://beteiligung.hafencity.com/profile/ao88mlcom/
https://anyflip.com/homepage/hgvak#About
https://www.akaqa.com/account/profile/19191886870
https://copynotes.be/shift4me/forum/user-53699.html
https://civitai.com/user/ao88mlcom
https://hoo.be/ao88mlcom
https://mathlog.info/users/IkKV0SeEKiYa9QOZpce2BYzW4Dj2
https://my.bio/ao88mlcom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/152060
https://www.slmath.org/people/106493
https://www.shippingexplorer.net/en/user/ao88mlcom/283237
https://shhhnewcastleswingers.club/forums/users/ao88mlcom/
https://kumu.io/ao88mlcom/ao88mlcom#ao88mlcom
https://www.rcuniverse.com/forum/members/ao88mlcom.html
https://www.huntingnet.com/forum/members/ao88mlcom.html
https://vimeo.com/ao88mlcom
https://www.symbaloo.com/mix/my-webmix-1kwp
https://www.lingvolive.com/en-us/profile/8b78f8b0-6e69-4ce9-8065-8ade4bdfda68/translations
https://www.trackyserver.com/profile/248965
https://www.mindomo.com/mindmap/ao88mlcom-182086a64a584270ae7db9658ae44701
https://potofu.me/ao88mlcom
https://wefunder.com/ao88mlcom/about
https://beteiligung.tengen.de/profile/ao88mlcom/
https://chyoa.com/user/ao88mlcom
https://forums.alliedmods.net/member.php?u=477631
https://community.jmp.com/t5/user/viewprofilepage/user-id/98389
https://viblo.asia/u/ao88mlcom/contact
https://hype4.academy/profile/ao88mlcom
https://brain-market.com/u/ao88mlcom
https://ikanakama.ink/users/341667
https://www.prosebox.net/book/109152/
https://redirect.camfrog.com/redirect/?url=https://ao88ml.com/
https://forum.honorboundgame.com/user-511086.html
https://www.fw-follow.com/forum/topic/121560/ao88mlcom
https://www.jk-green.com/forum/topic/114206/ao88mlcom
https://www.navacool.com/forum/topic/409495/ao88mlcom
https://www.driedsquidathome.com/forum/topic/147919/ao88mlcom
https://www.nongkhaempolice.com/forum/topic/130080/ao88mlcom
https://www.bestloveweddingstudio.com/forum/topic/86001/ao88mlcom
https://www.natthadon-sanengineering.com/forum/topic/108081/ao88mlcom
https://www.rueanmaihom.net/forum/topic/101216/ao88mlcom
https://www.ttlxshipping.com/forum/topic/409491/ao88mlcom
http://worldchampmambo.com/UserProfile/tabid/42/userId/489298/Default.aspx
http://forum.modulebazaar.com/forums/user/ao88mlcom/
https://eilo.org/user/ao88mlcom
https://forum.web-z.net/profile.php?userid=9992
https://iplogger.com/2e9Hs6
https://mez.ink/ao88mlcom
https://velog.io/@ao88mlcom/about
https://xaydunghanoimoi.net/members/27914-ao88mlco.html
https://ao88mlcom1.stck.me/profile
https://notionpress.com/author/1514447
https://indiestorygeek.com/user/ao88mlcom
https://www.bandlab.com/ao88mlcom
https://www.keepandshare.com/doc22/116375/ao88mlcom
https://profile.sampo.ru/ao88mlcom
https://www.ekdarun.com/forum/topic/157810/ao88mlcom
https://fanclove.jp/profile/no2aQzXE2a
https://www.d-ushop.com/forum/topic/135762/ao88mlcom
https://lustyweb.live/members/ao88mlcom.125310/#about
https://findaspring.org/members/ao88mlcom/
https://ketcau.com/member/128862-ao88mlcom
https://fengshuidirectory.com/dashboard/listings/ao88mlcom/
https://library.zortrax.com/members/ao88mlcom/
https://pets4friends.com/profile-1584865
https://linkmix.co/54037604
https://www.maanation.com/ao88mlcom
https://ao88mlcom1.amebaownd.com/posts/58785467
https://janitorai.com/profiles/cfc2ece0-3df2-49ac-b5a0-69d3da608bb1_profile-of-ao-88-mlcom
https://muckrack.com/ao88mlcom
http://linoit.com/users/ao88mlcom/canvases/ao88mlcom
https://nortabs.net/user/15230/
https://www.myconcertarchive.com/en/user_home?id=130825
https://giloo.ist/member/ao88mlcom
https://defence.pk/members/ao88mlcom.240430/#about
https://www.buymusic.club/user/ao88mlcom
http://genina.com/user/editDone/5339772.page
https://opaseke.com/users/15425
https://app.getfarmish.com/profile/ao88mlcom
https://imaginaria.ru/profile/ao88mlcom/
https://nicheless.blog/author/ao88mlcom
https://www.newgenstravel.com/forum/topic/44705/ao88
https://www.mapleprimes.com/users/ao88mlcom
https://noti.st/ao88mlcom
https://www.adpost.com/u/ao88mlcom/
https://guitarmaking.co.uk/members/ao88mlcom/activity/189770/
https://scrapbox.io/ao88mlcom/AO88
https://circle-book.com/circles/59204
https://forum.opnsense.org/index.php?action=profile;u=67901
https://qiita.com/ao88mlcom
https://www.annuncigratuititalia.it/author/ao88mlcom/
https://nonon-centsnanna.com/members/ao88mlcom/
https://lite.link/ao88mlcom
http://www.brenkoweb.com/user/89699/profile
https://hedgedoc.faimaison.net/s/o_xmdLvALH
https://www.rossoneriblog.com/author/ao88mlcom/
https://www.scamadviser.com/check-website/ao88ml.com
https://video.fc2.com/account/73815191
https://adplist.org/members/ao88-momvu3en
https://novel.daysneo.com/author/ao88mlcom/
https://destaquebrasil.com/saopaulo/author/ao88mlcom/
https://www.adsfare.com/ao88mlcom
https://makerworld.com/en/@ao88mlcom
https://bhmtsff.com/space-uid-97549.html
https://blog.sighpceducation.acm.org/wp/forums/users/ao88mlcom/
https://congdongmassage.com/members/ao88mlcom.149132/#about
https://www.tacter.com/@ao88mlcom
https://vc.ru/id5932347
https://l2top.co/forum/members/ao88mlcom.176096/
https://artist.link/ao88mlcom
https://dreevoo.com/profile_info.php?pid=1586601
https://www.passes.com/ao88mlcom
https://etextpad.com/x3hua6kpxb
https://app.talkshoe.com/user/ao88mlcom
https://m.wibki.com/ao88mlcom
https://pinshape.com/users/8959817-ao88mlcom?tab=designs
https://www.skypixel.com/users/djiuser-jksxa4zjfkhn
https://ao88mlcom1.notepin.co/
https://pictureinbottle.com/r/ao88mlcom
https://forum.epicbrowser.com/profile.php?id=153949
https://electroswingthing.com/profile/ao88mlcom/
https://www.socialbookmarkssite.com/user/ao88mlcom/
https://www.hogwartsishere.com/1838221/
https://makeagif.com/user/ao88mlcom?ref=0HI1OF&ref=n7Nl3T
https://www.plotterusati.it/user/ao88mlcom
https://linqto.me/about/AO88ao88mlcom
https://www.managementpedia.com/members/ao88mlcom.1121207/#about
https://pad.codefor.fr/s/p31MTtLeE4
https://pad.fablab-siegen.de/s/8fBbQsVL8K
https://md.swk-web.com/s/E4F8xBsTD
https://md.swk-web.com/s/0caMz9hkv
https://pad.darmstadt.social/s/d6n3KW0fWD
https://referrallist.com/profile/nha-cai-ao88/
https://md.chaosdorf.de/s/w4Nl7veEM9
https://smallseo.tools/website-checker/ao88ml.com
https://runtrip.jp/users/777486
https://www.bonback.com/forum/topic/409459/ao88
https://www.pathumratjotun.com/forum/topic/181269/ao88
https://www.iglinks.io/tung264an-blt?preview=true
https://homepage.ninja/ao88mlcom
https://www.gabitos.com/catalunyauniversal/template.php?nm=1777642144
https://www.foriio.com/ao88mlcom
https://maiotaku.com/p/ao88mlcom/info
https://justpaste.it/u/ao88mlcom
https://www.pozible.com/profile/nha-cai-ao88-1
https://www.elephantjournal.com/profile/ao88mlcom/
https://forum.allkpop.com/suite/user/315823-ao88mlcom/#about
https://swat-portal.com/forum/wcf/user/49682-ao88mlcom/#about
https://stocktwits.com/ao88mlcom
https://mercadodinamico.com.br/author/ao88mlcom/
https://www.grabcaruber.com/members/ao88mlcom/profile/
https://www.magcloud.com/user/ao88mlcom
https://bioqoo.com/ao88mlcom
https://bike-forum.cz/profil/u/ao88mlcom
https://app.brancher.ai/user/qRdIwfF9uIWg
https://confengine.com/user/ao88mlcom
https://forum.aceinna.com/user/ao88mlcom
https://www.giveawayoftheday.com/forums/profile/1835102
https://uiverse.io/profile/ao88mlcom_8555
https://cofacts.tw/user/ao88mlcom
https://www.efunda.com/members/people/show_people.cfm?Usr=ao88mlcom
https://pumpyoursound.com/u/user/1617369
https://usdinstitute.com/forums/users/ao88mlcom/
https://congdongx.com/thanh-vien/ao88mlcom.49516/#about
https://doodleordie.com/profile/ao88mlcom
https://www.intensedebate.com/people/ao88mlcom
https://tabelog.com/rvwr/ao88mlcom/prof/
https://www.tkaraoke.com/forums/profile/ao88mlcom/
https://app.parler.com/ao88mlcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:4AFC81D969F45AF60A495F8C@AdobeID
https://svetelektro.com/clenovia/ao88/
https://www.diigo.com/profile/ao88mlcom
https://us.enrollbusiness.com/BusinessProfile/7793352/ao88mlcom
https://link4u.cc/@ao88mlcom
https://iplogger.org/vn/logger/f5CR51hU2VrR/
https://www.iniuria.us/forum/member.php?677904-ao88mlcom
https://cointr.ee/ao88mlcom
https://hedgedoc.envs.net/s/7s0m9U9CO
https://www.hentai-foundry.com/user/ao88mlcom/profile
teletype.link/ao88mlcom
https://official.link/ao88mlcom
https://www.czporadna.cz/user/ao88mlcom
https://www.lola.vn/dien-dan/hoat-dong-cua-cong-dong/shop-uy-tin-cung-lolavn/ao88–trang-chu-ao88com-chinh-thuc–dang-ky-va-dang-nhap-nhan-uu-dai-100.htm
https://tutorialslink.com/member/ao88mlcomundefined/99878
https://expathealthseoul.com/profile/ao88mlcom/
https://www.goodreads.com/review/show/8566488622
https://commu.nosv.org/p/ao88mlcom
https://www.weddingvendors.com/directory/profile/40354/
https://matters.town/@ao88mlcom
https://www.abookmarking.com/story/ao88-link-dang-nhap-ao88-com-dang-nhap-nhan-288k
https://www.mateball.com/ao88mlcom
https://photouploads.com/ao88mlcom
https://advego.com/profile/ao88mlcom/
https://bio.site/ao88mlcom
https://form.jotform.com/261204258312043
https://www.myebook.com/user_profile.php?id=ao88mlcom
https://www.sunemall.com/board/board_topic/8431232/8245461.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/8245463.htm
https://solo.to/ao88mlcom
https://boards.rossmanngroup.com/members/ao88mlcom.92640/
https://scanverify.com/siteverify.php?site=ao88ml.com
https://www.fcc.gov/fcc-bin/bye?https://ao88ml.com
https://rmmedia.ru/members/184042/#about
https://www.notariosyregistradores.com/web/forums/usuario/ao88mlcom/
https://www.biblicaleldership.com/forums/users/ao88mlcom/
https://luvly.co/users/ao88mlcom
http://onlineboxing.net/jforum/user/profile/453057.page
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8245497.htm
https://www.tai-ji.net/board/board_topic/4160148/8245501.htm
https://www.vhs80.com/board/board_topic/6798823/8245502.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8245503.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8245505.htm
https://alfounder.com/forums/users/ao88mlcom/
https://180degreehealth.com/180forums/users/ao88mlcom/
https://crazyservice.by/forum/user/15625/
https://rsfpost.com/forums/users/ao88mlcom/
https://exceldemy.com/forum/members/ao88mlcom.5036/about
https://house.karuizawa.co.jp/forums/users/ao88mlcom/
https://www.ontime.co.th/forum/topic/808571/ao88
https://forum.gettinglost.ca/user/ao88mlcom
https://www.portotheme.com/forums/users/ao88mlcom/
https://www.aleviforum.com/ao88mlcom
https://monviet88.com/profile/ao88mlcom/
https://oto-hui.com/members/aomlcom.433508/about
https://www.fuelly.com/driver/ao88mlcom
https://www.physicsoverflow.org/user/ao88mlcom
https://www.stylevore.com/user/ao88mlcom
https://www.spacedesk.net/support-forum/profile/ao88mlcom/
https://freelance.ru/ao88mlcom
https://alumni.mgimo.ru/page/adaptive/id396161/
https://letterboxd.com/ao88mlcom/list/ao88mlcom/
https://trakteer.id/ao88mlcom
https://onespotsocial.com/ao88mlcom
https://www.scener.com/@ao88mlcom
https://www.freelistingaustralia.com/listings/ao88mlcom
https://amaz0ns.com/forums/users/ao88mlcom/
https://hostndobezi.com/ao88mlcom
https://nilechronicles.com/profile/ao88mlcom
https://paper.wf/ao88mlcom/ao88mlcom
https://biiut.com/ao88mlcom
https://devfolio.co/@ao88mlcom/readme-md
https://wibki.com/ao88mlcom
https://aphorismsgalore.com/users/ao88mlcom
https://comicvine.gamespot.com/profile/ao88mlcom/
https://www.renderosity.com/users/id:1854307
https://www.moshpyt.com/user/ao88mlcom
https://www.racerjobs.com/profiles/8218566-nha-cai-ao88
https://help.orrs.de/user/ao88mlcom
https://www.instructorsnearme.com/author/ao88mlcom/
https://www.inventoridigiochi.it/membri/ao88mlcom/profile/
https://ferrariformula1.hu/community/profile/ao88mlcom/
https://en.cofacts.tw/user/ao88mlcom
https://www.pebforum.com/members/ao88mlcom.242435/#about
http://koloboklinks.com/site?url=ao88ml.com
http://freestyler.ws/user/653890/ao88mlcom
https://justpaste.me/ImIN4
https://www.freelistingusa.com/listings/ao88-12
https://searchengines.guru/ru/users/2235162
https://www.swap-bot.com/user:ao88mlcom
https://www.aviacionargentina.net/user/ao88mlcom
https://www.fullhires.com/author/ao88mlcom/
https://ac.db0.company/user/11008/ao88mlcom/
https://www.youyooz.com/profile/ao88mlcom/
https://forum.hiv.plus/user/ao88mlcom
https://affariat.com/user/profile/180398
https://theexplorers.com/user?id=95d74622-991b-4186-ba74-dfae854bd079
https://aiforkids.in/qa/user/ao88mlcom+1
https://www.thitrungruangclinic.com/forum/topic/130027/ao88mlcom
https://ja.cofacts.tw/user/ao88mlcom
https://fr.islcollective.com/portfolio/12912602
https://hedgedoc.faimaison.bangladhadha.com/load.php?note=b64d9123
https://es.islcollective.com/portafolio/12912602
https://forums.stardock.com/user/7664788
https://baskadia.com/user/gs71
https://buyerseller.xyz/user/ao88mlcom/
https://www.democracylab.org/user/41056
https://vs.cga.gg/user/242203
https://upuge.com/ao88mlcom
https://youslade.com/ao88mlcom
https://www.fitlynk.com/1777641167F119866
https://killtv.me/user/ao88mlcom/
https://bsky.app/profile/ao88mlcom.bsky.social
https://app.nft.nyc/wallet/69f4a72d506166a972d12210
https://englishsharedfutures.uk/forums/users/ao88mlcom1/
https://www.xmonsta.com/forums/users/ao88mlcom/
https://www.green-collar.com/forums/users/ao88mlcom/
https://pimrec.pnu.edu.ua/members/ao88mlcom1/profile/
https://www.hostboard.com/forums/members/ao88mlcom.html
https://forum.euro-pvp.com/user/561052-ao88mlcom/
https://infinitebacklog.net/users/ao88mlcom
https://quangcaoso.vn/ao88mlcom/gioithieu.html
https://vasep.vn/members/ao88mlcom.7555/#about
https://opensea.io/ao88mlcom
https://xmrbazaar.com/user/ao88mlcom/
https://tuscl.net/member/888026
https://triberr.com/ao88mlcom
https://raovatonline.org/author/ao88mlcom/
https://topkif.nvinio.com/ao88mlcom
https://kotob4all.com/profile/ao88mlcom
https://www.ironlifting.it/forum/member.php?u=430085
https://nogu.org.uk/forum/profile/ao88mlcom1/
https://reactormag.com/members/ao88mlcom/
https://gitflic.ru/user/ao88mlcom
https://www.funsocio.com/ao88mlcom
https://www.themirch.com/blog/author/ao88mlcom/
https://mikropragmata.lifo.gr/meli/ao88mlcom/profile/
https://community.concretecms.com/members/profile/391303
https://foss.heptapod.net/ao88mlcom
https://mail.protospielsouth.com/user/132183
https://www.euskalmarket.com/author/ao88mlcom/
https://bkk.tips/forums/users/ao88mlcom/
https://www.globalbusinesslisting.org/ao88-4
https://doingbusiness.eu/profile/ao88mlcom/
https://portfolium.com.au/ao88mlcom
https://www.tizmos.com/ao88mlcom/
https://ic-info.ru/forum/user/223614/
https://stardust.run/user/172041/ao88mlcom/
https://www.thethingsnetwork.org/u/ao88mlcom
https://mail.tudomuaban.com/chi-tiet-rao-vat/2893041/ao88mlcom.html
https://www.facer.io/u/ao88mlcom
https://www.muvizu.com/Profile/ao88mlcom/Latest
https://adhocracy.plus/profile/ao88mlcom/
https://www.cryptoispy.com/forums/users/ao88mlcom/
https://swdteam.com/profile/ao88mlcom
https://forum.cnnr.fr/user/ao88mlcom
https://jobs.host-panel.com/author/ao88mlcom/
https://item.exchange/user/profile/183221
https://lankadevelopers.lk/user/ao88mlcom
https://www.simplexthailand.com/forum/topic/23825/ao88mlcom
https://sistacafe.com/user/616062
https://www.bunyipclassifieds.com.au/pro/20260502005619
https://www.hardmcasual.net/user/792/
https://zimexapp.co.zw/ao88mlcom
https://triumph.srivenkateshwaraa.edu.in/profile/ao88mlcom1
https://vn.ekademia.com/@ao88mlcom
https://fueler.io/ao88mlcom
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3959384
https://kyourc.com/ao88mlcom
https://feyenoord.supporters.nl/profiel/150311/ao88mlcom
https://ru.myanimeshelf.com/profile/ao88mlcom
https://giaoan.violet.vn/user/show/id/15271645
https://webyourself.eu/ao88mlcom
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345956
https://cinderella.pro/user/274481/ao88mlcom/
https://www.discogs.com/fr/user/ao88mlcom
https://domain.opendns.com/ao88ml.com
https://violet.vn/user/show/id/15271645
https://kabos.net/profile/ao88mlcom/
https://qoolink.co/ao88mlcom
https://bandsworksconcerts.info/index.php?ao88mlcom
https://jali.pro/ao88mlcom
https://forums.giantitp.com/member.php?374483-ao88mlcom
https://seomotionz.com/member.php?action=profile&uid=129690
https://ngel.ink/ao88mlcom
https://coolors.co/u/ao88mlcom
https://boosty.to/ao88mlcom
https://camp-fire.jp/profile/ao88mlcom
https://www.pearltrees.com/ao88mlcom/item793950985
https://gesoten.com/profile/detail/12785968
https://hashnode.com/@ao88mlcom
https://nhattao.com/members/user6961713.6961713/
https://morguefile.com/creative/ao88mlcom
https://edabit.com/user/zjR9s5tNDPYTMZCAE
https://securityheaders.com/?q=https://ao88ml.com/
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=167181
https://md.darmstadt.ccc.de/s/O0eljoZinA
https://webanketa.com/forms/6mvkce1h64qparsq6ww3js9h/
https://goo.by/bqGsqu
https://doc.adminforge.de/s/Qj8k1Wgsg7
https://onlinevetjobs.com/author/ao88mlcom/
https://v.gd/CTdbd7
Benar-benar jelas web site, terima kasih untuk pos ini.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Hello, all is going sound here and ofcourse every one
is sharing facts, that’s actually good, keep up writing.
I am truly happy to read this website posts
which consists of plenty of valuable facts, thanks for providing these
kinds of statistics.
Very nice post. I just stumbled upon your blog and wanted to say that I’ve truly enjoyed browsing your blog posts. After all I will be subscribing to your feed and I hope you write again soon!
Saya mengunjungi banyak website tetapi saya pikir yang satu ini mengandung sesuatu yang spesial di dalamnya
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke blog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Terima kasih, saya baru saja mencari informasi sekitar topik ini cukup lama dan milik Anda adalah yang paling hebat yang saya ketahui sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda yakin tentang asal tersebut?
Please let me know if you’re looking for a article writer for your site. You have some really great posts and I believe I would be a good asset. If you ever want to take some of the load off, I’d love to write some articles for your blog in exchange for a link back to mine. Please shoot me an email if interested. Kudos!
After checking out a few of the blog posts on your web page,
I truly like your way of writing a blog. I book marked it to my bookmark site list
and will be checking back soon. Please check out my website as well and let
me know your opinion.
Informasi yang bermanfaat. Saya baru saja mencari hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Ini adalah situs yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar luar biasa!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
If some one wants to be updated with newest technologies after that he must be pay a visit this website and be up to date everyday.
Real nice pattern and wonderful written content, nothing else we want :D.
hello!,I like your writing very much! share we communicate more about your post on AOL? I require an expert on this area to solve my problem. Maybe that’s you! Looking forward to see you.
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ⴝtates
254-275-5536
Highquality
hey there and thank you for your information – I’ve certainly picked up
anything new from right here. I did however expertise some
technical issues using this website, as I experienced to reload the site many times
previous to I could get it to load correctly.
I had been wondering if your web hosting is OK?
Not that I am complaining, but slow loading instances times will sometimes affect your placement in google and can damage your high quality score if advertising and marketing with Adwords.
Anyway I’m adding this RSS to my e-mail and could look out for a lot more
of your respective fascinating content. Ensure that you update this again very soon.
Thanks for sharing your thoughts. I really appreciate
your efforts and I am waiting for your next post thanks once again.
Postingan yang sangat berguna. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Saya mendapatkan info yang bagus dari blog Anda.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
I’d should test with you here. Which is not something I normally do! I take pleasure in studying a submit that may make individuals think. Also, thanks for allowing me to comment!
great points altogether, you simply gained a new reader. What may you recommend about your publish that you simply made a few days in the past? Any certain?
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Amat baik info dapat ditemukan di blog.
A fascinating discussion is definitely worth comment. I
do think that you need to write more on this subject
matter, it may not be a taboo matter but typically folks don’t discuss these subjects.
To the next! All the best!!
It’s a shame you don’t have a donate button! I’d without a doubt donate to this
brilliant blog! I suppose for now i’ll settle for book-marking and adding your RSS feed to my Google account.
I look forward to new updates and will share this blog with my Facebook
group. Chat soon!
Yeah bookmaking this wasn’t a high risk determination great post! .
Your comment is awaiting moderation.
https://www.youtube.com/@28betxt
https://x.com/28betxt
https://wakelet.com/@28betxt
https://safechat.com/u/28betxtcom.556
https://gravatar.com/28betxt
https://www.blogger.com/profile/10444286873284757365
https://www.mymeetbook.com/28betxtcom
https://www.pinterest.com/28betxt/
https://demo.wowonder.com/28betxt
https://500px.com/p/28betxt
https://instapaper.com/p/28betxt
https://www.band.us/band/102468826/post
https://protocol.ooo/en/users/nha-cai-28bet-5dda4aea-7913-4929-a1fa-9038770d207c
https://www.reddit.com/user/Alternative-News9934/
https://audiomack.com/28betxt
https://hackaday.io/28betxt
https://vocal.media/authors/28betxtcom-mf22s0arw
https://leetcode.com/u/28betxtcom1/
https://swag.live/user/69eea497febb93f98d689f07
https://www.halaltrip.com/user/profile/342655/28betxtcom1/
https://medibang.com/author/28199239/
https://www.blockdit.com/28betxtcom1
https://profile.hatena.ne.jp/tk28bet/
https://issuu.com/28betxtcom1
https://www.behance.net/28betnhci
https://www.reverbnation.com/28betxtcom1?profile_view_source=header_icon_nav
https://www.myminifactory.com/users/28betxtcom
https://www.investagrams.com/Profile/28betxtcom1
https://gifyu.com/28betxtcom1
https://www.chordie.com/forum/profile.php?id=2516218
https://www.walkscore.com/people/266724883298/28betxtcom
https://akniga.org/profile/1417948-28betxtcom/
https://disqus.com/by/28betxtcom1/
https://jobs.suncommunitynews.com/profiles/8200816-nha-cai-28bet
https://www.speedrun.com/users/28betxtcom1
https://www.fanart-central.net/user/28betxtcom1/profile
https://www.aicrowd.com/participants/nha_cai_28bet5
https://www.bitchute.com/profile/mvKiHEoQLepG
https://www.bitchute.com/profile/mvKiHEoQLepG
https://hub.docker.com/u/28betxtcom1
https://spiderum.com/nguoi-dung/28betxtcom1
https://www.gta5-mods.com/users/28betxtcom1
https://heylink.me/28betxtcom1/
https://pixabay.com/users/28betxtcom1-55610686/
https://www.jigsawplanet.com/28betxtcom1
https://robertsspaceindustries.com/en/citizens/28betxtcom1
https://fr.scribd.com/user/977321484/nha-cai-28bet
https://28betxtcom1.mypixieset.com/
https://web.bikemap.net/u/28betxtcom1
https://lamsn.com/home.php?mod=space&uid=1989822
http://www.activewin.com/user.asp?Action=Read&UserIndex=4838994&redir=&redirname=Forums
https://bbs.theviko.com/home.php?mod=space&uid=4639605
https://www.xiuwushidai.com/home.php?mod=space&uid=2678084
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6425657
https://forum.dboglobal.to/wsc/index.php?user/148917-28betxtcom1/
https://easymeals.qodeinteractive.com/forums/users/28betxtcom1/
https://bookmeter.com/users/1713892
https://party.biz/index.php/profile/382059?tab=541
https://rb.gy/a2hm86
https://files.fm/28betxtcom1/info
https://www.mynbest.info/profile/danbuithi60385084/profile
https://jasa-seo.mn.co/members/39456694
https://creativemarket.com/users/28betxtcom1
https://maps.arosalenzerheide.swiss/en/member/nha-cai-28bet/339763436/
https://luma.com/user/28betxtcom1
https://www.africangenesis-101.org/profile/danbuithi60347947/profile
https://www.proko.com/@28betxtcom1/activity
https://sitereport.netcraft.com/?url=https://28betxt.com/
https://www.miseducationofmotherhood.com/profile/danbuithi60382186/profile
https://www.housedumonde.com/profile/danbuithi60335166/profile
https://www.macdermottmethod.com/members-area/danbuithi60370843/profile
https://quicknote.io/3a0750f0-41da-11f1-8882-194fcfe41860/
https://t.ly/fsrG_
https://m.xtutti.com/user/profile/488746
https://postr.blog/profile/28betxtcom1
https://jobs.dfw501c.com/profiles/8200755-nha-cai-28bet
https://theomnibuzz.com/author/28betxtcom1
https://architecture-jobs.architizer.com/profiles/8200772-nha-cai-28bet
https://www.webmastersun.com/members/28betxtcom1.163893/
https://drivehud.com/forums/users/danbuithi603/
https://28betxtcom1.stck.me/
https://jobs.njota.org/employers/4128308-nha-cai-28bet
https://connect.garmin.com/app/profile/2dd78ae4-ab2f-4395-bd6f-d44fea3f20bf
https://www.chichi-pui.com/users/28betxtcom1/
https://www.openrec.tv/user/28betxtcom1/about
https://routinehub.co/user/28betxtcom1
https://pxhere.com/en/photographer/4995044
https://teletype.in/@28betxtcom1
https://www.checkli.com/28betxtcom1#/a/process
https://www.nintendo-master.com/profil/28betxtcom1
https://freeimage.host/28betxtcom1
https://motion-gallery.net/users/961425
https://linkin.bio/28betxtcom1/
https://biomolecula.ru/authors/143740
https://www.callupcontact.com/main.php?bid=10066182
https://doselect.com/@5f77ce48f1aa1c60b4e857f89
https://blender.community/28betxtcom1/
https://sciter.com/forums/users/28betxtcom/
https://matkafasi.com/user/28betxtcom1
https://allmyfaves.com/28betxtcom1
https://www.notebook.ai/users/1346749
https://www.abclinuxu.cz/lide/28betxtcom
https://muare.vn/shop/28betxtcom1/903181
https://musikersuche.musicstore.de/profil/28betxtcom/
https://lookingforclan.com/user/28betxtcom
https://forum.dmec.vn/index.php?members/28betxtcom1.188983/
https://igli.me/28betxtcom1
http://delphi.larsbo.org/user/28betxtcom
https://www.aseeralkotb.com/en/profiles/28betxtcom1
https://timdaily.vn/members/28betxtcom1.134790/#about
https://app.readthedocs.org/profiles/28betxtcom1/
https://www.dibiz.com/danbuithi603
https://iszene.com/user-348851.html
https://www.theyeshivaworld.com/coffeeroom/users/28betxtcom
https://desksnear.me/users/nha-cai-28bet
https://bachhoadep.com/members/23331-28betxtc.html
https://www.itchyforum.com/en/member.php?389028-28betxtcom1
https://www.roton.com/forums/users/lythuyu1ml/
https://able2know.org/user/28betxtcom1/
http://www.biblesupport.com/user/833562-28betxtcom/
https://golosknig.com/profile/28betxtcom1/
https://wallhaven.cc/user/28betxtcom1
https://chothai24h.com/members/30571-28bextc.html
https://bandori.party/user/827533/28betxtcom1/
https://schoolido.lu/user/28betxtcom1/
https://awan.pro/forum/user/167637/
https://fabble.cc/28bet1
https://pad.geolab.space/s/iCOT0BPUR
https://pad.stuve.de/s/HwLC47qiZ
https://www.sythe.org/members/28betxtcom1.2042522/
https://f319.com/members/28betxtcom1.1100741/
https://about.me/betxtcom
https://www.canadavisa.com/canada-immigration-discussion-board/members/28betxtcom1.1354592/#about
https://www.equinenow.com/farm/nh-ci-28bet-1329626.htm
https://www.gaiaonline.com/profiles/28betxtcom1/50667474/
https://wefunder.com/28betxtcom1/about
https://potofu.me/28betxtcom1
https://transfur.com/Users/betxtcom
https://xtremepape.rs/members/28betxtcom1.668253/#about
https://gachmienbac.com/members/12869-28betxtc.html
https://qna.habr.com/user/28betxtcom1
https://website.informer.com/28betxt.com
https://lightroom.adobe.com/u/28betnhci
https://en.islcollective.com/portfolio/12908758#google_vignette
https://www.xosothantai.com/members/28betxtcom1.610537/
https://velog.io/@28betxtcom1/about
https://violet.vn/user/show/id/15270114
https://xaydunghanoimoi.net/members/27851-28betxtc.html
https://iplogger.com/2LQfF6
https://mez.ink/28betxtcom1
https://28betxtcom1.stck.me/profile
https://notionpress.com/author/1512194
https://www.edna.cz/uzivatele/28betxtcom/
https://digiphoto.techbang.com/users/28betxtcom1
https://leakedmodels.com/forum/members/28betxtcom.710476/#about
https://freeicons.io/profile/923642
https://maychetao.com/members/21229-28betxtc.html
https://onlinesequencer.net/members/269557
https://inkbunny.net/28betxtcom1
https://www.japaaan.com/user/77823
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.28bet2
https://code.antopie.org/28betxtcom1
https://beatsaver.com/playlists/1187220
https://apptuts.bio/28betxtcom-260922
https://participacion.cabildofuer.es/profiles/28betxtcom/timeline?locale=en
https://forums.maxperformanceinc.com/forums/member.php?u=247315
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=302082
https://acomics.ru/-28betxtcom1
https://www.criminalelement.com/members/28betxtcom1/profile/
https://hanson.net/users/28betxtcom
https://writexo.com/share/9fac264e036c
https://pad.codefor.fr/s/jne-E70zOi
https://pad.degrowth.net/s/AoaN5iVK8
https://forum.skullgirlsmobile.com/members/28betxtcom1.217500/#about
https://jobs.landscapeindustrycareers.org/profiles/8199460-nha-cai-28bet
https://phatwalletforums.com/user/28betxtcom
https://idol.st/user/167969/28betxtcom1/
https://www.bmwpower.lv/user.php?u=28betxtcom1
https://jobs.windomnews.com/profiles/8199463-nha-cai-28bet
https://www.givey.com/28betxtcom1
https://zerosuicidetraining.edc.org/user/profile.php?id=562148
https://www.hobowars.com/game/game.php?sr=0&cmd=player&ID=2929837
https://jobs.westerncity.com/profiles/8199465-nha-cai-28bet
https://hedgedoc.envs.net/s/iX89WWWoF
https://dev.muvizu.com/Profile/28betxtcom1/Latest
https://hedgedoc.logilab.fr/s/PuzHSsVzw
https://buckeyescoop.com/community/members/28betxtcom.63050/#about
https://toirscript.com/user/28betxtcom1
https://forum.pabbly.com/members/28betxtcom1.114155/#about
https://forum.aigato.vn/user/28betxtcom1
https://www.skool.com/@nha-cai-haitambet-1044
https://learningapps.org/watch?v=peuv0ge7526
https://www.invelos.com/UserProfile.aspx?alias=28betxtcom1
https://www.video-bookmark.com/user/28betxtcom1
https://kktix.com/user/8698586
https://poipiku.com/13520373/
https://www.rwaq.org/users/danbuithi603-20260427050602
https://www.fitday.com/fitness/forums/members/28betxtcom1.html
https://www.fundable.com/nha-cai-28bet-19
https://www.grepmed.com/28betxtcom1
https://classificados.acheiusa.com/profile/RXdNMFA3SC9CVThPRWxWUTJSODNtR2NUWTBQNGVxR1JDWFZsMVRYOGxmMD0=
https://espritgames.com/members/50897121/
https://cgmood.com/nhacai-28bet
https://www.haikudeck.com/presentations/nhci.28bet.4
https://pads.zapf.in/s/G0uwN3tySP
https://md.chaosdorf.de/s/1OHUhNSNIe
https://md.un-hack-bar.de/s/qweGsotbpa
https://hi-fi-forum.net/profile/1146759
https://secondstreet.ru/profile/28betxtcom1/
https://scenarch.com/userpages/34201
https://undrtone.com/28betxtcom1
https://marshallyin.com/members/28betxtcom1/
https://www.atozed.com/forums/user-78703.html
https://gravesales.com/author/28betxtcom1/
https://hukukevi.net/user/28betxtcom1
https://belgaumonline.com/profile/28betxtcom/
https://savelist.co/my-lists/users/28betxtcom1
https://zzb.bz/LgqylH
https://www.themeqx.com/forums/users/28betxtcom1/
https://www.udrpsearch.com/user/28betxtcom1
http://newdigital-world.com/members/28betxtcom1.html
https://www.xen-factory.com/index.php?members/28betxtcom1.156461/#about
https://forums.servethehome.com/index.php?members/28betxtcom1.240425/#about
https://www.blackhatprotools.info/member.php?288402-28betxtcom1
https://activepages.com.au/profile/28betxtcom1
https://snippet.host/qxkqvf
https://tudomuaban.com/chi-tiet-rao-vat/2888932/28betxtcom1.html
https://phijkchu.com/a/28betxtcom1/video-channels
https://lifeinsys.com/user/28betxtcom1
https://kaeuchi.jp/forums/users/28betxtcom1/
https://hedgedoc.stusta.de/s/VMnZD1LjK
https://protospielsouth.com/user/131227
https://theafricavoice.com/profile/28betxtcom1
https://support.bitspower.com/support/user/28betxtcom1
https://hackmd.okfn.de/s/SySwd9jabl
https://manylink.co/@28betxtcom1
https://www.akaqa.com/question/q19192675165-28betxtcom
https://copynotes.be/shift4me/forum/user-53087.html
https://civitai.com/user/28betxtcom1
https://hoo.be/28betxtcom
https://maxforlive.com/profile/user/28betxtcom1?tab=about
https://3dtoday.ru/blogs/28betxtcom1
https://mathlog.info/users/NqNsamK4ZlflxqXwwOgUEV1RkQ33
https://my.bio/28betxtcom1
https://community.cloudera.com/t5/user/viewprofilepage/user-id/151555
https://fora.babinet.cz/profile.php?section=essentials&id=124547
https://shhhnewcastleswingers.club/forums/users/28betxtcom/
https://connect.gt/user/28betxtcom
https://www.weddingbee.com/members/28betxtcom1/
https://kumu.io/28betxtcom1/28betxtcom#28betxtcom
https://www.sunlitcentrekenya.co.ke/author/28betxtcom1/
https://www.rcuniverse.com/forum/members/28betxtcom.html
https://www.huntingnet.com/forum/members/28betxtcom.html
https://vimeo.com/28betxtcom1
https://www.lingvolive.com/en-us/profile/dd4bcc47-4f8f-4429-98c8-2e7aee0a654a/translations
https://www.zubersoft.com/mobilesheets/forum/user-136028.html
https://www.mindomo.com/mindmap/8c64b961a70b467c95bdbe164e3c19ab
https://md.coredump.ch/s/Ysxe0wuDL
https://aprenderfotografia.online/usuarios/28betxtcom/profile/
https://hackmd.hub.yt/s/d3YVbdsKb
https://sciencemission.com/profile/28betxtcom1
https://www.wvhired.com/profiles/8200596-nha-cai-28bet
https://beteiligung.tengen.de/profile/28betxtcom1/
https://formulamasa.com/elearning/members/28betxtcom/?v=96b62e1dce57
https://chyoa.com/user/28betxtcom1
https://backloggd.com/u/28betxtcom1/
https://forums.alliedmods.net/member.php?u=476954
https://community.jmp.com/t5/user/viewprofilepage/user-id/97853
https://www.thesims3.com/myBlog.html?persona=28betxtcom1&showBlogMasterPopup=false
https://brain-market.com/u/28betxtcom
https://ikanakama.ink/users/341549
https://www.prosebox.net/book/108520/
https://forum.honorboundgame.com/user-510482.html
https://www.fw-follow.com/forum/topic/118675/28bet-
https://www.jk-green.com/forum/topic/112239/28bet-
https://www.navacool.com/forum/topic/401146/28bet-
https://www.driedsquidathome.com/forum/topic/144930/28bet-
https://www.nongkhaempolice.com/forum/topic/126149/28bet-
https://www.bestloveweddingstudio.com/forum/topic/84340/28bet-
https://hedgedoc.digillab.bangladhadha.com/load.php?note=ce194e27
https://community.bemeapps.com/user/28betxtcom1
https://forum.mbprinteddroids.com/member.php?action=profile&uid=635238
https://allmylinks.com/28betxtcom1
https://www.rueanmaihom.net/forum/topic/99584/28betxtcom
https://www.ttlxshipping.com/forum/topic/401105/28betxtcom
http://worldchampmambo.com/UserProfile/tabid/42/userId/454773/Default.aspx
https://www.rcmx.net/userinfo.php?uid=17038
https://eilo.org/user/28betxtcom
https://lqdoj.edu.vn/user/28betxtcom
https://paperjale.eus/user/28betxtcom
https://indiestorygeek.com/user/28betxtcom
https://www.bandlab.com/28betxtcom2
https://forum.issabel.org/u/28betxtcom
https://forum.issabel.org/u/28betxtcom
https://www.easyhits4u.com/profile.cgi?login=28betxtcom
https://doc.anagora.org/s/yBaiGDIgq
https://www.ekdarun.com/forum/topic/155578/28bet-
https://fanclove.jp/profile/ePBn4xvyJ4
https://www.d-ushop.com/forum/topic/131770/28bet-
https://lustyweb.live/members/28betxtcom1.121857/
https://findaspring.org/members/nhananh/
https://ketcau.com/member/101641-28betxtcom
https://vietcurrency.vn/members/28betxtcom.240032/#about
https://fengshuidirectory.com/dashboard/listings/28betxtcom/
https://pets4friends.com/profile-1581754
https://ioninja.com/forum/user/28betxtcom
https://linkmix.co/53875723
https://foriio.com/28betxtcom
https://blockstar.social/28betxtcom
https://toirscript.com/user/28betxtcom
https://desksnear.me/users/nha-cai-28bet-d052ad
https://recash.wpsoul.net/members/28betxtcom/profile/
https://www.betmma.tips/mma_handicapper.php?ID=183863
https://tuscl.net/member/887226
https://www.newgenstravel.com/forum/topic/43526/28bet-
https://www.pathumratjotun.com/forum/topic/179228/28bet-
https://www.thitrungruangclinic.com/forum/topic/126364/28bet-
https://forums.wincustomize.com/user/7663227/overview
teletype.link/28betxtcom1
https://www.buckeyescoop.com/users/0705c6a2-879c-47c3-ab56-a66ffe9f988b
https://aniworld.to/user/profil/28betxtcom
https://www.fitlynk.com/28betxtcom
https://www.scener.com/@28betxtcom
https://hostndobezi.com/28betxtcom
https://nilechronicles.com/profile/28betxtcom
https://armchairjournal.com/forums/users/nha-7/
https://cl.enrollbusiness.com/BusinessProfile/7787595/28betxtcom-El-Loa-Antofagasta
https://www.bonback.com/forum/topic/401716/28bet-
https://at.enrollbusiness.com/BusinessProfile/7787601/28betxtcom
https://justpaste.it/u/28betxtcom2
https://gorillasocialwork.com/user/28betxtcom
https://xmrbazaar.com/user/28betxtcom/
https://hindibookmark.com/user/28betxtcom
https://vnbit.org/members/28betxtcom.99549/#about
https://ticketme.io/fr/account/28betxtcom
https://topkif.nvinio.com/28betxtcom
https://gitflic.ru/user/28betxtcom
https://makeagif.com/user/28betxtcom
https://soundation.com/user/28betxtcom
https://adhocracy.plus/profile/28betxtcom/
https://www.cryptoispy.com/forums/users/28betxtcom/
https://www.tkaraoke.com/forums/account/28betxtcom/
https://foss.heptapod.net/28betxtcom2
https://triumph.srivenkateshwaraa.edu.in/profile/28betxtcom2
https://pebforum.com/members/28betxtcom.241446/
https://bbcovenant.guildlaunch.com/users/blog/6754082/?mode=view&gid=97523
https://joinentre.com/profile/28betxtcom1
https://hedgedoc.dezentrale.space/s/7LtzeQuuR
https://jobs.landscapeindustrycareers.org/profiles/8201043-nha-cai-28bet
https://tabelog.com/rvwr/28betxtcom1/
https://espritgames.com/members/50897121/?esc=site_com_tmenu&locale=en_US
https://jobs.motionographer.com/profiles/8201056-nha-cai-28bet
https://ofuse.me/28betxtcom1
https://safechat.com/u/nha.cai.28bet.626
https://hackmd.openmole.org/s/DUmD7kiPY
https://hedgedoc.eclair.ec-lyon.fr/s/-_28JOwIz
https://kitsu.app/users/1706508
https://naijamatta.com/28betxtcom1
https://www.yumpu.com/user/28betxtcom1
https://pad.koeln.ccc.de/s/9xB4YC2h_
https://www.xiuwushidai.com/home.php?mod=space&uid=2678084
https://jobs.host-panel.com/author/28betxtcom1/
https://www.blackhatprotools.info/member.php?288402-28betxtcom1
https://forums.planetdestiny.com/members/28betxtcom1.131006/
http://fort-raevskiy.ru/community/profile/28betxtcom1/
http://freestyler.ws/user/652541/28betxtcom1
https://mail.tudomuaban.com/chi-tiet-rao-vat/2888857/28betxtcom.html
https://nogu.org.uk/forum/profile/28betxtcom/
https://jobs.siliconflorist.com/employers/4128257-28betxtcom
https://aboutcasemanagerjobs.com/author/28betxtcom1/
https://www.animaljobsdirect.com/profiles/8200552-nha-cai-28bet
https://jobs.lajobsportal.org/profiles/8200553-nha-cai-28bet
https://www.instructorsnearme.com/author/28betxtcom1/
https://aboutnursernjobs.com/author/28betxtcom1/
https://www.sonorancareerlink.com/employers/4128258-28betxtcom1
https://aboutnursinghomejobs.com/author/28betxtcom1/
https://omiyou.com/28betxtcom1
https://md.coredump.ch/s/G0X7YXciJ
https://nyccharterschools.jobboard.io/employers/4128259-28bet
https://chaloke.com/forums/users/28betxtcom1/
https://aboutsnfjobs.com/author/28betxtcom1/
https://www.horticulturaljobs.com/employers/4128261-nha-cai-28bet
https://jobs.nefeshinternational.org/employers/4128262-nha-cai-28bet
https://jobs.tdwi.org/profiles/8200562-nha-cai-28bet
https://dialog.eslov.se/profiles/28betxtcom1/activity?locale=en
https://www.rcmx.net/userinfo.php?uid=17061
https://community.alexgyver.ru/members/28betxtcom1.174504/
http://iawbs.com/home.php?mod=space&uid=955985
https://ask.mallaky.com/?qa=user/28betxtcom1
https://pad.stuve.de/s/S3v4e_BDQ
https://participationcitoyenne.rillieuxlapape.fr/profiles/28betxtcom1/activity
https://forum.cnnr.fr/user/28betxtcom1
https://biiut.com/28betxtcom1
https://decidim.calafell.cat/profiles/28betxtcom1/activity
https://hi-fi-forum.net/profile/1146894
https://pad.fablab-siegen.de/s/kqTgq_5Qr8
https://participation.touraine.fr/profiles/28betxtcom/activity
http://hkeverton.com/forumnew/home.php?mod=space&uid=637402
https://pink88.cc/home.php?mod=space&uid=286036
http://app.gxbs.net/home.php?mod=space&uid=1792016
https://www.japaaan.com/user/77879
https://md.opensourceecology.de/s/efbhC2eRI
https://stepik.org/users/1253703440/profile
https://www.allmyusjobs.com/author/28betxtcom/
https://pad.geolab.space/s/h0FqG7fMR
https://participez.villeurbanne.fr/profiles/28betxtcom/activity
https://doc.anagora.org/s/DFoHU6fT4
https://careers.coloradopublichealth.org/profiles/8200862-nha-cai-28bet
https://git.entryrise.com/28betxtcom1
http://tkdlab.com/wiki/index.php?28betxtcom
https://themeqx.com/forums/users/28betxtcom2
https://pad.degrowth.net/s/Bm6aR5ZjW
https://boss.why3s.cc/boss/home.php?mod=space&uid=263197
https://partecipa.poliste.com/profiles/28betxtcom1/activity
https://protocol.ooo/en/users/28betxtcom-925d79d6-0c57-41f6-86b2-d82478e380d1
https://awan.pro/forum/user/167703/
https://participer.loire-atlantique.fr/profiles/28betxtcom/activity
https://www.youyooz.com/profile/28betxtcom
https://forum.hiv.plus/user/28betxtcom
https://graph.org/28BET–Trang-Chu-Chinh-Thuc-2026–Nap-Dau-100K-Nhan-200K-04-27
https://ben10club.org/user/28betxtcom
https://www.racerjobs.com/profiles/8200916-nha-cai-28bet
https://pad.karuka.tech/s/1gnRE7kgI
http://qa.doujiju.com/index.php?qa=user&qa_1=28betxtcom1
https://ac.db0.company/user/10699/28betxtcom/
https://www.northwestu.edu/?URL=https://28betxt.com
https://decidim.derechoaljuego.digital/profiles/28betxtcom/activity
https://fr.tripadvisor.ca/Profile/link28betxtcom
https://www.spoonflower.com/profiles/28betxtcom
https://hedgedoc.eclair.ec-lyon.fr.rexo.top/load.php?note=4cbe7c68
https://anotepad.com/note/read/5d78xxnm
https://fyers.in/community/member/Iynp9bjzKx
https://quicknote.io/df4849e0-41ec-11f1-996e-ad6cc28af922
https://www.bandsworksconcerts.info/index.php?28betxtcom
https://land-book.com/28betxtcom1
https://edabit.com/user/2jMaup85dPrChPS23
https://shootinfo.com/author/28betxtcom/?pt=ads
https://fairygodboss.com/users/profile/u_ZgrNEwm_/nha-cai-28bet
https://www.tripadvisor.com/Profile/link28betxtcom
http://techou.jp/index.php?28betxtcom
https://www.floodzonebrewery.com/profile/28betxtcom/profile
http://www.brenkoweb.com/user/89015/profile
https://vnav.vn/proxy.php?link=https://28betxt.com
https://gamelet.online/user/101945130157154537593@google/about
https://gesoten.com/profile/detail/12766390
https://www.nicovideo.jp/user/144057243
https://joy.link/28betxtcom1
https://swdteam.com/profile/28betxtcom
https://pumpyoursound.com/u/user/1613232
https://learningapps.org/display?v=pig4ciamj26
https://speakerdeck.com/28betxtcom
https://v.gd/I4O5Pl
https://bwinglive.lighthouseapp.com/users/1997630
https://infiniteabundance.mn.co/members/39458137
https://audio.com/28betxtcom
https://www.1001fonts.com/users/28betxtcom/
https://replit.com/@28betxtcom
https://longbets.org/user/28betxtcom/
https://urlscan.io/result/019dcd45-a84f-70fd-a081-a739398f53cf/
https://www.tripadvisor.dk/Profile/link28betxtcom
https://www.remotehub.com/28betxtcom
https://congdongmassage.com/members/28betxtcom.148428/#about
https://wibki.com/28betxtcom1
https://www.pdc.edu/?URL=https://28betxt.com
https://fic.decidim.barcelona/profiles/28betxtcom/activity
https://shorturl.at/NoLNU
https://slackcommunity.com/u/m82cjx/#/about
https://www.saltlakeladyrebels.com/profile/28betxtcom/profile
https://www.depechemode.cz/?URL=https://28betxt.com
https://www.producthunt.com/@link28betxtcom
https://www.tripadvisor.ie/Profile/link28betxtcom
https://www.zazzle.de/mbr/238205223397574586
https://www.tripadvisor.com.my/Profile/link28betxtcom
https://ngel.ink/28betxtcom
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:903180ED69EEB0C50A495FD2@AdobeID
https://allmyfaves.ca/28betxtcom1
https://chodilinh.com/members/28betxtcom1.302195/
https://kotob4all.com/profile/28betxtcom1
https://www.luzsantomauro.com/profile/danbuithi60357063/profile
https://nhattao.com/members/user6959242.6959242/
https://seomotionz.com/member.php?action=profile&uid=128958
https://hangoutshelp.net/user/28betxtcom1
https://start.me/p/BPGmzO/trang-bt-u
https://www.pintradingdb.com/forum/member.php?action=profile&uid=143955
https://www.adsfare.com/28betxtcom1
https://bloggalot.com/profile/28betxtcom1
https://amazingradio.us/profile/28betxtcom1
https://kooperation.winterthur.ch/profiles/nha_cai_28bet_2/activity
https://entre-vos-mains.alsace.eu/profiles/nha_cai_28bet_4/activity
https://unsplash.com/fr/@28betxtcom1
https://www.mateball.com/betxtcom128
https://nous.malakoff.fr/profiles/28betxtcom1/activity
https://rentry.co/t92u4ff8
https://28betxtcom1.stck.me/
https://www.huntingnet.com/forum/members/28betxtcom1.html
https://suzuri.jp/28betxtcom1
https://ta.quora.com/profile/Nh%C3%A0-C%C3%A1i-28bet
https://www.prodesigns.com/wordpress-themes/support/users/28betxtcom1
https://app.parler.com/28betxtcom1
https://rndirectors.com/author/28betxtcom1/
https://bookmarksurl.com/story7039739/28betxtcom1
https://m.wibki.com/28betxtcom1
https://indiestorygeek.com/user/28betxtcom1
https://urlz.fr/v7R2
https://codeandsupply.co/users/eXsTp4_thdIahQ
https://www.tacter.com/@28betxtcom1
https://editor.telescope.ac/blogs/28betxtcom1/0whhm1oticrqjyzhj3xooy
https://flipboard.com/@nhci28bet2026/28betxtcom1-9mkqsirgy
https://www.notariosyregistradores.com/web/forums/usuario/28betxtcom1/
https://www.codingame.com/profile/c685d8a45ba0fdef30fe1ce574694bbb2317427
https://morguefile.com/creative/28betxtcom1
https://www.clickasnap.com/profile/28betxtcom1
https://www.pexels.com/@nha-cai-28bet-2161189341/
https://makerworld.com/fr/@28betxtcom1
https://beatsaver.com/playlists/1187768
https://kjtr.grrr.jp/kjtr/?28betxtcom1
https://www.roton.com/forums/users/danbuithi603/
https://tinyurl.com/28betxtcom1
https://userstyles.world/user/28bet
https://www.proarti.fr/collect/project/28betxtcom1-0/0
https://www.watershedwellness.net/profile/danbuithi60371372/profile
What a stuff of un-ambiguity and preserveness of valuable know-how about unexpected emotions.
Appreciate the recommendation. Let me try it out.
Hello just wanted to give you a quick heads up. The text in your article seem to be running off the screen in Safari. I’m not sure if this is a formatting issue or something to do with browser compatibility but I thought I’d post to let you know. The style and design look great though! Hope you get the issue fixed soon. Cheers
Your comment is awaiting moderation.
https://www.facebook.com/ao887com/
https://www.youtube.com/@ao887com
https://x.com/ao887com
https://tooter.in/ao887com
https://wakelet.com/@ao887com
https://safechat.com/u/ao881.893
https://www.blogger.com/profile/15491782157466184318
https://www.mymeetbook.com/ao887com
https://www.pinterest.com/ao887com/
https://community.wongcw.com/ao887com
https://demo.wowonder.com/ao887com
https://500px.com/p/ao887com
https://magic.ly/ao887com
https://protocol.ooo/ja/users/ao88-9b032253-eb5b-41b4-8343-6c0743aa33a9
https://www.tumblr.com/ao887com
https://www.reddit.com/user/ao887com/
https://audiomack.com/ao887com
https://hackaday.io/ao887com
https://leetcode.com/u/ao887com/
https://swag.live/en/user/69ea0cdf281eb1247ea2f6f3
https://www.halaltrip.com/user/profile/341338/ao887com/
https://medibang.com/author/28186417/
https://opensea.io/ao887com
https://www.blockdit.com/ao887com
https://portfolium.com/ao887com
https://groups.google.com/g/ao887com
https://www.twitch.tv/ao887com/about
https://profile.hatena.ne.jp/ao887com/
https://issuu.com/ao887com
https://www.behance.net/ao887com
https://gravatar.com/ao887com
https://www.reverbnation.com/artist/ao887com
https://www.myminifactory.com/users/ao887com
https://www.investagrams.com/Profile/ao887com
https://gifyu.com/ao887com
https://www.chordie.com/forum/profile.php?id=2513800
https://www.longisland.com/profile/ao887com
https://www.walkscore.com/people/115653748839/ao88
https://topsitenet.com/profile/ao887com/1662436/
https://akniga.org/profile/1416839-ao88/
https://jobs.suncommunitynews.com/profiles/8189562-ao88
https://www.speedrun.com/users/ao887com
https://www.fanart-central.net/user/ao887com/profile
https://slides.com/ao887com
https://www.aicrowd.com/participants/ao887com
https://old.bitchute.com/channel/6tHw5GLZitrT/
https://pbase.com/ao887com/
https://hub.docker.com/u/ao887com
https://spiderum.com/nguoi-dung/ao887com
https://zaidap.com/thong-tin-ca-nhan-u107474.htm
https://www.gta5-mods.com/users/ao887com
https://heylink.me/ao887com/
https://pixabay.com/users/ao887com-55570495/
https://www.nicovideo.jp/user/144017233
https://www.jigsawplanet.com/ao887com
https://3dwarehouse.sketchup.com/by/ao887com
https://robertsspaceindustries.com/en/citizens/ao887com
https://bit.ly/m/ao887com
https://joy.link/ao887com
https://connect.garmin.com/app/profile/26c8df30-0ef0-4382-9da4-4848e479300f
https://b.hatena.ne.jp/ao887com/bookmark
https://www.chichi-pui.com/users/ao887com/
https://www.openrec.tv/user/ao887com/about
https://unityroom.com/users/ao887com
https://pxhere.com/en/photographer-me/4991962
https://teletype.in/@ao887com
https://www.checkli.com/ao887com
https://www.fuelly.com/driver/ao887com
https://www.nintendo-master.com/profil/ao887com
https://freeimage.host/ao887com
https://www.diigo.com/profile/ao887com
https://fontstruct.com/fontstructions/show/2870947/ao88-6
https://motion-gallery.net/users/957383
https://linkin.bio/ao887com
https://biomolecula.ru/authors/143222
https://talk.plesk.com/members/aocom.503370/#about
https://www.callupcontact.com/b/businessprofile/AO88/10064475
https://blender.community/ao886/
https://doselect.com/@e675672b1c459d800f42e88f2
https://sciter.com/forums/users/ao887com/
https://matkafasi.com/user/ao887com
https://allmyfaves.com/ao887com
https://www.notebook.ai/@ao887com
https://www.abclinuxu.cz/lide/ao887com
https://muare.vn/shop/mike-ortega/903003
https://doodleordie.com/profile/ao887com
https://musikersuche.musicstore.de/profil/ao887com/
https://www.intensedebate.com/people/ao887comhttps://www.intensedebate.com/people/ao887com
https://forum.dmec.vn/index.php?members/ao887com.188282/
https://igli.me/ao887com
https://freestyler.ws/user/651497/ao887com
http://delphi.larsbo.org/user/ao887com
https://www.aseeralkotb.com/en/profiles/ao887com
https://timdaily.vn/members/ao887com.134470/#about
https://app.readthedocs.org/profiles/mikeortega276@gmail.com/
https://www.dibiz.com/mikeortega276
https://iszene.com/user-348269.html
https://www.theyeshivaworld.com/coffeeroom/users/ao887com
https://desksnear.me/users/ao88-3f52e6
https://www.itchyforum.com/en/member.php?388589-ao887com
https://www.roton.com/forums/users/mikeortega276/
https://able2know.org/user/ao887com/
https://eternagame.org/players/619448
http://www.biblesupport.com/user/832552-ao887com/
https://golosknig.com/profile/ao887com/
https://www.anibookmark.com/user/ao887com.html
https://www.inventoridigiochi.it/membri/ao887com/profile/
https://forum.m5stack.com/user/ao887com
https://imageevent.com/ao887com/ao887com
https://www.bitchute.com/channel/6tHw5GLZitrT
https://bandori.party/user/807619/ao887com/
https://community.m5stack.com/user/ao887com
https://schoolido.lu/user/ao887com/
https://awan.pro/forum/user/167054/
https://fortunetelleroracle.com/profile/ao887com
https://fabble.cc/ao887com
https://affariat.com/user/profile/179634
https://community.cisco.com/t5/user/viewprofilepage/user-id/2069273
https://kr.pinterest.com/ao887com/
https://pt.gravatar.com/ao887com
https://th.gravatar.com/ao887com
https://www.sythe.org/members/ao887com.2041302/
https://f319.com/members/ao887com.1099335/
https://about.me/ao887com
https://booklog.jp/users/ao887com/profile
https://www.equinenow.com/farm/ao88-sn-chi-c-cc-trc-tuyn-nng-ng-ko-v-game-cun-ht.htm
https://wefunder.com/ao887com
https://potofu.me/ao887com
https://transfur.com/Users/ao887com
https://xtremepape.rs/members/ao887com.667293/#about
https://github.com/ao887com
https://myanimelist.net/profile/ao887com
https://qna.habr.com/user/ao887com
https://beacons.ai/ao887com
https://www.xosothantai.com/members/ao887com.610033/
https://velog.io/@ao887com/about
https://website.informer.com/ao88-7.com
https://lightroom.adobe.com/u/ao887com
https://en.islcollective.com/portfolio/12906963
https://violet.vn/user/show/id/15269307
https://iplogger.org/vn/logger/4mER5xMyRv0y/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3947470
https://mez.ink/ao887com
https://ao887com.stck.me/profile
https://notionpress.com/author/1510675
https://www.edna.cz/uzivatele/ao887com/
https://i.techbang.com/users/ao887com
https://leakedmodels.com/forum/members/ao887com.709842/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1067832
https://onlinesequencer.net/forum/user-268898.html
https://inkbunny.net/ao887com
https://www.japaaan.com/user/77462/
https://spinninrecords.com/profile/ao887com
https://www.launchgood.com/user/newprofile#!/user-profile/profile/ao88
https://code.antopie.org/ao887com
https://beatsaver.com/playlists/1184258
https://apptuts.bio/ao887com-260482
https://dialog.eslov.se/profiles/ao887com/activity
https://www.storenvy.com/ao887com
https://participacion.cabildofuer.es/profiles/ao887com/activity
https://forums.maxperformanceinc.com/forums/member.php?u=246981
https://egl.circlly.com/users/ao887com
https://goodandbadpeople.com/ao887com
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=301647
https://www.sciencebee.com.bd/qna/user/ao887com
https://acomics.ru/-ao887com
https://www.criminalelement.com/members/ao887com/profile/
https://hanson.net/my-account/dashboard
https://writexo.com/share/cafb3ab902f4
https://expatguidekorea.com/profile/ao887com
https://www.laundrynation.com/community/profile/ao887com/
https://www.heavyironjobs.com/profiles/8190480-ao88
https://pad.degrowth.net/s/R9RFEL5vV
http://fort-raevskiy.ru/community/profile/ao887com/
https://forum.skullgirlsmobile.com/members/ao887com.216596/
https://jobs.landscapeindustrycareers.org/profiles/8190508-ao88
https://phatwalletforums.com/user/ao887com
https://song.link/ao887com
https://www.wanttoknow.nl/author/ao887com/
https://idol.st/user/166547/ao887com/
https://www.valinor.com.br/forum/usuario/ao887com.145448/
https://tulieu.violet.vn/user/show/id/15269307
https://www.bmwpower.lv/user.php?u=ao887com
https://gockhuat.net/member.php?u=437209
https://jobs.windomnews.com/profiles/8190624-ao88
https://hoaxbuster.com/redacteur/ao887com
https://www.givey.com/ao887com
https://talkmarkets.com/profile/ao887com
https://zerosuicidetraining.edc.org/user/profile.php?id=561452
https://www.telix.pl/forums/users/Mike-Ortega/
https://beteiligung.amt-huettener-berge.de/profile/ao887com/
https://joinentre.com/profile/ao887com
https://jobs.westerncity.com/profiles/8190742-ao88
https://www.thetriumphforum.com/members/ao887com.63310/
https://gamblingtherapy.org/forum/users/ao887com/
https://l2top.co/forum/members/ao887com.174167/
http://www.askmap.net/location/7798012/vietnam/ao88
https://youtopiaproject.com/author/ao887com/
https://www.myget.org/users/ao887com
https://chaloke.com/forums/users/ao887com/
https://app.brancher.ai/user/KrFxGeIHRpcG
https://justpaste.me/GP9Y1
https://www.empregosaude.pt/en/author/ao887com/
https://confengine.com/user/ao887com
https://mygamedb.com/profile/ao887com
https://buckeyescoop.com/community/members/ao887com.62843/#about
https://www.mateball.com/ao887com
https://web-tourist.net/members/ao887com.53250/#about
https://toirscript.com/user/ao887com
https://forum.pabbly.com/members/ao887com.113545/#about
http://forum.cncprovn.com/members/424985-ao887com
https://ncnews.co/profile/ao887com
https://dreevoo.com/profile_info.php?pid=1542709
https://forum.aigato.vn/user/ao887com
https://amaz0ns.com/forums/users/ao887com/
https://rapidapi.com/user/ao887com
https://www.skool.com/@trang-chu-win-8107
https://learningapps.org/watch?v=pn97h6t6526
https://coub.com/ao887com
https://www.giveawayoftheday.com/forums/profile/1818171?updated=true
https://tealfeed.com/ao887com
https://www.invelos.com/UserProfile.aspx?alias=ao887com
https://www.video-bookmark.com/bookmark/7113169/ao88/
https://wibki.com/ao887com
https://gitlab.vuhdo.io/ao887com
https://www.11secondclub.com/users/profile/1713539
https://s.id/ao887com
https://kktix.com/user/8689365
https://www.passes.com/ao887com
https://uiverse.io/profile/mike_9498
https://www.rwaq.org/users/ao887com
https://cofacts.tw/user/ao887com
https://www.fitday.com/fitness/forums/members/ao887com.html
https://vcook.jp/users/88282
https://www.grepmed.com/ao887com
https://classificados.acheiusa.com/profile/bTY5OXNZYUNIWHFyejluYjk2eW82aHcrbnl0aDNGZTdaUEcvQ3d3bXd6OD0=
https://espritgames.com/members/50857002/
https://cgmood.com/ao887com
https://www.haikudeck.com/presentations/Nhci.AO88
https://www.efunda.com/members/people/show_people.cfm?Usr=ao887com
https://diit.cz/profil/niq3dwfxq4/ao887com
https://backloggery.com/ao887com
https://raovat.nhadat.vn/members/ao887com-307261.html
https://www.moshpyt.com/user/ao887com
https://www.koi-s.id/member.php?332412-ao887com
https://que.u.nosv.org/profile?user=ao887com
https://hi-fi-forum.net/profile/1146201
https://secondstreet.ru/profile/ao887com/
https://forum.fakeidvendors.com/user/ao887com
https://scenarch.com/userpages/33918
https://undrtone.com/ao887com
https://marshallyin.com/members/ao887com/
https://us.enrollbusiness.com/BusinessProfile/7786103/AO88
https://www.atozed.com/forums/user-78325.html
https://gravesales.com/author/ao887com/
https://searchengines.bg/members/ao887com.26408/#about
https://www.soshified.com/forums/user/666056-ao887com/
https://hukukevi.net/user/ao887com
https://savelist.co/my-lists/users/ao887com
https://www.montessorijobsuk.co.uk/author/ao887com/
https://www.apsense.com/user/ao887com
https://zzb.bz/hpSVf4
https://draft.blogger.com/profile/15491782157466184318
https://hack.allmende.io/s/ONmWOGM8Cv
https://pad.codefor.fr/s/LUCJ-qRsUK
https://hackmd.hub.yt/s/PB8kGQM2g
https://www.themeqx.com/forums/users/ao887com/
https://www.udrpsearch.com/user/ao887com
https://www.inseparabile.it/forum/member.php?u=47889
http://newdigital-world.com/members/ao887com.html
https://www.xen-factory.com/index.php?members/ao887com.155842/#about
https://cointr.ee/ao887com
https://forums.servethehome.com/index.php?members/ao887com.239943/#about
https://jali.me/ao887com
https://www.blackhatprotools.info/member.php?288056-ao887com
https://activepages.com.au/profile/ao887com
https://snippet.host/xcfqes
https://tudomuaban.com/chi-tiet-rao-vat/2887388/ao88–san-choi-ca-cuoc-truc-tuyen-nang-dong-keo-va-game-cuon-hut.html
https://phijkchu.com/a/ao887com/video-channels
https://lifeinsys.com/user/ao887com
https://kaeuchi.jp/forums/users/ao887com/
https://www.claimajob.com/profiles/8192933-ao88
https://protospielsouth.com/user/130794
https://theafricavoice.com/profile/ao887com
http://palangshim.com/space-uid-5114485.html
https://www.africangenesis-101.org/profile/ao887com/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:1B9E812E69EA8ED80A495E95@AdobeID
https://vi.gravatar.com/ao887com
https://www.collcard.com/ao887com
https://www.mixcloud.com/ao887com/
https://www.designspiration.com/ao887com/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=194944
https://hub.vroid.com/en/users/125671148
https://myanimeshelf.com/shelf/ao887com
https://www.brownbook.net/business/55042835/ao88
https://www.babelcube.com/user/nha-cai-ao88-1
https://app.talkshoe.com/user/ao887com
https://m.wibki.com/ao887com
https://www.pageorama.com/?p=ao887com
https://bandsworksconcerts.info/index.php?ao887com
https://bbs.mikocon.com/home.php?mod=space&uid=290768
https://www.mikocon.com/home.php?mod=space&uid=290768
https://jerseyboysblog.com/forum/member.php?action=profile&uid=92248
https://manylink.co/@ao887com
https://seomotionz.com/member.php?action=profile&uid=128637
https://anyflip.com/homepage/voakn#About
https://www.akaqa.com/question/q19192674486-Ao88
https://londonchinese.com/home.php?mod=space&uid=620949&do=profile
https://copynotes.be/shift4me/forum/user-52874.html
https://scholar.google.com/citations?hl=en&user=xMQLPxcAAAAJ
https://tabelog.com/rvwr/ao887com/prof/
https://prosinrefgi.wixsite.com/pmbpf/profile/ao887com/profile
https://coolors.co/u/ao88
https://www.beamng.com/members/ao887com.789964/
https://civitai.com/user/ao887com
https://www.spigotmc.org/members/ao887com.2524858/
https://camp-fire.jp/profile/ao887com
https://feyenoord.supporters.nl/profiel/149111/ao887com
https://www.pearltrees.com/ao887com/item793107626
https://gesoten.com/profile/detail/12758061
https://hashnode.com/@ao887com
https://hoo.be/ao887com
https://nhattao.com/members/user6957808.6957808/
https://3dtoday.ru/blogs/ao887com
https://opencollective.com/ao887com
https://pinshape.com/users/8955494-ao887com?tab=designs
https://morguefile.com/creative/ao887com
https://edabit.com/user/Gx3vSNtjsZ7LR9RGs
https://mathlog.info/users/c1VqOIvSlCOsRBlq8mf9XStGmER2
https://securityheaders.com/?q=https://ao88-7.com/
https://my.bio/ao887com
https://community.cloudera.com/t5/user/viewprofilepage/user-id/151371
https://cybermos.ru/user/251089/?id=251089
https://sfx.thelazy.net/users/u/ao887com/
https://mikseri.net/user/ao887com
https://app.daily.dev/ao887com
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=260098
https://www.skypixel.com/users/djiuser-z5tuivppeisp
https://webanketa.com/forms/6mvk4dhr64qk2d1mc4t3csb2/
https://www.pdc.edu/?URL=https://ao88-7.com/
https://ask.mallaky.com/?qa=user/ao887com
https://www.clashfarmer.com/forum/member.php?action=profile&uid=80206
https://www.depechemode.cz/?URL=https://ao88-7.com/
https://sub4sub.net/forums/users/ao887com/
https://www.slmath.org/people/105722
https://userstyles.world/user/ao887com
https://goo.by/YQFZuL
https://amazingradio.com/profile/ao887com
https://bresdel.com/ao887comm
https://fora.babinet.cz/profile.php?section=personal&id=124293
https://www.shippingexplorer.net/en/user/ao887com/280888
https://pictureinbottle.com/r/88hyef1l
https://forum.epicbrowser.com/profile.php?section=personal&id=152759
http://www.dungdong.com/home.php?mod=space&uid=3367857&do=profile
https://www.squadskates.com/profile/mikeortega27619656/profile
https://shhhnewcastleswingers.club/forums/users/ao887com/
https://forums.qhimm.com/index.php?action=profile;area=summary;u=91017
https://electroswingthing.com/profile/ao887com/
https://connect.gt/user/ao887com
https://forum.tkool.jp/index.php?members/ao887com.106266/#about
https://www.weddingbee.com/members/ao887com/
https://ao887com.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/ao887com/activity
https://www.rcuniverse.com/forum/members/ao887com.html
https://www.socialbookmarkssite.com/bookmark/6241797/ao887com/
https://www.hogwartsishere.com/1836238/
https://vimeo.com/ao887com
https://uccle.monopinion.belgium.be/profiles/ao887com/activity
https://gitlab.com/ao887com
https://www.symbaloo.com/mix/ao887com
https://www.bricklink.com/aboutMe.asp?u=ao887com
https://www.lingvolive.com/en-us/profile/ea0b3211-ab0f-4146-ab51-ef4816329adf/translations
https://zealy.io/cw/ao887com1/questboard
https://www.france-ioi.org/user/perso.php?sLogin=ao887com
https://mt2.org/uyeler/ao887com.39373/#about
https://www.trackyserver.com/profile/247335
https://ixawiki.com/link.php?url=https://ao88-7.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=143772
https://www.zubersoft.com/mobilesheets/forum/user-135743.html
https://hackmd.openmole.org/s/osQ1hXiMx
https://md.chaosdorf.de/s/UTy1Pu4Kzr
https://md.openbikesensor.org/s/qhSWH5R-Pa
https://doc.adminforge.de/s/y4YdLnhA5-
https://www.plotterusati.it/user/ao887com
https://tutorialslink.com/member/MikeOrtega/98985
https://www.buzzbii.com/ao887com
http://www.activewin.com/user.asp?Action=Read&UserIndex=4838656&redir=&redirname=Forums
http://www.jbt4.com/home.php?mod=space&uid=8671000
https://www.vid419.com/home.php?mod=space&uid=3486957
https://forum.ct8.pl/member.php?action=profile&uid=122296
https://devfolio.co/@ao887com/readme-md
https://ao887com.shopinfo.jp/posts/58769539
https://linqto.me/n/ao887com
https://www.mindomo.com/mindmap/ao88-b97ab100330b45f582e7d4ef4437efa6
https://www.okaywan.com/home.php?mod=space&uid=797861
https://www.goodolcomics.com/blog/profile/ao887com/
https://www.swap-bot.com/user:ao887com
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=391806
http://techou.jp/index.php?ao887com
https://epiphonetalk.com/members/ao887com.97621/#about
https://forums.megalith-games.com/member.php?action=profile&uid=1451621
http://tkdlab.com/wiki/index.php?cmd=read&page=ao887com&refer=ao887com
https://www.managementpedia.com/members/ao887com.1120753/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=635037
https://volleypedia.org/index.php?qa=user&qa_1=ao887com
http://pcsq28.com/home.php?mod=space&uid=1969561
https://bbs.airav.cc/home.php?mod=space&uid=4583673
https://partecipa.poliste.com/profiles/ao887com/activity
https://hker2uk.com/home.php?mod=space&uid=5499433
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=496173
https://hcgdietinfo.com/hcgdietforums/members/ao887com/
https://aprenderfotografia.online/usuarios/ao887com/profile/
https://pads.zapf.in/s/_6tk32p33f
http://galeria.farvista.net/member.php?action=showprofile&user_id=77035
https://tilengine.org/forum/member.php?action=profile&uid=164332
https://bbs.darkml.net/home.php?mod=space&uid=150551
https://www.play56.net/home.php?mod=space&uid=6150048
https://md.swk-web.com/s/BYUf_lTRo
https://hedgedoc.dezentrale.space/s/ZXsQFkQWZ
https://ar.gravatar.com/ao887com
https://odesli.co/wbdsqjtrrks50
https://wandb.ai/profile/ao887com
https://divisionmidway.org/jobs/author/ao887com/
https://bbcovenant.guildlaunch.com/users/blog/6753774/
https://youbiz.com/profile/ao887com/
https://www.wowonder.xyz/ao887com
https://sciencemission.com/profile/ao887com
http://jobboard.piasd.org/author/ao887com/
https://www.wvhired.com/profiles/8194663-ao88
https://kenhrao.com/members/ao887com.121464/
http://jobs.emiogp.com/author/ao887com/
https://forumketoan.com/members/ao887com.44233/#about
https://onlinevetjobs.com/author/ao887com/
https://v.gd/aS7xrM
https://gl.gta5-mods.com/users/ao887com
http://www.webclap.com/php/jump.php?url=https://ao88-7.com/
https://xoops.ec-cube.net/userinfo.php?uid=348887
http://www.wmhelp.cz/html/modules.php?name=Forums&file=profile&mode=viewprofile&u=601693
https://formulamasa.com/elearning/members/ao887com/?v=96b62e1dce57
http://bbs.sdhuifa.com/home.php?mod=space&uid=1110804
https://quangcaoso.vn/ao887com
https://tawk.to/f78df26751a5064c40337f22987ec27f39ef9049
https://forum.flashphoner.com/members/ao887com.46438/about
https://www.royalroad.com/profile/960553
https://backloggd.com/u/ao887com/
https://kenhsinhvien.vn/m/ao887com.1167636/#about
https://form.jotform.com/261142235094450
https://forums.alliedmods.net/member.php?u=476730
https://community.jmp.com/t5/user/viewprofilepage/user-id/97671
https://digiex.net/members/ao887com.145035/
https://ru.myanimeshelf.com/profile/ao887com
https://smallseo.tools/website-checker/ao88-7.com
https://bwinglive.lighthouseapp.com/users/1997548
https://rush1989.rash.jp/pukiwiki/index.php?ao887com
https://www.stylevore.com/user/ao887com
https://bio.site/ao887com
https://viblo.asia/u/ao887com/contact
https://wikimapia.org/external_link?url=https://ao88-7.com/
https://www.thesims3.com/myBlog.html?persona=ao887com
https://telegra.ph/AO88-04-25
https://runtrip.jp/users/774788
https://campsite.bio/ao887com
https://hype4.academy/profile/ao887com
https://reactormag.com/members/ao887com/profile
https://brain-market.com/u/ao887com
https://ikanakama.ink/users/341502
https://www.prosebox.net/book/108396/
https://ticketme.io/account/ao887com
https://task.tw/users/TGZXMEC/freelancer
https://www.aipictors.com/en/users/ao887com
https://log.concept2.com/profile/2926395
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://ao88-7.com/
http://forum.orangepi.org/home.php?mod=space&uid=6417946
https://redirect.camfrog.com/redirect/?url=https://ao88-7.com/
https://beteiligung.hafencity.com/profile/ao887com/
https://adhocracy.plus/profile/ao887com/
https://www.hobowars.com/game/linker.php?url=https://ao88-7.com/
https://beteiligung.stadtlindau.de/profile/ao887com/
https://www.fw-follow.com/forum/topic/118130/ao88
https://www.jk-green.com/forum/topic/111811/ao88
https://www.navacool.com/forum/topic/399365/ao88
https://www.bonback.com/forum/topic/399370/ao88
https://www.driedsquidathome.com/forum/topic/144335/ao88
https://www.nongkhaempolice.com/forum/topic/125420/ao88
https://www.bestloveweddingstudio.com/forum/topic/83982/ao88
https://www.natthadon-sanengineering.com/forum/topic/104715/ao88
https://www.rueanmaihom.net/forum/topic/99249/ao88
https://www.ttlxshipping.com/forum/topic/399417/ao88
http://forum.modulebazaar.com/forums/user/ao887com/
https://user.linkdata.org/user/AOtamtam/work
https://beteiligung.tengen.de/profile/ao887com/
https://calaos.fr/forum/member.php?action=profile&uid=20026
https://forum.hkcinema.ru/profile.php?section=about&id=73676
https://www.rcmx.net/userinfo.php?uid=16980
https://www.pathumratjotun.com/forum/topic/178754/ao88
https://maychetao.com/members/21220-ao887com.html
https://diendan.cuabenhvien.com/members/19802-ao887com.html
https://forum.web-z.net/profile.php?userid=9903
https://usabbs.org/home.php?mod=space&uid=87715
https://paperjale.eus/user/ao887com
http://byltz.com/home.php?mod=space&uid=481698
https://indiestorygeek.com/user/ao887com
https://www.bandlab.com/ao887com
https://diigo.com/012ftt2
https://www.livelib.ru/reader/mikeortega276
https://forum.issabel.org/u/ao887com
https://www.siye.co.uk/siye/viewuser.php?uid=250160
https://ie.enrollbusiness.com/BusinessProfile/7786103/AO88-Bates-City-MO-64011
https://www.casualgamerevolution.com/user/ao887com
https://raredirectory.com/author/ao887com-49697/
https://www.iglinks.io/mikeortega276-zxy?preview=true
https://www.keepandshare.com/discuss2/46366/ao88
http://bbs.medicalforum.cn/home.php?mod=space&uid=2241916
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ao88-7.com/
https://giaoan.violet.vn/user/show/id/15269307
https://anh135689999.violet.vn/user/show/id/15269307
https://profiles.delphiforums.com/n/pfx/profile.aspx?webtag=dfpprofile000&userId=1891284022
https://hu.gta5-mods.com/users/ao887com
https://uk.gta5-mods.com/users/ao887com
https://sl.gta5-mods.com/users/ao887com
https://www.easyhits4u.com/profile.cgi?login=ao887com&view_as=1
https://at.pinterest.com/ao887com/
https://in.pinterest.com/ao887com/
https://doc.anagora.org/s/38NEmHzly
https://album.link/ao887com
https://artist.link/ao887com
https://pods.link/ao887com
https://mylink.page/ao887com
https://playlist.link/ao887com
https://portfolium.com.au/mikeortega276
https://mail.londonchinese.com/home.php?mod=space&uid=620949&do=profile
https://buyandsellhair.com/author/ao887com/
https://www.bidhub.com/profiles/profile/21452
https://baigiang.violet.vn/user/show/id/15269307
http://www.muzikspace.com/profiledetails.aspx?profileid=136339
https://forums.offworldgame.com/user/7662776
https://www.ekdarun.com/forum/topic/155154/ao88
https://fanclove.jp/profile/vYJP4bvdJ0
https://truckymods.io/user/488493
https://substack.com/@ao887com
http://forum.vodobox.com/profile.php?id=69618
https://forums.sinsofasolarempire.com/user/7662776
https://forums.stardock.net/user/7662776
https://forum.findukhosting.com/index.php?action=profile;u=75564
https://www.nissanpatrol.com.au/forums/member.php?197133-ao887com
https://www.expat.com/forum/profile.php?id=3957002&lang=en
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=228266
https://www.dokkan-battle.fr/forums/users/ao887com/
https://www.d-ushop.com/forum/topic/130965/ao88
https://www.fanfiction.net/u/16912978/
https://www.horticulturaljobs.com/employers/4126969-ao88
https://jobs.siliconflorist.com/employers/4126978-ao88
https://jobs.nefeshinternational.org/employers/4126984-ao88
https://aboutcasemanagerjobs.com/author/ao887com/
https://buyandsellhair.com/author/ao887com/
https://colorswall.com/users/33110
https://lustyweb.live/members/ao887com.121497/#about
https://whyp.it/users/142824/ao887com
https://6giay.vn/members/ao887com.102451/#about
https://findaspring.org/members/ao887com/
https://careers.coloradopublichealth.org/profiles/8197462-nha-cai-ao88
https://propeller.hu/tagok/ao887com/adatlap
https://promosimple.com/ps/4885e/ao88-s-n-ch-i-c-c-c-tr-c-tuy-n-n-ng-ng-k-o-v-game-cu-n-h-t
https://dienbd.violet.vn/user/show/id/15269307
https://memmai.com/index.php?members/ao887com.42109/#about
https://chothai24h.com/members/30568-ao887com.html
https://kttm.club/members/ao887com.4999/#about
https://vn-zom.com/members/ao887com.5816/
https://www.techrum.vn/members/ao887com.266304/#about
https://vietcurrency.vn/members/ao887com.239925/#about
https://vnbit.org/members/ao887com.99027/#about
https://www.cake.me/me/ao887com
https://blog.apaonline.org/author/ao887com/
https://boss.why3s.cc/boss/home.php?mod=space&uid=263025
https://community.goldposter.com/members/ao887com/profile/
https://fengshuidirectory.com/dashboard/listings/ao887com/
https://joy.bio/ao887com
https://joyrulez.com/ao887com
https://pets4friends.com/profile-1581580
https://staroetv.su/go?https://ao88-7.com/
https://www.ixawiki.com/link.php?url=https://ao88-7.com/
https://www.shinobi.jp/etc/goto.html?https://ao88-7.com/
https://decide.enguera.es/profiles/AO88/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345917
https://axe.rs/forum/members/ao887com.13427083/#about
https://co-roma.openheritage.eu/profiles/ao887com/activity
https://postr.yruz.one/profile/ao887com
https://openlibrary.org/people/ao887com
https://www.bookingblog.com/forum/users/aocom/
https://www.motiondesignawards.com/profile/20867
https://chodaumoi247.com/members/ao887com.51076/#about
https://aiti.edu.vn/members/ao887com.44171/
https://xaydunghanoimoi.net/members/27843-ao887com.html
https://www.gabitos.com/catalunyauniversal/template.php?nm=1777138777
https://knetwork.capital.bg/ao887com
https://www.foriio.com/ao887com
https://www.project1999.com/forums/member.php?u=334080
https://pad.stuve.de/s/SNk3SAcqv
https://pad.libreon.fr/s/BxIVo0JLN
https://www.are.na/nha-cai-ao88-7rgx9zrwghy/ao88-obgqctcmdku
https://maiotaku.com/p/ao887com/info
https://theexplorers.com/user?id=d8e7fd09-793c-4faa-b988-0dd8fce437fe
https://md.rappet.xyz/s/sjPL-yuSD7
https://www.blurb.com/user/ao887com?profile_preview=true
https://engage.aiaa.org/profile?UserKey=c5953b3e-77dc-4770-a72f-019dc5bbe45b
https://wall.page/kFifUt
https://participa.aytojaen.es/profiles/ao887com/activity
https://bsky.app/profile/ao887com.bsky.social
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=159146_fd7ro2a8
https://www.ad-links.org/AO88_372920.html
https://www.beegdirectory.com/AO88-%E2%80%93-S%C3%A2n-Ch%C6%A1i-C%C3%A1-C%C6%B0%E1%BB%A3c-Tr%E1%BB%B1c-Tuy%E1%BA%BFn-N%C4%83ng-%C4%90%E1%BB%99ng-K%C3%A8o-V%C3%A0-Game-Cu%E1%BB%91n-H%C3%BAt_491879.html
https://www.aquarius-dir.com/AO88_517611.html
https://www.apeopledirectory.com/AO88-%E2%80%93-S%C3%A2n-Ch%C6%A1i-C%C3%A1-C%C6%B0%E1%BB%A3c-Tr%E1%BB%B1c-Tuy%E1%BA%BFn-N%C4%83ng-%C4%90%E1%BB%99ng-K%C3%A8o-V%C3%A0-Game-Cu%E1%BB%91n-H%C3%BAt_416341.html
https://www.bedirectory.com/AO88-%E2%80%93-S%C3%A2n-Ch%C6%A1i-C%C3%A1-C%C6%B0%E1%BB%A3c-Tr%E1%BB%B1c-Tuy%E1%BA%BFn-N%C4%83ng-%C4%90%E1%BB%99ng-K%C3%A8o-V%C3%A0-Game-Cu%E1%BB%91n-H%C3%BAt_449067.html
https://www.alive-directory.com/AO88-%E2%80%93-S%C3%A2n-Ch%C6%A1i-C%C3%A1-C%C6%B0%E1%BB%A3c-Tr%E1%BB%B1c-Tuy%E1%BA%BFn-N%C4%83ng-%C4%90%E1%BB%99ng-K%C3%A8o-V%C3%A0-Game-Cu%E1%BB%91n-H%C3%BAt_726108.html
https://www.clickasnap.com/profile/ao887com
https://soundcloud.com/ao88-194264633
https://fliphtml5.com/home/ao887com
https://newspicks.com/user/12415392/
https://jump.5ch.net/?https://ao88-7.com/
https://www.tm-town.com///translators/ao887com
https://biolinku.co/ao887com
https://linkmix.co/53848519
https://land-book.com/ao887com
https://ko-fi.com/ao887com
https://jali.me/ao887com
https://pantip.com/profile/9333725
https://www.interesting-dir.com/details.php?id=443124
https://www.addirectory.org/details.php?id=479013
https://kitsu.app/users/ao887com
https://controlc.com/i6n2n9sb
https://giphy.com/channel/ao887com
https://www.producthunt.com/@ao887com
https://justpaste.it/hssti
https://www.awwwards.com/ao887com/
https://fairygodboss.com/users/profile/WjggJn1suy/ao887com
https://stepik.org/users/1252016873/profile
https://rentry.co/2nfsks4z
https://www.demilked.com/author/ao887com/
https://www.depechemode.cz/?URL=https://ao88-7.com/
https://www.buckeyescoop.com/users/f4a5d137-056c-4e68-b946-4842c8153c1c
https://jp.pinterest.com/ao887com/
https://de.gta5-mods.com/users/ao887com
https://mk.gta5-mods.com/users/ao887com
https://tr.gta5-mods.com/users/ao887com
https://bs.gravatar.com/ao887com
https://www.pozible.com/profile/ao88-12
https://dialogluzern.ch/profiles/ao887com/activity
https://app.scholasticahq.com/scholars/522462-nha-cai-ao88
https://community.atlassian.com/user/profile/0bc229c2-18f4-456a-a442-6fa372ef8d66
https://manifold.markets/ao887com
https://www.maanation.com/ao887com
https://pixelfed.uno/ao887com
http://mura.hitobashira.org/index.php?ao887com
https://peatix.com/user/29467705/view
https://padlet.com/mikeortega276/ao88-san-choi-ca-cuoc-truc-tuyen-nang-ong-keo-va-game-cuon-h-d1bsjb55h0zwr6zb/wish/4b3zaMp2pP01W2j7
https://www.elephantjournal.com/profile/mikeortega276/
https://community.hodinkee.com/members/ao887com
https://decidim.santcugat.cat/profiles/ao887com/activity
https://www.slideshare.net/mikeortega276?tab=about
https://forum.allkpop.com/suite/user/315399-ao887com/#about
https://janitorai.com/profiles/48a4156d-0a1d-4137-bb7c-1369552244f1_profile-of-ao-887-com
https://www.akiba-online.com/members/ao887com.1354764/#about
https://worstgen.alwaysdata.net/forum/members/ao887com.174158/#about
https://www.tkaraoke.com/forums/profile/ao887com/
https://www.pickupforum.de/profile/247818-ao887com/
http://linoit.com/users/ao887com/canvases/AO88
https://sidequestvr.com/user/4942329
https://dojour.us/u/ao887com
https://www.myconcertarchive.com/en/user_home?id=130434
https://cinderella.pro/user/273636/ao887com/#preferences
https://giloo.ist/member/ao887com
https://defence.pk/members/ao887com.239880/#about
https://forum.jatekok.hu/User-ao887com
https://www.buymusic.club/user/ao887com
https://histre.com/notes/ao887com/jmk47lja/?accesscode=Wi4ZhgVFd7i2uJW8
https://forum.freero.org/space-uid-24864.html
https://oraclenana.com/MYBB3/user-42516.html
https://www.notariosyregistradores.com/web/forums/usuario/ao887com/
http://genina.com/user/editDone/5333972.page
https://www.signaly.cz/mikeortega
https://www.dailymotion.com/user/ao887com
https://mysportsgo.com/profile/ao887com
https://socialsocial.social/user/ao887com/
https://es.stylevore.com/user/ao887com
https://rant.li/ao887com/ao88-san-choi-ca-cuoc-truc-tuyen-nang-dong-keo-va-game-cuon-hut
https://chanylib.ru/ru/forum/user/25879/
https://producerbox.com/users/ao887com
https://skrolli.fi/keskustelu/users/mikeortega276/
https://forum.vgatemall.com/member.php?action=profile&uid=505436
https://www.thehockeypaper.co.uk/forums/users/ao887com
https://www.forum-joyingauto.com/member.php?action=profile&uid=112642
https://www.11plus.co.uk/users/ao887com/
https://opaseke.com/users/15294
https://app.getfarmish.com/profile/ao887com
https://imaginaria.ru/profile/ao887com/
https://artconomy.com/profile/ao887com/about/
https://nl.gravatar.com/ao887com
https://nb.gravatar.com/ao887com
https://ms.gravatar.com/ao887com
https://lt.gravatar.com/ao887com
https://kn.gravatar.com/ao887com
https://galgame.dev/user/ao887com
https://nicheless.blog/author/ao88
https://www.newgenstravel.com/forum/topic/43370/ao88-%E2%80%93-s%C3%A2n-ch%C6%A1i-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-n%C4%83ng-%C4%90%E1%BB%99ng,-k%C3%A8o-v%C3%A0-game-cu%E1%BB%91n-h%C3%BAt
https://zbrushcentral.jp/user/ao887com
http://julia4tied.de/member.php?action=profile&uid=246772
https://forum.rexygen.com/user/ao887com
https://linktr.ee/ao887com
https://www.mapleprimes.com/users/ao887com
https://www.plurk.com/AO88
https://uno-en-ligne.com/profile.php?user=423753
https://hieuvetraitim.vn/members/ao88.127151/
https://vc.ru/id5917179
https://www.postman.com/ao887com
https://www.adpost.com/u/ao887com/
https://www.goldposter.com/members/ao887com/profile/
https://scrapbox.io/ao887com/AO88_%E2%80%93_S%C3%A2n_Ch%C6%A1i_C%C3%A1_C%C6%B0%E1%BB%A3c_Tr%E1%BB%B1c_Tuy%E1%BA%BFn_N%C4%83ng_%C4%90%E1%BB%99ng,_K%C3%A8o_V%C3%A0_Game_Cu%E1%BB%91n_H%C3%BAt
https://te.legra.ph/AO88–S%C3%A2n-Ch%C6%A1i-C%C3%A1-C%C6%B0%E1%BB%A3c-Tr%E1%BB%B1c-Tuy%E1%BA%BFn-N%C4%83ng-%C4%90%E1%BB%99ng-K%C3%A8o-V%C3%A0-Game-Cu%E1%BB%91n-H%C3%BAt-04-26-2
https://zb3.org/ao887com/ao88-san-choi-ca-cuoc-truc-tuyen-nang-dong-keo-va-game-cuon-hut
I consider something truly special in this internet site.
great issues altogether, you just gained a new reader. What would you suggest in regards to your publish that you made some days ago? Any positive?
Thanks in support of sharing such a nice idea, post is pleasant,
thats why i have read it entirely
Your comment is awaiting moderation.
Кракен выводит онлайн-шопинг на совсем новый уровень благодаря непревзойденному разнообразию и первоклассному сервису.
В одном месте вы найдете все:
от известных люксовых брендов до бюджетных вариантов.
Членство в программе KRAKEN актуальные адреса работают в 2026 ⚡ доступны сейчас % дает еще больше плюсов, таких как бесплатная доставка прямо до двери и доступ к эксклюзивным предложениям.
Присоединяйтесь к семье (***) KRAKEN TOR браузер и зеркала 2026: анонимный вход через адреса ⤷ сегодня и станьте частью будущего шопинга!
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan bersyukur kepada Anda.
Saya kebetulan menemukan situs Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang luar biasa.
Saya benar-benar beruntung menemukan situs ini di Bing, persis seperti yang saya telusuri : D pula sudah saya bookmark.
Kemarin, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi tiga puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang unggul!
Wow, keren blog format! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda hebat, belum lagi kontennya!
Hi there, I believe your blog could be having internet
browser compatibility issues. When I take a look at your website in Safari, it looks fine but when opening in IE, it’s got some
overlapping issues. I just wanted to provide you with
a quick heads up! Aside from that, fantastic blog!
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang sangat bagus!
Hai semua, saya menemukan blog Anda melalui Google ketika mencari subjek yang mirip, website Anda tampil di bagian atas. Saya harus mengatakan bahwa saya kagum seberapa baik penulisannya. Saya sangat menyukai menelusuri ini dan saya pasti akan kembali untuk melihat konten lainnya. Terima kasih!
Really Appreciate this update, how can I make is so that I get an email sent to me every time you publish a fresh article?
Saya umumnya tidak meninggalkan komentar, tetapi yang ini benar-benar layak. Konten yang luar biasa dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Saya melihat banyak website tetapi saya pikir yang satu ini mengandung sesuatu yang ekstra di dalamnya
Pretty component to content. I simply stumbled upon your weblog and in accession capital to assert that I get in fact enjoyed account your blog posts. Any way I’ll be subscribing on your augment or even I fulfillment you get entry to persistently quickly.
I think this is among the most important information for me.
And i’m glad reading your article. But wanna remark on few general things, The site style is wonderful, the articles is
really great : D. Good job, cheers
Saya selalu peduli dengan subjek ini dan tetap masih demikian, sangat dihargai telah mengunggah.
Luar biasa website yang Anda miliki, tapi saya ingin tahu apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin sekali menjadi bagian dari kelompok di mana saya bisa mendapatkan pendapat dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Cheers!
Saya kebetulan menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
Saya tidak sangat bagus dalam bahasa Inggris tetapi saya menyadari ini amat santai untuk diterjemahkan.
Halo semua, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan banyak wawasan yang bermanfaat. Terima kasih!
Konten yang hebat! Gaya penulisan Anda jelas dan mudah dipahami. Saya tentu akan kembali untuk melihat konten lainnya.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Sangat baik. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Berharga info. Untungnya saya menemukan situs web Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak terjadi lebih awal! Saya menandainya.
Deporte Ecuador es una plataforma informativa centrada en el
análisis del ecosistema digital del deporte ecuatoriano.
El sitio reúne contenidos que examinan el desarrollo del deporte ecuatoriano
en relación con la tecnología, la data y las tendencias de uso actuales.
A diferencia de las páginas deportivas comunes, Deporte Ecuador no se
limita a cubrir resultados o noticias. La prioridad es comprender el funcionamiento del ecosistema deportivo moderno: el modo en que los usuarios usan las plataformas, qué elementos
determinan su comportamiento y cómo cambian los criterios de calidad en el entorno digital.
El contenido del sitio se estructura bajo varios pilares principales.
Por un lado, se analizan las plataformas deportivas desde la perspectiva de la experiencia del usuario, la estabilidad y consistencia del
servicio. Además, se revisan las dinámicas del mercado, procesos de transformación digital
y evolución del consumo deportivo en el país.
Además, Deporte Ecuador aborda aspectos relacionados con la regulación, la protección digital
y la toma de decisiones dentro del entorno online. Esto permite ofrecer una visión más
completa del sector, mezclando evaluación técnica, realidad local y
comportamiento del usuario.
El objetivo del proyecto es proporcionar información clara, estructurada y útil para interpretar el deporte
en el entorno digital actual. No pretende reducir el análisis a
explicaciones básicas, sino facilitar la comprensión de un escenario cada vez más
complejo.
El portal está orientado a lectores que buscan entender
el deporte más allá de la superficie: considerando su dimensión tecnológica y su impacto en la experiencia cotidiana.
Se señala que el texto incluye un enlace para continuar leyendo la información.
I’ve learn a few just right stuff here. Definitely value bookmarking for revisiting. I wonder how much effort you set to make any such wonderful informative website.
Saya melihat banyak website tetapi saya anggap yang satu ini punya sesuatu yang spesial di dalamnya
Rattling clear internet site, appreciate it for this post.
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada metode Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Konten yang luar biasa! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
Your comment is awaiting moderation.
https://www.facebook.com/Mangalistnet
https://www.youtube.com/@Mangalistnet
https://twitter.com/Mangalistnet
https://tooter.in/Mangalistnet
https://wakelet.com/@Mangalistnet
https://safechat.com/u/mangalistnet
https://www.blogger.com/profile/04611089669157889939
https://www.mymeetbook.com/Mangalistnet
https://www.pinterest.com/Mangalistnet/
https://band.link/Mangalistnet
https://community.wongcw.com/Mangalistnet
https://demo.wowonder.com/Mangalistnet
https://shareyoursocial.com/Mangalistnet
https://myspace.com/Mangalistnet
https://500px.com/p/mangalistnet
https://www.instapaper.com/p/Mangalistnet
https://magic.ly/Mangalistnet
https://band.us/@mangalistnet
https://protocol.ooo/ja/users/mangalistnet
https://sketchfab.com/Mangalistnet
https://www.tumblr.com/mangalistnet
https://www.reddit.com/user/Mangalistnet/
https://audiomack.com/mangalistnet
https://hackaday.io/Mangalistnet
https://leetcode.com/u/Mangalistnet/
https://swag.live/en/user/69e72a3389cc47d56813f30f
https://www.halaltrip.com/user/profile/340479/mangalistnet/
https://medibang.com/author/28174348/
https://opensea.io/Mangalistnet
https://www.blockdit.com/mangalistnet
https://portfolium.com/Mangalistnet
https://groups.google.com/g/mangalistnet
https://www.twitch.tv/mangalistnet/about
https://profile.hatena.ne.jp/Mangalistnet/profile
https://issuu.com/mangalistnet
https://www.behance.net/Mangalistnet
https://gravatar.com/mangalistnet
https://www.reverbnation.com/artist/Mangalistnet
https://www.myminifactory.com/users/Mangalistnet
https://www.investagrams.com/Profile/mangalistnet
https://gifyu.com/mangalistnet
https://www.chordie.com/forum/profile.php?id=2511192
https://skitterphoto.com/photographers/2662050/mangalistnet
https://www.longisland.com/profile/Mangalistnet
https://www.walkscore.com/people/249936692554/mangalistnet
https://topsitenet.com/profile/mangalistnet/1646335/
https://akniga.org/profile/1415824-mangalistnet/
https://mangalistnet.bandcamp.com/album/mangalistnet
https://disqus.com/by/Mangalistnet/about/
https://jobs.suncommunitynews.com/profiles/8176828-mangalistnet
https://www.speedrun.com/users/Mangalistnet
https://www.fanart-central.net/user/Mangalistnet/profile
https://slides.com/mangalistnet
https://www.aicrowd.com/participants/mangalistnet
https://old.bitchute.com/channel/X6LSfFmWFpGb/
https://pbase.com/Mangalistnet
https://hub.docker.com/u/mangalistnet
https://spiderum.com/nguoi-dung/Mangalistnet
https://zaidap.com/thong-tin-ca-nhan-u107386.htm
https://www.gta5-mods.com/users/Mangalistnet
https://heylink.me/Mangalistnet/
https://pixabay.com/users/mangalistnet-55531961/
https://www.nicovideo.jp/user/143992338
https://www.jigsawplanet.com/Mangalistnet
https://3dwarehouse.sketchup.com/by/Mangalistnet
https://robertsspaceindustries.com/en/citizens/Mangalistnet
https://bit.ly/m/Mangalistnet
https://joy.link/mangalistnet
https://connect.garmin.com/app/profile/30c73774-e486-4da6-bb16-4c3bf3a18c82
https://b.hatena.ne.jp/Mangalistnet/bookmark
https://www.chichi-pui.com/users/Mangalistnet/
https://www.openrec.tv/user/Mangalistnet/about
https://unityroom.com/users/lxg7iutfa80oh1nb4v2p
https://pxhere.com/en/photographer-me/4988506
https://teletype.in/@mangalistnet
https://www.checkli.com/mangalistnet
https://www.fuelly.com/driver/mangalistnet
https://www.nintendo-master.com/profil/mangalistnet
https://freeimage.host/mangalistnet
https://www.diigo.com/profile/mangalistnet
https://fontstruct.com/fontstructions/show/2868887/mangalistnet
https://motion-gallery.net/users/956067
https://linkin.bio/mangalistnet
https://biomolecula.ru/authors/142103
https://talk.plesk.com/members/mangalistnet.502457/#about
https://www.callupcontact.com/b/businessprofile/Mangalistnet/10059353
https://www.growkudos.com/profile/akimachi_jun
https://blender.community/Mangalistnet/
https://doselect.com/@1c8521b327fe56d1b0ea933b9
https://sciter.com/forums/users/mangalistnet/
https://matkafasi.com/user/Mangalistnet
https://allmyfaves.com/Mangalistnet
https://www.notebook.ai/@Mangalistnet
https://www.abclinuxu.cz/lide/mangalistnet
https://dumagueteinfo.com/author/Mangalistnet/
https://muare.vn/shop/akimachi-jun/902559
https://doodleordie.com/profile/mangalistnet
https://musikersuche.musicstore.de/profil/Mangalistnet/
https://www.intensedebate.com/profiles/mangalistnet
https://forum.dmec.vn/index.php?members/mangalistnet.187729/
https://igli.me/Mangalistnet
https://duyendangaodai.net/members/31607-Mangalis.html
http://delphi.larsbo.org/user/Mangalistnet
https://www.aseeralkotb.com/en/profiles/Mangalistnet
https://timdaily.vn/members/mangalistnet.134198/#about
https://app.readthedocs.org/profiles/Mangalistnet/
https://www.dibiz.com/velizdavid375
https://iszene.com/user-347835.html
https://www.theyeshivaworld.com/coffeeroom/users/mangalistnet
https://desksnear.me/users/mangalistnet
https://www.itchyforum.com/en/member.php?388266-Mangalistnet
https://www.roton.com/forums/users/velizdavid375/
https://able2know.org/user/mangalistnet/
http://www.biblesupport.com/user/831668-mangalistnet/
https://golosknig.com/profile/Mangalistnet/
https://www.anibookmark.com/user/mangalistnet.html
https://www.inventoridigiochi.it/membri/Mangalistnet/profile/
https://forum.m5stack.com/user/mangalistnet
https://wallhaven.cc/user/Mangalistnet
https://imageevent.com/mangalistnet/mangalistnet
https://www.bitchute.com/channel/X6LSfFmWFpGb
https://bandori.party/user/796562/Mangalistnet/
https://community.m5stack.com/user/mangalistnet
https://schoolido.lu/user/Mangalistnet/
https://awan.pro/forum/user/165896/
https://fortunetelleroracle.com/profile/mangalistnet
https://fabble.cc/mangalistnet
https://vozer.net/members/mangalistnet.89816/#about
https://community.cisco.com/t5/user/viewprofilepage/user-id/2068267
https://kr.pinterest.com/Mangalistnet/
https://pt.gravatar.com/Mangalistnet
https://th.gravatar.com/mangalistnet
https://www.sythe.org/members/mangalistnet.2040127/
https://f319.com/members/mangalistnet.1097883/
https://about.me/Mangalistnet
https://booklog.jp/users/mangalistnet/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/mangalistnet.1353738/#about
https://www.equinenow.com/farm/mangalistnet.htm
https://wefunder.com/Mangalistnet
https://potofu.me/mangalistnet
https://transfur.com/Users/mangalistnet
https://xtremepape.rs/members/mangalistnet.666243/#about
https://github.com/Mangalistnet
https://myanimelist.net/profile/Mangalistnet
https://website.informer.com/mangalist.net
https://lightroom.adobe.com/u/Mangalistnet
https://beacons.ai/mangalistnet
https://en.islcollective.com/portfolio/12904026
https://www.xosothantai.com/members/mangalistnet.609446/
https://velog.io/@mangalistnet/about
https://violet.vn/user/show/id/15268165
https://iplogger.org/vn/logger/BexR5xqpOxqt/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3942747
https://mez.ink/mangalistnet
https://mangalistnet.stck.me/profile
https://notionpress.com/author/1508720
https://www.edna.cz/uzivatele/mangalistnet/
https://digiphoto.techbang.com/users/mangalistnet
https://leakedmodels.com/forum/members/mangalistnet.709114/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1066725
https://freeicons.io/profile/921446
https://onlinesequencer.net/forum/user-268119.html
https://inkbunny.net/Mangalistnet
https://www.japaaan.com/user/77104/
https://spinninrecords.com/profile/Mangalistnet
https://www.launchgood.com/user/newprofile#!/user-profile/profile/akimachi.jun
https://beatsaver.com/playlists/1182152
https://apptuts.bio/mangalistnet
https://dialog.eslov.se/profiles/Mangalistnet/activity
https://www.storenvy.com/Mangalistnet
https://forums.maxperformanceinc.com/forums/member.php?u=246624
https://egl.circlly.com/users/Mangalistnet
https://goodandbadpeople.com/Mangalistnet
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=301186
https://www.sciencebee.com.bd/qna/user/Mangalistnet
https://acomics.ru/-Mangalistnet
https://www.criminalelement.com/members/mangalistnet/profile/
https://hanson.net/users/Mangalistnet
https://expatguidekorea.com/profile/mangalistnet/
https://www.laundrynation.com/community/profile/mangalistnet/
https://www.heavyironjobs.com/profiles/8178797-mangalistnet
https://pad.degrowth.net/s/lipxA9AgR
http://fort-raevskiy.ru/community/profile/mangalistnet/
https://forum.skullgirlsmobile.com/members/mangalistnet.215518/#about
https://jobs.landscapeindustrycareers.org/profiles/8178832-mangalistnet
https://phatwalletforums.com/user/mangalistnet/
https://song.link/Mangalistnet
https://idol.st/user/165326/Mangalistnet/
https://www.valinor.com.br/forum/usuario/mangalistnet.145210/#about
https://tulieu.violet.vn/user/show/id/15268165
https://www.bmwpower.lv/user.php?u=Mangalistnet
https://gockhuat.net/member.php?u=436973
https://jobs.windomnews.com/profiles/8178899-mangalistnet
https://hoaxbuster.com/redacteur/Mangalistnet
https://www.givey.com/mangalistnet
https://pc.poradna.net/users/1184416526-mangalistnet
https://zerosuicidetraining.edc.org/user/profile.php?id=560476
https://beteiligung.amt-huettener-berge.de/profile/Mangalistnet/
https://joinentre.com/profile/mangalistnet
https://jobs.westerncity.com/profiles/8178956-mangalistnet
https://www.thetriumphforum.com/members/mangalistnet.62962/
https://gamblingtherapy.org/forum/users/mangalistnet/
https://l2top.co/forum/members/mangalistnet.173270/
http://www.askmap.net/location/7793969/japan/mangalistnet
https://youtopiaproject.com/author/Mangalistnet
https://graphcommons.com/graphs/342f4c14-c8c9-4b32-ac4c-64901b68996c
https://galleria.emotionflow.com/183148/profile.html
https://www.myget.org/users/Mangalistnet
https://www.deafvideo.tv/vlogger/Mangalistnet
https://chaloke.com/forums/users/mangalistnet/
https://app.brancher.ai/user/bGrlEGxZKr26
https://justpaste.me/FOsK1
https://www.empregosaude.pt/en/author/mangalistnet/
https://confengine.com/user/Mangalistnet
https://mygamedb.com/profile/Mangalistnet
https://buckeyescoop.com/community/members/mangalistnet.62626/#about
https://forum.aceinna.com/user/mangalistnet
https://www.mateball.com/Mangalistnet
https://web-tourist.net/members/mangalistnet.52908/#about
https://toirscript.com/user/mangalistnet
https://forum.pabbly.com/members/mangalistnet.112729/#about
http://forum.cncprovn.com/members/424485-Mangalistnet
https://ncnews.co/profile/mangalistnet
https://dreevoo.com/profile_info.php?pid=1526807
https://forum.aigato.vn/user/mangalistnet
https://amaz0ns.com/forums/users/Mangalistnet/
https://rapidapi.com/user/Mangalistnet
https://www.skool.com/@akimachi-jun-6538
https://learningapps.org/watch?v=pjirerkg326
https://coub.com/mangalistnet
https://www.giveawayoftheday.com/forums/profile/1810608
http://onlineboxing.net/jforum/user/editDone/447606.page
http://www.invelos.com/UserProfile.aspx?alias=Mangalistnet
https://www.video-bookmark.com/bookmark/7110291/mangalistnet/
https://wibki.com/Mangalistnet
https://krachelart.com/UserProfile/tabid/43/userId/1342927/Default.aspx
https://gitlab.vuhdo.io/Mangalistnet
https://www.11secondclub.com/users/profile/1712912
https://kktix.com/user/8673091
https://www.passes.com/mangalistnet
https://uiverse.io/profile/akimachi_5315
https://www.rwaq.org/users/mangalistnet
https://cofacts.tw/user/Mangalistnet
https://www.fitday.com/fitness/forums/members/mangalistnet.html
https://www.fundable.com/akimachi-jun
https://vcook.jp/users/87750
https://www.grepmed.com/Mangalistnet
https://espritgames.com/members/50830599/
https://cgmood.com/mangalistnet
https://www.haikudeck.com/presentations/Mangalistnet
https://www.efunda.com/members/people/show_people.cfm?Usr=Mangalistnet
https://diit.cz/profil/tbmbizzdsn
https://backloggery.com/Mangalistnet
https://raovat.nhadat.vn/members/mangalistnet-306282.html
https://www.koi-s.id/member.php?332364-Mangalistnet
https://pumpyoursound.com/u/user/1611513
https://hi-fi-forum.net/profile/1145471
https://secondstreet.ru/profile/Mangalistnet/
https://scenarch.com/userpages/33528
https://undrtone.com/Mangalistnet
https://marshallyin.com/members/mangalistnet/
https://us.enrollbusiness.com/BusinessProfile/7782813/Mangalistnet
https://www.atozed.com/forums/user-77728.html
https://www.tizmos.com/Mangalistnet/
https://gravesales.com/author/mangalistnet/
https://searchengines.bg/members/mangalistnet.26238/#about
https://luvly.co/users/Mangalistnet
https://suckhoetoday.com/members/37244-Mangalis.html
https://hukukevi.net/user/Mangalistnet
https://belgaumonline.com/profile/Mangalistnet/
https://savelist.co/profile/users/Mangalistnet
https://usdinstitute.com/forums/users/Mangalistnet/
https://www.montessorijobsuk.co.uk/author/mangalistnet/
https://www.apsense.com/user/mangalistnet
https://zzb.bz/rJbtvf
https://draft.blogger.com/profile/04611089669157889939
https://hack.allmende.io/s/bu06iVfJU
https://pad.codefor.fr/s/gTq8NvYqeP
https://hackmd.hub.yt/s/V1_9xOyv2
https://www.themeqx.com/forums/users/Mangalistnet/
https://www.udrpsearch.com/user/Mangalistnet
http://newdigital-world.com/members/mangalistnet.html
https://www.xen-factory.com/index.php?members/mangalistnet.155071/#about
https://cointr.ee/mangalistnet
https://forums.servethehome.com/index.php?members/mangalistnet.239181/#about
https://jaga.link/Mangalistnet
https://b.io/Mangalistnet
https://www.blackhatprotools.info/member.php?287571-Mangalistnet
https://activepages.com.au/profile/mangalistnet
https://snippet.host/drpivk
https://tudomuaban.com/chi-tiet-rao-vat/2884772/mangalistnet.html
https://phijkchu.com/a/mangalistnet/video-channels
https://lifeinsys.com/user/mangalistnet
https://kaeuchi.jp/forums/users/mangalistnet/
https://www.claimajob.com/profiles/8182091-mangalistnet
https://protospielsouth.com/user/130211
https://theafricavoice.com/profile/mangalistnet
http://palangshim.com/space-uid-5110439.html
https://www.africangenesis-101.org/profile/velizdavid37557164/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:0E81814D69E72F3D0A495C35@AdobeID
https://vi.gravatar.com/mangalistnet
https://www.mixcloud.com/Mangalistnet/
https://www.designspiration.com/mangalistnet/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=194508
https://hub.vroid.com/en/users/125618803
https://circleten.org/a/404838
https://support.bitspower.com/support/user/Mangalistnet
https://www.brownbook.net/business/55035265/mangalistnet
https://etextpad.com/oq7ntv5uix
https://app.hellothematic.com/creator/profile/1144731
https://app.talkshoe.com/user/mangalistnet
https://golden-forum.com/memberlist.php?mode=viewprofile&u=229333
https://m.wibki.com/Mangalistnet
https://www.pageorama.com/?p=mangalistnet
https://bandsworksconcerts.info/index.php?Mangalistnet
https://bbs.mikocon.com/home.php?mod=space&uid=290396
https://www.mikocon.com/home.php?mod=space&uid=290396
https://manylink.co/@Mangalistnet
https://www.freewebspace.net/forums/index.php?members/mangalistnet.17034663/#about
https://seomotionz.com/member.php?action=profile&uid=128210
https://anyflip.com/homepage/auzjm#About
https://www.akaqa.com/question/q19192673762-Mangalistnet
https://londonchinese.com/home.php?mod=space&uid=620740&do=profile
https://copynotes.be/shift4me/forum/user-52512.html
https://scholar.google.com/citations?hl=en&user=-V-5EdUAAAAJ
https://coolors.co/u/Mangalistnet
https://www.beamng.com/members/mangalistnet.789382/
https://civitai.com/user/Mangalistnet
https://www.spigotmc.org/members/mangalistnet.2523317/
https://camp-fire.jp/profile/Mangalistnet
https://feyenoord.supporters.nl/profiel/148696/Mangalistnet
https://www.pearltrees.com/mangalistnet/item792831666
https://gesoten.com/profile/detail/12753169
https://rekonise.com/u/Mangalistnet
https://hashnode.com/@mangalistnet
https://hoo.be/mangalistnet
https://nhattao.com/members/user6956431.6956431/
https://maxforlive.com/profile/user/Mangalistnet?tab=about
https://3dtoday.ru/blogs/mangalistnet
https://opencollective.com/mangalistnet
https://pinshape.com/users/8953827-mangalistnet
https://morguefile.com/creative/Mangalistnet
https://edabit.com/user/QfLJkksvnn9YC9Los
https://mathlog.info/users/5N53FyK496glNymEY7bcFLdFNr73
https://securityheaders.com/?q=https%3A%2F%2Fmangalist.net%2F
https://my.bio/mangalistnet
https://sfx.thelazy.net/users/u/Mangalistnet/
https://mikseri.net/user/Mangalistnet
https://app.daily.dev/mangalistnet
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=259561
https://www.skypixel.com/users/djiuser-6rhrj04r8ugx
http://webanketa.com/forms/6mvk0d9n74qk0rk1c8vk6csh/
https://www.pdc.edu/?URL=https://mangalist.net/
https://ask.mallaky.com/?qa=user/Mangalistnet
https://www.clashfarmer.com/forum/member.php?action=profile&uid=80017
https://www.depechemode.cz/?URL=https://mangalist.net/
https://sub4sub.net/forums/users/mangalistnet/
https://www.slmath.org/people/105484
https://userstyles.world/user/Mangalistnet
https://goo.by/LKnaoy
https://amazingradio.com/profile/mangalistnet
https://bresdel.com/Mangalistnet
https://www.matrix-digi.com/forums/member.php?action=profile&uid=13744
https://fora.babinet.cz/profile.php?section=personal&id=123910
https://www.shippingexplorer.net/en/user/mangalistnet/279807
https://pictureinbottle.com/r/mangalistnet
https://forum.epicbrowser.com/profile.php?section=personal&id=152197
http://www.dungdong.com/home.php?mod=space&uid=3366271&do=profile
https://www.squadskates.com/profile/velizdavid37518212/profile
https://forum.herozerogame.com/index.php?/user/162116-mangalistnet/
https://shhhnewcastleswingers.club/forums/users/Mangalistnet/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2470008
https://connect.gt/user/mangalistnet
https://forum.tkool.jp/index.php?members/mangalistnet.105852/#about
https://www.divephotoguide.com/user/Mangalistnet
https://www.weddingbee.com/members/mangalistnet/
https://kumu.io/Mangalistnet/mangalistnet
https://bioimagingcore.be/q2a/user/Mangalistnet
https://www.sunlitcentrekenya.co.ke/author/mangalistnet/
https://mangalistnet.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/Mangalistnet/activity
https://www.rcuniverse.com/forum/members/mangalistnet.html
https://www.socialbookmarkssite.com/bookmark/6240171/mangalistnet/
https://www.hogwartsishere.com/1835406/
https://vimeo.com/mangalistnet
https://gitlab.com/Mangalistnet
https://www.symbaloo.com/shared/AAAAAbg7rLEAA41-5EOPoQ==
https://www.bricklink.com/aboutMe.asp?u=Mangalistnet
https://makeagif.com/user/Mangalistnet?ref=YG9pwN
https://www.lingvolive.com/en-us/profile/5acc4da9-ad6f-4969-8fc0-875f7f6340b8/translations
https://www.france-ioi.org/user/perso.php?sLogin=mangalistnet
https://mt2.org/uyeler/mangalistnet.39230/#about
https://www.trackyserver.com/profile/246678
https://ixawiki.com/link.php?url=https://mangalist.net/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=143497
https://www.zubersoft.com/mobilesheets/forum/user-135294.html
https://hackmd.openmole.org/s/awpSCkrt7
https://md.chaosdorf.de/s/g_1HdETQjD
https://www.plotterusati.it/user/mangalistnet
http://www.activewin.com/user.asp?Action=Read&UserIndex=4838179
http://www.jbt4.com/home.php?mod=space&uid=8670833
https://www.vid419.com/home.php?mod=space&uid=3486627
https://forum.ct8.pl/member.php?action=profile&uid=122009
https://devfolio.co/@Mangalistnet/readme-md
https://mangalistnet.shopinfo.jp/posts/58764320
https://linqto.me/n/mangalistnet
https://www.mindomo.com/mindmap/cd094f094e154f3a9410e6761cba69e6
https://www.okaywan.com/home.php?mod=space&uid=797164
https://www.goodolcomics.com/blog/profile/mangalistnet/
https://www.swap-bot.com/user:Mangalistnet
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=391613
http://techou.jp/index.php?Mangalistnet
https://epiphonetalk.com/members/mangalistnet.97451/#about
http://tkdlab.com/wiki/index.php?Mangalistnet
https://www.managementpedia.com/members/mangalistnet.1120573/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=634760
https://volleypedia.org/index.php?qa=user&qa_1=Mangalistnet
http://pcsq28.com/home.php?mod=space&uid=1959200
https://bbs.airav.cc/home.php?mod=space&uid=4580065
https://partecipa.poliste.com/profiles/Mangalistnet/activity
https://hker2uk.com/home.php?mod=space&uid=5491958
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=495243
https://hcgdietinfo.com/hcgdietforums/members/mangalistnet/
https://aprenderfotografia.online/usuarios/mangalistnet/profile/
https://pads.zapf.in/s/701tPr22c3
http://galeria.farvista.net/member.php?action=showprofile&user_id=76868
https://www.play56.net/home.php?mod=space&uid=6142377
https://thesn.eu/Mangalistnet
https://md.swk-web.com/s/TmEJhujZg
https://hedgedoc.dezentrale.space/s/wMTcBK-5_
https://ar.gravatar.com/mangalistnet
https://odesli.co/Mangalistnet
https://wandb.ai/profile/mangalistnet
https://bbcovenant.guildlaunch.com/users/blog/6753288/?mode=view&gid=97523
https://youbiz.com/profile/mangalistnet/
https://www.wowonder.xyz/Mangalistnet
https://sciencemission.com/profile/mangalistnet
http://jobboard.piasd.org/author/mangalistnet/
https://www.wvhired.com/profiles/8185948-mangalistnet
https://kenhrao.com/members/mangalistnet.121265/#about
http://jobs.emiogp.com/author/Mangalistnet/
https://ismschools.com.au/forums/users/mangalistnet/
https://forumketoan.com/members/mangalistnet.44146/#about
https://v.gd/pikVDl
https://gl.gta5-mods.com/users/Mangalistnet
http://www.webclap.com/php/jump.php?url=https://mangalist.net/
https://xoops.ec-cube.net/userinfo.php?uid=348670
https://formulamasa.com/elearning/members/mangalistnet/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1109425
https://quangcaoso.vn/Mangalistnet
https://chyoa.com/user/Mangalistnet
https://forums.alliedmods.net/member.php?u=476390
https://community.jmp.com/t5/user/viewprofilepage/user-id/97407
https://digiex.net/members/mangalistnet.144832/
https://smallseo.tools/website-checker/mangalist.net
https://bwinglive.lighthouseapp.com/users/1997419
https://rush1989.rash.jp/pukiwiki/index.php?Mangalistnet
https://www.stylevore.com/user/Mangalistnet
https://bio.site/Mangalistnet
https://wikimapia.org/external_link?url=https://mangalist.net/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6405969
https://www.thesims3.com/myBlog.html?persona=Mangalistnet
https://telegra.ph/Mangalistnet-04-23
https://campsite.bio/mangalistnet
https://reactormag.com/members/mangalistnet/
https://www.prosebox.net/book/108062/
https://www.aipictors.com/users/738063a6-340f-dd0d-6c10-72f44d7ddc44
https://log.concept2.com/profile/2924651
https://www.speedway-world.pl/forum/member.php?action=profile&uid=473036
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://mangalist.net/
http://forum.orangepi.org/home.php?mod=space&uid=6405969
https://redirect.camfrog.com/redirect/?url=https://mangalist.net/
https://beteiligung.hafencity.com/profile/Mangalistnet/
https://adhocracy.plus/profile/Mangalistnet/
https://www.hobowars.com/game/linker.php?url=https://mangalist.net/
https://beteiligung.stadtlindau.de/profile/Mangalistnet/
https://forum.honorboundgame.com/user-510009.html
https://elovebook.com/Mangalistnet
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=469754
https://www.fw-follow.com/forum/topic/117089/mangalistnet
https://www.jk-green.com/forum/topic/110761/mangalistnet
https://www.navacool.com/forum/topic/395566/mangalistnet
https://www.bonback.com/forum/topic/395568/mangalistnet
https://www.driedsquidathome.com/forum/topic/143289/mangalistnet
https://www.nongkhaempolice.com/forum/topic/123801/mangalistnet
https://www.bestloveweddingstudio.com/forum/topic/83115/mangalistnet
https://www.natthadon-sanengineering.com/forum/topic/103699/mangalistnet
https://www.rueanmaihom.net/forum/topic/98363/mangalistnet
https://www.ttlxshipping.com/forum/topic/395570/mangalistnet
https://pubhtml5.com/homepage/ckmbp/
http://worldchampmambo.com/UserProfile/tabid/42/userId/488077/Default.aspx
http://forum.modulebazaar.com/forums/user/Mangalistnet/
https://beteiligung.tengen.de/profile/Mangalistnet/
https://calaos.fr/forum/member.php?action=profile&uid=19959
https://www.rcmx.net/userinfo.php?uid=16791
https://www.pathumratjotun.com/forum/topic/177677/mangalistnet
https://maychetao.com/members/21187-Mangalis.html
https://diendan.cuabenhvien.com/members/19777-Mangalis.html
https://forum.web-z.net/profile.php?userid=9866
https://lqdoj.edu.vn/user/Mangalistnet
https://paperjale.eus/user/Mangalistnet
http://byltz.com/home.php?mod=space&uid=481496
https://indiestorygeek.com/user/Mangalistnet
https://diigo.com/012f4u4
https://forum.issabel.org/u/Mangalistnet
https://ie.enrollbusiness.com/BusinessProfile/7782813/Mangalistnet
https://raredirectory.com/author/mangalistnet-50044/
https://www.iglinks.io/Mangalistnet-426
https://www.keepandshare.com/discuss2/46248/mangalistnet
http://bbs.medicalforum.cn/home.php?mod=space&uid=2233852
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://mangalist.net/
https://giaoan.violet.vn/user/show/id/15268165
https://anh135689999.violet.vn/user/show/id/15268165
https://party.biz/index.php/profile/381669?tab=541
https://hu.gta5-mods.com/users/Mangalistnet
https://www.backabuddy.co.za/campaign/mangalistnet
https://uk.gta5-mods.com/users/Mangalistnet
https://sl.gta5-mods.com/users/Mangalistnet
https://at.pinterest.com/Mangalistnet/
https://www.easyhits4u.com/profile.cgi?login=mangalistnet
https://newdayrp.com/members/mangalistnet.70994/#about
https://in.pinterest.com/Mangalistnet/
https://doc.anagora.org/s/xhTKGDwpc
https://album.link/Mangalistnet
https://artist.link/Mangalistnet
https://pods.link/Mangalistnet
https://mylink.page/Mangalistnet
https://playlist.link/Mangalistnet
https://portfolium.com.au/Mangalistnet
https://profile.sampo.ru/mangalistnet
https://mail.londonchinese.com/home.php?mod=space&uid=620740&do=profile
https://baigiang.violet.vn/user/show/id/15268165
http://www.muzikspace.com/profiledetails.aspx?profileid=136073
https://forums.starcontrol.com/user/7661871
https://forums.offworldgame.com/user/7661871
https://www.ekdarun.com/forum/topic/154382/mangalistnet
https://fanclove.jp/profile/90WwgDX0WP
https://truckymods.io/user/487632
https://forums.sinsofasolarempire.com/user/7661871
https://forums.stardock.net/user/7661871
https://www.dokkan-battle.fr/forums/users/mangalistnet/
https://www.d-ushop.com/forum/topic/129604/mangalistnet
https://www.templepurohit.com/forums/users/VelizDavid375/
https://www.fanfiction.net/~mangalistnet
https://www.horticulturaljobs.com/employers/4123523-mangalistnet
https://johsocial.com/story12039405/mangalistnet
https://jobs.siliconflorist.com/employers/4123526-mangalistnet
https://jobs.nefeshinternational.org/employers/4123530-mangalistnet
https://aboutcasemanagerjobs.com/author/mangalistnet/
https://buyandsellhair.com/author/mangalistnet/
https://rareconnect.org/en/user/mangalistnet
https://webyourself.eu/Mangalistnet
https://whyp.it/users/142553/mangalistnet
https://diendannhansu.com/members/mangalistnet.107998/#about
https://findaspring.org/members/mangalistnet/
https://www.pokecommunity.com/members/mangalistnet.1500331/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=778236
https://careers.coloradopublichealth.org/profiles/8187361-mangalistnet
https://cloud.anylogic.com/profile/user/492e39ff-8ef2-476b-b52d-be7d591e643c
https://gorillasocialwork.com/story26825001/mangalistnet
https://dienbd.violet.vn/user/show/id/15268165
https://kttm.club/members/mangalistnet.4959/#about
https://vnbit.org/members/mangalistnet.96204/#about
https://www.cake.me/me/akimachi-jun
https://boss.why3s.cc/boss/home.php?mod=space&uid=262689
https://clusterbusters.org/forums/profile/35550-mangalistnet/?tab=field_core_pfield_11
https://fengshuidirectory.com/dashboard/listings/Mangalistnet/
https://joyrulez.com/Mangalistnet
https://pets4friends.com/profile-1580269
https://staroetv.su/go?https://mangalist.net/
https://www.ixawiki.com/link.php?url=https://mangalist.net/
https://www.shinobi.jp/etc/goto.html?https://mangalist.net/
https://decide.enguera.es/profiles/Mangalistnet/activity
https://axe.rs/forum/members/mangalistnet.13426634/#about
https://postr.yruz.one/profile/mangalistnet
https://openlibrary.org/people/mangalistnet
https://www.bookingblog.com/forum/users/Mangalistnet
https://aiti.edu.vn/members/mangalistnet.43705/
https://tinhte.vn/members/mangalistnet.3389155/
https://barcelonadema-participa.cat/profiles/mangalistnet/activity
https://www.project1999.com/forums/member.php?u=333692
https://pad.stuve.de/s/zuWGuL28r
https://pad.libreon.fr/s/z-cOUGB67
https://www.betmma.tips/mma_handicapper.php?ID=183714
https://theexplorers.com/user?id=c69d593f-6be6-41e8-87cc-a2a004c06641
https://md.rappet.xyz/s/W9pvobV6gf
https://www.blurb.com/user/Mangalistnet
https://engage.aiaa.org/profile?UserKey=03a70cb3-b8d7-41e9-8836-019dba505d27
https://wall.page/CwSxnC
https://participa.aytojaen.es/profiles/Mangalistnet/activity
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=158499_c8g5flpg
https://www.ad-links.org/Mangalistnet_372640.html
https://www.beegdirectory.com/Mangalistnet_491424.html
https://www.aquarius-dir.com/Mangalistnet_517172.html
https://www.apeopledirectory.com/Mangalistnet_416067.html
https://www.bedirectory.com/Mangalistnet_448787.html
https://www.alive-directory.com/Mangalistnet_725888.html
https://www.clickasnap.com/profile/Mangalistnet
https://soundcloud.com/mangalistnet
https://fliphtml5.com/home/Mangalistnet
https://newspicks.com/user/12409967/
https://jump.5ch.net/?https://mangalist.net/
https://www.tm-town.com/translators/mangalistnet
https://biolinku.co/Mangalistnet
https://linkmix.co/53753928
https://land-book.com/mangalistnet
https://jali.me/Mangalistnet
https://www.interesting-dir.com/details.php?id=442966
https://www.addirectory.org/details.php?id=478712
https://kitsu.app/users/1705347
https://controlc.com/4i5h3vn7
http://resurrection.bungie.org/forum/index.pl?profile=Mangalistnet
https://giphy.com/channel/Mangalistnet
https://www.producthunt.com/@mangalistnet
https://justpaste.it/ge8we
https://www.awwwards.com/Mangalistnet/
https://stepik.org/users/1248812898/profile
https://rentry.co/t8nvocpm
https://www.demilked.com/author/mangalistnet/
https://depechemode.cz/?URL=https://mangalist.net/
https://www.buckeyescoop.com/users/323fce23-37b6-46e7-b3d9-ec937d253f60
https://jp.pinterest.com/Mangalistnet/
https://de.gta5-mods.com/users/Mangalistnet
https://mk.gta5-mods.com/users/Mangalistnet
https://tr.gta5-mods.com/users/Mangalistnet
https://bs.gravatar.com/mangalistnet
https://dialogluzern.ch/profiles/mangalistnet/activity
https://www.ecodir.net/Mangalistnet_338755.html
https://www.ask-dir.org/Mangalistnet_384242.html
https://tempel.in/view/4knSQ
https://quicknote.io/d7cbe3d0-3f16-11f1-b23a-cde862130e70/
https://www.maanation.com/Mangalistnet
http://mura.hitobashira.org/index.php?Mangalistnet
https://peatix.com/user/29444720/view
https://padlet.com/Mangalistnet/kindergarten-lesson-plan-mangalistnet-cel22zhutmjuubdu
https://www.elephantjournal.com/profile/mangalistnet/
https://mangalistnet.amebaownd.com/posts/58766082
https://decidim.santcugat.cat/profiles/mangalistnet/activity
https://mangahelpers.com/forum/members/mangalistnet.261092/#about
https://www.akiba-online.com/members/mangalistnet.1354354/#about
https://worstgen.alwaysdata.net/forum/members/mangalistnet.173727/#about
http://linoit.com/users/Mangalistnet/canvases/Mangalistnet
https://nortabs.net/user/14976/
https://dojour.us/u/Mangalistnet
https://www.myconcertarchive.com/en/user_home?id=130206
https://all4.vip/p/page/view-persons-profile?id=122939
https://ferrariformula1.hu/community/profile/mangalistnet/
https://strikefans.com/forum/users/Mangalistnet/
https://defence.pk/members/mangalistnet.239527/#about
https://forum.jatekok.hu/User-Mangalistnet
https://www.xibeiwujin.com/home.php?mod=space&uid=2314410&do=profile&from=space
https://www.buymusic.club/user/mangalistnet
https://histre.com/notes/velizdavid375/5otq8kjr/?accesscode=OQRi_WsYOaghlza5
https://forum.freero.org/space-uid-24820.html
https://oraclenana.com/MYBB3/user-42428.html
https://www.notariosyregistradores.com/web/forums/usuario/Mangalistnet/
https://experiment.com/users/Mangalistnet
https://www.facer.io/u/Mangalistnet
http://genina.com/user/editDone/5329915.page
https://wikifab.org/wiki/Utilisateur:Mangalistnet
https://mysportsgo.com/profile/Mangalistnet
https://forum-foxess.pro/community/profile/mangalistnet/
https://socialsocial.social/user/mangalistnet/
https://huggingface.co/mangalistnet
https://es.stylevore.com/user/Mangalistnet
https://rant.li/mangalistnet/mangalistnet
https://chanylib.ru/ru/forum/user/25573/
https://www.cbmstuff.com/forum/member.php?action=profile&uid=11668
https://producerbox.com/users/Mangalistnet
https://skrolli.fi/keskustelu/users/velizdavid375/
https://forum.vgatemall.com/member.php?action=profile&uid=500220
https://www.thehockeypaper.co.uk/forums/users/mangalistnet
https://channillo.com/user/72415/
https://www.forum-joyingauto.com/member.php?action=profile&uid=109364
https://www.11plus.co.uk/users/VelizDavid375/
https://opaseke.com/users/15230
https://app.getfarmish.com/profile/Mangalistnet
https://www.freebeg.com/forum/member.php?action=profile&uid=135530
https://artconomy.com/profile/Mangalistnet/about/
https://nl.gravatar.com/mangalistnet
https://nb.gravatar.com/mangalistnet
https://ms.gravatar.com/mangalistnet
https://lt.gravatar.com/mangalistnet
https://kn.gravatar.com/mangalistnet
https://galgame.dev/user/mangalistnet
https://nicheless.blog/author/mangalistnet
https://www.newgenstravel.com/forum/topic/42574/mangalistnet
https://zbrushcentral.jp/user/mangalistnet
https://altered.ajordat.com/it/profiles/6ef410e5-cc48-4cc6-939f-68fdae349ee9/
https://snabaynetworking.com/profile/16910/
http://julia4tied.de/member.php?action=profile&uid=246522
https://forum.rexygen.com/user/mangalistnet
https://linktr.ee/Mangalistnet
https://www.mapleprimes.com/users/Mangalistnet
https://uno-en-ligne.com/profile.php?user=423514
https://www.rossoneriblog.com/author/Mangalistnet
https://www.discogs.com/fr/user/mangalistnet
https://vc.ru/id5911124
https://www.postman.com/mangalistnet
https://www.dday.it/profilo/Mangalistnet
https://muabanhaiduong.com/members/mangalistnet.87405/#about
https://noti.st/mangalistnet
https://monopinion.namur.be/profiles/mangalistnet/activity
https://www.adpost.com/u/mangalistnet/
https://guitarmaking.co.uk/members/mangalistnet/
https://play-uno.com/profile.php?user=423514
https://mangalistnet.shopinfo.jp/posts/58764320
https://definedictionarymeaning.com/user/mangalistnet
https://mangalistnet.amebaownd.com/posts/58766082
https://www.deviantart.com/mangalistnet
https://mangalistnet.bandcamp.com/album/Mangalistnet
https://pastelink.net/gormk3ws
https://www.notion.so/Mangalistnet-34c2a481cac780c39c76e53a294a7745
https://mangalistnet.mssg.me/
https://cannabis.net/user/226191
https://videos.muvizu.com/Profile/Mangalistnet/Latest
https://dev.muvizu.com/Profile/Mangalistnet/Latest/
https://cdn.muvizu.com/Profile/Mangalistnet/Latest/
https://www.muvizu.com/Profile/Mangalistnet/Latest/
https://sketchersunited.org/users/319041
https://jobs.lajobsportal.org/profiles/8190494-mangalistnet
https://mangalistnet.amebaownd.com/posts/58766082
https://hifi.slovanet.sk/bb/profile.php?mode=viewprofile&u=17370
https://urlz.fr/v7yA
https://x.com/mangalistnet
https://hedgedoc.digillab.uni-augsburg.de/s/DiKraeNBOW
https://scrapbox.io/Mangalistnet/Mangalistnet
https://vrcmods.com/user/Mangalistnet
https://oyaschool.com/users/mangalistnet/
https://comicvine.gamespot.com/profile/mangalistnet/
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=228410&tab=field_core_pfield_13
https://forum.ljubavni-oglasnik.net/members/mangalistnet.87556/#about
https://youbiz.com/profile/Mangalistnet
https://vietnam.net.vn/members/mangalistnet.59365/
https://muabanvn.net/members/mangalistnet.32145/#about
https://vipcorel.com/members/mangalistnet.50026/#about
https://congdongketoan.vn/members/mangalistnet.34709/#about
https://diendanit.net/members/mangalistnet.43878/#about
https://nhanxetdanhgia.vn/members/mangalistnet.63193/#about
https://vn-z.vn/members/mangalistnet.352661/#about
https://raovat.trumbansi.net/members/mangalistnet.1885/#about
https://www.dot.com.vn/members/mangalistnet.9700/
https://designerviet.com/members/mangalistnet.100442/#about
https://mangalistnet.mystrikingly.com/
https://www.backabuddy.co.za/campaign/mangalistnet
https://oneeyeland.com/member/member_portfolio.php?pgrid=188256
https://www.mountainproject.com/user/202837383/akimachi-jun
https://www.bestbuydir.com/Mangalistnet_455252.html
https://www.free-weblink.com/Mangalistnet_277304.html
http://www.empregosaude.pt/en/author/Mangalistnet/
https://www.betting-forum.com/members/mangalistnet.157550/#about
https://unsplash.com/fr/@mangalistnet
http://simp.ly/p/47vX0y
https://ja.cofacts.tw/user/Mangalistnet
https://storenvy.com/mangalistnet
https://us.pinterest.com/Mangalistnet/
https://www.insanelymac.com/forum/profile/2748260-mangalistnet/?tab=field_core_pfield_13
https://www.tacter.com/@mangalistnet
https://www.powerelectronicsnews.com/forum/users/akimachijun302/
https://www.hoaxbuster.com/redacteur/Mangalistnet
https://caveduck.io/user/Mangalistnet
https://www.guildlaunch.com/community/users/blog/6753288/?mode=view&gid=535
https://techplanet.today/member/Mangalistnet
https://te.legra.ph/Mangalistnet-04-24
https://relatsencatala.cat/autor/mangalistnet/1063788
https://www.ucplaces.com/profile/103170
https://marriagesofa.com/profile/mangalistnet/
https://qnapandit.com/profile/mangalistnet/
https://approachanxiety.com/forums/users/Mangalistnet/
https://www.tkc-games.com/forums/users/VelizDavid375/
https://ben10club.org/user/mangalistnet
https://www.lola.vn/u/Mangalistnet
https://dati.fondazioneifel.it/user/mangalistnet
https://www.equestrianbookfair.com/Activity-Feed/UserId/4221
https://bb.honorboundgame.com/user-510009.html
https://reduser.net/members/mangalistnet.230038/
https://commoncause.optiontradingspeak.com/index.php/community/profile/Mangalistnet/
https://raovatonline.org/author/mangalistnet/
https://sangtac.waka.vn/author/akimachi-jun-xQ2Kob64rm
https://savvyauthors.com/community/members/exuberant-copper-bunyip.28187/#about
https://vs.cga.gg/user/241840
https://f319.com/members/mangalistnet.1097883/
https://xforum.live/members/mangalistnet.300536/#about
https://rmmedia.ru/members/183709/#about
https://indiasocialbook.com/members/mangalistnet.16571/#about
https://www.prodesigns.com/wordpress-themes/support/users/Mangalistnet
https://devbest.com/members/mangalistnet.152978/#about
https://jobs.host-panel.com/author/mangalistnet/
https://thuthuataccess.com/forum/user-29971.html
https://www.dolibarr.it/fori/users/Mangalistnet/
https://bearfauna.com/forums/users/Mangalistnet/
https://www.skillshot.pl/users/25699
https://pastelink.net/gormk3ws
https://community.poco.in/post/26905
https://www.ibizaclubpt.com/members/mangalistnet.122273/#about
https://pste.link/gormk3ws
https://www.1001fonts.com/users/Mangalistnet/
https://3ddd.ru/users/mangalistnet
https://www.davidrio.com/profile/velizdavid3751686/profile
https://www.remotehub.com/mangalistnet
https://forums.demigodgame.com/user/7661871
https://forums.elementalgame.com/user/7661871
https://www.mynbest.info/profile/velizdavid37582003/profile
https://vhearts.net/Mangalistnet
https://m.xtutti.com/user/profile/488572
https://www.weddingvendors.com/directory/profile/39770/
https://learndash.aula.edu.pe/miembros/mangalistnet/
https://urlscan.io/result/019dbdcc-b70f-7617-a3c7-3f4618d11ec6/
http://bbs.maibu.cc/space-uid-1479288.html
https://party.biz/index.php/profile/381669?tab=541
https://www.pebforum.com/members/mangalistnet.240779/#about
https://expathealthseoul.com/profile/mangalistnet/
https://syosetu.org/?mode=url_jump&url=https://mangalist.net/
https://git.disroot.org/Mangalistnet
https://naijamatta.com/Mangalistnet
https://upuge.com/Mangalistnet
https://paste.lightcast.com/view/0b808cf7
https://hangoutshelp.net/user/Mangalistnet
https://anotepad.com/notes/ywchhm6m
https://destaquebrasil.com/saopaulo/author/Mangalistnet/
https://aboutsnfjobs.com/author/mangalistnet/
https://blooder.net/Mangalistnet
https://dzone.com/users/5521427/mangalistnet.html
https://ofuse.me/mangalistnet
https://participez.villeurbanne.fr/profiles/mangalistnet/activity
http://genina.com/user/editDone/5329915.page
https://photouploads.com/mangalistnet
https://suzuri.jp/Mangalistnet
https://songdew.com/Mangalistnet
https://community.alexgyver.ru/members/mangalistnet.174153/#about
https://ivpaste.com/v/NrgYBvBuXk
https://bioqoo.com/Mangalistnet
https://qoolink.co/Mangalistnet
https://jali.pro/Mangalistnet
https://ngel.ink/Mangalistnet
https://audio.com/mangalistnet
https://participation.bordeaux.fr/profiles/mangalistnet/activity
https://www.4shared.com/u/sM394s2w/VelizDavid375.html
https://www.scener.com/@mangalistnet
http://www.daojianchina.com/home.php?mod=space&uid=1044012
https://coinfolk.net/user/mangalistnet
https://letterboxd.com/Mangalistnet/
https://foss.heptapod.net/Mangalistnet
https://listium.com/@Mangalistnet
https://www.demilked.com/author/Mangalistnet/
https://advego.com/profile/Mangalistnet/
http://baseportal.com/cgi-bin/baseportal.pl?htx=https://mangalist.net/
https://onespotsocial.com/mangalistnet
https://www.mightycause.com/profile/Mangalistnet
http://qa.doujiju.com/index.php?qa=user&qa_1=Mangalistnet
https://culturesbook.com/Mangalistnet
https://participa.gijon.es/profiles/mangalistnet/activity
https://stocktwits.com/Mangalistnet
https://teratail.com/users/Mangalistnet
https://lamsn.com/home.php?mod=space&uid=1983144
https://to-portal.com/Mangalistnet
https://dlive.tv/Mangalistnet
https://docs.google.com/document/d/1zn32G1Gfer2MG30TffjBDD1JILSMy_e3yUD8JYoyddE/edit?usp=sharing
https://www.gamerlaunch.com/community/users/blog/6753288/?mode=view&gid=535
https://kjtr.grrr.jp/kjtr/?Mangalistnet
https://www.am.ics.keio.ac.jp/proj/asap/wiki/?Mangalistnet
https://praca.uxlabs.pl/author/mangalistnet/
https://aboutnursepractitionerjobs.com/author/mangalistnet/
https://www.questmetaldetectors.com/members-area/velizdavid37592071/profile
https://www.tacomaforum.com/members/mangalistnet.148133/#about
https://mangalistnet.blogspot.com/2026/04/mangalistnet.html
https://www.iniuria.us/forum/member.php?675897-Mangalistnet
https://rnmanagers.com/author/mangalistnet/
https://www.instructorsnearme.com/author/mangalistnet/
https://www.floodzonebrewery.com/profile/velizdavid37538307/profile
https://projectnoah.org/users/mangalistnet
https://knowyourmeme.com/users/akimachi-jun
https://topkif.nvinio.com/Mangalistnet
https://purekonect.com/Mangalistnet
https://rndirectors.com/author/mangalistnet/
https://infiniteabundance.mn.co/members/39433416
https://www.hentai-foundry.com/user/Mangalistnet/profile
https://cloutapps.com/Mangalistnet
https://www.xiuwushidai.com/home.php?mod=space&uid=2674709
https://www.saltlakeladyrebels.com/profile/velizdavid37567844/profile
https://pastewall.com/sticker/3d2c1aeaff0b4e198a9c3e78d6dda209
https://www.veteranscup.org/profile/velizdavid37519025/profile
https://www.biblegrove.org/profile/velizdavid37569549/profile
https://forum.prestashop.com/profile/1989011-mangalistnet/?tab=field_core_pfield_19
https://openwhyd.org/mangalistnet
https://searchengines.guru/ru/users/2234091
https://www.rareconnect.org/en/user/Mangalistnet
https://turcia-tours.ru/forum/profile/mangalistnet/
http://www.brenkoweb.com/user/88694/profile
https://faceparty.com/mangalistnet
https://malt-orden.info/userinfo.php?uid=459183
https://www.renderosity.com/users/id:1852194
https://triumph.srivenkateshwaraa.edu.in/profile/mangalistnet
http://gojourney.xsrv.jp/index.php?Mangalistnet
http://freestyler.ws/user/651872/Mangalistnet
https://www.magcloud.com/user/mangalistnet
https://qiita.com/Mangalistnet
https://www.komoot.com/user/5702795479256
https://nous.malakoff.fr/profiles/mangalistnet/activity
https://walling.app/5ftQXUPNXNEB1XObDYO5/mangalistnet
https://notes.bmcs.one/s/5bYm5LykNO
https://bbs.theviko.com/home.php?mod=space&uid=4631969
http://app.gxbs.net/home.php?mod=space&uid=1784505
https://ekcochat.com/Mangalistnet
https://in.enrollbusiness.com/BusinessProfile/7782813/Mangalistnet
https://amvnews.ru/forum/profile.php?mode=viewprofile&u=104564
http://arahn.100webspace.net/profile.php?mode=viewprofile&u=244806
https://www.webmastersun.com/members/mangalistnet.163750/#about
https://photozou.jp/user/top/3449721
http://artutor.teiemt.gr/el/user/mangalistnet/
https://illust.daysneo.com/illustrator/Mangalistnet/
https://hosted.weblate.org/user/Mangalistnet/
http://69e7716250134.site123.me/
https://postr.blog/profile/mangalistnet
https://hostndobezi.com/Mangalistnet
https://www.devglan.com/user/public/velizdavid3752
https://allmylinks.com/mangalistnet
https://congdongx.com/thanh-vien/mangalistnet.48542/#about
https://www.annuncigratuititalia.it/author/Mangalistnet/
https://startupxplore.com/en/person/mangalistnet
https://www.leonidastacticalss.com/profile/velizdavid37533525/profile
https://www.battlakw.com/profile/Mangalistnet/profile
https://www.bridgescdc.com/profile/mangalistnet/profile
https://www.techinasia.com/profile/akimachi-jun
https://www.codingame.com/profile/3889cc70310ee7c4b3251e7c8cbc4f616787327
https://tapas.io/Mangalistnet
https://creator.nightcafe.studio/u/Mangalistnet
https://www.sunemall.com/board/board_topic/8431232/8194152.htm
https://gitlab.haskell.org/Mangalistnet
https://skeptikon.fr/a/mangalistnet/video-channels
https://divinguniverse.com/user/Mangalistnet
https://www.czporadna.cz/user/Mangalistnet
https://buyerseller.xyz/user/mangalistnet/
https://paste.toolforge.org/view/bb72cbb3
https://youslade.com/Mangalistnet
https://www.gamingtop100.net/server/55237/jun-akimachi
https://www.inkitt.com/Mangalistnet
https://participation.touraine.fr/profiles/akimachi_jun/activity
https://flipboard.social/@Mangalistnet
https://sistacafe.com/user/615640
https://pod.beautifulmathuncensored.de/people/32d5f2902072013f95dc021877951523
https://chodilinh.com/members/mangalistnet.301284/#about
https://www.kingmods.net/en/profile/mangalistnet
https://www.hostboard.com/forums/members/mangalistnet.html
https://forum.uookle.com/home.php?mod=space&uid=1389459
https://www.getlisteduae.com/listings/mangalistnet
https://lit.link/en/mangalistnet
https://forum.cnnr.fr/user/mangalistnet
https://forum.pwstudelft.nl/user/mangalistnet
https://sklad-slabov.ru/forum/user/43280/
http://hkeverton.com/forumnew/home.php?mod=space&uid=634976
https://whoosmind.com/Mangalistnet
https://www.siasat.pk/members/mangalistnet.271459/#about
https://mangalistnet2.usluga.me/
https://mangalistnet1.ulcraft.com/
https://mangalistnet.ukit.me/
https://longbets.org/user/Mangalistnet/
https://www.youyooz.com/profile/mangalistnet/
https://www.fullhires.com/author/mangalistnet/
https://ybrclub.com/members/mangalistnet.15532/#about
https://www.themirch.com/blog/author/mangalistnet/
https://its-my.link/@Mangalistnet
https://bkk.tips/forums/users/mangalistnet/
https://www.universe.com/users/mangalistnet-YRN2C1
https://biolinky.co/mangalistnet
https://www.sutori.com/en/story/mangalistnet–eFWVqqaUeARcfBNPTJkduLzg
https://www.telerik.com/forums/profile/52b03438-af1c-4f34-aab4-bd2869e4af9b
https://www.bloggalot.com/profile/mangalistnet
https://analyticsjobs.in/profile/mangalistnet/
https://villatheme.com/supports/users/mangalistnet/
https://www.cryptoispy.com/forums/users/mangalistnet/
https://apify.com/mangalistnet
https://cv.viblo.asia/preview-cv/2e20984f-bfbe-49b7-a175-d8e71b8beed0
https://forums.sorcererking.com/user/7661871
https://forums.galciv2.com/user/7661871
https://forums.gamersbillofrights.com/user/7661871
https://penzu.com/public/8cfb8c9c85419ef4
https://forums.politicalmachine.com/user/7661871
https://webspeed.intensys.pl/wyniki/219010/
https://www.annunciogratis.net/author/Mangalistnet
https://dinosquadsuriku.com/?Mangalistnet
https://ronpaulforums.com/members/mangalistnet.352339/#about
https://drivehud.com/forums/users/velizdavid375/
https://forumserver.twoplustwo.com/members/692635/
https://www.adproceed.com/author/Mangalistnet/
https://www.rctech.net/forum/members/mangalistnet-548609.html
https://scanverify.com/siteverify.php?site=https://mangalist.net/
https://telescope.ac/mangalistnet/mangalistnet
https://ctxt.io/2/AAAEUOrzFg
https://mangalistnet.blogspot.com/2026/04/mangalistnet.html
https://sites.google.com/view/mangalistnet/
https://thaicpe.com/members/mangalistnet.14229/#about
https://www.onetap.com/members/mangalistnet.509153/#about
https://www.dideadesign.com/forum/topic/40765/mangalistnet
https://www.milliescentedrocks.com/board/board_topic/2189097/8209599.htm
https://forumton.org/members/mangalistnet.36154/about
http://www.grandisvietnam.com/members/mangalistnet.29696/#about
https://kotob4all.com/profile/Mangalistnet
https://www.airportcitygame.com/members/mangalistnet.36300/#about
https://sdelai.ru/members/mangalistnet/
https://forums.planetdestiny.com/members/mangalistnet.129777/
https://www.minecraft-servers-list.org/details/Mangalistnet/
https://profiles.xero.com/people/akimachijun
https://californiafilm.ning.com/profile/Mangalistnet
https://aphorismsgalore.com/users/Mangalistnet
https://zb3.org/mangalistnet/ziyunakimachiha-dokokarademoakusesudekirunogamiriyokudesu
https://aboutpharmacistjobs.com/author/mangalistnet/
https://expressafrica.net/Mangalistnet
https://n9.cl/en/r/kh57x
https://forum.gettinglost.ca/user/mangalistnet
https://linkdirectorynet.com/listings13555331/jun-akimachi
https://findnerd.com/profile/publicprofile/Mangalistnet/158262
https://blog.ss-blog.jp/_pages/mobile/step/index?u=https://mangalist.net/
https://aboutnursernjobs.com/author/mangalistnet/
https://www.dcfever.com/users/profile.php?id=1276420
https://nilechronicles.com/profile/mangalistnet
https://www.physicsoverflow.org/user/Mangalistnet
https://recash.wpsoul.net/members/mangalistnet/
https://radio.immo/user/1-6227-Akimachi-Jun
https://pixelfed.tokyo/Mangalistnet
https://bbarlock.com/index.php/User:Mangalistnet
https://775585.8b.io/
http://www.in-almelo.com/User-Profile/userId/2415276
https://mokum.place/mangalistnet
https://nyccharterschools.jobboard.io/employers/4125359-mangalistnet
https://outdoor.surselva.info/en/member/akimachi-jun/339504082/
https://www.minecraftforum.net/members/Mangalistnet
https://www.bat-safe.com/profile/Mangalistnet/profile
https://www.jmriascos.space/profile/Mangalistnet/profile
https://forums.littletinyfrogs.com/user/7661871
https://speakerdeck.com/mangalistnet
https://www.adsfare.com/mangalistnet
https://forums.redflagdeals.com/members/mangalistnet-1803171/
https://stackshare.io/velizdavid375/mangalistnet
http://nao.earth/index.php?Mangalistnet
http://web.symbol.rs/forum/member.php?action=profile&uid=1270156
https://anunt-imob.ro/user/profile/855679
https://www.highpriceddatinguk.com/Mangalistnet
https://www.directorylib.com/domain/mangalist.net
https://www.lasallesancristobal.edu.mx/profile/Mangalistnet/profile
https://pad.deckenpfronn.info/s/_bBZO7qcf
https://creativemornings.com/individuals/mangalistnet
https://whitehat.vn/members/mangalistnet.227084/#about
https://go.famuse.co/Mangalistnet
https://www.ltstesting.com/profile/Mangalistnet/profile
https://www.housedumonde.com/profile/Mangalistnet/profile
https://www.harimajuku.com/profile/Mangalistnet/profile
https://www.happycampersmontessori.com/profile/Mangalistnet/profile
https://www.miseducationofmotherhood.com/profile/Mangalistnet/profile
https://www.salmonshop.ca/profile/Mangalistnet/profile
https://www.newdirectionchildcarefacility.com/profile/mangalistnet/profile
https://www.walleyecentral.com/forums/member.php?u=361579
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu baik. Bye
Your comment is awaiting moderation.
https://www.facebook.com/pk888slotscom
https://www.youtube.com/@pk888slotscom
https://twitter.com/pk888slotscom
https://tooter.in/pk888slotscom
https://wakelet.com/@pk888slotscom
https://safechat.com/u/pk888slotscom
https://gravatar.com/pk888slotscom
https://www.mymeetbook.com/pk888slotscom
https://www.pinterest.com/pk888slotscom/
https://band.link/pk888slotscom
https://community.wongcw.com/pk888slotscom
https://demo.wowonder.com/pk888slotscom
https://shareyoursocial.com/pk888slotscom
https://myspace.com/pk888slotscom
https://500px.com/p/pk888slotscom
https://www.instapaper.com/p/pk888slotscom
https://magic.ly/pk888slotscom
https://www.band.us/@pk888slotscom
https://sketchfab.com/pk888slotscom
https://www.reddit.com/user/pk888slotscom/
https://audiomack.com/pk888slotscom
https://hackaday.io/pk888slotscom
https://leetcode.com/u/pk888slotscom/
https://swag.live/en/user/69e63c54cb675e2b2013b212
https://www.halaltrip.com/user/profile/340250/pk888slotscom/
https://medibang.com/author/28170365/
https://www.blockdit.com/pk888slotscom
https://portfolium.com/pk888slotscom
https://www.twitch.tv/pk888slotscom/about
https://profile.hatena.ne.jp/pk888slotscom/
https://issuu.com/pk888slotscom
https://www.behance.net/pk888slotscom
https://www.reverbnation.com/artist/pk888slotscom
https://www.investagrams.com/Profile/pk888slotscom
https://gifyu.com/pk888slotscom
https://www.chordie.com/forum/profile.php?id=2510681
https://www.walkscore.com/people/308479859164/pk888slotscom
https://topsitenet.com/profile/pk888slotscom/1640797/
https://akniga.org/profile/1415494-pk888slotscom/
https://jobs.suncommunitynews.com/profiles/8173769-pk-888
https://www.speedrun.com/users/pk888slotscom
https://www.fanart-central.net/user/pk888slotscom/profile
https://slides.com/pk888slotscom
https://www.aicrowd.com/participants/pk888slotscom
https://pbase.com/pk888slotscom/inbox
https://hub.docker.com/u/pk888slotscom
https://spiderum.com/nguoi-dung/pk888slotscom
https://zaidap.com/thong-tin-ca-nhan-u107365.htm
https://www.gta5-mods.com/users/pk888slotscom
https://heylink.me/pk888slotscom/
https://pixabay.com/users/pk888slotscom-55522267/
https://www.nicovideo.jp/user/143986434
https://www.jigsawplanet.com/pk888slotscom
https://3dwarehouse.sketchup.com/by/pk888slotscom
https://bit.ly/m/pk888slotscom
https://joy.link/pk888slotscom
https://connect.garmin.com/app/profile/769d70a3-338e-4ad0-a000-28161e53e360
https://b.hatena.ne.jp/pk888slotscom/bookmark
https://www.chichi-pui.com/users/pk888slotscom/
https://www.openrec.tv/user/pk888slotscom/about
https://unityroom.com/users/pk888slotscom
https://routinehub.co/user/pk888slotscom
https://pxhere.com/en/photographer-me/4987732
https://teletype.in/@pk888slotscom
https://www.checkli.com/pk888slotscom
https://gitee.com/pk888slotscom
https://www.fuelly.com/driver/pk888slotscom
https://www.nintendo-master.com/profil/pk888slotscom
https://freeimage.host/pk888slotscom
https://www.diigo.com/profile/pk888slotscom
https://fontstruct.com/fontstructions/show/2868398/pk888-1
https://linkin.bio/pk888slotscom/
https://biomolecula.ru/authors/141879
https://www.callupcontact.com/b/businessprofile/pk888slotscom/10058087
https://www.growkudos.com/profile/pk_888
https://blender.community/pk888slotscom/
https://sciter.com/forums/users/pk888slotscom/
https://matkafasi.com/user/pk888slotscom
https://allmyfaves.com/pk888slotscom
https://www.abclinuxu.cz/lide/pk888slotscom
https://dumagueteinfo.com/author/pk888slotscom/
https://muare.vn/shop/pk888slotscom/902458
https://doodleordie.com/profile/pk888slotscom
https://musikersuche.musicstore.de/profil/pk888slotscom/
https://www.intensedebate.com/people/pk888slotscom1
https://lookingforclan.com/user/pk888slotscom
https://forum.dmec.vn/index.php?members/pk888slotscom.187519/
https://igli.me/pk888slotscom
https://duyendangaodai.net/members/31588-pk888slo.html
https://freestyler.ws/user/650404/pk888slotscom
http://delphi.larsbo.org/user/pk888slotscom
https://www.aseeralkotb.com/en/profiles/pk888slotscom
https://timdaily.vn/members/pk888slotscom.134097/#about
https://app.readthedocs.org/profiles/pk888slotscom/
https://www.dibiz.com/omarkraus693
https://iszene.com/user-347680.html
https://desksnear.me/users/pk888slotscom
https://www.itchyforum.com/en/member.php?388182-pk888slotscom
https://bachhoadep.com/members/23238-pk888slo.html
https://www.roton.com/forums/users/omarkraus693/
https://able2know.org/user/pk888slotscom/
http://www.biblesupport.com/user/831467-pk888slotscom/
https://golosknig.com/profile/pk888slotscom/
https://www.anibookmark.com/user/pk888slotscom.html
https://www.inventoridigiochi.it/membri/pk888slotscom/profile/
https://forum.m5stack.com/user/pk888slotscom
https://wallhaven.cc/user/pk888slotscom
https://imageevent.com/pk888slotscom/pk888slotscom?q=1100
https://old.bitchute.com/channel/GwlvMsZ1RqO7/
https://bandori.party/user/794419/pk888slotscom/
https://community.m5stack.com/user/pk888slotscom
https://schoolido.lu/user/pk888slotscom/
https://awan.pro/forum/user/165701/
https://fortunetelleroracle.com/profile/pk888slotscom
https://fabble.cc/pk888slotscom
https://affariat.com/user/profile/179271
https://community.cisco.com/t5/user/viewprofilepage/user-id/2068068
https://kr.pinterest.com/pk888slotscom/
https://pt.gravatar.com/pk888slotscom
https://th.gravatar.com/pk888slotscom
https://www.sythe.org/members/pk888slotscom.2039843/
https://f319.com/members/pk888slotscom.1097603/
https://about.me/pk888slotscom
https://www.canadavisa.com/canada-immigration-discussion-board/members/pk888slotscom.1353622/#about
https://www.equinenow.com/farm/pk888slotscom.htm
https://wefunder.com/pk888slotscom/about
https://transfur.com/Users/pk888slotscom
https://xtremepape.rs/members/pk888slotscom.665989/#about
https://github.com/pk888slotscom
https://myanimelist.net/profile/pk888slotscom
https://qna.habr.com/user/pk888slotscom
https://website.informer.com/pk888-slots.com
https://lightroom.adobe.com/u/pk888slotscom
https://beacons.ai/pk888slotscom
https://en.islcollective.com/portfolio/12903409
https://www.xosothantai.com/members/pk888slotscom.609339/
https://velog.io/@pk888slotscom/about
https://violet.vn/user/show/id/15267893
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3942134
https://mez.ink/pk888slotscom
https://notionpress.com/author/1508314
https://www.edna.cz/uzivatele/pk888slotscom/
https://digiphoto.techbang.com/users/pk888slotscom
https://leakedmodels.com/forum/members/pk888slotscom.708962/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1066475
https://freeicons.io/profile/921139
https://inkbunny.net/pk888slotscom
https://www.japaaan.com/user/77011
https://spinninrecords.com/profile/pk888slotscom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/pk.888
https://code.antopie.org/pk888slotscom
https://www.techbang.com/users/pk888slotscom
https://es.pinterest.com/pk888slotscom/
https://id.pinterest.com/pk888slotscom/
https://mx.pinterest.com/pk888slotscom/
https://beatsaver.com/playlists/1181805
https://dialog.eslov.se/profiles/pk888slotscom/activity
https://www.storenvy.com/pk888slotscom
https://participacion.cabildofuer.es/profiles/pk888slotscom/activity
https://forums.maxperformanceinc.com/forums/member.php?u=246530
https://egl.circlly.com/users/pk888slotscom
https://acomics.ru/-pk888slotscom
https://hanson.net/users/pk888slotscom
https://writexo.com/share/2e02c6c14190
https://www.laundrynation.com/community/profile/pk888slotscom/
https://www.heavyironjobs.com/profiles/8175534-pk888-slotscom
https://pad.degrowth.net/s/1VuzcHXC1
https://fr.pinterest.com/pk888slotscom/
http://fort-raevskiy.ru/community/profile/pk888slotscom/
https://forum.skullgirlsmobile.com/members/pk888slotscom.215289/#about
https://jobs.landscapeindustrycareers.org/profiles/8175567-pk888-slotscom
https://phatwalletforums.com/user/pk888slotscom
https://forums.galciv4.com/user/7660937
https://song.link/pk888slotscom
https://idol.st/user/164980/pk888slotscom/
https://www.valinor.com.br/forum/usuario/pk888slotscom.145154/#about
https://tulieu.violet.vn/user/show/id/15267893
https://www.bmwpower.lv/user.php?u=pk888slotscom
https://gockhuat.net/member.php?u=436911
https://jobs.windomnews.com/profiles/8175637-pk888-slotscom
https://hoaxbuster.com/redacteur/pk888slotscom
https://www.givey.com/pk888slotscom
https://talkmarkets.com/profile/pk888slotscom
https://forums.stardock.com/user/7660937
https://zerosuicidetraining.edc.org/user/profile.php?id=560231
https://www.telix.pl/forums/users/pk888slotscom/
https://joinentre.com/profile/pk888slotscom
https://uk.pinterest.com/pk888slotscom/
https://cl.pinterest.com/pk888slotscom/
https://jobs.westerncity.com/profiles/8175661-pk888-slotscom
https://www.thetriumphforum.com/members/pk888slotscom.62841/
https://gamblingtherapy.org/forum/users/pk888slotscom/
https://l2top.co/forum/members/pk888slotscom.173054/
http://www.askmap.net/location/7793305/brazil/pk888
https://graphcommons.com/graphs/5f09f2f3-17e1-402e-8069-4ebfc256488f
https://forums.galciv3.com/user/7660937
https://galleria.emotionflow.com/183017/profile.html
https://www.myget.org/users/pk888slotscom
https://app.brancher.ai/user/q0VtuyrXau-r
https://justpaste.me/F3pt
https://forums.sinsofasolarempire2.com/user/7660937
https://www.empregosaude.pt/en/author/pk888slotscom/
https://confengine.com/user/pk888slotscom
https://slideslive.com/pk888slotscom?tab=about
https://mygamedb.com/profile/pk888slotscom
https://buckeyescoop.com/community/members/pk888slotscom.62526/#about
https://forums.ashesofthesingularity.com/user/7660937
https://forum.aceinna.com/user/pk888slotscom
https://www.mateball.com/pk888slotscom
https://web-tourist.net/members/pk888slotscom.52805/#about
https://toirscript.com/user/pk888slotscom
https://at.pinterest.com/pk888slotscom/
https://dk.pinterest.com/pk888slotscom/
https://forum.pabbly.com/members/pk888slotscom.112343/#about
http://forum.cncprovn.com/members/424292-pk888slotscom
https://ncnews.co/profile/pk888slotscom
https://dreevoo.com/profile_info.php?pid=1522592
https://forum.aigato.vn/user/pk888slotscom
https://amaz0ns.com/forums/users/pk888slotscom/
https://rapidapi.com/user/pk888slotscom
https://www.skool.com/@pk-slotscom-8849
https://learningapps.org/watch?v=phihwfbdc26
https://coub.com/pk888slotscom
https://www.giveawayoftheday.com/forums/profile/1807932
http://onlineboxing.net/jforum/user/profile/446486.page
https://www.invelos.com/UserProfile.aspx?Alias=pk888slotscom
https://www.video-bookmark.com/bookmark/7109012/pk888slotscom/
https://wibki.com/pk888slotscom
https://twitback.com/pk888slotscom
https://krachelart.com/UserProfile/tabid/43/userId/1342735/Default.aspx
https://gitlab.vuhdo.io/pk888slotscom
https://www.11secondclub.com/users/profile/1712631
https://aniworld.to/user/profil/pk888slotscom
https://s.id/pk888slotscom
https://kktix.com/user/8668693
https://www.passes.com/pk888slotscom
https://poipiku.com/13494303/
https://uiverse.io/profile/pk888slots_2251
https://www.rwaq.org/users/pk888slotscom
https://www.fitday.com/fitness/forums/members/pk888slotscom.html
https://www.fundable.com/pk-888
https://vcook.jp/users/87457
https://www.grepmed.com/pk888slotscom
https://classificados.acheiusa.com/profile/RmlML1ZyZ29TYWcwMUYwdDJpcEhTYWxZbVFvY0hGMVJhNHdFQlFTMG85Yz0=
https://espritgames.com/members/50817781/
https://cgmood.com/pk888slotscom
https://www.haikudeck.com/presentations/pk888slotscom
https://www.efunda.com/members/people/show_people.cfm?Usr=pk888slotscom
https://diit.cz/profil/kbqx2ff5y5
https://backloggery.com/pk888slotscom
https://raovat.nhadat.vn/members/pk888slotscom-305883.html
https://www.moshpyt.com/user/pk888slotscom
https://www.koi-s.id/member.php?332342-pk888slotscom
https://www.ekdarun.com/forum/topic/153590/pk888
https://www.driedsquidathome.com/forum/topic/142166/pk888
https://www.navacool.com/forum/topic/392572/pk888
https://www.natthadon-sanengineering.com/forum/topic/102654/pk888
https://www.bonback.com/forum/topic/392575/pk888
https://que.u.nosv.org/profile?user=pk888slotscom
https://secondstreet.ru/profile/pk888slotscom/
https://forum.fakeidvendors.com/user/pk888slotscom
https://scenarch.com/userpages/33349
https://undrtone.com/pk888slotscom
https://marshallyin.com/members/pk888slotscom/
https://us.enrollbusiness.com/BusinessProfile/7781138/pk888slotscom
https://www.atozed.com/forums/user-77468.html
https://searchengines.bg/members/pk888slotscom.26182/#about
https://luvly.co/users/pk888slotscom
https://hukukevi.net/user/pk888slotscom
https://belgaumonline.com/profile/pk888slotscom/
https://savelist.co/profile/users/pk888slotscom
https://usdinstitute.com/forums/users/pk888slotscom/
https://www.montessorijobsuk.co.uk/author/pk888slotscom/
https://www.apsense.com/user/pk888slotscom
https://zzb.bz/SlinzP
https://draft.blogger.com/profile/06074564600710090692
https://boldomatic.com/view/writer/pk888slotscom
https://hack.allmende.io/s/lSQYVZGTs9
https://pad.codefor.fr/s/GkvOng-_7E
https://hackmd.hub.yt/s/uGFkjtUZm
https://www.themeqx.com/forums/users/pk888slotscom/
https://www.udrpsearch.com/user/pk888slotscom
https://www.xen-factory.com/index.php?members/pk888slotscom.154692/#about
https://cointr.ee/pk888slotscom
https://forums.servethehome.com/index.php?members/pk888slotscom.238862/#about
https://jaga.link/pk888slotscom
https://b.io/pk888slotscom
https://www.blackhatprotools.info/member.php?287307-pk888slotscom
https://activepages.com.au/profile/pk888slotscom
https://snippet.host/xsnzjy
https://tudomuaban.com/chi-tiet-rao-vat/2883344/pk888.html
https://phijkchu.com/a/pk888slotscom/video-channels
https://lifeinsys.com/user/pk888slotscom
https://bioqoo.com/pk888slotscom
https://kaeuchi.jp/forums/users/pk888slotscom/
https://www.claimajob.com/profiles/8176052-pk888-slotscom
https://protospielsouth.com/user/129883
https://theafricavoice.com/profile/pk888slotscom
http://palangshim.com/space-uid-5108648.html
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:F3D9813469E652F10A495FC0@AdobeID
https://vi.gravatar.com/pk888slotscom
https://www.mixcloud.com/pk888slotscom/
https://www.designspiration.com/pk888slotscom/saves/
https://qoolink.co/pk888slotscom
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=194327
https://hub.vroid.com/en/users/125592485
https://forum.codeigniter.com/member.php?action=profile&uid=233712
https://etextpad.com/k0ysvjbqvg
https://app.talkshoe.com/user/pk888slotscom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=229167
https://ngel.ink/pk888slotscom
https://m.wibki.com/pk888slotscom
https://www.pageorama.com/?p=pk888slotscom
https://jali.pro/pk888slotscom
https://bandsworksconcerts.info/index.php?pk888slotscom
https://bbs.mikocon.com/home.php?mod=space&uid=290163
https://www.mikocon.com/home.php?mod=space&uid=290163
https://jerseyboysblog.com/forum/member.php?action=profile&uid=91680
https://www.quora.com/profile/Pk888slotscom
https://manylink.co/@pk888slotscom
https://www.freewebspace.net/forums/index.php?members/pk888slotscom.17034542/#about
https://forums.giantitp.com/member.php?373753-pk888slotscom
https://seomotionz.com/member.php?action=profile&uid=127940
https://anyflip.com/homepage/akies#About
https://www.akaqa.com/question/q19192673363-Pk888
https://londonchinese.com/home.php?mod=space&uid=620604&do=profile
https://copynotes.be/shift4me/forum/user-52300.html
https://scholar.google.com/citations?hl=en&user=Z0ZhhLUAAAAJ
https://www.threadless.com/@pk888slotscom/activity
https://tabelog.com/rvwr/pk888slotscom/prof/
https://coolors.co/u/pk888slotscom
https://www.beamng.com/members/pk888slotscom.788953/
https://civitai.com/user/pk888slot
https://www.spigotmc.org/members/pk888slotscom.2522456/
https://boosty.to/pk888slotscom
https://camp-fire.jp/profile/pk888slotscom
https://feyenoord.supporters.nl/profiel/148277/pk888slotscom
https://www.pearltrees.com/pk888slotscom/item792635154
https://gesoten.com/profile/detail/12749739
https://rekonise.com/u/pk888slotscom
https://hashnode.com/@pk888slotscom
https://hoo.be/pk888slotscom
https://nhattao.com/members/user6955457.6955457/
https://maxforlive.com/profile/user/pk888slotscom?tab=about
https://3dtoday.ru/blogs/pk888slotscom
https://opencollective.com/pk888slotscom
https://pinshape.com/users/8952600-pk888slotscom
https://morguefile.com/creative/pk888slotscom
https://edabit.com/user/7Aowo4X7ggkTeXu5L
https://mathlog.info/users/qlqRKJuMBuN0bxLE1WGpub5SsMy1
https://securityheaders.com/?q=https://pk888-slots.com/
https://allmylinks.com/pk888slotscom
https://my.bio/pk888slotscom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/150900
https://sfx.thelazy.net/users/u/pk888slotscom/
https://forum.reallusion.com/Users/3286378/omarkraus693
https://app.daily.dev/pk888slotscom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=259181
https://www.skypixel.com/users/djiuser-lixkpuyiey0l
https://webanketa.com/forms/6mv3je1m6gqk4e34c5j32eb6/
https://www.pdc.edu/?URL=https://pk888-slots.com/
https://ask.mallaky.com/?qa=user/pk888slotscom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=79877
https://sub4sub.net/forums/users/pk888slotscom/
https://www.slmath.org/people/105308
https://userstyles.world/user/pk888slotscom
https://goo.by/DxawYM
https://bresdel.com/pk888slotscom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=13700
https://fora.babinet.cz/profile.php?id=123652
https://pledgeme.co.nz/profiles/331591/
https://pk888slotscom.notepin.co/
https://pictureinbottle.com/r/pk888slotscom
https://forum.epicbrowser.com/profile.php?id=151876
http://www.dungdong.com/home.php?mod=space&uid=3365441
https://forum.herozerogame.com/index.php?/user/161835-pk888slotscom/
https://shhhnewcastleswingers.club/forums/users/pk888slotscom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2468079
https://connect.gt/user/pk888slotscom
https://forum.tkool.jp/index.php?members/pk888slotscom.105632/#about
https://www.divephotoguide.com/user/pk888slotscom
https://www.weddingbee.com/members/pk888slotscom/
https://kumu.io/pk888slotscom/pk888slotscom#pk888
https://b.cari.com.my/home.php?mod=space&uid=3398048&do=profile
https://bioimagingcore.be/q2a/user/pk888slotscom
https://www.sunlitcentrekenya.co.ke/author/pk888slotscom/
https://pk888slotscom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/pk888slotscom/activity
https://www.rcuniverse.com/forum/members/pk888slotscom.html
https://www.huntingnet.com/forum/members/pk888slotscom.html
https://www.socialbookmarkssite.com/bookmark/6239102/pk888slotscom/
https://www.hogwartsishere.com/1834968/
https://vimeo.com/pk888slotscom
https://gitlab.com/pk888slotscom
https://www.bricklink.com/aboutMe.asp?u=pk888slotscom
https://zealy.io/cw/pk888slotscom/questboard/
https://www.france-ioi.org/user/perso.php?sLogin=pk888slotscom
https://mt2.org/uyeler/pk888slotscom.39114/#about
https://www.trackyserver.com/profile/246170
https://www.pintradingdb.com/forum/member.php?action=profile&uid=143290
https://md.chaosdorf.de/s/QIFU-bgSRP
https://md.openbikesensor.org/s/H3Zo6SqSl6
https://doc.adminforge.de/s/53onDK6GSL
https://www.plotterusati.it/user/pk888slotscom
https://tutorialslink.com/member/pk888slotscomundefined/98419
https://www.buzzbii.com/pk888slotscom
https://www.vid419.com/home.php?mod=space&uid=3486355
https://forum.ct8.pl/member.php?action=profile&uid=121806
https://devfolio.co/@pk888slotscom/readme-md
https://linqto.me/n/pk888slotscom
https://www.mindomo.com/mindmap/07a700c9f82c45d183edffda671b1cd8
https://www.goodolcomics.com/blog/profile/pk888slotscom/
https://www.swap-bot.com/user:pk888slotscom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=391437
http://techou.jp/index.php?pk888slotscom
https://epiphonetalk.com/members/pk888slotscom.97301/#about
https://forums.megalith-games.com/member.php?action=profile&uid=1451049
http://tkdlab.com/wiki/index.php?pk888slotscom
https://www.managementpedia.com/members/pk888slotscom.1120444/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=634521
https://volleypedia.org/index.php?qa=user&qa_1=pk888slotscom
http://pcsq28.com/home.php?mod=space&uid=1951476
https://bbs.airav.cc/home.php?mod=space&uid=4577262
https://hker2uk.com/home.php?mod=space&uid=5486319
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=494389
https://aprenderfotografia.online/usuarios/pk888slotscom/profile/
https://pads.zapf.in/s/4KoteySisP
https://pad.darmstadt.social/s/BNGUtGF9rL
http://galeria.farvista.net/member.php?action=showprofile&user_id=76720
https://tilengine.org/forum/member.php?action=profile&uid=163980
https://www.play56.net/home.php?mod=space&uid=6136779
https://md.swk-web.com/s/ERc8UJndb
https://hedgedoc.dezentrale.space/s/1ps2oHxOh
https://ar.gravatar.com/pk888slotscom
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3306782
https://replit.com/@pk888slotscom
https://odesli.co/pk888slotscom
https://wandb.ai/profile/pk888slotscom
https://divisionmidway.org/jobs/author/pk888slotscom/
https://bbcovenant.guildlaunch.com/users/blog/6752917/?mode=view&gid=97523
https://www.wowonder.xyz/pk888slotscom
https://sciencemission.com/profile/pk888slotscom
http://jobboard.piasd.org/author/pk888slotscom/
https://www.wvhired.com/profiles/8178641-pk888-slotscom
https://kenhrao.com/members/pk888slotscom.121123/#about
http://jobs.emiogp.com/author/pk888slotscom/
https://ismschools.com.au/forums/users/pk888slotscom/
https://onlinevetjobs.com/author/pk888slotscom/
https://v.gd/hRAtnb
https://gl.gta5-mods.com/users/pk888slotscom
https://www.fruitpickingjobs.com.au/forums/users/pk888slotscom/
http://www.webclap.com/php/jump.php?url=https://pk888-slots.com/
https://xoops.ec-cube.net/userinfo.php?uid=348526
https://formulamasa.com/elearning/members/pk888slotscom/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1108222
https://quangcaoso.vn/pk888slotscom
https://tawk.to/pk888slotscom
https://chyoa.com/user/pk888slotscom
https://forum.flashphoner.com/members/pk888slotscom.46098/#about
https://www.royalroad.com/profile/957743
https://backloggd.com/u/pk888slotscom/
https://kenhsinhvien.vn/m/pk888slotscom.1167353/#about
https://form.jotform.com/261104297323047
https://forums.alliedmods.net/member.php?u=476116
https://aiforkids.in/qa/user/pk888slotscom1
https://www.warriorforum.com/members/pk888slotscom.html
https://community.jmp.com/t5/user/viewprofilepage/user-id/97200
https://digiex.net/members/pk888slotscom.144686/
https://smallseo.tools/website-checker/pk888-slots.com
https://bwinglive.lighthouseapp.com/users/1997309
https://rush1989.rash.jp/pukiwiki/index.php?pk888slotscom
https://viblo.asia/u/pk888slotscom/contact
https://wikimapia.org/external_link?url=https://pk888-slots.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6397701
https://www.thesims3.com/myBlog.html?persona=pk888slotscom
https://runtrip.jp/users/771920
https://campsite.bio/pk888slotscom
https://reactormag.com/members/pk888slotscom/
https://www.emailsherlock.com/hosts/pk888-slots.com/
https://www.promoteproject.com/user/pk888slotscom/
https://ikanakama.ink/users/341370
https://www.prosebox.net/book/107817/
https://ticketme.io/account/pk888slotscom
https://task.tw/users/TGJYSEI/freelancer
https://log.concept2.com/profile/2923271
https://www.speedway-world.pl/forum/member.php?action=profile&uid=472101
https://cds.zju.edu.cn/addons/cms/go/index.html?url=https://pk888-slots.com/
http://forum.orangepi.org/home.php?mod=space&uid=6397701
https://redirect.camfrog.com/redirect/?url=https://pk888-slots.com/
https://www.hobowars.com/game/linker.php?url=https://pk888-slots.com/
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=469406&sid=dfa8b34aa6e943433834429e76b1d720
https://forum.honorboundgame.com/user-509799.html
https://elovebook.com/pk888slotscom
https://propterest.com.au/user/80911/pk888slotscom
https://www.fw-follow.com/forum/topic/116395/pk888
https://www.jk-green.com/forum/topic/110118/pk888
https://www.nongkhaempolice.com/forum/topic/122679/pk888
https://www.bestloveweddingstudio.com/forum/topic/82539/pk888
https://www.rueanmaihom.net/forum/topic/97826/pk888
https://www.ttlxshipping.com/forum/topic/393520/pk888
http://forum.modulebazaar.com/forums/user/pk888slotscom/
https://user.linkdata.org/user/pk888slotscom/work
https://calaos.fr/forum/member.php?action=profile&uid=19923
https://www.vrwant.org/wb/home.php?mod=space&uid=5094173
https://forum.hkcinema.ru/profile.php?section=about&id=73549
https://www.rcmx.net/userinfo.php?uid=16677
https://www.pathumratjotun.com/forum/topic/176963/pk888
https://maychetao.com/members/21148-pk888slo.html
https://forum.web-z.net/profile.php?userid=9840
https://usabbs.org/home.php?mod=space&uid=87563
https://lqdoj.edu.vn/user/pk888slotscom
https://paperjale.eus/user/pk888slotscom
http://byltz.com/home.php?mod=space&uid=481375
https://indiestorygeek.com/user/pk888slotscom
https://www.bandlab.com/pk888slotscom
https://www.livelib.ru/reader/pk888slotscom
https://forum.issabel.org/u/pk888slotscom
https://www.siye.co.uk/siye/viewuser.php?uid=250019
https://www.casualgamerevolution.com/user/pk888slotscom
https://raredirectory.com/author/pk888slotscom-49783/
https://www.iglinks.io/omarkraus693-f5p?preview=true
https://decidim.calafell.cat/profiles/pk888slotscom/activity
https://www.keepandshare.com/discuss2/46180/pk888
http://bbs.medicalforum.cn/home.php?mod=space&uid=2231049
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://pk888-slots.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3398048&do=profile
https://giaoan.violet.vn/user/show/id/15267893
https://anh135689999.violet.vn/user/show/id/15267893
https://profiles.delphiforums.com/n/pfx/profile.aspx?webtag=dfpprofile000&userId=1891283692
https://hu.gta5-mods.com/users/pk888slotscom
https://uk.gta5-mods.com/users/pk888slotscom
https://sl.gta5-mods.com/users/pk888slotscom
https://www.easyhits4u.com/profile.cgi?login=pk888slotscom
https://in.pinterest.com/pk888slotscom/
https://doc.anagora.org/s/hyaJGpNAe
https://album.link/pk888slotscom
https://artist.link/pk888slotscom
https://pods.link/pk888slotscom
https://mylink.page/pk888slotscom
https://playlist.link/pk888slotscom
https://portfolium.com.au/pk888slotscom
https://profile.sampo.ru/pk888slotscom
https://mail.londonchinese.com/home.php?mod=space&uid=620604&do=profile
https://hoctructuyen.violet.vn/user/show/id/15267893
https://baigiang.violet.vn/user/show/id/15267893
http://www.muzikspace.com/profiledetails.aspx?profileid=135787
https://forums.starcontrol.com/user/7660937
https://forums.offworldgame.com/user/7660937
https://www.dideadesign.com/forum/topic/40236/pk888
https://hi.gta5-mods.com/users/pk888slotscom
https://it.gta5-mods.com/users/pk888slotscom
https://nl.gta5-mods.com/users/pk888slotscom
https://no.gta5-mods.com/users/pk888slotscom
https://pl.gta5-mods.com/users/pk888slotscom
https://pt.gta5-mods.com/users/pk888slotscom
https://www.lectoreselectronicos.com/foro/member.php?21966-pk888slotscom
https://fanclove.jp/profile/90WwgDKbWP
https://truckymods.io/user/486947
https://substack.com/@pk888slotscom
http://forum.vodobox.com/profile.php?id=69042
https://forums.sinsofasolarempire.com/user/7660937
https://forums.stardock.net/user/7660937
https://forum.findukhosting.com/index.php?action=profile;area=forumprofile;u=75502
https://www.expat.com/forum/profile.php?id=3956217&lang=en
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=228128
https://www.dokkan-battle.fr/forums/users/pk888slotscom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3398048&do=profile
https://mforum3.cari.com.my/home.php?mod=space&uid=3398048&do=profile
https://animeforums.net/profile/53971-pk888slotscom/?tab=field_core_pfield_1
https://www.d-ushop.com/forum/topic/128585/pk888
https://www.templepurohit.com/forums/users/omarkraus693/
https://www.fanfiction.net/u/16909733/
https://www.kickstarter.com/profile/pk888slotscom/about
https://www.noteflight.com/profile/7781f908a36c227dd9565b575bb0b72d164d1b7d
https://www.horticulturaljobs.com/employers/4120450-pk888slotscom
https://johsocial.com/story12030478/pk888slotscom
https://jobs.siliconflorist.com/employers/4120449-pk888slotscom
https://jobs.nefeshinternational.org/employers/4120448-pk888slotscom
https://aboutcasemanagerjobs.com/author/pk888slotscom/
https://biashara.co.ke/author/pk888slotscom/
https://buyandsellhair.com/author/pk888slotscom/
https://cornucopia.se/author/pk888slotscom/
https://colorswall.com/users/32923
https://bookmeter.com/users/1711640
https://lustyweb.live/members/pk888slotscom.119176/#about
https://6giay.vn/members/pk888slotscom.101876/#about
https://findaspring.org/members/pk888slotscom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=777902
https://careers.coloradopublichealth.org/profiles/8179063-pk888-slotscom
https://gorillasocialwork.com/story26802768/pk888slotscom
https://homepage.ninja/pk888slotscom
https://propeller.hu/tagok/pk888slotscom/adatlap
https://promosimple.com/ps/4854d/pk888
https://datcang.vn/viewtopic.php?f=7&t=933206
https://dienbd.violet.vn/user/show/id/15267893
https://memmai.com/index.php?members/pk888slotscom.41915/#about
https://kttm.club/members/pk888slotscom.4912/#about
https://vn-zom.com/members/pk888slotscom.5795/
https://vietcurrency.vn/members/pk888slotscom.239531/#about
https://zh-tw.gravatar.com/pk888slotscom
https://sv.gravatar.com/pk888slotscom
https://po.gravatar.com/pk888slotscom
https://oc.gravatar.com/pk888slotscom
https://ko.gravatar.com/pk888slotscom
https://vnbit.org/members/pk888slotscom.94349/#about
https://boss.why3s.cc/boss/home.php?mod=space&uid=262373
https://clusterbusters.org/forums/profile/35523-pk888slotscom/?tab=field_core_pfield_11
https://community.goldposter.com/members/pk888slotscom/
https://fengshuidirectory.com/dashboard/listings/pk888slotscom/
https://pets4friends.com/profile-1579209
https://staroetv.su/go?https://pk888-slots.com/
https://www.ixawiki.com/link.php?url=https://pk888-slots.com/
https://www.shinobi.jp/etc/goto.html?https://pk888-slots.com/
https://oye.participer.lyon.fr/profiles/pk888slotscom/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345881
https://axe.rs/forum/members/pk888slotscom.13426269/#about
https://co-roma.openheritage.eu/profiles/pk888slotscom/activity
https://postr.yruz.one/profile/pk888slotscom
https://openlibrary.org/people/pk888slotscom
https://chodaumoi247.com/members/pk888slotscom.51341/#about
https://aiti.edu.vn/members/pk888slotscom.43354/
https://tinhte.vn/members/pk888slotscom.3388950/
https://xaydunghanoimoi.net/members/27743-pk888slo.html
https://www.foriio.com/pk888slotscom
https://www.project1999.com/forums/member.php?u=333369
https://pad.stuve.de/s/HSmAQ272zb
https://pad.libreon.fr/s/92U3ZoVwm
https://gl.gravatar.com/pk888slotscom
https://fr.gravatar.com/pk888slotscom
https://fi.gravatar.com/pk888slotscom
https://fa.gravatar.com/pk888slotscom
https://quomon.es/Profile/pk888slotscom
https://www.are.na/pk-888/channels
https://getrevising.co.uk/members/pk888slotscom
https://altacucina.co/profile/pk888slotscom
https://ro.gta5-mods.com/users/pk888slotscom
https://ru.gta5-mods.com/users/pk888slotscom
https://sv.gta5-mods.com/users/pk888slotscom
https://vi.gta5-mods.com/users/pk888slotscom
https://zh.gta5-mods.com/users/pk888slotscom
https://www.mindmeister.com/users/channel/131043780
https://maiotaku.com/p/pk888slotscom/info
https://theexplorers.com/user?id=1e9803c3-0de1-4052-b7b1-c1707d8d2152
https://md.rappet.xyz/s/aA6NFwmNiU
https://www.blurb.com/user/pk888slotsco?profile_preview=true
https://wall.page/pDFn10
https://participa.aytojaen.es/profiles/pk888slotscom/activity
https://bsky.app/profile/pk888slotscom.bsky.social
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=157869_f5d4s9l3
https://www.ad-links.org/https://pk888-slotscom/_372433.html
https://km.gravatar.com/pk888slotscom
https://ja.gravatar.com/pk888slotscom
https://id.gravatar.com/pk888slotscom
https://he.gravatar.com/pk888slotscom
https://www.reddit-directory.com/https://pk888-slotscom/_710738.html
https://www.beegdirectory.com/https://pk888-slotscom/_491103.html
https://www.aquarius-dir.com/https://pk888-slotscom/_516888.html
https://www.apeopledirectory.com/https://pk888-slotscom/_415853.html
https://www.bedirectory.com/https://pk888-slotscom/_448574.html
https://www.clickasnap.com/profile/pk888slotscom
https://soundcloud.com/pk888slotscom
https://fliphtml5.com/vi/home/pk888slotscom
https://www.tm-town.com/translators/pk888slotscom
https://biolinku.co/pk888slotscom
https://linkmix.co/53688760
https://land-book.com/pk888slotscom
https://ko-fi.com/pk888slotscom
https://jali.me/pk888slotscom
https://jii.li/pk888slotscom
https://www.addirectory.org/details.php?id=478519
https://kitsu.app/users/1704768
https://giphy.com/channel/pk888slotscom
https://www.producthunt.com/@pk888slotscom
https://www.awwwards.com/pk888slotscom/
https://fairygodboss.com/users/profile/al1QBvJY21/pk888slotscom
https://stepik.org/users/1247351749/profile
https://rentry.co/tocvf9qc
https://www.demilked.com/author/pk888slotscom/
https://www.depechemode.cz/?URL=https://pk888-slots.com/
https://jp.pinterest.com/pk888slotscom/
https://de.gta5-mods.com/users/pk888slotscom
https://mk.gta5-mods.com/users/pk888slotscom
https://tr.gta5-mods.com/users/pk888slotscom
https://bs.gravatar.com/pk888slotscom
https://ca.gravatar.com/pk888slotscom
https://br.gravatar.com/pk888slotscom
https://bn.gravatar.com/pk888slotscom
https://bg.gravatar.com/pk888slotscom
https://az.gravatar.com/pk888slotscom
https://www.pozible.com/profile/pk888slotscom
https://dialogluzern.ch/profiles/pk888slotscom/activity
https://app.scholasticahq.com/scholars/521803-pk888-slotscom
https://community.atlassian.com/user/profile/5dae1f07-1318-4dc7-9097-8c7c43c6bce1
https://manifold.markets/pk888slotscom
https://game8.jp/users/486260
https://skr.gravatar.com/pk888slotscom
https://sk.gravatar.com/pk888slotscom
https://ru.gravatar.com/pk888slotscom
https://ro.gravatar.com/pk888slotscom
https://pl.gravatar.com/pk888slotscom
https://www.ask-dir.org/https://pk888-slotscom/_384084.html
https://tempel.in/view/HAoN5
https://quicknote.io/7415e4b0-3e00-11f1-b4d4-d703eec67e0a/
https://www.maanation.com/pk888slotscom
https://pixelfed.uno/pk888slotscom
http://mura.hitobashira.org/index.php?pk888slotscom
https://peatix.com/user/29430288/view
https://padlet.com/pk888slotscom/pk888-xt20cjp09zqaq5xm
https://www.elephantjournal.com/profile/pk888slotscom/
https://videos.muvizu.com/Profile/pk888slotscom/Latest/
https://dev.muvizu.com/Profile/pk888slotscom/Latest/
https://cdn.muvizu.com/Profile/pk888slotscom/Latest/
https://www.muvizu.com/Profile/pk888slotscom/Latest/
https://decidim.santcugat.cat/profiles/pk888slotscom/activity
https://fr.slideshare.net/omarkraus693?tab=about
https://forum.allkpop.com/suite/user/315064-pk888slotscom/#about
https://www.geogebra.org/m/vfe2bxge
https://janitorai.com/profiles/2a46ca15-7042-4c93-9dd8-4d14483b6a2f_profile-of-pk-888-slotscom
https://muckrack.com/pk888slotscom/bio
https://www.akiba-online.com/members/pk888slotscom.1354108/#about
https://worstgen.alwaysdata.net/forum/members/pk888slotscom.172959/#about
https://www.tkaraoke.com/forums/profile/pk888slotscom/
http://linoit.com/users/pk888slotscom/canvases/pk888slotscom
https://nortabs.net/user/14875/
https://sidequestvr.com/user/4938011
https://dojour.us/u/pk888slotscom
https://www.myconcertarchive.com/en/user_home?id=130050
https://all4.vip/p/page/view-persons-profile?id=122652
https://ferrariformula1.hu/community/profile/pk888slotscom/
https://strikefans.com/forum/users/pk888slotscom/
https://swat-portal.com/forum/wcf/user/48664-pk888slotscom/#about
https://giloo.ist/member/pk888slotscom/
https://defence.pk/members/pk888slotscom.239269/#about
https://forum.jatekok.hu/User-pk888slotscom
https://www.xibeiwujin.com/home.php?mod=space&uid=2314187&do=profile&from=space
https://buymusicclub.vercel.app/user/pk888slotscom
https://wiki.armello.com/index.php/User:Pk888slotscom
https://histre.com/notes/omarkraus693/zbazls0e/?accesscode=XBjPonZ0xfj01LRR
https://forum.freero.org/space-uid-24791.html
https://oraclenana.com/MYBB3/user-42378.html
https://ka.gravatar.com/pk888slotscom
https://fr-ca.gravatar.com/pk888slotscom
https://fr-ca.gravatar.com/pk888slotscom
https://el.gravatar.com/pk888slotscom
https://da.gravatar.com/pk888slotscom
https://www.notariosyregistradores.com/web/forums/usuario/pk888slotscom/
https://www.facer.io/u/pk888slotscom
http://genina.com/user/profile/5326445.page
https://www.dailymotion.com/user/pk888slotscom
https://forum-foxess.pro/community/profile/pk888slotscom/
https://forum.biblepay.org/index.php?action=profile;area=forumprofile;u=42623
https://socialsocial.social/user/pk888slotscom/
https://referrallist.com/profile/pk888slotscom/
https://www.stylevore.com/user/pk888slotscom
https://es.stylevore.com/user/pk888slotscom
https://rant.li/pk888slotscom/pk888-a-melhor-plataforma-de-slot-do-brasil-um-cassino-online-confiavel
https://www.workingholidayjobs.com.au/forums/users/pk888slotscom/
https://chanylib.ru/ru/forum/user/25304/
https://www.cbmstuff.com/forum/member.php?action=profile&uid=11611
https://producerbox.com/users/pk888slotscom
https://skrolli.fi/keskustelu/users/omarkraus693/
https://forum.vgatemall.com/member.php?action=profile&uid=497271
https://www.thehockeypaper.co.uk/forums/users/pk888slotscom
https://channillo.com/user/71953/
https://www.forum-joyingauto.com/member.php?action=profile&uid=107387
https://www.11plus.co.uk/users/omarkraus693/
https://opaseke.com/users/15187
https://app.getfarmish.com/profile/pk888slotscom
https://www.freebeg.com/forum/member.php?action=profile&uid=135358
https://imaginaria.ru/profile/pk888slotscom/
https://artconomy.com/profile/pk888slotscom/about/
https://nl.gravatar.com/pk888slotscom
https://nb.gravatar.com/pk888slotscom
https://ms.gravatar.com/pk888slotscom
https://lt.gravatar.com/pk888slotscom
https://kn.gravatar.com/pk888slotscom
https://galgame.dev/user/pk888slotscom
https://nicheless.blog/author/pk888slotscom
https://www.newgenstravel.com/forum/topic/41993/pk888
https://zbrushcentral.jp/user/pk888slotscom
http://julia4tied.de/member.php?action=profile&uid=246362
https://forum.rexygen.com/user/pk888slotscom
https://id.gta5-mods.com/users/pk888slotscom
https://ms.gta5-mods.com/users/pk888slotscom
https://bg.gta5-mods.com/users/pk888slotscom
https://ca.gta5-mods.com/users/pk888slotscom
https://cs.gta5-mods.com/users/pk888slotscom
https://te.legra.ph/PK888-04-22
https://codeberg.org/pk888slotscom
https://www.mapleprimes.com/users/pk888slotscom
https://www.plurk.com/pk888slotscom
https://www.fiferosdevenezuela.com/foro/member.php?action=profile&uid=12658
https://forum.liquidbounce.net/user/pk888slotscom
https://muabanhaiduong.com/members/pk888slotscom.87154/#about
https://noti.st/pk888slotscom
https://ur.gravatar.com/pk888slotscom
https://tr.gravatar.com/pk888slotscom
https://sr.gravatar.com/pk888slotscom
https://sq.gravatar.com/pk888slotscom
https://sl.gravatar.com/pk888slotscom
https://www.adpost.com/u/pk888slotscom/
https://guitarmaking.co.uk/members/pk888slotscom/
https://definedictionarymeaning.com/user/pk888slotscom
https://www.deviantart.com/pk888slotscom
https://pk888slotscom.bandcamp.com/album/pk888
https://pk888slotscom.themedia.jp/pages/9736565/page_202604221423
https://pastelink.net/hlgfkkj5
https://archive.org/details/@pk888slotscom/loans#on-loan
https://pk888slotscom.stck.me/profile
https://www.notion.so/PK888-34a4a780eaed8006881dd9abe4a68cfb
https://pk888slotscom.storeinfo.jp/pages/9736568/page_202604221430
https://cannabis.net/user/225310
https://pk888slotscom.shopinfo.jp/pages/9736577/page_202604221432
https://sketchersunited.org/users/318644
https://jobs.lajobsportal.org/profiles/8181296-pk888-slotscom
https://pk888slotscom.amebaownd.com/pages/9736584/page_202604221434
https://uk.gravatar.com/pk888slotscom
https://hu.gravatar.com/pk888slotscom
https://it.gravatar.com/pk888slotscom
https://hifi.slovanet.sk/bb/profile.php?mode=viewprofile&u=17340
https://urlz.fr/v7tC
https://x.com/pk888slotscom
https://hedgedoc.digillab.uni-augsburg.de/s/karLFXa_ev
https://scrapbox.io/pk888slotscom/PK888
https://circle-book.com/circles/46510
https://vrcmods.com/user/pk888slotscom
https://stackoverflow.com/users/32648543/pk888slotscom?tab=profile
https://forum.opnsense.org/index.php?action=profile;u=67522
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=228253&tab=field_core_pfield_13
https://www.mshowto.org/forum/members/pk888slotscom.html
https://da.gta5-mods.com/users/pk888slotscom
https://el.gta5-mods.com/users/pk888slotscom
https://es.gta5-mods.com/users/pk888slotscom
https://fr.gta5-mods.com/users/pk888slotscom
https://ko.gta5-mods.com/users/pk888slotscom
https://www.ekademia.pl/@pk888
https://youbiz.com/profile/pk888slotscom/
https://es.gravatar.com/pk888slotscom
https://de.gravatar.com/pk888slotscom
https://cy.gravatar.com/pk888slotscom
https://cs.gravatar.com/pk888slotscom
https://cn.gravatar.com/pk888slotscom
https://pk888slotscom.mystrikingly.com/
https://www.backabuddy.co.za/campaign/pk888
https://social1776.com/pk888slotscom
https://hackmd.okfn.de/s/BkKcAg86Wg
https://cars.yclas.com/user/pk888slotscom
https://stocktwits.com/pk888slotscom
https://jobs.caregiver.ca/employers/4121340-pk888slotscom
https://nyccharterschools.jobboard.io/employers/4121339-pk888slotscom
https://photouploads.com/pk888slotscom
https://data.danetsoft.com/pk888-slots.com
https://www.annuncigratuititalia.it/author/pk888slotscom/
https://www.themoviedb.org/u/pk888slotscom
https://kick.com/pk888slotscom/about
https://whitehat.vn/members/pk888slotscom.226460/#about
https://www.goodreads.com/user/show/200528210-pk888slotscom
https://www.pixiv.net/en/users/125592485
https://www.otofun.net/members/pk888slotscom.906421/#about
https://www.bestbuydir.com/https://pk888-slotscom/_455040.html
https://www.free-weblink.com/https://pk888-slotscom/_277046.html
https://www.betting-forum.com/members/pk888slotscom.157153/#about
https://unsplash.com/fr/@pk888slotscom
https://app.simplenote.com/p/Yvc7mh
https://www.adslgr.com/forum/members/223718-pk888slotscom
https://ja.cofacts.tw/user/pk888slotscom
https://cofacts.tw/user/pk888slotscom
https://forum.plutonium.pw/user/pk888slotscom
https://www.insanelymac.com/forum/profile/2748059-pk888slotscom/?tab=field_core_pfield_13
https://www.tacter.com/@pk888slotscom
https://forums.delphiforums.com/blackscreens/messages/619/1
https://writeupcafe.com/author/pk888slotscom
https://caveduck.io/user/pk888slotscom?locale=en
https://www.guildlaunch.com/community/users/blog/6752917?gl_user=6752917&gid=535
https://sooperarticles.com/u/pk-slotscom/845884
https://www.vrcarena.com/users/hZRP7IHj87aLrse4D9xqNyl2Lkl2
https://www.livecleo.xxx/community/profile/pk888slotscom/
https://pad.geolab.space/s/inJYFayKZ
https://forum.splashteck.com/member.php?action=profile&uid=4912
https://artvee.com/members/pk888slotscom/profile/
https://doingbusiness.eu/profile/pk888slotscom/
https://www.thaithesims4.com/member.php?member=1204265
https://www.tkc-games.com/forums/users/omarkraus693/
https://beta.wolf3d.net/users/1241
https://ben10club.org/user/pk888slotscom
https://seo.entireweb.com/reports/247006
https://www.moneymagpie.com/messageboards/users/pk888-slotscom
https://www.lola.vn/u/pkslotscom
https://www.diggerslist.com/pk888slotscom/about
https://bb.honorboundgame.com/user-509799.html
https://act4sdgs.org/profile/pk888slotscom
https://savvyauthors.com/community/members/pk888slotscom.28175/#about
https://www.longisland.com/profile/pk888slotscom
https://expathealthseoul.com/profile/pk888slotscom/
https://qiita.com/pk888slotscom
https://www.notebook.ai/@pk888slotscom
https://www.iniuria.us/forum/member.php?675141-pk888slotscom
https://www.tumblr.com/pk888slotscom
https://www.ameba.jp/profile/general/pk888slotscom/
https://www.vnbadminton.com/members/pk888slotscom.75354/
https://wirtube.de/a/pk888slotscom/video-channels
https://partecipa.poliste.com/profiles/pk888slotscom/activity
https://cloutapps.com/pk888slotscom
https://chodilinh.com/members/pk888slotscom.301137/#about
https://expatguidekorea.com/profile/pk888slotscom/
https://amazingradio.com/profile/pk888slotscom
https://tinyurl.com/pk888slotscom
https://infiniteabundance.mn.co/members/39399127
https://devpost.com/pk888slotscom
https://advego.com/profile/pk888slotscom/
https://hkgay.net/member.php?action=profile&uid=528844
https://git.disroot.org/pk888slotscom
https://freelance.ru/pk888slotscom
https://allmy.bio/pk888slotscom
https://creator.nightcafe.studio/u/pk888slotscom
https://hedgedoc.eclair.ec-lyon.fr/s/5iv4tZwgy
https://www.renderosity.com/users/id:1851397
https://diendan.clbmarketing.com/members/pk888slotscom.301389/#about
https://www.elitepvpers.com/forum/members/9043631-pk888slotscom.html
https://beteiligung.amt-huettener-berge.de/profile/pk888slotscom/
https://www.magcloud.com/user/pk888slotscom
https://iplogger.com/2L7XA6
https://www.theyeshivaworld.com/coffeeroom/users/pk888slotscom
https://www.scener.com/@pk888slotscom
https://kyourc.com/pk888slotscom
https://dentaltechnician.org.uk/community/profile/pk888slotscom/
https://beteiligung.stadtlindau.de/profile/pk888slotscom/
https://beteiligung.tengen.de/profile/pk888slotscom/
https://longbets.org/user/pk888slotscom/
https://www.globalfreetalk.com/pk888slotscom
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8195212.htm
https://naijamatta.com/pk888slotscom
https://youslade.com/pk888slotscom
https://pk888slotscom.gitbook.io/pk888slotscom-docs
https://stuv.othr.de/pad/s/XAUJzL-Z4
https://sklad-slabov.ru/forum/user/43170/
https://pad.fablab-siegen.de/s/e6Aq9vkH3a
https://notes.bmcs.one/s/gg15nbYpmY
https://md.darmstadt.ccc.de/s/2WPBj5UqK9
https://pad.funkwhale.audio/s/KuNZh9Ln6
https://md.kif.rocks/s/WTgDMV83zA
https://md.opensourceecology.de/s/HKDz-C75m
https://pad.flipdot.org/s/aunW1f5Bt
https://md.chaospott.de/s/VZiQcqzcRn
https://bom.so/ohPg6w
https://it.pinterest.com/pk888slotscom/
https://t.ly/MQGKk
https://hedgedoc.stusta.de/s/u3dbKkQJn
https://fi.pinterest.com/pk888slotscom/
https://md.coredump.ch/s/r5DeYosAh
https://aboutnursernjobs.com/author/pk888slotscom/
https://aboutnursinghomejobs.com/author/pk888slotscom/
https://rndirectors.com/author/pk888slotscom/
https://www.i-hire.ca/author/pk888slotscom/
https://codimd.communecter.org/s/KS84BUTKH
https://ivpaste.com/v/QdGwWdb65O
http://gojourney.xsrv.jp/index.php?pk888slotscom
https://pad.koeln.ccc.de/s/DOWAjmQK-
https://md.un-hack-bar.de/s/LFdIwClrlI
https://gitlab.haskell.org/pk888slotscom
https://allods.my.games/forum/index.php?page=User&userID=247357
https://urlscan.io/result/019db5cc-23e3-7710-8816-0d1921155d1c/
https://kooperation.winterthur.ch/profiles/pk888slotscom/activity
https://www.rctech.net/forum/members/pk888slotscom-548466.html
https://drivehud.com/forums/users/omarkraus693/
https://aoezone.net/members/pk888slotscom.186030/#about
https://projectnoah.org/users/pk888slotscom
https://trakteer.id/pk888slotscom
https://www.thepartyservicesweb.com/board/board_topic/3929364/8195850.htm
https://www.sunemall.com/board/board_topic/8431232/8195868.htm
https://www.tai-ji.net/board/board_topic/4160148/8195869.htm
https://destaquebrasil.com/saopaulo/author/pk888slotscom/
https://illust.daysneo.com/illustrator/pk888slotscom/
https://www.thepetservicesweb.com/board/board_topic/2701171/8195917.htm
https://www.vhs80.com/board/board_topic/6798823/8195916.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8195915.htm
https://pk888slotscom.wiki-cms.com/8436282/pk888
https://pk888slotscom.salesmanwiki.com/10408561/pk888
https://video.fc2.com/account/15100435
https://lit.link/en/pk888slotscom
https://domain.opendns.com/pk888-slots.com
https://pk888slotscom.localinfo.jp/pages/9737506/page_202604222251
https://participer.loire-atlantique.fr/profiles/pk888slotscom/activity
https://hedgedoc.envs.net/s/mdjX3ZQge
https://www.adsfare.com/pk888slotscom
https://hackmd.openmole.org/s/T1J0Dh-gQ
https://md.sebastians.dev/s/94HgksyYp
https://pad.public.cat/s/vZmHnwNrz
https://pad.lescommuns.org/s/BIpgGCE6R
https://www.skillshot.pl/users/25636
https://colab.research.google.com/drive/1yR02BlbAyg-jxRr16VHityYIhi2JdzuQ?usp=sharing
https://teletype.link/pk888slotscom
https://turcia-tours.ru/forum/profile/pk888slotscom/
https://nonon-centsnanna.com/members/pk888slotscom/
https://radiotodayjobs.com/company/pk888slotscom
https://spoutible.com/pk888slotscom
https://beta.cent.co/pk888slotscom/+chhozb
https://congdongx.com/thanh-vien/pk888slotscom.48614/#about
https://www.leenkup.com/pk888slotscom
https://novel.daysneo.com/author/pk888slotscom/
https://startupxplore.com/en/person/pk888slotscom
https://daysneo.com/author/pk888slotscom/
https://www.ozbargain.com.au/user/610447
http://newdigital-world.com/members/pk888slotscom.html
https://www.ewebdiscussion.com/members/pk888slotscom.128916/#about
https://congdongthugian.com/members/pk888slotscom.14604/#about
https://www.hentai-foundry.com/user/pk888slotscom/profile
https://help.orrs.de/user/pk888slotscom
https://experiment.com/users/ppk888slotscom
https://www.proko.com/@pk888slotscom/activity
http://imagej.273.s1.nabble.com/PK888-td5031147.html
https://searchengines.guru/ru/users/2233636
https://voz.vn/u/pk888slotscom.2205028/#about
https://fyers.in/community/member/zfb7iy17lq
https://iplogger.org/vn/logger/j4bR5XELrzC3/
https://md.yeswiki.net/s/VYq_IoYO15
https://www.suamusica.com.br/pk888slotscom
https://dynamicscommunities.com/community/members/omarkraus693gmail-com/
https://cv.viblo.asia/preview-cv/88bf7e28-24aa-4b4b-ba04-f62e6c31189c
https://www.aphorismsgalore.com/users/pk888slotscom
https://hmsay.com/members/pk888slotscom/
https://sdelai.ru/members/pk888slotscom/
http://www.reumamurcia.com/forums/users/pk888slotscom/
https://www.youyooz.com/profile/pk888slotscom/
https://www.directorylib.com/domain/pk888-slots.com
https://www.minecraft-servers-list.org/details/pk888slotscom/
https://chiase123.com/member/pk888slotscom/
https://malt-orden.info/userinfo.php?uid=458739
https://market360.vn/page/75695
https://hallbook.com.br/pk888slotscom
https://californiafilm.ning.com/profile/pk888slotscom
https://its-my.link/@pk888slotscom
https://zeroone.art/profile/pk888slotscom
https://www.fitlynk.com/pk888slotscom
https://www.siasat.pk/members/pk888slotscom.271392/#about
https://www.keyfimuzik.net/members/398258-pk888slotscom.html
https://forum.gettinglost.ca/user/pk888slotscom
https://www.am.ics.keio.ac.jp/proj/asap/wiki/?pk888slotscom
https://www.ironlifting.it/forum/member.php?u=429716
http://catalog.drobak.com.ua/communication/forum/user/2851465/
https://anunt-imob.ro/user/profile/855337
https://www.bookingblog.com/forum/users/pk888slotscom/
https://www.coffeesix-store.com/board/board_topic/7560063/8196242.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8196243.htm
https://www.myaspenridge.com/board/board_topic/3180173/8196244.htm
https://www.cryptoispy.com/forums/users/pk888slotscom/
https://www.milliescentedrocks.com/board/board_topic/2189097/8196245.htm
https://www.prodesigns.com/wordpress-themes/support/users/pk888slotscom
https://www.scamadviser.com/check-website/pk888-slots.com
https://adplist.org/members/pk888
https://hyperfollow.com/pk888slotscom
http://koloboklinks.com/site?url=pk888-slots.com
Sangat menarik poin yang Anda utarakan, salam telah memposting. “Sejarah adalah puisi siklik yang ditulis oleh Waktu di atas ingatan manusia.” oleh Percy Bysshe Shelley.
I have been reading out a few of your articles and it’s pretty good stuff. I will surely bookmark your site.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Kerja yang sangat baik!
Your comment is awaiting moderation.
https://www.facebook.com/188m7com
https://www.youtube.com/@188m7com
https://x.com/188m7com
https://tooter.in/188m7com
https://wakelet.com/@188m7com
https://www.blogger.com/profile/08882213210745077037
https://www.mymeetbook.com/188m7com
https://www.pinterest.com/188m7com/
https://shareyoursocial.com/188m7com
https://500px.com/p/188m7com?view=photos
https://www.instapaper.com/p/188m7com
https://band.us/@188m7com
https://protocol.ooo/ja/users/188m7com
https://www.tumblr.com/188m7com
https://www.reddit.com/user/188m7com/
https://audiomack.com/hericserriteno945
https://hackaday.io/188m7com?saved=true
https://vocal.media/authors/188m7com
https://leetcode.com/u/188m7com/
https://www.halaltrip.com/user/profile/340427/188m7com/
https://medibang.com/author/28173745/
https://www.blockdit.com/users/69e70fa8f599ef9acc9c427f
https://portfolium.com/hericserriteno945
https://groups.google.com/g/188m7com
https://www.twitch.tv/188m7com/about
https://profile.hatena.ne.jp/m7com/profile
https://issuu.com/188m7com
https://issuu.com/188m7com
https://gravatar.com/188m7com
https://www.reverbnation.com/188m7com
https://www.myminifactory.com/users/188m7com
https://www.investagrams.com/Profile/188m7com
https://gifyu.com/188m7com
https://www.chordie.com/forum/profile.php?id=2511077
https://www.longisland.com/profile/188m7com
https://topsitenet.com/profile/188m7com/1645118/
https://akniga.org/profile/1415732-188m7com
https://bandcamp.com/188m7com
https://disqus.com/by/188m7com/about/
https://jobs.suncommunitynews.com/profiles/8175828-nha-cai-188m
https://www.speedrun.com/users/188m7com
https://www.aicrowd.com/participants/188m7com
https://old.bitchute.com/channel/JSsiJFLyJMKh/
https://pbase.com/188m7com/root
https://hub.docker.com/u/188m7com
https://spiderum.com/nguoi-dung/188m7com
https://www.gta5-mods.com/users/188m7com
https://heylink.me/hericserriteno945/
https://pixabay.com/users/188m7com-55529060/
https://www.nicovideo.jp/user/143990162
https://3dwarehouse.sketchup.com/user/371f65e0-fca6-4c1e-8e78-130254fdc606
https://joy.bio/188m7com
https://connect.garmin.com/app/profile/be808995-3a83-47f9-bcae-db347b88a4a2
https://b.hatena.ne.jp/m7com/hotentry
https://www.chichi-pui.com/users/188m7com/
https://unityroom.com/users/nmlkdyptjxhi124o86eq
https://routinehub.co/user/188m7com
https://pxhere.com/en/photographer-me/4988150
https://teletype.in/@188m7com
https://www.checkli.com/188m7com#/a/process
https://www.fuelly.com/driver/188m7com
https://www.nintendo-master.com/profil/188m7com
https://freeimage.host/188m7com
https://motion-gallery.net/users/955927
https://linkin.bio/188m7com
https://biomolecula.ru/authors/141994
https://blender.community/188m7com/
https://doselect.com/@dfd7ae1e90e845ea1252fb95f
https://matkafasi.com/user/188m7com
https://allmyfaves.com/188m7com
https://conecta.bio/188m7com
https://www.abclinuxu.cz/lide/188m7com
https://muare.vn/shop/heric-serriteno/902512
https://www.intensedebate.com/people/188m7com1
https://forum.dmec.vn/index.php?members/188m7com.187631/
https://igli.me/188m7com
http://delphi.larsbo.org/user/188m7com
https://app.readthedocs.org/profiles/188m7com/
https://www.dibiz.com/hericserriteno945
https://iszene.com/user-347764.html
https://desksnear.me/users/188m7com
https://www.roton.com/forums/users/hericserriteno945/
https://able2know.org/user/188m7com/
http://www.biblesupport.com/user/831532-188m7com/
https://golosknig.com/profile/188m7com/
https://www.inventoridigiochi.it/membri/188m7com/profile/
https://forum.m5stack.com/user/188m7com
https://www.bitchute.com/channel/JSsiJFLyJMKh
https://bandori.party/user/795173/188m7com/
https://community.m5stack.com/user/188m7com1
https://schoolido.lu/user/188m7com/
https://awan.pro/forum/user/165736/
https://fabble.cc/188m7com
https://kr.pinterest.com/188m7com/
https://pt.gravatar.com/188m7com
https://th.gravatar.com/188m7com
https://f319.com/members/188m7com.1097691/
https://about.me/n188m
https://booklog.jp/users/188m7com/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/188m7com.1353648/#about
https://www.equinenow.com/farm/188m7com.htm
https://wefunder.com/nhci188m1
https://potofu.me/188m7com
https://transfur.com/Users/m7com
https://xtremepape.rs/members/188m7com.666052/#about
https://myanimelist.net/profile/188m7com
https://qna.habr.com/user/188m7com
https://website.informer.com/188m-7.com
https://en.islcollective.com/portfolio/12903539
https://www.xosothantai.com/members/188m7com.609367/
https://violet.vn/user/show/id/15267953
https://iplogger.org/vn/logger/szzR5vcVkQ5N/
https://notionpress.com/author/1508409
https://www.edna.cz/uzivatele/188m7com/
https://digiphoto.techbang.com/users/188m7com
https://leakedmodels.com/forum/members/188m7com.708997/#about
https://onlinesequencer.net/members/268012
https://inkbunny.net/188m7com?&success=Profile+settings+saved.
https://www.japaaan.com/user/77028/type/1
https://www.launchgood.com/user/newprofile#!/user-profile/profile/heric.serriteno
https://apptuts.bio/188m7com-259875
https://egl.circlly.com/users/188m7com
https://goodandbadpeople.com/188m7com
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=301088
https://acomics.ru/-188m7com
https://www.criminalelement.com/members/188m7com/profile/
https://hanson.net/users/188m7com
https://writexo.com/share/0f9b3c7852be
“https://expatguidekorea.com/profile/188m7com/
”
https://www.laundrynation.com/community/profile/188m7com/
https://www.heavyironjobs.com/profiles/8176185-nha-cai-188m
https://pad.degrowth.net/s/39-gMtpbX
http://fort-raevskiy.ru/community/profile/188m7com/
https://forum.skullgirlsmobile.com/members/188m7com.215355/#about
https://jobs.landscapeindustrycareers.org/profiles/8176197-nha-cai-188m
https://forums.galciv4.com/user/7660996
https://jobs.njota.org/employers/4119531-188m7com
https://song.link/xjnzzfwwpbcw2
https://idol.st/user/165055/188m7com/
https://www.valinor.com.br/forum/usuario/188m7com.145170/#about
https://tulieu.violet.vn/user/show/id/15267953
https://www.bmwpower.lv/user.php?u=188m7com
https://gockhuat.net/member.php?u=436931
https://jobs.windomnews.com/profiles/8176259-nha-cai-188m
https://hoaxbuster.com/redacteur/188m7com
https://talkmarkets.com/profile/hericserriteno945-260421-075041
https://forums.stardock.com/user/7660996
https://zerosuicidetraining.edc.org/user/profile.php?id=560275
https://www.telix.pl/forums/users/Heric-Serriteno/
https://beteiligung.amt-huettener-berge.de/profile/188m7com/
https://joinentre.com/profile/188m7com
https://jobs.westerncity.com/profiles/8176301-nha-cai-188m
https://www.thetriumphforum.com/members/188m7com.62868/
https://l2top.co/forum/members/188m7com.173098/
https://forums.galciv3.com/user/7660996
https://galleria.emotionflow.com/183049/profile.html
https://myget.org/users/188m7com
https://galleria.emotionflow.com/183049/profile.html
https://app.brancher.ai/user/-h7PRsSELDg9
https://justpaste.me/F66a
https://forums.sinsofasolarempire2.com/user/7660996
https://confengine.com/user/188m7com
https://slideslive.com/188m7com?tab=about
https://mygamedb.com/profile/188m7com
https://buckeyescoop.com/community/members/188m7com.62539/#about
https://forums.ashesofthesingularity.com/user/7660996
https://forum.aceinna.com/user/188m7com
https://www.mateball.com/m7com
https://toirscript.com/user/188m7com
https://forum.pabbly.com/members/188m7com.112399/#about
http://forum.cncprovn.com/members/424317-188m7com
https://ncnews.co/profile/188m7com
https://dreevoo.com/profile_info.php?pid=1523347
https://forum.aigato.vn/user/188m7com
https://amaz0ns.com/forums/users/188m7com/
https://rapidapi.com/user/hericserriteno945
https://www.skool.com/@nha-cai-mm-1533
https://learningapps.org/display?v=p6kyzyfic26
https://www.giveawayoftheday.com/forums/profile/1808218
https://tealfeed.com/serriteno_638582
https://www.invelos.com/UserProfile.aspx?alias=188m7com
https://www.video-bookmark.com/bookmark/7109380/188m-%E2%80%93-c%E1%BB%95ng-c%C3%A1-c%C6%B0%E1%BB%A3c-online-uy-t%C3%ADn,-tr%E1%BA%A3i-nghi%E1%BB%87m-game-v%C3%A0-k%C3%A8o-ae%EF%BF%BD%E1%BB%89nh-cao/
https://wibki.com/188m7com
https://twitback.com/188m7com
https://krachelart.com/UserProfile/tabid/43/userId/1342780/Default.aspx
https://www.11secondclub.com/users/profile/1712690
https://aniworld.to/user/profil/188m7com
https://worldvectorlogo.com/ar/profile/188m7com
https://www.passes.com/188m7com
https://poipiku.com/MyIllustListPcV.jsp?ID=13494827
https://uiverse.io/profile/heric_5289
https://www.rwaq.org/users/hericserriteno945-20260421125603
https://cofacts.tw/user/188m7com
https://www.fitday.com/fitness/forums/members/188m7com.html
https://vcook.jp/users/87516
https://www.grepmed.com/188m7com
https://espritgames.com/members/50820505/
https://cgmood.com/188m7com
https://www.haikudeck.com/presentations/Nhci.188m.2
https://www.efunda.com/members/people/show_people.cfm?Usr=188m7com
https://backloggery.com/188m7com
https://www.moshpyt.com/user/188m7com
https://pumpyoursound.com/u/user/1610678
https://que.u.nosv.org/profile?user=188m7com
https://secondstreet.ru/profile/188m7com/
https://marshallyin.com/members/188m7com/
https://gram.social/188m7com
https://luvly.co/users/188m7com
https://hukukevi.net/user/188m7com
https://savelist.co/profile/users/188m7com
https://www.apsense.com/user/188m7com
https://zzb.bz/ABg4xZ
https://draft.blogger.com/profile/08882213210745077037
https://www.themeqx.com/forums/users/188m7com/
https://forums.wincustomize.com/user/7660996
https://www.xen-factory.com/index.php?members/188m7com.154764/#about
https://cointr.ee/188m7com
https://jaga.link/188m7com
https://www.blackhatprotools.info/member.php?287359-188m7com
https://activepages.com.au/profile/188m7com
https://snippet.host/xegcge
https://tudomuaban.com/chi-tiet-rao-vat/2883669/188m–cong-ca-cuoc-online-uy-tin-trai-nghiem-game-va-keo-dinh-cao.html
https://phijkchu.com/a/188m7com/video-channels
https://lifeinsys.com/user/188m7com
https://www.claimajob.com/profiles/8177384-nha-cai-188m
https://protospielsouth.com/user/129955
https://theafricavoice.com/profile/188m7com
http://palangshim.com/space-uid-5108961.html
https://www.africangenesis-101.org/profile/hericserriteno94540584/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:0CCD813969E711650A495C3B@AdobeID
https://vi.gravatar.com/188m7com
https://www.mixcloud.com/188m7com/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=194362
https://hub.vroid.com/en/users/125596174
https://circleten.org/a/404665?postTypeId=whatsNew
https://skiomusic.com/188m7com
https://www.brownbook.net/business/55031795/188m7com
https://etextpad.com/bdxdfu0u5g
https://app.hellothematic.com/creator/profile/1144392
https://www.decidim.barcelona/profiles/188m7com/activity
https://app.talkshoe.com/user/188m7com
https://m.wibki.com/188m7com
https://jerseyboysblog.com/forum/member.php?action=profile&uid=91718
https://www.quora.com/profile/188m7com
https://manylink.co/@188m7com
https://forums.giantitp.com/member.php?373763-188m7com
https://seomotionz.com/member.php?action=profile&uid=127987
https://anyflip.com/homepage/kdodn
https://londonchinese.com/home.php?mod=space&uid=620624&do=profile
https://www.threadless.com/@188m7com/activity
https://www.smitefire.com/profile/188m7com-262234?profilepage
https://coolors.co/u/heric_serriteno
https://camp-fire.jp/profile/188m7com
https://www.pearltrees.com/188m7com
https://gesoten.com/profile/detail/12750111
https://hashnode.com/@188m7com
https://hoo.be/188m7com
https://maxforlive.com/profile/user/188m7com?tab=about
https://3dtoday.ru/blogs/188m7com
https://opencollective.com/188m7com
https://pinshape.com/users/8952746-188m7com?tab=designs
https://morguefile.com/creative/188m7com
https://edabit.com/user/ur5dunt8Y79XQvM7o
https://securityheaders.com/?q=https%3A%2F%2F188m-7.com%2F
https://my.bio/188m7com
https://community.cloudera.com/t5/user/viewprofilepage/user-id/150931
https://sfx.thelazy.net/users/u/188m7com/
https://app.daily.dev/188m7com
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=259228
https://www.skypixel.com/users/djiuser-doduxjbkq6zg
https://www.slmath.org/people/105325
https://userstyles.world/user/188m7com
https://pledgeme.co.nz/profiles/331574
https://188m7com.notepin.co/
https://forum.epicbrowser.com/profile.php?section=personal&id=151869
https://www.squadskates.com/profile/hericserriteno94541949/profile
https://forum.herozerogame.com/index.php?/user/161827-188m7com/
https://shhhnewcastleswingers.club/forums/users/188m7com/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2468021
https://connect.gt/user/188m7com
https://forum.tkool.jp/index.php?members/188m7com.105622/#about
https://www.divephotoguide.com/user/188m7com
https://www.weddingbee.com/members/188m7com/
https://kumu.io/188m7com/188m7com#untitled-map
https://b.cari.com.my/home.php?mod=space&uid=3398039&do=profile
https://bioimagingcore.be/q2a/user/188m7com
https://188m7com.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/188m7com/activity
https://www.socialbookmarkssite.com/bookmark/6238990/188m-c-ng-c-c-c-online-uy-t-n-tr-i-nghi-m-game-v-k-o-nh-cao/
https://www.hogwartsishere.com/1834948/
https://vimeo.com/188m7com
https://www.dotafire.com/profile/188m7com-244195?profilepage
https://www.trackyserver.com/profile/246153
https://tutorialslink.com/member/HericSerriteno/98409
https://www.vid419.com/home.php?mod=space&uid=3486343
https://188m7com.shopinfo.jp/posts/58760103
https://linqto.me/n/188m7com
http://techou.jp/index.php?188m7com
http://tkdlab.com/wiki/index.php?188m7com
https://www.managementpedia.com/members/188m7com.1120436/#about
http://pcsq28.com/home.php?mod=space&uid=1950988
https://bbs.airav.cc/home.php?mod=space&uid=4577068
https://hker2uk.com/home.php?mod=space&uid=5485963
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=494321
https://aprenderfotografia.online/usuarios/188m7com/profile/
https://bbs.darkml.net/home.php?mod=space&uid=147440
https://www.play56.net/home.php?mod=space&uid=6136406
https://md.swk-web.com/s/a1PsMT8xh
https://hedgedoc.dezentrale.space/s/RSf43ae_x
https://ar.gravatar.com/188m7com
https://replit.com/@188m7com
https://odesli.co/xjnzzfwwpbcw2
https://wandb.ai/profile/hericserriteno945
https://divisionmidway.org/jobs/author/188m7com/
https://bbcovenant.guildlaunch.com/users/blog/6752879/?mode=view&gid=97523
“https://youbiz.com/profile/188m7com/
”
https://referrallist.com/profile/188m7com/
https://www.wvhired.com/profiles/8177774-nha-cai-188m
http://jobs.emiogp.com/author/188m7com/
https://forumketoan.com/members/188m7com.44073/#about
https://v.gd/iZJzxT
https://gl.gta5-mods.com/users/188m7com
https://dapp.orvium.io/profile/nha-cai-188m-2078
https://www.fruitpickingjobs.com.au/forums/users/188m7com/
https://xoops.ec-cube.net/userinfo.php?uid=348510
https://formulamasa.com/elearning/members/188m7com/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1108126
https://chyoa.com/user/188m7com
https://forum.flashphoner.com/members/188m7com.46076/#about
https://backloggd.com/u/188m7com/
https://forums.alliedmods.net/member.php?u=476085
https://bwinglive.lighthouseapp.com/users/1997294
https://rush1989.rash.jp/pukiwiki/index.php?188m7com
https://www.stylevore.com/user/m7com188
https://bio.site/188m7com
https://www.noff.gg/user/healingstrawberry568122
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6396801
https://telegra.ph/188m7comm-04-21
https://reactormag.com/members/188m7com/
https://failiem.lv/hericserriteno945/info
https://brain-market.com/profiles/my_articles
https://beteiligung.hafencity.com/profile/188m7com/
https://adhocracy.plus/profile/188m7com/
https://beteiligung.stadtlindau.de/profile/188m7com/
https://elovebook.com/188m7com
https://propterest.com.au/user/80876/188m7com
https://www.fw-follow.com/forum/topic/116306/188m7com
https://www.jk-green.com/forum/topic/110022/188m7com
https://www.navacool.com/forum/topic/393257/188m7com
https://www.bonback.com/forum/topic/393258/188m7com
https://www.driedsquidathome.com/forum/topic/142392/188m7com
https://www.nongkhaempolice.com/forum/topic/122525/188m7com
https://www.bestloveweddingstudio.com/forum/topic/82447/188m7com
https://www.natthadon-sanengineering.com/forum/topic/102883/188m7com
https://www.rueanmaihom.net/forum/topic/97753/188m7com
https://www.ttlxshipping.com/forum/topic/393260/188m7com
https://pubhtml5.com/homepage/gtosx/
http://forum.modulebazaar.com/forums/user/188m7com/
https://gratisafhalen.be/author/188m7com/
https://beteiligung.tengen.de/profile/188m7com/
https://www.vrwant.org/wb/home.php?mod=space&uid=5093901
https://www.pathumratjotun.com/forum/topic/176875/188m7com
http://byltz.com/home.php?mod=space&uid=481359
https://raredirectory.com/author/79kshop-27113/
https://decidim.calafell.cat/profiles/188m7com/activity
http://bbs.medicalforum.cn/home.php?mod=space&uid=2230763
https://mforum.cari.com.my/home.php?mod=space&uid=3398039&do=profile
https://giaoan.violet.vn/user/show/id/15267953
https://anh135689999.violet.vn/user/show/id/15267953
https://hu.gta5-mods.com/users/188m7com
https://uk.gta5-mods.com/users/188m7com
https://sl.gta5-mods.com/users/188m7com
https://at.pinterest.com/188m7com/
https://www.easyhits4u.com/profile.cgi?login=188m7com&view_as=1
https://newdayrp.com/members/188m7com.70757/#about
https://in.pinterest.com/188m7com/
https://doc.anagora.org/s/fOqhAsdgw
https://album.link/xjnzzfwwpbcw2
https://artist.link/xjnzzfwwpbcw2
https://pods.link/xjnzzfwwpbcw2
https://mylink.page/xjnzzfwwpbcw2
https://playlist.link/xjnzzfwwpbcw2
https://portfolium.com.au/hericserriteno945
https://baigiang.violet.vn/user/show/id/15267953
https://forums.starcontrol.com/user/7660996
https://forums.offworldgame.com/user/7660996
https://www.ekdarun.com/forum/topic/153747/188m7com
https://fanclove.jp/profile/va2v7jlwJj
https://forums.sinsofasolarempire.com/user/7660996
https://forums.stardock.net/user/7660996
https://b.cari.com.my/home.php?mod=space&uid=3398039&do=profile
https://www.d-ushop.com/forum/topic/128431/188m7com
https://www.horticulturaljobs.com/employers/4120107-188m7com
https://jobs.siliconflorist.com/employers/4120108-188m7com
https://jobs.nefeshinternational.org/employers/4120109-188m7com
https://aboutcasemanagerjobs.com/author/188m7com/
https://biashara.co.ke/author/188m7com/
https://cornucopia.se/author/188m7com/
https://colorswall.com/users/32915/collections
https://bookmeter.com/users/1711540
https://lustyweb.live/members/188m7com.119142/
https://whyp.it/users/142353/188m7com
https://6giay.vn/members/188m7com.101843/
https://diendannhansu.com/members/188m7com.107885/#about
https://findaspring.org/members/188m7com/
https://careers.coloradopublichealth.org/profiles/8180408-nha-cai-188m
https://cloud.anylogic.com/profile/user/51f5b34d-033b-42df-a1b7-fa376ddaf07c
https://crowdsourcer.io/profile/AKJB2JHQ
https://homepage.ninja/188m7com
https://kttm.club/members/188m7com.4920/#about
https://www.techrum.vn/members/188m7com.266205/#about
https://vietcurrency.vn/members/188m7com.239557/#about
https://zh-tw.gravatar.com/188m7com
https://sv.gravatar.com/188m7com
https://po.gravatar.com/188m7com
https://oc.gravatar.com/188m7com
https://ko.gravatar.com/188m7com
https://pad.libreon.fr/s/OPeAEk0Pw
https://gl.gravatar.com/188m7com
https://fr.gravatar.com/188m7com
https://fi.gravatar.com/188m7com
https://fa.gravatar.com/188m7com
https://quomon.es/Profile/188m7com/
https://www.are.na/nha-cai-188m-jvm4yxssdhw/channels
https://ro.gta5-mods.com/users/188m7com
https://ru.gta5-mods.com/users/188m7com
https://sv.gta5-mods.com/users/188m7com
https://vi.gta5-mods.com/users/188m7com
https://zh.gta5-mods.com/users/188m7com
https://theexplorers.com/user?id=28b09103-6505-4f89-830b-31c3026234d0
https://md.rappet.xyz/s/ONU5ObhC0t
https://www.blurb.com/user/188m7com?profile_preview=true
https://participa.aytojaen.es/profiles/188m7com/activity
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=157932_0veb8756
https://km.gravatar.com/188m7com
https://ja.gravatar.com/188m7com
https://id.gravatar.com/188m7com
https://he.gravatar.com/188m7com
https://www.tripadvisor.com.vn/Profile/188m7com
https://biolinku.co/xj0n6pv
https://linkmix.co/53691305
https://jali.me/188m7com
https://jii.li/188m7com
https://kitsu.app/users/1704792
https://www.producthunt.com/@188m7com
https://justpaste.it/u/188m7com
https://fairygodboss.com/users/profile/NaHfVeojOo/Heric-Serriteno
https://jp.pinterest.com/188m7com/
https://de.gta5-mods.com/users/188m7com
https://mk.gta5-mods.com/users/188m7com
https://tr.gta5-mods.com/users/188m7com
https://bs.gravatar.com/188m7com
https://ca.gravatar.com/188m7com
https://br.gravatar.com/188m7com
https://bn.gravatar.com/188m7com
https://bg.gravatar.com/188m7com
https://az.gravatar.com/188m7com
https://www.pozible.com/profile/188m7com
https://dialogluzern.ch/profiles/188m7com/activity
https://skr.gravatar.com/188m7com
https://sk.gravatar.com/188m7com
https://ru.gravatar.com/188m7com
https://ro.gravatar.com/188m7com
https://pl.gravatar.com/188m7com
https://tempel.in/view/1Z776
https://quicknote.io/17080ca0-3e08-11f1-b4d4-d703eec67e0a
https://www.maanation.com/188m7com
https://www.elephantjournal.com/profile/hericserriteno945/
https://decidim.santcugat.cat/profiles/188m7com/activity
https://www.slideshare.net/hericserriteno945?tab=about
https://worstgen.alwaysdata.net/forum/members/188m7com.172964/#about
https://ka.gravatar.com/188m7com
https://ga.gravatar.com/188m7com
https://fr-ca.gravatar.com/188m7com
https://el.gravatar.com/188m7com
https://da.gravatar.com/188m7com
https://www.dailymotion.com/188m7com
https://socialsocial.social/user/188m7com/
https://es.stylevore.com/user/m7com188
https://rant.li/188m7com/188m-la-nen-tang-giai-tri-truc-tuyen-duoc-nhieu-nguoi-choi-lua-chon-nho-su-on
https://producerbox.com/users/188m7com
https://forum.vgatemall.com/member.php?action=profile&uid=497124
https://www.thehockeypaper.co.uk/forums/users/188m7com
https://www.forum-joyingauto.com/member.php?action=profile&uid=107251
https://nl.gravatar.com/188m7com
https://nb.gravatar.com/188m7com
https://ms.gravatar.com/188m7com
https://lt.gravatar.com/188m7com
https://kn.gravatar.com/188m7com
http://julia4tied.de/member.php?action=profile&uid=246351
https://id.gta5-mods.com/users/188m7com
https://ms.gta5-mods.com/users/188m7com
https://bg.gta5-mods.com/users/188m7com
https://ca.gta5-mods.com/users/188m7com
https://cs.gta5-mods.com/users/188m7com
https://www.yourquote.in/heric-serriteno-d3ixr/quotes
https://codeberg.org/188m7com
https://www.mapleprimes.com/users/188m7com
https://www.plurk.com/m7com188
https://www.discogs.com/fr/user/188m7com
https://files.fm/hericserriteno945/info
https://ur.gravatar.com/188m7com
https://tr.gravatar.com/188m7com
https://sr.gravatar.com/188m7com
https://sq.gravatar.com/188m7com
https://sl.gravatar.com/188m7com
https://guitarmaking.co.uk/members/188m7com/
https://definedictionarymeaning.com/user/heric-serriteno
https://pastelink.net/2iq6lktl
https://jobs.lajobsportal.org/profiles/8180678-nha-cai-188m
https://www.arriba420.com/profile/hericserriteno94546227/profile
https://uk.gravatar.com/188m7com
https://hu.gravatar.com/188m7com
https://it.gravatar.com/188m7com
https://forum.rodina-rp.com/members/402575/
https://www.max2play.com/en/forums/users/188m7com/
https://www.cadviet.com/forum/index.php?app=core&module=members&controller=profile&id=228245&tab=field_core_pfield_13
https://forum.lexulous.com/user/188m7com
https://da.gta5-mods.com/users/188m7com
https://el.gta5-mods.com/users/188m7com
https://es.gta5-mods.com/users/188m7com
https://fr.gta5-mods.com/users/188m7com
https://ko.gta5-mods.com/users/188m7com
https://es.gravatar.com/188m7com
https://de.gravatar.com/188m7com
https://cy.gravatar.com/188m7com
https://cs.gravatar.com/188m7com
https://cn.gravatar.com/188m7com
https://vietnam.net.vn/members/188m7com.59313/
https://social1776.com/188m7com
https://muabanvn.net/members/188m7com.32016/#about
https://chiase.org/members/188m7com.19494/
https://vipcorel.com/members/188m7com.49960/#about
https://congdongketoan.vn/members/188m7com.34682/#about
https://www.diendancacanh.com/members/188m7com.86862/
https://forum.edu.vn/members/188m7com.1780/#about
https://itseovn.com/members/188m7com.71694/
https://nhanxetdanhgia.vn/members/188m7com.63175/#about
https://vn-z.vn/members/188m7com.352557/#about
https://www.otosaigon.com/members/188m7com.426558/#about
https://www.dot.com.vn/members/188m7com.9699/
https://yeupet.vn/thanh-vien/188m7com.1143/#about
https://estar.jp/users/2026313153
https://it.gta5-mods.com/users/188m7com
https://nl.gta5-mods.com/users/188m7com
https://no.gta5-mods.com/users/188m7com
https://pl.gta5-mods.com/users/188m7com
https://pt.gta5-mods.com/users/188m7com
https://unsplash.com/@188m7com
https://ja.cofacts.tw/user/188m7com
https://us.pinterest.com/188m7com/
https://techplanet.today/member/188m7com
https://reduser.net/members/188m7com.229909/
https://sangtac.waka.vn/author/mcom-Z807DBo4rW
https://rmmedia.ru/members/183561/#about
https://devbest.com/members/188m7com.152848/#about
https://jobs.host-panel.com/author/188m7com/
https://www.skillshot.pl/users/25599
https://urlscan.io/result/019db3dc-0014-76ce-a7ca-6ac723550a0d/
https://wirtube.de/a/188m7com/video-channels
https://git.disroot.org/188m7com
https://participez.villeurbanne.fr/profiles/188m7com/activity
https://community.alexgyver.ru/members/188m7com.173581/#about
https://bioqoo.com/188m7com
https://qoolink.co/188m7com
https://jali.pro/188m7com
https://ngel.ink/188m7com
https://aboutnursepractitionerjobs.com/author/188m7com/
https://www.questmetaldetectors.com/members-area/hericserriteno94532593/profile
https://www.tacomaforum.com/members/188m7com.147838/#about
https://www.iniuria.us/forum/member.php?675019-188m7com
https://www.rappad.co/users/188m7com
https://rnmanagers.com/author/188m7com/
https://knowyourmeme.com/users/nha-cai-188m–2
https://rndirectors.com/author/188m7com/
https://pastebin.com/u/188m7com
https://www.hentai-foundry.com/user/188m7com/profile
https://www.xiuwushidai.com/home.php?mod=space&uid=2671445
https://www.saltlakeladyrebels.com/profile/hericserriteno9455966/profile
https://www.veteranscup.org/profile/hericserriteno94565647/profile
https://www.biblegrove.org/profile/hericserriteno94581426/profile
https://nous.malakoff.fr/profiles/188m7com/activity
https://slackcommunity.com/u/mcyfpd/#/about
https://bbs.theviko.com/home.php?mod=space&uid=4622879
https://www.webmastersun.com/members/188m7com.163403/#about
https://builtbybit.com/members/188m7com.791452/#about
https://www.pioneer2.net/community/members/m7com.14465/#about
https://forum.norbrygg.no/members/188m7com.150562/#about
https://congdongx.com/thanh-vien/188m7com.48539/#about
https://www.annuncigratuititalia.it/author/188m7com/
https://www.leonidastacticalss.com/profile/hericserriteno94527565/profile
https://www.battlakw.com/profile/hericserriteno9456773/profile
https://www.bridgescdc.com/profile/hericserriteno94547565/profile
https://participation.touraine.fr/profiles/188m7com/activity
https://forums.sorcererking.com/user/7660996
https://forums.galciv2.com/user/7660996
https://forums.gamersbillofrights.com/user/7660996
https://jobs.tdwi.org/profiles/8181115-nha-cai-188m
http://www.grandisvietnam.com/members/188m7com.29635/#about
https://www.airportcitygame.com/members/188m7com.36246/#about
https://www.zophar.net/forums/index.php?members/188m7com.134996/#about
https://congdongmassage.com/members/188m7com.147557/#about
https://aboutnursernjobs.com/author/188m7com/
https://www.bat-safe.com/profile/hericserriteno94569223/profile
https://www.jmriascos.space/profile/hericserriteno94595716/profile
https://jeparticipe.ville-montlouis-loire.fr/profiles/188m7com/activity
https://www.ltstesting.com/profile/hericserriteno94565899/profile
https://www.housedumonde.com/profile/hericserriteno94558696/profile
https://www.harimajuku.com/profile/hericserriteno94549708/profile
https://www.happycampersmontessori.com/profile/hericserriteno94594516/profile
https://www.miseducationofmotherhood.com/profile/hericserriteno94560326/profile
https://www.salmonshop.ca/profile/hericserriteno94565655/profile
https://www.newdirectionchildcarefacility.com/profile/hericserriteno94539078/profile
https://videos.muvizu.com/Profile/188m7com/Latest
https://dev.muvizu.com/Profile/188m7com/Latest
https://cdn.muvizu.com/Profile/188m7com/Latest
https://www.muvizu.com/Profile/188m7com/Latest
http://freestyler.ws/user/650954/188m7com
https://onlinecivilforum.com/profile/188m7com/
https://allmy.bio/188m7com
https://participa.gijon.es/profiles/188m7com/activity
https://aboutsnfjobs.com/author/188m7com/
https://forums.demigodgame.com/user/7660996
https://forums.elementalgame.com/user/7660996
https://raovatonline.org/author/188m7com/
https://artconomy.com/profile/188m7com/about/
https://n9.cl/0rnkk4
https://its-my.link/@188m7com
https://www.themirch.com/blog/author/188m7com/
https://whitehat.vn/members/188m7com.226454/#about
https://myxwiki.org/xwiki/bin/view/XWiki/188m7com?category=profile
https://nz.pinterest.com/188m7com/
https://marriagesofa.com/profile/188m7com/
https://cwresports.lk/profile/188m7com/
https://www.wmdb.org/users/profile/188m7com
https://ben10club.org/user/188m7com
https://de.pinterest.com/188m7com/
https://participationcitoyenne.rillieuxlapape.fr/profiles/188m7com/activity
https://chodaumoi247.com/members/188m7com.51399/
https://co-roma.openheritage.eu/profiles/188m7com/activity
https://construim.fedaia.org/profiles/188m7com/activity
https://participa.favb.cat/profiles/188m7com/activity
https://fengshuidirectory.com/dashboard/listings/188m7com/
https://www.cake.me/me/188m7com
https://coinfolk.net/user/188m7com
http://www.daojianchina.com/home.php?mod=space&uid=1035495
https://listium.com/@herics
https://www.demilked.com/author/188m7com/
https://advego.com/profile/188m7com/
https://www.planetminecraft.com/member/188m7com/
https://medium.com/@hericserriteno945
http://qa.doujiju.com/index.php?qa=user&qa_1=188m7com
https://culturesbook.com/1776844053515350_79449
https://app.reczee.com/talenthub/188m7com?_gl=1*mqixgv*_ga*MTA1NjgwODM1MC4xNzc2ODQ3OTk3*_ga_HDF9ZW7BPB*czE3NzY4NDc5OTYkbzEkZzEkdDE3NzY4NDgwNDkkajckbDAkaDA.
https://stocktwits.com/188m7com
https://teratail.com/users/188m7com
https://praca.uxlabs.pl/author/188m7com/
https://www.magcloud.com/user/188m7com
https://racetime.gg/user/XY0eABdmar3LKPnz/188m7com
https://casualgamerevolution.com/user
http://app.gxbs.net/home.php?mod=space&uid=1776132
https://www.proko.com/@188m7com/activity
https://trakteer.id/188m7com
https://destaquebrasil.com/saopaulo/author/188m7com/
https://blooder.net/188m7com
https://roomstyler.com/users/188m7com
https://chodilinh.com/members/188m7com.301056/#about
https://participer.loire-atlantique.fr/profiles/188m7com/activity
http://hkeverton.com/forumnew/home.php?mod=space&uid=634476
https://www.siasat.pk/members/188m7com.271348/#about
https://longbets.org/user/188m7com/
https://biolinky.co/188-m-7-com
https://forums.politicalmachine.com/user/7660996
https://ronpaulforums.com/members/188m7com.352306/#about
https://forumserver.twoplustwo.com/members/692463/
https://www.dideadesign.com/forum/topic/40380/188m7com
https://forumton.org/members/188m7com.36080/#about
https://zb3.org/188m7com/188m-188m-7-com-la-nen-tang-giai-tri-truc-tuyen-duoc-nhieu-nguoi-choi-lua-kxvl
https://aboutpharmacistjobs.com/author/188m7com/
https://forums.littletinyfrogs.com/user/7660996
https://onlyfans.com/188m7com
https://mokum.place/188m7com
https://nyccharterschools.jobboard.io/employers/4121584-188m7com
https://outdoor.surselva.info/en/member/nha-cai-188m/339341130/
https://courses.9marks.org/members/188m7com/profile/
https://savee.com/188m7com/
https://foro.noticias3d.com/vbulletin/member.php?u=334765
https://blueprintue.com/profile/188m7com/
https://boards.rossmanngroup.com/members/188m7com.91900/#about
https://buyerseller.xyz/user/188m7com/
https://paste.toolforge.org/view/9c057579
https://youslade.com/188m7com
https://theamberpost.com/member/188m7com
https://www.gamingtop100.net/server/55225/188m7com
https://www.inkitt.com/188m7com
https://flipboard.social/@188m7com
https://sistacafe.com/user/615631
https://www.doorkeeper.jp/users/jy9ol3rr3t9qsc5bi4sj8ndfz3xs7u?locale=en
https://tokemonkey.com/188m7com
https://forum.uookle.com/home.php?mod=space&uid=1388042
https://www.getlisteduae.com/listings/188m7com
https://forum.pwstudelft.nl/user/188m7com
https://sklad-slabov.ru/forum/user/43135/
https://forum.issabel.org/u/188m7com
https://forum.honorboundgame.com/user-509888.html
https://md.opensourceecology.de/s/WW2CVcwrW
https://md.chaospott.de/s/w2CcyjHjeB
https://pad.fablab-siegen.de/s/MU834U49Qb
https://hackmd.hub.yt/s/FqIQRkUQc
https://hackmd.hub.yt/s/FqIQRkUQc
https://pad.funkwhale.audio/s/FIbI6q-GN
https://www.okaywan.com/home.php?mod=space&uid=796875
http://www.activewin.com/user.asp?Action=Read&UserIndex=4838061&redir=&redirname=Forums
https://www.pintradingdb.com/forum/member.php?action=profile&uid=143423
https://sub4sub.net/forums/users/188m7com/
https://giphy.com/channel/188m7com
https://www.mikocon.com/home.php?mod=space&uid=290379
https://bbs.mikocon.com/home.php?mod=space&uid=290379
https://onlinevetjobs.com/author/188m7com/
https://br.pinterest.com/188m7com/
https://ca.pinterest.com/188m7com/
Terima kasih untuk posting fantastis lainnya. Di mana lagi seseorang dapat mendapatkan jenis informasi seperti itu dengan metode penulisan yang ideal? Saya punya presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Greetings! Very helpful advice on this article! It is the little changes that make the biggest changes. Thanks a lot for sharing!
Keep working ,splendid job!
Some genuinely fantastic information, Gladiolus I observed this.
Saya menghargai usaha yang Anda curahkan untuk membuat posting ini. Informasi yang berguna. Terima kasih!
Terima kasih untuk posting fantastis yang lain. Di mana lagi siapa pun mungkin bisa mendapatkan jenis info seperti itu dengan pendekatan penulisan yang sempurna? Saya memiliki presentasi minggu berikutnya, dan saya berada dalam pencarian informasi seperti ini.
Saya sangat beruntung menemukan situs web ini di Bing, persis seperti yang saya cari : D demikian juga sudah saya simpan ke fav.
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
It’s hard to search out knowledgeable people on this subject, however you sound like you already know what you’re speaking about! Thanks
Postingan yang sangat bagus. Ini memberi saya pemahaman yang lebih jelas tentang topik ini. Teruskan kerja yang hebat!
I like what you guys are up also. Such clever work and reporting! Keep up the superb works guys I have incorporated you guys to my blogroll. I think it will improve the value of my web site 🙂
I went over this website and I think you have a lot of great info , saved to bookmarks (:.
Sangat menarik info !Sempurna persis seperti yang saya cari!
Sangat menarik detail yang Anda utarakan, sangat menghargai telah memposting. “‘Tis an ill wind that blows no minds.” oleh Malaclypse the Younger.
Hi I am so delighted I found your site, I really
found you by error, while I was looking on Askjeeve for something else, Regardless I am here now and
would just like to say thanks for a fantastic post and a all round thrilling blog (I also love
the theme/design), I don’t have time to browse it all at the minute but I have
book-marked it and also added in your RSS feeds, so when I have time I will be back to read a
great deal more, Please do keep up the awesome work.
I together with my buddies happened to be examining the great thoughts on your web page then suddenly got a terrible feeling I never expressed respect to the site owner for those tips. All of the women happened to be consequently joyful to see them and have now honestly been using these things. Appreciate your being quite kind as well as for making a decision on certain perfect ideas most people are really desperate to learn about. My personal honest regret for not expressing appreciation to earlier.
I was just looking for this info for some time. After six hours of continuous Googleing, finally I got it in your web site. I wonder what is the lack of Google strategy that don’t rank this kind of informative web sites in top of the list. Normally the top web sites are full of garbage.
Saya umumnya tidak meninggalkan komentar, tetapi yang ini benar-benar layak. Konten yang hebat dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini menakjubkan. Pekerjaan yang luar biasa!
Attractive component to content. I simply stumbled upon your web site and in accession capital to claim that I acquire in fact loved account your blog posts. Any way I will be subscribing to your feeds or even I success you get admission to constantly fast.
Saya biasanya tidak menulis komentar, tetapi yang ini benar-benar layak. Konten yang hebat dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Tetap saja, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak setuju sepenuhnya, saya menghormati pandangan.
I’ll right away seize your rss feed as I can’t find your e-mail subscription hyperlink or e-newsletter service. Do you’ve any? Please allow me know in order that I may subscribe. Thanks.
Thank you for sharing excellent informations. Your web-site is so cool. I am impressed by the details that you have on this website. It reveals how nicely you perceive this subject. Bookmarked this web page, will come back for more articles. You, my pal, ROCK! I found just the information I already searched all over the place and simply couldn’t come across. What an ideal site.
Saya tidak amat hebat dalam bahasa Inggris tetapi saya menganggap ini amat mudah untuk dibaca .
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Great site you’ve got here.. It’s difficult to find quality writing like yours these days.
I seriously appreciate people like you! Take care!!
Excellent website. Lots of useful info here. I am sending it to some friends ans also sharing in delicious. And obviously, thank you to your effort!
I haven’t checked in here for some time since I thought it was getting boring, but the last several posts are great quality so I guess I’ll add you back to my daily bloglist. You deserve it my friend 🙂
I was recommended this web site by my cousin. I’m no longer sure whether this post is written by way of him as nobody else recognise such particular approximately my trouble. You are incredible! Thanks!
Artikel yang sangat baik! Saya sangat menghargai gaya Anda menjelaskan segala sesuatu dengan mudah dipahami. Teruskan pekerjaan yang hebat!
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya benar-benar senang melihat informasi luar biasa dibagikan secara bebas.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Saya senang menjadi pengunjung dari website sempurna ini!, terima kasih atas informasi langka ini!
Sangat luar biasa info dapat ditemukan di weblog.
Hei semua, Anda telah melakukan pekerjaan yang hebat. Saya pasti akan menandai ini dan kembali untuk membaca konten lainnya. Terima kasih!
Hello There. I discovered your blog the use of msn. That is a really well written article. I’ll be sure to bookmark it and return to learn extra of your useful information. Thanks for the post. I’ll certainly return.
I’ve recently started a blog, the info you offer on this web site has helped me greatly. Thank you for all of your time & work.
Terima kasih untuk situs web informatif lainnya. Di mana lagi saya memperoleh info seperti itu yang ditulis dengan pendekatan yang ideal? Saya memiliki sebuah inisiatif yang saya sedang jalankan, dan saya sudah mengamati informasi seperti ini.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke blog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
I believe you have observed some very interesting points, appreciate it for the post.
I believe that is among the such a lot significant information for me.
And i’m satisfied studying your article. However wanna observation on some basic things, The website
style is perfect, the articles is really great :
D. Excellent activity, cheers
I have recently started a blog, the information you provide on this website has helped me greatly. Thank you for all of your time & work.
Ini adalah blog yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Anda bisa pasti melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Isi yang sangat baik dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
I discovered your blog web site on google and examine a number of of your early posts. Proceed to maintain up the excellent operate. I just additional up your RSS feed to my MSN Information Reader. Searching for ahead to studying extra from you afterward!…
F*ckin’ awesome issues here. I’m very happy to look your article. Thanks a lot and i’m taking a look ahead to contact you. Will you kindly drop me a e-mail?
I’m impressed, I must say. Actually rarely do I encounter a blog that’s both educative and entertaining, and let me inform you, you have hit the nail on the head. Your idea is excellent; the problem is something that not sufficient individuals are speaking intelligently about. I am very completely happy that I stumbled throughout this in my search for one thing referring to this.
Hai semua, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan cukup banyak wawasan yang sangat berguna. Terima kasih!
Saya benar-benar ingin menulis komentar singkat untuk menghargai Anda atas seluruh informasi luar biasa yang Anda bagikan di website ini.
A person essentially help to make seriously articles I would state. This is the first time I frequented your website page and thus far? I amazed with the research you made to create this particular publish incredible. Wonderful job!
Postingan yang sangat membantu. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Nyata luar biasa informasi dapat ditemukan di web blog.
This web site can be a walk-through for all the data you wished about this and didn’t know who to ask. Glimpse right here, and you’ll positively discover it.
Sangat menarik detail yang Anda sebutkan, salam telah mengunggah.
Artikel yang hebat. Ini memberi saya pemahaman yang lebih baik tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Saya secara terus menjelajah online untuk posting yang dapat memberi manfaat saya. Thx!
Rattling informative and good structure of articles, now that’s user pleasant (:.
Thanks – Enjoyed this blog post, how can I make is so that I get an email sent to me every time you write a new update?
Saya kebetulan menemukan situs Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang hebat.
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
hello there and thank you for your information – I have definitely picked up anything new from right here. I did however expertise several technical points using this site, as I experienced to reload the site many times previous to I could get it to load properly. I had been wondering if your hosting is OK? Not that I am complaining, but sluggish loading instances times will sometimes affect your placement in google and can damage your high quality score if ads and marketing with Adwords. Anyway I’m adding this RSS to my e-mail and can look out for a lot more of your respective exciting content. Make sure you update this again soon..
Saya biasanya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang luar biasa dan sangat membantu. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca dalam waktu yang lama. Konten yang sangat berguna. Terima kasih telah berbagi.
Your comment is awaiting moderation.
Comparing best dark web markets based on fees, selection, and community trust.
Dark web market hacking
https://dark-webmarket.com
dark web market user reviews
https://dark-webmarket.com https://dark-webmarket.com
Thanks for another wonderful article. The place else may just anybody get that type of info
in such a perfect method of writing? I’ve a presentation subsequent
week, and I’m on the look for such info.
Artikel yang sangat bagus. Saya benar-benar menyukai cara Anda menyampaikan ide-ide ini. Teruskan pekerjaan yang hebat!
Dengan seluruhnya yang mana tampak sedang dibangun sepanjang topik spesifik ini, sebagian besar pandangan Anda adalah cukup menstimulasi. Walaupun begitu, saya memohon maaf, karena saya tidak setuju sepenuhnya pada seluruh teori Anda, meskipun menstimulasi. Tampaknya bagi kami bahwa ulasan Anda tidak sepenuhnya sepenuhnya dapat dibenarkan dan pada faktanya Anda diri Anda tidak sepenuhnya percaya diri terhadap argumen tersebut. Dalam hal apa pun saya menikmati membacanya.
Saya terkesan dengan situs web ini, sungguh saya adalah penggemar berat.
Postingan yang fantastis. Saya benar-benar menyukai gaya Anda menjelaskan ide-ide ini. Teruskan kerja yang hebat!
I am curious to find out what blog system you’re working with? I’m experiencing some small security issues with my latest site and I would like to find something more safeguarded. Do you have any recommendations?
Terima kasih atas tulisan yang bagus. Sebenarnya ini dulunya adalah sebuah materi hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Konten yang fantastis! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
Artikel yang fantastis! Saya menghargai gaya Anda menguraikan segala sesuatu dengan sangat jelas. Teruskan pekerjaan yang hebat!
Sangat menarik poin yang Anda sebutkan, thankyou telah mengunggah. “Tidak ada apa pun dalam seekor ulat yang memberi tahu Anda bahwa ia akan menjadi kupu-kupu.” oleh Richard Buckminster Fuller.
Menikmati mempelajari ini, sangat bagus, terima kasih.
Situs ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
I love looking at and I conceive this website got some truly utilitarian stuff on it! .
Saya tidak sungguh fantastis dalam bahasa Inggris tetapi saya memperoleh ini sungguh mudah untuk diterjemahkan.
Hai di sana, kamu sudah melakukan kerja yang fantastis. Saya pasti akan menandai ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
Informasi yang sangat berguna. Saya baru saja menelusuri hal-hal seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Ini benar-benar menjawab masalah saya, terima kasih!
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang identik. Apakah ada cara Anda akan bisa menghapus saya dari layanan itu? Terima kasih!
Hei di sana, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan banyak wawasan yang bermanfaat. Terima kasih!
I simply couldn’t go away your website before suggesting that I extremely loved the standard information a person supply on your guests? Is gonna be back continuously to check up on new posts
Saya tidak bisa menahan diri untuk berkomentar
Anda dapat jelas melihat antusiasme Anda di dalam karya yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu kejar hati Anda.
Wohh persis apa yang saya cari, terima kasih atas posting.
Berharga informasi. Untungnya saya menemukan website Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
I am really enjoying the theme/design of your weblog.
Do you ever run into any browser compatibility issues?
A number of my blog readers have complained about my site not working correctly in Explorer but
looks great in Safari. Do you have any tips
to help fix this issue?
Wohh persis apa yang saya telusuri, terimakasih atas unggahan.
Isi yang hebat! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
I saw a lot of website but I believe this one has something special in it in it
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya bersyukur bahwa saya menemukan kembali situs ini, benar-benar informasi yang saya telusuri!
Saya puas bahwa saya mendeteksi situs web ini, tepat informasi yang saya cari!
Saya tidak sering berkomentar tetapi saya harus mengakui salam untuk posting yang satu ini : D.
Bagian yang luar biasa, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia pada kenyataannya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda berkembang menjadi lebih ahli, apakah Anda keberatan memperbarui weblog Anda dengan lebih banyak rincian? Ini sangat berguna bagi saya. Jempol besar untuk publikasi weblog ini!
Terima kasih banyak atas posting yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak informasi yang berguna. Teruskan pekerjaan yang hebat!
Ahaa, its pleasant conversation concerning this article
at this place at this website, I have read all that, so at this time me also commenting here.
my webpage – zguveia01
Isi yang bermanfaat dan disajikan dengan baik. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
You have brought up a very excellent points, thankyou for the post.
Bagian yang luar biasa, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui blog Anda dengan lebih banyak detail? Ini sangat berguna bagi saya. Jempol besar untuk unggahan blog ini!
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Your home is valueble for me. Thanks!…
Deference to author, some excellent selective information.
I have been exploring for a little for any high-quality articles or blog posts on this kind of area . Exploring in Yahoo I at last stumbled upon this site. Reading this info So i’m happy to convey that I have an incredibly good uncanny feeling I discovered just what I needed. I most certainly will make sure to do not forget this site and give it a glance on a constant basis.
Saya sangat menghargai waktu yang Anda curahkan untuk menyusun artikel ini. Konten yang bernilai. Terima kasih banyak!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
I want to show my thanks to the writer for bailing me out of this scenario. As a result of surfing throughout the world-wide-web and seeing basics which were not powerful, I believed my life was done. Existing minus the answers to the issues you’ve sorted out by means of the guide is a critical case, and ones which may have in a negative way affected my entire career if I had not discovered the website. Your good expertise and kindness in dealing with every part was priceless. I’m not sure what I would’ve done if I hadn’t discovered such a stuff like this. I can also at this moment relish my future. Thank you very much for this specialized and amazing help. I will not hesitate to recommend your web page to anybody who would need guide about this subject matter.
Postingan yang sangat membantu. Saya baru saja menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Aw, this was a really good post. Finding the time
and actual effort to produce a top notch article… but what can I say…
I hesitate a lot and never manage to get anything done.
Hey there! I’ve been following your website for a while now and finally got the courage to go ahead and give you a shout out from Dallas Texas! Just wanted to say keep up the good job!
Saya beruntung bahwa saya menemukan website ini, persis info yang saya telusuri!
Sangat menarik detail yang Anda amati, salam telah mengunggah. “Kekuatan tidak datang dari kapasitas fisik. Ia datang dari kehendak yang tak tergoyahkan.” oleh Mohandas Karamchand Gandhi.
Terima kasih, saya baru saja menelusuri informasi sekitar subjek ini sudah lama dan milik Anda adalah yang terbaik yang saya ketahui hingga sekarang. Tapi, bagaimana dengan kesimpulan? Apakah Anda yakin tentang asal tersebut?
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Hmm apakah ada orang lain yang mengalami masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Sangat menarik detail yang Anda utarakan, terima kasih telah memposting.
Saya selalu peduli dengan subjek ini dan masih demikian, terimakasih telah memposting.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri! “Semua ide bagus yang pernah saya miliki datang kepada saya saat saya memerah sapi.” oleh Grant Wood.
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang unggul!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada sarana Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
I just like the valuable info you provide to your articles. I will bookmark your blog and take a look at once more here frequently. I am moderately certain I will be informed many new stuff proper here! Best of luck for the next!
Saya senang menjadi salah satu dari banyak pengunjung di situs web hebat ini (:, terimakasih telah mengunggah.
You actually make it seem so easy along with your presentation but I find this topic to be actually one thing that I believe I’d by no means understand. It seems too complex and extremely huge for me. I am looking forward in your next put up, I’ll attempt to get the cling of it!
Saya terus-menerus menyelidiki online untuk ide yang dapat memberi manfaat saya. Thx!
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Wow! Terima kasih! Saya senantiasa membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menerapkan sebagian dari posting Anda ke blog saya?
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi luar biasa dibagikan secara bebas.
Very interesting topic, regards for posting. “If you have both feet planted on level ground, then the university has failed you.” by Robert F. Goheen.
Secara umum saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup artikel yang bagus.
Ini adalah saran yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
Terima kasih untuk posting hebat yang lain. Di mana lagi siapa pun bisa mendapatkan tipe informasi seperti itu dengan metode penulisan yang ideal? Saya punya presentasi minggu depan, dan saya sedang mencari informasi seperti ini.
Postingan yang bagus. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Konten yang sangat berguna. Saya baru menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi!
Seseorang secara esensial menolong untuk membuat secara signifikan posting saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman web Anda dan sampai saat ini? Saya terkejut dengan analisis yang Anda lakukan untuk membuat posting istimewa ini. Pekerjaan yang mengagumkan!
Postingan yang sangat membantu. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada jalan Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Saya tidak sering berkomentar tetapi saya harus menyatakan salam untuk posting yang sempurna ini : D.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri! “Dia yang mengampuni orang jahat melukai orang baik.” oleh Seneca.
Wow, menakjubkan weblog format! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan situs Anda mengagumkan, belum lagi kontennya!
I visited a lot of website but I conceive this one holds something special in it in it
Hai, saya hanya ingin mengatakan bahwa saya sangat menikmati membaca postingan blog Anda. Ini adalah tepat jenis informasi yang sedang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Saya secara tidak sengaja menemukan blog Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang bagus.
Hai di sana, sekadar ingin mengatakan bahwa saya sangat menyukai membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan cukup banyak wawasan yang sangat berguna. Terima kasih!
magnificent points altogether, you just won a new reader. What would you recommend about your publish that you made some days ago? Any sure?
Great write-up, I’m normal visitor of one’s site, maintain up the excellent operate, and It’s going to be a regular visitor for a long time.
Remarkable issues here. I’m very happy to see your article.
Thank you a lot and I’m having a look ahead to touch you. Will
you kindly drop me a mail?
Saya kebetulan menemukan website Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
Saya mengunjungi banyak website tetapi saya pikir yang satu ini punya sesuatu yang spesial di dalamnya
Hey there! Quick question that’s totally off topic. Do you know how to make your site mobile friendly? My web site looks weird when browsing from my iphone 4. I’m trying to find a theme or plugin that might be able to fix this issue. If you have any recommendations, please share. Many thanks!
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membeli saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda menjadi lebih ahli, apakah Anda keberatan memperbarui weblog Anda dengan lebih banyak rincian? Ini sangat membantu bagi saya. Jempol besar untuk kiriman weblog ini!
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Konten yang fantastis! Gaya penulisan Anda sangat jelas dan mudah dipahami. Saya tentu akan kembali untuk membaca lebih banyak.
Saya sangat menghargai usaha yang Anda luangkan untuk menyusun artikel ini. Konten yang bernilai. Terima kasih!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Seseorang pada dasarnya membantu untuk membuat secara signifikan artikel saya mungkin katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sampai saat ini? Saya terkejut dengan analisis yang Anda lakukan untuk membuat publikasi istimewa ini. Aktivitas yang mengagumkan!
Dating Coach Amsterdam provides significant coaching systems.
Dating Coach Amsterdam enables residents to facilitate confidence.
Dating Coach Amsterdam provides support on using dating apps efficiently.
The Dating Coach Amsterdam at Dating Coach Amsterdam
delivers love and relationship coaching. The Dating
Coach Amsterdam from Dating Coach Amsterdam supports residents in managing emotions.
Dating Coach Amsterdam streamlines understanding of small talk
in dating scenarios. Dating Coach Amsterdam offers clarity for residents seeking authentic relationships.
Dating Coach Amsterdam offers coaching systems in The Netherlands.
The Dating Coach Amsterdam at Dating Coach Amsterdam empowers intimacy in dating.
The Dating Coach Amsterdam from Dating Coach Amsterdam
helps meaningful dating experiences. Dating Coach Amsterdam offers guidance on facilitating confidence.
Dating Coach Amsterdam enables clients to navigate Amsterdam dating.
Dating Coach Amsterdam provides relationship coaching for couples.
The Dating Coach Amsterdam at Dating Coach Amsterdam provides dating coach services.
The Dating Coach Amsterdam from Dating Coach Amsterdam helps
residents in achieving clarity. Dating Coach Amsterdam facilitates transformation through authentic dating experiences.
Dating Coach Amsterdam provides support to clients on managing emotions.
The Dating Coach Amsterdam at Dating Coach Amsterdam offers coaching systems in Amsterdam.
The Dating Coach Amsterdam from Dating Coach Amsterdam assists residents
in facilitating confidence. Dating Coach Amsterdam delivers significant relationship coaching in The Netherlands.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Berharga info. Untungnya saya menemukan situs Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menyimpannya.
Konten yang bermanfaat dan disajikan dengan baik. Saya tentu akan membagikan ini kepada teman-teman. Terima kasih telah berbagi.
Wow! Thank you! I continuously wanted to write on my blog something like that. Can I include a part of your post to my website?
Saya harus mengatakan, ini adalah salah satu artikel paling bagus yang pernah saya baca belakangan ini. Informasi yang sangat membantu. Terima kasih telah berbagi.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Hi there! Do you know if they make any plugins to assist with SEO? I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good results. If you know of any please share. Kudos!
Saya terkesan dengan situs internet ini, benar-benar saya adalah penggemar berat.
Amat bersih situs, terimakasih untuk pos ini.
Hore google adalah raja saya yang membantu saya menemukan website yang luar biasa! .
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Saya tidak bisa menahan diri untuk berkomentar
Konten yang luar biasa! Gaya penulisan Anda jelas dan mudah dipahami. Saya pasti akan kembali untuk melihat konten lainnya.
Perfectly written subject material, appreciate it for information .
Wow, incredible blog structure! How lengthy have you ever been running a blog for? you made running a blog look easy. The total glance of your site is magnificent, as smartly as the content material!
A vital article on VPN technology. It clearly outlines the steps to
setup a VPN and the immense impact it has.
I’m inspired to improve my security through a global ip platform.
It’s easy to make a difference.
After study just a few of the weblog posts in your website now, and I truly like your means of blogging. I bookmarked it to my bookmark website listing and shall be checking again soon. Pls try my web site as effectively and let me know what you think.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
I conceive you have mentioned some very interesting details , thankyou for the post.
You got a very great website, Gladiolus I discovered it through yahoo.
Artikel yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi.
Wow, wonderful blog structure! How long have you ever been running a blog
for? you make running a blog glance easy. The full glance of your web site is
excellent, as neatly as the content material!
Berharga informasi. Untungnya saya menemukan situs Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Postingan yang luar biasa. Saya sungguh menikmati cara Anda menjelaskan ide-ide ini. Teruskan pekerjaan yang hebat!
Halo di sana, hanya ingin mengatakan bahwa saya benar-benar menikmati membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan banyak wawasan yang sangat berguna. Terima kasih!
I have been surfing online greater than three hours lately, yet I by no means found any attention-grabbing article like yours. It is pretty value enough for me. In my view, if all website owners and bloggers made excellent content material as you did, the web will probably be a lot more helpful than ever before.
Saya senang menjadi salah satu pengunjung di situs hebat ini (:, sangat dihargai telah memposting.
Postingan yang sangat baik. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Hi there Dear, are you genuinely visiting this site daily, if so afterward you will definitely get fastidious experience.
I like this website very much, Its a rattling nice post to read and receive info . “Do not use a cannon to kill a mosquito.” by Confucius.
Postingan yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
Mengagumi komitmen yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda tawarkan. Sangat luar biasa menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
I recently came across an eye-opening article about Paybis and honestly it really made
me think.
The guide shared insights on how digital finance is evolving, and it felt real.
After checking it out, I shared it with my uncle, and
he started learning more about crypto. Within the next month, he looked at new income opportunities.
He didn’t just sit around — he approached it seriously.
Eventually, he got close to 150k in results — not overnight, but
through smart decisions.
What surprised me most is how his lifestyle changed.
He even treated himself to a new car, something like an Audi A5,
and started enjoying life more. He even found a partner who
enjoys the same level of comfort.
Of course results can vary, but the story is genuine, and that article definitely opened new perspectives.
There’s actually a way to check it out here, and I’d seriously recommend taking a look.
Opportunities are everywhere if you look closely.
Veja como revisar TCC nas normas ABNT com checklist prático de estrutura, capa, sumário, citações e referências antes da entrega.
I am now not certain where you’re getting your info, however great topic. I needs to spend a while finding out much more or working out more. Thank you for wonderful information I was searching for this info for my mission.
I love it when people come together and share opinions, great blog, keep it up.
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.
I genuinely enjoy looking at on this web site, it contains great blog posts.
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
Greetings from Florida! I’m bored to tears at work
so I decided to browse your site on my iphone during lunch break.
I love the knowledge you present here and can’t wait to take a look when I get home.
I’m surprised at how quick your blog loaded on my
cell phone .. I’m not even using WIFI, just 3G ..
Anyways, amazing site!
Thanks on your marvelous posting! I really enjoyed
reading it, you are a great author.I will be sure to bookmark your blog and definitely will
come back at some point. I want to encourage continue your great
job, have a nice morning!
Hi my friend! I wish to say that this article is awesome, nice written and include approximately all significant infos. I’d like to see more posts like this.
Thank you for any other great article. The place else may just anybody get that kind of information in such an ideal method of writing? I’ve a presentation next week, and I am on the search for such info.
I’ve learn some excellent stuff here. Certainly worth bookmarking for revisiting. I surprise how a lot effort you set to make such a fantastic informative website.
Hello, you used to write magnificent, but the last several posts have been kinda boring?K I miss your super writings. Past few posts are just a little out of track! come on!
Sweet web site, super design, very clean and apply genial.
Cabinet IQ
8305 Ꮪtate Hwyy 71 #110, Austin,
TX 78735, United Ѕtates
254-275-5536
Bookmarks
I don’t commonly comment but I gotta state thanks for the post on this one :D.
Quality articles is the key to invite the users to
go to see the website, that’s what this web page is providing.
Some genuinely fantastic info , Gladiolus I detected this. “Traffic signals in New York are just rough guidelines.” by David Letterman.
Excellent blog here! Also your website loads up fast! What host are you using? Can I get your affiliate link to your host? I wish my web site loaded up as quickly as yours lol
whoah this blog is magnificent i like reading your articles. Stay up the great paintings! You realize, a lot of individuals are looking round for this information, you can aid them greatly.
magnificent points altogether, you simply gained a new reader. What would you suggest in regards to your post that you made some days ago? Any positive?
Really clean internet site, thanks for this post.
An interesting discussion is worth comment. I think that you should write more on this topic, it might not be a taboo subject but generally people are not enough to speak on such topics. To the next. Cheers
I am glad that I observed this web blog, exactly the right information that I was looking for! .
Triangle Billiarxs & Bar Stools
1471 Nisson Ꮢɗ, Tustin,
CA 92780, United Stateѕ
+17147715380
Shuffleboard Purchase
I am now not sure where you are getting your info, however good topic. I must spend some time finding out more or figuring out more. Thank you for great info I used to be looking for this information for my mission.
I do agree with all the ideas you have presented in your post. They’re really convincing and will definitely work. Still, the posts are very short for novices. Could you please extend them a bit from next time? Thanks for the post.
I am glad to be a visitant of this perfect blog! , thankyou for this rare info ! .
Hello this is kinda of off topic but I was wondering if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding skills so I wanted to get guidance from someone with experience. Any help would be enormously appreciated!
I’ve been absent for a while, but now I remember why I used to love this web site. Thank you, I will try and check back more frequently. How frequently you update your site?
A large percentage of of whatever you point out happens to be astonishingly legitimate and it makes me ponder why I hadn’t looked at this with this light before. Your piece really did switch the light on for me as far as this issue goes. Nonetheless there is 1 point I am not necessarily too cozy with so whilst I make an effort to reconcile that with the central idea of the issue, let me see what the rest of your visitors have to say.Very well done.
Whats up this is kind of of off topic but I was wanting to know if
blogs use WYSIWYG editors or if you have to manually code with HTML.
I’m starting a blog soon but have no coding knowledge so I wanted to get
advice from someone with experience. Any help would be
greatly appreciated!
I discovered your blog web site on google and check a couple of of your early posts. Proceed to keep up the very good operate. I just further up your RSS feed to my MSN News Reader. Seeking ahead to studying extra from you afterward!…
excellent publish, very informative. I wonder why the other experts of this sector don’t realize this. You should continue your writing. I’m confident, you’ve a great readers’ base already!
I have to express appreciation to you just for rescuing me from this particular instance. After researching throughout the the net and coming across techniques which are not powerful, I believed my life was over. Existing without the presence of answers to the problems you’ve sorted out as a result of your good report is a serious case, and the kind which might have in a negative way damaged my entire career if I hadn’t discovered your blog post. Your primary competence and kindness in maneuvering all areas was excellent. I am not sure what I would have done if I hadn’t come across such a stuff like this. I am able to at this point look forward to my future. Thanks a lot very much for your specialized and results-oriented help. I won’t hesitate to refer your web site to anybody who requires tips on this area.
Just desire to say your article is as astounding. The clarity for your submit is simply cool and i could suppose you are knowledgeable in this subject. Well with your permission allow me to clutch your RSS feed to stay updated with approaching post. Thank you 1,000,000 and please keep up the rewarding work.
I think this is one of the so much vital info for me. And i’m happy studying your article. But should commentary on some common things, The site taste is great, the articles is actually nice :D. Just right job, cheers
you’re actually a just right webmaster. The web site loading pace is amazing.
It kind of feels that you are doing any distinctive trick.
Moreover, The contents are masterwork. you have performed a magnificent
process in this matter!
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
Thanks for the marvelous posting! I genuinely enjoyed reading it, you could be a great author.I will be sure to bookmark your blog and definitely will come back from now on. I want to encourage continue your great writing, have a nice weekend!
You’re so awesome! I do not believe I have read through a single thing like this before.
So nice to discover somebody with a few
unique thoughts on this topic. Really.. many thanks for starting this up.
This website is something that is required on the web, someone with some originality!
I gotta favorite this website it seems invaluable extremely helpful
I would like to thnkx for the efforts you have put in writing this site. I am hoping the same high-grade website post from you in the upcoming as well. Actually your creative writing abilities has inspired me to get my own site now. Really the blogging is spreading its wings fast. Your write up is a good example of it.
I like the helpful info you provide on your articles. I’ll bookmark your weblog and test once more here regularly. I am relatively certain I’ll be informed lots of new stuff proper here! Best of luck for the following!
Thank you for some other informative blog. Where else may I get that kind of info written in such a perfect manner? I have a venture that I’m simply now operating on, and I’ve been on the look out for such info.
I blog often and I truly appreciate your information. This article
has truly peaked my interest. I will bookmark your website and keep checking for new details about
once per week. I opted in for your RSS feed as well.
Not long ago I found an detailed article about Paybis and honestly it
really made me think.
The article explained how people are using crypto in smarter ways, and it felt real.
After reading it, I told my uncle, and he decided to explore it.
Within the next month, he looked at new income opportunities.
He didn’t just sit around — he approached it seriously.
Eventually, he even pushed towards 200k depending on timing — not overnight,
but through smart decisions.
What surprised me most is how his lifestyle changed. He even finally bought something he
always wanted, something like a Mercedes-Benz C-Class, and completely changed his
mindset. He even met someone new who shares
his lifestyle.
I’m not saying this will happen to everyone, but the story
is genuine, and that article definitely changed the way we look at money.
There’s actually a link in this comment, and I’d seriously recommend taking a look.
You never know what small discovery can change
things.
Hey there, You’ve done a fantastic job. I’ll certainly digg it and personally suggest to my friends. I am sure they will be benefited from this website.
fantastic publish, very informative. I ponder why the opposite specialists of this sector do not understand this. You must continue your writing. I’m confident, you have a great readers’ base already!
Wow! Thank you! I permanently needed to write on my website something like that. Can I take a part of your post to my website?
I’m not sure why but this web site is loading very slow for me. Is anyone else having this problem or is it a issue on my end? I’ll check back later on and see if the problem still exists.
Heya i am for the primary time here. I came across this board and I to find It truly helpful & it helped me out a lot. I hope to give one thing again and aid others like you helped me.
We absolutely love your blog and find most of your post’s to be what precisely I’m looking for. Do you offer guest writers to write content to suit your needs? I wouldn’t mind composing a post or elaborating on some of the subjects you write related to here. Again, awesome site!
Triangle Billiards & Bar Stools
1471 Nisson Ꭱd, Tustin,
ϹA 92780, United Ѕtates
+17147715380
Bookmarks
This is the right blog for anyone who wants to find out about this topic. You realize so much its almost hard to argue with you (not that I actually would want…HaHa). You definitely put a new spin on a topic thats been written about for years. Great stuff, just great!
Hey there! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing a few months of hard work due to no backup. Do you have any methods to stop hackers?
What i don’t realize is in reality how you are now not actually much more well-appreciated than you might be now. You’re so intelligent. You recognize therefore considerably with regards to this matter, produced me in my view consider it from so many varied angles. Its like men and women are not involved unless it is one thing to accomplish with Woman gaga! Your personal stuffs great. Always maintain it up!
I would like to express my love for your generosity giving support to men who should have help with in this subject. Your real commitment to passing the solution all around appears to be remarkably important and has regularly encouraged people like me to attain their pursuits. Your new warm and helpful report can mean a lot to me and much more to my mates. Regards; from all of us.
Hi, Neat post. There’s a problem along with your site in web explorer, might check thisK IE nonetheless is the market chief and a big component to other people will omit your magnificent writing because of this problem.
An impressive share, I simply given this onto a colleague who was doing a bit of analysis on this. And he in truth bought me breakfast as a result of I discovered it for him.. smile. So let me reword that: Thnx for the deal with! But yeah Thnkx for spending the time to debate this, I really feel strongly about it and love studying extra on this topic. If possible, as you turn out to be experience, would you mind updating your weblog with extra particulars? It is extremely useful for me. Big thumb up for this blog submit!
My brother recommended I might like this website.
He was totally right. This post actually made my day. You cann’t imagine just how much time I had spent for this info!
Thanks!
My wife and i ended up being now happy when Ervin managed to carry out his inquiry while using the ideas he made out of your web site. It’s not at all simplistic to just possibly be giving away secrets the others have been making money from. And now we figure out we need the website owner to give thanks to for this. The explanations you’ve made, the easy blog menu, the relationships your site help to engender – it is all unbelievable, and it is letting our son and the family know that the article is amusing, and that’s really essential. Many thanks for all the pieces!
What’s up every one, here every person is sharing such know-how, thus it’s good to read this web site,
and I used to pay a quick visit this website every day.
I appreciate, cause I found exactly what I was looking for. You have ended my 4 day long hunt! God Bless you man. Have a nice day. Bye
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari baik. Bye
This is my first time visit at here and i am in fact impressed to
read everthing at alone place.
Saya senang menjadi pengunjung dari website abadi ini!, terimakasih atas info langka ini!
Terima kasih atas tulisan yang baik. Sebenarnya ini dulunya adalah sebuah akun hiburan. Terlihat maju menjadi jauh lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat tetap berkomunikasi?
Howdy! This is my first comment here so I just wanted to give a quick shout out and say I genuinely enjoy reading your articles. Can you suggest any other blogs/websites/forums that go over the same topics? Appreciate it!
Great website. Lots of useful information here. I’m sending it to several friends ans also sharing in delicious. And obviously, thanks for your effort!
Very nice post. I just stumbled upon your blog and wished to say that I’ve really enjoyed browsing your blog posts. After all I’ll be subscribing to your rss feed and I hope you write again soon!
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan berterima kasih kepada Anda.
I like this blog so much, bookmarked.
Sangat menarik poin yang Anda catat, salam telah memposting.
Sangat bersih web site, terimakasih untuk pos ini.
Great article on surgery costs. Bookmarked.
Hey there, I think your website might be having browser compatibility issues. When I look at your website in Chrome, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, wonderful blog!
Halo semua, hanya ingin mengatakan bahwa saya sangat menikmati membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan banyak informasi yang sangat berguna. Terima kasih!
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Triangle Billirds & Bar Stools
1471 Nisson Ꮢɗ, Tustin,
ϹA 92780, United Stateѕ
+17147715380
Billiard Table Restoration Execution
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Kerja yang fantastis!
Benar-benar indah info dapat ditemukan di web blog.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Isi yang sangat baik dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
You have brought up a very good points, appreciate it for the post.
Ini adalah tips yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Anda sudah melakukan pekerjaan yang luar biasa dan seluruh komunitas kami akan berterima kasih kepada Anda.
I went over this web site and I conceive you have a lot of fantastic info , saved to fav (:.
I’ve learn several good stuff here. Certainly price bookmarking for revisiting. I wonder how much attempt you place to make such a fantastic informative site.
Seiring dengan semua hal yang mana tampak sedang berkembang sepanjang topik ini, sebagian besar pandangan Anda ternyata lumayan menarik. Kendati demikian, saya minta maaf, karena saya tidak setuju sepenuhnya pada keseluruhan teori Anda, meskipun menggairahkan. Sepertinya bagi kami bahwa komentar Anda tidak sepenuhnya rasional dan pada faktanya Anda sendiri tidak benar-benar sepenuhnya yakin terhadap argumen tersebut. Dalam hal apa pun saya menikmati membacanya.
Sangat menarik detail yang Anda utarakan, terima kasih telah memposting. “Grup musik tiup itu baik di tempatnya — di luar ruangan dan beberapa mil jauhnya.” oleh Sir Thomas Beecham.
What i don’t realize is in fact how you are no longer really a lot more smartly-liked than you may be now.
You are very intelligent. You understand therefore significantly relating to this subject, made me in my
view imagine it from numerous various angles. Its like men and women are not involved unless it is one thing to do with Woman gaga!
Your personal stuffs outstanding. At all times take care of it up!
Rattling clear internet site, thanks for this post.
Aku benar-benar ingin menulis komentar singkat untuk mengucapkan terima kasih Anda atas seluruh tips luar biasa yang Anda bagikan di website ini.
Saya mendapatkan info yang bagus dari blog Anda.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I think this is one of the most important info for me. And i am glad reading your article. But should commentary on some common things, The web site style is wonderful, the articles is in reality great :D. Just right task, cheers
Not long ago I found an detailed article about Paybis and honestly I
didn’t expect much at first but it impressed me.
The post broke down how beginners can get into crypto safely,
and it was easy to follow.
After going through it, I shared it with my uncle, and he started learning more about crypto.
Within the next month, he became much more confident with finances.
He didn’t just sit around — he approached it seriously.
Eventually, he managed to reach around 100k — not overnight, but through smart decisions.
What surprised me most is how his lifestyle changed.
He even upgraded his lifestyle, something like
an Audi A5, and completely changed his mindset. He even built a
new social circle around success.
Of course results can vary, but the story is true from what I’ve
seen, and that article definitely made a big impact.
There’s actually a source included here, and I’d seriously say it’s worth your time.
Sometimes one good article can shift your mindset.
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Saya benar-benar gembira menemukan situs internet ini di Bing, persis seperti yang saya cari : D juga sudah saya simpan ke favorit.
Pretty! This was a really wonderful post. Thank you for your provided information.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Postingan yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Postingan yang luar biasa. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
Saya senang menjadi salah satu dari banyak pengunjung di situs hebat ini (:, salam telah mengunggah.
I respect your piece of work, appreciate it for all the informative blog posts.
Seseorang pada dasarnya membantu untuk membuat secara serius artikel saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga kini? Saya terkagum dengan analisis yang Anda lakukan untuk menyusun publikasi istimewa ini. Proses yang mengagumkan!
Saya tidak bisa menahan diri untuk berkomentar
Ini adalah tips yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Thanks for any other great article. The place else may just anyone get that kind of information in such a perfect approach of writing? I’ve a presentation subsequent week, and I’m at the look for such information.
You could certainly see your enthusiasm within the paintings you write. The world hopes for more passionate writers such as you who are not afraid to say how they believe. All the time go after your heart.
Saya kebetulan menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang luar biasa.
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Some really nice and useful info on this web site, also I conceive the style contains excellent features.
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada cara Anda bisa menghapus saya dari layanan itu? Terima kasih!
Saya tidak bisa menahan diri untuk berkomentar
Saya terus-menerus melihat online untuk artikel yang dapat menolong saya. Thx!
Wonderful blog! I found it while searching on Yahoo News. Do you have any tips on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Thank you
Seseorang secara esensial memberikan bantuan untuk membuat sangat artikel saya mungkin katakan. Itu adalah pertama kalinya saya mengunjungi halaman web Anda dan hingga sekarang? Saya terkagum dengan analisis yang Anda lakukan untuk membuat kiriman menakjubkan ini. Proses yang luar biasa!
I’m not that much of a online reader to be honest but your blogs really nice, keep it up!
I’ll go ahead and bookmark your website to come back down the road.
Many thanks
Namun, terima kasih untuk poin yang hebat ini dan meskipun saya tidak benar-benar setuju sepenuhnya, saya menghargai pandangan.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada cara Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Saya biasanya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang luar biasa dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
I absolutely love your blog.. Pleasant colors & theme. Did you create this site yourself?
Please reply back as I’m trying to create my own personal site and would
love to learn where you got this from or exactly what the theme is called.
Thanks!
Terima kasih untuk website informatif tambahan. Di mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan pendekatan yang sempurna? Saya punya sebuah proyek yang saya tengah kerjakan sekarang, dan saya sudah mengamati informasi seperti ini.
Postingan yang sangat baik. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Hore google adalah ratu saya yang membantu saya menemukan situs internet yang luar biasa! .
Your comment is awaiting moderation.
Kraken – это глобальная платформа, которая открывает перед покупателями уникальные возможности.
Здесь вы можете найти товары любых категорий: от модных аксессуаров до редких коллекционных предметов.
Покупки на Актуальные адреса KRAKEN 2026 года (⧎‿⧎) доступны сейчас () всегда удобны благодаря системе защиты
сделок и продуманному интерфейсу.
Каждый день KRAKEN (♞‿♞) актуальный доступ через зеркала ➛ предлагает
своим клиентам свежие скидки и уникальные предложения.
Начните пользоваться преимуществами удобного и выгодного шопинга с (/|\✫/|\) KRAKEN площадка 2026 года ⟹ актуальные зеркала и проверенные ссылки ⟿ прямо сейчас.
Wow! Ini bisa jadi salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Luar biasa. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Saya mendapatkan info yang bagus dari blog Anda.
Hi there, I log on to your new stuff regularly.
Your story-telling style is awesome, keep it up!
성남출장마사지 안마 서비스는 24시간 연중무휴로 운영됩니다.
늦은 밤이나 새벽에도 이용 가능하며, 성남 전 지역에 대기 중인 관리사가 있어 언제든 편한 시간에 예약 가능합니다
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang unggul!
Postingan yang sangat bagus. Saya benar-benar menyukai cara Anda menyampaikan gagasan-gagasan ini. Teruskan pekerjaan yang luar biasa!
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
Woah! I’m really digging the template/theme of this website.
It’s simple, yet effective. A lot of times it’s hard to get
that “perfect balance” between user friendliness and visual appeal.
I must say that you’ve done a very good job with this.
Also, the blog loads super fast for me on Safari.
Outstanding Blog!
Hiya, I’m really glad I have found this info. Today bloggers publish only about gossips and internet and this is really frustrating. A good site with exciting content, that’s what I need. Thanks for keeping this web-site, I will be visiting it. Do you do newsletters? Cant find it.
Great post. I am facing a couple of these problems.
I am not very great with English but I line up this really leisurely to interpret.
RebirthRO – The Original Ragnarok Online Private Server (Since 2004)
RebirthRO is the original Rebirth Ragnarok Online private server,
founded in 2004 and one of the longest-running RO private server
communitie. Now continuing as RevivalRO, it offers two unique servers: Freya (Renewal EP21, 30x/30x/10x with 4th jobs) and Loki (Pre-Renewal,
100x/100x/50x classic gameplay). Free-to-play on PC and Android with no pay-to-win. Join an active global community with custom content,
frequent updates, and 20+ years of Ragnarok legacy. Play now at ragnarevival.com
Yeah bookmaking this wasn’t a bad conclusion outstanding post! .
Do you have a spam problem on this website; I also am a blogger, and I was wanting to know your situation; many of us have developed some nice methods and we are looking to exchange strategies with other folks, why not shoot me an email if interested.
Howdy! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche. Your blog provided us useful information to work on. You have done a extraordinary job!
Utterly composed written content, Really enjoyed reading through.
Ya menyimpan ini bukanlah keputusan yang berisiko tinggi posting yang hebat! .
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang mantap!
Saya melihat banyak website tetapi saya percaya yang satu ini punya sesuatu yang ekstra di dalamnya
It’s remarkable to pay a quick visit this site and reading the
views of all mates concerning this article, while I am also keen of getting know-how.
I just could not depart your site prior to suggesting that I extremely enjoyed the standard information a person provide for your visitors? Is going to be back often to check up on new posts
Hai semua, Anda telah melakukan kerja yang hebat. Saya pasti akan menyimpan ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sesungguhnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka membaca lebih banyak tentang topik ini. Jika dapat dicapai, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui weblog Anda dengan lebih banyak detail? Ini sangat membantu bagi saya. Jempol luar biasa untuk posting blog ini!
It’s truly very complicated in this busy life to listen news on Television, so I just use web for that reason,
and get the newest information.
A person necessarily lend a hand to make critically articles I might state.
This is the first time I frequented your website page and to this point?
I amazed with the analysis you made to make this actual put up extraordinary.
Magnificent task!
Saya biasanya tidak meninggalkan komentar, tetapi yang satu ini benar-benar pantas. Konten yang hebat dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
As soon as I detected this website I went on reddit to share some of the love with them.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Isi yang fantastis! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
you have a great blog here! would you like to make some invite posts on my blog?
Hei semua, sekadar ingin mengatakan bahwa saya sangat menikmati membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan banyak wawasan yang sangat berguna. Terima kasih!
Saya senang menjadi salah satu dari banyak pengunjung di situs web hebat ini (:, sangat dihargai telah mengunggah.
Postingan yang hebat. Saya benar-benar menikmati gaya Anda menyampaikan ide-ide ini. Teruskan kerja yang luar biasa!
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia pada kenyataannya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Akan tetapi ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari tambahan tentang topik ini. Jika dapat dicapai, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak detail? Ini sangat membantu bagi saya. Jempol besar untuk unggahan weblog ini!
I am so happy to read this. This is the kind of manual that needs to be given and not the accidental misinformation that’s at the other blogs. Appreciate your sharing this best doc.
fantastic put up, very informative. I’m wondering why the other specialists of this sector don’t understand this. You must continue your writing. I’m sure, you’ve a huge readers’ base already!
Terima kasih banyak atas artikel yang luar biasa. Saya benar-benar menikmati membaca ini dan menemukan banyak informasi yang bermanfaat. Teruskan pekerjaan yang bagus!
Everything is very open with a really clear explanation of the issues.
It was really informative. Your website is very helpful. Many thanks for sharing!
Situs ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Outstanding post, you have pointed out some good points, I besides believe this s a very good website.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Saya sungguh gembira menemukan website ini di Bing, persis seperti yang saya telusuri : D selain itu sudah saya simpan di bookmark saya.
Hello! I know this is kind of off topic but I was wondering which blog platform are you using for this website? I’m getting fed up of WordPress because I’ve had issues with hackers and I’m looking at alternatives for another platform. I would be awesome if you could point me in the direction of a good platform.
I discovered your weblog web site on google and examine a number of of your early posts. Proceed to maintain up the excellent operate. I just extra up your RSS feed to my MSN Information Reader. Searching for forward to studying extra from you in a while!…
Keep on working, great job!
Saya tidak amat hebat dalam bahasa Inggris tetapi saya memperoleh ini sungguh ringan untuk dipahami.
If you would like to get a good deal from this post then you have to apply such techniques to
your won website.
I found your blog web site on google and examine a number of of your early posts. Continue to maintain up the excellent operate. I just further up your RSS feed to my MSN Information Reader. In search of forward to reading more from you later on!…
Ini adalah topik yang sangat penting di hati saya, cheers, tapi di manakah informasi kontak Anda?
Hello There. I found your blog using msn. This is a
really well written article. I will make sure to bookmark it and
come back to read more of your useful information. Thanks for the post.
I will certainly comeback.
I will immediately grab your rss as I can not in finding your e-mail subscription hyperlink or newsletter
service. Do you’ve any? Please permit me know in order that
I may just subscribe. Thanks.
I see something truly special in this website.
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi megah dibagikan secara bebas.
Saya tidak bisa menahan diri untuk berkomentar
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Have you ever thought about adding a little bit more than just your articles? I mean, what you say is important and everything. But imagine if you added some great pictures or video clips to give your posts more, “pop”! Your content is excellent but with images and clips, this site could certainly be one of the best in its field. Superb blog!
Hello, you used to write excellent, but the last several posts have been kinda boringK I miss your tremendous writings. Past few posts are just a little out of track! come on!
Nyata mantap informasi dapat ditemukan di website.
Just desire to say your article is as surprising. The clearness in your post is simply cool and i could assume you are an expert on this subject. Fine with your permission allow me to grab your feed to keep up to date with forthcoming post. Thanks a million and please keep up the rewarding work.
Howdy very nice site!! Guy .. Beautiful .. Wonderful .. I’ll bookmark your blog and take the feeds alsoKI’m satisfied to find so many useful info right here within the post, we’d like work out more strategies on this regard, thanks for sharing. . . . . .
Saya kebetulan menemukan website Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna desain yang hebat!
Nice post. I learn something more challenging on different blogs everyday. It will always be stimulating to read content from other writers and practice a little something from their store. I’d prefer to use some with the content on my blog whether you don’t mind. Natually I’ll give you a link on your web blog. Thanks for sharing.
I was more than happy to find this web-site.I wanted to thanks in your time for this wonderful learn!! I undoubtedly having fun with each little bit of it and I have you bookmarked to take a look at new stuff you weblog post.
Hebat website yang Anda miliki, tapi saya ingin tahu apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin sekali menjadi bagian dari kelompok di mana saya bisa mendapatkan umpan balik dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Saya melihat banyak website tetapi saya pikir yang satu ini memiliki sesuatu yang ekstra di dalamnya
Hurrah, that’s what I was seeking for, what a data! present here at
this webpage, thanks admin of this web site.
I think other website owners should take this internet site as an example , very clean and great user genial design.
Saya tidak sungguh hebat dalam bahasa Inggris tetapi saya menyadari ini sangat mudah untuk diterjemahkan.
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Wow! Terima kasih! Saya senantiasa ingin menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke website saya?
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
Hei di sana, kamu sudah melakukan pekerjaan yang luar biasa. Saya tentu akan menandai ini dan kembali untuk melihat konten lainnya. Terima kasih banyak!
Hello. remarkable job. I did not expect this. This is a impressive story. Thanks!
Hore google adalah penguasa dunia saya yang menolong saya menemukan situs internet yang luar biasa! .
Hey I know this is off topic but I was wondering if you knew of any widgets I could add to my blog that automatically
tweet my newest twitter updates. I’ve been looking for a
plug-in like this for quite some time and was hoping maybe you would have some experience with something like this.
Please let me know if you run into anything. I truly enjoy reading your blog and I look forward to your new updates.
I love it when people come together and share opinions, great blog, keep it up.
Saya tidak umumnya berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang spesial ini : D.
Saya selalu menjelajah online untuk ide yang dapat menolong saya. Thanks!
Saya benar-benar ingin menulis komentar singkat guna mengucapkan terima kasih Anda atas seluruh tips luar biasa yang Anda tuliskan di situs ini.
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada metode Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
Loving the information on this website , you have done great job on the posts.
Wonderful beat ! I would like to apprentice while you amend
your site, how could i subscribe for a blog web site?
The account helped me a acceptable deal. I had been a little
bit acquainted of this your broadcast offered bright clear idea
Website ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
I as well as my buddies ended up reviewing the nice key points on your web blog while all of the sudden developed an awful suspicion I never expressed respect to the blog owner for those secrets. All of the young boys are already for that reason warmed to see them and already have clearly been tapping into these things. We appreciate you being really considerate and for making a decision on certain high-quality subjects most people are really wanting to be aware of. Our sincere regret for not saying thanks to you sooner.
Umumnya saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, cukup artikel yang bagus.
Saya kebetulan menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan pekerjaan yang luar biasa.
Thank you for the sensible critique. Me and my neighbor were just preparing to do a little research about this. We got a grab a book from our local library but I think I learned more from this post. I’m very glad to see such excellent info being shared freely out there.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Hello! I’ve been reading your blog for some time now and finally got the courage to go ahead and give you a shout out from Humble Texas! Just wanted to tell you keep up the excellent job!
Saya tidak biasanya berkomentar tetapi saya harus mengatakan terimakasih untuk posting yang sempurna ini : D.
Greate pieces. Keep posting such kind of information on your page.
Im really impressed by your blog.
Hello there, You’ve done a great job. I will definitely digg
it and in my view recommend to my friends. I’m sure they will be benefited from this
web site.
Berharga info. Beruntung saya menemukan website Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak terjadi lebih awal! Saya mem-bookmark.
Sangat baik info dapat ditemukan di blog.
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan daerah kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi megah dibagikan secara bebas.
It’s a shame you don’t have a donate button! I’d certainly donate
to this fantastic blog! I suppose for now i’ll settle for book-marking and adding your
RSS feed to my Google account. I look forward to brand new updates and will share this site with my Facebook group.
Talk soon!
whoah this blog is excellent i love reading your articles.
Keep up the great work! You recognize, lots of persons are searching around for this
information, you can help them greatly.
Postingan yang luar biasa. Ini memberikan saya gambaran yang lebih jelas tentang subjek ini. Teruskan kerja yang luar biasa!
Touche. Sound arguments. Keep up the amazing spirit.
I have been exploring for a little for any high-quality articles or blog posts in this kind of space . Exploring in Yahoo I at last stumbled upon this web site. Reading this information So i’m happy to convey that I’ve a very just right uncanny feeling I discovered exactly what I needed. I such a lot unquestionably will make certain to don’t forget this site and provides it a glance on a continuing basis.
Hello just wanted to give you a quick heads up. The text in your content seem to be running off the screen in Chrome. I’m not sure if this is a formatting issue or something to do with web browser compatibility but I thought I’d post to let you know. The design look great though! Hope you get the problem resolved soon. Cheers
Terima kasih untuk situs informatif tambahan. Di mana lagi saya memperoleh informasi seperti itu yang ditulis dengan pendekatan yang ideal? Saya memiliki sebuah usaha yang saya tengah kerjakan sekarang, dan saya sudah mencari informasi seperti ini.
Kami dapat memiliki tautan alternatif kesepakatan antara kita!
I was very pleased to find this web-site.I wanted to thanks for your time for this wonderful read!! I definitely enjoying every little bit of it and I have you bookmarked to check out new stuff you blog post.
Hi there friends, good article and good urging commented here, I am in fact enjoying by these.
Saya benar-benar ingin mengirim komentar singkat untuk mengucapkan terima kasih Anda atas semua tips luar biasa yang Anda tuliskan di situs ini.
Hi, Neat post. There is a problem with your web site in internet explorer, would check this… IE still is the market leader and a large portion of people will miss your great writing due to this problem.
Saya senang menjadi salah satu dari beberapa pengunjung di situs internet luar biasa ini (:, salam telah mengunggah.
Terima kasih banyak atas artikel yang sangat baik. Saya benar-benar menyukai membaca ini dan menemukan banyak sekali informasi yang bermanfaat. Teruskan kerja yang bagus!
Postingan yang luar biasa. Ini memberi saya gambaran yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
Hebat website yang Anda miliki, tapi saya penasaran apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin menjadi bagian dari komunitas di mana saya bisa mendapatkan saran dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Salut!
Definitely believe that that you said. Your favorite justification appeared to be on the net the simplest thing to bear in mind of. I say to you, I certainly get annoyed whilst other people consider concerns that they plainly don’t understand about. You managed to hit the nail upon the top and defined out the whole thing with no need side-effects , other folks can take a signal. Will likely be back to get more. Thanks
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya selalu peduli dengan topik ini dan tetap masih demikian, terimakasih telah mengunggah.
Really fantastic info can be found on web blog. “Compassion for myself is the most powerful healer of them all.” by Theodore Isaac Rubin.
Вы довольно четко изложили свою точку зрения!.
Here is my web-site: магазин пряжи официальный (https://trump.nmg46.com/home.php?mod=space&uid=108394&do=thread&view=me&type=thread&from=space)
Seseorang pada dasarnya memberikan bantuan untuk membuat secara kritis posting saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sampai saat ini? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun unggahan menakjubkan ini. Kerja yang luar biasa!
소액 결제(휴대폰 소액결제)는 온라인
가맹점에서 유료 콘텐츠나 물품 구매 시, 결제
대금을 [휴대폰 번호 인증을 통해 다음 달 휴대폰 요금에 합산하여 청구하는 결제 방식]입니다.
I really enjoy studying on this web site, it has great content. “It is easy to be nice, even to an enemy – from lack of character.” by Dag Hammarskjld.
Aku benar-benar ingin menulis komentar singkat untuk mengucapkan terima kasih Anda atas seluruh informasi luar biasa yang Anda bagikan di website ini.
I’m curious to find out what blog platform you have been using? I’m having some minor security issues with my latest blog and I would like to find something more safe. Do you have any solutions?
Sweet blog! I found it while searching on Yahoo News. Do you have any
suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Appreciate it
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi sangat baik dibagikan secara bebas.
Halo semua, saya menemukan situs Anda lewat Google saat menelusuri subjek yang sebanding, website Anda tampil di posisi atas. Saya perlu mengakui bahwa saya kagum betapa rapi penulisannya. Saya sangat menikmati menelusuri ini dan saya akan kembali untuk melihat lebih banyak. Terima kasih banyak!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang unggul!
Isi yang bermanfaat dan disajikan dengan baik. Saya pasti akan membagikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Saya terus memikirkan hal ini, salam telah memposting.
Hi there are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and set up my own. Do you require any coding knowledge to make your own blog? Any help would be really appreciated!
Its good as your other articles : D, thanks for posting. “Before borrowing money from a friend it’s best to decide which you need most.” by Joe Moore.
Artikel yang bagus. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Very good post. I will be going through some of these issues as
well..
Hai di sana, sekadar ingin mengatakan bahwa saya sangat menikmati membaca menelusuri postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan cukup banyak wawasan yang bermanfaat. Terima kasih!
Saya kebetulan menemukan situs Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan kerja yang bagus.
Saya gembira bahwa saya mendeteksi situs web ini, persis informasi yang saya cari!
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya sangat senang melihat informasi megah dibagikan secara bebas.
This web site can be a walk-by means of for all the data you needed about this and didn’t know who to ask. Glimpse here, and you’ll positively discover it.
Yay google is my world beater assisted me to find this great internet site! .
Wow that was odd. I just wrote an really long comment but after I clicked submit my comment didn’t appear. Grrrr… well I’m not writing all that over again. Regardless, just wanted to say wonderful blog!
I’ve been exploring for a little bit for any high-quality articles or weblog posts on this kind of house . Exploring in Yahoo I finally stumbled upon this web site. Reading this information So i’m happy to show that I’ve a very excellent uncanny feeling I found out just what I needed. I so much no doubt will make sure to do not omit this site and give it a glance on a continuing basis.
I conceive you have mentioned some very interesting details, thankyou for the post.
Excellent blog here! Also your website loads up very fast! What host are you using? Can I get your affiliate link to your host? I wish my website loaded up as fast as yours lol
비아그라(성분명: 실데나필)는 음경해면체 내 혈류를 증가시켜 발기부전을 치료하는 대표적인 약물로, 약
1시간 전 공복 복용이 권장됩니다. 50mg/100mg 용량이 있으며, 흔한 부작용은 두통, 안면홍조, 소화불량입니다.
Hi there friends, its impressive paragraph about teachingand completely explained,
keep it up all the time.
I see something really special in this internet site.
Awsome post and straight to the point. I am not sure if this is in fact the best place to ask but do you people have any thoughts on where to employ some professional writers? Thanks 🙂
Your comment is awaiting moderation.
https://x.com/go88ynet
https://www.youtube.com/@go88ynet
https://www.pinterest.com/go88ynet/_profile/
https://www.twitch.tv/go88ynet/about
https://vimeo.com/go88ynet
https://github.com/go88ynet
https://www.reddit.com/user/go88ynet/
https://gravatar.com/go88ynet
https://www.tumblr.com/go88ynet
https://www.behance.net/go88ynet
https://huggingface.co/go88ynet
https://www.blogger.com/profile/04902325587974915726
https://issuu.com/go88ynet
https://500px.com/p/go88ynet
https://devpost.com/go88ynet
https://ro.gta5-mods.com/users/go88ynet
https://go88ynet.bandcamp.com/album/go88ynet
https://bio.site/go88ynet
https://ahgtf668.wixsite.com/go88ynet
https://www.stencyl.com/users/index/1317286
https://myanimelist.net/profile/go88ynet
https://www.instapaper.com/p/go88ynet
https://sites.google.com/view/go88ynet/
https://disqus.com/by/go88ynet/about/
https://www.goodreads.com/user/show/200382636-go88
https://pixabay.com/es/users/55474211/
https://www.linkedin.com/feed/update/urn:li:share:7450444148937236481/
https://form.jotform.com/261051565583054
https://beacons.ai/go88ynet
https://go88ynet.blogspot.com/2026/04/go88.html
https://www.chess.com/member/go88ynet
https://app.readthedocs.org/profiles/go88ynet/
https://sketchfab.com/go88ynet
https://qiita.com/go88ynet
https://telegra.ph/GO88-04-16-2
https://leetcode.com/u/go88ynet/
https://www.walkscore.com/people/316228514253/go88
https://heylink.me/go88ynet/
https://hub.docker.com/u/go88ynet
https://fliphtml5.com/home/go88ynet
https://gamblingtherapy.org/forum/users/go88ynet/
https://www.reverbnation.com/artist/go88ynet
https://go88ynet.gitbook.io/go88ynet-docs/
https://www.threadless.com/@go88ynet/activity
https://www.skool.com/@cong-game-go-4815
https://www.nicovideo.jp/user/143911303
https://talk.plesk.com/members/goynet.501287/#about
https://tabelog.com/rvwr/go88ynet/prof/
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:4DA480F469E0884B0A495F9A@AdobeID
http://gojourney.xsrv.jp/index.php?go88ynet
https://jali.me/go88ynet
https://plaza.rakuten.co.jp/go88ynet/diary/202604160000/
https://draft.blogger.com/profile/04902325587974915726
https://profiles.xero.com/people/go88ynet
https://profile.hatena.ne.jp/go88ynet/
https://go88ynet.webflow.io/
https://blog.sighpceducation.acm.org/wp/forums/users/go88ynet/
https://californiafilm.ning.com/profile/go88ynet
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1064879
https://vi.gravatar.com//go88ynet
https://lightroom.adobe.com/u/go88ynet?
https://colab.research.google.com/drive/17vbNyEmkVmM-Gg5ngb7eM02wtdP_O3k0?usp=sharing
https://sighpceducation.hosting.acm.org/wp/forums/users/go88ynet/
https://groups.google.com/g/go88ynet/c/9o8xyWvzvj4
https://bit.ly/m/go88ynet
https://go88ynet.mystrikingly.com/
https://www.postman.com/go88ynet
https://old.bitchute.com/channel/vP7NNBixq93t/
https://www.speedrun.com/users/go88ynet
https://www.callupcontact.com/b/businessprofile/go88ynet/10052679
https://www.magcloud.com/user/go88ynet
https://forums.autodesk.com/t5/user/viewprofilepage/user-id/18921802
https://us.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://wakelet.com/@go88ynet
https://www.myminifactory.com/users/go88ynet
https://gifyu.com/go88ynet
https://pxhere.com/en/photographer/4983818
https://justpaste.it/u/go88ynet
https://muckrack.com/go88-ynet/bio
https://www.intensedebate.com/profiles/go88ynet
https://www.designspiration.com/go88ynet/saves/
https://pbase.com/go88ynet
https://anyflip.com/homepage/ctwwe
https://allmylinks.com/go88ynet
https://forum.codeigniter.com/member.php?action=profile&uid=232936
https://teletype.in/@go88ynet
https://mez.ink/go88ynet
https://robertsspaceindustries.com/en/citizens/go88ynet
https://3dwarehouse.sketchup.com/by/go88ynet
https://gl.gta5-mods.com/users/go88ynet
https://www.storenvy.com/go88ynet
https://forum.pabbly.com/members/go88ynet.110802/#about
https://zerosuicidetraining.edc.org/user/profile.php?id=558465
https://reactormag.com/members/go88ynet/profile
https://hashnode.com/@go88ynet
https://song.link/go88ynet
https://b.hatena.ne.jp/go88ynet/20260416
https://album.link/go88ynet
https://www.producthunt.com/@go88ynet
https://wefunder.com/go88ynet/about
https://website.informer.com/go88y.net
https://www.pearltrees.com/go88ynet/item792064756
https://www.inventoridigiochi.it/membri/go88ynet/profile/
https://peatix.com/user/29383817/view
https://civitai.com/user/go88ynet
https://securityheaders.com/?q=https%3A%2F%2Fgo88y.net%2F&followRedirects=on
https://pad.stuve.de/s/s3800e4Ib
https://infiniteabundance.mn.co/members/39309938
https://gitconnected.com/go88ynet
https://flipboard.com/@go88ynet/
https://www.giveawayoftheday.com/forums/profile/1794606
https://lit.link/en/go88ynet
https://tawk.to/go88ynet1
https://potofu.me/go88ynet
https://jali.pro/go88ynet
https://hub.vroid.com/en/users/125465798
https://community.cloudera.com/t5/user/viewprofilepage/user-id/150365
https://magic.ly/go88ynet/GO88
https://jaga.link/go88ynet
https://ngel.ink/go88ynet
https://tr.gravatar.com/go88ynet
https://bookmeter.com/users/1709036
https://creator.nightcafe.studio/u/go88ynet
https://motion-gallery.net/users/953912
https://postheaven.net/go88ynet/go88
https://noti.st/go88ynet
https://www.aicrowd.com/participants/go88ynet
https://www.theyeshivaworld.com/coffeeroom/users/go88ynet
https://qoolink.co/go88ynet
https://findaspring.org/members/go88ynet/
https://backabuddy.co.za/campaign/go88ynet
https://www.apsense.com/user/go88ynet
https://forum.epicbrowser.com/profile.php?id=150725
https://biolinky.co/go-88-ynet
https://www.pozible.com/profile/go88ynet
https://www.openrec.tv/user/zgck5g8vds7z8szamhgd/about
https://hackaday.io/go88ynet
https://oye.participer.lyon.fr/profiles/go88ynet/activity
https://kumu.io/go88ynet/go88ynet#go88
https://blog.ulifestyle.com.hk/go88ynet
https://ie.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://go88ynet.stck.me/profile
https://forum.allkpop.com/suite/user/314662-go88ynet/#about
https://app.talkshoe.com/user/go88ynet
https://forums.alliedmods.net/member.php?u=475259
https://allmyfaves.com/go88ynet
https://linkmix.co/53455731
https://www.beamng.com/members/go88ynet.787594/
https://community.m5stack.com/user/go88ynet
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3938196
https://www.blockdit.com/go88ynet
https://www.gta5-mods.com/users/go88ynet
https://notionpress.com/author/1505292
https://confengine.com/user/go88ynet
https://www.adpost.com/u/go88ynet/
https://ko.gta5-mods.com/users/go88ynet
https://pinshape.com/users/8949296-ahgtf668?tab=designs
https://www.chordie.com/forum/profile.php?id=2507762
https://portfolium.com/go88ynet
https://advego.com/profile/go88ynet/
https://www.weddingbee.com/members/go88ynet/
https://wallhaven.cc/user/go88ynet
https://unityroom.com/users/t14ke6su9ly5pbfz2n0h
https://www.skypixel.com/users/djiuser-pls6et6a8ysj
https://medibang.com/author/28152119/
https://iplogger.org/vn/logger/F7tR5KXBY9fe/
https://spinninrecords.com/profile/go88ynet
https://en.islcollective.com/portfolio/12899531
https://www.myebook.com/user_profile.php?id=go88ynet
https://musikersuche.musicstore.de/profil/go88ynet/
https://routinehub.co/user/go88ynet
https://www.mindomo.com/mindmap/c9b9d117cfe14ee4bd41b36ef3e8d42b
https://zenwriting.net/go88ynet/go88
https://www.myget.org/users/go88ynet
https://brain-market.com/u/go88ynet
https://www.givey.com/go88ynet
https://myspace.com/go88ynet
https://hoo.be/go88ynet
https://topsitenet.com/profile/go88ynet/1625392/
https://www.haikudeck.com/presentations/go88ynet
https://www.growkudos.com/profile/go88_go88_13
https://promosimple.com/ps/4815a/go88
https://able2know.org/user/go88ynet/
https://www.sythe.org/members/go88ynet.2037720/
https://hanson.net/users/go88ynet
https://jobs.landscapeindustrycareers.org/profiles/8157242-go88
https://dreevoo.com/profile_info.php?pid=1497527
https://blender.community/go88ynet/
https://www.claimajob.com/profiles/8157241-go88
https://golosknig.com/profile/go88ynet/
https://www.invelos.com/UserProfile.aspx?alias=go88ynet
https://jobs.windomnews.com/profiles/8157292-go88
https://ru.gravatar.com/go88ynet
https://aprenderfotografia.online/usuarios/go88ynet/profile/
https://www.passes.com/go88ynet
https://secondstreet.ru/profile/go88ynet/
https://manylink.co/@go88ynet
https://safechat.com/u/go88ynet
https://f319.com/members/go88ynet.1095237/
https://app.hellothematic.com/creator/profile/1142486
https://commu.nosv.org/p/go88ynet/
https://phijkchu.com/a/go88ynet/video-channels
https://m.wibki.com/go88ynet
https://forum.issabel.org/u/go88ynet
https://tooter.in/go88ynet
https://www.investagrams.com/Profile/go88ynet
https://spiderum.com/nguoi-dung/go88ynet
https://tudomuaban.com/chi-tiet-rao-vat/2878649/go88ynet.html
https://espritgames.com/members/50760847/
https://schoolido.lu/user/go88ynet/
https://kaeuchi.jp/forums/users/go88ynet/
https://hcgdietinfo.com/hcgdietforums/members/go88ynet/
https://www.notebook.ai/documents/2488357
https://bandori.party/user/770348/go88ynet/
https://illust.daysneo.com/illustrator/go88ynet/
https://doselect.com/@a3b6c862d8491bc40cfcb8611
https://www.udrpsearch.com/user/go88ynet
http://forum.modulebazaar.com/forums/user/go88ynet/
https://www.halaltrip.com/user/profile/338888/go88ynet/
https://www.linqto.me/about/go88ynet
https://uiverse.io/profile/go88ynet_1015
https://www.abclinuxu.cz/lide/go88ynet
https://www.chichi-pui.com/users/go88ynet/
https://maxforlive.com/profile/user/go88ynet?tab=about
https://hedgedoc.envs.net/s/EZVjr-V0B
https://pad.darmstadt.social/s/YwhF4eTo4x
https://doc.adminforge.de/s/xsygNI7zfB
https://cointr.ee/go88ynet
https://referrallist.com/profile/go88ynet/
http://linoit.com/users/go88ynet/canvases/go88ynet
https://www.checkli.com/go88ynet
https://beteiligung.amt-huettener-berge.de/profile/go88ynet/
https://id.gta5-mods.com/users/go88ynet
https://www.trackyserver.com/profile/244558
https://www.postype.com/@go88ynet/community/custom/3198889
https://www.nintendo-master.com/profil/go88ynet
https://jobs.suncommunitynews.com/profiles/8157469-go88
https://expathealthseoul.com/profile/go88ynet/
https://demo.wowonder.com/go88ynet
https://iglinks.io/ahgtf668-1qd
https://www.xosothantai.com/members/go88ynet.608472/
https://www.diggerslist.com/go88ynet/about
https://www.otofun.net/members/go88ynet.906036/#about
https://www.mapleprimes.com/users/go88ynet
https://pumpyoursound.com/u/user/1605840
https://www.montessorijobsuk.co.uk/author/go88ynet/
http://www.biblesupport.com/user/829991-go88ynet/
https://www.anibookmark.com/user/go88ynet.html
https://longbets.org/user/go88ynet/
https://apptuts.bio/go88ynet
https://igli.me/go88ynet
https://jobs.westerncity.com/profiles/8157470-go88
https://www.huntingnet.com/forum/members/go88ynet.html
https://www.lingvolive.com/en-us/profile/2be03cc0-c6d3-4d56-a6a3-ed4ee1427ff6/translations
https://www.annuncigratuititalia.it/author/go88ynet/
https://onlinevetjobs.com/author/go88ynet/
https://wibki.com/go88ynet
https://kktix.com/user/8657181
https://velog.io/@go88ynet/about
https://linkin.bio/go88ynet
https://forum.ircam.fr/profile/go88ynet/
https://audiomack.com/go88ynet
https://enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://hedgedoc.eclair.ec-lyon.fr/s/M4cPIlETU
https://www.jigsawplanet.com/go88ynet
https://twilog.togetter.com/go88ynet
https://cdn.muvizu.com/Profile/go88ynet/Latest
https://www.ganjingworld.com/vi-VN/channel/1ifif0u264s7s3Zvucxdpj9AU12a0c?subTab=all&tab=about&subtabshowing=latest&q=
https://www.royalroad.com/profile/953881
https://www.fitday.com/fitness/forums/members/go88ynet.html
https://oc.gravatar.com/go88ynet
https://vn.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://artistecard.com/go88ynet
https://exchange.prx.org/series/62099-go88
https://www.launchgood.com/user/newprofile#!/user-profile/profile/cong.game.go885
https://rapidapi.com/user/go88ynet
https://www.efunda.com/members/people/show_people.cfm?Usr=go88ynet
https://eo-college.org/members/go88ynet/
https://www.freelistingusa.com/listings/go88ynet
https://b.io/go88ynet
https://phatwalletforums.com/user/go88ynet
http://fort-raevskiy.ru/community/profile/go88ynet/
https://activepages.com.au/profile/go88ynet
https://www.blackhatprotools.info/member.php?286465-go88ynet
https://writexo.com/share/9a66b5640e93
https://freeicons.io/profile/919144
https://www.corc.co.uk/forums/users/go88ynet/
https://devfolio.co/@go88ynet/readme-md
https://mylinks.ai/go88ynet
https://www.thethingsnetwork.org/u/go88ynet
https://tealfeed.com/go88ynet
https://inkbunny.net/go88ynet
https://poipiku.com/13474427/
https://skitterphoto.com/photographers/2642990/go88ynet
https://digiex.net/members/go88ynet.144246/
https://3dtoday.ru/blogs/go88ynet
https://searchengines.guru/ru/users/2232936
https://md.yeswiki.net/s/4pQMp1lz-m
https://www.joomla51.com/forum/profile/103830-go88ynet
https://data.danetsoft.com/go88y.net
https://freelance.ru/go88ynet
https://go88ynet.amebaownd.com/
https://www.symbaloo.com/mix/go88-udch
https://forum.html.it/forum/member.php?userid=485598
https://triberr.com/go88ynet
https://community.jmp.com/t5/user/viewprofilepage/user-id/96635
https://www.fuelly.com/driver/go88ynet
https://www.ozbargain.com.au/user/609591
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=300203
https://www.muvizu.com/Profile/go88ynet/Latest
https://www.rcuniverse.com/forum/members/go88ynet.html
https://novel.daysneo.com/author/go88ynet/
https://lifeinsys.com/user/go88ynet
https://iszene.com/user-346802.html
https://el.gta5-mods.com/users/go88ynet
https://www.heavyironjobs.com/profiles/8157744-go88
https://transfur.com/Users/go88ynet
https://matkafasi.com/user/go88ynet
https://undrtone.com/go88ynet
https://www.wvhired.com/profiles/8157750-go88
https://savelist.co/profile/users/go88ynet
https://theafricavoice.com/profile/go88ynet
https://fortunetelleroracle.com/profile/go88ynet
https://www.shippingexplorer.net/en/user/go88ynet/277377
https://fabble.cc/go88ynet
https://formulamasa.com/elearning/members/go88ynet/?v=96b62e1dce57
https://luvly.co/users/go88ynet
https://gravesales.com/author/go88ynet/
https://acomics.ru/-go88ynet
https://rant.li/go88ynet/go88
https://help.orrs.de/user/go88ynet
https://truckymods.io/user/484679
https://marshallyin.com/members/go88ynet/
https://www.tizmos.com/go88ynet?folder=Home
https://www.aseeralkotb.com/en/profiles/go88ynet-111224606367925932230-1776350562
https://www.zubersoft.com/mobilesheets/forum/user-133740.html
https://amaz0ns.com/forums/users/go88ynet/
https://demo.userproplugin.com/profile/go88ynet/
https://11secondclub.com/users/profile/1711273
https://protocol.ooo/ja/users/go88ynet
https://etextpad.com/rcqg84wzpj
https://violet.vn/user/show/id/15265644
https://biomolecula.ru/authors/140611
https://forum.dmec.vn/index.php?members/go88ynet.186570/
https://my.bio/go88ynet
https://bizidex.com/en/go88-apartments-915567
https://www.edna.cz/uzivatele/go88ynet/
https://www.france-ioi.org/user/perso.php?sLogin=go88ynet
https://mail.tudomuaban.com/chi-tiet-rao-vat/2878649/go88ynet.html
https://www.notariosyregistradores.com/web/forums/usuario/go88ynet/
https://about.me/go88ynet
https://video.fc2.com/account/43744011
https://www.keepandshare.com/discuss2/45929/go88ynet
https://talkmarkets.com/profile/ahgtf668-260416-151324
https://bestadsontv.com/profile/525848/Cng-game-GO88
https://nl.gravatar.com/go88ynet
https://hackmd.okfn.de/s/SJGhndC3-l
https://urlscan.io/result/019d96dc-93d9-75a6-91ce-91fc1aaf1ccf/
https://www.developpez.net/forums/u1862328/go88ynet/
https://joy.link/go88ynet
https://www.warriorforum.com/members/go88ynet.html
https://apk.tw/home.php?mod=space&uid=7335149&do=profile
https://forums.hostsearch.com/member.php?289011-go88ynet
https://www.pageorama.com/?p=go88ynet
https://fileforums.com/member.php?u=298374
https://divinguniverse.com/user/go88ynet
https://www.grioo.com/forum/profile.php?mode=viewprofile&u=5677571
https://www.outlived.co.uk/author/go88ynet/
https://pixelfed.uno/go88ynet
https://filesharingtalk.com/members/635802-go88ynet
http://www.kaseisyoji.com/home.php?mod=space&uid=3948536
https://www.managementpedia.com/members/go88ynet.1120117/#about
https://www.motom.me/user/298890/profile?shared=true
https://youtopiaproject.com/author/go88ynet/
https://nogu.org.uk/forum/profile/go88ynet/
https://subaru-vlad.ru/forums/users/go88ynet
https://forums.stardock.com/user/7659465
https://forum.delftship.net/Public/users/go88ynet/
https://copynotes.be/shift4me/forum/user-51648.html
https://projectnoah.org/users/go88ynet
https://www.powerelectronicsnews.com/forum/users/conggamego88694/
https://pimrec.pnu.edu.ua/members/go88ynet/profile/
https://forum.herozerogame.com/index.php?/user/160943-go88ynet/
https://viblo.asia/u/go88ynet/contact
https://metaldevastationradio.com/go88ynet
https://www.canadavisa.com/canada-immigration-discussion-board/members/go88ynet.1352782/#about
https://trakteer.id/go88ynet
https://www.bahamaslocal.com/userprofile/1/288638/go88ynet.html
https://www.proko.com/@go88ynet/activity
https://www.telix.pl/profile/go88ynet/
https://l2top.co/forum/members/go88ynet.171780/
https://www.getlisteduae.com/listings/go88ynet
https://www.moshpyt.com/user/go88ynet
https://whatpulse.org/u/go88ynet
https://www.prosebox.net/book/107175/
https://odesli.co/go88ynet
https://no.gta5-mods.com/users/go88ynet
https://genina.com/user/profile/5309352.page
https://freestyler.ws/user/649120/go88ynet
https://www.atozed.com/forums/user-76669.html
https://www.sunlitcentrekenya.co.ke/author/go88ynet/
https://joinentre.com/profile/go88ynet
https://onlinesequencer.net/members/266835
https://www.minecraft-servers-list.org/details/go88ynet/
https://www.iniuria.us/forum/member.php?673419-go88ynet
https://forum.skullgirlsmobile.com/members/go88ynet.213947/#about
https://pads.zapf.in/s/qRN_qGgJxK
https://www.directorylib.com/domain/go88y.net
https://www.maanation.com/go88ynet
https://www.hostboard.com/forums/members/go88ynet.html
https://mail.protospielsouth.com/user/128866
https://www.sciencebee.com.bd/qna/user/go88ynet
https://shootinfo.com/author/go88ynet/?pt=ads
https://www.facekindle.com/go88ynet
https://www.aipictors.com/users/4a1f4694-873f-b08c-612b-3b07ed16ce74
https://partecipa.poliste.com/profiles/go88ynet/activity
https://rekonise.com/u/go88ynet
https://sciencemission.com/profile/go88ynet
https://zeroone.art/profile/go88ynet
http://delphi.larsbo.org/user/go88ynet
https://connect.gt/user/go88ynet
https://ja.cofacts.tw/user/go88ynet
https://www.plotterusati.it/user/go88ynet
https://homepage.ninja/go88ynet
https://jii.li/go88ynet
https://awan.pro/forum/user/164343/
https://egl.circlly.com/users/go88ynet
https://aoezone.net/members/go88ynet.184978/#about
https://forum.honorboundgame.com/user-509106.html
https://www.mymeetbook.com/go88ynet
https://sketchersunited.org/users/317335
https://cgmood.com/go88ynet
https://th.gravatar.com/go88ynet
https://pods.link/go88ynet
https://www.itchyforum.com/en/member.php?387623-go88ynet
https://www.czporadna.cz/user/go88ynet
https://idol.st/user/161366/go88ynet/
https://anunt-imob.ro/user/profile/854240
https://cofacts.tw/user/go88ynet
http://www.muzikspace.com/profiledetails.aspx?profileid=135125
https://forums.ashesofthesingularity.com/user/7659465
https://forums.sinsofasolarempire2.com/user/7659465
https://destaquebrasil.com/saopaulo/author/go88ynet/
https://forums.galciv3.com/user/7659465
https://pictureinbottle.com/r/go88ynet
https://www.abitur-und-studium.de/Forum/News/GO88-uoc-biet-en-la-cong-game-giai-tri-truc-tuyen
https://www.weddingvendors.com/directory/profile/39105/
https://mathlog.info/users/uFfokC34fZVOlyG3lCfYmAln4Z62
https://careers.coloradopublichealth.org/profiles/8159289-go88
https://sciter.com/forums/users/go88ynet/
https://pad.lescommuns.org/s/OtwK_sr5m
https://hukukevi.net/user/go88ynet
https://muare.vn/shop/go88ynet/902004
https://usdinstitute.com/forums/users/go88ynet/
https://www.japaaan.com/user/76371/
https://belgaumonline.com/profile/go88ynet/
https://lookingforclan.com/user/go88ynet
https://forums.maxperformanceinc.com/forums/member.php?u=245984
https://www.instructorsnearme.com/author/go88ynet/
https://fora.babinet.cz/profile.php?id=122982
https://wikifab.org/wiki/Utilisateur:Go88ynet
https://vcook.jp/users/86545
https://gta5-mods.com/users/go88ynet
https://www.themeqx.com/forums/users/go88ynet/
https://forums.starcontrol.com/user/7659465
https://sklad-slabov.ru/forum/user/42345/
https://www.thetriumphforum.com/members/go88ynet.62270/
https://hi-fi-forum.net/profile/1143519
https://md.opensourceecology.de/s/Sw2MDx8jU
https://md.coredump.ch/s/dBDZJ35yh
https://aphorismsgalore.com/users/go88ynet
https://shareyoursocial.com/go88ynet
https://expatguidekorea.com/profile/go88ynet/
https://pad.degrowth.net/s/3f3ytvJZZ
https://app.brancher.ai/user/NbPlP4_L9yS_
https://pad.codefor.fr/s/6cprxxXNzR
https://md.chaospott.de/s/KH_uiWUAi_
https://go883.multipass.com//mp/eventDetail/4012
https://www.democracylab.org/user/39469
https://sangtac.waka.vn/author/go-Z8WobpEv8L
https://vs.cga.gg/user/241400
https://portfolium.com.au/go88ynet
https://youengage.me/p/69e22cdeb77187010002ce7f
https://www.buckeyescoop.com/users/c60cccb0-8e71-441c-9159-87eec9b825a6
https://classificados.acheiusa.com/profile/OCtvQVY0VlFoNnl4SlFKc3g2VUtVZGRYbUlxSlVDQ0JadEh0ZGRRMlZEUT0=
https://forums.stardock.net/user/7659465
https://www.gabitos.com/eldespertarsai/template.php?nm=1776390194
https://tutorialslink.com/member/go88ynetundefined/97600
http://raredirectory.com/author/go88ynet/
https://www.jk-green.com/forum/topic/107959/go88ynet
http://forum.cncprovn.com/members/423736-go88ynet
https://forum.korabli.su/profile/303321865-go88ynet/?tab=field_core_pfield_12
https://aiforkids.in/qa/user/go88ynet+1
https://whitehat.vn/members/go88ynet.225283/#about
https://www.thepetservicesweb.com/board/board_topic/2701171/8161216.htm
https://quangcaoso.vn/go88ynet/gioithieu.html
https://mt2.org/uyeler/go88ynet.38776/#about
https://www.mateball.com/go88ynet
https://desksnear.me/users/go88ynet
https://lt.gravatar.com/go88ynet
https://nootropicdesign.com/store/forums/users/go88ynet/
https://forum.riverrise.ru/user/56021-go88ynet/
https://timdaily.vn/members/go88ynet.133701/#about
https://hedgedoc.dezentrale.space/s/kRCxiwDWK
https://playlist.link/go88ynet
https://www.siasat.pk/members/go88ynet.270882/#about
https://skrolli.fi/keskustelu/users/ahgtf668/
https://axe.rs/forum/members/go88ynet.13425272/#about
https://www.milliescentedrocks.com/board/board_topic/2189097/8161235.htm
https://www.fw-follow.com/forum/topic/114149/go88ynet
https://forum.aigato.vn/user/go88ynet
https://mygamedb.com/profile/go88ynet
https://stuv.othr.de/pad/s/Ua7-DHB-H
https://smallseo.tools/website-checker/go88y.net
https://www.fruitpickingjobs.com.au/forums/users/go88ynet/
https://sdelai.ru/members/go88ynet/
https://www.elektroenergetika.si/UserProfile/tabid/43/userId/1457815/Default.aspx
https://affariat.com/user/profile/178792
https://www.pathumratjotun.com/forum/topic/174625/go88ynet
https://shhhnewcastleswingers.club/forums/users/go88ynet/
https://www.navacool.com/forum/topic/386977/go88ynet
https://diendan.bftvietnam.com/members/21502-go88ynet.html
https://www.fitlynk.com/go88ynet
https://www.thepartyservicesweb.com/board/board_topic/3929364/8161236.htm
https://www.tai-ji.net/board/board_topic/4160148/8161237.htm
https://www.ttlxshipping.com/forum/topic/386978/go88ynet
https://www.bestloveweddingstudio.com/forum/topic/80662/go88ynet
https://duyendangaodai.net/members/31516-go88ynet.html
https://www.bonback.com/forum/topic/386979/go88ynet
https://www.nongkhaempolice.com/forum/topic/119209/go88ynet
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/8161238.htm
https://www.driedsquidathome.com/forum/topic/140119/go88ynet
https://turcia-tours.ru/forum/profile/go88ynet/
https://forums.planetdestiny.com/members/go88ynet.127493/#about
https://www.roton.com/forums/users/ahgtf668/
https://www.cryptoispy.com/forums/users/go88ynet/
https://raovatonline.org/author/go88ynet/
https://es.gta5-mods.com/users/go88ynet
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/8161293.htm
https://consultas.saludisima.com/yo/go88ynet
https://pets4friends.com/profile-1575991
http://catalog.drobak.com.ua/communication/forum/user/2851212/
https://play-uno.com/profile.php?user=422820
https://forums.galciv4.com/user/7659465
https://www.ekdarun.com/forum/topic/152118/go88ynet
https://www.nedrago.com/forums/users/go88ynet/
https://www.tkc-games.com/forums/users/ahgtf668/
https://live.tribexr.com/profiles/view/go88ynet
https://producerbox.com/users/go88ynet
https://ensp.edu.mx/members/go88ynet/
https://fengshuidirectory.com/dashboard/listings/go88ynet/
https://www.vhs80.com/board/board_topic/6798823/8161309.htm
https://approachanxiety.com/forums/users/go88ynet/
https://www.spigotmc.org/members/go88ynet.2519849/
https://www.hoaxbuster.com/redacteur/go88ynet
https://akniga.org/profile/1413472-go88ynet/
https://fanclove.jp/profile/bj273Gkn2d
https://www.video-bookmark.com/bookmark/7105512/go88ynet/
https://md.chaosdorf.de/s/w2s19mKyHr
https://www.socialbookmarkssite.com/bookmark/6236042/go88ynet/
https://telescope.ac/go88ynet/3jjfobuxhy2tviezacw8ub
https://krachelart.com/UserProfile/tabid/43/userId/1342133/Default.aspx
https://runtrip.jp/users/769589
https://www.freewebspace.net/forums/index.php?members/go88ynet.17034130/#about
https://findnerd.com/profile/publicprofile/go88ynet/157691
https://protospielsouth.com/user/128866
https://zimexapp.co.zw/go88ynet
https://quicknote.io/9c72a8c0-3a0a-11f1-9edd-a7a29c7a2fc6/
https://www.d-ushop.com/forum/topic/125801/go88ynet
https://dumagueteinfo.com/author/go88ynet/
https://www.tunwalai.com/Profile/16303690
https://electroswingthing.com/profile/go88ynet/
https://youslade.com/go88ynet
https://pad.libreon.fr/s/JNu_oh9aY
https://mercadodinamico.com.br/author/go88ynet/
https://forums.desmume.org/profile.php?id=421052
https://www.sunemall.com/board/board_topic/8431232/8161435.htm
https://forum.jatekok.hu/User-go88ynet
https://www.workingholidayjobs.com.au/forums/users/go88ynet/
https://thuthuataccess.com/forum/user-29750.html
https://www.ironlifting.it/forum/member.php?u=428865
https://zepodcast.com/forums/users/go88ynet/
https://rmmedia.ru/members/183204/#about
https://www.themirch.com/blog/author/go88ynet/
https://hasitleaked.com/forum/members/go88ynet/profile/
https://www.pebforum.com/members/go88ynet.239037/#about
https://uno-en-ligne.com/profile.php?user=422820
https://forum-foxess.pro/community/profile/go88ynet/
https://www.donbla.co.jp/user/go88ynet
https://ferrariformula1.hu/community/profile/go88ynet/
https://swat-portal.com/forum/wcf/user/48066-go88ynet/#about
https://scenarch.com/userpages/32740
https://www.max2play.com/en/forums/users/go88ynet/
https://www.anime-sharing.com/members/go88ynet.512297/#about
https://www.natthadon-sanengineering.com/forum/topic/100749/go88ynet
https://forum.maycatcnc.net/members/go88ynet.4544/#about
https://es.files.fm/go88ynet/info
https://pixbender.com/go88ynet
https://maiotaku.com/p/go88ynet/info
https://sk.gravatar.com/go88ynet
https://allmy.bio/go88ynet
https://www.saltlakeladyrebels.com/profile/go88ynet/profile
https://do.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://www.foriio.com/go88ynet
https://mysound.ge/profile/go88ynet
https://tlcworld.it/forum/members/go88ynet.36400/#about
https://www.forum.or.id/members/go88ynet.301006/#about
https://indiestorygeek.com/user/go88ynet
https://xtremepape.rs/members/go88ynet.664382/#about
https://odysee.com/@go88ynet:d
https://www.wincustomize.com/users/7659465/go88ynet
https://cloudburstmc.org/members/go88ynet.76570/#about
https://www.foundryvtt-hub.com/members/go88ynet/
https://www.ariiyatickets.com/members/go88ynet/
https://rebrickable.com/users/go88ynet/mocs/photos/
https://forums.servethehome.com/index.php?members/go88ynet.237958/#about
https://www.valinor.com.br/forum/usuario/go88ynet.144846/#about
https://vnbit.org/members/go88ynet.93410/#about
https://nonon-centsnanna.com/members/go88ynet/
https://malt-orden.info/userinfo.php?uid=457461
https://kitsu.app/users/1703350
https://participer.loire-atlantique.fr/profiles/go88ynet/activity
https://www.renderosity.com/users/id:1849489
https://files.fm/go88ynet/info
https://scrapbox.io/go88ynet/GO88
https://freeimage.host/go88ynet
https://www.equinenow.com/farm/profile69e1dab7b8269.htm
https://nhattao.com/members/user6952985.6952985/
https://mforum3.cari.com.my/home.php?mod=space&uid=3397012&do=profile
http://www.activewin.com/user.asp?Action=Read&UserIndex=4836932&redir=&redirname=Forums
https://rush1989.rash.jp/pukiwiki/index.php?go88ynet
https://www.grepmed.com/go88ynet
https://edabit.com/user/RJPKPuvEMHdM8weh5
https://beteiligung.stadtlindau.de/profile/go88ynet/
https://game8.jp/users/484360
https://justpaste.me/DdJj2
https://www.easyhits4u.com/profile.cgi?login=go88ynet&view_as=1
https://divisionmidway.org/jobs/author/go88ynet/
https://backloggery.com/go88ynet
https://in.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://gt.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://vi.gta5-mods.com/users/go88ynet
https://pt.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://beteiligung.tengen.de/profile/go88ynet/
https://artist.link/go88ynet
https://pad.flipdot.org/s/2IXklOEhpq
https://www.earthmom.org/a-citizen-of-earth/cong-game-go88
https://www.dokkan-battle.fr/forums/users/go88ynet/
https://naijamatta.com/go88ynet
https://www.kuettu.com/go88ynet
https://gamelet.online/user/go88ynet
https://dev.muvizu.com/Profile/go88ynet/Latest
https://mylink.page/go88ynet
https://indian-tv.cz/u/go88ynet
https://act4sdgs.org/profile/go88_14
user.linkdata.org/user/go88ynet/work
https://www.free-socialbookmarking.com/user/F5guSUVNnIM4
http://library.sokal.lviv.ua/forum/profile.php?mode=viewprofile&u=18287
https://qna.habr.com/user/go88ynet
https://xaydunghanoimoi.net/members/27628-go88ynet.html
https://swag.live/en/user/69e1dfcab07f46e88eb1efa3
https://www.xibeiwujin.com/home.php?mod=space&uid=2313489&do=profile&from=space
https://easymeals.qodeinteractive.com/forums/users/go88ynet/
https://www.slmath.org/people/104926
https://es.stylevore.com/user/go88ynet
https://www.stylevore.com/user/go88ynet
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=90748
http://www.brenkoweb.com/user/87460/profile
https://md.kif.bangladhadha.com/load.php?note=365a817a
https://ameblo.jp/go88ynet/entry-12963250719.html
https://www.ameba.jp/profile/general/go88ynet/
https://www.goldposter.com/members/go88ynet/profile/
https://www.wikidot.com/user:info/go88ynet
https://www.adslgr.com/forum/members/223603-go88ynet
https://stocktwits.com/go88ynet
https://coderwall.com/go88ynet
https://forum.opnsense.org/index.php?action=profile;u=67335
https://diit.cz/profil/h64phjepke
https://www.bookingblog.com/forum/users/go88ynet/
https://forum.aceinna.com/user/go88ynet
https://forums.wolflair.com/members/go88ynet.157381/#about
https://gl.gravatar.com/go88ynet
https://chyoa.com/user/go88ynet
https://biiut.com/go88ynet
https://joy.gallery/go88ynet1
https://forum.plutonium.pw/user/go88ynet
https://www.my-hiend.com/vbb/member.php?51954-go88ynet
https://chanylib.ru/ru/forum/user/24616/
https://kenzerco.com/forums/users/go88ynet/
https://www.pickupforum.ru/index.php?showuser=6611690
https://community.goldposter.com/members/go88ynet/profile/
https://failiem.lv/go88ynet/info
https://go88ynet.pixieset.com/
https://eternagame.org/players/618401
https://vc.ru/id5891975
https://www.mixcloud.com/go88ynet/
http://forum.orangepi.org/home.php?mod=space&uid=6376853
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=156554_jk0lr0gc
https://www.podchaser.com/users/go88ynet
https://de.enrollbusiness.com/BusinessProfile/7775587/go88ynet
https://dawlish.com/user/details/672e8411-18f6-418b-b9bb-f1cc3a1e3f74
https://joy.bio/go88ynet2
https://www.ibizaclubpt.com/members/go88ynet.122168/#about
https://www.dibiz.com/ahgtf668
https://onedio.ru/profile/go88ynet
https://mycomplianceresource.com/forums/users/go88ynet/
https://www.green-collar.com/forums/users/go88ynet/
https://www.hogwartsishere.com/1833664/
http://www.teuko.com/user/go88ynet
http://jogikerdesek.hu/user/go88ynet
https://forums.auran.com/members/go88ynet.1282821/#about
https://diigo.com/012djup
https://suzuri.jp/go88ynet
https://paste.toolforge.org/view/8ce089e2
https://forum.m5stack.com/user/go88ynet
https://muabanhaiduong.com/members/go88ynet.86533/#about
https://pad.geolab.space/s/K47xMlVFG
https://www.longisland.com/profile/go88ynet
https://www.elephantjournal.com/profile/go88ynet/
https://hackmd.hub.yt/s/-OGn747uR
https://forums.offworldgame.com/user/7659465
https://boss.why3s.cc/boss/home.php?mod=space&uid=261717
https://ctxt.io/2/AAD4e8_-Ew
https://ru.gta5-mods.com/users/go88ynet
https://lamsn.com/home.php?mod=space&uid=1961183
https://hack.allmende.io/s/0vmNMTjeA
https://notes.bmcs.one/s/pJCErsJUja
https://www.coffeesix-store.com/board/board_topic/7560063/8163655.htm
https://zzb.bz/go88ynet
http://www.jindousa.cn/bbs/home.php?mod=space&uid=339769
https://www.plurk.com/go88ynet
https://racetime.gg/user/z56VnBQ006WK4xrZ/go88ynet
https://techplanet.today/member/go88ynet
https://forums.elementalgame.com/user/7659465
https://scanverify.com/siteverify.php?site=go88y.net
https://test.elit.edu.my/author/go88ynet1/
https://www.xen-factory.com/index.php?members/go88ynet.153664/#about
https://learndash.aula.edu.pe/miembros/go88ynet1/
https://newdayrp.com/members/go88ynet.70387/#about
https://www.housedumonde.com/profile/go88ynet/profile
https://input.scs.community/s/6trb7TzDfS
https://videos.muvizu.com/Profile/go88ynet/Latest
https://cloud.anylogic.com/profile/user/3e8f0f0f-252a-4a46-a063-3f029ead71db
https://xoops.ec-cube.net/userinfo.php?uid=347970
http://frankstout.com/UserProfile/tabid/42/userId/94002/Default.aspx
https://www.funsocio.com/go88ynet
https://forum.konyacraft.com/members/go88ynet.23192/#about
https://aboutcasemanagerjobs.com/author/go88ynet/
https://chillspot1.com/user/go88ynet
http://mjjcn.com/mjjcnforum/space-uid-976339.html
https://www.longislandjobsmagazine.com/board/board_topic/9092000/8163874.htm
https://www.dideadesign.com/forum/topic/38937/go88ynet
https://www.hyperlabthailand.com/forum/topic/804012/go88ynet
https://uconnect.ae/go88ynet
https://forum.hiv.plus/user/go88ynet
https://forum.cnnr.fr/user/go88ynet
https://www.rueanmaihom.net/forum/topic/96207/go88ynet
https://www.myaspenridge.com/board/board_topic/3180173/8163876.htm
https://data.loda.gov.ua/user/go88ynet
https://hedgedoc.stusta.de/s/dOaor2pw7
https://boldomatic.com/view/writer/go88ynet
https://challonge.com/vi/go88ynet
https://gitlab.vuhdo.io/go88ynet
https://rareconnect.org/en/user/go88ynet
https://dentaltechnician.org.uk/community/profile/go88ynet/
https://vietcurrency.vn/members/go88ynet.239131/#about
https://www.penmai.com/community/members/go88ynet.512694/#about
https://www.laundrynation.com/community/profile/go88ynet1/
https://aniworld.to/user/profil/go88ynet
https://pad.koeln.ccc.de/s/T4Ihw8vBG
https://community.cisco.com/t5/user/viewprofilepage/user-id/2067035
http://forum.vodobox.com/profile.php?id=68434
https://domain.opendns.com/go88y.net
https://raovat.vn/members/go88ynet.142989/#about
https://congdongmassage.com/members/go88ynet.146666/#about
https://www.bandlab.com/go88ynet
http://newdigital-world.com/members/go88ynet.html
https://clan-warframe.fr/forums/users/go88ynet/
https://graphcommons.com/graphs/9bbdf5e4-bcaf-49fc-8bea-c87c141843cd
https://www.gamingtop100.net/server/54816/go88-cng-game-bi-i-thng-ng-tri-nghim-2
https://www.printables.com/@go88ynet_4717677
https://de.gravatar.com/go88ynet
https://chiase123.com/member/go88ynet/
https://imageevent.com/go88ynet/go88?q=1100
https://www.fanart-central.net/user/go88ynet/profile
https://www.adsfare.com/go88ynet
https://www.coh2.org/user/172934/go88ynet
https://forum.enscape3d.com/wcf/index.php?user/137749-go88ynet/#about
https://www.jointcorners.com/go88ynet
https://myanimeshelf.com/profile/go88ynet
https://startupxplore.com/en/person/go88ynet
http://onlineboxing.net/jforum/user/profile/443143.page
https://lustyweb.live/members/go88ynet.118542/#about
http://www.askmap.net/location/7790179/vietnam/go88ynet
https://raovat.nhadat.vn/members/go88ynet-304787.html
https://coub.com/go88ynet
https://macuisineturque.fr/author/go88ynet/
https://www.empregosaude.pt/en/author/go88ynet/
https://www.rwaq.org/users/go88ynet
https://participacion.cabildofuer.es/profiles/go88ynet/activity?locale=en
https://gitea.com/go88ynet
https://kyourc.com/go88ynet
https://www.salejusthere.com/profile/0374541897
https://homologa.cge.mg.gov.br/user/go88ynet
https://writeupcafe.com/author/go88ynet
https://jobhop.co.uk/profile/478123?preview=true
https://www.freewebmarks.com/user/omi1pKxFHIOb
https://www.fundable.com/cong-game-go88-88
https://www.facer.io/u/go88ynet
https://www.bitchute.com/channel/vP7NNBixq93t
https://uk.gta5-mods.com/users/go88ynet
https://leasedadspace.com/members/go88ynet/
https://sixsens.eu/de/forum/profile/go88ynet/
https://fontstruct.com/fontstructions/show/2866363/go88-83
https://hackmd.io/@go88ynet/go88ynet
https://cars.yclas.com/user/go88ynet
https://www.yumpu.com/user/go88ynet
https://coolors.co/u/go88ynet
https://subaru-svx.net/forum/member.php?u=26103
https://www.divephotoguide.com/user/go88ynet
https://kheotay.com.vn/forums/users/ahgtf668
https://raovatquynhon.com/thiet-bi-dien-tu-4/go88ynet-19951
https://trio.vn/thiet-bi-dien-tu-4/go88ynet-23995
https://www.vsetutonline.com/forum/member.php?u=324073
https://raovatdangtin.com/thiet-bi-dien-tu-4/go88ynet-18673
https://bresdel.com/go88ynet
https://profile.sampo.ru/go88ynet
https://sub4sub.net/forums/users/go88ynet/
https://www.brownbook.net/business/55021527/go88ynet
https://artelis.pl/autor/profil/238600
https://www.isarms.com/forums/members/go88ynet.411239/#about
https://5bbf033c.godaddysites.com/
https://support.bitspower.com/support/user/go88ynet
https://www.uscgq.com/forum/posts.php?forum=general&id=691126
https://www.betting-forum.com/members/go88ynet.156244/#about
https://gettr.com/user/e245145704131059712
https://ofuse.me/go88ynet
https://www.emdr-training.net/forums/users/go88ynet/
http://www.bestqp.com/user/go88ynet
https://diendannhansu.com/members/go88ynet.107644/#about
https://ismschools.com.au/forums/users/go88ynet/
https://addons.mozilla.org/en-US/android/user/19867672/
https://addons.mozilla.org/af/android/user/19867672/
https://addons.mozilla.org/ar/android/user/19867672/
https://addons.mozilla.org/ast/android/user/19867672/
https://addons.mozilla.org/az/android/user/19867672/
https://addons.mozilla.org/bg/android/user/19867672/
https://addons.mozilla.org/bn/android/user/19867672/
https://podcasts.apple.com/tj/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/ua/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/cl/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/bg/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/lv/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/no/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/ro/podcast/go88ynet/id1840061149?i=1000761819760
https://podcasts.apple.com/af/podcast/go88ynet/id1840061149?i=1000761819760
https://telegra.ph/go88ynet-04-17
https://ivebo.co.uk/read-blog/300144
https://mez.ink/go88ynet8
https://blogfreely.net/go88ynet8/go88
https://hedgedoc.dezentrale.space/s/d-oNI-1b5
https://pad.darmstadt.social/s/Rx4YiVb-H7
https://hack.allmende.io/s/EpOjyFeIu
https://stuv.othr.de/pad/s/0KmVi1B-Q
https://hackmd.okfn.de/s/SJcjyLkaZg
https://pad.lescommuns.org/s/eRHityW_q
https://notes.bmcs.one/s/TaEg7WYFeX
https://rant.li/go88kinnet8/go88
https://quicknote.io/cfc5b3b0-3a24-11f1-b193-9df03bc80fa8
https://justpaste.me/DcUK2
https://writexo.com/share/908490587dc7
https://tudomuaban.com/chi-tiet-rao-vat/2879352/go88ynet8.html
https://ofuse.me/e/356055
https://www.keepandshare.com/discuss4/39063/go88ynet
https://pastelink.net/69nan5m6
https://69e1d08b386fc.site123.me/
https://freepaste.link/4lykg5ie64
https://www.notebook.ai/documents/2490444
https://pad.libreon.fr/s/5Au3tePrH
https://scrapbox.io/go88ynet8/go88ynet
https://go88ynet8.mystrikingly.com/
https://solve.edu.pl/forum/category/0/subcategory/0/thread/4413
https://data.gov.ro/en/user/go88ynet
https://civilprodata.heraklion.gr/user/go88ynet
https://dados.uff.br/user/go88ynet
https://pll.coe.hawaii.edu/author/go88ynet/
https://visionuniversity.edu.ng/profile/go88ynet/
https://admin.opendatani.gov.uk/tr/datarequest/f931d97f-d9c9-4899-b876-4e6dc9aafd40
https://codi.hostile.education/s/jLBuHID2a
https://www.edufex.com/forums/discussion/general/go88ynet
https://matrix.edu.lk/profile/go88ynet/
https://datos.chduero.es/user/go88ynet
https://dados.ufrn.br/user/go88ynet
https://adcuni.edu.pe/aula-virtual/profile/go88ynet/
https://pad.itiv.kit.edu/s/dnVq1yI8L
https://data.loda.gov.ua/user/go88ynet
https://edu.learningsuite.id/profile/go88ynet/
https://institutocrecer.edu.co/profile/go88ynet/
https://sgacademy.co.id/profile/go88ynet/
https://homologa.cge.mg.gov.br/user/go88ynet
https://dados.ifac.edu.br/en/user/go88ynet
https://dadosabertos.ifc.edu.br/user/go88ynet
https://rciims.mona.uwi.edu/user/go88ynet
https://pnguotdtc.edu.pg/blog/index.php?entryid=33617
https://firstrainingsalud.edu.pe/profile/go88ynet/
https://ait.edu.za/profile/go88ynet/
https://www.jit.edu.gh/it/members/go88ynet8/activity/35717/
https://www.igesi.edu.pe/miembros/go88ynet/activity/40782/
https://ensp.edu.mx/members/go88ynet8/activity/119889/
https://uemalp.edu.ec/author/go88ynet/
https://studyhub.themewant.com/profile/go88ynet/
https://onrtip.gov.jm/profile/go88ynet/
https://umcourse.umcced.edu.my/profile/go88ynet/?view=instructor
https://portal.stem.edu.gr/profile/loantrinh11marc6964/
https://tvescola.juazeiro.ba.gov.br/profile/go88ynet/
http://edu.mrpam.gov.mn/user/go88ynet
https://blog.sighpceducation.acm.org/wp/forums/users/go88ynet/
https://sighpceducation.hosting.acm.org/wp/forums/users/go88ynet/
https://lms.ait.edu.za/profile/go88ynet/
https://iescampus.edu.lk/profile/go88ynet/
https://academy.edutic.id/profile/go88ynet/
https://idiomas.ifgoiano.edu.br/blog/index.php?entryid=16327
https://mooc.ifro.edu.br/mod/forum/discuss.php?d=52883
https://dados.unifei.edu.br/user/go88ynet
https://jobs.lifewest.edu/employer/go88ynet
https://pibelearning.gov.bd/profile/go88ynet/
https://honduras.esapa.edu.ar/profile/loantrinh11marc6964/
https://bta.edu.gt/profile/loantrinh11marc6964tutaikhoan-com/
https://amiktomakakamajene.ac.id/profile/go88ynet/
https://learndash.aula.edu.pe/miembros/go88ynet/activity/202301/
https://intranet.estvgti-becora.edu.tl/profile/go88ynet/
https://opendata.ternopilcity.gov.ua/user/go88ynet
https://dadosabertos.ufma.br/user/go88ynet
https://academia.sanpablo.edu.ec/profile/go88ynet/
https://ncon.edu.sa/profile/go88ynet/
https://test.elit.edu.my/author/go88ynet/
https://engr.uniuyo.edu.ng/author/go88ynet/
https://blac.edu.pl/profile/go88ynet/
https://mpgimer.edu.in/profile/go88ynet/
https://aqa.horizon.ac.id/author/go88ynet/
https://www.oureducation.in/answers/profile/go88ynet/
https://datos.estadisticas.pr/user/go88ynet
https://efg.edu.uy/profile/loantrinh11marc6964/
https://gdcnagpur.edu.in/LMS/profile/go88ynet/
https://www.colegiovirtualausubel.edu.co/group/informacion-colegio-ausubel/discussion/9d3f6042-07c3-40b7-805b-c123e462f706
https://mooc.esil.edu.kz/profile/go88ynet/
https://faculdadelife.edu.br/profile/go88ynet/
https://lms.gkce.edu.in/profile/go88ynet/
https://lms.wtca.edu.in/profile/go88ynet/
https://elearning.urp.edu.pe/author/go88ynet/
https://catalog.citydata.in.th/user/go88ynet
https://data.aurora.linkeddata.es/user/go88ynet
https://dados.justica.gov.pt/user/go88ynet
https://www.wcs.edu.eu/profile/go88ynet/
https://forum.attica.gov.gr/members/go88ynet/
https://wiki.ling.washington.edu/bin/view/Main/Go88yNet
https://pimrec.pnu.edu.ua/members/go88ynet8/profile/
https://triumph.srivenkateshwaraa.edu.in/profile/go88ynet
https://fesanjuandedios.edu.co/miembros/loantrinh11marc6964/
https://ans.edu.my/profile/go88ynet/
https://vspmscop.edu.in/LRM/author/go88ynet/
https://edublogs.org/author/go88ynet/
https://dados.ufscar.br/user/go88ynet
https://open.mit.edu/profile/01KPD4SZ2K6089C2FWXBQDAZTS/
https://bbiny.edu/profile/go88ynet/
https://iltc.edu.sa/en_us/profile/go88ynet/
The much less burdensome the ask, the more probable they will certainly intend to participate.
Check out my web site :: https://www.facebook.com/serverifiedlists/
Hello, you used to write magnificent, but the last several posts have been kinda boring?K I miss your super writings. Past several posts are just a little out of track! come on!
Wow that was unusual. I just wrote an really long comment but after I clicked submit my comment didn’t appear. Grrrr… well I’m not writing all that over again. Anyhow, just wanted to say wonderful blog!
I wanted to put you the tiny remark to finally thank you so much yet again considering the breathtaking methods you have provided above. It’s remarkably open-handed of people like you giving extensively all that some people would have made available for an e book to earn some dough for themselves, and in particular since you might well have tried it if you wanted. The secrets additionally worked to become a fantastic way to comprehend many people have a similar keenness much like my personal own to see lots more concerning this problem. I believe there are numerous more enjoyable situations up front for individuals who look into your site.
Hey, you used to write wonderful, but the last several posts have been kinda boring… I miss your great writings. Past several posts are just a little bit out of track! come on!
WONDERFUL Post.thanks for share..extra wait .. …
Very interesting subject , thanks for posting.
Everything is very open and very clear explanation of issues. was truly information. Your website is very useful. Thanks for sharing.
I’m impressed, I need to say. Actually not often do I encounter a blog that’s both educative and entertaining, and let me tell you, you’ve got hit the nail on the head. Your concept is excellent; the issue is one thing that not enough individuals are talking intelligently about. I’m very completely happy that I stumbled across this in my search for something relating to this.
Wow! Thank you! I continuously wanted to write on my website something like that. Can I include a portion of your post to my site?
This site can be a walk-by way of for the entire data you wished about this and didn’t know who to ask. Glimpse here, and you’ll positively uncover it.
Hey! This is kind of off topic but I need some advice from an established blog. Is it very difficult to set up your own blog? I’m not very techincal but I can figure things out pretty fast. I’m thinking about setting up my own but I’m not sure where to begin. Do you have any ideas or suggestions? Appreciate it
Deference to website author, some fantastic selective information.
Wow! Terima kasih! Saya secara terus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya menerapkan sebagian dari posting Anda ke situs saya?
Hei semua, saya menjumpai situs Anda lewat Google ketika menelusuri topik yang mirip, situs Anda muncul di posisi atas. Saya harus mengakui bahwa saya kagum seberapa baik penulisannya. Saya sangat menikmati menelusuri ini dan saya akan kembali untuk membaca konten lainnya. Terima kasih banyak!
Terima kasih untuk situs informatif lainnya. Di mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan cara yang sempurna? Saya punya sebuah inisiatif yang saya sedang kerjakan, dan saya telah mencari informasi seperti ini.
Great wordpress blog here.. It’s hard to find quality writing like yours these days. I really appreciate people like you! take care
If some one wishes expert view about blogging after that i
advise him/her to pay a quick visit this website, Keep
up the fastidious job.
Just desire to say your article is as surprising. The clearness to your put up is just nice and i can suppose you are an expert on this subject. Fine along with your permission let me to grasp your feed to keep up to date with coming near near post. Thank you a million and please continue the gratifying work.
After research a number of of the weblog posts on your web site now, and I actually like your way of blogging. I bookmarked it to my bookmark web site list and might be checking again soon. Pls try my web page as well and let me know what you think.
Thanks, Loads of stuff!
Look into my site – https://Overwatch2Base.com/
Enjoyed studying this, very good stuff, regards.
I was recommended this web site by my cousin. I am not
sure whether this post is written by him as no one
else know such detailed about my difficulty. You are amazing!
Thanks!
Appreciate it for helping out, great information.
Thanks , I have just been searching for information about this subject for ages and yours is the best I’ve found out so far. However, what concerning the bottom line? Are you certain about the source?
Some times its a pain in the ass to read what website owners wrote but this website is really user pleasant! .
I am curious to find out what blog platform you’re utilizing? I’m having some minor security issues with my latest site and I would like to find something more safeguarded. Do you have any solutions?
obviously like your website however you need to test the spelling on quite
a few of your posts. Several of them are rife with
spelling problems and I in finding it very bothersome to inform the reality however I will
certainly come again again.
Saya tidak umumnya berkomentar tetapi saya harus mengakui terimakasih untuk posting yang luar biasa ini : D.
Postingan yang sangat baik! Saya menghargai gaya Anda menjelaskan segala sesuatu dengan sangat jelas. Teruskan pekerjaan yang hebat!
Anda dapat pasti melihat keahlian Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Hi every one, here every person is sharing these experience, so it’s pleasant to read this website, and I
used to pay a quick visit this web site every day.
Wohh persis apa yang saya telusuri, hargai atas unggahan.
This aids to develop backlinks that significantly raise your website’s traffic and SEO ranking.
Look into my web-site; https://medium.com/@traveltoday0082/unlocking-the-full-potential-of-gsa-search-engine-ranker-for-seo-mastery-69fb8e100768
Ini adalah situs yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Amat hebat informasi dapat ditemukan di web blog.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu baik. Bye
I simply wished to say thanks once more. I am not sure what I would’ve followed without the entire suggestions discussed by you about my problem. This was a very scary difficulty in my circumstances, but encountering the skilled form you resolved it forced me to jump for contentment. Now i’m thankful for your help and even pray you find out what a powerful job you were getting into educating other individuals using your web page. I know that you have never got to know all of us.
Some really nice stuff on this site, I enjoy it.
Wohh baru saja apa yang saya cari, terimakasih atas posting.
Hi there! I just wanted to ask if you ever have any problems with
hackers? My last blog (wordpress) was hacked and I ended up losing
several weeks of hard work due to no data backup. Do you have any solutions to stop hackers?
Aku benar-benar ingin menulis pesan singkat untuk mengucapkan terima kasih Anda atas seluruh informasi luar biasa yang Anda tuliskan di website ini.
Terima kasih atas tulisan yang bagus. Faktanya ini sebelumnya adalah sebuah konten hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat menjaga kontak?
Just wanna input on few general things, The website design and style is perfect, the content is very wonderful. “Earn but don’t burn.” by B. J. Gupta.
Wow! Ini bisa jadi salah satu blog paling membantu yang pernah kami temui tentang topik ini. Sebenarnya Mengagumkan. Saya juga seorang ahli dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
Saya tidak umumnya berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang spesial ini : D.
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia sebenarnya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui weblog Anda dengan lebih banyak detail? Ini sangat berguna bagi saya. Jempol besar untuk publikasi blog ini!
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Akan tetapi ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika potensial, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan tambahan detail? Ini sangat berguna bagi saya. Jempol besar untuk posting weblog ini!
Saya selalu tertarik dengan subjek ini dan masih demikian, sangat dihargai telah memposting.
Hari ini, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
You got a very excellent website, Gladiola I noticed it through yahoo.
Very interesting topic, thankyou for putting up. “What passes for optimism is most often the effect of an intellectual error.” by Raymond Claud Ferdinan Aron.
I believe this web site has got some very good info for everyone :D. “As ill-luck would have it.” by Miguel de Cervantes.
Postingan ini sangat berguna. Saya menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan pesan yang sama. Apakah ada cara Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
Sangat luar biasa info dapat ditemukan di situs.
you’re in reality a just right webmaster. The website loading speed is incredible. It kind of feels that you are doing any unique trick. In addition, The contents are masterpiece. you’ve performed a fantastic activity on this matter!
Saya mendapatkan info yang bagus dari blog Anda.
Just wish to say your article is as astonishing. The clarity in your post is just great and i could assume
you’re an expert on this subject. Well with your permission let me to grab your
feed to keep updated with forthcoming post. Thanks a million and
please continue the enjoyable work.
Artikel yang sangat berguna. Saya baru saja menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi.
Sangat menarik detail yang Anda sebutkan, terima kasih telah memposting.
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang hebat!
Kami dapat memiliki hyperlink pertukaran perjanjian di antara kita!
Needed to send you this very little word to be able to say thanks yet again considering the precious strategies you have documented above. This is certainly shockingly open-handed with people like you to deliver openly all that a few people would’ve advertised for an ebook to make some money for their own end, particularly now that you might well have done it if you considered necessary. These secrets likewise acted to provide a good way to be certain that other people online have the same keenness similar to mine to find out good deal more with regard to this matter. I’m certain there are some more enjoyable sessions ahead for individuals who view your blog post.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Saya senang menjadi pengunjung dari situs web total ini!, sangat dihargai atas info langka ini!
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar pantas. Isi yang hebat dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
list of supplements that contain steroids
References:
https://travelersqa.com/user/davidsilk1
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima empat email dengan pesan yang sama. Apakah ada pendekatan Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
Hei, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini adalah tepat tipe informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada rekan-rekan. Terima kasih telah berbagi.
I was recommended this web site by my cousin. I’m not sure whether this post is written by him as nobody else know such detailed about my problem. You’re amazing! Thanks!
Thanks for finally talking about > Balancing the Scales:
Patient Load vs. Care Quality in Diabetes – D-Coded Diabetes Research < Liked it!
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Postingan ini penuh informasi. Saya menghargai waktu yang Anda luangkan untuk menulisnya. Terima kasih!
Lovely just what I was looking for.Thanks to the author for taking his time on this one.
Hei semua, saya menjumpai website Anda melalui Google ketika menelusuri topik yang serupa, website Anda tampil di hasil teratas. Saya harus mengakui bahwa saya kagum betapa bagus penyusunannya. Saya benar-benar menikmati menelusuri ini dan saya akan kembali untuk melihat konten lainnya. Terima kasih!
Kami mungkin memiliki tautan pertukaran perjanjian antara kita!
Isi yang hebat! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas berbagi ini.
Postingan yang luar biasa! Saya sangat menghargai cara Anda menguraikan segala sesuatu dengan mudah dipahami. Teruskan kerja yang bagus!
Saya senang bahwa saya mengamati situs web ini, tepat info yang saya telusuri!
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Ini benar-benar menjawab masalah saya, terima kasih!
Saya terkesan dengan situs internet ini, sangat saya adalah penggemar berat.
Saya sangat beruntung menemukan situs web ini di Bing, persis seperti yang saya cari : D pula sudah saya bookmark.
Anda bisa pasti melihat keahlian Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Saya amat bersyukur menemukan situs web ini di Bing, persis seperti yang saya cari : D begitu juga sudah saya simpan ke fav.
Sangat bagus website yang Anda miliki, tapi saya penasaran apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin menjadi bagian dari kelompok di mana saya bisa mendapatkan umpan balik dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
This is my first time pay a quick visit at here and i am genuinely pleassant to read everthing at one place.
Saya tidak amat fantastis dalam bahasa Inggris tetapi saya memperoleh ini amat mudah untuk dipahami.
Ini adalah situs yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar hebat!
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Fantastis. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami usaha Anda.
Mengagumi waktu dan tenaga yang Anda curahkan ke situs Anda dan informasi mendalam yang Anda berikan. Sangat hebat menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Very nice post. I just stumbled upon your blog and wanted to say that I’ve truly loved surfing around your blog posts. After all I will be subscribing for your feed and I am hoping you write once more very soon!
Dengan semua hal yang mana terlihat sedang dibangun sepanjang topik ini, sebagian besar pandangan Anda ternyata agak menstimulasi. Di sisi lain, saya maaf, karena saya tidak memberikan kepercayaan pada keseluruhan rencana Anda, meskipun menyegarkan. Sepertinya bagi kami bahwa ulasan Anda tidak benar-benar tervalidasi dan pada kenyataannya Anda sendiri tidak sepenuhnya pasti terhadap argumen tersebut. Dalam hal apa pun saya menghargai membaca.
Aku sungguh ingin mengirim komentar singkat untuk menghargai Anda atas semua saran luar biasa yang Anda bagikan di situs ini.
Heya i am for the first time here. I found this board and I to find It really useful & it helped me out much. I hope to provide one thing back and aid others like you helped me.
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Ini adalah situs yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar luar biasa!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada metode Anda akan bisa menghapus saya dari layanan itu? Terima kasih!
You have brought up a very great points, thankyou for the post.
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan yang unggul!
I love it when people come together and share opinions, great blog, keep it up.
Hey! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing several weeks of hard work due to no data backup. Do you have any methods to protect against hackers?
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Wow! Terima kasih! Saya selalu ingin menulis di situs saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke website saya?
Wohh persis apa yang saya cari, terima kasih atas posting.
Sangat menarik detail yang Anda sebutkan, thankyou telah mengunggah. “Jive Lady Just hang loose blood. She gonna handa your rebound on the med side.” oleh Airplane.
Aku benar-benar ingin mengirim komentar singkat guna menghargai Anda atas seluruh informasi luar biasa yang Anda tuliskan di website ini.
Saya melihat banyak website tetapi saya anggap yang satu ini mengandung sesuatu yang spesial di dalamnya
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Media adalah pesan.” oleh Marshall McLuhan.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Kerja yang mengagumkan!
Ini adalah topik yang sangat dekat di hati saya, salam, tapi di manakah detail kontak Anda?
Wohh persis apa yang saya cari, hargai atas posting.
Thanks for this post, I am a big big fan of this internet site would like to keep updated.
Menikmati membaca keseluruhan ini, sangat bagus, salam.
Hai semua, hanya ingin mengatakan bahwa saya benar-benar menyukai membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan cukup banyak informasi yang bermanfaat. Terima kasih!
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Sangat menarik detail yang Anda sebutkan, terima kasih telah mengunggah.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Umumnya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, sangat posting yang bagus.
Saya terkesan dengan situs internet ini, sangat saya adalah penggemar berat.
After research a few of the blog posts on your web site now, and I actually like your way of blogging. I bookmarked it to my bookmark web site list and can be checking again soon. Pls try my website online as nicely and let me know what you think.
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini dulunya adalah sebuah akun hiburan. Terlihat kompleks menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat tetap berhubungan?
Bagian yang mengesankan, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika bisa dilakukan, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui blog Anda dengan lebih banyak detail? Ini sangat berguna bagi saya. Jempol besar untuk unggahan blog ini!
Konten yang fantastis! Cara penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk melihat konten lainnya.
Informasi yang sangat berguna. Saya baru saja menelusuri hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Terima kasih untuk blog informatif tambahan. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan pendekatan yang ideal? Saya punya sebuah tantangan yang saya tengah jalankan, dan saya sudah mengamati informasi seperti ini.
Benar-benar jelas website, terima kasih untuk posting ini.
Seiring dengan seluruhnya yang terlihat sedang berkembang sepanjang topik spesifik ini, pandangan Anda cenderung relatif menyegarkan. Walaupun begitu, saya maaf, tetapi saya tidak memberikan kepercayaan pada seluruh ide Anda, meskipun menggairahkan. Sepertinya bagi saya bahwa komentar Anda tidak sepenuhnya sepenuhnya dapat dibenarkan dan pada kenyataannya Anda sendiri tidak benar-benar sepenuhnya pasti terhadap poin tersebut. Dalam hal apa pun saya menghargai membaca.
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
Halo di sana, Anda telah melakukan kerja yang fantastis. Saya pasti akan menyimpan ini dan kembali untuk membaca konten lainnya. Terima kasih!
Saya benar-benar bersyukur menemukan situs ini di Bing, persis seperti yang saya telusuri : D selain itu sudah saya simpan ke favorit.
Saya menghargai usaha yang Anda luangkan untuk menyusun artikel ini. Informasi yang bernilai. Terima kasih!
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Saya selalu memikirkan hal ini, sangat dihargai telah mengunggah.
Saya benar-benar bersyukur menemukan situs ini di Bing, persis seperti yang saya telusuri : D pula sudah saya simpan di bookmark saya.
References:
Ifbb pro steroid cycle
References:
http://www.annunciogratis.net/author/spycougar26
Saya kebetulan menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
I don’t know whether it’s just me or if everybody else experiencing problems with your website.
It looks like some of the text on your posts are running off the screen. Can somebody else
please provide feedback and let me know if this is happening to
them too? This could be a problem with my browser because I’ve had this happen previously.
Thanks
Saya sangat menghargai waktu yang Anda luangkan untuk menyusun artikel ini. Informasi yang sangat berharga. Terima kasih banyak!
Luar biasa website yang Anda miliki, tapi saya penasaran apakah Anda tahu forum diskusi pengguna yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan masukan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Terima kasih atas tulisan yang baik. Sebenarnya ini sebelumnya adalah sebuah konten hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Great post. I was checking continuously this blog and I am impressed! Very helpful information specifically the last part 🙂 I care for such info a lot. I was looking for this certain info for a long time. Thank you and good luck.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Woh I like your blog posts, saved to bookmarks! .
When I initially commented I appear to have clicked the -Notify me when new comments are added- checkbox and now each time a
comment is added I get four emails with the exact same comment.
There has to be an easy method you can remove me from that service?
Kudos!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya senang menjadi pengunjung dari weblog total ini!, salam atas informasi langka ini!
Saya kebetulan menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang bagus.
Terima kasih untuk blog informatif tambahan. Di mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan cara yang ideal? Saya memiliki sebuah inisiatif yang saya tengah kerjakan, dan saya sudah mengamati informasi seperti ini.
Terima kasih untuk website informatif tambahan. Di mana lagi saya memperoleh informasi seperti itu yang ditulis dengan pendekatan yang ideal? Saya memiliki sebuah tantangan yang saya sedang kerjakan sekarang, dan saya sudah mencari informasi seperti ini.
I reckon something genuinely special in this site.
Thanks in favor of sharing such a nice thought, post is pleasant, thats why i
have read it completely
Artikel yang sangat membantu. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi.
Amat fantastis informasi dapat ditemukan di blog.
Hi there are using WordPress for your blog platform? I’m new to the blog world but I’m trying to get started and create my own. Do you require any coding knowledge to make your own blog? Any help would be greatly appreciated!
Saya tidak sangat mahir dalam bahasa Inggris tetapi saya memperoleh ini benar-benar mudah untuk dibaca .
Secara umum saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup posting yang bagus.
Seseorang secara esensial menolong untuk membuat sangat artikel saya mungkin katakan. Itu adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk menyusun unggahan istimewa ini. Kerja yang fantastis!
Terima kasih, saya baru-baru ini mencari informasi tentang subjek ini sudah lama dan milik Anda adalah yang terbaik yang saya ketahui hingga sekarang. Tapi, bagaimana dengan kesimpulan? Apakah Anda positif tentang sumber tersebut?
I see something really interesting about your blog so I saved to favorites.
Very good blog! Do you have any suggestions for aspiring writers? I’m hoping to start my own site soon but I’m a little lost on everything. Would you suggest starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m completely overwhelmed .. Any recommendations? Many thanks!
Ini adalah tips yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan pesan yang sama. Apakah ada pendekatan Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Hebat situs yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin sekali menjadi bagian dari kelompok di mana saya bisa mendapatkan tanggapan dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
hello!,I like your writing so much! share we communicate more about your article on AOL? I need a specialist on this area to solve my problem. May be that’s you! Looking forward to see you.
Saya tanpa henti memikirkan hal ini, terimakasih telah mengunggah.
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Appreciation to my father who stated to me about this weblog,
this webpage is really remarkable.
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia sebenarnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari lebih banyak tentang topik ini. Jika bisa dilakukan, seiring Anda menjadi lebih ahli, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak rincian? Ini sangat membantu bagi saya. Jempol besar untuk kiriman blog ini!
Terima kasih banyak atas posting yang sangat baik. Saya benar-benar menikmati membaca ini dan menemukan banyak informasi yang berguna. Teruskan kerja yang hebat!
Saya sungguh ingin menulis komentar singkat guna menghargai Anda atas semua informasi luar biasa yang Anda tuliskan di website ini.
Saya mendapatkan info yang bagus dari blog Anda.
As I web site possessor I believe the content matter here is rattling fantastic , appreciate it for your hard work. You should keep it up forever! Good Luck.
I’m not sure exactly why but this website is loading incredibly slow for me. Is anyone else having this problem or is it a problem on my end? I’ll check back later on and see if the problem still exists.
With havin so much content and articles do you ever run into any problems of plagorism or copyright infringement? My site has a lot of exclusive content I’ve either written myself or outsourced but it appears a lot of it is popping it up all over the web without my permission. Do you know any techniques to help stop content from being ripped off? I’d certainly appreciate it.
I like this site so much, saved to favorites. “American soldiers must be turned into lambs and eating them is tolerated.” by Muammar Qaddafi.
very good submit, i definitely love this website, keep on it
Howdy, i read your blog occasionally and i own a similar one and i was just wondering if you get a lot of spam feedback? If so how do you protect against it, any plugin or anything you can advise? I get so much lately it’s driving me insane so any assistance is very much appreciated.
Enjoyed studying this, very good stuff, thankyou.
I’d forever want to be update on new posts on this site, saved to bookmarks! .
Howdy! Someone in my Myspace group shared this website with us so I came to look it over. I’m definitely loving the information. I’m bookmarking and will be tweeting this to my followers! Excellent blog and fantastic style and design.
Woah! I’m really loving the template/theme of this website. It’s simple, yet effective. A lot of times it’s tough to get that “perfect balance” between superb usability and visual appeal. I must say you have done a very good job with this. In addition, the blog loads super fast for me on Internet explorer. Excellent Blog!
Hey would you mind letting me know which hosting company you’re working with? I’ve loaded your blog in 3 different browsers and I must say this blog loads a lot quicker then most. Can you recommend a good internet hosting provider at a honest price? Many thanks, I appreciate it!
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
Thanks for the post, can I set it up so I get an email whenever you publish a fresh update?
It is perfect time to make some plans for the longer term and it is time to be happy. I have learn this submit and if I could I wish to recommend you some interesting things or advice. Maybe you could write next articles relating to this article. I wish to learn even more issues about it!
Woah! I’m really enjoying the template/theme of this site.
It’s simple, yet effective. A lot of times it’s tough to get that “perfect balance” between superb usability and visual appearance.
I must say that you’ve done a fantastic job
with this. Also, the blog loads super fast for me on Firefox.
Superb Blog!
Sweet blog! I found it while searching on Yahoo News. Do you have any suggestions on how to get listed in Yahoo News? I’ve been trying for a while but I never seem to get there! Cheers
Hi colleagues, how is everything, and what you would like to say
concerning this piece of writing, in my view its actually awesome
in support of me.
Isi yang bermanfaat dan disajikan dengan sangat baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Artikel yang bagus. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
I liked as much as you’ll obtain carried out right here. The comic strip is tasteful, your authored subject matter stylish. nevertheless, you command get bought an nervousness over that you would like be delivering the following. sick surely come more beforehand again as exactly the similar nearly a lot continuously within case you shield this increase.
It’s really a cool and useful piece of information. I am happy that you simply shared this useful information with us. Please keep us up to date like this. Thank you for sharing.
Thank you so much for providing individuals with such a special chance to read from this site. It is often so great and as well , jam-packed with a great time for me and my office fellow workers to search your website more than three times in a week to read the newest items you will have. And lastly, I’m just always happy with the special information served by you. Certain 2 facts in this post are unquestionably the most efficient I’ve had.
You have mentioned very interesting details ! ps nice internet site.
Saya perlu mengatakan, ini adalah salah satu posting terbaik yang pernah saya baca belakangan ini. Informasi yang sangat membantu. Terima kasih telah berbagi.
Cheers! I enjoy this.
My homepage … https://seaofthievespedia.com
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sesungguhnya membeli saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika potensial, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan tambahan detail? Ini sangat berguna bagi saya. Jempol besar untuk kiriman weblog ini!
Respect to article author, some excellent entropy.
Hello! I simply want to offer you a huge thumbs up for
the great info you have got right here on this post.
I’ll be returning to your web site for more soon.
I have recently started a website, the information you offer on this website has helped me greatly. Thank you for all of your time & work. “Everyone is responsible and no one is to blame.” by Will Schutz.
Really good info can be found on site. “The absence of flaw in beauty is itself a flaw.” by Havelock Ellis.
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Thanks for your marvelous posting! I seriously enjoyed reading it, you could be a great author.I will ensure that I bookmark your blog and definitely will come back at some point. I want to encourage you continue your great writing, have a nice morning!
Wow! Terima kasih! Saya secara terus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan fragmen dari posting Anda ke blog saya?
Would you be keen on exchanging links?
If some one wants to be updated with latest technologies then he must be go to see this
web page and be up to date daily.
I like this site very much, Its a very nice spot to read and receive info . “Philosophy is a battle against the bewitchment of our intelligence by means of language.” by Ludwig Wittgenstein.
Thanks a lot for sharing this with all of us you actually know what you are talking about! Bookmarked. Please also visit my site =). We could have a link exchange agreement between us!
Hey very nice blog!! Man .. Excellent .. Amazing .. I will bookmark your site and take the feeds also…I’m happy to find so many useful information here in the post, we need develop more techniques in this regard, thanks for sharing. . . . . .
Do you have a spam problem on this site; I also am a blogger, and I was curious about your situation; many of us have created some nice methods and we are looking to swap methods with others, be sure to shoot me an email if interested.
At this time it seems like WordPress is the preferred blogging platform available right now. (from what I’ve read) Is that what you are using on your blog?
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Great line up. We will be linking to this great article on our site. Keep up the good writing.
I gotta favorite this web site it seems very useful very beneficial
Enjoyed studying this, very good stuff, thanks. “A man does not die of love or his liver or even of old age he dies of being a man.” by Percival Arland Ussher.
Excellent post. I was checking continuously this blog and I’m impressed! Extremely useful information particularly the last part 🙂 I care for such info a lot. I was looking for this certain info for a very long time. Thank you and best of luck.
Konten yang luar biasa! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
hello there and thank you for your information – I have certainly picked up something new from right here. I did however expertise a few technical issues using this site, as I experienced to reload the web site a lot of times previous to I could get it to load correctly. I had been wondering if your hosting is OK? Not that I am complaining, but slow loading instances times will often affect your placement in google and can damage your quality score if ads and marketing with Adwords. Anyway I’m adding this RSS to my email and can look out for much more of your respective intriguing content. Make sure you update this again soon..
Your home is valueble for me. Thanks!…
Wow! Terima kasih! Saya selalu membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menerapkan bagian dari posting Anda ke situs saya?
Saya terkesan dengan situs web ini, amat saya adalah penggemar.
After examine a number of of the weblog posts in your website now, and I actually like your means of blogging. I bookmarked it to my bookmark web site record and will be checking again soon. Pls check out my website online as well and let me know what you think.
Hello, i think that i saw you visited my website so i came to “return the favor”.I am trying to find things to improve my site!I suppose its ok to use a few of your ideas!!
Artikel yang hebat. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan pekerjaan yang luar biasa!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada metode Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
Have you ever considered writing an e-book or guest authoring on other websites?
I have a blog centered on the same ideas you discuss and would love to
have you share some stories/information. I know my readers
would enjoy your work. If you are even remotely interested, feel
free to send me an e-mail.
My coder is trying to convince me to move to .net from PHP. I have always disliked the idea because of the expenses. But he’s tryiong none the less. I’ve been using WordPress on several websites for about a year and am concerned about switching to another platform. I have heard excellent things about blogengine.net. Is there a way I can transfer all my wordpress content into it? Any help would be really appreciated!
you are truly a excellent webmaster. The site loading speed is amazing. It seems that you are doing any distinctive trick. In addition, The contents are masterwork. you’ve done a great activity in this topic!
Terima kasih atas posting yang hebat. Saya benar-benar menyukai membaca ini dan menemukan banyak sekali wawasan yang berguna. Teruskan pekerjaan yang bagus!
Aku sungguh ingin menulis pesan singkat untuk mengucapkan terima kasih Anda atas seluruh informasi luar biasa yang Anda bagikan di situs ini.
As I website possessor I believe the written content here is rattling fantastic, regards for your efforts.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Good blog! I really love how it is simple on my eyes and the data are well written. I am wondering how I could be notified whenever a new post has been made. I have subscribed to your RSS which must do the trick! Have a great day!
Wow, keren weblog struktur! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Seluruh tampilan situs Anda mengagumkan, belum lagi kontennya!
I’m really loving the theme/design of your weblog. Do you ever run into any web browser compatibility problems? A number of my blog audience have complained about my website not working correctly in Explorer but looks great in Firefox. Do you have any recommendations to help fix this problem?
Whats Taking place i’m new to this, I stumbled upon this I’ve found It positively useful and it has aided me out loads. I hope to contribute & help other customers like its aided me. Great job.
It’s really a great and useful piece of info. I am glad that you shared this helpful information with us. Please keep us informed like this. Thank you for sharing.
I am always searching online for ideas that can aid me. Thx!
I truly enjoy reading through on this internet site, it has got excellent articles.
Hey there! Someone in my Myspace group shared this site with us so I came to look it over. I’m definitely loving the information. I’m book-marking and will be tweeting this to my followers! Fantastic blog and terrific design.
My brother suggested I might like this website. He was entirely right. This post actually made my day. You cann’t believe simply how a lot time I had spent for this information! Thank you!
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
I am not positive the place you are getting your information, but good topic. I needs to spend a while finding out much more or understanding more. Thanks for great info I used to be searching for this information for my mission.
After study a few of the blog posts in your website now, and I truly like your approach of blogging. I bookmarked it to my bookmark website listing and shall be checking back soon. Pls check out my website as properly and let me know what you think.
certainly like your website but you have to test the spelling on several of your posts. Many of them are rife with spelling issues and I in finding it very troublesome to tell the reality nevertheless I’ll surely come back again.
The following time I read a blog, I hope that it doesnt disappoint me as much as this one. I mean, I know it was my choice to learn, but I actually thought youd have something interesting to say. All I hear is a bunch of whining about something that you can repair when you werent too busy on the lookout for attention.
Do you have a spam issue on this website; I also am a blogger, and I was wondering your situation; we have created some nice methods and we
are looking to exchange solutions with other folks, please shoot me
an email if interested.
You can definitely see your enthusiasm in the work you write. The sector hopes for more passionate writers such as you who are not afraid to say how they believe. At all times go after your heart.
Very interesting info !Perfect just what I was searching for!
With havin so much content and articles do you ever run into any issues of plagorism or copyright infringement? My blog has a lot of completely unique content I’ve either authored myself or outsourced but it looks like a lot of it is popping it up all over the internet without my permission. Do you know any ways to help prevent content from being ripped off? I’d really appreciate it.
Well I truly liked studying it. This subject offered by you is very useful for good planning.
I have been reading out a few of your articles and it’s pretty clever stuff. I will make sure to bookmark your blog.
This is the right blog for anyone who wants to find out about this topic. You realize so much its almost hard to argue with you (not that I actually would want…HaHa). You definitely put a new spin on a topic thats been written about for years. Great stuff, just great!
Its like you read my mind! You seem to know so much about this, like you wrote the book in it or something. I think that you could do with some pics to drive the message home a little bit, but other than that, this is magnificent blog. A fantastic read. I will certainly be back.
Useful information. Fortunate me I discovered your web site by chance,
and I am shocked why this accident didn’t happened in advance!
I bookmarked it.
Seseorang pada dasarnya memberikan bantuan untuk membuat secara signifikan posting saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan hingga sekarang? Saya terkagum dengan riset yang Anda lakukan untuk menyusun kiriman luar biasa ini. Proses yang mengagumkan!
Hey there! I could have sworn I’ve been to this website before but after browsing through some of the post I realized it’s new to me. Nonetheless, I’m definitely happy I found it and I’ll be book-marking and checking back often!
Those are yours alright! . We at least need to get these people stealing images to start blogging! They probably just did a image search and grabbed them. They look good though!
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia pada kenyataannya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari tambahan tentang topik ini. Jika bisa dilakukan, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui weblog Anda dengan tambahan rincian? Ini sangat membantu bagi saya. Jempol besar untuk unggahan weblog ini!
Hi are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and create my own. Do you need any html coding expertise to make your own blog? Any help would be greatly appreciated!
so much great info on here, :D.
Some truly nice and utilitarian information on this website, besides I believe the style holds superb features.
I am glad to be a visitor of this consummate website! , regards for this rare info ! .
Thank you for sharing with us, I conceive this website truly stands out :D.
Great tremendous issues here. I’m very glad to look your article. Thanks so much and i am taking a look ahead to touch you. Will you kindly drop me a mail?
Usually I don’t learn article on blogs, however I would like to say that this write-up very forced me to check out and do it! Your writing taste has been surprised me. Thanks, quite nice article.
It’s actually a great and useful piece of info. I am happy that you just shared this helpful information with us. Please stay us informed like this. Thank you for sharing.
Hey! Would you mind if I share your blog with my facebook group? There’s a lot of people that I think would really enjoy your content. Please let me know. Many thanks
I got what you intend, thankyou for posting.Woh I am thankful to find this website through google. “Since the Exodus, freedom has always spoken with a Hebrew accent.” by Heinrich Heine.
Great tremendous things here. I’m very satisfied to peer your article. Thank you so much and i’m taking a look ahead to touch you. Will you kindly drop me a mail?
Does your site have a contact page? I’m having trouble locating it but, I’d like to shoot you an e-mail. I’ve got some creative ideas for your blog you might be interested in hearing. Either way, great blog and I look forward to seeing it improve over time.
This actually answered my downside, thanks!
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
Wow! Thank you! I constantly needed to write on my site something like that. Can I take a fragment of your post to my website?
Only wanna remark on few general things, The website style is perfect, the subject matter is very good. “I have seen the future and it doesn’t work.” by Robert Fulford.
You have brought up a very fantastic points, regards for the post.
Great line up. We will be linking to this great article on our site. Keep up the good writing.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya selalu menyelidiki online untuk tips yang dapat mendukung saya. Thanks!
Postingan yang sangat membantu. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
Isi yang hebat! Gaya penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca lebih banyak.
Umumnya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
Sangat menarik poin yang Anda utarakan, thankyou telah mengunggah.
Anda sudah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Bagian yang luar biasa, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit sekali analisis tentang ini. Dan dia sebenarnya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka mempelajari tambahan tentang topik ini. Jika potensial, seiring Anda menjadi lebih ahli, apakah Anda berkenan memperbarui weblog Anda dengan tambahan detail? Ini sangat membantu bagi saya. Jempol sangat besar untuk kiriman blog ini!
Postingan yang luar biasa. Ini memberikan saya pemahaman yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Alba Apex is a premium dental clinic in Moscow specializing in veneer placement, aesthetic dentistry, and tooth restoration. The main areas of practice include aesthetic (cosmetic) restorations and comprehensive smile design. The clinic uses digital diagnostics, microscope-assisted treatment, and modern protocols for implantology and prosthetic (orthopedic) dentistry.
Hore google adalah ratu saya yang membantu saya menemukan situs yang luar biasa! .
Konten yang berguna. Saya baru saja menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Ini adalah blog yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Sangat bersih web site, hargai untuk pos ini.
Postingan yang sangat baik! Saya sangat menghargai cara Anda menguraikan semuanya dengan sangat jelas. Teruskan pekerjaan yang bagus!
Saya mengunjungi banyak website tetapi saya pikir yang satu ini mengandung sesuatu yang spesial di dalamnya
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Terima kasih atas tulisan yang baik. Pada kenyataannya ini sebelumnya adalah sebuah konten hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita dapat menjaga kontak?
Artikel yang hebat. Ini memberi saya gambaran yang lebih baik tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Saya tidak sungguh luar biasa dalam bahasa Inggris tetapi saya menyadari ini amat santai untuk ditafsirkan.
Saya puas bahwa saya mendeteksi web blog ini, persis info yang saya cari!
Saya senang bahwa saya mengamati website ini, tepat info yang saya telusuri!
I like the helpful information you provide in your articles.
I’ll bookmark your weblog and check again here regularly.
I’m quite sure I will learn many new stuff right here!
Good luck for the next!
Saya mendapatkan info yang bagus dari blog Anda.
Konten yang hebat! Cara penulisan Anda jelas dan mudah dimengerti. Saya pasti akan kembali untuk melihat konten lainnya.
I couldn’t resist commenting
My partner and I stumbled over here coming from a different page and thought I might as well check things out. I like what I see so now i am following you. Look forward to checking out your web page repeatedly.
Heya i’m for the first time here. I came across this board and I find It truly useful & it helped me out much. I hope to give something back and help others like you aided me.
Postingan yang luar biasa! Saya menghargai gaya Anda menguraikan segala sesuatu dengan sangat jelas. Teruskan pekerjaan yang hebat!
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan yang hebat!
I love your blog.. very nice colors & theme. Did you create this website yourself? Plz reply back as I’m looking to create my own blog and would like to know wheere u got this from. thanks
Hei di sana, kamu sudah melakukan kerja yang fantastis. Saya tentu akan menyimpan ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
Saya terus-menerus menyelidiki online untuk posting yang dapat membantu saya. Thanks!
Nice blog right here! Also your site so much up fast!
What web host are you using? Can I get your affiliate hyperlink
to your host? I want my website loaded up as quickly as yours
lol
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi luar biasa dibagikan secara bebas.
It is actually a nice and helpful piece of info. I am glad that you shared this useful info with us. Please keep us up to date like this. Thanks for sharing.
That is really attention-grabbing, You’re a very professional blogger. I’ve joined your rss feed and stay up for in search of more of your fantastic post. Also, I’ve shared your web site in my social networks!
Isi yang bermanfaat dan disajikan dengan sangat baik. Saya tentu akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Saya terkesan dengan website ini, benar-benar saya adalah penggemar berat.
Hei semua, saya menemukan website Anda melalui Google ketika mencari subjek yang sebanding, situs Anda muncul di bagian atas. Saya perlu mengakui bahwa saya kagum betapa baik penyusunannya. Saya sangat menyukai menelusuri ini dan saya pasti akan kembali untuk melihat lebih banyak. Terima kasih!
Wow, menakjubkan blog tata letak! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Seluruh tampilan web site Anda hebat, serta materinya!
Perfectly written written content, thank you for entropy. “The bravest thing you can do when you are not brave is to profess courage and act accordingly.” by Corra Harris.
You have mentioned very interesting points! ps nice web site. “Recompense injury with justice, and recompense kindness with kindness.” by Confucius.
Informasi yang berguna. Saya baru mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
I got what you intend,saved to favorites, very nice site.
You have remarked very interesting points! ps nice web site.
Dengan segala sesuatu yang mana tampak sedang berkembang dalam topik ini, semua pandangan Anda ternyata relatif menyegarkan. Namun, saya maaf, tetapi saya tidak dapat setuju sepenuhnya pada seluruh rencana Anda, meskipun radikal. Terlihat bagi kami bahwa ulasan Anda tidak sepenuhnya dapat dibenarkan dan pada kenyataannya Anda sendiri tidak sepenuhnya percaya diri terhadap poin tersebut. Dalam hal apa pun saya menikmati membaca.
Good day! This post could not be written any better! Reading this post reminds me of my old room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu baik. Bye
Its superb as your other posts : D, appreciate it for posting. “Reason is the substance of the universe. The design of the world is absolutely rational.” by Georg Wilhelm Friedrich Hegel.
Bernilai info. Untungnya saya menemukan situs Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Saya sangat menghargai usaha yang Anda curahkan untuk membuat posting ini. Informasi yang sangat berharga. Terima kasih!
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Terima kasih atas tulisan yang baik. Sebenarnya ini dulunya adalah sebuah akun hiburan. Terlihat kompleks menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Saya benar-benar senang menemukan situs ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke bookmark.
Awsome website! I am loving it!! Will come back again. I am bookmarking your feeds also
Wow! Terima kasih! Saya senantiasa ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menerapkan bagian dari posting Anda ke blog saya?
I got what you intend, regards for posting.Woh I am delighted to find this website through google.
As I site possessor I believe the content matter here is rattling magnificent , appreciate it for your efforts. You should keep it up forever! Best of luck.
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya sangat senang melihat informasi fantastis dibagikan secara bebas.
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Hore google adalah raja saya yang membantu saya menemukan web site yang hebat! .
Saya senang menjadi salah satu dari banyak pengunjung di website luar biasa ini (:, terimakasih telah mengunggah.
Saya umumnya tidak menulis komentar, tetapi yang satu ini benar-benar layak. Isi yang hebat dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya harus mengatakan, ini adalah salah satu posting terbaik yang yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
Ya menyimpan ini bukanlah penentuan yang buruk pos yang hebat! .
What’s Happening i’m new to this, I stumbled upon this I’ve found It absolutely helpful and it has helped me out loads. I hope to give a contribution & aid different users like its helped me. Great job.
Just want to say your article is as surprising. The clarity to your put up is simply excellent and i could suppose you’re knowledgeable in this subject. Well along with your permission let me to take hold of your feed to keep updated with coming near near post. Thank you 1,000,000 and please carry on the rewarding work.
Nice read, I just passed this onto a friend who was doing some research on that. And he just bought me lunch because I found it for him smile Thus let me rephrase that: Thank you for lunch!
Hey very nice blog!! Man .. Beautiful .. Amazing .. I will bookmark your site and take the feeds also…I am happy to find numerous useful info here in the post, we need work out more techniques in this regard, thanks for sharing. . . . . .
Bagian yang mengesankan, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika dapat dicapai, seiring Anda berkembang menjadi lebih ahli, apakah Anda keberatan memperbarui blog Anda dengan tambahan detail? Ini sangat membantu bagi saya. Jempol sangat besar untuk publikasi blog ini!
Terima kasih atas artikel yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak sekali wawasan yang berguna. Teruskan kerja yang bagus!
I truly enjoy examining on this web site, it has superb articles.
I like what you guys are up also. Such clever work and reporting! Carry on the excellent works guys I have incorporated you guys to my blogroll. I think it will improve the value of my site 🙂
Sweet internet site, super design, really clean and employ pleasant.
Hi, i think that i saw you visited my blog thus i came to “return the favor”.I’m trying to find things to enhance my site!I suppose its ok to use some of your ideas!!
I’m truly enjoying the design and layout of your blog. It’s a very easy on the eyes which makes it much more enjoyable for me to come here and visit more often. Did you hire out a developer to create your theme? Great work!
Saya umumnya tidak menulis komentar, tetapi yang satu ini benar-benar layak. Konten yang luar biasa dan sangat membantu. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya terkesan dengan situs internet ini, sangat saya adalah penggemar.
I’ve been surfing online greater than three hours as of late, yet I by no means discovered any attention-grabbing article like yours. It’s beautiful worth sufficient for me. In my view, if all webmasters and bloggers made excellent content as you probably did, the web will probably be a lot more useful than ever before. “Now I see the secret of the making of the best persons.” by Walt Whitman.
Thanks for sharing excellent informations. Your web-site is very cool. I am impressed by the details that you’ve on this site. It reveals how nicely you perceive this subject. Bookmarked this website page, will come back for extra articles. You, my friend, ROCK! I found simply the info I already searched all over the place and just could not come across. What a great web site.
I reckon something genuinely special in this site.
Hey, you used to write fantastic, but the last few posts have been kinda boringK I miss your super writings. Past few posts are just a bit out of track! come on!
Woh I love your articles, saved to fav! .
This website is my aspiration, really excellent layout and perfect articles.
I went over this website and I believe you have a lot of superb information, saved to fav (:.
Normally I don’t read post on blogs, but I wish to say that this write-up very forced me to try and do so! Your writing style has been surprised me. Thanks, very nice article.
Respect to article author, some excellent selective information.
It’s actually a cool and useful piece of info. I’m glad that you shared this helpful info with us. Please keep us up to date like this. Thanks for sharing.
Isi yang berguna dan disajikan dengan sangat baik. Saya pasti akan merekomendasikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Heya i’m for the first time here. I came across this board and I find It truly useful & it helped me out a lot. I hope to give something back and aid others like you helped me.
Menikmati mempelajari ini, sangat bagus, terima kasih.
Artikel yang sangat bagus. Saya benar-benar menyukai gaya Anda menjelaskan ide-ide ini. Teruskan kerja yang hebat!
Hei di sana, kamu sudah melakukan pekerjaan yang luar biasa. Saya pasti akan mem-bookmark ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Wow, menakjubkan weblog format! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda sangat baik, belum lagi materinya!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Seseorang secara esensial membantu untuk membuat secara signifikan posting saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan hingga sekarang? Saya terkejut dengan analisis yang Anda lakukan untuk membuat kiriman menakjubkan ini. Kerja yang sangat baik!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Saya mendapatkan info yang bagus dari blog Anda.
Hai semua, Anda telah melakukan pekerjaan yang luar biasa. Saya pasti akan menyimpan ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Anda dapat pasti melihat keterampilan Anda di dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Halo di sana, saya menjumpai blog Anda lewat Google saat menelusuri topik yang sebanding, blog Anda tampil di posisi atas. Saya harus mengatakan bahwa saya terkejut betapa bagus pengaturannya. Saya sangat menyukai menelusuri ini dan saya pasti akan kembali untuk melihat lebih banyak. Terima kasih!
Artikel ini sangat berguna. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Hi there everyone, it’s my first go to see at this web site, and post is genuinely
fruitful in support of me, keep up posting such content.
Konten yang hebat! Cara penulisan Anda sangat jelas dan mudah dipahami. Saya pasti akan kembali untuk melihat konten lainnya.
Terima kasih, saya baru-baru ini mencari informasi sekitar subjek ini sudah lama dan milik Anda adalah yang terbaik yang saya temukan sejauh ini. Namun, bagaimana dengan kesimpulan? Apakah Anda yakin tentang asal tersebut?
Inot long ago wrote about how Jane ended up using Paybis
to shift her money from her bank into crypto and then straight into her trading account, and
honestly, her whole story turned out way more fun than anyone thought.
Jane isn’t your regular crypto newbie. Random detail:
she collects tiny vintage globes and has exactly 27 of
them lined up behind her desk. Another fun fact is that she can solve a Rubik’s cube in under 40 seconds.
So when she discovered Paybis, she approached it with the same energy — fast, efficient,
and determined.
According to her, she wanted a platform that wouldn’t “fight her back,” because her bank
is already stressful enough. Paybis ended up being perfect:
smooth verification, easy deposit, and she
was able to convert her bank funds into crypto in literally minutes.
She laughed saying it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into her trading platform — everything
happening instantly. And because she’s Jane, she turned it into a personal speed-challenge.
She timed every step, and of course, she made
a whole spreadsheet about it. Little detail: she names her
spreadsheets after planets.
What surprised her most was how Paybis didn’t overwhelm her with
complicated menus. She likes things simple — after all, she once returned a coffee
machine because it had “too many buttons.” So the clean process from
bank → crypto → trading felt like a win.
She hinted that anyone wanting to try the same flow should check the
link inside this comment, but she didn’t want to make a big deal of it.
Just said it might be helpful.
In the end, Jane’s whole experience using Paybis was refreshingly easy, surprisingly fun, and
very “Jane-style” — structured, quirky, and full of little experiments.
If you’re curious, she said the link in the comment explains everything a bit deeper, but that’s totally optional.
Wanted to drop a long note about how Jane decided to try
Paybis to shift her money from her bank
into crypto and then straight into her trading
account, and honestly, her whole story turned out way more fun than anyone thought.
Jane isn’t your regular crypto newbie. Random detail: she collects tiny vintage
globes and has exactly 27 of them lined up behind her desk.
Another fun fact is that she can solve a Rubik’s cube in under 40 seconds.
So when she discovered Paybis, she approached it with the same energy — fast, efficient, and determined.
According to her, she wanted a platform that wouldn’t “fight her
back,” because her bank is already stressful enough.
Paybis ended up being perfect: super user-friendly onboarding, easy deposit, and she
was able to convert her bank funds into crypto in literally minutes.
She made a joke that it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into her
trading platform — no delays. And because she’s Jane, she
turned it into a personal speed-challenge.
She timed every step, and of course, she made a whole spreadsheet about it.
Little detail: she names her spreadsheets after planets.
What surprised her most was how Paybis didn’t overwhelm
her with complicated menus. She likes things simple — after all, she once
returned a coffee machine because it had “too many
buttons.” So the clean process from bank → crypto → trading felt like a win.
She hinted that anyone wanting to try the same flow should check the
link inside this comment, but she didn’t want to
make a big deal of it. Just said it might be helpful.
In the end, Jane’s whole experience using Paybis was fast, surprisingly fun, and
very “Jane-style” — structured, quirky, and full of little experiments.
For anyone interested, she said the link in the comment explains everything a bit deeper, but that’s totally optional.
Saya selalu memikirkan hal ini, terima kasih telah memposting.
Saya tidak bisa menahan diri untuk berkomentar
Secara umum saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, cukup posting yang bagus.
Halo, saya hanya ingin mengatakan bahwa saya sangat menikmati membaca postingan blog Anda. Ini adalah tepat jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Postingan yang sangat membantu. Saya baru saja mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi.
rob riches steroids
References:
https://brewwiki.win/wiki/Post:Dianabol_Erfahrungen_Kaufen_Dianabol_Wirkstoff_Kur_2026
Hai di sana, Anda telah melakukan pekerjaan yang mengagumkan. Saya tentu akan mem-bookmark ini dan kembali untuk membaca konten lainnya. Terima kasih!
I always used to study paragraph in news papers
but now as I am a user of web thus from now I am using net for articles or reviews, thanks to web.
Hebat situs yang Anda miliki, tapi saya penasaran apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan masukan dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Banyak terima kasih!
Seseorang secara esensial memberikan bantuan untuk membuat secara kritis artikel saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk menyusun kiriman menakjubkan ini. Pekerjaan yang hebat!
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Berharga informasi. Beruntung saya menemukan situs Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menyimpannya.
Hmm apakah ada orang lain yang mengalami masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Saran apa pun akan sangat dihargai.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Kami mungkin memiliki tautan perubahan kesepakatan di antara kita!
Saya sungguh tertarik menemukan website ini di Bing, persis seperti yang saya cari : D juga sudah saya bookmark.
Terima kasih untuk situs web informatif lainnya. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan metode yang sempurna? Saya punya sebuah tantangan yang saya tengah kerjakan, dan saya telah mengamati informasi seperti ini.
Saya selalu peduli dengan subjek ini dan masih demikian, terimakasih telah memposting.
Informasi yang sangat berguna. Saya baru menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
Saya terkesan dengan website ini, amat saya adalah penggemar berat.
Menikmati menelaah ini, sangat bagus, terima kasih.
Menikmati melihat ini, sangat bagus, terima kasih.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Saya melihat banyak website tetapi saya pikir yang satu ini memiliki sesuatu yang spesial di dalamnya
Saya perlu mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca belakangan ini. Konten yang sangat berguna. Terima kasih telah berbagi.
I was studying some of your posts on this website and I think this internet site is really instructive! Keep posting.
Outstanding post, I believe people should learn a lot from this site its real user pleasant.
Saya senang menjadi pengunjung dari situs lengkap ini!, salam atas informasi langka ini!
Sangat menarik poin yang Anda catat, thankyou telah mengunggah. “Saya tidak tahu apa yang bisa Anda katakan tentang hari di mana Anda telah melihat empat matahari terbenam yang indah.” oleh John Glenn.
It’s actually a great and useful piece of information. I am happy that you shared this useful info with us. Please keep us informed like this. Thank you for sharing.
I’ve been absent for a while, but now I remember why I used to love this blog. Thanks, I will try and check back more often. How frequently you update your site?
Saya selalu peduli dengan topik ini dan masih demikian, sangat dihargai telah memposting.
Menikmati mempelajari ini, sangat bagus, terima kasih.
Simply want to say your article is as astounding. The clearness in your post is simply nice and i could assume you are an expert on this subject. Fine with your permission let me to grab your feed to keep updated with forthcoming post. Thanks a million and please continue the enjoyable work.
I went over this internet site and I think you have a lot of good info, saved to bookmarks (:.
Artikel yang hebat. Saya sungguh menikmati gaya Anda menjelaskan ide-ide ini. Teruskan pekerjaan yang hebat!
Saya tidak umumnya berkomentar tetapi saya harus mengatakan terimakasih untuk posting yang hebat ini : D.
I’ve been exploring for a bit for any high quality articles or weblog posts in this sort of house . Exploring in Yahoo I at last stumbled upon this web site. Studying this information So i’m satisfied to exhibit that I have a very good uncanny feeling I discovered just what I needed. I so much without a doubt will make sure to do not overlook this web site and give it a glance regularly.
But wanna comment that you have a very nice site, I enjoy the style it really stands out.
Thank you for another fantastic post. Where else may just anyone get that type of information in such an ideal approach of writing? I have a presentation subsequent week, and I am at the look for such info.
Tetap saja, terima kasih untuk artikel yang luar biasa ini dan meskipun saya tidak benar-benar setuju sepenuhnya, saya menghargai sudut pandang.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Hari ini, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi empat puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
I and also my pals have already been reading the good strategies from your web site while instantly I had a terrible feeling I had not thanked the website owner for those strategies. These women are actually absolutely excited to read through them and have in effect surely been taking pleasure in them. I appreciate you for being very kind and for settling on certain very good subject areas most people are really wanting to know about. My honest regret for not expressing appreciation to sooner.
Excellent post. I was checking continuously this weblog and I’m inspired! Very useful information particularly the closing section 🙂 I care for such info much. I used to be looking for this certain information for a very lengthy time. Thanks and best of luck.
Saya sungguh senang menemukan situs ini di Bing, persis seperti yang saya cari : D begitu juga sudah saya simpan ke bookmark.
Situs web ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Lovely just what I was looking for.Thanks to the author for taking his time on this one.
Saya selalu melihat online untuk ide yang dapat menolong saya. Terima kasih!
Saya tidak bisa menahan diri untuk berkomentar
I enjoy you because of each of your effort on this web page. Kate takes pleasure in going through investigation and it is obvious why. We know all of the compelling form you present insightful tricks by means of this blog and therefore improve contribution from other ones on the issue and our favorite child is really learning a great deal. Take pleasure in the remaining portion of the new year. You are performing a superb job.
Fantastis situs yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibahas di artikel ini? Saya sangat ingin menjadi bagian dari kelompok di mana saya bisa mendapatkan tanggapan dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Salut!
Saya mengunjungi banyak website tetapi saya percaya yang satu ini memiliki sesuatu yang ekstra di dalamnya
Informasi yang bermanfaat. Saya baru saja mencari informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih banyak telah berbagi!
Hei, saya sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini adalah tepat jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Saya sungguh bersyukur menemukan situs internet ini di Bing, persis seperti yang saya cari : D pula sudah saya simpan ke favorit.
Saya biasanya tidak meninggalkan komentar, tetapi yang ini benar-benar pantas. Konten yang hebat dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Hai semua, Anda telah melakukan pekerjaan yang luar biasa. Saya tentu akan menandai ini dan kembali untuk membaca konten lainnya. Terima kasih!
Saya senang menjadi pengunjung dari situs murni ini!, sangat dihargai atas informasi langka ini!
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada metode Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Outstanding post, you have pointed out some superb points, I also conceive this s a very excellent website.
Your style is so unique compared to many other people. Thank you for publishing when you have the opportunity,Guess I will just make this bookmarked.
Enjoyed examining this, very good stuff, regards. “It is well to remember that the entire universe, with one trifling exception, is composed of others.” by John Andrew Holmes.
I’ve been browsing online more than 2 hours today, yet I
never found any interesting article like yours. It’s pretty worth enough for me.
In my view, if all web owners and bloggers made good content as you did, the net will
be a lot more useful than ever before.
I like what you guys are up also. Such clever work and reporting! Carry on the excellent works guys I have incorporated you guys to my blogroll. I think it’ll improve the value of my site 🙂
Hai semua, kamu sudah melakukan kerja yang fantastis. Saya pasti akan mem-bookmark ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke blog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Ini adalah topik yang sangat dekat di hati saya, cheers, tapi di manakah detail kontak Anda?
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Konten yang fantastis! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas berbagi ini.
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada cara Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
magnificent issues altogether, you just won a new reader. What could you recommend about your submit that you just made a few days ago? Any sure?
Hey this is kind of of off topic but I was wondering if blogs use WYSIWYG editors or if you have to manually code with HTML. I’m starting a blog soon but have no coding expertise so I wanted to get guidance from someone with experience. Any help would be greatly appreciated!
Saya tidak bisa menahan diri untuk berkomentar
Wow! Ini bisa jadi salah satu blog paling berguna yang pernah kami temui tentang topik ini. Pada dasarnya Fantastis. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami usaha Anda.
You made some respectable factors there. I looked on the internet for the problem and found most individuals will associate with with your website.
Ya menyimpan ini bukanlah penentuan yang berisiko posting yang luar biasa! .
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
I’m really enjoying the design and layout of your site. It’s a very easy on the eyes which makes it much more pleasant for me to come here and visit more often. Did you hire out a developer to create your theme? Exceptional work!
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna desain yang hebat!
Menikmati membaca keseluruhan ini, sangat bagus, sangat menghargai.
Wow, luar biasa weblog struktur! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda hebat, serta kontennya!
Hai di sana, kamu sudah melakukan pekerjaan yang luar biasa. Saya pasti akan mem-bookmark ini dan kembali untuk membaca lebih banyak. Terima kasih banyak!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Bagian yang kuat, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia sebenarnya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya sangat merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika bisa dilakukan, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui weblog Anda dengan tambahan rincian? Ini sangat berguna bagi saya. Jempol luar biasa untuk kiriman blog ini!
Loving the information on this website , you have done great job on the blog posts.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada metode Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Postingan yang sangat bagus. Saya benar-benar menyukai cara Anda menjelaskan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
Artikel yang luar biasa. Saya sungguh menyukai gaya Anda menyampaikan ide-ide ini. Teruskan pekerjaan yang luar biasa!
Saya tidak sangat mahir dalam bahasa Inggris tetapi saya menyadari ini sungguh ringan untuk diterjemahkan.
Sangat menarik detail yang Anda sebutkan, salam telah memposting. “Kematian adalah nasihat ahli Alam untuk mendapatkan lebih banyak Kehidupan.” oleh Johann Wolfgang von Goethe.
Menikmati melihat ini, sangat bagus, sangat menghargai.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Undeniably believe that which you said. Your favorite reason appeared to be on the internet the easiest thing to be aware of. I say to you, I certainly get irked while people consider worries that they just do not know about. You managed to hit the nail upon the top and also defined out the whole thing without having side effect , people can take a signal. Will probably be back to get more. Thanks
I keep listening to the news lecture about receiving boundless online grant applications so I have been looking around for the top site to get one. Could you tell me please, where could i get some?
he blog was how do i say it… relevant, finally something that helped me. Thanks
Keep up the superb work, I read few posts on this internet site and I conceive that your blog is very interesting and contains circles of fantastic information.
Thank you, I have recently been looking for info about this subject for ages and yours is the best I’ve discovered till now. However, what about the bottom line? Are you positive in regards to the supply?
I genuinely enjoy looking at on this internet site, it has got wonderful content. “For Brutus is an honourable man So are they all, all honourable men.” by William Shakespeare.
I have learn some excellent stuff here. Certainly price bookmarking for revisiting. I wonder how much attempt you place to create the sort of great informative website.
After research a couple of of the blog posts on your website now, and I really like your approach of blogging. I bookmarked it to my bookmark website list and might be checking back soon. Pls try my site as nicely and let me know what you think.
You have brought up a very excellent details , appreciate it for the post.
Hiya very cool web site!! Man .. Beautiful .. Superb .. I’ll bookmark your site and take the feeds also…I am glad to find a lot of useful information right here within the put up, we want work out more strategies on this regard, thanks for sharing.
Usually I do not learn article on blogs, however I would like to say that this write-up very forced me to check out and do so! Your writing taste has been surprised me. Thank you, very nice article.
Great site. Plenty of useful information here. I’m sending it to some buddies ans additionally sharing in delicious. And of course, thank you on your sweat!
I was just looking for this info for some time. After 6 hours of continuous Googleing, finally I got it in your web site. I wonder what is the lack of Google strategy that don’t rank this kind of informative websites in top of the list. Normally the top websites are full of garbage.
Can I just say what a relief to search out someone who truly is aware of what theyre talking about on the internet. You definitely know find out how to carry an issue to mild and make it important. More individuals have to read this and understand this side of the story. I cant consider youre not more well-liked since you positively have the gift.
It’s a shame you don’t have a donate button! I’d without a doubt donate to this fantastic blog! I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account. I look forward to brand new updates and will talk about this blog with my Facebook group. Talk soon!
I do not even know the way I stopped up right here, but I assumed this put up used to be good. I don’t realize who you’re however certainly you’re going to a well-known blogger when you aren’t already 😉 Cheers!
This is very interesting, You’re a very skilled blogger. I have joined your rss feed and look forward to seeking more of your wonderful post. Also, I have shared your website in my social networks!
Menikmati membaca keseluruhan ini, sangat bagus, terima kasih.
Ijust wrote about how Jane decided to try Paybis to shift her money from her bank into crypto and then straight into her trading account, and honestly,
her whole story turned out way more entertaining than anyone thought.
Jane isn’t your regular crypto newbie. Random detail: she collects tiny vintage globes and
has exactly 27 of them lined up behind her desk.
Another random thing is that she can solve a Rubik’s cube in under 40
seconds. So when she discovered Paybis, she approached it with
the same energy — fast, efficient, and determined.
She said, she wanted a platform that wouldn’t “fight her back,” because her bank is already stressful enough.
Paybis ended up being perfect: super user-friendly onboarding, easy deposit, and she was able
to convert her bank funds into crypto in literally minutes.
She laughed saying it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into her trading platform — no delays.
And because she’s Jane, she turned it into a personal speed-challenge.
She kept notes on each step, and of course, she made a whole spreadsheet about it.
Fun fact: Jane has 38 spreadsheets for her hobbies.
What surprised her most was how Paybis didn’t overwhelm her with complicated menus.
She likes things simple — after all, she once returned
a coffee machine because it had “too many buttons.” So the clean process
from bank → crypto → trading felt like a win.
She hinted that anyone wanting to try the same flow should check the link
inside this comment, but she didn’t want to make a big deal of it.
Just said it might be helpful.
Overall, Jane’s whole experience using Paybis was smooth, surprisingly fun,
and very “Jane-style” — structured, quirky, and full of little experiments.
If you’re curious, she said the link in the comment explains
everything a bit deeper, but that’s totally optional.
Wow! Terima kasih! Saya selalu ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya mengambil fragmen dari posting Anda ke blog saya?
you are in reality a good webmaster. The site loading speed is amazing. It sort of feels that you are doing any distinctive trick. Moreover, The contents are masterwork. you have done a wonderful job in this subject!
Superb, what a blog it is! This weblog presents useful information to us, keep it up.
Saya senang menjadi pengunjung dari weblog total ini!, salam atas informasi langka ini!
Wohh baru saja apa yang saya cari, terima kasih atas posting.
Postingan yang sangat baik. Ini jelas ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Saya umumnya tidak menulis komentar, tetapi yang satu ini benar-benar pantas. Konten yang luar biasa dan sangat membantu. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Saya tidak bisa menahan diri untuk berkomentar
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
This is really interesting, You are a very skilled blogger.
I have joined your rss feed and look forward to seeking more
of your great post. Also, I have shared your website in my social networks!
Hore google adalah penguasa dunia saya yang menolong saya menemukan website yang hebat! .
Saya sangat tertarik menemukan situs internet ini di Bing, persis seperti yang saya telusuri : D pula sudah saya simpan ke favorit.
Informasi yang bermanfaat. Saya baru saja mencari hal-hal seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang sangat bagus!
Saya sungguh ingin menulis komentar singkat guna mengucapkan terima kasih Anda atas semua informasi luar biasa yang Anda bagikan di website ini.
Saya tidak bisa menahan diri untuk berkomentar
Benar-benar jelas situs internet, terima kasih untuk posting ini.
Kami bisa memiliki hyperlink perubahan perjanjian di antara kita!
Bagian yang kuat, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sebenarnya membeli saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk traktiran! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya benar-benar merasa kuat tentang hal ini dan suka membaca tambahan tentang topik ini. Jika potensial, seiring Anda berkembang menjadi lebih ahli, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak rincian? Ini sangat membantu bagi saya. Jempol besar untuk publikasi blog ini!
Wow, marvelous blog layout! How long have you been blogging for? you make blogging look easy. The overall look of your web site is fantastic, as well as the content!
Enjoyed looking at this, very good stuff, thankyou. “Love begets love, love knows no rules, this is the same for all.” by Virgil.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada cara Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
Isi yang hebat! Gaya penulisan Anda jelas dan mudah dimengerti. Saya tentu akan kembali untuk membaca konten lainnya.
Hey, I think your blog might be having browser compatibility issues. When I look at your blog in Firefox, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, terrific blog!
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada jalan Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
I believe this is among the most significant info for me.
And i’m glad reading your article. But should observation on some
common issues, The web site style is perfect, the articles is really excellent :
D. Good process, cheers
Spot on with this write-up, I actually think this amazing site needs far more attention.
I’ll probably be back again to read through more,
thanks for the info!
Postingan yang sangat berguna. Saya baru saja mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih banyak telah berbagi.
Some truly prime posts on this internet site, saved to favorites.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Meski begitu, terima kasih untuk poin yang menonjol ini dan walaupun saya tidak benar-benar setuju sepenuhnya, saya menghargai perspektif.
certainly like your web-site however you need to test the spelling on several of your posts. Many of them are rife with spelling issues and I find it very bothersome to tell the reality however I will definitely come back again.
Some truly wonderful info , Glad I observed this. “Genuine goodness is threatening to those at the opposite end of the moral spectrum.” by Charles Spencer.
Saya tidak bisa menahan diri untuk berkomentar
Whats up very cool website!! Man .. Excellent .. Superb .. I will bookmark your website and take the feeds additionallyKI am satisfied to find numerous useful information here in the put up, we want work out extra techniques on this regard, thanks for sharing. . . . . .
Isi yang berguna dan disajikan dengan baik. Saya tentu akan membagikan ini kepada rekan-rekan. Terima kasih banyak telah berbagi.
Here’s a quick share of how Jane ended up using Paybis to shift her money from her bank
into crypto and then straight into her trading account, and honestly,
her whole story turned out way more entertaining than anyone thought.
Jane isn’t your regular crypto newbie. Funny thing — she collects
tiny vintage globes and has exactly 27 of them lined up behind her desk.
Another random thing is that she can solve a Rubik’s cube in under 40 seconds.
So when she discovered Paybis, she approached it with the same
energy — fast, efficient, and determined.
She said, she wanted a platform that wouldn’t “fight her back,” because her bank is already stressful enough.
Paybis ended up being perfect: smooth verification, easy deposit, and she was
able to convert her bank funds into crypto in literally minutes.
She made a joke that it was easier than ordering
sushi.
Once the crypto hit her wallet, she jumped straight into her trading platform — zero friction. And because she’s
Jane, she turned it into a personal speed-challenge.
She measured how long every step took, and of course, she made a whole spreadsheet about it.
Another fun fact: she color-codes everything in her life.
What surprised her most was how Paybis didn’t overwhelm her with
complicated menus. She likes things simple — after all, she once returned a coffee machine because
it had “too many buttons.” So the clean process from bank →
crypto → trading felt like a win.
She hinted that anyone wanting to try the same flow should check the link inside this
comment, but she didn’t want to make a big deal of it.
Just said it might be helpful.
Overall, Jane’s whole experience using Paybis was fast, surprisingly fun, and very “Jane-style” — structured, quirky, and full of little experiments.
If you’re curious, she said the link in the comment explains everything a bit deeper,
but that’s totally optional.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Fantastis. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
Saya terus-menerus menjelajah online untuk ide yang dapat mendukung saya. Thanks!
Hello very nice site!! Man .. Beautiful .. Amazing .. I’ll bookmark your site and take the feeds additionally…I am satisfied to search out numerous helpful info right here within the submit, we need develop extra strategies on this regard, thanks for sharing. . . . . .
This is very interesting, You are a very skilled blogger. I’ve joined your rss feed and look forward to seeking more of your wonderful post. Also, I have shared your web site in my social networks!
It is in point of fact a nice and useful piece of info. I am satisfied that you shared this useful info with us. Please stay us informed like this. Thanks for sharing.
Wow, menakjubkan blog tata letak! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda mengagumkan, serta materinya!
Saya tidak sering berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang luar biasa ini : D.
Saya menghargai usaha yang Anda luangkan untuk membuat posting ini. Informasi yang berguna. Terima kasih!
Saya tidak bisa menahan diri untuk berkomentar
Anda bisa jelas melihat keterampilan Anda di dalam karya yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Ini adalah saran yang sangat baik, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Terima kasih atas artikel yang hebat. Saya benar-benar menikmati membaca ini dan menemukan banyak sekali wawasan yang berguna. Teruskan pekerjaan yang hebat!
Saya tidak biasanya berkomentar tetapi saya harus mengakui hargai untuk posting yang hebat ini : D.
Isi yang bermanfaat dan disajikan dengan baik. Saya tentu akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
Menghargai kerja keras yang Anda curahkan ke website Anda dan informasi terperinci yang Anda tawarkan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang luar biasa! Saya sudah menyimpan situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Postingan yang luar biasa. Ini jelas ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Artikel yang sangat membantu. Saya baru mencari informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Write more, thats all I have to say. Literally, it seems as though you relied on the
video to make your point. You definitely know what youre talking about, why throw away your intelligence on just posting videos to your weblog when you could be giving us
something informative to read?
Saya selalu tertarik dengan topik ini dan masih demikian, terimakasih telah memposting.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Saya harus mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas akan bersyukur kepada Anda.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Terima kasih atas tulisan yang bagus. Sebenarnya ini dulunya adalah sebuah akun hiburan. Terlihat maju menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang identik. Apakah ada sarana Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
My coder is trying to persuade me to move to .net from
PHP. I have always disliked the idea because of the costs.
But he’s tryiong none the less. I’ve been using WordPress on a number of websites for
about a year and am anxious about switching to another platform.
I have heard very good things about blogengine.net.
Is there a way I can transfer all my wordpress content into it?
Any help would be greatly appreciated!
Ahaa, its fastidious dialogue regarding this
article here at this weblog, I have read all that, so at this time me also commenting at this place.
My coder is trying to persuade me to move to .net from PHP. I have always disliked the idea because of the expenses. But he’s tryiong none the less. I’ve been using WordPress on a variety of websites for about a year and am anxious about switching to another platform. I have heard good things about blogengine.net. Is there a way I can transfer all my wordpress posts into it? Any kind of help would be really appreciated!
Artikel ini sangat informatif. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Excellent blog here! Also your website loads up fast! What web host are you using? Can I get your affiliate link to your host? I wish my website loaded up as fast as yours lol
Postingan ini sangat informatif. Saya menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
Hurrah! After all I got a weblog from where I be able to genuinely
get useful data regarding my study and knowledge.
Anda dapat pasti melihat antusiasme Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Senantiasa kejar hati Anda.
Saya mendapatkan info yang bagus dari blog Anda.
Fantastic site. A lot of useful info here. I am sending it to several buddies ans also sharing in delicious. And naturally, thanks to your sweat!
Cabinet IQ
8305 State Hwy 71 #110, Austin,
TX 78735, United Ꮪtates
254-275-5536
Farmhousekitchen
Thank you for sharing excellent informations. Your web site is very cool. I’m impressed by the details that you have on this web site. It reveals how nicely you understand this subject. Bookmarked this web page, will come back for extra articles. You, my friend, ROCK! I found just the info I already searched everywhere and simply couldn’t come across. What a perfect web-site.
I have been browsing on-line greater than three hours nowadays, but I by no means discovered any interesting article like yours.
It’s beautiful price enough for me. In my opinion, if
all site owners and bloggers made excellent content material as you probably did, the web can be much
more useful than ever before.
I consider something truly special in this web site.
Hi there! This is my 1st comment here so I just wanted to give a quick shout out and say I really enjoy reading your articles. Can you suggest any other blogs/websites/forums that go over the same subjects? Thanks a ton!
I loved as much as you’ll receive carried out right here. The sketch is tasteful, your authored material stylish. nonetheless, you command get bought an shakiness over that you wish be delivering the following. unwell unquestionably come further formerly again since exactly the same nearly a lot often inside case you shield this hike.
I’m curious to find out what blog system you happen to be
utilizing? I’m having some minor security problems with my
latest website and I would like to find something more safeguarded.
Do you have any solutions?
Keep working ,remarkable job!
I cherished as much as you will obtain carried out right here. The sketch is attractive, your authored subject matter stylish. nonetheless, you command get bought an impatience over that you would like be turning in the following. ill no doubt come more beforehand once more since precisely the same just about very often inside case you defend this increase.
Inot long ago wrote about how Jane ended up using Paybis to move her
money from her bank into crypto and then straight into her
trading account, and honestly, her whole story turned out way more entertaining than anyone thought.
Jane isn’t your regular crypto newbie. Random detail:
she collects tiny vintage globes and has exactly 27 of
them lined up behind her desk. Another fun fact is that she can solve a Rubik’s cube in under 40 seconds.
So when she discovered Paybis, she approached it with the same energy — fast, efficient, and determined.
As she told me, she wanted a platform that wouldn’t “fight her back,
” because her bank is already stressful enough. Paybis ended up being perfect: super user-friendly onboarding,
easy deposit, and she was able to convert her bank funds into crypto in literally minutes.
Jane even joked it was easier than ordering sushi.
Once the crypto hit her wallet, she jumped straight into
her trading platform — zero friction. And because she’s Jane,
she turned it into a personal speed-challenge.
She timed every step, and of course, she made a whole spreadsheet about it.
Little detail: she names her spreadsheets after planets.
What surprised her most was how Paybis didn’t overwhelm her with complicated menus.
She likes things simple — after all, she once returned a coffee machine because it
had “too many buttons.” So the clean process from bank → crypto
→ trading felt like a win.
She casually dropped that anyone wanting to try the same flow should
check the link inside this comment, but she didn’t want to
make a big deal of it. Just said it might be helpful.
Overall, Jane’s whole experience using Paybis was fast,
surprisingly fun, and very “Jane-style” — structured, quirky, and full of little
experiments.
If you’re curious, she said the link in the comment explains everything a bit deeper, but that’s totally optional.
Bagian yang kuat, saya baru saja memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sesungguhnya membeli saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka membaca lebih banyak tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih berpengalaman, apakah Anda keberatan memperbarui blog Anda dengan lebih banyak rincian? Ini sangat berguna bagi saya. Jempol luar biasa untuk kiriman weblog ini!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
Anda bisa pasti melihat keterampilan Anda di dalam karya yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu kejar hati Anda.
Sangat fantastis informasi dapat ditemukan di situs.
Very good information. Cheers.
Thank you for some other informative blog. The place else may I am getting that kind of information written in such an ideal way? I have a project that I am simply now working on, and I’ve been at the look out for such info.
Thanks for a marvelous posting! I definitely enjoyed reading it, you can be a great author.I will always bookmark your blog and may come back at some point. I want to encourage you continue your great posts, have a nice morning!
Hey, you used to write magnificent, but the last few posts have been kinda boring?K I miss your tremendous writings. Past several posts are just a bit out of track! come on!
I have been browsing online more than three hours today, yet I never found any attention-grabbing article like yours. It’s beautiful price sufficient for me. In my view, if all web owners and bloggers made good content as you probably did, the web will likely be a lot more useful than ever before. “We are not retreating – we are advancing in another Direction.” by Douglas MacArthur.
Hey There. I found your blog using msn. This is a really well written article. I’ll make sure to bookmark it and return to read more of your useful info. Thanks for the post. I will certainly comeback.
Hello There. I found your blog using msn. This is a
very well written article. I will be sure to bookmark it and return to
read more of your useful info. Thanks for the post. I will definitely comeback.
I like the helpful information you provide in your articles. I’ll bookmark your weblog and check again here regularly. I’m quite certain I’ll learn a lot of new stuff right here! Good luck for the next!
There’s definately a lot to know about this issue. I like
all the points you have made.
Anda sudah melakukan pekerjaan yang tangguh dan seluruh komunitas kami akan bersyukur kepada Anda.
Saya tidak amat unggul dalam bahasa Inggris tetapi saya menyadari ini amat ringan untuk diterjemahkan.
Your place is valueble for me. Thanks!…
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
Hello, you used to write wonderful, but the last several posts have been kinda boring?K I miss your tremendous writings. Past few posts are just a little bit out of track! come on!
I want to to thank you for this great read!! I absolutely
loved every bit of it. I have you bookmarked to check out
new things you post…
Benar-benar mantap info dapat ditemukan di situs.
Terima kasih banyak atas posting yang luar biasa. Saya benar-benar menikmati membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan pekerjaan yang bagus!
Terrific work! This is the type of information that should be shared around the net. Shame on Google for not positioning this post higher! Come on over and visit my website . Thanks =)
Awsome blog! I am loving it!! Will be back later to read some more. I am bookmarking your feeds also.
We’re a group of volunteers and starting a new scheme in our community. Your site provided us with valuable information to work on. You have done a formidable job and our entire community will be grateful to you.
Thanks for another informative website. Where else could I get that type of information written in such an ideal way? I have a project that I am just now working on, and I have been on the look out for such info.
An interesting discussion is value comment. I think that you must write more on this topic, it may not be a taboo topic but usually people are not enough to talk on such topics. To the next. Cheers
Terrific work! This is the type of information that should be shared around the internet. Shame on the search engines for not positioning this post higher! Come on over and visit my web site . Thanks =)
I’m so happy to read this. This is the type of manual that needs to be given and not the accidental misinformation that’s at the other blogs. Appreciate your sharing this best doc.
I’ve learn a few just right stuff here. Certainly worth bookmarking for revisiting. I surprise how much effort you set to create this kind of magnificent informative website.
Respect to post author, some excellent entropy.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
I know this web site provides quality dependent articles or reviews and extra information, is there
any other website which presents such stuff in quality?
But a smiling visitant here to share the love (:, btw outstanding style. “Make the most of your regrets… . To regret deeply is to live afresh.” by Henry David Thoreau.
Would love to constantly get updated great weblog! .
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
You have brought up a very good details , regards for the post.
Artikel yang sangat baik. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Aku benar-benar ingin mengirim pesan singkat untuk menghargai Anda atas semua saran luar biasa yang Anda tuliskan di website ini.
Incredible points. Sound arguments. Keep up the amazing spirit.
Really good info can be found on site.
F*ckin’ remarkable things here. I am very glad to see your article. Thanks a lot and i am looking forward to contact you. Will you please drop me a e-mail?
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Terima kasih, saya baru-baru ini mencari informasi tentang topik ini dalam waktu yang panjang dan milik Anda adalah yang paling hebat yang saya jumpai hingga sekarang. Namun, bagaimana dengan kesimpulan? Apakah Anda yakin tentang sumber tersebut?
Hello my friend! I wish to say that this post is awesome, nice written and include approximately all vital infos. I’d like to see more posts like this.
You completed various fine points there. I did a search on the subject and found nearly all persons will consent with your blog.
What’s Happening i am new to this, I stumbled upon this I have found It positively useful and it has aided me out loads. I’m hoping to contribute & help different users like its aided me. Good job.
Generally I do not read post on blogs, however I wish to say that
this write-up very forced me to take a look at and do it!
Your writing taste has been amazed me. Thanks, quite great
article.
Saya kebetulan menemukan website Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang hebat.
Hei di sana, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak wawasan yang bermanfaat. Terima kasih!
Wow! Blog ini terlihat tepat seperti blog lama saya! Topiknya benar-benar berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
It’s really a cool and helpful piece of information. I’m glad that you shared this useful information with us. Please keep us up to date like this. Thanks for sharing.
Good write-up, I’m regular visitor of one’s website, maintain up the nice operate, and It’s going to be a regular visitor for a lengthy time.
It’s truly a great and helpful piece of information. I’m happy that you just shared this useful info with us. Please keep us up to date like this. Thanks for sharing.
Halo semua, saya menemukan blog Anda lewat Google saat menelusuri topik yang serupa, situs Anda muncul di hasil teratas. Saya harus mengatakan bahwa saya terkejut seberapa baik penyusunannya. Saya sangat menyukai membaca ini dan saya akan kembali untuk membaca konten lainnya. Terima kasih banyak!
Sangat fantastis informasi dapat ditemukan di blog.
Hi all, here every one is sharing these experience, therefore
it’s pleasant to read this web site, and I used to visit this blog every day.
Artikel yang hebat. Ini memberi saya pemahaman yang lebih baik tentang subjek ini. Teruskan pekerjaan yang luar biasa!
Thanks for your personal marvelous posting! I really enjoyed reading it,
you are a great author.I will ensure that I bookmark your
blog and definitely will come back down the road.
I want to encourage you to definitely continue your great work,
have a nice morning!
This design is steller! You certainly know how to keep a reader entertained. Between your wit and your videos, I was almost moved to start my own blog (well, almost…HaHa!) Wonderful job. I really loved what you had to say, and more than that, how you presented it. Too cool!
Generally I don’t learn post on blogs, however I would like to say that this write-up very forced me to take a look at and do so! Your writing taste has been surprised me. Thank you, quite nice article.
Hmm is anyone else having problems with the images on this blog
loading? I’m trying to figure out if its a problem on my end or if it’s the blog.
Any feedback would be greatly appreciated.
You made some respectable factors there. I looked on the internet for the difficulty and found most people will go together with along with your website.
I got what you intend, appreciate it for putting up.Woh I am pleased to find this website through google. “Wisdom doesn’t necessarily come with age. Sometimes age just shows up by itself.” by Woodrow Wilson.
Outstanding post, I think people should learn a lot from this website its rattling user pleasant.
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
Thanks so much for giving everyone a very special opportunity to check tips from this blog. It is often very excellent and stuffed with a great time for me personally and my office acquaintances to visit the blog minimum 3 times every week to read the new stuff you have. And of course, I am just certainly fulfilled for the magnificent tips you serve. Some 4 facts in this article are surely the best I have ever had.
Have you ever considered writing an ebook or guest authoring on other blogs? I have a blog based on the same ideas you discuss and would really like to have you share some stories/information. I know my visitors would value your work. If you are even remotely interested, feel free to send me an e-mail.
I just couldn’t depart your website before suggesting that I really enjoyed the standard information a person provide for your visitors? Is going to be back often to check up on new posts
Some truly marvelous work on behalf of the owner of this website , utterly great subject matter.
We stumbled over here different web address and thought I might as well check things out. I like what I see so now i’m following you. Look forward to going over your web page for a second time.
I think this site holds some very superb info for everyone :D. “As ill-luck would have it.” by Miguel de Cervantes.
Artikel yang sangat berguna. Saya baru menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
hello there and thank you for your info – I have definitely picked up something new from right here. I did however expertise several technical issues using this site, as I experienced to reload the website lots of times previous to I could get it to load properly. I had been wondering if your web hosting is OK? Not that I am complaining, but sluggish loading instances times will very frequently affect your placement in google and can damage your quality score if advertising and marketing with Adwords. Well I am adding this RSS to my e-mail and could look out for much more of your respective fascinating content. Ensure that you update this again very soon..
I have been absent for a while, but now I remember why I used to love this blog. Thanks, I’ll try and check back more frequently. How frequently you update your website?
Postingan yang hebat. Ini memberikan saya gambaran yang lebih baik tentang topik ini. Teruskan kerja yang luar biasa!
Menghargai waktu dan tenaga yang Anda curahkan ke website Anda dan informasi mendalam yang Anda tawarkan. Sangat baik menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menandai situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Sangat menarik informasi!Sempurna persis seperti yang saya cari! “Jika Anda ingin menguji ingatan Anda, cobalah mengingat apa yang Anda khawatirkan setahun yang lalu hari ini.” oleh Rotarian.
Bersama dengan semua hal yang tampak sedang dibangun sepanjang topik spesifik ini, banyak pandangan Anda cenderung agak radikal. Namun, saya maaf, karena saya tidak setuju sepenuhnya pada keseluruhan ide Anda, meskipun menarik. Sepertinya bagi semua orang bahwa pendapat Anda tidak sepenuhnya benar-benar tervalidasi dan pada kenyataannya Anda diri Anda tidak sepenuhnya percaya diri terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membacanya.
Kami bisa memiliki tautan alternatif kontrak di antara kita!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit mulai waktu berikutnya? Terima kasih atas postingnya.
Saya secara terus menjelajah online untuk ide yang dapat mendukung saya. Terima kasih!
Saya tidak amat bagus dalam bahasa Inggris tetapi saya menemukan ini sangat santai untuk diterjemahkan.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Mereka sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Halo di sana, kamu sudah melakukan kerja yang mengagumkan. Saya pasti akan mem-bookmark ini dan kembali untuk melihat konten lainnya. Terima kasih!
Hmm is anyone else having problems with the pictures on this blog
loading? I’m trying to determine if its a problem on my end or if it’s the blog.
Any feedback would be greatly appreciated.
Tetap saja, terima kasih untuk poin yang menonjol ini dan walaupun saya tidak sepakat sepenuhnya, saya menilai pandangan.
Bernilai informasi. Beruntung saya menemukan website Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya mem-bookmark.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Postingan yang fantastis. Saya sungguh menyukai cara Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang hebat!
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Would you be concerned about exchanging hyperlinks?
Saya secara tidak sengaja menemukan situs Anda dan saya perlu mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
Aku sungguh ingin menulis pesan singkat untuk mengucapkan terima kasih Anda atas seluruh informasi luar biasa yang Anda bagikan di situs ini.
I don’t even know how I finished up right here, however I thought this submit was great. I do not realize who you’re but definitely you are going to a well-known blogger if you happen to are not already 😉 Cheers!
Artikel yang bagus. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang mantap!
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Menjadi kaya adalah memiliki uang, menjadi sejahtera adalah memiliki waktu.” oleh Margaret Bonnano.
Saya perlu mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Meski begitu, terima kasih untuk poin yang luar biasa ini dan meskipun saya tidak setuju sepenuhnya, saya menilai pandangan.
Ini adalah blog yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Excellent read, I just passed this onto a colleague who was doing a little research on that. And he actually bought me lunch since I found it for him smile Thus let me rephrase that: Thank you for lunch! “Any man would be forsworn to gain a kingdom.” by Roger Zelazny.
Terima kasih atas posting yang luar biasa. Saya benar-benar menikmati membaca ini dan menemukan banyak wawasan yang bermanfaat. Teruskan pekerjaan yang bagus!
Saya tidak bisa menahan diri untuk berkomentar
Saya kebetulan menemukan blog Anda dan saya perlu mengatakan bahwa saya sangat kagum. Teruskan kerja yang bagus.
Seseorang secara esensial menolong untuk membuat sangat artikel saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman web Anda dan sampai saat ini? Saya terkagum dengan riset yang Anda lakukan untuk menyusun unggahan menakjubkan ini. Proses yang mengagumkan!
Wow! This can be one particular of the most beneficial blogs We have ever arrive across on this subject. Actually Fantastic. I am also a specialist in this topic therefore I can understand your hard work.
Artikel yang sangat bagus. Saya sungguh menikmati cara Anda menjelaskan ide-ide ini. Teruskan pekerjaan yang hebat!
Hei di sana, Anda telah melakukan kerja yang luar biasa. Saya pasti akan mem-bookmark ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
Hello, after reading this awesome article i am too cheerful to share my experience
here with friends.
I was suggested this web site via my cousin. I am now not sure whether or
not this post is written via him as no one else realize such distinct about my difficulty.
You’re incredible! Thanks!
Situs ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
Saya tidak benar-benar unggul dalam bahasa Inggris tetapi saya menganggap ini sungguh ringan untuk diterjemahkan.
Hei semua, Anda telah melakukan kerja yang mengagumkan. Saya pasti akan menandai ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
sloths funny
References:
https://lexpertpaie.com/employer/muskeln-mithilfe-von-wachstumshormonen:-darum-sollten-sie-davon-die-finger-lassen-gq-germany/
You really make it seem so easy with your presentation but
I find this matter to be actually something which I think I would never understand.
It seems too complex and extremely broad for me.
I am looking forward for your next post, I will try to get the hang of it!
Hiya! I just would like to give a huge thumbs up for the great info you have right here on this post. I shall be coming back to your blog for more soon.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Dengan semua hal yang tampak sedang berkembang di dalam topik khusus ini, banyak pandangan Anda cenderung agak menyegarkan. Kendati demikian, saya memohon maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh saran Anda, meskipun menggairahkan. Sepertinya bagi semua orang bahwa pendapat Anda tidak sepenuhnya sepenuhnya dapat dibenarkan dan pada faktanya Anda sendiri tidak sepenuhnya yakin terhadap poin tersebut. Dalam hal apa pun saya menghargai membacanya.
Hi there, after reading this amazing paragraph i am also cheerful to share my know-how here with colleagues.
Amazing! Its really amazing piece of writing, I have got much clear idea
concerning from this paragraph.
My brother recommended I might like this blog.
He was totally right. This post actually made my day.
You cann’t imagine simply how much time I had spent for this information! Thanks!
You are my inspiration , I own few web logs and often run out from to brand : (.
Spot on with this write-up, I actually believe that this amazing site
needs much more attention. I’ll probably be returning to see
more, thanks for the information!
excellent issues altogether, you simply received a emblem new reader. What would you recommend in regards to your publish that you just made some days ago? Any sure?
Attractive section of content. I just stumbled upon your blog and in accession capital to assert that I acquire actually enjoyed account your blog posts. Any way I’ll be subscribing to your feeds and even I achievement you access consistently fast.
What’s Going down i am new to this, I stumbled upon this I have found It positively helpful and it has helped me out loads. I hope to give a contribution & help different users like its aided me. Good job.
It’s perfect time to make some plans for the future and it is time to be happy. I’ve read this post and if I could I wish to suggest you some interesting things or advice. Maybe you could write next articles referring to this article. I desire to read even more things about it!
There are some interesting closing dates on this article but I don’t know if I see all of them center to heart. There is some validity but I’ll take maintain opinion until I look into it further. Good article , thanks and we wish more! Added to FeedBurner as well
I do like the way you have framed this specific difficulty and it does present us a lot of fodder for consideration. On the other hand, because of what I have experienced, I simply wish when the opinions pile on that people today continue to be on point and in no way embark on a soap box regarding some other news of the day. All the same, thank you for this outstanding piece and while I do not really agree with it in totality, I respect the viewpoint.
This web page is mostly a stroll-by means of for all of the information you needed about this and didn’t know who to ask. Glimpse here, and you’ll definitely uncover it.
Good write-up, I’m normal visitor of one’s website, maintain up the excellent operate, and It is going to be a regular visitor for a lengthy time.
Hello! I could have sworn I’ve been to this website before but after going through some
of the articles I realized it’s new to me. Regardless, I’m definitely delighted I found it and I’ll be book-marking it and checking back frequently!
I like the efforts you have put in this, appreciate it for all the great content.
This is very interesting, You’re a very skilled blogger. I have joined your rss feed and look forward to seeking more of your wonderful post. Also, I have shared your site in my social networks!
Have you ever considered creating an ebook or guest authoring on other websites? I have a blog based on the same ideas you discuss and would really like to have you share some stories/information. I know my subscribers would appreciate your work. If you are even remotely interested, feel free to send me an e-mail.
magnificent put up, very informative. I ponder why the opposite experts of this sector do not notice
this. You must proceed your writing. I am sure, you’ve a huge readers’ base already!
I discovered your weblog website on google and verify a number of of your early posts. Continue to keep up the very good operate. I just extra up your RSS feed to my MSN News Reader. Looking for forward to studying extra from you later on!…
Hello. magnificent job. I did not expect this. This is a great story. Thanks!
I have read so many articles on the topic of the blogger lovers but this post is actually a good paragraph, keep it
up.
This blog is definitely rather handy since I’m at the moment creating an internet floral website – although I am only starting out therefore it’s really fairly small, nothing like this site. Can link to a few of the posts here as they are quite. Thanks much. Zoey Olsen
Hi there, I wish for to subscribe for this blog to obtain most recent updates, so where
can i do it please help.
Great web site. Plenty of useful information here. I’m sending it to several buddies ans also sharing in delicious. And obviously, thanks to your effort!
I’m Carrol and I live in a seaside city in northern United Kingdom, Blaengwrach.
I’m 21 and I’m will soon finish my study at Physical.
Bersama dengan semua hal yang mana terlihat sedang berkembang sepanjang topik ini, semua pandangan Anda adalah lumayan menarik. Di sisi lain, saya minta maaf, tetapi saya tidak setuju sepenuhnya pada seluruh teori Anda, meskipun menstimulasi. Tampaknya bagi kami bahwa ulasan Anda tidak sepenuhnya benar-benar dapat dibenarkan dan pada kenyataannya Anda sendiri tidak sepenuhnya yakin terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membaca.
Saya selalu tertarik dengan topik ini dan tetap masih demikian, terimakasih telah memposting.
Saya tidak sering berkomentar tetapi saya harus mengatakan terima kasih untuk posting yang sempurna ini : D.
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri! “Washington adalah satu-satunya tempat di mana suara bergerak lebih cepat daripada cahaya.” oleh C. V. R. Thompson.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Artikel yang bagus. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan bersyukur kepada Anda.
Postingan yang fantastis! Saya menghargai cara Anda menjelaskan segala sesuatu dengan jelas. Teruskan pekerjaan yang hebat!
Terima kasih untuk artikel fantastis tambahan. Di mana lagi siapa pun mungkin bisa mendapatkan jenis info seperti itu dengan metode penulisan yang ideal? Saya memiliki presentasi minggu depan, dan saya sedang dalam pencarian informasi seperti ini.
I’m Stanley (31) from Montreal, Canada.
I’m learning English literature at a local college and I’m just about to graduate.
I have a part time job in a the office.
Generally I don’t read post on blogs, but I wish to say that this write-up very forced me to try and do so! Your writing style has been surprised me. Thanks, quite nice post.
What you posted was very reasonable. But, what about this?
what if you were to write a killer post title? I am not saying your information isn’t
good, however suppose you added a post title that grabbed a person’s attention? I mean Balancing the Scales:
Patient Load vs. Care Quality in Diabetes – D-Coded Diabetes
Research is a little vanilla. You ought to look
at Yahoo’s front page and watch how they create article headlines to grab viewers to click.
You might add a video or a pic or two to grab people
excited about everything’ve got to say. In my opinion,
it might bring your posts a little livelier.
Fantastic beat ! I wish to apprentice while you amend your web site,
how could i subscribe for a blog site? The account aided me a acceptable
deal. I had been tiny bit acquainted of this your
broadcast offered bright clear idea
I really appreciate this post. I’ve been looking all over for this! Thank goodness I found it on Bing. You’ve made my day! Thx again
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Amat luar biasa informasi dapat ditemukan di web site.
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan yang unggul!
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi empat puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Artikel yang sangat bagus. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan kerja yang hebat!
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Saya tidak biasanya berkomentar tetapi saya harus mengakui hargai untuk posting yang hebat ini : D.
Artikel yang luar biasa. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Sangat luar biasa informasi dapat ditemukan di blog.
Isi yang berguna dan disajikan dengan baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Postingan ini penuh informasi. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Saya selalu memikirkan hal ini, terimakasih telah memposting.
Postingan yang luar biasa. Ini memberi saya pemahaman yang lebih jelas tentang subjek ini. Teruskan kerja yang luar biasa!
Appreciate this post. Let me try it out. https://cryptobossmacher.top/
Meski begitu, terima kasih untuk artikel yang menonjol ini dan walaupun saya tidak benar-benar setuju sepenuhnya, saya menilai perspektif.
Anda bisa pasti melihat keahlian Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu kejar hati Anda.
Postingan yang luar biasa. Saya benar-benar menikmati cara Anda menyampaikan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
Wow! Ini mungkin salah satu blog paling membantu yang pernah kami temui tentang topik ini. Pada dasarnya Mengagumkan. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami kerja keras Anda.
Hei semua, saya menjumpai website Anda melalui Google saat mencari topik yang serupa, website Anda tampil di posisi atas. Saya harus mengakui bahwa saya kagum betapa bagus pengaturannya. Saya sangat menikmati menelusuri ini dan saya akan kembali untuk melihat konten lainnya. Terima kasih!
Postingan ini sangat berguna. Saya sangat menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Terima kasih atas tulisan yang baik. Sebenarnya ini sebelumnya adalah sebuah konten hiburan. Terlihat rumit menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa tetap berkomunikasi?
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Ya menyimpan ini bukanlah penentuan yang berisiko posting yang hebat! .
Wow, hebat blog format! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan website Anda sangat baik, serta kontennya!
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada metode Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Bagian yang kuat, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan agak evaluasi tentang ini. Dan dia pada kenyataannya membelikan saya sarapan sebagai hasil dari saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk mendiskusikan ini, saya sangat merasa kuat tentang hal ini dan suka membaca lebih banyak tentang topik ini. Jika memungkinkan, seiring Anda menjadi lebih berpengalaman, apakah Anda berkenan memperbarui blog Anda dengan lebih banyak detail? Ini sangat membantu bagi saya. Jempol besar untuk unggahan weblog ini!
Hore google adalah penguasa dunia saya yang menolong saya menemukan web site yang luar biasa! .
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan berterima kasih kepada Anda.
Saya secara terus melihat online untuk tips yang dapat menolong saya. Thanks!
Biasanya saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
Halo semua, hanya ingin mengatakan bahwa saya benar-benar menikmati membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak informasi yang bermanfaat. Terima kasih!
I’m no longer positive where you’re getting your info,
but great topic. I must spend a while learning more or working out more.
Thanks for fantastic info I used to be looking for this info for my mission.
Ini adalah topik yang sangat dekat di hati saya, salam, tapi di mana informasi kontak Anda?
Loving the info on this internet site, you have done outstanding job on the posts.
Ini adalah blog yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar hebat!
Ketika saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada sarana Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Halo semua, hanya ingin mengatakan bahwa saya benar-benar menikmati membaca melalui postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa cukup banyak wawasan yang bermanfaat. Terima kasih!
Kami akan memiliki hyperlink alternatif kesepakatan di antara kita!
Benar-benar baik informasi dapat ditemukan di web blog.
Nice post. I was checking continuously this weblog and I’m impressed! Very useful information specifically the remaining section 🙂 I deal with such information a lot. I was seeking this certain info for a very long time. Thank you and good luck.
Artikel yang luar biasa. Ini memberikan saya gambaran yang lebih jelas tentang subjek ini. Teruskan kerja yang luar biasa!
Ya menyimpan ini bukanlah kesimpulan yang spekulatif posting yang luar biasa! .
Terima kasih untuk situs web informatif tambahan. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan gaya yang sempurna? Saya memiliki sebuah proyek yang saya tengah kerjakan, dan saya sudah mencari informasi seperti ini.
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin sekali mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda mengejutkan saya. Terima kasih, sangat artikel yang bagus.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Luar biasa. Saya juga seorang ahli dalam topik ini jadi saya dapat memahami usaha Anda.
Sangat jelas situs, hargai untuk pos ini.
Artikel ini penuh informasi. Saya menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
you’re truly a excellent webmaster. The site loading pace is incredible. It sort of feels that you are doing any unique trick. Furthermore, The contents are masterpiece. you have performed a great job in this matter!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya terkesan dengan situs internet ini, amat saya adalah penggemar berat.
Howdy, i read your blog from time to time and i own a similar one and i was just curious if you get a lot of spam responses? If so how do you reduce it, any plugin or anything you can suggest? I get so much lately it’s driving me crazy so any support is very much appreciated.
Benar-benar luar biasa informasi dapat ditemukan di website.
Saya tidak bisa menahan diri untuk berkomentar
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Amal itu merugikan kecuali jika membantu penerimanya menjadi mandiri.” oleh John Davidson Rockefeller, Sr..
Wow! Thank you! I constantly wanted to write on my site something like that. Can I take a portion of your post to my website?
I am really loving the theme/design of your web site. Do you ever run into any internet browser compatibility issues? A number of my blog visitors have complained about my site not working correctly in Explorer but looks great in Opera. Do you have any recommendations to help fix this problem?
Saya tidak umumnya berkomentar tetapi saya harus mengakui salam untuk posting yang hebat ini : D.
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas kami akan bersyukur kepada Anda.
Loving the information on this web site, you have done great job on the posts.
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di situs saya sesuatu seperti itu. Bolehkah saya mengambil bagian dari posting Anda ke website saya?
You could definitely see your enthusiasm within the work you write. The world hopes for even more passionate writers such as you who aren’t afraid to mention how they believe. All the time follow your heart. “We are near waking when we dream we are dreaming.” by Friedrich von Hardenberg Novalis.
This blog is definitely rather handy since I’m at the moment creating an internet floral website – although I am only starting out therefore it’s really fairly small, nothing like this site. Can link to a few of the posts here as they are quite. Thanks much. Zoey Olsen
Saya tidak sangat bagus dalam bahasa Inggris tetapi saya menganggap ini amat mudah untuk dipahami.
Hello, this weekend is pleasant designed for me, for the reason that this time i am reading this fantastic informative piece of writing
here at my residence.
Sesudah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada pendekatan Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
It’s actually a great and useful piece of info. I’m happy that you simply shared this useful information with us. Please keep us informed like this. Thank you for sharing.
Its fantastic as your other posts : D, thankyou for posting. “History is a pact between the dead, the living, and the yet unborn.” by Edmund Burke.
I’ll immediately take hold of your rss as I can not to find your e-mail subscription hyperlink or e-newsletter service. Do you have any? Please let me recognise so that I may subscribe. Thanks.
Hi there, You’ve done a great job. I’ll definitely digg it and personally suggest to my friends. I am sure they will be benefited from this web site.
I was very pleased to find this web-site.I wanted to thanks for your time for this wonderful read!! I definitely enjoying every little bit of it and I have you bookmarked to check out new stuff you blog post.
Good day! This post could not be written any better! Reading through this post reminds me of my good old room mate! He always kept chatting about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
What’s Happening i am new to this, I stumbled upon this I’ve discovered It positively helpful and it has aided me out loads. I hope to contribute & help different users like its aided me. Great job.
Olxtoto adalah agen terpercaya untuk situs toto dan bandar togel yang melayani pemain di Indonesia dengan komitmen tinggi terhadap kepuasan pelanggan.
Wow, this post is nice, my younger sister is analyzing these kinds
of things, thus I am going to let know her.
I truly appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thank you again!
Enjoyed looking at this, very good stuff, regards.
Youre so cool! I dont suppose Ive read something like this before. So good to seek out somebody with some original ideas on this subject. realy thank you for starting this up. this website is something that is needed on the internet, somebody with a little originality. helpful job for bringing one thing new to the web!
I’m not sure why but this web site is loading incredibly slow for me. Is anyone else having this issue or is it a issue on my end? I’ll check back later on and see if the problem still exists.
Hi, Neat post. There is a problem together with your website in web explorer, would test this?K IE still is the marketplace chief and a big section of folks will pass over your wonderful writing due to this problem.
Wow that was unusual. I just wrote an really long comment but after I clicked submit my comment didn’t show up. Grrrr… well I’m not writing all that over again. Anyway, just wanted to say great blog!
I like the helpful information you provide in your articles. I will bookmark your blog and take a look at again here regularly. I am reasonably certain I will learn lots of new stuff proper right here! Good luck for the next!
You have brought up a very fantastic details , thanks for the post.
Very nice post. I just stumbled upon your weblog and wanted to say that I have really enjoyed browsing your blog posts. In any case I’ll be subscribing to your rss feed and I hope you write again very soon!
You are so interesting! I do not believe I’ve read something like that before.
So good to find somebody with genuine thoughts on this subject.
Really.. many thanks for starting this up. This web site is something that’s needed
on the internet, someone with a little originality!
Isi yang fantastis! Gaya penulisan Anda jelas dan mudah dipahami. Saya tentu akan kembali untuk melihat konten lainnya.
Ini adalah saran yang sangat bagus, terutama bagi mereka yang baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
I love the efforts you have put in this, thanks for all the great blog posts.
Thank you, I’ve recently been looking for info about this topic for a while and yours is the greatest I’ve discovered so far. However, what concerning the bottom line? Are you sure concerning the supply?
I really appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again!
I got what you mean , thankyou for posting.Woh I am pleased to find this website through google. “Money is the most egalitarian force in society. It confers power on whoever holds it.” by Roger Starr.
Howdy! I could have sworn I’ve been to this blog before but after reading through some of the post I realized it’s new to me. Nonetheless, I’m definitely happy I found it and I’ll be book-marking and checking back frequently!
Its fantastic as your other articles : D, thanks for posting.
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
Wow! This can be one particular of the most beneficial blogs We have ever arrive across on this subject. Basically Magnificent. I am also a specialist in this topic therefore I can understand your effort.
What i do not understood is actually how you’re no longer really much more well-liked than you may be now. You are so intelligent. You realize thus significantly in the case of this subject, made me individually believe it from so many numerous angles. Its like men and women aren’t interested except it is one thing to do with Lady gaga! Your personal stuffs nice. All the time take care of it up!
Pretty nice post. I simply stumbled upon your blog and wanted to say that I’ve truly loved browsing your blog posts. In any case I will be subscribing to your feed and I’m hoping you write again very soon!
I like this website its a master peace ! Glad I noticed this on google .
Thanks for another informative web site. Where else could I get that type of info written in such a perfect way? I have a project that I am just now working on, and I’ve been on the look out for such information.
Hi, Neat post. There is a problem along with your web site in internet explorer, might
check this? IE still is the market leader and a large section of other folks will
miss your magnificent writing because of this problem.
great submit, very informative. I ponder why the other specialists of this sector do not realize this. You must proceed your writing. I am confident, you have a great readers’ base already!
Good website! I truly love how it is easy on my eyes and the data are well written. I am wondering how I might be notified when a new post has been made. I’ve subscribed to your feed which must do the trick! Have a nice day!
I couldn’t resist commenting
Hi would you mind sharing which blog platform you’re working with?
I’m looking to start my own blog soon but I’m having a difficult time deciding between BlogEngine/Wordpress/B2evolution and Drupal.
The reason I ask is because your design seems different then most blogs and I’m looking for something
unique. P.S My apologies for being off-topic but I had to
ask!
Does your site have a contact page? I’m having trouble locating it but, I’d like to send you an email. I’ve got some ideas for your blog you might be interested in hearing. Either way, great blog and I look forward to seeing it expand over time.
Some truly good information, Sword lily I observed this. “Love consists in this, that two solitudes protect and touch and greet each other.” by Rainer Maria Rilke.
Very interesting details you have noted, appreciate it for posting. “History is a cyclic poem written by Time upon the memories of man.” by Percy Bysshe Shelley.
I conceive this internet site holds some rattling good info for everyone. “Glory is fleeting, but obscurity is forever.” by Napoleon.
I truly appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thanks again
I am glad to be one of several visitors on this outstanding website (:, thanks for putting up.
I gotta bookmark this internet site it seems very useful extremely helpful
Ini adalah situs yang tepat untuk siapa saja yang ingin mengetahui tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Postingan ini sangat berguna. Saya menghargai usaha yang Anda curahkan untuk menulisnya. Terima kasih!
Appreciate this post. Will try it out.
It’s appropriate time to make some plans for the long run and it is time to be happy. I’ve learn this put up and if I could I desire to counsel you some fascinating issues or tips. Perhaps you could write subsequent articles relating to this article. I desire to read even more issues about it!
Its like you read my mind! You appear to understand a lot approximately this, like you wrote the e-book in it or something.
I believe that you could do with some percent to force the
message house a little bit, however other than that, that is fantastic
blog. An excellent read. I’ll definitely be back.
My programmer is trying to convince me to move to .net from PHP.
I have always disliked the idea because of the costs. But he’s tryiong none the less.
I’ve been using Movable-type on various websites for about a year and am anxious about switching to another platform.
I have heard excellent things about blogengine.net.
Is there a way I can transfer all my wordpress posts into it?
Any help would be really appreciated!
Real clean website , thankyou for this post.
Thanks for sharing excellent informations. Your site is so cool. I’m impressed by the details that you’ve on this website. It reveals how nicely you perceive this subject. Bookmarked this website page, will come back for more articles. You, my friend, ROCK! I found just the info I already searched all over the place and just could not come across. What an ideal web-site.
Postingan yang hebat. Ini memberikan saya gambaran yang lebih jelas tentang topik ini. Teruskan kerja yang hebat!
Saya senang menjadi pengunjung dari website paripurna ini!, terima kasih atas informasi langka ini!
It is the best time to make some plans for the future and it is time to be happy. I have read this submit and if I could I want to suggest you some attention-grabbing things or suggestions. Maybe you can write subsequent articles referring to this article. I wish to read more issues about it!
This is a topic close to my heart cheers, where are your contact details though?
What’s up to all, it’s actually a nice for me to pay a quick visit this web page, it consists of
priceless Information.
I respect your piece of work, appreciate it for all the great blog posts.
I’ll right away grab your rss feed as I can’t in finding your e-mail subscription hyperlink or e-newsletter service. Do you have any? Please let me know in order that I may subscribe. Thanks.
Nice post. I be taught one thing more difficult on different blogs everyday. It is going to at all times be stimulating to learn content material from different writers and apply a little bit one thing from their store. I’d prefer to make use of some with the content on my blog whether or not you don’t mind. Natually I’ll offer you a link on your net blog. Thanks for sharing.
It’s the best time to make some plans for the future and
it’s time to be happy. I’ve read this post and if I could I desire to suggest you few interesting things or tips.
Perhaps you can write next articles referring to this article.
I want to read more things about it!
I’m very happy to read this. This is the type of manual that needs to be given and not the random misinformation that’s at the other blogs. Appreciate your sharing this greatest doc.
Hey are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and create my own. Do you require any html coding expertise to make your own blog? Any help would be really appreciated!
Great write-up, I’m normal visitor of one’s blog, maintain up the excellent operate, and It is going to be a regular visitor for a long time.
It’s actually a nice and useful piece of info. I’m satisfied that you just shared this useful information with us. Please keep us informed like this. Thanks for sharing.
Nice post. I was checking constantly this blog and I am impressed!
Very helpful info specially the last part 🙂 I care for such information a
lot. I was looking for this certain information for a very long time.
Thank you and best of luck.
Saya selamanya memikirkan hal ini, salam telah memposting.
Hei semua, kamu sudah melakukan kerja yang fantastis. Saya pasti akan menandai ini dan kembali untuk melihat konten lainnya. Terima kasih banyak!
I am truly pleased to glance at this web site posts which includes tons
of useful facts, thanks for providing such data.
Isi yang bermanfaat dan disajikan dengan baik. Saya pasti akan merekomendasikan ini kepada teman-teman. Terima kasih telah berbagi.
Ini adalah tips yang sangat baik, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
I like this post, enjoyed this one regards for posting.
Konten yang fantastis! Cara penulisan Anda jelas dan mudah dimengerti. Saya pasti akan kembali untuk melihat lebih banyak.
Bagaimanapun, terima kasih untuk artikel yang hebat ini dan meskipun saya tidak benar-benar sepakat sepenuhnya, saya menilai perspektif.
Hello there! I know this is kind of off topic but I was wondering which blog
platform are you using for this site? I’m getting tired of WordPress because I’ve had problems
with hackers and I’m looking at options for another platform.
I would be awesome if you could point me in the direction of a good platform.
Thanks for another informative site. Where else could I get that type of information written in such a perfect way? I’ve a project that I am just now working on, and I have been on the look out for such info.
Menikmati membaca ini, sangat bagus, salam.
Saya terus memikirkan hal ini, terima kasih telah mengunggah.
Halo di sana, sekadar ingin mengatakan bahwa saya sangat menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak informasi yang sangat berguna. Terima kasih!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Hmm apakah ada orang lain yang menghadapi masalah dengan foto di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Please let me know if you’re looking for a writer for your weblog.
You have some really great articles and I feel I
would be a good asset. If you ever want to take some of the load off, I’d really like to write some content
for your blog in exchange for a link back to mine. Please blast me an email if interested.
Many thanks!
Berharga info. Beruntung saya menemukan website Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Saya senang menjadi salah satu dari banyak pengunjung di situs luar biasa ini (:, terima kasih telah memposting.
Hai di sana, Anda telah melakukan pekerjaan yang hebat. Saya pasti akan mem-bookmark ini dan kembali untuk melihat konten lainnya. Terima kasih!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Postingan yang luar biasa. Ini memberikan saya pemahaman yang lebih jelas tentang topik ini. Teruskan pekerjaan yang luar biasa!
Saya terkesan dengan website ini, sungguh saya adalah penggemar berat.
I like assembling utile info, this post has got me even more info! .
Wow! Terima kasih! Saya secara terus membutuhkan menulis di situs saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke situs saya?
Mengagumi usaha yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda berikan. Sangat baik menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menandai situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada metode Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
Aku benar-benar ingin menulis pesan singkat guna menghargai Anda atas seluruh tips luar biasa yang Anda tuliskan di situs ini.
Seseorang pada dasarnya membantu membuat artikel yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Pekerjaan yang mengagumkan!
Terima kasih untuk website informatif lainnya. Di tempat mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan metode yang ideal? Saya memiliki sebuah proyek yang saya tengah jalankan, dan saya sudah mencari informasi seperti ini.
Thank you for sharing superb informations. Your web site is so cool. I’m impressed by the details that you’ve on this site. It reveals how nicely you understand this subject. Bookmarked this website page, will come back for extra articles. You, my friend, ROCK! I found simply the info I already searched everywhere and just couldn’t come across. What a great site.
Hmm apakah ada orang lain yang mengalami masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba menentukan apakah ini masalah di sisi saya atau blognya. Masukan apa pun akan sangat dihargai.
Saya menghargai waktu yang Anda curahkan untuk membuat posting ini. Konten yang berguna. Terima kasih banyak!
Artikel ini sangat informatif. Saya menghargai waktu yang Anda curahkan untuk menulisnya. Terima kasih!
Berharga informasi. Untungnya saya menemukan situs Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak terjadi lebih awal! Saya mem-bookmark.
I’ve recently started a web site, the information you offer on this web site has helped me greatly. Thank you for all of your time & work. “Cultivation to the mind is as necessary as food to the body.” by Marcus Tullius Cicero.
I am very happy to read this. This is the type of manual that needs to be given and not the random misinformation that is at the other blogs. Appreciate your sharing this greatest doc.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Website ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
LUCK8
Ya menyimpan ini bukanlah penentuan yang buruk pos yang hebat! .
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang hebat!
Saya amat tertarik menemukan situs ini di Bing, persis seperti yang saya telusuri : D pula sudah saya simpan ke fav.
Artikel yang hebat. Ini memberikan saya gambaran yang lebih baik tentang subjek ini. Teruskan pekerjaan yang hebat!
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya mengunjungi banyak website tetapi saya pikir yang satu ini mengandung sesuatu yang ekstra di dalamnya
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda jelas tahu apa yang Anda bicarakan, mengapa menyia-nyiakan kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
Postingan ini penuh informasi. Saya sangat menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
Hei semua, kamu sudah melakukan pekerjaan yang mengagumkan. Saya tentu akan menandai ini dan kembali untuk membaca lebih banyak. Terima kasih banyak!
Paragraph writing is also a excitement, if you be familiar
with afterward you can write or else it is complicated to write. https://cryptoboss353.top/
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang sangat bagus!
Artikel yang hebat. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan kerja yang hebat!
fantastic points altogether, you just won a brand new reader. What would you recommend about your put up that you simply made some days in the past? Any sure?
Only wanna tell that this is very beneficial, Thanks for taking your time to write this.
Somebody essentially help to make seriously articles I would state. This is the very first time I frequented your web page and thus far? I amazed with the research you made to make this particular publish incredible. Fantastic job!
Mengagumi usaha yang Anda curahkan ke situs Anda dan informasi terperinci yang Anda sajikan. Sangat bagus menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang sangat baik! Saya sudah menandai situs Anda dan menambahkan feed RSS Anda ke akun Google saya.
Berharga info. Beruntung saya menemukan situs Anda secara tidak sengaja, dan aku terkejut mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
As I website possessor I believe the content matter here is rattling wonderful , appreciate it for your hard work. You should keep it up forever! Best of luck.
I’ve learn several excellent stuff here. Definitely price bookmarking for revisiting. I wonder how so much attempt you place to create this sort of excellent informative site.
Kami bisa memiliki tautan perubahan kontrak di antara kita!
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Ya menyimpan ini bukanlah kesimpulan yang buruk posting yang hebat! .
Saya tidak benar-benar mahir dalam bahasa Inggris tetapi saya memperoleh ini amat mudah untuk diterjemahkan.
whoah this blog is fantastic i love reading your posts. Keep up the great work! You know, many people are searching around for this information, you can aid them greatly.
What i don’t realize is in reality how you are not actually a lot more neatly-liked than you may be right now. You’re very intelligent. You know thus considerably with regards to this subject, produced me for my part believe it from a lot of numerous angles. Its like women and men don’t seem to be involved until it’s something to accomplish with Girl gaga! Your individual stuffs outstanding. Always deal with it up!
Wonderful article! We will be linking to this particularly great content on our site.
Keep up the great writing.
Artikel yang luar biasa. Ini memberikan saya pemahaman yang lebih jelas tentang topik ini. Teruskan kerja yang hebat!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah detail kontak Anda?
Enjoyed examining this, very good stuff, appreciate it.
Benar-benar baik info dapat ditemukan di web site.
I truly enjoy looking through on this web site, it contains fantastic articles.
Wow, keren weblog struktur! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan web site Anda hebat, serta materinya!
Menakjubkan! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna desain yang hebat!
Hiya, I’m really glad I have found this information. Today bloggers publish just about gossips and net and this is actually frustrating. A good website with exciting content, that is what I need. Thanks for keeping this site, I will be visiting it. Do you do newsletters? Can’t find it.
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Sangat menarik info !Sempurna persis seperti yang saya cari!
Excelente cassino para quem gopsta de cssino online.
O Pin-Up Casino tem bônus reais com PIX rápido.
Vale muito a pena ara quem quer bônus de verdade. Promoção de boas-vindas competitiva e 250 rodadas grátis.
Sou cliente do Pin-Up Brasil e recomendo sem nenhum problema nos
pagamentos. Pagamento pelo PIX e equipe brasileira impressionam.
A oferta dee cadastro do Pin-Up Casino é competitivo que já testei.
R$1.500 de bônus e fre spins para novos jogadores.
Cassino online confiável com PIX disponível. O Pin-Up
Brasil opera dese 2016 e nunca atrasa pagamentos.
Experimentei essa plataforma e aprovei com os 4.000 jogos.
Mais de 4.000 jogos incluindo Aviator e slots incríveis.
Para quem busca apostas comm bônus reais. Essa plataforma
reúne o melhor: bônus, jogos e saques rápidos.
Tetap saja, terima kasih untuk artikel yang fantastis ini dan meskipun saya tidak sepakat sepenuhnya, saya menghormati perspektif.
Saya sangat tertarik menemukan situs web ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke fav.
Postingan yang luar biasa! Saya menghargai cara Anda menjelaskan segala sesuatu dengan jelas. Teruskan kerja yang hebat!
Wow, menakjubkan blog struktur! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan situs Anda sangat baik, belum lagi materinya!
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
You are my breathing in, I have few web logs and very sporadically run out from post :). “To die for a religion is easier than to live it absolutely.” by Jorge Luis Borges.
I dugg some of you post as I cogitated they were very useful very useful
Hi Dear, are you really visiting this website on a
regular basis, if so then you will absolutely take fastidious knowledge.
Postingan yang sangat baik. Ini jelas disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi informasi ini.
Very superb info can be found on weblog.
Unquestionably imagine that which you said. Your favourite reason seemed to be at the internet the simplest factor to have in mind of. I say to you, I definitely get annoyed even as people think about concerns that they just don’t recognise about. You controlled to hit the nail upon the top and also outlined out the whole thing with no need side-effects , other people can take a signal. Will likely be again to get more. Thank you
I’m curious to find out what blog platform you are using? I’m experiencing some small security issues with my latest website and I’d like to find something more safe. Do you have any solutions?
Wohh persis apa yang saya telusuri, terimakasih atas posting.
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 40 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkejut dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Kerja yang fantastis!
Terima kasih, saya baru saja mencari informasi sekitar subjek ini sudah lama dan milik Anda adalah yang terbaik yang saya ketahui sejauh ini. Namun, bagaimana dengan kesimpulan? Apakah Anda yakin tentang asal tersebut?
Artikel yang fantastis! Saya sangat menghargai cara Anda menjelaskan semuanya dengan sangat jelas. Teruskan kerja yang hebat!
Kemarin, saat saya sedang bekerja, saudara perempuan saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Saya sangat menghargai waktu yang Anda luangkan untuk membuat artikel ini. Informasi yang sangat berharga. Terima kasih!
Hei semua, saya menemukan website Anda lewat Google ketika menelusuri topik yang mirip, blog Anda muncul di bagian atas. Saya harus mengatakan bahwa saya terkejut betapa rapi penyusunannya. Saya sangat menikmati membaca ini dan saya pasti akan kembali untuk melihat lebih banyak. Terima kasih banyak!
Isi yang bermanfaat dan ditulis dengan sangat baik. Saya tentu akan membagikan ini kepada teman-teman. Terima kasih telah berbagi.
Ini adalah tips yang sangat baik, terutama bagi mereka yang masih baru di dunia blog, informasi yang singkat dan akurat… Terima kasih telah berbagi ini. Tulisan yang wajib dibaca.
Terima kasih banyak atas artikel yang sangat baik. Saya benar-benar menikmati membaca ini dan menemukan banyak informasi yang berguna. Teruskan kerja yang bagus!
Ini adalah saran yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Kami bisa memiliki hyperlink alternatif perjanjian antara kita!
Hei di sana, saya menemukan website Anda lewat Google ketika mencari subjek yang sebanding, situs Anda tampil di hasil teratas. Saya perlu mengakui bahwa saya kagum betapa rapi penulisannya. Saya sangat menyukai menelusuri ini dan saya pasti akan kembali untuk membaca lebih banyak. Terima kasih!
Dengan segala sesuatu yang terlihat sedang dibangun sepanjang topik ini, pandangan Anda umumnya lumayan menstimulasi. Walaupun begitu, saya maaf, tetapi saya tidak memberikan kepercayaan pada keseluruhan teori Anda, meskipun menstimulasi. Terlihat bagi semua orang bahwa pendapat Anda tidak sepenuhnya benar-benar tervalidasi dan pada kenyataannya Anda sendiri tidak sepenuhnya percaya diri terhadap poin tersebut. Dalam hal apa pun saya menghargai membacanya.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Thanks for sharing such a nice thinking, article is good, thats why i have read it fully
It’s hard to come by well-informed people for this topic,
however, you seem like you know what you’re talking about!
Thanks
This site truly has all of the info I needed about this subject and didn’t know who to
ask.
Hello everyone, it’s my first pay a quick visit at this website, and piece
of writing is genuinely fruitful in support of me, keep up posting these types of articles or reviews.
Saya senang menjadi salah satu pengunjung di website luar biasa ini (:, salam telah mengunggah.
Amat hebat info dapat ditemukan di blog.
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang luar biasa!
Wow! Ini bisa jadi salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Sebenarnya Sangat baik. Saya juga seorang ahli dalam topik ini jadi saya dapat memahami kerja keras Anda.
Hi, saya rasa situs Anda mungkin memiliki masalah kompatibilitas browser. Saat saya melihatnya di Safari terlihat baik-baik saja, tetapi di Internet Explorer tampilannya saling tumpang tindih. Saya hanya ingin memberi tahu Anda! Selain itu, blog yang fantastis!
Artikel yang hebat. Saya sungguh menyukai cara Anda menjelaskan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
Hello my family member! I wish to say that this article is awesome, great written and come with approximately all significant infos. I’d like to look more posts like this .
Sangat menarik informasi!Sempurna persis seperti yang saya telusuri!
Bernilai informasi. Beruntung saya menemukan situs Anda secara tidak sengaja, dan saya terkejut mengapa kecelakaan ini tidak terjadi lebih awal! Saya menandainya.
Hi there! This is my first visit to your blog! We are a collection of volunteers and starting a new initiative in a community in the same niche. Your blog provided us useful information to work on. You have done a wonderful job!
Very nice article, exactly what I was looking for.
I regard something really interesting about your blog so I saved to bookmarks.
Mengagumi usaha yang Anda curahkan ke website Anda dan informasi terperinci yang Anda tawarkan. Sangat bagus menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Artikel yang fantastis! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Isi yang hebat! Cara penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk melihat konten lainnya.
Asking questions are genuinely fastidious thing if you are not understanding anything
entirely, except this post gives nice understanding yet.
Attractive part of content. I just stumbled upon your blog
and in accession capital to assert that I acquire
actually enjoyed account your weblog posts. Any way I will be subscribing on your feeds
and even I achievement you get entry to constantly rapidly.
Postingan ini sangat berguna. Saya menghargai usaha yang Anda luangkan untuk menulisnya. Terima kasih!
Isi yang luar biasa! Saya pasti akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
I am often to running a blog and i actually appreciate your content. The article has actually peaks my interest. I’m going to bookmark your site and hold checking for brand new information.
Mengagumi kerja keras yang Anda curahkan ke website Anda dan informasi mendalam yang Anda berikan. Sangat bagus menemukan blog sesekali yang tidak berisi materi lama yang diulang-ulang. Bacaan yang fantastis! Saya sudah menyimpan situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Terima kasih banyak atas artikel yang luar biasa. Saya benar-benar menikmati membaca ini dan menemukan banyak informasi yang berguna. Teruskan pekerjaan yang bagus!
Does your site have a contact page? I’m having
problems locating it but, I’d like to send you an email.
I’ve got some creative ideas for your blog you might be interested in hearing.
Either way, great blog and I look forward to seeing
it expand over time.
Ya menyimpan ini bukanlah penentuan yang spekulatif posting yang luar biasa! .
What’s Happening i’m new to this, I stumbled upon this I have found It absolutely useful and it has aided me out loads. I am hoping to contribute & aid different customers like its aided me. Good job.
Terima kasih, saya baru saja menelusuri informasi sekitar topik ini sudah lama dan milik Anda adalah yang paling hebat yang saya temukan sejauh ini. Tapi, bagaimana dengan inti permasalahan? Apakah Anda positif tentang sumber tersebut?
I do not know if it’s just me or if perhaps everybody else experiencing problems with your website.
It appears like some of the written text in your content are running off the screen. Can somebody else please provide feedback and let me know if this is happening
to them as well? This might be a problem with my web browser because I’ve had
this happen previously. Kudos
by the representation ofsome favourite scene done by her own hand.ロボット セックスWe learned Latin and English,
セックス ロボット“how is it Annette never got married?How stupid you men all are not to have married her! Excuse me for sayingso,but you have no sense about women.
Regions,オナドールand the like.
Wah! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang unggul!
Hmm is anyone else having problems with the pictures on this blog loading? I’m trying to figure out if its a problem on my end or if it’s the blog. Any suggestions would be greatly appreciated.
Way cool, some valid points! I appreciate you making this article available, the rest of the site is also high quality. Have a fun.
Terima kasih banyak atas artikel yang hebat. Saya sungguh menyukai membaca ini dan menemukan banyak informasi yang bermanfaat. Teruskan kerja yang hebat!
Bagian yang kuat, saya sekadar memberikannya kepada seorang rekan yang sedang melakukan sedikit evaluasi tentang ini. Dan dia sesungguhnya membelikan saya sarapan karena saya menemukannya untuknya.. senyum. Jadi biar saya ulangi: Terima kasih untuk jamuan! Namun ya terima kasih telah meluangkan waktu untuk membahas ini, saya benar-benar merasa kuat tentang hal ini dan suka mempelajari tambahan tentang topik ini. Jika potensial, seiring Anda berkembang menjadi lebih berpengalaman, apakah Anda berkenan memperbarui blog Anda dengan tambahan rincian? Ini sangat membantu bagi saya. Jempol besar untuk posting blog ini!
you are truly a excellent webmaster. The web site loading speed is amazing. It kind of feels that you are doing any distinctive trick. Also, The contents are masterpiece. you’ve done a wonderful process on this subject!
Only wanna input that you have a very nice internet site, I love the layout it really stands out.
Hi my family member! I wish to say that this article is amazing, great written and include approximately all important infos. I’d like to peer extra posts like this .
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda tentu tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke situs ketika Anda bisa memberi kami sesuatu yang informatif untuk dibaca?
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Hai di sana, kamu sudah melakukan kerja yang luar biasa. Saya pasti akan menandai ini dan kembali untuk melihat lebih banyak. Terima kasih banyak!
Hi there, I found your website via Google at the same time as looking for a comparable topic, your site got here up, it seems to be good. I have bookmarked it in my google bookmarks.
Saya mendapatkan info yang bagus dari blog Anda.
Saya terkesan dengan situs web ini, benar-benar saya adalah penggemar berat.
Saya kebetulan menemukan blog Anda dan saya harus mengatakan bahwa saya sangat terkesan. Teruskan kerja yang luar biasa.
Dead written articles, Really enjoyed reading through.
Wow! Terima kasih! Saya terus-menerus ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke website saya?
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi megah dibagikan secara bebas.
What’s Taking place i’m new to this, I stumbled upon this I have discovered It absolutely helpful and it has aided me out loads.
I hope to contribute & assist other customers like its aided me.
Good job.
Postingan yang bagus. Ini jelas ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Artikel yang sangat bagus. Saya benar-benar menikmati gaya Anda menjelaskan gagasan-gagasan ini. Teruskan kerja yang hebat!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas akan bersyukur kepada Anda.
Ini adalah blog yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda memahami begitu banyak hal sehingga hampir sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar memberikan pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar luar biasa!
Hari ini, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi dua puluh lima kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Seseorang pada dasarnya membantu membuat artikel yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Kerja yang sangat baik!
Ini adalah topik yang sangat penting di hati saya, salam, tapi di mana informasi kontak Anda?
Bersama dengan segala sesuatu yang tampak sedang berkembang sepanjang topik ini, semua pandangan Anda cenderung sangat menstimulasi. Meskipun demikian, saya minta maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh rencana Anda, meskipun radikal. Terlihat bagi kami bahwa pendapat Anda tidak benar-benar tervalidasi dan pada faktanya Anda sendiri tidak sepenuhnya pasti terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membaca.
Thank you for sharing excellent informations. Your site is so cool. I am impressed by the details that you’ve on this site. It reveals how nicely you understand this subject. Bookmarked this website page, will come back for more articles. You, my friend, ROCK! I found just the information I already searched all over the place and simply couldn’t come across. What a great website.
Great post. I used to be checking constantly this blog and I’m impressed! Extremely useful info specifically the remaining section 🙂 I maintain such information much. I used to be looking for this certain information for a very long time. Thanks and best of luck.
As I website owner I believe the content material here is real superb, thankyou for your efforts.
Saya senang bahwa saya menemukan blog ini, persis info yang saya cari!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Definitely believe that which you said. Your favorite justification seemed to be on the net the simplest thing to be aware of. I say to you, I certainly get annoyed while people consider worries that they plainly don’t know about. You managed to hit the nail upon the top and defined out the whole thing without having side effect , people could take a signal. Will likely be back to get more. Thanks
wonderful post, very informative. I wonder why the other
experts of this sector don’t realize this. You should continue your writing.
I’m sure, you have a huge readers’ base already!
I am not certain where you’re getting your info, however good topic. I must spend a while studying much more or understanding more. Thanks for magnificent information I was looking for this information for my mission.
Please let me know if you’re looking for a article writer for your
site. You have some really good posts and I believe I would
be a good asset. If you ever want to take some of the load off, I’d absolutely love to write some articles for your blog in exchange for a link back to mine.
Please send me an email if interested. Kudos!
Valuable info. Lucky me I found your web site by accident, and I am shocked why this accident didn’t happened earlier! I bookmarked it.
Hi, i read your blog from time to time and i own a similar one and i was just wondering if you get a lot of spam comments? If so how do you prevent it, any plugin or anything you can suggest? I get so much lately it’s driving me insane so any support is very much appreciated.
You have brought up a very wonderful details, appreciate it for the post.
Some truly great information, Gladiola I discovered this.
I’ve recently started a site, the information you provide on this site has helped me greatly. Thank you for all of your time & work. “The very ink with which history is written is merely fluid prejudice.” by Mark Twain.
Do you mind if I quote a couple of your posts as long as I provide credit and sources back to your weblog? My website is in the very same area of interest as yours and my visitors would truly benefit from a lot of the information you present here. Please let me know if this ok with you. Thank you!
Would you be taken with exchanging links?
It’s really a nice and helpful piece of information. I am satisfied that you just shared this useful info with us. Please stay us informed like this. Thanks for sharing.
Hello There. I found your blog using msn. That is an extremely well written article. I will make sure to bookmark it and return to read extra of your useful info. Thank you for the post. I’ll definitely return.
I do like the way you have presented this situation and it really does give us a lot of fodder for consideration. However, through what precisely I have observed, I simply trust when the actual responses pile on that folks continue to be on issue and in no way start on a tirade associated with the news of the day. Yet, thank you for this exceptional point and while I can not concur with the idea in totality, I value the perspective.
Thanks for the good writeup. It if truth be told used to be a enjoyment account it. Glance complicated to more delivered agreeable from you! By the way, how could we communicate?
Saya benar-benar ingin mengirim komentar singkat untuk mengucapkan terima kasih Anda atas seluruh saran luar biasa yang Anda bagikan di situs ini.
Postingan yang hebat. Saya benar-benar menyukai gaya Anda menyampaikan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
I enjoy you because of all your valuable hard work on this blog. My mom delights in carrying out internet research and it is simple to grasp why. Most of us learn all regarding the dynamic tactic you deliver precious strategies on your web blog and as well welcome response from other ones on that content then our daughter is now being taught a whole lot. Take pleasure in the remaining portion of the new year. You are performing a fantastic job.
Enjoyed examining this, very good stuff, regards. “Hereafter, in a better world than this, I shall desire more love and knowledge of you.” by William Shakespeare.
Amat jelas website, salam untuk pos ini.
Dengan semua hal yang mana tampak sedang berkembang sepanjang topik spesifik ini, banyak pandangan Anda ternyata lumayan menstimulasi. Kendati demikian, saya memohon maaf, karena saya tidak setuju sepenuhnya pada seluruh ide Anda, meskipun menarik. Terlihat bagi saya bahwa ulasan Anda tidak sepenuhnya sepenuhnya rasional dan pada faktanya Anda sendiri tidak sepenuhnya percaya diri terhadap pernyataan tersebut. Dalam hal apa pun saya menghargai membaca.
Terima kasih atas tulisan yang baik. Pada kenyataannya ini sebelumnya adalah sebuah akun hiburan. Terlihat rumit menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita bisa menjaga kontak?
Situs web ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Howdy! Someone in my Myspace group shared this site with us so I came to give it a look.
I’m definitely loving the information. I’m bookmarking
and will be tweeting this to my followers! Terrific blog and
great design.
Very interesting subject , regards for putting up.
You actually make it seem so easy with your presentation but I find this topic to be really something which I think I would never understand. It seems too complicated and extremely broad for me. I’m looking forward for your next post, I will try to get the hang of it!
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada sarana Anda dapat mengeluarkan saya dari layanan itu? Terima kasih!
Nyata bersih website, salam untuk posting ini.
Saya amat senang menemukan website ini di Bing, persis seperti yang saya telusuri : D demikian juga sudah saya simpan ke bookmark.
I’m now not certain the place you are getting your information, however good topic. I needs to spend some time learning more or understanding more. Thanks for great info I was looking for this info for my mission.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Appreciate it! An abundance of posts.
Saya mendapatkan info yang bagus dari blog Anda.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Postingan yang sangat baik. Ini jelas ditulis dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
Kami mungkin memiliki tautan perubahan perjanjian antara kita!
Postingan yang hebat. Ini memberikan saya pemahaman yang lebih jelas tentang topik ini. Teruskan pekerjaan yang hebat!
Halo semua, sekadar ingin mengatakan bahwa saya sangat menyukai membaca melalui postingan Anda. Saya tidak yakin mengapa tetapi saya merasakan banyak wawasan yang sangat berguna. Terima kasih!
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini istimewa. Pekerjaan yang mengagumkan!
Wah! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang sangat bagus!
Aku sungguh ingin menulis komentar singkat untuk menghargai Anda atas semua informasi luar biasa yang Anda tuliskan di situs ini.
What’s up everyone, it’s my first pay a quick visit at this website, and piece of writing is genuinely fruitful in support of me, keep up posting these articles or reviews.
Isi yang bermanfaat dan ditulis dengan sangat baik. Saya tentu akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Terima kasih untuk blog informatif lainnya. Di tempat mana lagi saya bisa mendapatkan informasi seperti itu yang ditulis dengan gaya yang sempurna? Saya memiliki sebuah tantangan yang saya sedang kerjakan sekarang, dan saya telah mencari informasi seperti ini.
Hello there, I found your web site via Google while looking for a related topic, your site came up, it looks great. I’ve bookmarked it in my google bookmarks.
Great beat ! I would like to apprentice while you amend your website, how could i subscribe for a blog site? The account helped me a acceptable deal. I had been a little bit acquainted of this your broadcast provided bright clear concept
Great post. I was checking continuously this blog and I am impressed! Very useful information specially the final part 🙂 I maintain such info a lot. I was looking for this particular information for a very lengthy time. Thanks and best of luck.
It’s really a great and helpful piece of information. I am glad that you shared this useful info with us. Please keep us up to date like this. Thanks for sharing.
You have remarked very interesting points! ps decent internet site.
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four e-mails with the same comment. Is there any way you can remove me from that service? Many thanks!
There are definitely lots of particulars like that to take into consideration. That is a nice level to convey up. I offer the thoughts above as general inspiration but clearly there are questions like the one you carry up where an important factor will be working in honest good faith. I don?t know if best practices have emerged round issues like that, but I’m certain that your job is clearly identified as a good game. Both girls and boys really feel the impression of just a second’s pleasure, for the rest of their lives.
Its like you learn my mind! You seem to know so much approximately this, like you wrote
the e book in it or something. I believe that you could do with some percent to drive the message house a little bit, but instead
of that, this is fantastic blog. An excellent read.
I’ll certainly be back.
Simply want to say your article is as surprising. The clearness in your post is simply excellent and i could assume you’re an expert on this subject. Fine with your permission let me to grab your RSS feed to keep updated with forthcoming post. Thanks a million and please keep up the gratifying work.
Lovely website! I am loving it!! Will come back again. I am taking your feeds also.
Bagaimanapun, terima kasih untuk poin yang hebat ini dan meskipun saya tidak sepakat sepenuhnya, saya menghargai pandangan.
Some genuinely howling work on behalf of the owner of this web site, perfectly outstanding written content.
Terima kasih atas tulisan yang bagus. Pada kenyataannya ini dulunya adalah sebuah akun hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Ngomong-ngomong, bagaimana kita bisa tetap berkomunikasi?
Perfectly composed content material, regards for entropy. “The last time I saw him he was walking down Lover’s Lane holding his own hand.” by Fred Allen.
Website ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menyadarinya.
I’m impressed, I need to say. Actually not often do I encounter a blog that’s each educative and entertaining, and let me inform you, you could have hit the nail on the head. Your concept is excellent; the problem is something that not sufficient persons are talking intelligently about. I’m very glad that I stumbled throughout this in my search for one thing referring to this.
Seseorang pada dasarnya membantu membuat posting yang sangat baik, saya akan katakan. Ini adalah pertama kali saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat publikasi khusus ini luar biasa. Pekerjaan yang luar biasa!
Hai di sana, saya menemukan blog Anda lewat Google ketika mencari topik yang serupa, website Anda tampil di bagian atas. Saya harus mengatakan bahwa saya terkejut betapa rapi pengaturannya. Saya benar-benar menyukai membaca ini dan saya akan kembali untuk membaca lebih banyak. Terima kasih banyak!
Hi there! Do you use Twitter? I’d like to follow you if that would be okay. I’m undoubtedly enjoying your blog and look forward to new updates.
Hello, i believe that i saw you visited my blog so i got here to
go back the prefer?.I am trying to in finding
things to enhance my site!I guess its good enough to use
a few of your concepts!!
You could definitely see your expertise in the work you write. The sector hopes for even more passionate writers like you who are not afraid to mention how they believe. Always go after your heart.
I know this web site gives quality dependent articles or reviews and extra information, is there any other
website which provides these kinds of things in quality?
wonderful submit, very informative. I ponder why the opposite experts of this sector do not realize this. You should proceed your writing. I am confident, you’ve a great readers’ base already!
Very interesting information!Perfect just what I was searching for!
Hey! This is my first visit to your blog! We are a group of volunteers and starting a new project in a community in the same niche. Your blog provided us valuable information to work on. You have done a wonderful job!
Aw, this was an exceptionally nice post. Spending some time and actual effort to make a superb article… but
what can I say… I procrastinate a whole lot and don’t manage to
get anything done.
Do you have a spam issue on this website; I also am a blogger, and I was curious about your situation; we have created some nice procedures and we are looking to exchange techniques with others, please shoot me an e-mail if interested.
Hello, I do think your site might be having web browser compatibility issues.
Whenever I look at your site in Safari, it looks fine but
when opening in Internet Explorer, it’s got some overlapping issues.
I simply wanted to give you a quick heads up!
Apart from that, excellent website!
First off I want to say terrific blog! I had a quick question that I’d
like to ask if you don’t mind. I was curious to find out how you center yourself and clear
your mind prior to writing. I’ve had trouble clearing my thoughts in getting my thoughts
out there. I do enjoy writing but it just seems like the first 10 to 15 minutes are usually lost just trying to figure out how to begin. Any recommendations or tips?
Appreciate it!
Saya terkesan dengan situs web ini, sangat saya adalah penggemar.
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada metode Anda mungkin bisa menghapus saya dari layanan itu? Terima kasih!
An interesting discussion is value comment. I feel that you need to write more on this subject, it won’t be a taboo subject however generally individuals are not enough to talk on such topics. To the next. Cheers
Seseorang secara esensial membantu untuk membuat sangat posting saya akan katakan. Itu adalah pertama kalinya saya mengunjungi halaman situs web Anda dan hingga kini? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun posting istimewa ini. Kerja yang fantastis!
Postingan yang hebat. Saya benar-benar menyukai gaya Anda menyampaikan ide-ide ini. Teruskan pekerjaan yang hebat!
Saya sangat menghargai usaha yang Anda luangkan untuk menyusun posting ini. Informasi yang berguna. Terima kasih banyak!
What’s up to every single one, it’s genuinely a nice for me
to go to see this website, it consists of important Information.
Fantastis blog yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin menjadi bagian dari komunitas di mana saya bisa mendapatkan masukan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Cheers!
Saya menghargai waktu yang Anda curahkan untuk menyusun posting ini. Konten yang bernilai. Terima kasih!
Hey! Do you know if they make any plugins to assist with SEO?
I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good gains.
If you know of any please share. Kudos!
Saya senang menjadi salah satu dari beberapa pengunjung di situs luar biasa ini (:, salam telah mengunggah.
Thank you for any other fantastic article. Where else may just anyone get that type of information in such a perfect approach of writing? I have a presentation next week, and I am on the look for such information.
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Hmm is anyone else having problems with the images on this blog loading?
I’m trying to figure out if its a problem on my
end or if it’s the blog. Any suggestions would be greatly appreciated.
Saya perlu mengatakan, ini adalah salah satu artikel terbaik yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Anda bisa pasti melihat keahlian Anda dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
Saya terkesan dengan website ini, sungguh saya adalah penggemar berat.
Saya sangat gembira menemukan website ini di Bing, persis seperti yang saya cari : D pula sudah saya simpan ke favorit.
Menikmati membaca keseluruhan ini, sangat bagus, sangat menghargai.
Postingan yang luar biasa. Ini memberi saya pemahaman yang lebih jelas tentang subjek ini. Teruskan kerja yang hebat!
Isi yang fantastis! Saya pasti akan kembali untuk membaca konten lainnya. Terima kasih atas informasi ini.
Saya terus memikirkan hal ini, terima kasih telah memposting.
This beginner guide clearly explains how to sell bitcoin in india.
Sangat baik informasi dapat ditemukan di blog.
Saya sungguh ingin menulis pesan singkat guna mengucapkan terima kasih Anda atas semua saran luar biasa yang Anda bagikan di website ini.
I just like the helpful information you supply to your articles.
I will bookmark your blog and check once more here regularly.
I’m quite sure I’ll be informed many new stuff right here!
Good luck for the next!
Excellent blog here! Also your web site loads up fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my site loaded up as quickly as yours lol
Hey There. I found your blog using msn. This is a very well written article.
I’ll be sure to bookmark it and come back to read more of your
useful information. Thanks for the post. I’ll certainly return.
Hi! I know this is somewhat off topic but I was wondering if you knew
where I could get a captcha plugin for my comment form?
I’m using the same blog platform as yours and I’m having trouble finding one?
Thanks a lot!
Very interesting info!Perfect just what I was looking for!
Menikmati mempelajari ini, sangat bagus, salam.
Sangat menarik info !Sempurna persis seperti yang saya cari! “Orang neurotik membangun istana di udara, orang psikotik tinggal di dalamnya. Ibu saya membersihkannya.” oleh Rita Rudner.
I was reading some of your posts on this site and I think this website is real informative! Retain putting up.
I believe this internet site has got some rattling wonderful info for everyone :D.
Hi there, i read your blog from time to time and i own a similar one and i was just wondering if you get a lot of
spam comments? If so how do you prevent it, any plugin or anything you
can suggest? I get so much lately it’s driving me mad so any assistance is very much appreciated.
Howdy! I’m at work surfing around your blog from my new apple iphone!
Just wanted to say I love reading your blog and look forward to all your posts!
Keep up the excellent work! https://m.auto-first.cn/adc/?url=https://rt.chat-rulet-18.com/
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga harimu menyenangkan. Bye
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Menikmati menelaah ini, sangat bagus, salam.
Thanks a lot for sharing this with all people you really recognize what you’re talking approximately! Bookmarked. Please also talk over with my web site =). We may have a hyperlink exchange contract among us!
Hai semua, sekadar ingin mengatakan bahwa saya sangat menyukai membaca menelusuri postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasa banyak wawasan yang sangat berguna. Terima kasih!
Terima kasih atas kritik yang masuk akal. Saya & tetangga saya baru saja bersiap untuk melakukan sedikit riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih jelas dari postingan ini. Saya sangat senang melihat informasi hebat dibagikan secara bebas.
Ini adalah tips yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan tepat… Terima kasih telah berbagi ini. Artikel yang wajib dibaca.
Hello, everything is going fine here and ofcourse every one is sharing information, that’s in fact excellent, keep up writing.
Hei, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini merupakan persis tipe informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Saya tidak bisa menahan diri untuk berkomentar
Saya selalu memikirkan hal ini, terimakasih telah memposting.
Bersama dengan seluruhnya yang mana tampak sedang berkembang di dalam topik khusus ini, semua pandangan Anda cenderung lumayan menstimulasi. Namun, saya minta maaf, karena saya tidak setuju sepenuhnya pada seluruh saran Anda, meskipun menyegarkan. Terlihat bagi kami bahwa komentar Anda tidak sepenuhnya benar-benar tervalidasi dan pada kenyataannya Anda diri Anda tidak benar-benar sepenuhnya pasti terhadap poin tersebut. Dalam hal apa pun saya menghargai membaca.
It’s a pity you don’t have a donate button! I’d without a doubt donate to this outstanding blog! I suppose for now i’ll settle for book-marking and adding your RSS feed to my Google account. I look forward to brand new updates and will share this website with my Facebook group. Chat soon!
Saya terkesan dengan situs ini, sangat saya adalah penggemar berat.
Sangat menarik poin yang Anda utarakan, terima kasih telah mengunggah. “Jive Lady Just hang loose blood. She gonna handa your rebound on the med side.” oleh Airplane.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Pretty section of content. I just stumbled upon your blog and in accession capital to assert that I acquire actually enjoyed account your blog posts. Any way I’ll be subscribing to your augment and even I achievement you access consistently rapidly.
Situs web ini benar-benar merupakan penjelasan menyeluruh untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Anda dapat jelas melihat keterampilan Anda dalam karya yang Anda tulis. Sektor berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu kejar hati Anda.
I loved as much as you will receive carried
out right here. The sketch is attractive, your authored subject matter stylish.
nonetheless, you command get got an shakiness over that
you wish be delivering the following. unwell unquestionably come more
formerly again since exactly the same nearly very often inside case you shield this hike.
I’m not that much of a online reader to be honest but your sites really nice, keep it up!
I’ll go ahead and bookmark your site to come back in the future.
Many thanks
Saya harus mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca dalam waktu yang lama. Konten yang sangat membantu. Terima kasih telah berbagi.
Terima kasih untuk situs web informatif lainnya. Di mana lagi saya memperoleh info seperti itu yang ditulis dengan pendekatan yang sempurna? Saya punya sebuah tantangan yang saya tengah jalankan, dan saya telah mengamati informasi seperti ini.
Terima kasih untuk website informatif tambahan. Di mana lagi saya memperoleh info seperti itu yang ditulis dengan cara yang sempurna? Saya punya sebuah proyek yang saya tengah kerjakan sekarang, dan saya sudah mencari informasi seperti ini.
Dengan hampir semuanya yang mana terlihat sedang berkembang sepanjang topik khusus ini, semua pandangan Anda cenderung cukup menstimulasi. Walaupun begitu, saya maaf, tetapi saya tidak dapat setuju sepenuhnya pada keseluruhan saran Anda, meskipun menarik. Terlihat bagi saya bahwa komentar Anda tidak benar-benar tervalidasi dan pada kenyataannya Anda diri Anda tidak sepenuhnya yakin terhadap argumen tersebut. Dalam hal apa pun saya menikmati membaca.
I have been examinating out many of your articles and i can claim pretty clever stuff. I will make sure to bookmark your website.
Konten yang fantastis! Cara penulisan Anda jelas dan mudah dimengerti. Saya pasti akan kembali untuk melihat konten lainnya.
Ini benar-benar menjawab masalah saya, terima kasih!
Menikmati menelusuri ini, sangat bagus, terima kasih.
Saya tidak benar-benar bagus dalam bahasa Inggris tetapi saya menyadari ini sangat ringan untuk ditafsirkan.
Great article! We will be linking to this great content on our website.
Keep up the great writing.
Saya benar-benar ingin menulis pesan singkat untuk mengucapkan terima kasih Anda atas seluruh tips luar biasa yang Anda bagikan di website ini.
Saya perlu mengatakan, ini adalah salah satu posting paling bagus yang pernah saya baca belakangan ini. Informasi yang sangat berguna. Terima kasih telah berbagi.
Good posts, Thank you.
Situs web ini benar-benar merupakan panduan lengkap untuk semua informasi yang Anda inginkan tentang hal ini dan tidak tahu kepada siapa harus bertanya. Lihat sekilas di sini, dan Anda pasti akan menemukannya.
Ini adalah saran yang sangat bagus, terutama bagi mereka yang masih baru di dunia blog, informasi yang ringkas dan akurat… Terima kasih telah berbagi ini. Tulisan yang harus dibaca.
Ini adalah saran yang sangat baik, terutama bagi mereka yang masih baru di dunia blog, informasi yang singkat dan tepat… Terima kasih telah berbagi ini. Artikel yang harus dibaca.
Anda telah melakukan pekerjaan yang luar biasa dan seluruh komunitas akan berterima kasih kepada Anda.
Saya selalu tertarik dengan subjek ini dan tetap masih demikian, terimakasih telah memposting.
Artikel yang hebat. Saya benar-benar menyukai cara Anda menjelaskan ide-ide ini. Teruskan pekerjaan yang luar biasa!
Wow! Ini mungkin salah satu blog paling bermanfaat yang pernah kami temui tentang topik ini. Pada dasarnya Luar biasa. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami kerja keras Anda.
Your means of describing everything in this paragraph is really good, every one can easily be aware of it, Thanks a lot.
Anda bisa pasti melihat antusiasme Anda dalam pekerjaan yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu ikuti hati Anda.
You actually make it appear really easy along with
your presentation however I find this matter to be actually one thing which I feel I
might never understand. It seems too complicated and very extensive for me.
I am taking a look forward in your next publish, I will try to get the dangle of it!
Look at my website: ผลฮานอย lottovip
Saya perlu mengatakan, ini adalah salah satu artikel paling bagus yang yang pernah saya baca belakangan ini. Konten yang sangat berguna. Terima kasih telah berbagi.
You could certainly see your enthusiasm in the work you write.
The arena hopes for more passionate writers like you who aren’t afraid to
say how they believe. All the time follow your heart.
Terima kasih untuk posting megah lainnya. Di mana lagi siapa pun dapat mendapatkan tipe info seperti itu dengan gaya penulisan yang ideal? Saya memiliki presentasi minggu berikutnya, dan saya berada mencari informasi seperti ini.
Saved as a favorite, I really like your blog!
Wohh tepat apa yang saya telusuri, salam atas posting.
It’s really a nice and helpful piece of information. I am glad that you shared this helpful info with us. Please keep us informed like this. Thanks for sharing.
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
Saya tidak umumnya berkomentar tetapi saya harus mengakui terima kasih untuk posting yang luar biasa ini : D.
Kami akan memiliki hyperlink perdagangan perjanjian di antara kita!
Saya harus mengatakan, ini adalah salah satu artikel paling bagus yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Ini adalah topik yang sangat penting di hati saya, cheers, tapi di mana informasi kontak Anda?
Ini adalah topik yang sangat dekat di hati saya, salam, tapi di manakah detail kontak Anda?
Thanks for helping out, excellent info. “The four stages of man are infancy, childhood, adolescence, and obsolescence.” by Bruce Barton.
누군가가 블로그 및 사이트 구축에 대한 전문가의 견해가 필요하다면, 이 웹페이지를 방문하라고 제안합니다.
멋진 작업을 계속하세요.
Hmm is anyone else encountering problems with the pictures on this blog
loading? I’m trying to figure out if its a problem on my end or
if it’s the blog. Any responses would be greatly appreciated.
Hello, i feel that i saw you visited my site thus i came to “return the choose”.I am trying to find issues to enhance my site!I assume its adequate to make use of some of your ideas!!
That is the suitable weblog for anyone who desires to search out out about this topic. You realize a lot its almost arduous to argue with you (not that I really would want…HaHa). You undoubtedly put a brand new spin on a topic thats been written about for years. Great stuff, just nice!
Hi there! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing months of hard work due to no data backup. Do you have any solutions to protect against hackers?
Thanks for one’s marvelous posting! I genuinely enjoyed reading it, you are a great author.I will make certain to bookmark your blog and will eventually come back someday. I want to encourage you to continue your great writing, have a nice morning!
Utterly indited content material, appreciate it for information .
Hello my family member! I wish to say that this article is awesome, nice written and include almost all vital infos. I’d like to peer extra posts like this.
It’s amazing to pay a quick visit this website and reading
the views of all friends about this piece of writing, while
I am also zealous of getting know-how.
Terrific post however , I was wondering if you could write a litte more on this topic? I’d be very grateful if you could elaborate a little bit more. Thanks!
Thanks a bunch for sharing this with all of us you actually realize what you are speaking approximately! Bookmarked. Kindly also talk over with my web site =). We could have a link exchange agreement among us!
Great content, Many thanks!
Also visit my site – https://www.skinhudlaege.dk/tidsbestilling
I have been exploring for a bit for any high
quality articles or blog posts in this sort of area .
Exploring in Yahoo I eventually stumbled upon this site.
Reading this info So i am happy to exhibit that I’ve a very excellent uncanny
feeling I found out just what I needed. I so much indisputably will make certain to don?t omit this web
site and give it a look regularly.
Saved as a favorite, I really like your blog!
very good post, i certainly love this web site, carry on it
I still remember the moment, but the day I stepped into the backend of the sports world, everything I thought I
knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw
how the entire industry had turned into this multi-layered financial machine, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers”
anymore. They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really is between order and total digital
disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines.
One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially
the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually
works, they can always look it up directly from the source.
The full explanations are there, and they’re
honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of sponsorship deals
— things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had become
a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring, but
now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching
the digital version of an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did
an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting
more information directly from the source. It’s all publicly
explained — and believe me, once you read
it, you’ll never look at sports or betting the same
way again.
It’s an amazing post designed for all the web people; they will get advantage from it
I am sure.
Do you mind if I quote a few of your posts as long
as I provide credit and sources back to your webpage?
My blog site is in the exact same niche as
yours and my users would genuinely benefit from some of the information you provide here.
Please let me know if this alright with you. Many thanks!
It’s not my first time to visit this web site,
i am visiting this website dailly and take good data from here everyday.
I keep listening to the rumor speak about getting boundless online grant applications so I have been looking around for the best site to get one. Could you tell me please, where could i acquire some?
Yay google is my king aided me to find this outstanding site! .
Keep this going please, great job!
I am extremely impressed with your writing skills as well as with the layout
on your blog. Is this a paid theme or did you modify it
yourself? Anyway keep up the excellent quality writing,
it is rare to see a nice blog like this one today.
I just like the valuable information you supply to your articles.
I will bookmark your blog and check once more right
here frequently. I’m fairly certain I will learn many new stuff right right here!
Good luck for the next!
Very good info. Lucky me I found your website by chance
(stumbleupon). I have bookmarked it for later!
Hi there, this weekend is good for me, as this time i am reading this fantastic informative post here at my residence.
What a data of un-ambiguity and preserveness of valuable knowledge on the topic of
unexpected feelings.
Heya i am for the primary time here. I found this board and I find It truly helpful
& it helped me out much. I hope to present something again and aid
others such as you helped me.
Good article. I am going through some of these issues as well..
Sangat menarik poin yang Anda sebutkan, salam telah mengunggah. “Cara paling pasti untuk menyingkirkan orang yang membosankan adalah meminjamkan uang kepadanya.” oleh Paul Louis Courier.
Hello there, I discovered your website by means of Google even as looking for a related topic, your website came up,
it seems to be great. I have bookmarked it
in my google bookmarks.
Hi there, just turned into alert to your blog thru Google, and located that it’s truly informative.
I’m going to watch out for brussels. I’ll be grateful when you continue
this in future. Lots of people might be benefited from your writing.
Cheers!
I wanted to thank you for this wonderful read!!
I certainly loved every little bit of it. I have you book-marked to look at new stuff you post…
Yes! Finally something about migliore casinò online
estero.
This is a very good tip particularly to those new to the blogosphere.
Short but very precise info… Thank you for
sharing this one. A must read post!
Saya perlu mengatakan, ini adalah salah satu artikel paling bagus yang yang pernah saya baca dalam waktu yang lama. Informasi yang sangat membantu. Terima kasih telah berbagi.
Hai di sana, Anda telah melakukan kerja yang luar biasa. Saya pasti akan menyimpan ini dan kembali untuk membaca konten lainnya. Terima kasih banyak!
Many Singapore parents tᥙrn to primary math tuition to make
sure their children stay on track ԝith the demanding MOE syllabus аnd prevent lagging compared to classmates.
Numerous Singapore parents choose secondary-level math tuition tߋ
ensure tһeir children remaіn ahead in аn environment whеre subject streaming heavily reky ⲟn mathematics reѕults.
JC math tuition holds рarticular vaⅼue for students targeting prestigious university pathways ⅼike compսter
science, economics, actuarial science, оr data analytics, ѡһere excellent Н2 Mathematics grades
serves аs a key admission requirement.
Іn Singapore’ѕ fast-paced and highly competitive education ѕystem, virtual mathematics tutoring һas emerged аs
a vital resource for primary students, offering flexible scheduling ɑnd
tailored individual support tо һelp yoᥙng learners thorouցhly understand foundational PSLE topics ⅼike fractions, ratios аnd
speed-distance ρroblems from home ᴡithout rigid centre schedules.
Inevitably, OMT’ѕ th᧐rough services weave pleasure гight
int᧐ mathematics education, aiding trainees drop
deeply crazy ɑnd soar in their exams.
Expand your horizons wіth OMT’s upcoming brand-neѡ physical area օpening іn September 2025,
offering a l᧐t more opportunities fоr hands-on mathematics expedition.
Singapore’ѕ focuus օn critical believing
tһrough mathematics highlights tһе іmportance оf
math tuition, wһich assists trainees establish tһe analytical skills required ƅy tһe country’s forward-thinking curriculum.
Tuition programs fоr primary school math concentrate ߋn mistake analysis
from past PSLE papers, teaching students t᧐ avoid repeating
mistakes іn computations.
Secondary math tuition conquers tһe limitations oof bіg class
dimensions, ցiving concentrated focus tһat improves understanding for O Level prep ԝork.
Getting ready fоr the changability of A Level concerns, tuition develops adaptive analytic
techniques f᧐r real-time exam situations.
Ꮤhat sets OMT apart is its personalized syllabus tһat
aligns ѡith MOE whіle providing flexible pacing, allowing innovative students t᧐ increase tһeir learning.
Selection оf practice inquiries ѕia, preparing ʏou cօmpletely
fߋr any kіnd of math examination and better scores.
Tuition reveals trainees tο diverse inquiry kinds, expanding tһeir readiness for unpredictable Singaporte
mathematics tests.
mʏ blog – math tuition centre
I think that is one of the such a lot important info for me.
And i’m satisfied reading your article. But want to commentary on some general things, The site
style is perfect, the articles is in reality nice : D.
Just right job, cheers
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex izle,sikiş videoları,sikiş izle,
seks izle,seks videoları,porno,Porno Film izle,Sex Seyret,Mobil Sikiş,
Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno izle,sarhoş
pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,Porno Anne,
Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,
abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,
porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep tayyip erdogan sikiş,recep
tayyip erdogan sex,İsmet İnönü porno,Celal Bayar porno,Cemal
Gürsel porno,Cevdet Sunay porno,Fahri Korutürk
porno,Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah
Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut
Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,Binali Yıldırım porno,
Ahmet Davutoğlu porno,Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü
porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif Şener porno,Mehmet Şimşek
sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,
İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal
Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş
ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,
Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek ifşa,Recep
Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet
Şimşek Porno ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya
Porno ifşa,Yılmaz Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno
ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat Kurum Porno
ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat Porno ifşa,İbrahim Yumaklı
Porno ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak
Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,
brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel
Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno ifşa,Tuncer Bakırhan Porno ifşa,
Müsavat Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,
Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal
Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit
Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih Karahan Porno ifşa,Ali
Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,Mansur Yavaş
Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,
Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno
ifşa,Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras
Porno ifşa,Cevdet Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah
Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım Porno
ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç Porno ifşa,
Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno
ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno
ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi
Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya
Yanık Porno ifşa,Mustafa Şentop Porno ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,
Mehmet Metiner Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,Mustafa
Destici Porno ifşa,Ümit Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör
Geçer Porno ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,
Koç Ailesi Porno ifşa,Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,Esas Holding
Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı ve Ailesi
Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding
Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding
Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,
Üs Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu
Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı Holding Porno ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno ifşa,
Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,
Yıldırım Ailesi Porno ifşa,Yıldırım Holding Porno ifşa,
M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,Sevda-Serra Sabancı Porno
ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner
Porno ifşa,Ciner Grubu Porno ifşa,Mehmet Cengiz Porno
ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno ifşa,
Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa
Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno ifşa,Çolakoğlu Grubu
Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno
ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno
ifşa,Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi
Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,
Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,
Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,
Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno ifşa,Alaton Ailesi Porno ifşa,
Alarko Holding Porno ifşa,Garih Ailesi Porno
ifşa,Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar
Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi
Porno ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,
Demet Sabancı Çetindoğan Porno ifşa,Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,
Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu
Porno ifşa,Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça
Holding Porno ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC
Holding Porno ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner
Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker
Ailesi Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi
Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi
Porno ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi Porno
ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök Porno
ifşa,Atlantik Holding Porno ifşa,Nilüfer Dinçkök Çiftçi Porno ifşa,
Yalçın Sabancı Porno ifşa,Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet
Porno ifşa,Yaşar Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu
Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu
Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay
Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi
Porno ifşa,Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu
Porno ifşa,Gürsel Ailesi Porno ifşa,Kiska
Holding Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu
Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,Kiler Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi
Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor
Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno
ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
When I initially commented I clicked the “Notify me when new comments are added” checkbox and
now each time a comment is added I get three e-mails with
the same comment. Is there any way you can remove people
from that service? Cheers!
Quality content is the important to be a focus for the people to pay a quick
visit the website, that’s what this web page is
providing.
This site definitely has all of the information and facts I needed about this subject and didn’t know who to ask.
作为中国最具影响力的输入法产品之一,搜狗输入法(Sougou 输入法)凭借强大的智能引擎和丰富的功能模块赢得了广大用户的青睐。这里为你准备了最新的 搜狗输入法下载 通道,提供官网正版的安装资源,支持在 Windows 和 Mac 等多种平台上下载安装与使用。搜狗输入法拥有业内领先的智能词库和智能联想技术,可以根据用户习惯实时优化输入结果,提高整体打字效率。它支持拼音、笔画、五笔、智能ABC 等多种输入方式,并具备语音输入与手写输入等便捷功能,适合不同用户习惯。除了实用功能之外,搜狗输入法还提供丰富的主题皮肤和表情包,让你打字时也能体验美观的界面与个性化视觉效果。在下载过程中,本站提供的链接均来源于
搜狗输入法官网 官方正版,不含任何捆绑软件,安全可靠。如果你希望提升中文输入速度、享受智能输入体验,就不要错过这一强大的工具。现在就点击下载最新版搜狗输入法,开启更高效、更智能的中文输入之旅!
Hello there, just became alert to your blog through Google, and found that it is really informative.
I’m going to watch out for brussels. I will appreciate if you continue this in future.
Numerous people will be benefited from your writing.
Cheers!
Please let me know if you’re looking for a article writer for your weblog.
You have some really good articles and I think I would be a good asset.
If you ever want to take some of the load off, I’d really like to write some articles for your blog in exchange for a link back to mine.
Please blast me an email if interested. Thanks!
These are truly fantastic ideas in about blogging. You have touched
some pleasant factors here. Any way keep up wrinting.
Great blog here! Also your site loads up very fast!
What web host are you using? Can I get your affiliate link to your host?
I wish my website loaded up as fast as yours lol
In a society where academic performance ցreatly shapes
future opportunities, many Singapore families ѕee еarly primary math
tuition аs a prudent long-term decision fοr sustained success.
Іn Singapore’s rigorous secondary education landscape, math tuition Ƅecomes indispensable fօr students to confidently conquer challenging topics ѕuch as algebra, geometry, trigonometry, ɑnd statistics tһat form the core
foundation for O-Level achievement.
А laгge proportion of JC students rely heavily оn math
tuition to gain mastery оver and refine sophisticated proƄlem-solving techniques f᧐r the abstract, proof-oriented questions that define Н2 Math examination papers.
Ꭲhe growing popularity օf virtual А-Level
mathematics support іn Singapore һas made high-calibre instruction accessible еven to JC students balancing co-curricular activities and academics, ԝith on-demand replays enabling
efficient, stress-free revision ⲟf both pure aand statistics
components.
OMT’ѕ neighborhood fforums enable peer ideas, ԝһere shared mathematics insights stimulate love аnd
cumulative drive fօr examination quality.
Experience flexible knowing anytime, аnywhere throᥙgh OMT’ѕ thorоugh online е-learning platform,
featuring unlimited access tߋ video lessons
aand interactive quizzes.
Ꮃith students іn Singapore Ƅeginning official math education fгom the firѕt day and facing high-stakes evaluations, math tuition ᥙѕes tһe additional edge required
tօ achieve tοp performance in thіѕ essential subject.
Improving primary education ԝith math tuition prepares trainees fօr PSLE
bу cultivating a development fгame of mind toᴡard challenging subjects liҝe balance and transformations.
Building confidence ᴡith constant tuition assistance іs crucial,
as O Levels can be demanding, and positive students carry ⲟut mucһ bеtter undеr pressure.
Ultimately, junior college math tuition іs vital to securing top
A Level resᥙlts, opening doors to distinguished scholarships аnd һigher education ɑnd learning chances.
OMT’ѕ proprietary educational program enhances MOE requirements tһrough an ɑll natural technique that nurtures ƅoth scholastic skills and an enthusiasm fοr mathematics.
OMT’ѕ e-learning minimizes mathematics stress аnd anxiety lor, mɑking you a ⅼot mоre confident
and causing hіgher examination marks.
Math tuition constructs ɑ solid portfolio ߋf abilities, enhancing Singapore students’ resumes fоr scholarships based οn exam
outcomes.
Visit mʏ page :: secondary 4 math
I blog quite often and I really appreciate your content. The article
has really peaked my interest. I am going to take a note of your
blog and keep checking for new details about once per
week. I opted in for your Feed as well.
Consistent primary math tuition helps ʏoung learners
overcome common challenges ѕuch as model drawing and rapid calculation skills, ѡhich are heavily tested іn school examinations.
Numerous Singapore parents invest іn secondary-level math tuition tⲟ maintain а
strong academic edge іn an environment wheгe subject streaming heavily rely оn mathematics results.
A larցe proportion of JC students rely heavily ⲟn math tuition to develop profound conceptual insight аnd sharpen advanced strategies fߋr the conceptually deep and proof-based questions tһat
characterise H2 Math examination papers.
Тhe growing popularity of virtual A-Level mathematics support іn Singapore һaѕ maɗe high-calibre instruction accessible еven t᧐ JC students balancing сo-curricular activities and academics, ᴡith
recorded sessions enabling efficient, stress-free revision ߋf bοtһ pure and
statistics components.
Interdisciplinary web ⅼinks in OMT’s lessons reveal
math’ѕ adaptability, stimulating curiosity ɑnd inspiration for exam achievements.
Unlock үouг child’s сomplete potential in mathematics with
OMT Math Tuition’ѕ expert-led classes, tailored tⲟ Singapore’s
MOEcurriculum for primary school, secondary, ɑnd JC students.
In Singapore’s extensive education ѕystem, ԝhere mathematics іѕ mandatory аnd takes
in around 1600 h᧐urs of curriculum tіme in primary school and
secondary schools, math tuition ƅecomes vital tο һelp students constduct а strong foundation f᧐r
long-lasting success.
Ꮃith PSLE math concerns frequently involving real-ԝorld
applications, tuition օffers targeted practice tо develop crucial believing skills vital fⲟr higһ ratings.
Secondary math tuition ցets rid of the restrictions of bіg class dimensions,
offering concentrated focus tһat enhances understanding fοr OLevel preparation.
Tuition integrates pure ɑnd used mathematics perfectly,
preparing students foг the interdisciplinary nature ᧐f A Level troubles.
OMT’ѕ proprietary curriculum complements tһe MOE educational program Ьy providing detailed malfunctions οf complex subjects,
guaranteeing students construct ɑ stronger fundamental understanding.
Detailed options ցiven on the internet leh, training yоu hօw to resolve troubles correctly fߋr far Ƅetter qualities.
Singapore parents purchase math tuition tо ensure tһeir kids fulfill tһе
high assumptions of tһе education and learning systеm
foг test success.
Ꮋere is my site … math tuition reviews Singapore
I read this paragraph completely regarding the difference of hottest and earlier technologies, it’s amazing article.
Tulis lebih banyak, hanya itu yang ingin saya katakan. Secara harfiah, sepertinya Anda mengandalkan video untuk menyampaikan poin Anda. Anda pasti tahu apa yang Anda bicarakan, mengapa membuang kecerdasan Anda hanya dengan memposting video ke weblog ketika Anda bisa memberi kami sesuatu yang mencerahkan untuk dibaca?
I would like to thank you for the efforts you have put in penning this website.
I’m hoping to see the same high-grade content by you later on as well.
In fact, your creative writing abilities has motivated
me to get my own, personal website now 😉
I always used to read post in news papers but now as I am a user of net therefore from now I am using net for posts, thanks to web.
Superb material. Kudos!
I truly enjoy reading on this web site, it holds superb blog posts. “A man of genius has been seldom ruined but by himself.” by Samuel Johnson.
In a society whеre academic performance heavily determines future opportunities, countless Singapore families ѕee еarly primary math
tuition аs a smart proactive step for sustained success.
Math tuition ⅾuring secondary years strengthens complex ⲣroblem-solving skills, ԝhich prove essential ƅeyond tests future pursuits іn STEMfields, engineering, economics,
ɑnd data-reⅼated disciplines.
Іn Singapore’s intensely demanding JC landscape, tuition fоr H2 Mathematics
proves indispensable fоr students to deeply understand complex concepts lіke vectors,
complex numЬers, sequences and series, probability, аnd statistical methods tһat carry significant weight in A-Level papers.
Іn Singapore’ѕ faѕt-paced ɑnd highly competitive education ѕystem, remote math lessons һas emerged
aѕ a preferred choice fоr primary students, offering flexible scheduling
аnd personalised one-tо-one guidance tⲟ help young
learners firmly grasp foundational PSLE topics including
heuristics ɑnd model method fr᧐m home wіthout rigid centre schedules.
Personalized advice fгom OMT’s experienced tutors aids pupils overcome mathematics hurdles, cultivating ɑ
heartfelt connection tߋ tһe subject ɑnd inspiration foг tests.
Ϲhange mathematics challenges іnto triumphs with OMT Math Tuition’ѕ
blend օf online and on-site alternatives, ƅacked by a performance history ߋf traiee excellence.
As math forms tһе bedrock оf sensiЬⅼe thinking and vital problem-solving inn
Singapore’ѕ education ѕystem, professional math tuition ρrovides the tailored assistance needеd to tսrn challenges
into triumphs.
Ԝith PSLE math questions ߋften involving real-world applications, tuition supplies targeted practice tо
develop vital believing skills іmportant fοr high ratings.
Alternative development ԝith math tuition not
јust enhances О Level scores уet additionally ɡrows ѕensible reasoning abilities
beneficial fⲟr lifelong understanding.
Personalized junior college tuition assists connect tһe space from O Level to A Level math, mɑking certain trainees adapt tօ the boosted rigor аnd deepness cаlled
fоr.
OMT sets apart with ɑn exclusive educational program
tһat sustains MOE content uѕing multimedia
assimilations, ѕuch аs video clip explanations ᧐f
key theories.
OMT’s online neighborhood proᴠides support leh,ԝherе you
can ask questions and improve your learning f᧐r far better
grades.
Вy concentrating on error evaluation, math tuition avoids recurring
blunders tһat might set yⲟu back priceless marks іn Singapore exams.
ᒪ᧐ok at my web blog: o level maths tuition singaopre
Hi there very nice web site!! Guy .. Excellent ..
Wonderful .. I will bookmark your site and take the feeds additionally?
I am happy to search out so many useful info
here within the put up, we’d like develop extra
strategies in this regard, thank you for sharing.
. . . . .
Excellent blog here! Also your web site loads up fast! What web host are you using?
Can I am getting your associate hyperlink in your host?
I wish my site loaded up as fast as yours lol
Hi there! I could have sworn I’ve been to your blog before
but after looking at some of the articles I realized it’s new to me.
Anyhow, I’m definitely delighted I stumbled upon it
and I’ll be book-marking it and checking back frequently!
Saya umumnya tidak meninggalkan komentar, tetapi yang satu ini benar-benar layak. Konten yang sangat baik dan berguna. Terima kasih banyak telah meluangkan waktu untuk menulis ini.
Wow, keren blog tata letak! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan web site Anda hebat, serta kontennya!
It’s laborious to find knowledgeable individuals on this topic, however you sound like you already know what you’re talking about! Thanks
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex izle,sikiş videoları,sikiş izle,
seks izle,seks videoları,porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno izle,sarhoş
pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,Porno Anne,Porno izlesene,Sikiş Video,HD
Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,porno
porno,porn porn,milli porno,Drunk Porn,recep
tayyip erdoğan porno,recep tayyip erdogan,recep
tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü
porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,
Fahri Korutürk porno,Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes porno,Bülent Ecevit porno,
Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz
Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex
kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem
sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım
Akbulut sex kaseti,Hasan Celal Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,
Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil
Çiçek ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno
ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno
ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet Nuri
Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar Porno
ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir
Uraloğlu Porno ifşa,Ömer Bolat Porno ifşa,İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno
ifşa,Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno
ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel
Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno ifşa,
Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno
ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut
Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno
ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit Porno ifşa,Selçuk
Bayraktaroğlu Porno ifşa,Fatih Karahan Porno ifşa,Ali
Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,
Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek
Porno ifşa,Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno ifşa,
Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,
Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil
Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül
Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım Porno
ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç
Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı Porno
ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno ifşa,Mustafa
Şentop Porno ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi
Porno ifşa,Gülşah Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,Sırrı
Süreyya Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail
Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit Özdağ Porno ifşa,Muharrem
İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri
Aslan Porno ifşa,Güngör Geçer Porno ifşa,Büşra Özdemir
Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi
Porno ifşa,Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,Esas Holding Porno ifşa,Erol Sabancı
ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı ve Ailesi Porno ifşa,
Tara Ailesi Porno ifşa,Enka Holding Porno ifşa,Eczacıbaşı
Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur
Ailesi Porno ifşa,Üs Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi
Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu Porno
ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno
ifşa,Tosyalı Holding Porno ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno
ifşa,Borusan Holding Porno ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,
Yıldırım Ailesi Porno ifşa,Yıldırım Holding Porno ifşa,M.
Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,Mehmet Başaran Porno ifşa,
Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,
Sevda-Serra Sabancı Porno ifşa,Gülçelik Ailesi Porno ifşa,
Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,Mehmet
Cengiz Porno ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno
ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno
ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat Porno ifşa,
Sezai Bacaksız Porno ifşa,Demir Sabancı
Porno ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno
ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu
Ailesi Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi
İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet
Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno ifşa,
Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih Ailesi Porno ifşa,Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,
Yamantürk Ailesi Porno ifşa,Güriş Holding Porno
ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi
Porno ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,
Demet Sabancı Çetindoğan Porno ifşa,Demsa Group Porno ifşa,
Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno
ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno ifşa,Lodrik Ailesi
Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,Yahya Kiğılı Porno
ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding
Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding Porno ifşa,
Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno
ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi Porno ifşa,Eti Grubu Porno
ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök
Holding Porno ifşa,Ömer Dinçkök Porno ifşa,Atlantik Holding Porno ifşa,Nilüfer Dinçkök
Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,Yasa
Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno
ifşa,Yaşar Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno
ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay
Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,
Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno
ifşa,Kiska Holding Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno
ifşa,Yıldızlar Yatırım Holding Porno ifşa,
Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu Porno ifşa,
Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,
Kiler Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,
Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,Karamancı
Ailesi Porno ifşa,Orta Anadolu Tekstil Porno ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi
Porno ifşa,Erbakır Porno ifşa
Isi yang luar biasa! Gaya penulisan Anda sangat jelas dan mudah dipahami. Saya tentu akan kembali untuk membaca lebih banyak.
Hei semua, hanya ingin mengatakan bahwa saya sangat menikmati membaca menelusuri postingan Anda. Saya tidak tahu pasti mengapa tetapi saya merasakan cukup banyak wawasan yang bermanfaat. Terima kasih!
I think the admin of this web site is actually working hard in support
of his web site, since here every stuff is quality based stuff.
This is a great tip especially to those fresh to the blogosphere.
Simple but very accurate information… Thank you for sharing this one.
A must read post!
Great article! This is the kind of information that are meant
to be shared across the internet. Shame on the seek engines for now not positioning this publish higher!
Come on over and seek advice from my web site .
Thanks =)
What a stuff of un-ambiguity and preserveness of precious knowledge concerning
unpredicted feelings.
Wonderful beat ! I would like to apprentice even as you
amend your web site, how could i subscribe for a blog website?
The account aided me a appropriate deal. I had been a little bit familiar of this your broadcast provided
brilliant clear idea
With havin so much written content do you ever run into any issues of plagorism or copyright infringement?
My blog has a lot of completely unique content I’ve either written myself or outsourced but it looks
like a lot of it is popping it up all over the internet without my authorization.
Do you know any methods to help stop content from being ripped off?
I’d certainly appreciate it.
I was recommended this blog via my cousin. I am not certain whether this post
is written through him as nobody else know such designated about my difficulty.
You are wonderful! Thanks!
Hei di sana, sekadar ingin mengatakan bahwa saya benar-benar menikmati membaca menelusuri postingan Anda. Saya tidak yakin mengapa tetapi saya merasa banyak informasi yang bermanfaat. Terima kasih!
Wohh tepat apa yang saya telusuri, terima kasih atas unggahan.
It’s an awesome piece of writing designed for
all the online viewers; they will get advantage from it
I am sure.
I pay a visit each day some sites and information sites to read articles or reviews, except this website gives feature
based articles.
Need an affordable bail bonds company? Your search ends at
our experienced bondsmen for prompt bail bond solutions.
You can get quick release services at affordable rates.
Call our licensed bondsmen anytime to secure quick release.
https://www.google.com/url?q=https://cailbailbonds.com/
Hai semua, saya menemukan website Anda lewat Google saat menelusuri subjek yang mirip, situs Anda tampil di hasil teratas. Saya harus mengatakan bahwa saya terkejut seberapa baik penyusunannya. Saya benar-benar menyukai membaca ini dan saya akan kembali untuk membaca lebih banyak. Terima kasih!
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
you are in point of fact a good webmaster.
The website loading velocity is incredible. It seems that you’re doing any distinctive trick.
In addition, The contents are masterpiece. you have performed a great job in this
topic!
Thank you, Loads of content.
What’s up, this weekend is nice in favor of me, because this point
in time i am reading this great informative post here at my home.
I take pleasure in, lead to I discovered just what I was looking
for. You have ended my four day lengthy hunt!
God Bless you man. Have a nice day. Bye
I really like what you guys are usually up too. This kind of clever
work and exposure! Keep up the amazing works guys I’ve included you
guys to blogroll.
Sangat menarik informasi!Sempurna persis seperti yang saya cari! “Inti dari menyelesaikan sesuatu adalah mengetahui apa yang harus dibiarkan tidak dilakukan.” oleh Lady Reading.
I used to be suggested this blog by way of my cousin. I’m now not sure whether this publish is written through him as nobody else know such targeted about my problem. You’re amazing! Thanks!
certainly like your web-site however you have to test the spelling on several of your posts. A number of them are rife with spelling problems and I find it very troublesome to inform the truth however I will surely come back again.
My family members always say that I am killing my time here at web, except I
know I am getting know-how all the time by reading such fastidious posts.
Valuable forum posts Cheers.
Wow! Terima kasih! Saya secara terus membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke website saya?
Wow, this article is nice, my younger sister is analyzing these things, thus I
am going to let know her.
Having read this I thought it wwas extremely enlightening.
I appreciate you finding the time and energy to put this informative article
together. I once again find myself spendimg a significant amount of time both reading and posting
comments. But so what, it was still woorth it!
Mɑny Singapore parents tᥙrn to primary math tuition tօ
ensure tһeir children кeep pace in the demanding MOE syllabus ɑnd ɑvoid falling ƅehind compared to classmates.
Secondary math tuition plays а pivotal role іn bridging understanding shortfalls, ⲣarticularly during
tһe shift from primary heuristic methods tо the more abstract аnd theoretical content introduced іn secondary school.
Ӏn addіtion to examination гesults, high-quality JC math tuition develops lasting intellectual resilience, sharpens һigher-оrder reasoning,
and readies candidates effectively f᧐r the analtical rigour of university-level study
іn STEM and quantitative disciplines.
Тhе growing popularity ߋf online math tuition іn Singapore һas
made top-quality tutoring accessible еven to JC students juggling CCAs
аnd heavy workloads, ᴡith recorded sessions enabling efficient, stress-free revision оf bօth pure
and statistics components.
Versatile pacing іn OMT’ѕ e-learning allows students savor math success, constructing deep love ɑnd motivation fⲟr exam performance.
Unlock уour child’ѕ comρlete potential іn mathematics witһ OMT Math Tuition’ѕ
expert-led classes, customized to Singapore’s MOE syllabus fߋr primary school, secondary, and JC students.
Ꮃith mathematics integrated seamlessly іnto Singapore’ѕ class settings to benefit ƅoth teachers and trainees, dedicated math tuition amplifies tһese gains bʏ providing tailored support fοr sustained achievement.
Tuition emphasizes heuristic ρroblem-solving techniques,
іmportant f᧐r dealing ᴡith PSLE’ѕ tough word issues tһat require multiple steps.
Linking math concepts tօ real-world circumstances via tuition ɡrows understanding,
mɑking O Level application-based inquirids
mߋге friendly.
Tuition ѕhows mistake evaluation strategies, helping junior college pupils
аvoid typical challenges іn Α Level computations and evidence.
OMTstands оut with itѕ syllabus designed tօ sustain MOE’s by incorporating mindfulness strategies tо
decrease mathematics anxiety tһroughout rеsearch studies.
Νo demand to tɑke a trip, just visit from home leh, saving
time to resеarch moгe and push yoᥙr math grades һigher.
Οn-line math tuition supplies adaptability fоr hectic Singapore trainees, enabling anytime accessibility tⲟ resources
for mսch bеtter exam preparation.
안녕하세요, 저는 kavin입니다, 처음으로 아무데서 댓글을 남기는 중입니다, 이 포스트을 읽고 이 훌륭한
단락 때문에 댓글을 남길 수 있다고 생각했습니다.
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sepenuhnya berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna desain yang luar biasa!
Artikel yang luar biasa. Ini memberi saya gambaran yang lebih jelas tentang topik ini. Teruskan kerja yang luar biasa!
Hi there I am so happy I found your site, I really found you by accident, while I was researching on Aol for something else, Regardless I am here now and would just
like to say kudos for a remarkable post and a all round thrilling blog (I also
love the theme/design), I don’t have time to browse it all
at the minute but I have saved it and also added your RSS feeds, so when I have time I will be back to read
a great deal more, Please do keep up the great work.
You actually said that very well!
Saya mendapatkan info yang bagus dari blog Anda.
Why people still make use of to read news papers when in this technological world everything is accessible on net?
This is really interesting, You are a very skilled blogger.
I have joined your rss feed and look forward to seeking more of your fantastic post.
Also, I have shared your website in my social networks!
Wohh baru saja apa yang saya cari, terimakasih atas unggahan.
What’s up mates, how is the whole thing, and what you wish for to say concerning this article,
in my view its truly remarkable for me.
Kudos! I enjoy this.
Hi to every one, because I am truly eager of reading this blog’s post to
be updated regularly. It consists of good stuff.
I visited multiple blogs but the audio feature for audio songs
current at this web page is really excellent.
Wow that was odd. I just wrote an very long
comment but after I clicked submit my comment didn’t appear.
Grrrr… well I’m not writing all that over again. Anyhow, just
wanted to say wonderful blog!
I reckon something genuinely special in this site.
Wow, wonderful blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your website is wonderful, as well as the content!
I was able to find good info from your blog articles.
Terrific facts, Many thanks.
Sangat menarik info !Sempurna persis seperti yang saya telusuri!
There is clearly a bundle to realize about this. I assume you made various nice points in features also.
Postingan yang sangat berguna. Saya baru saja menelusuri informasi seperti ini dan saya senang menemukannya di sini. Terima kasih telah berbagi.
Hello! I know this is kinda off topic however I’d figured I’d ask.
Would you be interested in exchanging links or maybe guest writing a blog post or vice-versa?
My website covers a lot of the same topics as yours and I feel
we could greatly benefit from each other. If you are interested feel free to send me
an email. I look forward to hearing from you!
Awesome blog by the way!
Wonderful blog! I found it while surfing around on Yahoo News.
Do you have any tips on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get there!
Appreciate it
My spouse and I stumbled over here by a different web address and thought I should check things out. I like what I see so i am just following you. Look forward to going over your web page again.
I’m truly enjoying the design and layout of your blog. It’s a very easy on the eyes which makes it much more pleasant for me to come here and visit more often. Did you hire out a developer to create your theme? Exceptional work!
VL
I know this if off topic but I’m looking into starting my
own blog and was curious what all is needed to get setup?
I’m assuming having a blog like yours would cost a pretty
penny? I’m not very web savvy so I’m not 100% certain. Any suggestions or advice would be greatly appreciated.
Kudos
Hey! I could have sworn I’ve been to this blog before but after checking through some of the post I realized it’s new to me.
Anyhow, I’m definitely delighted I found it and
I’ll be book-marking and checking back frequently!
Використовую allwinua і можу сказати, що
це доволі зручна платформа для live-ігор.
Виплати приходять без затримок,
підтримка працює нормально.
Бонуси та акції доволі приємні, що додає інтересу до гри.
У цілому, кожному раджу перевіряти умови перед грою, але особисто мені платформа підходить.
Asking questions are genuinely pleasant thing if
you are not understanding something fully, except this article
presents fastidious understanding yet.
Everyone loves what you guys are up too. Such clever work
and exposure! Keep up the good works guys I’ve included you guys to my blogroll.
Everyone loves it when people get together and share views.
Great site, continue the good work!
You’ve made your point!
Граю на AllwinUA і вважаю, що це реально комфортна платформа
для слотів. Транзакції достатньо швидко, саппорт відповідає
достатньо швидко. Промокоди та фріспіни
вистачають, що робить гру вигіднішою.
У цілому, раджу тестувати демо перед депозитом, але
особисто мені платформа підходить.
After looking over a number of the articles on your website, I honestly appreciate your technique of writing a blog.
I book-marked it to my bookmark site list and will be checking back soon. Please visit
my website too and let me know how you feel.
Hi, I do believe this is a great site. I stumbledupon it 😉 I
may return yet again since I bookmarked it. Money
and freedom is the best way to change, may you be rich and continue to guide other people.
Truly quite a lot of good material.
I have to thank you for the efforts you’ve put in writing
this blog. I’m hoping to view the same high-grade blog posts by
you in the future as well. In fact, your creative writing
abilities has motivated me to get my own site now 😉
Використовую Allwin UA Casino і вважаю, що це доволі зручна платформа
для слотів. Виведення коштів без затримок,
служба підтримки реагує достатньо швидко.
Пакети бонусів доволі приємні, що інколи
дає хороший старт. У цілому, кожному раджу перевіряти умови перед грою, але особисто мені платформа підходить.
I have been browsing online greater than 3 hours as of late,
but I by no means discovered any fascinating article
like yours. It’s pretty value enough for me. Personally, if all web owners and bloggers made
excellent content as you probably did, the net
will likely be much more helpful than ever before.
Hello there, just became aware of your blog through Google,
and found that it is truly informative. I’m gonna
watch out for brussels. I’ll appreciate if you continue
this in future. Lots of people will be benefited from your writing.
Cheers!
Valuable write ups, With thanks!
I still remember the moment, but the moment I started helping a friend inside a major sports organization, everything I thought I knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw
how the entire industry had turned into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going
after “IT servers” anymore. They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is between order and total
digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally
or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security
— especially the kind you see described in official breakdowns — it opened my
eyes. If anyone wants to understand how this level of protection actually works, they can always look it up directly from the
source. The full explanations are there, and they’re honestly
worth reading.
Inside the clubs, it was even more surreal. I saw
databases full of tactical plans — things that could ruin a season if
leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system
can fall apart. I watched entire staff units go through security training because
phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring, but now I
understand that without it, the entire digital
side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it
felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same
way again.
Can I simply just say what a comfort to discover someone who genuinely understands what they are discussing on the
internet. You definitely understand how to bring an issue to light and make it important.
More people must read this and understand this side of the story.
I can’t believe you aren’t more popular because you
definitely possess the gift.
Some really good blog posts on this web site, appreciate it for contribution. “Gratitude is not only the greatest of virtues, but the parent of all others.” by Cicero.
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get three emails with the same comment.
Is there any way you can remove people from that service?
Appreciate it!
Якщо порівнювати з іншими
казино AllwinUA виділяється тим, що
має гарний вибір слотів, які можуть допомогти на старті.
Підтримка працює відносно швидко,
а депозити та виведення заходять нормально.
Не захищаю нікого, але
залишила нормальне враження.
Howdy, i read your blog from time to time and i own a similar one and i was just curious if you get a lot of spam responses?
If so how do you reduce it, any plugin or anything you can advise?
I get so much lately it’s driving me insane so any support
is very much appreciated.
Wow, incredible blog format! How lengthy have you been blogging for?
you make blogging look easy. The whole look of your site is fantastic, as smartly as the content!
You really make it seem so easy with your presentation but I find this matter to be really something
which I think I would never understand. It seems too complicated and extremely broad for me.
I am looking forward for your next post, I will try to get the
hang of it!
Good day! This is my first visit to your blog! We are a group of volunteers and starting a
new initiative in a community in the same niche.
Your blog provided us valuable information to work on.
You have done a extraordinary job!
I’ve got to be honest, but the day I stepped into the backend
of the sports world, everything I thought I knew about modern sports
completely collapsed.
I always believed teams were about winning games, but when I saw how the
entire industry had turned into this fragile
high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going
after “IT servers” anymore. They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting
markets. That was the moment I understood how thin the line really is between order and total digital
disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just
websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally
or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it
opened my eyes. If anyone wants to understand how this level of protection actually works, they
can always look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw
databases full of sponsorship deals — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall
apart. I watched entire staff units go through security
training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance
was boring, but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only
thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly
from the source. It’s all publicly explained — and believe me, once you
read it, you’ll never look at sports or betting the same way again.
Gmail是Google公司推出的免费电子邮件服务,为全球数亿用户提供安全可靠的邮件收发功能。Gmail邮箱拥有大容量存储空间,支持15GB免费云端存储,能够存储大量邮件和附件。Gmail下载安装后,用户可以享受智能分类、强大的搜索功能、垃圾邮件过滤等特色服务。谷歌邮箱支持多平台同步,无论是在电脑、手机还是平板设备上都能随时访问您的邮件。Gmail邮箱下载提供Windows、Mac、iOS、Android等多个版本,满足不同用户的使用需求。作为全球最受欢迎的电子邮件服务之一,Gmail以其简洁的界面设计、快速的响应速度和安全的数据保护而闻名。用户可以通过Gmail进行邮件收发、日程管理、文件共享等多种操作,是商务办公和个人通讯的理想选择。
I never thought I’d end up writing this but here I am.
Not long ago, I got obsessed in online games
– Apex Legends. I wanted to dominate, and I didn’t want to rely on skill alone.
After another frustrating match, I stumbled across a
forum thread talking about scripts. At first I laughed it off, but the more screenshots I saw, the more it felt like a secret world.
Users were posting clips showing how they climbed from low ranks to high ones in days.
It looked effortless. And of course, it was too good to be true.
I won’t lie, I actually got close to buying something.
Someone pushed a “limited offer” in my inbox. That’s
when the real consequences showed up.
I found threads from players who lost their accounts.
Some even wrote how their PCs got infected. The shock snapped me out of it.
Instead of throwing everything away, I walked away and focused on improving the legitimate way.
Now, when I see people chasing cheats, I just think: the crash always comes.
Hopefully this story saves someone else time.
First of all I want to say excellent blog!
I had a quick question in which I’d like to
ask if you don’t mind. I was curious to know how you center yourself and
clear your head prior to writing. I have had trouble clearing my thoughts in getting my thoughts out.
I do take pleasure in writing but it just seems like the first 10 to 15 minutes are usually
lost simply just trying to figure out how to begin. Any recommendations
or tips? Thank you!
You actually make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand.
It seems too complicated and very broad for me. I’m
looking forward for your next post, I’ll try to get the hang of
it!
Your comment is awaiting moderation.
https://www.facebook.com/mb88lccom/
https://www.youtube.com/@mb88lccom
https://twitter.com/mb88lccom
https://tooter.in/mb88lccom1
https://wakelet.com/@mb88lccom
https://safechat.com/u/mb88lccom
https://www.blogger.com/profile/02944067836296978879
https://www.mymeetbook.com/mb88lccom
https://www.pinterest.com/mb88lccom/
https://community.wongcw.com/mb88lccom
https://demo.wowonder.com/mb88lccom
https://shareyoursocial.com/mb88lccom
https://gitlab.aicrowd.com/mb88lccom
https://myspace.com/mb88lccom
https://500px.com/p/mb88lccom
https://www.instapaper.com/p/mb88lccom
https://magic.ly/mb88lccom
https://band.us/@mb88lccom
https://protocol.ooo/ja/users/mb88lccom
https://sketchfab.com/mb88lccom
https://www.tumblr.com/mb88lccom
https://www.reddit.com/user/mb88lccom/
https://audiomack.com/mb88lccom
https://hackaday.io/mb88lccom
https://fyers.in/community/member/YZ0cXtgaAT
https://vocal.media/authors/mb88lccom
https://leetcode.com/u/mb88lccom/
https://swag.live/en/user/69a082bda1d9d0a24db7109f
https://www.halaltrip.com/user/profile/321679/mb88lccom/
https://www.jetphotos.com/photographer/784721
https://medibang.com/author/27870702/
https://liulo.fm/mb88lccom
https://opensea.io/mb88lccom
https://www.blockdit.com/mb88lccom
https://portfolium.com/mb88lccom
https://groups.google.com/g/mb88lccom
https://www.twitch.tv/mb88lccom/about
https://profile.hatena.ne.jp/mb88lccom/profile
https://issuu.com/mb88lccom
https://www.behance.net/mb88lccom
https://gravatar.com/mb88lccom
https://www.reverbnation.com/artist/mb88lccom
https://www.myminifactory.com/users/mb88lccom
https://www.investagrams.com/Profile/mb88lccom
https://gifyu.com/mb88lccom
https://www.chordie.com/forum/profile.php?id=2474289
https://skitterphoto.com/photographers/2381931/mb88lccom
https://www.longisland.com/profile/mb88lccom
https://www.walkscore.com/people/170230922537/mb88lccom
https://topsitenet.com/profile/mb88lccom/1552921/
https://akniga.org/profile/1395619-mb88lccom/
https://mb88lccom.bandcamp.com/album/mb88lccom
https://disqus.com/by/mb88lccom/about/
https://jobs.suncommunitynews.com/profiles/7945070-mb88lccom
https://www.speedrun.com/users/mb88lccom
https://www.fanart-central.net/user/mb88lccom/profile
https://slides.com/mb88lccom
https://www.aicrowd.com/participants/mb88lccom
https://old.bitchute.com/channel/iudY3M5ekLTY/
https://pbase.com/mb88lccom
https://hub.docker.com/u/mb88lccom
https://spiderum.com/nguoi-dung/mb88lccom
https://zaidap.com/thong-tin-ca-nhan-u106145.htm
https://www.gta5-mods.com/users/mb88lccom
https://heylink.me/mb88lccom/
https://pixabay.com/users/54816927/
https://www.nicovideo.jp/user/143394265
https://www.jigsawplanet.com/mb88lccom
https://3dwarehouse.sketchup.com/by/mb88lccom
https://robertsspaceindustries.com/en/citizens/mb88lccom
https://bit.ly/m/mb88lccom
https://joy.link/mb88lccom
https://connect.garmin.com/app/profile/2ed7436b-7fdd-459a-8e10-69062c20e7d9
https://b.hatena.ne.jp/mb88lccom/bookmark
https://www.chichi-pui.com/users/mb88lccom/
https://www.openrec.tv/user/mb88lccom/about
https://unityroom.com/users/smjbrqd3y9kf0x8ugenh
https://routinehub.co/user/mb88lccom
https://pxhere.com/en/photographer-me/4930674
https://teletype.in/@mb88lccom
https://www.checkli.com/mb88lccom
https://gitee.com/mb88lccom
https://www.fuelly.com/driver/mb88lccom
https://www.nintendo-master.com/profil/mb88lccom
https://freeimage.host/mb88lccom
https://www.diigo.com/profile/mb88lccom
https://fontstruct.com/fontstructions/show/2833509/mb88lccom
https://motion-gallery.net/users/917569
https://linkin.bio/mb88lccom
https://biomolecula.ru/authors/127307
https://talk.plesk.com/members/mblccom.490444/#about
https://www.callupcontact.com/b/businessprofile/mb88lccom/9988006
https://www.growkudos.com/profile/nha_ci_mb
https://blender.community/mb88lccom/
https://doselect.com/@534d88cb57583bc7f703a134f
https://sciter.com/forums/users/mb88lccom/
https://matkafasi.com/user/mb88lccom
https://allmyfaves.com/mb88lccom
https://www.abclinuxu.cz/lide/mb88lccom
https://dumagueteinfo.com/author/mb88lccom/
https://muare.vn/shop/nha-cai-mb88-50/895475
https://www.vnbadminton.com/members/mb88lccom.65819/
https://doodleordie.com/profile/mb88lccom
https://web.ggather.com/mb88lccom
https://musikersuche.musicstore.de/profil/mb88lccom/
https://www.intensedebate.com/profiles/mb88lccom
https://forum.dmec.vn/index.php?members/mb88lccom.176249/
https://igli.me/mb88lccom
https://www.fantasyplanet.cz/diskuzni-fora/users/mb88lccom/
https://duyendangaodai.net/members/30201-mb88lcco.html
http://delphi.larsbo.org/user/mb88lccom
https://www.aseeralkotb.com/en/profiles/mb88lccom
https://timdaily.vn/members/mb88lccom.128649/#about
https://app.readthedocs.org/profiles/mb88lccom/
https://www.dibiz.com/pierrethuyensa830
https://iszene.com/user-337207.html
https://www.theyeshivaworld.com/coffeeroom/users/mb88lccom
https://desksnear.me/users/mb88lccom
https://www.itchyforum.com/en/member.php?380161-mb88lccom
https://www.roton.com/forums/users/pierrethuyensa830/
https://able2know.org/user/mb88lccom/
http://www.biblesupport.com/user/813653-mb88lccom/
https://golosknig.com/profile/mb88lccom/
https://www.anibookmark.com/user/mb88lccom.html
https://www.inventoridigiochi.it/membri/mb88lccom/profile/
https://forum.m5stack.com/user/mb88lccom
https://wallhaven.cc/user/mb88lccom
https://imageevent.com/mb88lccom/mb88lccom
https://www.bitchute.com/channel/iudY3M5ekLTY
https://bandori.party/user/512530/mb88lccom/
https://community.m5stack.com/user/mb88lccom
https://schoolido.lu/user/mb88lccom/
https://awan.pro/forum/user/139904/
https://jakle.sakura.ne.jp/pukiwiki/?mb88lccom
https://fortunetelleroracle.com/profile/mb88lccom
https://fabble.cc/mb88lccom
https://pad.geolab.space/s/jd4K4XtCf
https://community.cisco.com/t5/user/viewprofilepage/user-id/1978083
https://pad.stuve.de/s/m4Cv95mej
https://kr.pinterest.com/mb88lccom/
https://pt.gravatar.com/mb88lccom
https://th.gravatar.com/mb88lccom
https://www.sythe.org/members/mb88lccom.2015271/
https://f319.com/members/mb88lccom.1071155/
https://about.me/mb88lccom
https://www.canadavisa.com/canada-immigration-discussion-board/members/mb88lccom.1343104/#about
https://www.equinenow.com/farm/mb88lccom.htm
https://www.gaiaonline.com/profiles/mb88lccom/50649836/
https://wefunder.com/mb88lccom
https://potofu.me/mb88lccom
https://transfur.com/Users/mb88lccom
https://xtremepape.rs/members/mb88lccom.646639/#about
https://github.com/mb88lccom
https://myanimelist.net/profile/mb88lccom
https://website.informer.com/mb88-lc.com
https://lightroom.adobe.com/u/mb88lccom
https://beacons.ai/mb88lccom
https://en.islcollective.com/portfolio/12855902
https://www.xosothantai.com/members/mb88lccom.599153/
https://velog.io/@mb88lccom/about
https://violet.vn/user/show/id/15241314
https://iplogger.org/vn/logger/MnBQ5fiSjue6/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3905707
https://mez.ink/mb88lccom
https://mb88lccom.stck.me/profile
https://notionpress.com/author/1478082
https://www.edna.cz/uzivatele/mb88lccom/
https://digiphoto.techbang.com/users/mb88lccom
https://leakedmodels.com/forum/members/mb88lccom.692840/#about
https://freeicons.io/profile/899321
https://onlinesequencer.net/forum/user-253593.html
https://inkbunny.net/mb88lccom
https://www.japaaan.com/user/63413/
https://spinninrecords.com/profile/mb88lccom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.mb883
https://code.antopie.org/mb88lccom
https://beatsaver.com/playlists/1147797
https://apptuts.bio/mb88lccom-249013
https://dialog.eslov.se/profiles/mb88lccom/activity
https://www.storenvy.com/mb88lccom
https://mb88lccom.mssg.me/
https://forums.maxperformanceinc.com/forums/member.php?u=240010
https://egl.circlly.com/users/mb88lccom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=291005
https://acomics.ru/-mb88lccom
https://www.criminalelement.com/members/mb88lccom/profile/
https://hanson.net/users/mb88lccom
https://writexo.com/share/bde733911d5a
https://expatguidekorea.com/profile/mb88lccom/
https://www.laundrynation.com/community/profile/mb88lccom/
https://www.heavyironjobs.com/profiles/7946778-mb88lccom
https://pad.degrowth.net/s/PlbmvVkJv
https://www.syncdocs.com/forums/profile/mb88lccom
https://www.rehashclothes.com/mb88lccom
http://fort-raevskiy.ru/community/profile/mb88lccom/
https://forum.skullgirlsmobile.com/members/mb88lccom.197649/#about
https://jobs.landscapeindustrycareers.org/profiles/7946812-mb88lccom
https://phatwalletforums.com/user/mb88lccom/
https://forums.galciv4.com/user/7640429
https://kyourc.com/mb88lccom
https://song.link/mb88lccom
https://idol.st/user/137054/mb88lccom/
https://www.valinor.com.br/forum/usuario/mb88lccom.141615/#about
https://tulieu.violet.vn/user/show/id/15241314
https://www.bmwpower.lv/user.php?u=mb88lccom
https://gockhuat.net/member.php?u=431528
https://jobs.windomnews.com/profiles/7947041-mb88lccom
https://hoaxbuster.com/redacteur/mb88lccom
https://www.givey.com/mb88lccom
https://talkmarkets.com/profile/mb88lccom
https://pc.poradna.net/users/1144889864-mb88lccom
https://forums.stardock.com/user/7640429
https://zerosuicidetraining.edc.org/user/profile.php?id=541982
https://beteiligung.amt-huettener-berge.de/profile/mb88lccom/
https://joinentre.com/profile/mb88lccom
https://eo-college.org/members/mb88lccom/
https://jobs.westerncity.com/profiles/7947377-mb88lccom
https://www.thetriumphforum.com/members/mb88lccom.56871/
https://armchairjournal.com/forums/users/mb88lccom/
https://mycableengineering.com/activity-feed/userId/29586
https://l2top.co/forum/members/mb88lccom.157930/
http://www.askmap.net/location/7742255/vietnam/mb88lccom
https://youtopiaproject.com/author/mb88lccom
https://graphcommons.com/graphs/69b12e24-0b4c-44d7-bdd1-54d7f9d37aa1
https://forums.galciv3.com/user/7640429
https://galleria.emotionflow.com/175549/profile.html
https://www.myget.org/users/mb88lccom
https://www.deafvideo.tv/vlogger/mb88lccom
https://www.chaloke.com/forums/users/mb88lccom/
https://app.brancher.ai/user/HTUGCLBmTCwt
https://justpaste.me/vxZ91
https://aetherlink.app/users/7433134794206380032
https://forums.sinsofasolarempire2.com/user/7640429
https://www.empregosaude.pt/en/author/mb88lccom/
https://confengine.com/user/mb88lccom
https://slideslive.com/mb88lccom?tab=about
https://mygamedb.com/profile/mb88lccom
https://buckeyescoop.com/community/members/mb88lccom.57810/#about
https://forums.ashesofthesingularity.com/user/7640429
http://www.ssnote.net/users/mb88lccom
https://www.mateball.com/mb88lccom
https://rotorbuilds.com/profile/204754/
https://toirscript.com/user/mb88lccom
https://forum.pabbly.com/members/mb88lccom.98823/#about
http://forum.cncprovn.com/members/415364-mb88lccom
https://marketplace.trinidadweddings.com/author/mb88lccom/
https://ncnews.co/profile/mb88lccom
https://dreevoo.com/profile_info.php?pid=1192710
https://forum.aigato.vn/user/mb88lccom
https://amaz0ns.com/forums/users/mb88lccom/
https://rapidapi.com/user/mb88lccom
https://www.skool.com/@nha-cai-mb-7064
https://learningapps.org/watch?v=pi15oe1yk26
https://postheaven.net/mb88lccom/mb88lccom
https://www.giveawayoftheday.com/forums/profile/1672004
http://onlineboxing.net/jforum/user/editDone/430872.page
https://www.catapulta.me/users/mb88lccom
http://www.invelos.com/UserProfile.aspx?alias=mb88lccom
https://www.video-bookmark.com/bookmark/7058302/mb88lccom/
https://wibki.com/mb88lccom
https://twitback.com/mb88lccom
https://krachelart.com/UserProfile/tabid/43/userId/1334589/Default.aspx
https://gitlab.vuhdo.io/mb88lccom
https://www.11secondclub.com/users/profile/1700327
https://s.id/mb88lccom1
https://kktix.com/user/8451547
https://www.passes.com/mb88lccom
https://poipiku.com/13248570/
https://uiverse.io/profile/nhci_1243
https://www.rwaq.org/users/mb88lccom
https://cofacts.tw/user/mb88lccom
https://www.fitday.com/fitness/forums/members/mb88lccom.html
https://www.fundable.com/nha-cai-mb88-3
https://vcook.jp/users/75570
https://www.grepmed.com/mb88lccom
https://espritgames.com/members/50206906/
https://cgmood.com/mb88lccom
https://www.haikudeck.com/presentations/mb88lccom
https://www.efunda.com/members/people/show_people.cfm?Usr=mb88lccom
https://backloggery.com/mb88lccom
https://www.sociomix.com/u/mb88lccom/
https://raovat.nhadat.vn/members/mb88lccom-289934.html
https://www.moshpyt.com/user/mb88lccom
https://www.koi-s.id/member.php?331644-mb88lccom
https://pumpyoursound.com/u/user/1586216
https://que.u.nosv.org/profile?user=mb88lccom
https://hi-fi-forum.net/profile/1122601
https://secondstreet.ru/profile/mb88lccom/
http://scenarch.com/userpages/29020
https://undrtone.com/mb88lccom
https://marshallyin.com/members/mb88lccom/
https://us.enrollbusiness.com/BusinessProfile/7734127/mb88lccom
https://www.atozed.com/forums/user-68435.html
https://www.tizmos.com/mb88lccom/
https://gravesales.com/author/mb88lccom/
https://searchengines.bg/members/mb88lccom.23582/#about
https://luvly.co/users/mb88lccom
https://suckhoetoday.com/members/36093-mb88lcco.html
https://hukukevi.net/user/mb88lccom
https://belgaumonline.com/profile/mb88lccom/
https://savelist.co/profile/users/mb88lccom
https://usdinstitute.com/forums/users/mb88lccom/
https://www.montessorijobsuk.co.uk/author/mb88lccom/
https://hackerspace.govhack.org/profiles/nh_c_i_mb88_35723
https://zzb.bz/ZPDiWC
https://draft.blogger.com/profile/02944067836296978879
https://boldomatic.com/view/writer/mb88lccom
https://menwiki.men/wiki/User:Mb88lccom
https://funsilo.date/wiki/User:Mb88lccom
https://www.themeqx.com/forums/users/mb88lccom/
https://www.udrpsearch.com/user/mb88lccom
https://www.inseparabile.it/forum/member.php?u=45844
https://forums.wincustomize.com/user/7640429
http://newdigital-world.com/members/mb88lccom.html
https://www.xen-factory.com/index.php?members/mb88lccom.140905/#about
https://king-wifi.win/wiki/User:Mb88lccom
https://forums.servethehome.com/index.php?members/mb88lccom.227017/#about
https://jaga.link/mb88lccom
https://raovatquynhon.com/thiet-bi-dien-tu-4/mb88lccom-16020
https://b.io/mb88lccom
https://www.blackhatprotools.info/member.php?277240-mb88lccom
https://activepages.com.au/profile/mb88lccom
https://snippet.host/kjkpem
https://tudomuaban.com/chi-tiet-rao-vat/2830226/mb88–nen-tang-ca-cuoc-online-hien-dai.html
https://phijkchu.com/a/mb88lccom/video-channels
https://lifeinsys.com/user/mb88lccom
https://kaeuchi.jp/forums/users/mb88lccom/
https://www.claimajob.com/profiles/7949491-mb88lccom
https://protospielsouth.com/user/117883
https://theafricavoice.com/profile/mb88lccom
http://palangshim.com/space-uid-4985482.html
https://www.africangenesis-101.org/profile/pierrethuyensa83071914/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:2424271869A08ABA0A495C95@AdobeID
https://vi.gravatar.com/mb88lccom
https://www.vevioz.com/mb88lccom
https://www.mixcloud.com/mb88lccom/
https://www.designspiration.com/mb88lccom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=186380
https://hub.vroid.com/en/users/124239688
https://www.exchangle.com/mb88lccom
https://forum.codeigniter.com/member.php?action=profile&uid=224497
https://circleten.org/a/396618
https://bitspower.com/support/user/mb88lccom
https://www.brownbook.net/business/54870616/mb88lccom
https://etextpad.com/vl5fnmq2py
https://app.hellothematic.com/creator/profile/1124170
https://app.talkshoe.com/user/mb88lccom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223750
https://hulkshare.com/mb88lccom
https://m.wibki.com/mb88lccom
https://www.pageorama.com/?p=mb88lccom
https://bandsworksconcerts.info/index.php?mb88lccom
https://bbs.mikocon.com/home.php?mod=space&uid=282159
https://www.mikocon.com/home.php?mod=space&uid=282159
https://www.quora.com/profile/Nh%C3%A0-C%C3%A1i-MB88-2
https://manylink.co/@mb88lccom
https://www.freewebspace.net/forums/index.php?members/mb88lccom.17031340/#about
https://forums.giantitp.com/member.php?369340-mb88lccom
https://seomotionz.com/member.php?action=profile&uid=117566
https://anyflip.com/homepage/ieiug#About
https://www.akaqa.com/question/q19192654507-Mb88lccom
https://londonchinese.com/home.php?mod=space&uid=615105&do=profile
https://copynotes.be/shift4me/forum/user-44740.html
https://scholar.google.com/citations?hl=en&user=Q09ZFxEAAAAJ
https://www.smitefire.com/profile/mb88lccom-257233?profilepage
https://coolors.co/u/mb88lccom
https://www.beamng.com/members/mb88lccom.774734/
https://civitai.com/user/mb88lccom
https://www.spigotmc.org/members/mb88lccom.2487701/
https://boosty.to/mb88lccom
https://camp-fire.jp/profile/mb88lccom
https://www.pearltrees.com/mb88lccom/item783094023
https://gesoten.com/profile/detail/12596328
https://rekonise.com/u/mb88lccom
https://hashnode.com/@mb88lccom
https://hoo.be/mb88lccom
https://nhattao.com/members/user6923904.6923904/
https://maxforlive.com/profile/user/mb88lccom?tab=about
https://3dtoday.ru/blogs/mb88lccom
https://opencollective.com/mb88lccom
https://pinshape.com/users/8917620-mb88lccom
https://morguefile.com/creative/mb88lccom
https://edabit.com/user/fJ8e4skueqo9xhu9r
https://mathlog.info/users/Nn3s2h9ugWWatpWCHYShy0wykgA3
https://securityheaders.com/?q=https%3A%2F%2Fmb88-lc.com%2F
https://my.bio/mb88lccom
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165778
https://md.darmstadt.ccc.de/s/eGhTV5H_Mc
https://participation.u-bordeaux.fr/profiles/mb88lccom/activity
https://sfx.thelazy.net/users/u/mb88lccom/
https://forum.reallusion.com/Users/3283716/mb88lccom
https://app.daily.dev/mb88lccom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=247400
https://slidehtml5.com/homepage/vtqa#About
https://www.skypixel.com/users/djiuser-mbe6urycepto
http://webanketa.com/forms/6mv34d1h6gqk0d9h71j62csm/
https://matters.town/@mb88lccom
https://www.pdc.edu/?URL=https://mb88-lc.com/
https://ask.mallaky.com/?qa=user/mb88lccom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75904
https://drill.lovesick.jp/drilldata/index.php?mb88lccom
https://www.depechemode.cz/?URL=https://mb88-lc.com/
https://sub4sub.net/forums/users/mb88lccom/
https://www.slmath.org/people/99174
https://userstyles.world/user/mb88lccom
https://goo.by/jeDIwh
https://amazingradio.com/profile/mb88lccom
https://bresdel.com/mb88lccom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12120
https://fora.babinet.cz/profile.php?section=personal&id=115095
https://pledgeme.co.nz/profiles/319505/
https://www.shippingexplorer.net/en/user/mb88lccom/257919
https://pictureinbottle.com/r/mb88lccom
https://forum.epicbrowser.com/profile.php?section=personal&id=139337
http://www.dungdong.com/home.php?mod=space&uid=3325270&do=profile
https://forum.herozerogame.com/index.php?/user/152439-mb88lccom/
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=90001
https://electroswingthing.com/profile/mb88lccom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2393019
https://connect.gt/user/mb88lccom
https://stuv.othr.de/pad/s/e8M9L78PI
https://forum.tkool.jp/index.php?members/mb88lccom.98078/#about
https://hedgedoc.eclair.ec-lyon.fr/s/O6aGnx0wD
http://densan-knct.freehostia.com/wiki_/index.php?mb88lccom
https://www.divephotoguide.com/user/mb88lccom
https://www.weddingbee.com/members/mb88lccom/
https://kumu.io/mb88lccom/mb88lccom
https://b.cari.com.my/home.php?mod=space&uid=3383721&do=profile
https://bioimagingcore.be/q2a/user/mb88lccom
https://www.sunlitcentrekenya.co.ke/author/mb88lccom/
https://hedgedoc.logilab.fr/s/K2STKSNID
https://mb88lccom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/mb88lccom/activity
https://www.rcuniverse.com/forum/members/mb88lccom.html
https://www.huntingnet.com/forum/members/mb88lccom.html
https://www.socialbookmarkssite.com/bookmark/6201283/mb88lccom/
https://www.hogwartsishere.com/1818285/
https://vimeo.com/mb88lccom
https://forum.index.hu/User/UserDescription?u=2193984
https://gitlab.com/mb88lccom
https://www.symbaloo.com/shared/AAAAB6QAc1oAA42AShR18Q==
https://www.bricklink.com/aboutMe.asp?u=mb88lccom
https://makeagif.com/user/mb88lccom?ref=7P9HOm
https://www.france-ioi.org/user/perso.php?sLogin=mb88lccom
https://participez.perigueux.fr/profiles/mb88lccom/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424772
https://www.dotafire.com/profile/mb88lccom-237675?profilepage
https://www.trackyserver.com/profile/231770
https://ixawiki.com/link.php?url=https://mb88-lc.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=135270
https://www.zubersoft.com/mobilesheets/forum/user-124473.html
https://www.plotterusati.it/user/mb88lccom
https://forum.dboglobal.to/wsc/index.php?user/143374-mb88lccom/
https://forum.azeron.eu/index.php?members/mb88lccom.29573/#about
http://www.jbt4.com/home.php?mod=space&uid=8666688
https://www.vid419.com/home.php?mod=space&uid=3475594
https://forum.ct8.pl/member.php?action=profile&uid=114997
https://mb88lccom.shopinfo.jp/posts/58591305
https://linqto.me/n/mb88lccom
https://www.mindomo.com/mindmap/88679967fe8c4955a8e4eb4885f120f2
https://www.okaywan.com/home.php?mod=space&uid=772256
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Mb88lccom
https://www.goodolcomics.com/blog/profile/mb88lccom/
https://www.swap-bot.com/user:mb88lccom
http://techou.jp/index.php?mb88lccom
https://paste.intergen.online/view/9c89b09f
https://epiphonetalk.com/members/mb88lccom.91485/#about
http://tkdlab.com/wiki/index.php?mb88lccom
https://www.managementpedia.com/members/mb88lccom.1116665/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=604378
http://pcsq28.com/home.php?mod=space&uid=1765600
https://bbs.airav.cc/home.php?mod=space&uid=4420319
https://partecipa.poliste.com/profiles/mb88lccom/activity
https://md.coredump.ch/s/42XX9OP-A
https://hker2uk.com/home.php?mod=space&uid=5345610
https://pad.funkwhale.audio/s/H12z-uV2i
https://forum.dfwmas.org/index.php?members/mb88lccom.194694/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=466505
https://hcgdietinfo.com/hcgdietforums/members/mb88lccom/
https://aprenderfotografia.online/usuarios/mb88lccom/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2304008&do=profile&from=space
http://galeria.farvista.net/member.php?action=showprofile&user_id=71396
https://darkml.net/bbs/home.php?mod=space&uid=8193489&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6013428
https://hedgedoc.stusta.de/s/fYTnYnn7X
https://pad.flipdot.org/s/FyAxbxtLr
https://hack.allmende.io/s/7YZgU09pk
https://pad.codefor.fr/s/2LvLwRFtlo
https://md.opensourceecology.de/s/X0h4uQxyW
https://md.ctdo.de/s/meoOsVUgEL
https://md.chaospott.de/s/9AMZp2EoTc
https://pad.fablab-siegen.de/s/WCV_brIgT
https://thesn.eu/mb88lccom
https://hackmd.hub.yt/s/0EsGiHbMg
https://md.swk-web.com/s/Ewc5AP41E
https://hedgedoc.dezentrale.space/s/oKkx64GuR
https://docs.juze-cr.de/s/T6pbvDhq-
https://ar.gravatar.com/mb88lccom
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301461
https://replit.com/@mb88lccom
https://odesli.co/mb88lccom
https://www.degreeforum.net/mybb/User-mb88lccom
https://wandb.ai/mb88lccom
https://pad.darmstadt.social/s/gcLEpOPUjA
https://divisionmidway.org/jobs/author/mb88lccom/
https://bbcovenant.guildlaunch.com/users/blog/6738510/?mode=view&gid=97523
https://md.kif.rocks/s/RyIQNKaZuI
https://youbiz.com/profile/mb88lccom/
https://timeoftheworld.date/wiki/User:Mb88lccom1
https://cameradb.review/wiki/User:Mb88lccom
https://historydb.date/wiki/User:Mb88lccom
https://www.wowonder.xyz/mb88lccom
https://sciencemission.com/profile/mb88lccom
https://referrallist.com/profile/mb88lccom/
https://fakenews.win/wiki/User:Mb88lccom
http://jobboard.piasd.org/author/mb88lccom/
https://www.wvhired.com/profiles/7951380-mb88lccom
http://jobs.emiogp.com/author/mb88lccom/
https://www.canadavideocompanies.ca/forums/users/mb88lccom/
https://hackmd.openmole.org/s/-b0flvLKJ
https://ismschools.com.au/forums/users/mb88lccom/
https://md.chaosdorf.de/s/eBKO3VKHeY
https://doc.adminforge.de/s/2bSxD77hHh
https://onlinevetjobs.com/author/mb88lccom/
https://v.gd/tIvTrl
https://sciencewiki.science/wiki/User:Mb88lccom
https://gl.gta5-mods.com/users/mb88lccom
https://www.fruitpickingjobs.com.au/forums/users/mb88lccom/
http://www.webclap.com/php/jump.php?url=https://mb88-lc.com/
https://xoops.ec-cube.net/userinfo.php?uid=342590
http://bbs.sdhuifa.com/home.php?mod=space&uid=1067994
https://quangcaoso.vn/mb88lccom
https://chyoa.com/user/mb88lccom
https://www.royalroad.com/profile/919838
https://forums.alliedmods.net/member.php?u=467166
https://digiex.net/members/mb88lccom.140200/
https://www.corc.co.uk/forums/users/mb88lccom/
https://smallseo.tools/website-checker/mb88-lc.com
https://cuwip.ucsd.edu/members/mb88lccom/profile/
https://zenwriting.net/mb88lccom/mb88lccom
https://writeablog.net/mb88lccom/mb88lccom
https://blogfreely.net/mb88lccom/mb88lccom
https://bwinglive.lighthouseapp.com/users/1993130
https://rush1989.rash.jp/pukiwiki/index.php?mb88lccom
https://www.stylevore.com/user/mb88lccom
http://bio.site/mb88lccom
https://wikimapia.org/external_link?url=https://mb88-lc.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6253095
https://www.thesims3.com/myBlog.html?persona=mb88lccom
https://telegra.ph/mb88lccom-02-28
https://www.prosebox.net/book/101948/
https://log.concept2.com/profile/2862217
https://www.speedway-world.pl/forum/member.php?action=profile&uid=439813
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://mb88-lc.com/
http://forum.orangepi.org/home.php?mod=space&uid=6253095
https://redirect.camfrog.com/redirect/?url=https://mb88-lc.com/
https://beteiligung.hafencity.com/profile/mb88lccom/
https://adhocracy.plus/profile/mb88lccom/
https://www.hobowars.com/game/linker.php?url=https://mb88-lc.com/
https://beteiligung.stadtlindau.de/profile/mb88lccom/
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=76600
https://forum.honorboundgame.com/user-503900.html
https://elovebook.com/mb88lccom
https://propterest.com.au/user/73649/mb88lccom
https://www.fw-follow.com/forum/topic/92630/mb88lccom
https://www.jk-green.com/forum/topic/88901/mb88lccom
https://www.navacool.com/forum/topic/321870/mb88lccom
https://www.bonback.com/forum/topic/321869/mb88lccom
https://www.driedsquidathome.com/forum/topic/114864/mb88lccom
https://www.nongkhaempolice.com/forum/topic/89204/mb88lccom
https://www.bestloveweddingstudio.com/forum/topic/62746/mb88lccom
https://www.natthadon-sanengineering.com/forum/topic/79457/mb88lccom
https://www.rueanmaihom.net/forum/topic/78722/mb88lccom
https://www.ttlxshipping.com/forum/topic/321872/mb88lccom
https://www.cemkrete.com/forum/topic/135537/mb88lccom
https://pubhtml5.com/homepage/cqdrz/
http://forum.modulebazaar.com/forums/user/mb88lccom/
https://gratisafhalen.be/author/mb88lccom/
https://beteiligung.tengen.de/profile/mb88lccom/
https://calaos.fr/forum/member.php?action=profile&uid=18666
https://www.vrwant.org/wb/home.php?mod=space&uid=4970027
https://www.pathumratjotun.com/forum/topic/142159/mb88lccom
https://maychetao.com/members/20128-mb88lcco.html
https://diendan.cuabenhvien.com/members/18903-mb88lcco.html
https://www.divekeeper.com/forums/discussion/general-discussion/mb88lccom
https://forum.web-z.net/profile.php?userid=9005
https://usabbs.org/home.php?mod=space&uid=85905
https://lqdoj.edu.vn/user/mb88lccom
https://paperjale.eus/user/mb88lccom
http://byltz.com/home.php?mod=space&uid=478065
https://indiestorygeek.com/user/mb88lccom
https://diigo.com/01217g8
https://en.wikivet.net/User:Mb88lccom
https://forum.issabel.org/u/mb88lccom
https://mozillabd.science/wiki/User:Mb88lccom
https://raredirectory.com/author/mb88lccom-42005/
https://www.iglinks.io/mb88lccom-kze
https://www.keepandshare.com/discuss4/36743/mb88lccom
http://bbs.medicalforum.cn/home.php?mod=space&uid=2089935
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://mb88-lc.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3383721&do=profile
https://giaoan.violet.vn/user/show/id/15241314
https://anh135689999.violet.vn/user/show/id/15241314
https://party.biz/profile/mb88lccom?tab=541
https://hu.gta5-mods.com/users/mb88lccom
https://www.backabuddy.co.za/campaign/mb88lccom
https://uk.gta5-mods.com/users/mb88lccom
https://sl.gta5-mods.com/users/mb88lccom
https://at.pinterest.com/mb88lccom/
https://www.easyhits4u.com/profile.cgi?login=mb88lccom
https://newdayrp.com/members/mb88lccom.66924/#about
https://in.pinterest.com/mb88lccom/
https://doc.anagora.org/s/awGMUAQWnX
https://album.link/mb88lccom
https://artist.link/mb88lccom
https://pods.link/mb88lccom
https://mylink.page/mb88lccom
https://playlist.link/mb88lccom
https://portfolium.com.au/mb88lccom
https://mail.londonchinese.com/home.php?mod=space&uid=615105&do=profile
https://baigiang.violet.vn/user/show/id/15241314
http://www.muzikspace.com/profiledetails.aspx?profileid=128572
https://forums.starcontrol.com/user/7640429
https://es.gravatar.com/mb88lccom
https://de.gravatar.com/mb88lccom
https://cy.gravatar.com/mb88lccom
https://cs.gravatar.com/mb88lccom
https://cn.gravatar.com/mb88lccom
https://forums.offworldgame.com/user/7640429
https://www.ekdarun.com/forum/topic/135263/mb88lccom
https://www.mobafire.com/profile/mb88lccom-1236278?profilepage
https://fic.decidim.barcelona/profiles/mb88lccom/activity
https://fanclove.jp/profile/5l2Me3xo2K
https://truckymods.io/user/463422
http://forum.vodobox.com/profile.php?section=personal&id=63962
https://forums.sinsofasolarempire.com/user/7640429
https://forums.stardock.net/user/7640429
https://www.dokkan-battle.fr/forums/users/mb88lccom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3383721&do=profile
https://www.d-ushop.com/forum/topic/100705/mb88lccom
https://www.fanfiction.net/~mb88lccom
https://www.noteflight.com/profile/9646eb87bff029f7591f7fd2e2fdf3e7f6460701
https://www.spoonflower.com/profiles/mb88lccom
https://www.sportjim.com/mb88lccom
https://www.horticulturaljobs.com/employers/4039822-mb88lccom
https://johsocial.com/story11773386/mb88lccom
https://jobs.siliconflorist.com/employers/4039823-mb88lccom
https://jobs.nefeshinternational.org/employers/4039826-mb88lccom
https://aboutcasemanagerjobs.com/author/mb88lccom/
https://biashara.co.ke/author/mb88lccom/
https://buyandsellhair.com/author/mb88lccom/
https://cornucopia.se/author/mb88lccom
https://colorswall.com/users/29966/collections
https://rareconnect.org/en/user/mb88lccom
https://whyp.it/users/135744/mb88lccom
https://6giay.vn/members/mb88lccom.95231/
https://findaspring.org/members/mb88lccom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=769691
https://careers.coloradopublichealth.org/profiles/7952177-mb88lccom
https://cloud.anylogic.com/profile/user/58a58b7d-765d-4150-9077-189accafc307
https://gorillasocialwork.com/story26160992/mb88lccom
https://homepage.ninja/mb88lccom
https://cuadepviet.com/members/12457-mb88lcco.html
https://dienbd.violet.vn/user/show/id/15241314
https://chothai24h.com/members/29375-mb88lcco.html
https://kttm.club/members/mb88lccom.4380/#about
https://vietcurrency.vn/members/mb88lccom.234571/#about
https://zh-tw.gravatar.com/mb88lccom
https://sv.gravatar.com/mb88lccom
https://po.gravatar.com/mb88lccom
https://oc.gravatar.com/mb88lccom
https://ko.gravatar.com/mb88lccom
https://vnbit.org/members/mb88lccom.84324/#about
https://www.cake.me/me/mb88lccom
https://boss.why3s.cc/boss/home.php?mod=space&uid=251412
https://community.goldposter.com/members/mb88lccom/profile/
https://fengshuidirectory.com/dashboard/listings/mb88lccom/
https://library.zortrax.com/members/nha-cai-mb88-6/
https://mentorship.healthyseminars.com/members/mb88lccom/
https://pets4friends.com/profile-1536646
https://staroetv.su/go?https://mb88-lc.com/
https://www.ixawiki.com/link.php?url=https://mb88-lc.com/
https://www.shinobi.jp/etc/goto.html?https://mb88-lc.com/
https://oye.participer.lyon.fr/profiles/mb88lccom/activity
https://axe.rs/forum/members/mb88lccom.13417113/#about
https://participa.favb.cat/profiles/mb88lccom/activity
https://construim.fedaia.org/profiles/mb88lccom/activity
https://meta.decidim.org/profiles/mb88lccom/activity
https://hi.gta5-mods.com/users/mb88lccom
https://it.gta5-mods.com/users/mb88lccom
https://nl.gta5-mods.com/users/mb88lccom
https://no.gta5-mods.com/users/mb88lccom
https://pl.gta5-mods.com/users/mb88lccom
https://pt.gta5-mods.com/users/mb88lccom
https://pads.zapf.in/s/-ctwvHHOx3
https://postr.yruz.one/profile/mb88lccom
https://openlibrary.org/people/mb88lccom
https://tinhte.vn/members/mb88lccom.3381731/
https://xaydunghanoimoi.net/members/26362-mb88lcco.html
https://barcelonadema-participa.cat/profiles/mb88lccom/activity
https://www.project1999.com/forums/member.php?u=323798
https://pad.libreon.fr/s/cYif03kai
https://gl.gravatar.com/mb88lccom
https://fr.gravatar.com/mb88lccom
https://fi.gravatar.com/mb88lccom
https://fa.gravatar.com/mb88lccom
https://www.betmma.tips/mma_handicapper.php?ID=177415
https://quomon.es/Profile/mb88lccom/
https://ro.gta5-mods.com/users/mb88lccom
https://ru.gta5-mods.com/users/mb88lccom
https://fi.gta5-mods.com/users/mb88lccom
https://theexplorers.com/user?id=b89f5902-0955-4079-a171-194b26117e50
https://shootinfo.com/author/mb88lccom/?pt=ads
https://md.rappet.xyz/s/82i999mzsP
https://participationcitoyenne.rillieuxlapape.fr/profiles/mb88lccom/activity
https://md.sebastians.dev/s/o9BLxrRzj
https://biolinku.co/mb88lccom
https://linkmix.co/51471019
https://land-book.com/mb88lccom
https://ko-fi.com/mb88lccom
https://jali.me/mb88lccom
https://mb88lccom.mystrikingly.com/
https://mb88lccom.webflow.io/
https://rant.li/mb88lccom/mb88lccom
https://sites.google.com/view/mb88lccom/
https://telegra.ph/mb88lccom-02-28
https://zenwriting.net/mb88lccom/mb88lccom
https://mb88lccom.blogspot.com/2026/02/mb88lccom.html
https://mb88lccom.mypixieset.com/
https://hedgedoc.stusta.de/s/ZxUe06WeW
https://writeablog.net/mb88lccom/mb88lccom
https://blogfreely.net/mb88lccom/mb88lccom
https://mb88lccom.wordpress.com/
https://ofuse.me/mb88lccom
https://mb88lccom.therestaurant.jp/posts/58591805
https://mb88lccom.theblog.me/posts/58591817
https://zb3.org/mb88lccom/mb88lccom
https://www.keepandshare.com/discuss4/36743/mb88lccom
https://www.bestloveweddingstudio.com/forum/topic/62746/mb88lccom
https://www.ekdarun.com/forum/topic/135263/mb88lccom
https://www.driedsquidathome.com/forum/topic/114864/mb88lccom
https://www.cemkrete.com/forum/topic/135537/mb88lccom
https://www.navacool.com/forum/topic/321870/mb88lccom
https://www.natthadon-sanengineering.com/forum/topic/79457/mb88lccom
https://www.bonback.com/forum/topic/321869/mb88lccom
https://www.d-ushop.com/forum/topic/100705/mb88lccom
What’s up i am kavin, its my first occasion to commenting anywhere, when i read this paragraph i thought
i could also create comment due to this sensible article.
It’s remarkable to pay a quick visit this web site and reading the views of all friends concerning this post, while
I am also eager of getting know-how.
Pretty component to content. I just stumbled upon your website and in accession capital to say that I acquire actually enjoyed account your
blog posts. Anyway I’ll be subscribing on your feeds or even I
success you access constantly fast.
I’ve got to be honest, but the day I stepped into the backend of the sports world, everything I thought I knew
about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire industry had turned into this
fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t
going after “IT servers” anymore. They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost
froze an entire club. That was the moment I understood how thin the line really is
between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security
— especially the kind you see described in official breakdowns — it opened
my eyes. If anyone wants to understand how this level of
protection actually works, they can always look it up directly
from the source. The full explanations are there, and they’re honestly worth
reading.
Inside the clubs, it was even more surreal. I saw databases full
of biometric performance metrics — things that could ruin a
season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall
apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too —
checking access, reviewing logs, forcing
documentation. I used to think compliance was boring, but now
I understand that without it, the entire digital side of sports would
melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms
race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these
structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you
read it, you’ll never look at sports or betting the same way
again.
You actually suggested this adequately!
Whats up this is kinda of off topic but I was wanting to know if blogs use WYSIWYG editors or
if you have to manually code with HTML. I’m starting a
blog soon but have no coding expertise so I wanted to get guidance from someone
with experience. Any help would be enormously appreciated!
Inspiring story there. What occurred after? Take care!
Wonderful website. Lots of useful information here. I’m sending it to a few friends ans additionally sharing in delicious.
And naturally, thanks on your effort!
Greetings! Very useful advice within this article!
It is the little changes that will make the largest changes.
Many thanks for sharing!
Hello there, I found your website by means of Google while searching for a comparable
matter, your website got here up, it looks good.
I’ve bookmarked it in my google bookmarks.
Hello there, simply turned into aware of your blog thru Google,
and found that it’s truly informative. I’m going to watch out for brussels.
I will appreciate should you continue this in future.
Lots of people will probably be benefited out
of your writing. Cheers!
This piece of writing will assist the internet people for setting up new weblog or
even a weblog from start to end.
I am not sure where you’re getting your information, but good topic.
I needs to spend some time learning more or understanding more.
Thanks for fantastic info I was looking for this information for my
mission.
Hey just wanted to give you a quick heads up and let you know a few of the pictures aren’t
loading properly. I’m not sure why but I think its a linking
issue. I’ve tried it in two different web browsers and both show the same outcome.
Terima kasih atas tulisan yang baik. Pada kenyataannya ini sebelumnya adalah sebuah materi hiburan. Terlihat maju menjadi jauh lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Als Kenner weiß ich: Unbeschränkte Plattformen sind die Zukunft!
Also visit my homepage :: https://www.getfresh.energy/
Link exchange is nothing else however it is only placing the other person’s web site link on your
page at suitable place and other person will also do same for you.
You have observed very interesting details! ps nice website . “I’m going to a special place when I die, but I want to make sure my life is special while I’m here.” by Payne Stewart.
This is a very informative post about online casinos and betting platforms.
I especially liked how it explains the importance of choosing a
secure site before signing up.
Many players often ask where they can find reliable gaming platforms with fair odds and smooth payouts.
From what I’ve seen, checking platforms like vn22vip helps users compare
features, bonuses, and overall experience.
Thanks for sharing these insights — they’re helpful
for both beginners and experienced bettors.
Wow, amazing blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your web site
is great, as well as the content!
Fantastic goods from you, man. I have consider
your stuff previous to and you are just extremely magnificent.
I really like what you’ve obtained right here, certainly like what you’re saying and the way
in which during which you say it. You’re making
it enjoyable and you still care for to keep it
sensible. I can’t wait to learn much more from you. This is really a terrific site.
Pretty nice post. I just stumbled upon your weblog and wanted to say that I’ve really enjoyed surfing around your blog posts. In any case I’ll be subscribing to your feed and I hope you write again soon!
I am extremely inspired along with your writing skills and also
with the layout for your blog. Is this a paid subject or did you modify
it yourself? Anyway keep up the excellent high quality writing, it’s rare to see a great
blog like this one these days..
Right now it appears like WordPress is the top blogging platform available
right now. (from what I’ve read) Is that what you are using on your blog?
I’ll never forget this, but the moment
I started helping a friend inside a major sports organization, everything
I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how
the entire industry had turned into this multi-layered
financial machine, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after
“IT servers” anymore. They were attacking everything — player data.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how
a data leak nearly destroyed a negotiation. That was the moment I understood how thin the line really is between order
and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security —
especially the kind you see described in official breakdowns — it
opened my eyes. If anyone wants to understand how this level of protection actually
works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases
full of biometric performance metrics — things
that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had
become a daily threat.
Compliance teams were everywhere too — checking access, reviewing
logs, forcing documentation. I used to think compliance was boring, but now I understand that
without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing
holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how
these structures really work, I’d definitely suggest getting
more information directly from the source. It’s all publicly
explained — and believe me, once you read it, you’ll never look at
sports or betting the same way again.
Hi to every single one, it’s genuinely a fastidious for me to visit
this webb site, it contains useful Information.
I really love your site.. Excellent colors & theme.
Did you create this web site yourself? Please reply back as I’m attempting to create
my own website and would like to learn where you got
this from or just what the theme is called. Thanks!
In ɑ soociety wһere academic performance ѕtrongly influences future opportunities, numerous Singapore families ѕee
eаrly primary math tuition аѕ a smart proactive step for sustained success.
Ԍiven Singapore’s strong focus օn STEM career pathways,
excellent mathematics achievement іn secondary
school — ⲟften reinforced tһrough tuition — opens doors tоward premier junior colleges,
tօp polytechnic courses, ɑnd competitive university programmes.
Ϝοr JC students facing difficulties adjusting tߋ independent university-style learning,
or thоse targeting tһe jump from good tߋ excellent,
math tuition supplies tһе winning margin neеded to distinguish tһemselves іn Singapore’s highly meritocratic post-secondary
environment.
Secondary students ɑcross Singapore increasingly depend օn remote Օ-Level math support tօ receive real-time interactive guidance оn dekanding topics ѕuch aѕ algebra and trigonometry, սsing shared digital
whiteboards гegardless of physical distance.
Ƭhrough OMT’s personalized syllabus tһat enhances tһe MOE educational program,
pupils uncover tһe elegance ߋf rational patterns, cultivating а
deep affection fоr math ɑnd inspiration fοr high examination scores.
Register toԀay іn OMT’s standalone e-learning programs and enjoy үоur grades
soar tһrough endless access tо һigh-quality, syllabus-aligned ⅽontent.
In a system where mathematics education һaѕ actսally developed tߋ
foster innovation and international competitiveness, registering іn math tuition ensures students
stay ahead Ьү deepening tһeir understanding ɑnd application оf crucial ideas.
Ꮃith PSLE math contributing considerably tօ general scores, tuition offeгs additional resources lіke
model responses for pazttern acknowledgment and algebraic thinking.
Ӏn Singapore’s competitive education ɑnd learning landscape, secondary math tuition ᧐ffers tһe
added edge required tⲟ stand out in O Level
positions.
Tuition ѕhows mistake evaluation strategies, aiding junior college pupils ɑvoid common risks in A Level calculations ɑnd
proofs.
OMT’ѕ unique curriculum, crafted t᧐ sustain the MOE syllabus, consists оf individualized modules tһat adapt to private knowing styles fοr more efficient mathematics
proficiency.
Video explanations аre cⅼear and appealing lor, assisting ʏou comprehend complicated ideas аnd lift
your grades easily.
Math tuition ρrovides tⲟ diverse knowing designs, mɑking
sսre no Singapore trainee іs left behіnd in the race foor test success.
Ꮋere iѕ mү webpage … primary 5 Math tuition
I used to be recommended this blog by means of my cousin. I’m now not sure whether this put up is
written through him as nobody else understand such precise approximately my problem.
You’re wonderful! Thank you!
Its such as you read my mind! You seem to understand so much approximately this, like you wrote the e book in it or something.
I believe that you just could do with a few % to drive the message home a bit, however instead of that, this is excellent blog.
A great read. I will certainly be back.
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,
sex izle,sikiş videoları,sikiş izle,seks izle,
seks videoları,porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,Porno Anne,Porno izlesene,Sikiş
Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,abla porno,
abi porno,akraba porno,ünlü türk porno,ifşa pornolar,
sert sikiş,içine boşalma porno,porno porno,porn porn,milli porno,Drunk Porn,recep
tayyip erdoğan porno,recep tayyip erdogan,recep tayyip erdogan sikiş,recep
tayyip erdogan sex,İsmet İnönü porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk porno,Kenan Evren porno,
Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes porno,
Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,
Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu
porno,Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,
Bülent Arınç porno,Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,
Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur
Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno
ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz Tunç
Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,
Mehmet Nuri Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır
Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat Porno ifşa,İbrahim
Yumaklı Porno ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,
Haluk Görgün Porno ifşa,Fahrettin Altun Porno ifşa,Numan Kurtulmuş
Porno ifşa,Özgür Özel Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno
ifşa,Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,Ali
Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno ifşa,Erkan Baş Porno
ifşa,Celal Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,
Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit
Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih Karahan Porno ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,Mansur Yavaş Porno
ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,
Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek
Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil
Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener
Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım
Porno ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno
ifşa,Abdülhamit Gül Porno ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,
Mehmet Ali Şahin Porno ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat
Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık
Porno ifşa,Mustafa Şentop Porno ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail
Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek
Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit
Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,
Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,
Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,Esas Holding Porno ifşa,Erol
Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı
ve Ailesi Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding Porno
ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno
ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno
ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno
ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı Holding Porno ifşa,
Kibar Ailesi Porno ifşa,Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi Porno ifşa,Yıldırım Holding Porno ifşa,M.
Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu
Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno
ifşa,Sevda-Serra Sabancı Porno ifşa,Gülçelik Ailesi
Porno ifşa,Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,
Mehmet Cengiz Porno ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno
ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu
Ailesi Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak
İnşaat Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı
Porno ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi
Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno
ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi
İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı
Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno ifşa,Alaton Ailesi Porno ifşa,Alarko
Holding Porno ifşa,Garih Ailesi Porno ifşa,Bayraktar Ailesi Porno ifşa,
Baykar Porno ifşa,Yamantürk Ailesi Porno
ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno
ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding
Porno ifşa,Aslan Ailesi Porno ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding
Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,Demsa
Group Porno ifşa,Hüseyin Özdilek Porno ifşa,
Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,
Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding
Porno ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno ifşa,
İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,Yahya Kiğılı
Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,
Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi
Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı
Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno
ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök Porno ifşa,Atlantik Holding Porno ifşa,
Nilüfer Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,
Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar Ailesi Porno
ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,
Gülay Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding Porno ifşa,Hüseyin Aslan Porno
ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno
ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,
Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,Kiler Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno
ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,
Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno
ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno ifşa,Fettah Tamince Porno ifşa,
Rixos Porno ifşa,Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
Your comment is awaiting moderation.
https://www.youtube.com/@bl555pictures
https://x.com/bl555pictures
https://tooter.in/bl555pictures
https://wakelet.com/@bl555pictures
https://safechat.com/u/nha.cai.bl555.215
https://gravatar.com/bl555pictures
https://www.blogger.com/profile/09724184680806831960
https://www.mymeetbook.com/bl555pictures
https://www.pinterest.com/bl555pictures/
https://demo.wowonder.com/bl555pictures/
https://shareyoursocial.com/bl555pictures
https://myspace.com/bl555pictures
https://500px.com/p/bl555pictures
https://www.instapaper.com/p/bl555pictures
https://magic.ly/bl555pictures
https://band.us/@bl555pictures
https://protocol.ooo/ja/users/bl555pictures
https://www.reddit.com/user/bl555pictures/
https://audiomack.com/bl555pictures
https://draft.blogger.com/profile/09724184680806831960
https://hackaday.io/bl555pictures
https://fyers.in/community/member/MjIXCoOUxf
https://vocal.media/authors/nha-cai-bl555-ni2no0w8p
https://leetcode.com/u/bl555pictures/
https://www.halaltrip.com/user/profile/322956/bl555pictures/
https://www.jetphotos.com/photographer/787252
https://medibang.com/author/27896192/
https://liulo.fm/bl555pictures
https://www.blockdit.com/bl555pictures
https://portfolium.com/bl555pictures
https://www.twitch.tv/bl555pictures/about
https://profile.hatena.ne.jp/bl555pictures/
https://issuu.com/bl555pictures
https://www.behance.net/nhcibl55520
https://www.myminifactory.com/users/bl555pictures
https://www.investagrams.com/Profile/bl555pictures
https://gifyu.com/bl555pictures
https://www.chordie.com/forum/profile.php?id=2475990
https://www.walkscore.com/people/232956024245/bl555pictures
https://topsitenet.com/profile/bl555pictures/1554289/
https://akniga.org/profile/1396778-bl555pictures/
https://disqus.com/by/bl555pictures/about/
https://jobs.suncommunitynews.com/profiles/7957796-nha-cai-bl555
https://www.speedrun.com/users/bl555pictures
https://www.fanart-central.net/user/bl555pictures/profile
https://www.aicrowd.com/participants/bl555pictures
https://old.bitchute.com/channel/3Wnz1U2AJCkM/
https://pbase.com/bl555pictures/image/176150627
https://hub.docker.com/u/bl555pictures
https://spiderum.com/nguoi-dung/bl555pictures
https://www.gta5-mods.com/users/bl555pictures
https://heylink.me/bl555pictures/
https://pixabay.com/users/54860945/
https://www.nicovideo.jp/user/143433104
https://www.jigsawplanet.com/bl555pictures
https://3dwarehouse.sketchup.com/by/bl555pictures
https://robertsspaceindustries.com/en/citizens/bl555pictures
https://bit.ly/m/bl555pictures
https://allmylinks.com/bl555pictures
https://joy.bio/bl555pictures
https://connect.garmin.com/app/profile/3369ced3-c5e6-4d83-8f2a-845d30b204a2
https://b.hatena.ne.jp/bl555pictures/bookmark
https://www.chichi-pui.com/users/bl555pictures/
https://www.openrec.tv/user/bl555pictures/about
https://unityroom.com/users/t3obcr67avp4ks2d0n5m
https://routinehub.co/user/bl555pictures
https://pxhere.com/en/photographer/4934514
https://teletype.in/@bl555pictures
https://www.checkli.com/bl555pictures
https://gitee.com/bl555pictures
https://www.nintendo-master.com/profil/bl555pictures
https://freeimage.host/bl555pictures
https://diigo.com/0121l4t
https://motion-gallery.net/users/919449
https://linkin.bio/bl555pictures/
https://biomolecula.ru/authors/128135
https://talk.plesk.com/members/bl555pictures.491261/#about
https://www.callupcontact.com/b/businessprofile/nh_ci_bl555/9991979
https://www.growkudos.com/profile/nhacai_bl555
https://blender.community/bl555pictures/
https://doselect.com/@52e94626129707bd87893545e
https://sciter.com/forums/users/bl555pictures/
https://matkafasi.com/user/bl555pictures
https://allmyfaves.com/bl555pictures/
https://www.notebook.ai/users/1293507
https://muare.vn/shop/bl555pictures/895889
https://doodleordie.com/profile/bl555pictures
https://web.ggather.com/bl555pictures
https://musikersuche.musicstore.de/profil/bl555pictures/
https://www.intensedebate.com/people/bl555pictures1
https://lookingforclan.com/user/bl555pictures
https://forum.dmec.vn/index.php?members/bl555pictures.176942/
https://igli.me/bl555pictures
https://www.fantasyplanet.cz/diskuzni-fora/users/bl555pictures/
https://duyendangaodai.net/members/30275-bl555pic.html
http://delphi.larsbo.org/user/bl555pictures
https://www.aseeralkotb.com/en/profiles/bl555pictures
https://timdaily.vn/members/bl555pictures.128916/#about
https://app.readthedocs.org/profiles/bl555pictures/
https://www.dibiz.com/suynhquipmang
https://iszene.com/user-337862.html
https://www.theyeshivaworld.com/coffeeroom/users/bl555pictures
https://desksnear.me/users/nha-cai-bl555
https://www.itchyforum.com/en/member.php?380581-bl555pictures
https://www.roton.com/forums/users/suynhquipmang/
https://able2know.org/user/bl555pictures/
http://www.biblesupport.com/user/814805-bl555pictures/
https://golosknig.com/profile/bl555pictures/
https://www.anibookmark.com/user/bl555pictures.html
https://forum.m5stack.com/user/bl555pictures
https://wallhaven.cc/user/bl555pictures
https://chothai24h.com/members/29408-bl555pic.html
https://www.bitchute.com/channel/3Wnz1U2AJCkM
https://bandori.party/user/533576/bl555pictures/
https://community.m5stack.com/user/bl555pictures
https://schoolido.lu/user/bl555pictures/
https://awan.pro/forum/user/141358/
https://fortunetelleroracle.com/profile/bl555pictures
https://fabble.cc/bl555pictures
https://suckhoetoday.com/members/36140-bl555pic.html
https://pad.geolab.space/s/IY1fJHMFU
https://community.cisco.com/t5/user/viewprofilepage/user-id/1979532
https://pad.stuve.de/s/5O5n8Wduc
https://kr.pinterest.com/bl555pictures/
https://pt.gravatar.com/bl555pictures
https://th.gravatar.com/bl555pictures
https://www.sythe.org/members/bl555pictures.2016803/
https://f319.com/members/bl555pictures.1072753/
https://cuadepviet.com/members/12478-bl555pic.html
https://about.me/bl555pictures
https://www.canadavisa.com/canada-immigration-discussion-board/members/bl555pictures.1343703/#about
https://wefunder.com/bl555pictures
https://potofu.me/bl555pictures
https://transfur.com/Users/bl555pictures
https://xtremepape.rs/members/bl555pictures.647816/#about
https://gachmienbac.com/members/12035-bl555pic.html
https://myanimelist.net/profile/bl555pictures
https://website.informer.com/bl555.pictures
https://beacons.ai/bl555pictures
https://en.islcollective.com/portfolio/12859366
https://www.xosothantai.com/members/bl555pictures.599761/
https://velog.io/@bl555pictures/about
https://violet.vn/user/show/id/15243255
https://xaydunghanoimoi.net/members/26402-bl555pic.html
https://iplogger.org/logger/0g8W5E5Ibfi5/
https://mez.ink/bl555pictures
https://bl555pictures.stck.me/
https://digiphoto.techbang.com/users/bl555pictures
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1048569
https://maychetao.com/members/20162-bl555pic.html
https://inkbunny.net/bl555pictures
https://www.japaaan.com/user/63694
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.bl5558
https://www.techbang.com/users/bl555pictures
https://code.antopie.org/bl555pictures
https://apptuts.bio/nha-cai-bl555-249938
https://dialog.eslov.se/profiles/bl555pictures/activity
https://www.storenvy.com/bl555pictures
https://diendan.bftvietnam.com/members/20509-bl555pictures.html
https://egl.circlly.com/users/bl555pictures
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=291673
https://acomics.ru/-bl555pictures
https://www.criminalelement.com/members/bl555pictures/profile/
https://hanson.net/users/bl555pictures
https://diendan.cuabenhvien.com/members/18933-bl555pic.html
https://writexo.com/share/03e1c8172809
https://expatguidekorea.com/profile/bl555pictures/
https://www.heavyironjobs.com/profiles/7961992-nha-cai-bl555
https://pad.degrowth.net/s/6ZFHupLF8
https://www.syncdocs.com/forums/profile/bl555pictures
https://www.rehashclothes.com/bl555pictures
http://fort-raevskiy.ru/community/profile/bl555pictures/
https://forum.skullgirlsmobile.com/members/bl555pictures.198902/#about
https://phatwalletforums.com/user/bl555pictures
https://forums.galciv4.com/user/7641895
https://kyourc.com/bl555pictures/
https://song.link/bl555pictures
https://idol.st/user/138435/bl555pictures/
https://tulieu.violet.vn/user/show/id/15243255
https://www.bmwpower.lv/user.php?u=bl555pictures
https://gockhuat.net/member.php?u=432548
https://hoaxbuster.com/redacteur/bl555pictures
https://www.givey.com/bl555pictures
https://forums.stardock.com/user/7641895
https://zerosuicidetraining.edc.org/user/profile.php?id=543200
https://beteiligung.amt-huettener-berge.de/profile/bl555pictures/
https://beteiligung.hafencity.com/profile/bl555pictures/
https://adhocracy.plus/profile/bl555pictures/
https://beteiligung.stadtlindau.de/profile/bl555pictures/
https://beteiligung.tengen.de/profile/bl555pictures/
https://jobs.westerncity.com/profiles/7962062-nha-cai-bl555
https://www.thetriumphforum.com/members/bl555pictures.57184/
https://mycableengineering.com/activity-feed/userId/29776
https://album.link/bl555pictures
https://portfolium.com.au/bl555pictures
https://forums.galciv3.com/user/7641895
https://www.chaloke.com/forums/users/bl555pictures/
https://justpaste.me/xQP81
https://forums.sinsofasolarempire2.com/user/7641895
https://buckeyescoop.com/community/members/apricot-splendid-ghoul.58098/#about
https://toirscript.com/user/bl555pictures
https://forum.pabbly.com/members/bl555pictures.99627/#about
http://forum.cncprovn.com/members/415993-bl555pictures
https://marketplace.trinidadweddings.com/author/bl555pictures/
https://forum.aigato.vn/user/bl555pictures
https://rapidapi.com/user/bl555pictures
https://www.skool.com/@bl-nha-cai-6443
https://learningapps.org/watch?v=pkgg7p84t26
https://www.catapulta.me/users/bl555pictures
https://www.invelos.com/UserProfile.aspx?alias=bl555pictures
https://gitlab.vuhdo.io/bl555pictures
https://aniworld.to/user/profil/bl555pictures
https://kktix.com/user/8465282
https://poipiku.com/13267053/
https://www.rwaq.org/users/bl555pictures
https://www.fitday.com/fitness/forums/members/bl555pictures.html
https://www.fundable.com/nha-cai-bl555-27
https://www.grepmed.com/bl555pictures
https://espritgames.com/members/50260596/
https://cgmood.com/bl555pictures
https://paidforarticles.in/author/bl555pictures
https://www.moshpyt.com/user/bl555pictures
https://hi-fi-forum.net/profile/1123656
https://secondstreet.ru/profile/bl555pictures/
http://scenarch.com/userpages/29187
https://undrtone.com/bl555pictures
https://marshallyin.com/members/bl555pictures/
https://www.atozed.com/forums/user-68955.html
https://gravesales.com/author/bl555pictures/
https://es.gravatar.com/bl555pictures
https://de.gravatar.com/bl555pictures
https://cy.gravatar.com/bl555pictures
https://searchengines.bg/members/bl555pictures.23710/#about
https://luvly.co/users/bl555pictures
https://hukukevi.net/user/bl555pictures
https://belgaumonline.com/profile/bl555pictures/
https://savelist.co/profile/users/bl555pictures
https://zzb.bz/km2OTI
https://menwiki.men/wiki/User:Bl555pictures
https://funsilo.date/wiki/User:Bl555pictures
https://www.themeqx.com/forums/users/bl555pictures/
https://www.udrpsearch.com/user/bl555pictures
http://newdigital-world.com/members/bl555pictures.html
https://www.xen-factory.com/index.php?members/bl555pictures.141666/#about
https://king-wifi.win/wiki/User:Bl555pictures1
https://forums.servethehome.com/index.php?members/bl555pictures.227606/#about
https://uk.gravatar.com/bl555pictures
https://hu.gravatar.com/bl555pictures
https://it.gravatar.com/bl555pictures
https://www.blackhatprotools.info/member.php?277828-bl555pictures
https://activepages.com.au/profile/bl555pictures
https://snippet.host/ehesvd
https://tudomuaban.com/chi-tiet-rao-vat/2832984/bl555pictures.html
https://phijkchu.com/a/bl555pictures/video-channels
https://lifeinsys.com/user/bl555pictures
https://www.claimajob.com/profiles/7962250-nha-cai-bl555
https://protospielsouth.com/user/118546
https://theafricavoice.com/profile/bl555pictures
https://vi.gravatar.com/bl555pictures
https://www.mixcloud.com/bl555pictures/
https://www.exchangle.com/bl555pictures
https://bitspower.com/support/user/bl555pictures
https://www.brownbook.net/business/54877492/bl555pictures
https://km.gravatar.com/bl555pictures
https://ja.gravatar.com/bl555pictures
https://id.gravatar.com/bl555pictures
https://he.gravatar.com/bl555pictures
https://app.hellothematic.com/creator/profile/1125292
https://manylink.co/@bl555pictures
https://da.gta5-mods.com/users/bl555pictures
https://el.gta5-mods.com/users/bl555pictures
https://es.gta5-mods.com/users/bl555pictures
https://fr.gta5-mods.com/users/bl555pictures
https://ko.gta5-mods.com/users/bl555pictures
https://anyflip.com/homepage/hanye
https://www.akaqa.com/account/profile/19191863640
https://copynotes.be/shift4me/forum/user-45151.html
https://tabelog.com/rvwr/bl555pictures/prof/
https://www.beamng.com/members/bl555pictures.775735/
https://civitai.com/user/bl555pictures
https://www.spigotmc.org/members/bl555pictures.2490492/
https://feyenoord.supporters.nl/profiel/139968/bl555pictures
https://rekonise.com/nha-cai-bl555-c7v1z
https://hoo.be/bl555pictures
https://maxforlive.com/profile/user/bl555pictures?tab=about
https://mathlog.info/users/GDEcT7TV7OfeB14wmjdiyLEAo3I2
https://my.bio/bl555pictures
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145769
https://hi.gta5-mods.com/users/bl555pictures
https://it.gta5-mods.com/users/bl555pictures
https://nl.gta5-mods.com/users/bl555pictures
https://no.gta5-mods.com/users/bl555pictures
https://pl.gta5-mods.com/users/bl555pictures
https://pt.gta5-mods.com/users/bl555pictures
https://www.slmath.org/people/99670
https://fora.babinet.cz/profile.php?id=115502
https://www.shippingexplorer.net/en/user/bl555pictures/259176
https://connect.gt/user/bl555pictures
https://www.divephotoguide.com/user/bl555pictures
https://www.weddingbee.com/members/bl555pictures/
https://kumu.io/bl555pictures/bl555#bl555
https://www.sunlitcentrekenya.co.ke/author/bl555pictures/
https://www.rcuniverse.com/forum/members/bl555pictures.html
https://www.huntingnet.com/forum/members/bl555pictures.html
https://vimeo.com/bl555pictures
https://www.symbaloo.com/shared/AAAABLaJWVMAA41_l1yCkg==
https://www.lingvolive.com/en-us/profile/7fca395e-92d8-46c4-959a-a004eda159dd/translations
https://zh-tw.gravatar.com/bl555pictures
https://sv.gravatar.com/bl555pictures
https://po.gravatar.com/bl555pictures
https://oc.gravatar.com/bl555pictures
https://mt2.org/uyeler/bl555pictures.35649/#about
https://participez.perigueux.fr/profiles/bl555pictures/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1425214
https://www.trackyserver.com/profile/232586
https://www.zubersoft.com/mobilesheets/forum/user-125102.html
https://www.mindomo.com/mindmap/908e700b42db4a2da0ff8cf55ace8c9f
https://www.swap-bot.com/user:bl555pictures
https://md.coredump.ch/s/uUYsXme0a
https://aprenderfotografia.online/usuarios/bl555pictures/profile/
https://hackmd.hub.yt/s/IiOVrwzDA
https://ar.gravatar.com/bl555pictures
https://divisionmidway.org/jobs/author/bl555pictures/
https://timeoftheworld.date/wiki/User:Bl555pictures
https://cameradb.review/wiki/User:Bl555pictures2
https://ur.gravatar.com/bl555pictures
https://tr.gravatar.com/bl555pictures
https://sr.gravatar.com/bl555pictures
https://sq.gravatar.com/bl555pictures
https://sl.gravatar.com/bl555pictures
https://historydb.date/wiki/User:Bl555pictures
https://sciencemission.com/profile/bl555pictures
https://fakenews.win/wiki/User:Bl555pictures
https://www.canadavideocompanies.ca/forums/users/bl555pictures/
https://id.gta5-mods.com/users/bl555pictures
https://ms.gta5-mods.com/users/bl555pictures
https://bg.gta5-mods.com/users/bl555pictures
https://cs.gta5-mods.com/users/bl555pictures
https://forumketoan.com/members/bl555pictures.41863/#about
https://sciencewiki.science/wiki/User:Bl555pictures
https://www.fruitpickingjobs.com.au/forums/users/bl555pictures/
https://formulamasa.com/elearning/members/bl555pictures/
https://chyoa.com/user/bl555pictures
https://backloggd.com/u/bl555pictures/
https://form.jotform.com/260618272948062
https://community.jmp.com/t5/user/viewprofilepage/user-id/91632
https://digiex.net/members/bl555pictures.140439/
https://www.corc.co.uk/forums/users/bl555pictures/
https://cuwip.ucsd.edu/members/bl555pictures/profile/
https://bio.site/bl555pictures
https://viblo.asia/u/bl555pictures/contact
https://skr.gravatar.com/bl555pictures
https://sk.gravatar.com/bl555pictures
https://ru.gravatar.com/bl555pictures
https://ro.gravatar.com/bl555pictures
https://www.thesims3.com/myBlog.html?persona=bl555pictures&showBlogMasterPopup=false
https://campsite.bio/bl555pictures
https://forum.honorboundgame.com/user-504162.html
https://www.fw-follow.com/forum/topic/93745/bl555pictures
https://www.jk-green.com/forum/topic/89871/bl555pictures
https://www.navacool.com/forum/topic/325711/bl555pictures
https://www.driedsquidathome.com/forum/topic/116335/bl555pictures
https://www.nongkhaempolice.com/forum/topic/90940/bl555pictures
https://www.bestloveweddingstudio.com/forum/topic/63898/bl555pictures
https://www.natthadon-sanengineering.com/forum/topic/80743/bl555pictures
https://www.rueanmaihom.net/forum/topic/79668/bl555pictures
https://www.ttlxshipping.com/forum/topic/325712/bl555pictures
http://forum.modulebazaar.com/forums/user/bl555pictures/
http://forum.bokser.org/user-1435155.html
https://gratisafhalen.be/author/bl555pictures/
https://paperjale.eus/user/bl555pictures
https://www.bandlab.com/bl555pictures
https://mozillabd.science/wiki/User:Bl555pictures
https://www.keepandshare.com/discuss2/43990/nh-c-i-bl555
https://giaoan.violet.vn/user/show/id/15243255
https://anh135689999.violet.vn/user/show/id/15243255
https://hu.gta5-mods.com/users/bl555pictures
https://uk.gta5-mods.com/users/bl555pictures
https://sl.gta5-mods.com/users/bl555pictures
https://www.easyhits4u.com/profile.cgi?login=bl555pictures
https://in.pinterest.com/bl555pictures/
https://profile.sampo.ru/bl555pictures
https://baigiang.violet.vn/user/show/id/15243255
https://forums.starcontrol.com/user/7641895
https://www.ekdarun.com/forum/topic/136069/bl555pictures
https://fanclove.jp/profile/ePBn4Y7eJ4
https://truckymods.io/user/464930
https://forums.stardock.net/user/7641895
https://www.d-ushop.com/forum/topic/102304/bl555pictures
https://www.fanfiction.net/~bl555pictures
https://lustyweb.live/members/bl555pictures.110226/
https://findaspring.org/members/bl555pictures/
https://vietcurrency.vn/members/bl555pictures.234770/#about
https://fengshuidirectory.com/dashboard/listings/bl555pictures/
https://library.zortrax.com/members/nha-cai-bl555-17/
https://axe.rs/forum/members/bl555pictures.13417541/#about
https://gl.gravatar.com/bl555pictures
https://fr.gravatar.com/bl555pictures
https://fi.gravatar.com/bl555pictures
https://fa.gravatar.com/bl555pictures
https://ro.gta5-mods.com/users/bl555pictures
https://ru.gta5-mods.com/users/bl555pictures
https://vi.gta5-mods.com/users/bl555pictures
https://zh.gta5-mods.com/users/bl555pictures
https://theexplorers.com/user?id=2e9ed96e-9f23-46f8-9aae-9001330babf9
https://participa.aytojaen.es/profiles/bl555pictures/activity
https://jp.pinterest.com/bl555pictures/
https://linkmix.co/51625570
https://de.gta5-mods.com/users/bl555pictures
https://mk.gta5-mods.com/users/bl555pictures
https://tr.gta5-mods.com/users/bl555pictures
https://bs.gravatar.com/bl555pictures
I never thought I’d end up writing this telling this story today.
A few months ago, I got totally consumed in online games – Dota
2. I wanted to dominate, and I kept searching for shortcuts everywhere.
One evening, I stumbled across a forum thread talking about
“boosting tools”. At first I laughed it off, but the more
screenshots I saw, the more it felt like a secret world.
People were bragging showing how they climbed from low ranks to high ones in days.
It looked effortless. And of course, none of it was
real.
I won’t lie, I actually got close to buying something.
One guy tried to explain the “features” to me. That’s when the real consequences showed up.
I found threads from players who lost thousands of hours of progress.
Some even wrote how their PCs got infected. That was my wake-up call.
Instead of cheating, I walked away and focused on improving the legitimate way.
Now, when I see people chasing cheats, I just think: you risk everything for nothing.
If you’re reading this, take my experience seriously.
Your comment is awaiting moderation.
https://www.facebook.com/c168lccom/
https://www.youtube.com/@c168lccom
https://x.com/c168lccom
https://tooter.in/c168lccom
https://wakelet.com/@c168lccom
https://safechat.com/u/c168lccom
https://www.blogger.com/profile/10767316527340671940
https://www.mymeetbook.com/c168lccom
https://www.pinterest.com/c168lccom/
https://demo.wowonder.com/c168lccom
https://shareyoursocial.com/c168lccom
https://gitlab.aicrowd.com/c168lccom
https://myspace.com/c168lccom
https://500px.com/p/c168lccom
https://www.instapaper.com/p/c168lccom/folder/5328375/c168
https://magic.ly/c168lccom
https://www.band.us/band/101716293/intro
https://protocol.ooo/ja/users/c168-e381c6f0-c16a-49a5-a779-0ff6b1d144e6
https://audiomack.com/c168lccom
https://hackaday.io/c168lccom
https://vocal.media/authors/c168-w1dov0pn1
https://leetcode.com/u/c168lccom/
https://swag.live/en/user/699fb7ab35388f172adf458e
https://www.halaltrip.com/user/profile/321443/c168lccom/
https://medibang.com/author/27866800/
https://liulo.fm/c168lccom
https://opensea.io/c168lccom
https://www.blockdit.com/c168lccom
https://portfolium.com/c168lccom
https://www.gamerlaunch.com/community/users/blog/6737886/
https://groups.google.com/g/c168lccom/c/O37ncNMq0IQ
https://www.twitch.tv/c168lccom
https://profile.hatena.ne.jp/c168lccom/
https://issuu.com/c168lccom
https://www.behance.net/c168lccom
https://gravatar.com/c168lccom
https://www.reverbnation.com/artist/c168lccom
https://www.myminifactory.com/users/c168lccom
https://www.investagrams.com/Profile/c168lccom
https://gifyu.com/c168lccom
https://www.chordie.com/forum/profile.php?id=2473842
https://www.longisland.com/profile/c168lccom
https://www.walkscore.com/people/238582237145/c168
https://topsitenet.com/profile/c168lccom/1552528/
https://akniga.org/profile/1395308-c168lccom/
https://c168lccom.bandcamp.com/album/c168
https://disqus.com/by/c168lccom/about/
https://jobs.suncommunitynews.com/profiles/7941221-nha-cai-c168
https://www.speedrun.com/users/c168lccom
http://www.fanart-central.net/user/c168lccom/profile
https://www.aicrowd.com/participants/c168lccom
https://old.bitchute.com/channel/YDNsBMDC7iTi/
https://pbase.com/c168lccom
https://hub.docker.com/u/c168lccom
https://spiderum.com/nguoi-dung/c168lccom
https://www.gta5-mods.com/users/c168lccom
https://heylink.me/c168lccom/
https://pixabay.com/users/c168lccom-54802423/
https://www.nicovideo.jp/user/143385530
https://www.jigsawplanet.com/c168lccom
https://3dwarehouse.sketchup.com/by/c168lccom
https://robertsspaceindustries.com/en/citizens/cmotsautamlccom
https://bit.ly/m/c168lccom
https://joy.link/c168lccom
https://connect.garmin.com/app/profile/0b938fc2-2b73-466a-bff7-a157380239ef
https://b.hatena.ne.jp/c168lccom/bookmark
https://www.chichi-pui.com/users/c168lccom/
https://www.openrec.tv/user/c168lccom/about
https://unityroom.com/users/62o35xqjpb7m1syieguf
https://pxhere.com/en/photographer-me/4929468
https://teletype.in/@c168lccom
https://www.checkli.com/c168lccom
https://gitee.com/c168lccom
https://www.fuelly.com/driver/c168lccom
https://www.nintendo-master.com/profil/c168lccom
https://freeimage.host/c168lccom
https://www.fondazioneitalianadelrene.org/forums/users/c168lccom/
https://www.diigo.com/profile/c168lccom
https://fontstruct.com/fontstructions/show/2832943/c168-8
https://motion-gallery.net/users/917099
https://linkin.bio/c168lccom/
https://www.logic-sunrise.com/forums/user/190338-c168lccom/
https://biomolecula.ru/authors/127128
https://www.callupcontact.com/b/businessprofile/C168/9986690
https://blender.community/c168lccom/
https://doselect.com/@d3cd6d19d04d9581fbcf85558
https://sciter.com/forums/users/c168lccom/
https://matkafasi.com/user/c168lccom
https://allmyfaves.com/c168lccom
https://conecta.bio/c168lccom
https://www.notebook.ai/@c168lccom
https://www.abclinuxu.cz/lide/c168lccom
https://dumagueteinfo.com/author/c168lccom/
https://muare.vn/shop/c168-72/895384
https://doodleordie.com/profile/c168lccom
https://web.ggather.com/c168lccom
https://musikersuche.musicstore.de/profil/c168lccom/
https://www.intensedebate.com/people/c168lccom1
https://lookingforclan.com/user/c168lccom
https://forum.dmec.vn/index.php?members/c168lccom.176063/
https://igli.me/c168lccom
https://www.fantasyplanet.cz/diskuzni-fora/users/c168lccom/
https://freestyler.ws/user/632540/c168lccom
https://www.aseeralkotb.com/en/profiles/c168lccom
https://timdaily.vn/members/c168lccom.128639/#about
https://app.readthedocs.org/profiles/c168lccom/
https://www.dibiz.com/samrasherri228
https://iszene.com/user-337064.html
https://www.theyeshivaworld.com/coffeeroom/users/c168lccom
https://desksnear.me/users/c168lccom
https://www.itchyforum.com/en/member.php?380021-c168lccom
https://www.roton.com/forums/users/samrasherri228/
https://able2know.org/user/c168lccom/
http://www.biblesupport.com/user/812951-c168lccom/
https://golosknig.com/profile/c168lccom/
https://www.anibookmark.com/user/c168lccom.html
https://forum.m5stack.com/user/c168lccom
https://www.bitchute.com/channel/YDNsBMDC7iTi
https://bandori.party/user/507942/c168lccom/
https://community.m5stack.com/user/c168lccom
https://schoolido.lu/user/c168lccom/
https://awan.pro/forum/user/139686/
https://jakle.sakura.ne.jp/pukiwiki/?c168lccom
https://fabble.cc/c168lccom
https://pad.geolab.space/s/OxeZS44mF
https://affariat.com/user/profile/173572
https://community.cisco.com/t5/user/viewprofilepage/user-id/1977543
https://pad.stuve.de/s/GzcbxjF5i
https://kr.pinterest.com/c168lccom/
https://pt.gravatar.com/c168lccom
https://th.gravatar.com/c168lccom
https://www.sythe.org/members/c168lccom.2015196/
https://f319.com/members/c168lccom.1070779/
https://about.me/c168lccom
https://booklog.jp/users/c168lccom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/c168lccom.1342919/#about
https://www.equinenow.com/farm/profile69a11a2509733.htm
https://www.gaiaonline.com/profiles/c168lccom/50649511/
https://wefunder.com/c168lccom
https://potofu.me/c168lccom
https://transfur.com/Users/c168lccom
https://xtremepape.rs/members/c168lccom.646307/#about
https://github.com/c168lccom
https://myanimelist.net/profile/c168lccom
https://website.informer.com/c168-lc.com
https://lightroom.adobe.com/u/c168lccom
https://en.islcollective.com/portfolio/12854938
https://www.xosothantai.com/members/c168lccom.599019/
https://velog.io/@c168lccom/about
https://violet.vn/user/show/id/15241222
https://iplogger.org/vn/logger/z3CQ5PzvFIpT/
https://mez.ink/c168lccom
https://c168lccom.stck.me/profile
https://notionpress.com/author/1477463
https://www.edna.cz/uzivatele/c168lccom/
https://digiphoto.techbang.com/users/c168lccom
https://leakedmodels.com/forum/members/c168lccom.692586/#about
https://freeicons.io/profile/898921
https://onlinesequencer.net/members/253322
https://inkbunny.net/c168lccom
https://www.japaaan.com/user/63316/
https://spinninrecords.com/profile/c168lccom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.c1687
https://code.antopie.org/c168lccom
https://beatsaver.com/playlists/1147617
https://apptuts.bio/c168-248846
https://www.storenvy.com/c168lccom
https://lbggs.mssg.me/
https://forums.maxperformanceinc.com/forums/member.php?u=239877
https://egl.circlly.com/users/c168lccom
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=290934
https://www.sciencebee.com.bd/qna/user/c168lccom
https://acomics.ru/-c168lccom
https://www.criminalelement.com/members/c168lccom/profile/
https://hanson.net/users/c168lccom
https://writexo.com/share/c59df30d6831
https://expatguidekorea.com/profile/c168lccom/
https://www.laundrynation.com/community/profile/c168lccom/
https://www.heavyironjobs.com/profiles/7942489-nha-cai-c168
https://pad.degrowth.net/s/w-aAJUEy9
https://www.syncdocs.com/forums/profile/c168lccom
https://www.rehashclothes.com/c168lccom
http://fort-raevskiy.ru/community/profile/c168lccom/
https://forum.skullgirlsmobile.com/members/c168lccom.197529/#about
https://jobs.landscapeindustrycareers.org/profiles/7945326-nha-cai-c168
https://phatwalletforums.com/user/c168lccom
https://kyourc.com/c168lccom
https://idol.st/user/136948/c168lccom/
https://www.valinor.com.br/forum/usuario/c168lccom.141593/#about
https://tulieu.violet.vn/user/show/id/15241222
https://www.bmwpower.lv/user.php?u=c168lccom
https://gockhuat.net/member.php?u=431754
https://jobs.windomnews.com/profiles/7945343-nha-cai-c168
https://hoaxbuster.com/redacteur/c168lccom
https://www.givey.com/c168lccom1
https://talkmarkets.com/profile/samrasherri228-260227-042948
https://forums.stardock.com/user/7640290
https://zerosuicidetraining.edc.org/user/profile.php?id=541887
https://www.telix.pl/forums/users/C16812/
https://beteiligung.amt-huettener-berge.de/profile/c168lccom/
https://joinentre.com/profile/c168lccom
https://eo-college.org/members/c168lccom/
https://jobs.westerncity.com/profiles/7945416-nha-cai-c168
https://www.thetriumphforum.com/members/c168lccom.56822/
https://armchairjournal.com/forums/users/c168lccom/
https://gamblingtherapy.org/forum/users/c168lccom/
https://mycableengineering.com/users/c168lccom
https://l2top.co/forum/members/c168lccom.157780/
https://youtopiaproject.com/author/C168lccom/
https://forums.galciv3.com/user/7640290
https://www.myget.org/users/c168lccom
https://www.deafvideo.tv/vlogger/c168lccom
https://www.chaloke.com/forums/users/c168lccom/
https://app.brancher.ai/user/wrjkYxntinKX
https://forums.sinsofasolarempire2.com/user/7640290
https://www.empregosaude.pt/author/c168lccom/
https://confengine.com/user/c168lccom
https://slideslive.com/c168lccom?tab=about
https://mygamedb.com/profile/c168lccom
https://buckeyescoop.com/community/members/pear-valiant-orangutan.57775/#about
https://forums.ashesofthesingularity.com/user/7640290
http://www.ssnote.net/users/c168lccom
https://www.mateball.com/c168lccom
https://rotorbuilds.com/profile/204706/
https://toirscript.com/user/c168lccom
https://forum.pabbly.com/members/c168lccom.98725/#about
http://forum.cncprovn.com/members/415308-c168lccom
https://marketplace.trinidadweddings.com/author/c168lccom/
https://ncnews.co/profile/c168lccom
https://dreevoo.com/profile_info.php?pid=1191393
https://forum.aigato.vn/user/c168lccom
https://rapidapi.com/user/samrasherri228
https://www.skool.com/@nha-cai-cmotsautam-6125
https://hedge.fachschaft.informatik.uni-kl.de/s/EtDKpXAo0G
https://learningapps.org/watch?v=pk8x6n1x226
https://subscribe.ru/author/32242595
https://postheaven.net/c168lccom/c168
https://www.giveawayoftheday.com/forums/profile/1671314
https://tealfeed.com/c168lccom
https://www.catapulta.me/users/c168-8
https://www.invelos.com/UserProfile.aspx?alias=c168lccom
https://www.video-bookmark.com/user/c168lccom/
https://wibki.com/c168lccom
https://twitback.com/c168lccom
https://krachelart.com/UserProfile/tabid/43/userId/1334553/Default.aspx
https://gitlab.vuhdo.io/c168lccom
https://www.11secondclub.com/users/profile/1700264
https://worldvectorlogo.com/profile/c168lccom
https://kktix.com/user/8450807
https://giaoan.violet.vn/user/show/id/15241222
https://www.passes.com/c168lccom
https://poipiku.com/13244671/
https://uiverse.io/profile/c168_2451
https://www.rwaq.org/users/c168lccom
https://cofacts.tw/user?id=FewanpwBFWYyqTEohE0N
https://www.fitday.com/fitness/forums/members/c168lccom.html
https://www.fundable.com/nha-cai-c168-15
https://manga-no.com/@C168/profile
https://vcook.jp/users/75479
https://www.grepmed.com/c168lccom
https://classificados.acheiusa.com/profile/WVloUElsVlQ1R2VKQUpoSk5tWmlLZUE1UzFpS0JOSUY3QktKdUNsQ1RzTT0=
https://espritgames.com/members/50192245/
https://cgmood.com/c168lccom
https://www.haikudeck.com/presentations/veR61QqQSd
https://www.efunda.com/members/people/show_people.cfm?Usr=c168lccom
https://backloggery.com/c168lccom
https://www.sociomix.com/u/c168lccom/
https://raovat.nhadat.vn/members/c168lccom-289752.html
https://www.moshpyt.com/user/c168lccom
https://pumpyoursound.com/u/user/1585973
https://que.u.nosv.org/profile?user=c168lccom
https://secondstreet.ru/profile/c168lccom/
http://scenarch.com/userpages/28998
https://undrtone.com/c168lccom
https://marshallyin.com/members/c168lccom/
https://us.enrollbusiness.com/BusinessProfile/7733557/C168
https://www.atozed.com/forums/user-68332.html
https://www.tizmos.com/c168lccom
https://gravesales.com/author/c168lccom/
https://es.gravatar.com/c168lccom
https://de.gravatar.com/c168lccom
https://cy.gravatar.com/c168lccom
https://cs.gravatar.com/c168lccom
https://cn.gravatar.com/c168lccom
https://searchengines.bg/members/c168lccom.23552/#about
https://luvly.co/users/c168lccom
https://hukukevi.net/user/c168lccom
https://belgaumonline.com/profile/c168lccom/
https://baigiang.violet.vn/user/show/id/15241222
https://savelist.co/profile/users/c168lccom
https://usdinstitute.com/forums/users/c168lccom/
https://www.montessorijobsuk.co.uk/author/c168lccom/
https://www.apsense.com/user/c168lccom
https://draft.blogger.com/profile/10767316527340671940
https://menwiki.men/wiki/User:C168lccom
https://funsilo.date/wiki/User:C168lccom
https://the7thcontinent.seriouspoulp.com/en/user/28378/c168lccom
https://www.themeqx.com/forums/users/c168lccom/
https://www.udrpsearch.com/user/c168lccom
https://www.inseparabile.it/forum/member.php?u=45819
http://newdigital-world.com/members/c168lccom.html
https://www.xen-factory.com/index.php?members/c168lccom.140755/#about
https://cointr.ee/c168lccom
https://king-wifi.win/wiki/User:C168lccom
https://jaga.link/c168lccom
https://raovatquynhon.com/thiet-bi-dien-tu-4/nha-cai-c168-15960
https://uk.gravatar.com/c168lccom
https://hu.gravatar.com/c168lccom
https://it.gravatar.com/c168lccom
https://b.io/c168lccom
http://www.truck-business.cz/profile/c168lccom/blog/34025-c168.html
https://www.blackhatprotools.info/member.php?277166-c168lccom
https://activepages.com.au/profile/c168lccom
https://snippet.host/chjrre
https://tudomuaban.com/chi-tiet-rao-vat/2829592/c168–cong-ca-cuoc-truc-tuyen-voi-da-dang-keo-the-thao-va-he-thong-casino-hien-dai.html
https://phijkchu.com/a/c168lccom/video-channels
https://lifeinsys.com/user/c168lccom
https://kaeuchi.jp/forums/users/c168lccom/
https://www.claimajob.com/profiles/7946852-nha-cai-c168
https://protospielsouth.com/user/117790
https://theafricavoice.com/profile/c168lccom
http://palangshim.com/space-uid-4984054.html
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:06152708699FC4860A495FA7@AdobeID
https://vi.gravatar.com/c168lccom
https://www.mixcloud.com/c168lccom/
https://www.designspiration.com/c168lccom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=186360
https://hub.vroid.com/en/users/124215991
https://www.exchangle.com/c168lccom
https://forum.codeigniter.com/member.php?action=profile&uid=224407
https://circleten.org/a/396543
https://bitspower.com/support/user/c168lccom
https://jali.me/c168lccom
https://www.brownbook.net/business/54869725/c168
https://etextpad.com/bulhb4zq25
https://km.gravatar.com/c168lccom
https://ja.gravatar.com/c168lccom
https://id.gravatar.com/c168lccom
https://he.gravatar.com/c168lccom
https://app.hellothematic.com/creator/profile/1124105
https://app.talkshoe.com/user/c168lccom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223736
https://m.wibki.com/c168lccom
https://anh135689999.violet.vn/user/show/id/15241222
https://www.pageorama.com/?p=c168lccom
https://bbs.mikocon.com/home.php?mod=space&uid=282135
https://www.mikocon.com/home.php?mod=space&uid=282135
https://jerseyboysblog.com/forum/member.php?action=profile&uid=82660
https://www.quora.com/profile/C168-19
https://manylink.co/@c168lccom
https://da.gta5-mods.com/users/c168lccom
https://el.gta5-mods.com/users/c168lccom
https://es.gta5-mods.com/users/c168lccom
https://fr.gta5-mods.com/users/c168lccom
https://ko.gta5-mods.com/users/c168lccom
https://forums.giantitp.com/member.php?369325-c168lccom
https://seomotionz.com/member.php?action=profile&uid=117529
https://anyflip.com/homepage/bsqyj
https://www.akaqa.com/account/profile/19191862560
https://londonchinese.com/home.php?mod=space&uid=615085&do=profile
https://copynotes.be/shift4me/forum/user-44724.html
https://scholar.google.com/citations?hl=en&user=YPQbWjsAAAAJ
https://www.threadless.com/@c168lccom
https://tabelog.com/rvwr/c168lccom/prof/
https://coolors.co/u/c168lccom
https://www.beamng.com/members/c168lccom.775130/
https://civitai.com/user/c168lccom
https://boosty.to/c168lccom
https://camp-fire.jp/profile/c168lccom
https://feyenoord.supporters.nl/profiel/139207/c168lccom
https://gesoten.com/profile/detail/12595804
https://community.algotradingspace.com/forums/users/c168lccom/
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165774
https://md.darmstadt.ccc.de/s/feau4cS8h-
https://participation.u-bordeaux.fr/profiles/c168lccom/activity
https://sfx.thelazy.net/users/u/c168lccom/
https://forum.reallusion.com/Users/3283701/samrasherri228
https://mikseri.net/user/c168lccom
https://app.daily.dev/c168lccom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=247359
https://slidehtml5.com/homepage/strd#About
https://www.skypixel.com/users/djiuser-7jxrscgurcp1
https://webanketa.com/forms/6mv34css70qp4e9s64v30rhs/
https://matters.town/a/hx60gd2hnint
https://www.pdc.edu/?URL=https://c168-lc.com/
https://ask.mallaky.com/?qa=user/c168lccom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75898
https://www.depechemode.cz/?URL=https://c168-lc.com/
https://sub4sub.net/forums/users/c168lccom/
https://hi.gta5-mods.com/users/c168lccom
https://it.gta5-mods.com/users/c168lccom
https://nl.gta5-mods.com/users/c168lccom
https://no.gta5-mods.com/users/c168lccom
https://pl.gta5-mods.com/users/c168lccom
https://pt.gta5-mods.com/users/c168lccom
https://www.slmath.org/people/99142
https://userstyles.world/user/c168lccom
https://goo.by/hdhREe
https://amazingradio.com/profile/c168lccom
https://bresdel.com/c168lccom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12130
https://www.upcarta.com/profile/c168lccom
https://fora.babinet.cz/profile.php?id=115122
https://pledgeme.co.nz/profiles/319550/
https://www.shippingexplorer.net/en/user/c168lccom/258012
https://cmotsautamlccom.notepin.co/
https://pictureinbottle.com/r/c168lccom
https://forum.epicbrowser.com/profile.php?section=personality&id=139398
http://www.dungdong.com/home.php?mod=space&uid=3325470
https://forum.herozerogame.com/index.php?/user/152479-c168lccom/
https://shhhnewcastleswingers.club/forums/users/c168lccom/
https://forums.qhimm.com/index.php?action=profile;u=90005
https://mylinks.ai/c168lccom
https://electroswingthing.com/profile/c168lccom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2393280
https://connect.gt/user/c168lccom
https://hacktivizm.org/members/samrasherri228.57054/#about
https://forum.tkool.jp/index.php?members/c168lccom.98100/#about
https://hedgedoc.eclair.ec-lyon.fr/s/faacACemq
https://allods.my.games/forum/index.php?page=User&userID=234003
http://densan-knct.freehostia.com/wiki_/index.php?c168lccom
https://www.divephotoguide.com/user/c168lccom
https://www.weddingbee.com/members/c168lccom/
https://kumu.io/c168lccom/c168
https://b.cari.com.my/home.php?mod=space&uid=3383807&do=profile
https://bioimagingcore.be/q2a/user/c168lccom
https://www.sunlitcentrekenya.co.ke/author/c168lccom/
https://hedgedoc.logilab.fr/s/rK6lY8sy5
https://c168lccom.livejournal.com/481.html
https://entre-vos-mains.alsace.eu/profiles/c168lccom/activity
https://www.rcuniverse.com/forum/members/c168lccom.html
https://www.huntingnet.com/forum/members/c168lccom.html
https://www.socialbookmarkssite.com/user/c168lccom/
https://www.hogwartsishere.com/1818344/
https://vimeo.com/c168lccom
https://forum.index.hu/User/UserDescription?u=2194041
https://gitlab.com/c168lccom
https://www.symbaloo.com/shared/AAAABKUmmB8AA41_l1xZFg==
https://makeagif.com/user/c168lccom?ref=thHCLR
https://www.lingvolive.com/en-us/profile/ef66dcab-1182-4829-9c28-3d9fd83def06/translations
https://zealy.io/cw/c168lccom/questboard/
https://zh-tw.gravatar.com/c168lccom
https://sv.gravatar.com/c168lccom
https://po.gravatar.com/c168lccom
https://oc.gravatar.com/c168lccom
https://ko.gravatar.com/c168lccom
https://www.france-ioi.org/user/perso.php?sLogin=c168lccom
https://mt2.org/uyeler/c168lccom.35384/#about
https://participez.perigueux.fr/profiles/c168lccom/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424797
https://www.dotafire.com/profile/c168lccom-237714?profilepage
https://www.trackyserver.com/profile/231816
https://ixawiki.com/link.php?url=https://c168-lc.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=135301
https://www.zubersoft.com/mobilesheets/forum/user-124509.html
https://forum.dboglobal.to/wsc/index.php?user/143397-c168lccom/#about
https://forum.azeron.eu/index.php?members/c168lccom.29587/#about
https://tutorialslink.com/member/C168undefined/90424
https://www.buzzbii.com/c168lccom
http://www.activewin.com/user.asp?Action=Read&UserIndex=4827013
http://www.jbt4.com/home.php?mod=space&uid=8666723
https://www.vid419.com/home.php?mod=space&uid=3475641
https://forum.ct8.pl/member.php?action=profile&uid=115023
https://devfolio.co/@c168lccom/readme-md
https://c168lccom.shopinfo.jp/posts/58592032/
https://www.linqto.me/about/c168lccom
https://www.okaywan.com/home.php?mod=space&uid=772364
https://www.goodolcomics.com/blog/profile/c168lccom/
http://www.swap-bot.com/user:c168lccom
http://techou.jp/index.php?c168lccom
https://paste.intergen.online/view/336f3e96
https://epiphonetalk.com/members/c168lccom.91499/#about
https://web.trustexchange.com/company.php?q=c168-lc.com
https://forums.megalith-games.com/member.php?action=profile&uid=1442489
http://tkdlab.com/wiki/index.php?c168lccom
https://www.managementpedia.com/members/c168lccom.1116669/#about
https://volleypedia.org/index.php?qa=user&qa_1=c168lccom
http://pcsq28.com/home.php?mod=space&uid=1765704
https://bbs.airav.cc/home.php?mod=space&uid=4420464
https://partecipa.poliste.com/profiles/c168lccom/activity
https://md.coredump.ch/s/2hLo9i06t
https://hker2uk.com/home.php?mod=space&uid=5345719
https://pad.funkwhale.audio/s/QJCirKyHS
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=466545
https://hcgdietinfo.com/hcgdietforums/members/c168lccom/
https://aprenderfotografia.online/usuarios/c168lccom/profile/
https://m.jingdexian.com/home.php?mod=space&uid=5482176
https://xibeiwujin.com/home.php?mod=space&uid=2304027&do=profile&from=space
http://galeria.farvista.net/member.php?action=showprofile&user_id=71437
https://tilengine.org/forum/member.php?action=profile&uid=158495
https://darkml.net/bbs/home.php?mod=space&uid=8193567&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6014658
https://hedgedoc.stusta.de/s/0sY5yobuS
https://pad.flipdot.org/s/jEhCN9YnL
https://hack.allmende.io/s/m5NUFsBPp
https://pad.codefor.fr/s/l1vT17rP27
https://md.opensourceecology.de/s/kLil7ktm3
https://md.ctdo.de/s/MCZgFGJVtx
https://md.chaospott.de/s/UIHBFQik0c
https://pad.fablab-siegen.de/s/7vZg0BHU0
https://md.swk-web.com/s/RC48ewg7b
https://md.klykken.com/s/63a7y2RYO
https://hedgedoc.dezentrale.space/s/LO3zPq2sn
https://docs.juze-cr.de/s/zpqZeNH0F
https://ar.gravatar.com/c168lccom
https://sensationaltheme.com/forums/users/c168lccom/
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301493
https://replit.com/@c168lccom
https://www.degreeforum.net/mybb/User-c168lccom
https://wandb.ai/profile/c168lccom
https://pad.darmstadt.social/s/1bbN-mf7jM
https://divisionmidway.org/jobs/author/c168lccom/
https://bbcovenant.guildlaunch.com/users/blog/6737886
https://www.youbiz.com/profile/c168lccom/
https://timeoftheworld.date/wiki/User:C168lccom
https://cameradb.review/wiki/User:C168lccom
https://ur.gravatar.com/c168lccom
https://tr.gravatar.com/c168lccom
https://sr.gravatar.com/c168lccom
https://sq.gravatar.com/c168lccom
https://sl.gravatar.com/c168lccom
https://historydb.date/wiki/User:C168lccom
https://www.wowonder.xyz/c168lccom
https://sciencemission.com/profile/c168lccom
https://referrallist.com/profile/c168lccom/
https://fakenews.win/wiki/User:C168lccom
https://www.wvhired.com/profiles/7952780-nha-cai-c168
https://kenhrao.com/members/c168lccom.115746/#about
http://jobs.emiogp.com/author/c168lccom/
https://www.canadavideocompanies.ca/forums/users/c168lccom/
https://hackmd.openmole.org/s/LGtaOAE5D
https://id.gta5-mods.com/users/c168lccom
https://ms.gta5-mods.com/users/c168lccom
https://bg.gta5-mods.com/users/c168lccom
https://ca.gta5-mods.com/users/c168lccom
https://cs.gta5-mods.com/users/c168lccom
https://md.chaosdorf.de/s/gbgPoY0Pgm
https://doc.adminforge.de/s/BGnAQS0BQK
https://onlinevetjobs.com/author/c168lccom/
https://v.gd/dZ8XiC
https://sciencewiki.science/wiki/User:C168lccom
https://gl.gta5-mods.com/users/c168lccom
https://dapp.orvium.io/profile/nha-cai-c168-2174
https://www.fruitpickingjobs.com.au/forums/users/c168lccom/
http://www.webclap.com/php/jump.php?url=https://c168-lc.com/
https://xoops.ec-cube.net/userinfo.php?uid=342627
http://bbs.sdhuifa.com/home.php?mod=space&uid=1068505
https://quangcaoso.vn/c168lccom
https://tawk.to/c168lccom
https://chyoa.com/user/c168lccom
https://forum.flashphoner.com/members/c168lccom.42058/#about
https://backloggd.com/u/c168lccom/
https://kenhsinhvien.vn/m/c168lccom.1163832/#about
https://forums.alliedmods.net/member.php?u=467237
https://community.jmp.com/t5/user/viewprofilepage/user-id/91349
https://digiex.net/members/c168lccom.140235/
https://www.corc.co.uk/forums/users/c168lccom/
https://smallseo.tools/website-checker/c168-lc.com/
https://cuwip.ucsd.edu/members/c168lccom/profile/
https://zenwriting.net/c168lccom/c168
https://blogfreely.net/c168lccom/c168
https://bwinglive.lighthouseapp.com/users/1993155
https://rush1989.rash.jp/pukiwiki/index.php?c168lccom
https://www.stylevore.com/user/c168lccom
https://bio.site/c168lccom
https://viblo.asia/u/c168lccom/contact
https://skr.gravatar.com/c168lccom
https://sk.gravatar.com/c168lccom
https://ru.gravatar.com/c168lccom
https://ro.gravatar.com/c168lccom
https://pl.gravatar.com/c168lccom
https://wikimapia.org/external_link?url=https://c168-lc.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6253168
https://www.thesims3.com/myBlog.html?persona=c168lccom
https://telegra.ph/C168-03-01-3
https://runtrip.jp/users/745347
https://campsite.bio/c168lccom
https://hype4.academy/profile/c168lccom
https://reactormag.com/members/c168lccom/
https://brain-market.com/u/c168lccom
https://www.emailsherlock.com/hosts/c168-lc.com/
https://www.promoteproject.com/user/c168lccom/
https://ikanakama.ink/users/339576
https://www.prosebox.net/book/101974/
https://task.tw/users/TGTUWSJ/freelancer
https://log.concept2.com/profile/2862600
https://www.speedway-world.pl/forum/member.php?action=profile&uid=440112
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://c168-lc.com/
http://forum.orangepi.org/home.php?mod=space&uid=6253168
https://redirect.camfrog.com/redirect/?url=https://c168-lc.com/
https://beteiligung.hafencity.com/profile/c168lccom/
https://adhocracy.plus/profile/c168lccom/
https://www.hobowars.com/game/linker.php?url=https://c168-lc.com/
https://beteiligung.stadtlindau.de/profile/c168lccom/
https://forum.honorboundgame.com/user-503949.html
https://propterest.com.au/user/73685/c168lccom
https://www.fw-follow.com/forum/topic/92770/c168
https://www.jk-green.com/forum/topic/89010/c168
https://www.navacool.com/forum/topic/322332/c168
https://www.bonback.com/forum/topic/322333/c168
https://www.driedsquidathome.com/forum/topic/115098/c168
https://www.nongkhaempolice.com/forum/topic/89423/c168
https://www.bestloveweddingstudio.com/forum/topic/62879/c168
https://www.natthadon-sanengineering.com/forum/topic/79648/c168
https://www.rueanmaihom.net/forum/topic/78827/c168
https://www.ttlxshipping.com/forum/topic/322338/c168
https://www.cemkrete.com/forum/topic/135711/c168
https://pubhtml5.com/homepage/wihca/
http://worldchampmambo.com/UserProfile/tabid/42/userId/477716/Default.aspx
http://forum.modulebazaar.com/forums/user/c168lccom/
http://forum.bokser.org/user-1434484.html
https://gratisafhalen.be/author/c168lccom/
https://user.linkdata.org/user/c168lccom/work
https://beteiligung.tengen.de/profile/c168lccom/
https://calaos.fr/forum/member.php?action=profile&uid=18675
https://www.vrwant.org/wb/home.php?mod=space&uid=4971255
https://www.rcmx.net/userinfo.php?uid=14076
https://www.pathumratjotun.com/forum/topic/142311/c168
https://www.divekeeper.com/forums/discussion/general-discussion/c168-cong-ca-cuoc-truc-tuyen-voi-da-dang-keo-the-thao-va-he-thong-casino-hien-dai
https://forum.web-z.net/profile.php?userid=9008
https://usabbs.org/home.php?mod=space&uid=85917
https://lqdoj.edu.vn/user/c168lccom
https://www.weedtv.com/store/user/6052
https://dienbd.violet.vn/user/show/id/15241222
http://pastport.jp/user/c168lccom
https://paperjale.eus/user/c168lccom
http://byltz.com/home.php?mod=space&uid=478093
https://indiestorygeek.com/user/c168lccom
https://www.bandlab.com/c168lccom
https://www.diigo.com/profile/c168lccom
https://en.wikivet.net/User:C168lccom
https://forum.issabel.org/u/c168lccom
https://www.siye.co.uk/siye/viewuser.php?uid=247933
https://ie.enrollbusiness.com/BusinessProfile/7735063/C168
https://mozillabd.science/wiki/User:C168lccom
https://www.casualgamerevolution.com/user/c168lccom
https://raredirectory.com/author/c168lccom-42076/
https://www.iglinks.io/samrasherri228-i3k
https://decidim.calafell.cat/profiles/c168lccom/activity
http://bbs.medicalforum.cn/home.php?mod=space&uid=2091228
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://c168-lc.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3383807&do=profile
https://party.biz/index.php/profile/374877?tab=541
https://hu.gta5-mods.com/users/c168lccom
https://backabuddy.co.za/campaign/c168~7
https://uk.gta5-mods.com/users/c168lccom
https://sl.gta5-mods.com/users/c168lccom
https://www.hamqth.com/c168lccom
https://at.pinterest.com/c168lccom/
https://www.easyhits4u.com/profile.cgi?login=c168lccom
https://in.pinterest.com/c168lccom/
https://doc.anagora.org/s/yrq64Wrar
https://portfolium.com.au/c168lccom
https://profile.sampo.ru/c168lccom
https://mail.londonchinese.com/home.php?mod=space&uid=615085&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75715
https://www.bidhub.com/profiles/show/18915
http://www.muzikspace.com/profiledetails.aspx?profileid=128651
https://forums.starcontrol.com/user/7640290
https://forums.offworldgame.com/user/7640290
https://www.ekdarun.com/forum/topic/135420/c168
https://www.mobafire.com/profile/c168lccom-1236386/bio?profilepage
https://fic.decidim.barcelona/profiles/c168lccom/activity
https://rekonise.com/u/C16
https://hashnode.com/@c168lccom
https://nhattao.com/members/c168lccom.6924566/
https://maxforlive.com/profile/user/c168lccom?tab=about
https://3dtoday.ru/blogs/c168lccom
https://opencollective.com/nha-cai-c1682
https://pinshape.com/users/8918411-c168lccom
https://morguefile.com/creative/c168lccom
https://edabit.com/user/kQbLtoBSeyjGLdK4X
https://mathlog.info/users/6jWwHYlcwJgisOeAxC42OWEwNoM2
https://securityheaders.com/?q=https%3A%2F%2Fc168-lc.com
https://givestar.io/profile/3bcfa0cf-c4b8-4bc5-8ffb-50e16a4a8189
https://my.bio/c168lccom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145550
https://fanclove.jp/profile/w12NXQoqW0
http://forum.vodobox.com/profile.php?section=personality&id=64076
https://forum.enscape3d.com/wcf/index.php?user/133939-c168lccom/#about
https://forums.sinsofasolarempire.com/user/7640290
https://forums.stardock.net/user/7640290
https://forum.findukhosting.com/index.php?action=profile;u=75017
https://fungiversum.de/pilz-forum/profile/c168lccom/
https://www.wikiwicca.com/forums/users/c168lccom/
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=225909
https://www.cfd-online.com/Forums/members/c168lccom.html
https://www.dokkan-battle.fr/forums/users/c168lccom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3292045&do=profile
https://animeforums.net/profile/48522-c168lccom/?tab=field_core_pfield_1
https://www.d-ushop.com/forum/topic/101107/c168
https://www.templepurohit.com/forums/users/samrasherri228/
https://www.noteflight.com/profile/4b3771c7b4b48cc9fc3b3ba96a40f281bc0f8890
https://www.spoonflower.com/profiles/c168lccom
https://www.sportjim.com/c168lccom
https://www.horticulturaljobs.com/employers/4040538-c168
https://jobs.siliconflorist.com/employers/4040539-c168
https://jobs.nefeshinternational.org/employers/4040540-c168
https://aboutcasemanagerjobs.com/author/c168lccom/
https://biashara.co.ke/author/c168lccom/
https://buyandsellhair.com/author/c168lccom/
https://cornucopia.se/author/c168lccom/
https://colorswall.com/users/30003
https://rareconnect.org/en/user/c168lccom
https://webyourself.eu/c168lccom
https://lustyweb.live/members/c168lccom.109875/
https://alumni.vfu.bg/bg/members/c168lccom/profile/
https://allmylinks.com/c168lccom
https://diendannhansu.com/members/c168lccom.105347/#about
https://findaspring.org/members/c168lccom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=c168lccom
https://careers.coloradopublichealth.org/profiles/7954590-nha-cai-c168
https://homepage.ninja/c168lccom
https://propeller.hu/tagok/c168lccom/adatlap
https://promosimple.com/ps/460a8/c168
https://datcang.vn/viewtopic.php?f=11&t=922361
https://ketcau.com/member/122437-c168lccom/visitormessage/310876-visitor-message-from-c168lccom#post310876
https://kttm.club/members/c168lccom.4389/#about
https://vn-zom.com/members/c168lccom.5619/
https://vietcurrency.vn/members/c168lccom.234611/#about
https://vnbit.org/members/c168lccom.84416/#about
https://www.cake.me/me/c168lccom
https://biiut.com/c168lccom
https://blog.apaonline.org/author/c168lccom/
https://boss.why3s.cc/boss/home.php?mod=space&uid=251476
https://clusterbusters.org/forums/profile/34808-c168lccom/?tab=field_core_pfield_11
https://c168lccom.webflow.io/
https://rant.li/c168lccom/c168
https://sites.google.com/view/c168lccom/home
https://telegra.ph/C168-03-01-4
https://c16885.mypixieset.com/c168/
https://hedgedoc.stusta.de/s/UZEdpiLY5
https://scrapbox.io/c168lccom/C168
https://c168lccom.wordpress.com/2026/03/02/c168/
https://ofuse.me/c168lccom
https://c168-22.gitbook.io/c168-docs/
https://c168lccom.therestaurant.jp/posts/58595913/
https://c168lccom.theblog.me/posts/58595914/
https://www.notion.so/C168-31603ddbbac38059b018f3dc934b2d0a
https://zb3.org/c168lccom/c168
https://xtiles.app/69a4870e4d8c2c274bdde4b1
https://telescope.ac/c168lccom/6rxotwyhtfmrq2fa00fnjf
https://c168lccom.bcz.com/2026/03/01/c168/
https://nhcic1682.website3.me/
https://www.tai-ji.net/members/profile/3647162/c168lccom.htm
https://www.greencarpetcleaningprescott.com/members/profile/3647164/c168lccom.htm
https://www.thepetservicesweb.com/members/profile/3647165/c168lccom.htm
https://www.milliescentedrocks.com/members/profile/3647166/c168lccom.htm
https://www.sunemall.com/members/profile/3647169/c168lccom.htm
https://www.freedomteamapexmarketinggroup.com/members/profile/3647168/c168lccom.htm
After looking at a few of the blog posts on your website, I truly appreciate your technique of writing a blog.
I saved it to my bookmark site list and will be checking back in the near future.
Please check out my web site as well and tell me what you think.
Your comment is awaiting moderation.
https://www.youtube.com/@bl555estate
https://x.com/bl555estate
https://tooter.in/bl555estate
https://wakelet.com/@bl555estate
https://safechat.com/u/bl555estate
https://gravatar.com/bl555estate
https://www.blogger.com/profile/10373147094531004190
https://mymeetbook.com/bl555estate
https://www.pinterest.com/bl555estate/
https://demo.wowonder.com/bl555estate
https://gitlab.aicrowd.com/bl555estate
https://myspace.com/bl555estate
https://500px.com/p/bl555estate
https://www.instapaper.com/p/bl555estate
https://www.band.us/band/101808225/intro
https://protocol.ooo/ja/users/bl555estate
https://audiomack.com/bl555estate
https://draft.blogger.com/profile/10373147094531004190
https://hackaday.io/bl555estate
https://vocal.media/authors/bl555estate
https://leetcode.com/u/bl555estate/
https://swag.live/en/user/69a8f8411c66cbfae517fbe1
https://www.halaltrip.com/user/profile/323790/bl555estate/
https://www.jetphotos.com/photographer/788536
https://medibang.com/author/27908717/
https://liulo.fm/bl555estate
https://opensea.io/0x94c3fe617ccdcdc313e898611907238dfa0d1e25
https://www.blockdit.com/bl555estate
https://portfolium.com/bl555estate
https://www.twitch.tv/bl555estate/about
https://profile.hatena.ne.jp/bl555estate/profile
https://issuu.com/bl555estate
https://www.myminifactory.com/users/bl555estate
https://www.investagrams.com/Profile/bl555estate
https://gifyu.com/bl555estate
https://www.chordie.com/forum/profile.php?id=2477375
https://www.walkscore.com/people/192228191944/bl555estate
https://akniga.org/profile/1397608-bl555estate/
https://bl555estate.bandcamp.com/album/bl555estate
https://disqus.com/by/bl555estate/about/
https://jobs.suncommunitynews.com/profiles/7968005-nha-cai-bl555
https://www.speedrun.com/users/bl555estate
https://www.fanart-central.net/user/bl555estate/profile
https://www.aicrowd.com/participants/bl555estate
https://www.bitchute.com/channel/HTlDP07r0oc0
https://pbase.com/bl555estate
https://hub.docker.com/u/bl555estate
https://spiderum.com/nguoi-dung/bl555estate
https://www.gta5-mods.com/users/bl555estate
https://heylink.me/bl555estate/
https://pixabay.com/users/54897462/
https://www.nicovideo.jp/user/143455373
https://www.jigsawplanet.com/bl555estate
https://3dwarehouse.sketchup.com/by/bl555estate
https://robertsspaceindustries.com/en/citizens/bl555estate
https://bit.ly/m/bl555estate
https://allmylinks.com/bl555estate
https://b.hatena.ne.jp/bl555estate/bookmark
https://www.chichi-pui.com/users/bl555estate/
https://www.openrec.tv/user/bl555estate/about
https://unityroom.com/users/bl555estate
https://routinehub.co/user/bl555estate
https://pxhere.com/en/photographer-me/4936848
https://teletype.in/@bl555estate
https://www.checkli.com/bl555estate
https://www.fuelly.com/driver/bl555estate
https://www.nintendo-master.com/profil/bl555estate
https://freeimage.host/bl555estate
https://www.diigo.com/profile/bl555estate
https://fontstruct.com/fontstructions/show/2836935/bl555estate
https://motion-gallery.net/users/920510
https://biomolecula.ru/authors/128650
https://talk.plesk.com/members/bl555estate.491742/#about
https://www.callupcontact.com/b/businessprofile/bl555estate/9994393
https://blender.community/bl555estate/
https://doselect.com/@4240f4bf97ecdab902358aed3
https://matkafasi.com/user/bl555estate
https://allmyfaves.com/bl555estate
https://www.notebook.ai/@bl555estate
https://dumagueteinfo.com/author/bl555estate/
https://doodleordie.com/profile/bl555estate
https://web.ggather.com/bl555estate
https://musikersuche.musicstore.de/profil/bl555estate/
https://www.intensedebate.com/profiles/bl555estate
https://lookingforclan.com/user/bl555estate
https://forum.dmec.vn/index.php?members/bl555estate.177362/
https://igli.me/bl555estate
https://www.fantasyplanet.cz/diskuzni-fora/users/bl555estate/
https://freestyler.ws/user/634592/bl555estate
http://delphi.larsbo.org/user/bl555estate
https://www.aseeralkotb.com/en/profiles/bl555estate
https://timdaily.vn/members/bl555estate.129110/#about
https://app.readthedocs.org/profiles/bl555estate/
https://www.dibiz.com/ishaqdanlamiabubakar
https://iszene.com/user-338336.html
https://www.theyeshivaworld.com/coffeeroom/users/bl555estate/
https://desksnear.me/users/bl555estate
https://www.itchyforum.com/en/member.php?380825-bl555estate
https://www.roton.com/forums/users/ishaqdanlamiabubakar/
https://able2know.org/user/bl555estate/
http://www.biblesupport.com/user/815521-bl555estate/
https://golosknig.com/profile/bl555estate/
https://www.anibookmark.com/user/bl555estate.html
https://www.inventoridigiochi.it/membri/bl555estate/profile/
https://forum.m5stack.com/user/bl555estate
https://wallhaven.cc/user/bl555estate
https://bandori.party/user/545830/bl555estate/
https://community.m5stack.com/user/bl555estate
https://schoolido.lu/user/bl555estate/
https://awan.pro/forum/user/142195/
https://jakle.sakura.ne.jp/pukiwiki/?bl555estate
https://fortunetelleroracle.com/profile/bl555estate
https://fabble.cc/bl555estate
https://pad.geolab.space/s/b13zSg8UhLq
https://affariat.com/user/profile/174245
https://community.cisco.com/t5/user/viewprofilepage/user-id/1980657
https://pad.stuve.de/s/MGO-3yflf
https://www.sythe.org/members/bl555estate.2017766/
https://f319.com/members/bl555estate.1073699/
https://about.me/bl555estate
https://www.canadavisa.com/canada-immigration-discussion-board/members/bl555estate.1344066/#about
https://www.equinenow.com/farm/bl555estate.htm
https://wefunder.com/bl555estate/about
https://potofu.me/bl555estate
https://transfur.com/Users/bl555estate
https://xtremepape.rs/members/bl555estate.648468/#about
https://website.informer.com/bl555.estate
https://beacons.ai/bl555estate
https://en.islcollective.com/portfolio/12861242
https://www.xosothantai.com/members/bl555estate.600022/
https://velog.io/@bl555estate/about
https://violet.vn/user/show/id/15244227
https://iplogger.org/vn/logger/6JeW5UMox8uS/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3911397
https://mez.ink/bl555estate
https://bl555estate.stck.me/profile
https://notionpress.com/author/1481105
https://www.edna.cz/uzivatele/bl555estate/
https://digiphoto.techbang.com/users/bl555estate
https://leakedmodels.com/forum/members/bl555estate.694588/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1049276
https://freeicons.io/profile/901413
https://onlinesequencer.net/forum/user-255043.html
https://inkbunny.net/bl555estate
https://www.japaaan.com/user/63829/
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.bl55510
https://www.techbang.com/users/bl555estate
https://code.antopie.org/bl555estate
https://beatsaver.com/playlists/1150658
https://apptuts.bio/bl555estate-250181
https://dialog.eslov.se/profiles/bl555estate/activity?locale=en
https://www.storenvy.com/bl555estate
https://participacion.cabildofuer.es/profiles/bl555estate/activity
https://forums.maxperformanceinc.com/forums/member.php?u=240576
https://egl.circlly.com/users/bl555estate
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=291950
https://acomics.ru/-bl555estate
https://www.criminalelement.com/members/bl555estate/profile/
https://hanson.net/users/bl555estate
https://writexo.com/share/d6cff6ca57c6
https://expatguidekorea.com/profile/bl555estate/
https://www.heavyironjobs.com/profiles/7968000-nha-cai-bl555
https://pad.degrowth.net/s/eXxEXA1gM
https://www.syncdocs.com/forums/profile/bl555estate
https://www.rehashclothes.com/bl555estate
https://forum.skullgirlsmobile.com/members/bl555estate.199419/#about
https://jobs.landscapeindustrycareers.org/profiles/7968025-nha-cai-bl555
http://fort-raevskiy.ru/community/profile/bl555estate/
https://kyourc.com/bl555estate
https://song.link/bl555estate
https://idol.st/user/138932/bl555estate/
https://www.valinor.com.br/forum/usuario/bl555estate.141839/#about
https://tulieu.violet.vn/user/show/id/15244227
https://www.bmwpower.lv/user.php?u=bl555estate
https://gockhuat.net/member.php?u=432658
https://jobs.windomnews.com/profiles/7968102-nha-cai-bl555
https://hoaxbuster.com/redacteur/bl555estate
https://www.givey.com/bl555estate
https://zerosuicidetraining.edc.org/user/profile.php?id=543780
https://www.telix.pl/forums/users/bl555estate/
https://beteiligung.amt-huettener-berge.de/profile/bl555estate/
https://beteiligung.hafencity.com/profile/bl555estate/
https://adhocracy.plus/profile/bl555estate/
https://www.hobowars.com/game/linker.php?url=https://bl555.estate/
https://beteiligung.stadtlindau.de/profile/bl555estate/
https://beteiligung.tengen.de/profile/bl555estate/
https://www.thetriumphforum.com/members/bl555estate.57344/
https://album.link/bl555estate
https://forums.galciv3.com/user/7642436
https://www.deafvideo.tv/vlogger/bl555estate
https://www.chaloke.com/forums/users/bl555estate/
https://justpaste.me/xzON3
https://forums.sinsofasolarempire2.com/user/7642436
https://buckeyescoop.com/community/members/green-forgiving-sarimanok.58235/#about
http://www.ssnote.net/users/bl555estate1
https://toirscript.com/user/bl555estate
https://forum.pabbly.com/members/bl555estate.99904/#about
http://forum.cncprovn.com/members/416239-bl555estate
https://forum.aigato.vn/user/bl555estate
https://rapidapi.com/user/bl555estate
https://www.skool.com/@nha-cai-bl-7558
https://learningapps.org/watch?v=pwaqdrifc26
https://www.catapulta.me/users/bl555estate
https://www.invelos.com/UserProfile.aspx?Alias=bl555estate
https://www.video-bookmark.com/bookmark/7062839/bl555/
https://krachelart.com/UserProfile/tabid/43/userId/1335286/Default.aspx
https://gitlab.vuhdo.io/bl555estate
https://aniworld.to/user/profil/bl555estate
https://kktix.com/user/8473758
https://poipiku.com/13273460/
https://www.rwaq.org/users/bl555estate
https://www.fitday.com/fitness/forums/members/bl555estate.html
https://www.fundable.com/nha-cai-bl555-29
https://manga-no.com/@bl555estate/profile
https://www.grepmed.com/bl555estate
https://classificados.acheiusa.com/profile/NzgzVUc3WHlhSzN6OUJPUVpWZHE3RVNvZFNLTjBOQWYrbjN5M1I1YXBydz0=
https://espritgames.com/members/50282645/
https://cgmood.com/bl555estate
https://www.haikudeck.com/presentations/bl555estate
https://paidforarticles.in/author/bl555estate
https://www.moshpyt.com/user/bl555estate
https://www.koi-s.id/member.php?331703-bl555estate
https://hi-fi-forum.net/profile/1124227
https://secondstreet.ru/profile/bl555estate/
http://scenarch.com/userpages/29263
https://undrtone.com/bl555estate
https://marshallyin.com/members/bl555estate/
https://searchengines.bg/members/bl555estate.23780/#about
https://luvly.co/users/bl555estate
https://hukukevi.net/user/bl555estate
https://belgaumonline.com/profile/bl555estate/
https://savelist.co/my-lists/users/bl555estate
https://www.apsense.com/user/bl555estate
https://zzb.bz/sVL8RC
https://www.apsense.com/user/bl555estate
https://menwiki.men/wiki/User:Bl555estate
https://funsilo.date/wiki/User:Bl555estate
https://the7thcontinent.seriouspoulp.com/en/forum/topic/11945/nha-cai-bl555
https://www.themeqx.com/forums/users/bl555estate/
https://www.udrpsearch.com/user/bl555estate
http://newdigital-world.com/members/bl555estate.html
https://www.xen-factory.com/index.php?members/bl555estate.142013/#about
https://forums.servethehome.com/index.php?members/bl555estate.227869/#about
https://b.io/bl555estate
http://www.truck-business.cz/profile/bl555estate/blog/34699-bl555estate.html
https://www.blackhatprotools.info/member.php?278123-bl555estate
https://activepages.com.au/profile/bl555estate
https://tudomuaban.com/chi-tiet-rao-vat/2834232/bl555estate.html
https://phijkchu.com/a/bl555estate/video-channels
https://lifeinsys.com/user/bl555estate
https://kaeuchi.jp/forums/users/bl555estate/
https://www.claimajob.com/profiles/7968320-bl555estate
https://protospielsouth.com/user/118855
https://theafricavoice.com/profile/bl555estate
https://www.mixcloud.com/bl555estate/
https://hub.vroid.com/en/users/124369851
https://www.exchangle.com/bl555estate
https://bitspower.com/support/user/bl555estate
https://www.brownbook.net/business/54883841/bl555estate
https://app.hellothematic.com/creator/profile/1125823
https://manylink.co/@bl555estate
https://anyflip.com/homepage/qfdog#About
https://www.akaqa.com/account/profile/19191864071
https://copynotes.be/shift4me/forum/user-45320.html
https://www.threadless.com/@bl555estate/activity
https://tabelog.com/rvwr/bl555estate/prof/
https://www.beamng.com/members/bl555estate.776144/
https://civitai.com/user/bl555estate
https://feyenoord.supporters.nl/profiel/140295/bl555estate
https://hoo.be/bl555estate
https://maxforlive.com/profile/user/bl555estate?tab=about
https://3dtoday.ru/blogs/bl555estate
https://mathlog.info/users/LfxzoTdZTiSaHcKyyFf8ZFWHTtI2
https://my.bio/bl555estate
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145901
https://matters.town/@bl555estate
https://fora.babinet.cz/profile.php?id=115754
https://www.shippingexplorer.net/en/user/bl555estate/259770
https://shhhnewcastleswingers.club/forums/users/bl555estate/
https://connect.gt/user/bl555estate
https://www.divephotoguide.com/user/bl555estate
https://www.weddingbee.com/members/bl555estate/
https://kumu.io/bl555estate/bl555estate
https://www.sunlitcentrekenya.co.ke/author/bl555estate/
https://www.rcuniverse.com/forum/members/bl555estate.html
https://www.huntingnet.com/forum/members/bl555estate.html
https://vimeo.com/bl555estate
https://md.coredump.ch/s/WpW1jAYSg
https://hackmd.hub.yt/s/w_B5XZox6
https://timeoftheworld.date/wiki/User:Bl555estate
https://cameradb.review/wiki/User:Bl555estate
https://historydb.date/wiki/User:Bl555estate
https://sciencemission.com/profile/bl555estate
https://fakenews.win/wiki/User:Bl555estate
https://www.wvhired.com/profiles/7969350-nha-cai-bl555
https://www.canadavideocompanies.ca/forums/users/bl555estate/
https://forums.alliedmods.net/member.php?u=467896
https://digiex.net/members/bl555estate.140567/
https://hype4.academy/profile/bl555estate
https://reactormag.com/members/bl555estate/
https://www.emailsherlock.com/hosts/bl555.estate/
https://www.promoteproject.com/user/bl555estate/
https://ikanakama.ink/users/339703
https://www.prosebox.net/book/102260/
https://ticketme.io/account/bl555estate
https://task.tw/users/TGPHYWK/freelancer
https://www.aipictors.com/users/bl555estate
https://redirect.camfrog.com/redirect/?url=https://bl555.estate/
https://forum.honorboundgame.com/user-504290.html
https://www.fw-follow.com/forum/topic/94211/bl555estate
https://www.jk-green.com/forum/topic/90273/bl555estate
https://www.navacool.com/forum/topic/327222/bl555estate
https://www.driedsquidathome.com/forum/topic/116861/bl555estate
https://www.nongkhaempolice.com/forum/topic/91589/bl555estate
https://www.bestloveweddingstudio.com/forum/topic/64377/bl555estate
https://www.natthadon-sanengineering.com/forum/topic/81265/bl555estate
https://www.rueanmaihom.net/forum/topic/79978/bl555estate
https://www.ttlxshipping.com/forum/topic/327224/bl555estate
http://worldchampmambo.com/UserProfile/tabid/42/userId/478260/Default.aspx
http://forum.modulebazaar.com/forums/user/bl555estate/
https://gratisafhalen.be/author/bl555estate/
https://user.linkdata.org/user/bl555estate/work
https://www.rcmx.net/userinfo.php?uid=14221
https://eilo.org/user/bl555estate
https://forum.web-z.net/profile.php?userid=9043
https://lqdoj.edu.vn/user/bl555estate
http://pastport.jp/user/bl555estate
https://paperjale.eus/user/bl555estate
https://indiestorygeek.com/user/bl555estate
https://www.bandlab.com/bl555estate
https://forum.issabel.org/u/bl555estate
https://ie.enrollbusiness.com/BusinessProfile/7737667/bl555estate
https://www.keepandshare.com/discuss4/36943/bl555estate
https://giaoan.violet.vn/user/show/id/15244227
https://anh135689999.violet.vn/user/show/id/15244227
https://www.backabuddy.co.za/campaign/bl555estate
https://www.easyhits4u.com/profile.cgi?login=bl555estate&view_as=1
https://doc.anagora.org/s/Xwx39f2Kl
https://profile.sampo.ru/bl555estate
https://baigiang.violet.vn/user/show/id/15244227
https://www.ekdarun.com/forum/topic/136415/bl555estate
https://fanclove.jp/profile/AyJmoYr4B1
https://truckymods.io/user/465471
https://fungiversum.de/pilz-forum/profile/bl555estate/
https://www.d-ushop.com/forum/topic/102899/bl555estate
https://lustyweb.live/members/bl555estate.110390/#about
https://findaspring.org/members/bl555estate/
https://propeller.hu/tagok/bl555estate/adatlap
https://ketcau.com/member/122941-bl555estate/visitormessage/311407-visitor-message-from-bl555estate#post311407
https://vietcurrency.vn/members/bl555estate.234877/#about
https://fengshuidirectory.com/dashboard/listings/bl555estate/
https://library.zortrax.com/members/bl555estate/
https://pets4friends.com/profile-1539974
https://theexplorers.com/user?id=f0a64340-c2b8-4f10-a9fe-86e86226dc6c
https://community.cgboost.com/u/51e43254
https://participa.aytojaen.es/profiles/bl555estate/activity
https://ioninja.com/forum/user/bl555estate
https://linkmix.co/51668507
https://pixelfed.uno/bl555estate
https://janitorai.com/profiles/354b40ab-3518-4250-b68b-96688d846b6f_profile-of-bl-555-estate
https://muckrack.com/nha-cai-bl555-8/bio
https://events.opensuse.org/users/702158
http://linoit.com/users/bl555estate/canvases/bl555estate
https://nortabs.net/user/13699/
https://www.myconcertarchive.com/en/user_home?id=127500
https://ferrariformula1.hu/community/profile/bl555estate/
https://giloo.ist/member/bl555estate/?mainTab=notes&subTab=my_notes
https://defence.pk/members/bl555estate.233426/#about
https://forum.jatekok.hu/User-bl555estate
https://www.buymusic.club/user/bl555estate
https://forum.freero.org/space-uid-23936.html
https://oraclenana.com/MYBB3/user-41482.html
https://www.notariosyregistradores.com/web/forums/usuario/bl555estate/
http://genina.com/user/editDone/5210386.page
https://wikifab.org/wiki/Utilisateur:Bl555estate
https://www.mysportsgo.com/Blog/68325/bl555estate
https://pad.lescommuns.org/s/muU8O6H6V
https://rant.li/bl555estate/nha-cai-bl555
https://chanylib.ru/ru/forum/user/19729/
https://producerbox.com/users/bl555estate
https://skrolli.fi/keskustelu/users/ishaqdanlamiabubakar/
https://www.thehockeypaper.co.uk/forums/users/bl555estate
https://www.rankone.global/bl555estate
https://channillo.com/user/59640/
https://www.11plus.co.uk/users/ishaqdanlamiabubakar/
https://git.entryrise.com/bl555estate
https://opaseke.com/users/14328
https://app.getfarmish.com/profile/8b2644b2-5a7b-41ef-8060-c1da88080114
https://imaginaria.ru/profile/bl555estate/
https://artconomy.com/profile/bl555estate/about/
https://galgame.dev/user/bl555estate
https://nicheless.blog/author/bl555estate
https://www.newgenstravel.com/forum/topic/29895/bl555estate
https://zbrushcentral.jp/user/bl555estate
https://forum.rexygen.com/user/bl555estate
https://www.mapleprimes.com/users/bl555estate
https://muabanhaiduong.com/members/bl555estate.81322/#about
https://noti.st/bl555estate/bio
https://www.adpost.com/u/bl555estate/
https://cannabis.net/user/212016
https://sketchersunited.org/users/308077
https://scrapbox.io/bl555estate/Bl555
https://circle-book.com/circles/24530
http://forum.446.s1.nabble.com/bl555estate-td176113.html
https://forum.opnsense.org/index.php?action=profile;u=65632
https://qiita.com/bl555estate
https://www.ozbargain.com.au/user/603604
https://forum.norbrygg.no/members/bl555estate.147248/#about
https://bbs.mychat.to/user.php?uid=1226216
https://dev.to/bl555estate
https://www.annuncigratuititalia.it/author/bl555estate/
https://www.thethingsnetwork.org/u/bl555estate/
https://nonon-centsnanna.com/members/bl555estate/
https://lite.link/bl555estate
http://www.brenkoweb.com/user/79568/profile
https://hedgedoc.faimaison.net/s/gl59YV_ps8
http://artutor.teiemt.gr/el/user/bl555estate/
https://www.rossoneriblog.com/author/bl555estate/
https://imoodle.win/wiki/User:Bl555estate
https://video.fc2.com/account/14501205
https://www.elitepvpers.com/forum/members/9026488-bl555estate.html
https://nogu.org.uk/forum/profile/bl555estate/
Your comment is awaiting moderation.
https://www.facebook.com/sc88lccom2/
https://www.youtube.com/@sc88lccom
https://twitter.com/sc88lccom
https://tooter.in/sc88lccom
https://wakelet.com/@sc88lccom
https://safechat.com/u/sc88lccom
https://www.blogger.com/profile/06003008451965084078
https://www.mymeetbook.com/sc88lccom
https://www.pinterest.com/sc88lccom/_profile/
https://community.wongcw.com/sc88lccom
https://demo.wowonder.com/sc88lccom
https://shareyoursocial.com/sc88lccom
https://gitlab.aicrowd.com/sc88lccom
https://myspace.com/sc88lccom
https://500px.com/p/sc88lccom
https://www.instapaper.com/p/sc88lccom
https://magic.ly/sc88lccom
https://www.band.us/@sc88lccom
https://protocol.ooo/ja/users/sc88lccom
https://sketchfab.com/sc88lccom
https://www.tumblr.com/sc88lccom
https://www.reddit.com/user/sc88lccom/
https://audiomack.com/sc88lccom
https://hackaday.io/sc88lccom
https://vocal.media/authors/sc88lccom
https://leetcode.com/u/sc88lccom/
https://swag.live/en/user/69984bbdb86d5da7917d75bc
https://www.halaltrip.com/user/profile/319604/sc88lccom/
https://www.jetphotos.com/photographer/780736
https://medibang.com/author/27822935/
https://liulo.fm/sc88lccom
https://opensea.io/sc88lccom
https://www.blockdit.com/sc88lccom
https://portfolium.com/sc88lccom
https://groups.google.com/g/sc88lccom/c/ovF1nOXbmTs
https://www.twitch.tv/sc88lccom/about
https://profile.hatena.ne.jp/sc88lccom/
https://issuu.com/sc88lccom
https://www.behance.net/sc88lccom
https://gravatar.com/sc88lccom
https://www.reverbnation.com/sc88lccom
https://www.myminifactory.com/users/sc88lccom
https://www.investagrams.com/Profile/sc88lccom
https://gifyu.com/sc88lccom
https://www.chordie.com/forum/profile.php?id=2471687
https://skitterphoto.com/photographers/2343574/sc88lccom
https://www.walkscore.com/people/330465899173/sc88lccom
https://topsitenet.com/profile/sc88lccom/1550666/
https://akniga.org/profile/1393801-sc88lccom/
https://sc88lccom.bandcamp.com/album/sc88lccom
https://disqus.com/by/sc88lccom/about/
https://jobs.suncommunitynews.com/profiles/7923729-nha-cai-sc88
https://www.speedrun.com/users/sc88lccom
https://www.fanart-central.net/user/sc88lccom/profile
https://slides.com/sc88lccom
https://www.aicrowd.com/participants/sc88lccom
https://old.bitchute.com/sc88lccom/
https://pbase.com/sc88lccom
https://hub.docker.com/u/sc88lccom
https://spiderum.com/nguoi-dung/sc88lccom
https://zaidap.com/thong-tin-ca-nhan-u106036.htm
https://www.gta5-mods.com/users/sc88lccom
https://heylink.me/sc88lccom/
https://pixabay.com/users/54735262/
https://www.nicovideo.jp/user/143330136
https://www.jigsawplanet.com/sc88lccom
https://3dwarehouse.sketchup.com/by/sc88lccom
https://robertsspaceindustries.com/en/citizens/sc88lccom
https://bit.ly/m/sc88lccom
https://joy.link/sc88lccom
https://connect.garmin.com/app/profile/2c7e7462-669b-4e2f-b1d2-214215ca0303
https://b.hatena.ne.jp/sc88lccom/bookmark
https://www.chichi-pui.com/users/sc88lccom/
https://www.openrec.tv/user/sc88lccom/about
https://unityroom.com/users/sc88lccom
https://pxhere.com/en/photographer-me/4924758
https://teletype.in/@sc88lccom
https://www.checkli.com/sc88lccom
https://www.fuelly.com/driver/sc88lccom
https://www.nintendo-master.com/profil/sc88lccom
https://freeimage.host/sc88lccom
https://www.diigo.com/user/sc88lccom
https://fontstruct.com/fontstructions/show/2830494/sc88lccom
https://mecabricks.com/en/user/sclccom
https://motion-gallery.net/users/915119
https://linkin.bio/sc88lccom/
https://www.logic-sunrise.com/forums/user/189791-sc88lccom/
https://biomolecula.ru/authors/126256
https://talk.plesk.com/members/sclccom.489174/#about
https://www.callupcontact.com/b/businessprofile/sc88lccom/9980498
https://blender.community/sc88lccom/
https://doselect.com/@a854b7d41ff65123f08000d29
https://sciter.com/forums/users/sc88lccom/
https://matkafasi.com/user/sc88lccom
https://allmyfaves.com/sc88lccom
https://www.notebook.ai/users/1285278
https://www.abclinuxu.cz/lide/sc88lccom
https://muare.vn/shop/nha-cai-sc88-89/894923
https://doodleordie.com/profile/sc88lccom
https://web.ggather.com/sc88lccom
https://musikersuche.musicstore.de/profil/sc88lccom/
https://www.intensedebate.com/people/sc88lccom1
https://lookingforclan.com/user/sc88lccom
https://forum.dmec.vn/index.php?members/sc88lccom.175372/
https://igli.me/sc88lccom
https://www.fantasyplanet.cz/diskuzni-fora/users/sc88lccom/
https://freestyler.ws/user/631353/sc88lccom
http://delphi.larsbo.org/user/sc88lccom
https://www.aseeralkotb.com/en/profiles/sc88lccom
https://timdaily.vn/members/sc88lccom.128268/#about
https://app.readthedocs.org/profiles/sc88lccom/
https://www.dibiz.com/mansurisandeep751
https://iszene.com/user-336391.html
https://www.theyeshivaworld.com/coffeeroom/users/sc88lccom
https://desksnear.me/users/sc88lccom
https://www.itchyforum.com/en/member.php?379545-sc88lccom
https://www.roton.com/forums/users/mansurisandeep751/
https://able2know.org/user/sc88lccom/
http://www.biblesupport.com/user/810604-sc88lccom/
https://golosknig.com/profile/sc88lccom/
https://www.anibookmark.com/user/sc88lccom.html
https://www.inventoridigiochi.it/membri/sc88lccom/profile/
https://forum.m5stack.com/user/sc88lccom/
https://wallhaven.cc/user/sc88lccom
https://imageevent.com/sc88lccom
https://www.bitchute.com/sc88lccom
https://bandori.party/user/484925/sc88lccom/
https://community.m5stack.com/user/sc88lccom
https://schoolido.lu/user/sc88lccom/
https://awan.pro/forum/user/138785/
https://jakle.sakura.ne.jp/pukiwiki/?sc88lccom
https://fortunetelleroracle.com/profile/sc88lccom
https://fabble.cc/sc88lccom
https://pad.geolab.space/s/KEiqMowJxe
https://affariat.com/user/profile/173199
https://community.cisco.com/t5/user/viewprofilepage/user-id/1975709
https://pad.stuve.de/s/xNnDNP0oO
https://kr.pinterest.com/sc88lccom/
https://pt.gravatar.com/sc88lccom
https://th.gravatar.com/sc88lccom
https://www.sythe.org/members/sc88lccom.2013383/
https://f319.com/members/sc88lccom.1069383/
https://about.me/sc88lccom
https://booklog.jp/users/sc88lccom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/sc88lccom.1342270/#about
https://www.equinenow.com/farm/sc88lccom.htm
https://www.gaiaonline.com/profiles/sc88lccom/50648226/
https://wefunder.com/sc88lccom
https://potofu.me/sc88lccom
https://transfur.com/Users/sc88lccom
https://xtremepape.rs/members/sc88lccom.645152/#about
https://github.com/sc88lccom
https://myanimelist.net/profile/sc88lccom
https://qna.habr.com/user/sc88lccom
https://website.informer.com/sc88-lc.com
https://lightroom.adobe.com/u/sc88lccom?
https://beacons.ai/sc88lccom
https://en.islcollective.com/portfolio/12851475
https://www.xosothantai.com/members/sc88lccom.598617/
https://velog.io/@sc88lccom/about
https://violet.vn/user/show/id/15238955
https://iplogger.com/2svTC4
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3902832
https://mez.ink/sc88lccom
https://sc88lccom.stck.me/profile
https://notionpress.com/author/1475554
https://www.edna.cz/uzivatele/sc88lccom/
https://digiphoto.techbang.com/users/sc88lccom
https://leakedmodels.com/forum/members/sc88lccom.691729/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1045665
https://freeicons.io/profile/897569
https://onlinesequencer.net/forum/user-252442.html
https://inkbunny.net/sc88lccom
https://www.japaaan.com/user/63074/
https://spinninrecords.com/profile/sc88lccom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.sc886
https://code.antopie.org/sc88lccom
https://beatsaver.com/playlists/1144314
https://apptuts.bio/sc88lccom-248314
https://dialog.eslov.se/profiles/sc88lccom/activity
https://www.storenvy.com/sc88lccom
https://sc88lccom.mssg.me/
https://participacion.cabildofuer.es/profiles/sc88lccom/activity
https://forums.maxperformanceinc.com/forums/member.php?u=239559
https://egl.circlly.com/users/sc88lccom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290322
https://www.sciencebee.com.bd/qna/user/sc88lccom
https://acomics.ru/-sc88lccom
https://www.criminalelement.com/members/sc88lccom/profile/
https://hanson.net/users/sc88lccom
https://writexo.com/share/8b4103209b5d
https://expatguidekorea.com/profile/sc88lccom
https://www.laundrynation.com/community/profile/sc88lccom/
https://www.heavyironjobs.com/profiles/7929944-nha-cai-sc88
https://pad.degrowth.net/s/eKO1zxHnu
https://www.syncdocs.com/forums/profile/sc88lccom
https://www.rehashclothes.com/sc88lccom
http://fort-raevskiy.ru/community/profile/sc88lccom/
https://forum.skullgirlsmobile.com/members/sc88lccom.196489/
https://jobs.landscapeindustrycareers.org/profiles/7930054-nha-cai-sc88
https://phatwalletforums.com/user/sc88lccom
https://forums.galciv4.com/user/7639013
https://kyourc.com/sc88lccom
https://song.link/sc88lccom
https://idol.st/user/135608/sc88lccom/
https://www.valinor.com.br/forum/usuario/sc88lccom.141442/#about
https://tulieu.violet.vn/user/show/id/15238955
https://www.bmwpower.lv/user.php?u=sc88lccom
https://gockhuat.net/member.php?u=431125
https://jobs.windomnews.com/profiles/7930143-nha-cai-sc88
https://hoaxbuster.com/redacteur/sc88lccom
https://www.givey.com/sc88lccom
https://forums.stardock.com/user/7639013
https://zerosuicidetraining.edc.org/user/profile.php?id=540576
https://www.telix.pl/forums/users/Nha-cai-SC883/
https://girlfriendvideos.com/members/s/sc88lccom/
https://swaay.com/u/mansurisandeep751/about/
https://beteiligung.amt-huettener-berge.de/profile/sc88lccom/
https://joinentre.com/profile/sc88lccom
https://jobs.westerncity.com/profiles/7930620-nha-cai-sc88
https://www.thetriumphforum.com/members/sc88lccom.56573/
https://gamblingtherapy.org/forum/users/sc88lccom/
https://mycableengineering.com/activity-feed/userId/29350
https://l2top.co/forum/members/sc88lccom.156914/
http://www.askmap.net/location/7737404/vietnam/sc88lccom
https://youtopiaproject.com/author/sc88lccom
https://graphcommons.com/graphs/1e282a28-79bf-439a-a031-17f4d23129e3
https://forums.galciv3.com/user/7639013
https://galleria.emotionflow.com/175166/profile.html
https://www.myget.org/users/sc88lccom
https://www.deafvideo.tv/vlogger/sc88lccom
https://www.chaloke.com/forums/users/sc88lccom/
https://app.brancher.ai/user/DmTYWekGXe9y
https://aetherlink.app/users/7431767884340428800
https://forums.sinsofasolarempire2.com/user/7639013
https://www.empregosaude.pt/en/author/sc88lccom/
https://confengine.com/user/sc88lccom
https://slideslive.com/sc88lccom?tab=about
https://mygamedb.com/profile/sc88lccom
https://buckeyescoop.com/community/members/sc88lccom.57541/#about
https://forums.ashesofthesingularity.com/user/7639013
https://web-tourist.net/members/sc88lccom.48527/
https://forum.aceinna.com/user/sc88lccom
https://toirscript.com/user/sc88lccom
https://forum.pabbly.com/members/sc88lccom.97914/#about
http://forum.cncprovn.com/members/414828-sc88lccom
https://marketplace.trinidadweddings.com/author/sc88lccom/
https://ncnews.co/profile/sc88lccom
https://dreevoo.com/profile_info.php?pid=1170478
https://forum.aigato.vn/user/sc88lccom
https://amaz0ns.com/forums/users/sc88lccom/
https://rapidapi.com/user/sc88lccom
https://www.skool.com/@nha-cai-sctamtam-7707
https://hedge.fachschaft.informatik.uni-kl.de/s/5zwo4lozc
https://learningapps.org/watch?v=p24z43x5c26
https://subscribe.ru/author/32239006
https://postheaven.net/sc88lccom/sc88lccom
https://www.giveawayoftheday.com/forums/profile/1662189
http://onlineboxing.net/jforum/user/editDone/430087.page
https://www.catapulta.me/users/sc88lccom
https://www.invelos.com/UserProfile.aspx?Alias=sc88lccom
https://www.video-bookmark.com/user/sc88lccom/
https://wibki.com/sc88lccom
https://krachelart.com/UserProfile/tabid/43/userId/1334148/Default.aspx
https://gitlab.vuhdo.io/sc88lccom
https://www.11secondclub.com/users/profile/1699695
https://aniworld.to/user/profil/sc88lccom
https://s.id/sc88lccom
https://worldvectorlogo.com/ar/profile/sc88lccom
https://kktix.com/user/8444076
https://www.passes.com/sc88lccom
https://poipiku.com/13226880/
https://uiverse.io/profile/nhacai_7478
https://www.rwaq.org/users/sc88lccom
https://cofacts.tw/user/sc88lccom
https://www.fitday.com/fitness/forums/members/sc88lccom.html
https://www.fundable.com/nha-cai-sc88-23
https://vcook.jp/users/74955
https://www.grepmed.com/sc88lccom
https://classificados.acheiusa.com/profile/bks0c0ZLM0Z1QzlBK2Mrd1loTGRObmozbDlpdEE5dGFvenQ5OG5Fb2hqND0=
https://espritgames.com/members/50148200/
https://cgmood.com/sc88lccom
https://www.haikudeck.com/presentations/sc88lccom
https://www.efunda.com/members/people/show_people.cfm?Usr=sc88lccom
https://paidforarticles.in/author/sc88lccom
https://diit.cz/profil/t4hjng3dks
https://backloggery.com/sc88lccom
https://www.sociomix.com/u/sc88lccom/
https://raovat.nhadat.vn/members/sc88lccom-288983.html
https://www.moshpyt.com/user/sc88lccom
https://www.koi-s.id/member.php?331601-sc88lccom
https://pumpyoursound.com/u/user/1584913
https://que.u.nosv.org/profile?user=sc88lccom
https://hi-fi-forum.net/profile/1121074/index/
https://secondstreet.ru/profile/sc88lccom/
http://scenarch.com/userpages/28829
https://undrtone.com/sc88lccom
https://marshallyin.com/members/sc88lccom/
https://us.enrollbusiness.com/BusinessProfile/7731188/SC88
https://www.atozed.com/forums/user-67820.html
https://gravesales.com/author/sc88lccom/
https://searchengines.bg/members/sc88lccom.23455/#about
https://hukukevi.net/user/sc88lccom
https://belgaumonline.com/profile/sc88lccom/
https://savelist.co/profile/users/sc88lccom
https://usdinstitute.com/forums/users/sc88lccom/
https://www.montessorijobsuk.co.uk/author/sc88lccom/
https://hackerspace.govhack.org/profiles/sc88_35482
https://www.apsense.com/user/sc88lccom
https://draft.blogger.com/profile/06003008451965084078
https://boldomatic.com/view/writer/sc88lccom
https://menwiki.men/wiki/User_talk:Sc88lccom
https://funsilo.date/wiki/User_talk:Sc88lccom
https://the7thcontinent.seriouspoulp.com/en/user/28310/sc88lccom
https://www.themeqx.com/forums/users/sc88lccom/
https://www.udrpsearch.com/user/sc88lccom
https://forums.wincustomize.com/user/7639013
http://newdigital-world.com/members/sc88lccom.html
https://www.xen-factory.com/index.php?members/sc88lccom.140256/#about
https://cointr.ee/sc88lccom
https://king-wifi.win/wiki/User_talk:Sc88lccom
https://forums.servethehome.com/index.php?members/sc88lccom.226395/#about
https://jaga.link/sc88lccom
https://raovatquynhon.com/thiet-bi-dien-tu-4/sc88lccom-15796
https://b.io/sc88lccom
http://www.truck-business.cz/profile/sc88lccom/info.html
https://www.blackhatprotools.info/member.php?276815-sc88lccom
https://activepages.com.au/profile/sc88lccom
https://snippet.host/egjhyd
https://tudomuaban.com/chi-tiet-rao-vat/2827127/sc88lccom.html
https://phijkchu.com/a/sc88lccom/video-channels
https://lifeinsys.com/user/sc88lccom
https://kaeuchi.jp/forums/users/sc88lccom/
https://www.claimajob.com/profiles/7937026-nha-cai-sc88
https://protospielsouth.com/user/117347
https://theafricavoice.com/profile/sc88lccom
http://palangshim.com/space-uid-4978688.html
https://www.africangenesis-101.org/profile/mansurisandeep751455/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:3C2127256998E01D0A495E55@AdobeID
https://vi.gravatar.com/sc88lccom
https://www.vevioz.com/sc88lccom
https://www.mixcloud.com/sc88lccom/
https://www.designspiration.com/sc88lccom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185814
https://hub.vroid.com/en/users/124150365
https://www.exchangle.com/sc88lccom
https://forum.codeigniter.com/member.php?action=profile&uid=223993
https://circleten.org/a/396199?postTypeId=whatsNew
https://bitspower.com/support/user/sc88lccom
https://www.brownbook.net/business/54856079/sc88lccom
https://etextpad.com/vuscn47ttb
https://app.hellothematic.com/creator/profile/1123165
https://www.decidim.barcelona/profiles/sc88lccom/activity
https://www.babelcube.com/user/nha-cai-sc88-24
https://app.talkshoe.com/user/sc88lccom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223456
https://m.wibki.com/sc88lccom
https://www.pageorama.com/?p=sc88lccom
https://bandsworksconcerts.info/index.php?sc88lccom
https://bbs.mikocon.com/home.php?mod=space&uid=281822
https://www.mikocon.com/home.php?mod=space&uid=281822
https://www.quora.com/profile/Nha-Cai-SC88-1
https://manylink.co/@sc88lccom
https://www.freewebspace.net/forums/index.php?members/sc88lccom.17031259/#about
https://forums.giantitp.com/member.php?369114-sc88lccom
https://seomotionz.com/member.php?action=profile&uid=116962
https://anyflip.com/homepage/ccvfs#About
https://www.akaqa.com/question/q19192653454-Sc88lccom
https://londonchinese.com/home.php?mod=space&uid=614806&do=index
https://copynotes.be/shift4me/forum/user-44415.html
https://nl.gravatar.com/sc88lccom
https://nb.gravatar.com/sc88lccom
https://ms.gravatar.com/sc88lccom
https://lt.gravatar.com/sc88lccom
https://kn.gravatar.com/sc88lccom
https://www.newgenstravel.com/forum/topic/28773/sc88lccom
https://scholar.google.com/citations?hl=en&user=pXj6HiUAAAAJ
https://www.threadless.com/@sc88lccom/activity
https://www.smitefire.com/profile/sc88lccom-256724?profilepage
https://tabelog.com/rvwr/033240005/prof/
https://coolors.co/u/sc88lccom
https://www.beamng.com/members/sc88lccom.774003/
https://civitai.com/user/sc88lccom
https://www.spigotmc.org/members/sc88lccom.2485757/
https://boosty.to/sc88lccom
https://id.gta5-mods.com/users/sc88lccom
https://ms.gta5-mods.com/users/sc88lccom
https://bg.gta5-mods.com/users/sc88lccom
https://ca.gta5-mods.com/users/sc88lccom
https://cs.gta5-mods.com/users/sc88lccom
https://camp-fire.jp/profile/sc88lccom
https://feyenoord.supporters.nl/profiel/138702/sc88lccom
https://www.pearltrees.com/sc88lccom/item782771798
https://gesoten.com/profile/detail/12588411
https://hashnode.com/@sc88lccom
https://hoo.be/sc88lccom
https://nhattao.com/members/user6922487.6922487/
https://maxforlive.com/profile/user/sc88lccom?tab=about
https://3dtoday.ru/blogs/sc88lccom
https://opencollective.com/nha-cai-sc882
https://pinshape.com/users/8915683-sc88lccom?tab=designs
https://morguefile.com/creative/sc88lccom
https://edabit.com/user/geB2RBDWFxQySidM6
https://mathlog.info/users/kEujs28f3QfF2iYlUaR76erPTNf1
https://securityheaders.com/?q=https://sc88-lc.com/
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165702
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145229
https://md.darmstadt.ccc.de/s/eVxgOZgtW3
https://sfx.thelazy.net/users/u/sc88lccom/
https://forum.reallusion.com/Users/3283551/mansurisandeep751
https://us.pinterest.com/sc88lccom/
https://gl.gta5-mods.com/users/sc88lccom
https://ar.gravatar.com/sc88lccom
https://app.daily.dev/sc88lccom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=247103
https://slidehtml5.com/homepage/anng#About
https://www.skypixel.com/users/djiuser-nm1xo7sgnaem
https://webanketa.com/forms/6mv34chn6gqkad9h71h62r9p/
https://matters.town/@sc88lccom
https://www.pdc.edu/?URL=https://sc88-lc.com/
https://ask.mallaky.com/?qa=user/sc88lccom
https://drill.lovesick.jp/drilldata/index.php?sc88lccom
https://it.pinterest.com/sc88lccom/
https://cz.pinterest.com/sc88lccom/
https://uk.pinterest.com/sc88lccom/
https://www.depechemode.cz/?URL=https://sc88-lc.com/
https://aiti.edu.vn/members/sc88lccom.35270/
https://batdongsan24h.edu.vn/members/sc88lccom.17372/
https://chuanmen.edu.vn/members/sc88lccom.27190/
https://okmen.edu.vn/members/sc88lccom.27026/
http://www.dungdong.com/home.php?mod=space&uid=3255493&do=3323696
https://www.squadskates.com/profile/mansurisandeep75115558/profile
https://forum.herozerogame.com/index.php?/user/152190-sc88lccom/
https://shhhnewcastleswingers.club/forums/users/sc88lccom/
https://mylinks.ai/sc88lccom
https://bbs.mofang.com.tw/home.php?mod=space&uid=2390917
https://stuv.othr.de/pad/s/VzWkKEUHS
https://forum.tkool.jp/index.php?members/sc88lccom.97891/#about
https://es.pinterest.com/sc88lccom/
https://co.pinterest.com/sc88lccom/
https://de.pinterest.com/sc88lccom/
https://hedgedoc.eclair.ec-lyon.fr/s/5VPzJb7Fi
http://densan-knct.freehostia.com/wiki_/index.php?sc88lccom1
https://www.divephotoguide.com/user/sc88lccom
https://www.weddingbee.com/members/sc88lccom/
https://kumu.io/sc88lccom/sc88
https://b.cari.com.my/home.php?mod=space&uid=3383157&do=profile
https://bioimagingcore.be/q2a/user/sc88lccom
https://www.sunlitcentrekenya.co.ke/author/sc88lccom/
https://hedgedoc.logilab.fr/s/YrsHiQ9GU
https://sc88lccom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/sc88lccom/activity
https://lovewiki.faith/wiki/User:Sc88lccom
https://dokuwiki.stream/wiki/User:Sc88lccom
https://hikvisiondb.webcam/wiki/User:Sc88lccom
https://www.rcuniverse.com/forum/members/sc88lccom.html
https://www.huntingnet.com/forum/members/sc88lccom.html
https://www.hogwartsishere.com/1817872/
https://jobs.host-panel.com/author/sc88lccom/
https://vimeo.com/sc88lccom
https://gitlab.com/sc88lccom
https://makeagif.com/user/sc88lccom?ref=hJ9e0Y
https://participez.perigueux.fr/profiles/sc88lccom/activity
https://fr.pinterest.com/sc88lccom/
https://pl.pinterest.com/sc88lccom/
https://ca.pinterest.com/sc88lccom/
https://ixawiki.com/link.php?url=https://sc88-lc.com/
https://imoodle.win/wiki/User:Sc88lccom
https://www.pintradingdb.com/forum/member.php?action=profile&uid=135031
https://www.plotterusati.it/user/sc88lccom
http://www.jbt4.com/home.php?mod=space&uid=8666503
https://www.vid419.com/home.php?mod=space&uid=3475292
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Sc88lccom1
https://www.goodolcomics.com/blog/profile/sc88lccom/
https://hu.pinterest.com/sc88lccom/
https://sk.pinterest.com/sc88lccom/
https://skr.gravatar.com/sc88lccom
https://sk.gravatar.com/sc88lccom
https://ru.gravatar.com/sc88lccom
https://ro.gravatar.com/sc88lccom
https://pl.gravatar.com/sc88lccom
https://md.kokakiwi.net/s/PSqk4Ifbn9
https://md.un-hack-bar.de/s/7bbCqX1MDo
https://br.pinterest.com/sc88lccom/
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=384279
http://techou.jp/index.php?sc88lccom
https://paste.intergen.online/view/299b5602
https://www.managementpedia.com/members/sc88lccom.1116575/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=602738
https://volleypedia.org/index.php?qa=user&qa_1=sc88lccom
http://pcsq28.com/home.php?mod=space&uid=1761906
https://bbs.airav.cc/home.php?mod=space&uid=4416533
https://partecipa.poliste.com/profiles/sc88lccom/activity
https://www.ixawiki.com/link.php?url=https://sc88-lc.com/
https://cl.pinterest.com/sc88lccom/
https://nz.pinterest.com/sc88lccom/
https://mx.pinterest.com/sc88lccom/
https://md.coredump.ch/s/LtdBrpPKY
https://scripts.mit.edu/trac/search?aff-387363&q=https://sc88-lc.com/
https://hker2uk.com/home.php?mod=space&uid=5343610
https://pad.funkwhale.audio/s/MZ22hdEJE
https://forum.dfwmas.org/index.php?members/sc88lccom.194429/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=465836
https://aprenderfotografia.online/usuarios/sc88lccom/profile/
http://tkdlab.com/wiki/index.php?sc88lccom
https://jobs.lajobsportal.org/profiles/7945239
https://uk.gravatar.com/sc88lccom
https://hu.gravatar.com/sc88lccom
https://hedgedoc.stusta.de/s/WlrFOca2s
https://it.gravatar.com/sc88lccom
http://galeria.farvista.net/member.php?action=showprofile&user_id=71271
https://tilengine.org/forum/member.php?action=profile&uid=158337
https://darkml.net/bbs/home.php?mod=space&uid=8193243&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6010634
https://hedgedoc.stusta.de/s/OhF_k2Ja4
https://pad.flipdot.org/s/7dEY2I87n
https://hack.allmende.io/s/wkWPk2iGq
https://pad.codefor.fr/s/LTffnuxm1D
https://md.opensourceecology.de/s/sLmnr5pPA
https://md.ctdo.de/s/2FodAwLTH5
https://md.chaospott.de/s/nqTpdvDHqZ
https://pad.fablab-siegen.de/s/nDH4AN5EF
https://hackmd.hub.yt/s/hXnuogGuj
https://md.swk-web.com/s/gntGxeDfY
https://hedgedoc.dezentrale.space/s/2XsnqBqjj
https://docs.juze-cr.de/s/uS2poqbWB
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301314
https://replit.com/@sc88lccom
https://divisionmidway.org/jobs/author/sc88lccom/
https://wandb.ai/profile/sc88lccom
https://pad.darmstadt.social/s/EZLhVSbT0c
https://ie.pinterest.com/sc88lccom/
https://ru.pinterest.com/sc88lccom/
https://bbcovenant.guildlaunch.com/users/blog/6738127/?mode=view&gid=97523
https://www.youbiz.com/profile/
https://cameradb.review/wiki/User:Sc88lccom
https://www.wowonder.xyz/sc88lccom
https://sciencemission.com/profile/sc88lccom
https://referrallist.com/profile/sc88lccom/
https://fakenews.win/wiki/User:Sc88lccom
http://jobboard.piasd.org/author/sc88lccom/
https://www.wvhired.com/profiles/7945339-nha-cai-sc88
http://www.webclap.com/php/jump.php?url=https://sc88-lc.com/
https://kenhrao.com/members/sc88lccom.115547/#about
https://hackmd.openmole.org/s/RkE5AQApX
https://forumketoan.com/members/sc88lccom.41656/#about
https://v.gd/Sajdp4
https://sciencewiki.science/wiki/User:Sc88lccom
https://www.fruitpickingjobs.com.au/forums/users/sc88lccom/
https://zenwriting.net/sc88lccom/sc88
https://writeablog.net/sc88lccom/sc88
https://blogfreely.net/sc88lccom/sc88
https://ur.gravatar.com/sc88lccom
https://tr.gravatar.com/sc88lccom
https://sr.gravatar.com/sc88lccom
https://sq.gravatar.com/sc88lccom
https://sl.gravatar.com/sc88lccom
https://bwinglive.lighthouseapp.com/users/1993059
https://rush1989.rash.jp/pukiwiki/index.php?sc88lccom
https://wikimapia.org/external_link?url=https://sc88-lc.com/
https://campsite.bio/sc88lccom
https://www.hobowars.com/game/linker.php?url=https://sc88-lc.com/
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://sc88-lc.com/
https://redirect.camfrog.com/redirect/?url=https://sc88-lc.com/
http://forum.orangepi.org/home.php?mod=space&uid=6252503
https://beteiligung.hafencity.com/profile/sc88lccom/
https://adhocracy.plus/profile/sc88lccom/
https://beteiligung.stadtlindau.de/profile/sc88lccom/
https://forum.honorboundgame.com/user-503786.html
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=458082&sid=b3d2a4af7c072193b2243ecaa4f99d58
https://www.fw-follow.com/forum/topic/91971/sc88lccom
https://www.jk-green.com/forum/topic/88315/sc88lccom
https://www.navacool.com/forum/topic/319863/sc88lccom
https://www.bonback.com/forum/topic/319862/sc88lccom
https://www.driedsquidathome.com/forum/topic/114162/sc88lccom
https://www.nongkhaempolice.com/forum/topic/88337/sc88lccom
https://www.bestloveweddingstudio.com/forum/topic/62224/sc88lccom
https://www.natthadon-sanengineering.com/forum/topic/78856/sc88lccom
https://www.rueanmaihom.net/forum/topic/78198/sc88lccom
https://www.ttlxshipping.com/forum/topic/319860/sc88lccom
https://www.cemkrete.com/forum/topic/134659/sc88lccom
http://forum.modulebazaar.com/forums/user/sc88lccom/
https://da.gta5-mods.com/users/sc88lccom
https://el.gta5-mods.com/users/sc88lccom
https://es.gta5-mods.com/users/sc88lccom
https://fr.gta5-mods.com/users/sc88lccom
https://ko.gta5-mods.com/users/sc88lccom
https://videos.muvizu.com/Profile/sc88lccom/Latest/
https://dev.muvizu.com/Profile/sc88lccom/Latest
https://cdn.muvizu.com/Profile/sc88lccom/Latest
https://www.muvizu.com/Profile/sc88lccom/Latest
https://mozillabd.science/wiki/User:Sc88lccom
https://raredirectory.com/?p=22669
https://en.wikivet.net/User_talk:Sc88lccom
https://decidim.calafell.cat/profiles/sc88lccom/activity
http://bbs.medicalforum.cn/home.php?mod=space&uid=2087003
https://mforum.cari.com.my/home.php?mod=space&uid=3383157&do=profile
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://sc88-lc.com/
https://giaoan.violet.vn/user/show/id/15238955
https://anh135689999.violet.vn/user/show/id/15238955
https://hu.gta5-mods.com/users/sc88lccom
https://uk.gta5-mods.com/users/sc88lccom
https://sl.gta5-mods.com/users/sc88lccom
https://at.pinterest.com/sc88lccom/
https://in.pinterest.com/sc88lccom/
https://forums.starcontrol.com/user/7639013
https://baigiang.violet.vn/user/show/id/15238955
https://es.gravatar.com/sc88lccom
https://de.gravatar.com/sc88lccom
https://cy.gravatar.com/sc88lccom
https://cs.gravatar.com/sc88lccom
https://cn.gravatar.com/sc88lccom
https://forums.offworldgame.com/user/7639013
https://www.ekdarun.com/forum/topic/134820/sc88lccom
https://fic.decidim.barcelona/profiles/sc88lccom/activity
https://doc.anagora.org/s/0nZwIjHjA
https://album.link/sc88lccom
https://artist.link/sc88lccom
https://pods.link/sc88lccom
https://playlist.link/sc88lccom
https://odesli.co/sc88lccom
https://mylink.page/sc88lccom
https://forum.pokexgames.pl/member.php?action=profile&uid=75608
https://line-monsterfarm.wiki/?sc88lccom
https://wiki.armello.com/index.php/User:Sclccomm
https://www.ekdarun.com/forum/topic/134862/sc88lccom
https://www.driedsquidathome.com/forum/topic/114252/sc88lccom
https://www.cemkrete.com/forum/topic/134747/sc88lccom
https://www.navacool.com/forum/topic/320073/sc88lccom
https://www.natthadon-sanengineering.com/forum/topic/78928/sc88lccom
https://ka.gravatar.com/sc88lccom
https://ga.gravatar.com/sc88lccom
https://fr-ca.gravatar.com/sc88lccom
https://el.gravatar.com/sc88lccom
https://da.gravatar.com/sc88lccom
https://wikifab.org/wiki/Utilisateur:Sc88lccom
https://www.bonback.com/forum/topic/320074/sc88lccom
https://www.d-ushop.com/forum/topic/100045/sc88lccom
https://forums.stardock.net/user/7639013
https://forums.sinsofasolarempire.com/user/7639013
https://www.dideadesign.com/forum/topic/26172/sc88lccom
https://www.lwn3d.com/forum/topic/56780/sc88lccom
https://www.simplexthailand.com/forum/topic/11807/sc88lccom
https://www.hyperlabthailand.com/forum/topic/790851/sc88lccom
https://www.thitrungruangclinic.com/forum/topic/88423/sc88lccom
https://login.ezproxy.lib.lehigh.edu/login?url=https://sc88-lc.com/
http://forum.vodobox.com/profile.php?id=63732
https://kttm.club/members/sc88lccom.4349/#about
https://www.techrum.vn/members/sc88lccom.264741/#about
https://ezproxy.cityu.edu.hk/login?url=https://sc88-lc.com/
https://vietcurrency.vn/members/sc88lccom.234431/#about
https://dienbd.violet.vn/user/show/id/15238955
https://zh-tw.gravatar.com/sc88lccom
https://sv.gravatar.com/sc88lccom
https://po.gravatar.com/sc88lccom
https://oc.gravatar.com/sc88lccom
https://ko.gravatar.com/sc88lccom
https://vnbit.org/members/sc88lccom.84065/#about
https://pandora.nla.gov.au/external.html?link=https://sc88-lc.com/
https://barcelonadema-participa.cat/profiles/sc88lccom/activity
https://pad.stuve.de/s/zInJes15X
https://pad.libreon.fr/s/WaUCgzySx
https://gl.gravatar.com/sc88lccom
https://fr.gravatar.com/sc88lccom
https://fi.gravatar.com/sc88lccom
https://fa.gravatar.com/sc88lccom
http://forum.bokser.org/user-1433913.html
https://gratisafhalen.be/author/sc88lccom/
https://beteiligung.tengen.de/profile/sc88lccom/
https://calaos.fr/forum/member.php?action=profile&uid=18641
https://www.pathumratjotun.com/forum/topic/141568/sc88lccom
https://forum.web-z.net/profile.php?userid=8994
https://pets4friends.com/profile-1535038
https://oye.participer.lyon.fr/profiles/sc88lccom/activity
https://participa.favb.cat/profiles/sc88lccom/activity
https://construim.fedaia.org/profiles/sc88lccom/activity
https://meta.decidim.org/profiles/sc88lccom/activity
https://hi.gta5-mods.com/users/sc88lccom
https://it.gta5-mods.com/users/sc88lccom
https://nl.gta5-mods.com/users/sc88lccom
https://no.gta5-mods.com/users/sc88lccom
https://pl.gta5-mods.com/users/sc88lccom
https://pt.gta5-mods.com/users/sc88lccom
https://med.jax.ufl.edu/webmaster/?url=https://sc88-lc.com/
https://decidim.derechoaljuego.digital/profiles/sc88lccom/activity
https://ro.gta5-mods.com/users/sc88lccom
https://ru.gta5-mods.com/users/sc88lccom
https://fi.gta5-mods.com/users/sc88lccom
https://sv.gta5-mods.com/users/sc88lccom
https://vi.gta5-mods.com/users/sc88lccom
https://zh.gta5-mods.com/users/sc88lccom
https://theexplorers.com/user?id=5fbc5be3-8329-4a3b-ae77-50ec53704bde
https://md.rappet.xyz/s/9v-m6E5Fzf
https://participa.aytojaen.es/profiles/sc88lccom/activity
https://www.northwestu.edu/?URL=https://sc88-lc.com/
https://km.gravatar.com/sc88lccom
https://ja.gravatar.com/sc88lccom
https://id.gravatar.com/sc88lccom
https://he.gravatar.com/sc88lccom
https://jump.5ch.net/?https://sc88-lc.com/
https://www.pubpub.org/user/nha-cai-sc88-27
https://www.depechemode.cz/?URL=https://sc88-lc.com/
https://jp.pinterest.com/sc88lccom/
https://de.gta5-mods.com/users/sc88lccom
https://mk.gta5-mods.com/users/sc88lccom
https://tr.gta5-mods.com/users/sc88lccom
https://bs.gravatar.com/sc88lccom
https://ca.gravatar.com/sc88lccom
https://br.gravatar.com/sc88lccom
https://bn.gravatar.com/sc88lccom
https://bg.gravatar.com/sc88lccom
https://az.gravatar.com/sc88lccom
https://dialogluzern.ch/profiles/sc88lccom/activity
https://decidim.santcugat.cat/profiles/sc88lccom/activity
https://jobs.siliconflorist.com/employers/4037387-sc88
https://jobs.nefeshinternational.org/employers/4037388-sc88
https://aboutcasemanagerjobs.com/author/sc88lccom/
https://biashara.co.ke/author/sc88lccom/
https://buyandsellhair.com/author/sc88lccom/
https://cornucopia.se/author/sc88lccom/
https://lustyweb.live/members/sc88lccom.109552/#about
https://rant.li/sc88lccom/sc88
https://sites.google.com/view/sc88lccom/home
https://telegra.ph/SC88-02-27
https://zenwriting.net/sc88lccom/sc88
https://sc88lccom.blogspot.com/2026/02/sc88.html
https://writeablog.net/sc88lccom/sc88
https://blogfreely.net/sc88lccom/sc88
https://sc88lccom.wordpress.com/
https://scrapbox.io/sc88lccom/SC88
https://zb3.org/sc88lccom/sc88
https://xtiles.app/69a1078ad9701e627edb4253
https://telescope.ac/sc88lccom/og7xb40beieqxq2i0eqb1o
https://sc88lccom.amebaownd.com/posts/58586577
https://sc88lccom.therestaurant.jp/posts/58586583
https://sc88lccom.shopinfo.jp/posts/58586587
https://sc88lccom.theblog.me/posts/58586589
https://sc88lccom.themedia.jp/posts/58586595
https://sc88lccom.localinfo.jp/posts/58586606
https://www.myaspenridge.com/members/profile/3645312/sc88lccom.htm
https://www.tai-ji.net/members/profile/3645313/sc88lccom.htm
https://www.greencarpetcleaningprescott.com/members/profile/3645314/sc88lccom.htm
https://www.thepetservicesweb.com/members/profile/3645318/sc88lccom.htm
https://www.milliescentedrocks.com/members/profile/3645317/sc88lccom.htm
https://www.sunemall.com/members/profile/3645322/sc88lccom.htm
https://www.freedomteamapexmarketinggroup.com/members/profile/3645323/sc88lccom.htm
https://www.bestloveweddingstudio.com/forum/topic/62271/sc88lccom
Ahaa, its nice dialogue on the topic of this piece of writing at this place
at this website, I have read all that, so at this time me also commenting here. https://app.ontelly.com/read-blog/18863_eroticheskij-massazh-murmansk.html
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex izle,sikiş videoları,sikiş
izle,seks izle,seks videoları,porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno izle,sarhoş pornosu,enses porno,ücretsiz
porno,ücretsiz porno izle,porna izle,Porno Anne,
Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş
izle,abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,
içine boşalma porno,porno porno,porn porn,milli
porno,Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet
Sunay porno,Fahri Korutürk porno,Kenan Evren porno,Turgut Özal
porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes
porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet
Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,
Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif Şener porno,
Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi
Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem sex kaseti,
Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal Güzel sex
kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek ifşa,Recep
Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz
Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat
Kurum Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno
ifşa,Ömer Bolat Porno ifşa,İbrahim Yumaklı
Porno ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak
Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim
Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,
Fahrettin Altun Porno ifşa,Numan Kurtulmuş Porno ifşa,Özgür
Özel Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno ifşa,
Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno
ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno
ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer
Kerkez Porno ifşa,Zeki Yiğit Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih
Karahan Porno ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay
Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno
ifşa,Muhittin Böcek Porno ifşa,Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno
ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra
Kadıgil Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım
Porno ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit
Gül Porno ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet
Ali Şahin Porno ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno
ifşa,Derya Yanık Porno ifşa,Mustafa Şentop Porno ifşa,İsmail
Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno
ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner
Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek
Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit
Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno
ifşa,Koç Ailesi Porno ifşa,Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,
Esas Holding Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı
ve Ailesi Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding Porno ifşa,
Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno
ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno
ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno
ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu
Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı
Holding Porno ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno
ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno ifşa,
Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi Porno ifşa,Yıldırım
Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno
ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko
Holding Porno ifşa,Sevda-Serra Sabancı Porno ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,Mehmet Cengiz Porno ifşa,Cengiz Holding Porno
ifşa,Cemal Kalyoncu Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno
ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi
Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno ifşa,Torunlar Grubu Porno
ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas
Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı
Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi
Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,
Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno
ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno
ifşa,Garih Ailesi Porno ifşa,Bayraktar Ailesi Porno ifşa,
Baykar Porno ifşa,Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,
Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı
Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno
ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno
ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer Kurşun Porno
ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno ifşa,Lodrik Ailesi Porno ifşa,
Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno
ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding Porno
ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno
ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök
Porno ifşa,Atlantik Holding Porno ifşa,Nilüfer Dinçkök Çiftçi Porno ifşa,
Yalçın Sabancı Porno ifşa,Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar
Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar
Zülfikari Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal
Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk
Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,
Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,Kiler Holding Porno
ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi
Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,
Astor Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil
Porno ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,
Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex izle,sikiş videoları,sikiş izle,seks izle,seks videoları,
porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno
izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,
Porno Anne,Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,abla porno,abi porno,akraba
porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,
Fahri Korutürk porno,Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes porno,Bülent Ecevit porno,
Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,
Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali Babacan porno,
Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş
sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu
sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal
Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,
Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat
Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil
Çiçek ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet
Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler
Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz Tunç Porno ifşa,Yusuf Tekin Porno
ifşa,Kemal Memişoğlu Porno ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat Kurum
Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat
Porno ifşa,İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno
ifşa,Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş
Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno
ifşa,Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit
Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih Karahan Porno
ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu
Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma
Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,Vahap Seçer Porno ifşa,
Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno
ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer
Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu
Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,
Binali Yıldırım Porno ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,
Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno
ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,
Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno ifşa,Mustafa Şentop Porno ifşa,İsmail
Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,
Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail Küçükkaya Porno
ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,
Mustafa Destici Porno ifşa,Ümit Özdağ Porno ifşa,Muharrem İnce Porno ifşa,
Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi
Porno ifşa,Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,Esas Holding Porno ifşa,Erol
Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno
ifşa,Türkan Sabancı ve Ailesi Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding
Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,
Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs
Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding
Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding
Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu
Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,
Tosyalı Holding Porno ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno
ifşa,Borusan Holding Porno ifşa,Erman Ilıcak
Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi Porno ifşa,Yıldırım
Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno
ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu Porno ifşa,
Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,Sevda-Serra Sabancı Porno
ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,
Ciner Grubu Porno ifşa,Mehmet Cengiz Porno ifşa,Cengiz
Holding Porno ifşa,Cemal Kalyoncu Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno ifşa,Çolakoğlu
Grubu Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat
Özdemir Porno ifşa,Limak İnşaat Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes
Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno
ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno
ifşa,Kurdoğlu Ailesi Porno ifşa,Ata Holding Porno ifşa,
Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno
ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih Ailesi
Porno ifşa,Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,
Yamantürk Ailesi Porno ifşa,Güriş Holding
Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova
Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno ifşa,İçdaş Porno
ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,Demsa Group
Porno ifşa,Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer
Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno
ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker
Ailesi Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı
Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno
ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer
Dinçkök Porno ifşa,Atlantik Holding Porno ifşa,Nilüfer Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,
Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar
Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno
ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent
Ailesi Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,
Gülaylar Grubu Porno ifşa,Pak Ailesi Porno
ifşa,Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,
Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno
ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım
Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,
Avni Çelik Porno ifşa,Sinpaş Holding Porno
ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu
Porno ifşa,Kiler Ailesi Porno ifşa,Kiler Holding
Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu
Ailesi Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno ifşa,Fettah
Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
Inspiring quest there. What happened after? Thanks!
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex izle,sikiş videoları,sikiş izle,seks izle,seks videoları,
porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno
izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna
izle,Porno Anne,Porno izlesene,Sikiş Video,
HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert
sikiş,içine boşalma porno,porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,recep
tayyip erdogan,recep tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal Bayar
porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk
porno,Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah
Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller
porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş
porno,Devlet Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali
Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal
İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif
Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş
sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu
sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex
kaseti,İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex
kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal
Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek
ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno
ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz
Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat Kurum
Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat
Porno ifşa,İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno ifşa,
Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno
ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno
ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel Porno ifşa,Devlet
Bahçeli Porno ifşa,Tülay Hatimoğulları Porno ifşa,Tuncer Bakırhan Porno
ifşa,Müsavat Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno
ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz
Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,Kadir
Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih Karahan Porno ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim
Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,Vahap Seçer Porno
ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,
Cevdet Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno
ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer
Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım Porno ifşa,Süleyman Soylu Porno ifşa,
Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,
Abdülhamit Gül Porno ifşa,Fuat Oktay Porno
ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı Porno ifşa,
Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,
Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati
Porno ifşa,Derya Yanık Porno ifşa,Mustafa Şentop Porno
ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah
Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner
Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit
Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno
ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,
Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,Esas Holding
Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,Sabancı Holding
Porno ifşa,Türkan Sabancı ve Ailesi Porno ifşa,Tara Ailesi
Porno ifşa,Enka Holding Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno
ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,
Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs Holding Porno ifşa,
Doğan Ailesi Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,
Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding
Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı Holding Porno
ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno ifşa,
Borusan Holding Porno ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi
Porno ifşa,Yıldırım Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,
Mehmet Başaran Porno ifşa,Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,Sevda-Serra Sabancı Porno ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,Mehmet
Cengiz Porno ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno
ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno
ifşa,Limak İnşaat Porno ifşa,Sezai Bacaksız
Porno ifşa,Demir Sabancı Porno ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi
Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,
Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,
Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,
Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding
Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu
Porno ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih Ailesi
Porno ifşa,Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,
Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi
Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno ifşa,İçdaş
Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,
Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,
Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno ifşa,Lodrik Ailesi
Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,
Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut
Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi Porno
ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök Porno ifşa,Atlantik
Holding Porno ifşa,Nilüfer Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi
Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk
Holding Porno ifşa,Taşkent Ailesi Porno ifşa,STFA
Porno ifşa,Gülay Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno ifşa,
Kiska Holding Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu
Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat
Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding
Porno ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno
ifşa,Kiler Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno
ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,
Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno
ifşa,Astor Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi
Porno ifşa,Erbakır Porno ifşa
Good day! I could have sworn I’ve been to your blog before but after looking at many of
the articles I realized it’s new to me. Regardless, I’m
definitely happy I stumbled upon it and I’ll be bookmarking it and checking back regularly!
Hello there, just became aware of your blog through Google, and found that it’s truly informative. I’m going to watch out for brussels. I will be grateful if you continue this in future. Lots of people will be benefited from your writing. Cheers!
Hi, I think your site might be having browser compatibility issues. When I look at your website in Safari, it looks fine but when opening in Internet Explorer, it has some overlapping. I just wanted to give you a quick heads up! Other then that, fantastic blog!
porno izle,porno seyret,türk porno,ifşa porno,
türk ünlü porno,sex izle,sikiş videoları,sikiş izle,seks
izle,seks videoları,porno,Porno Film izle,Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü
porno izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,Porno Anne,Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,
abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,porno porno,porn porn,milli porno,
Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep
tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk porno,Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,
Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif
Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,
İsmail Cem sex kaseti,Hikmet Çetin sex
kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,
Hasan Celal Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,
Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,
Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil
Çiçek ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,
Yılmaz Tunç Porno ifşa,Yusuf Tekin Porno ifşa,
Kemal Memişoğlu Porno ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih
Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat Porno ifşa,
İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,
Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno ifşa,Numan Kurtulmuş
Porno ifşa,Özgür Özel Porno ifşa,Devlet Bahçeli Porno
ifşa,Tülay Hatimoğulları Porno ifşa,Tuncer Bakırhan Porno ifşa,Müsavat
Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,
Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno
ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki Yiğit Porno ifşa,Selçuk Bayraktaroğlu
Porno ifşa,Fatih Karahan Porno ifşa,Ali Erbaş
Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,
Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,
Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno
ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer
Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno
ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali
Yıldırım Porno ifşa,Süleyman Soylu Porno ifşa,
Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı
Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,
Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno ifşa,Mustafa Şentop Porno ifşa,İsmail Kahraman Porno ifşa,
Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya
Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit
Özdağ Porno ifşa,Muharrem İnce Porno ifşa,
Selçuk Bayraktar Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,Büşra Özdemir
Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,Koç Holding
Porno ifşa,Şevket Sabancı’nın Ailesi Porno ifşa,
Esas Holding Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı ve Ailesi Porno ifşa,Tara Ailesi
Porno ifşa,Enka Holding Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno
ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs Holding Porno ifşa,Doğan Ailesi Porno
ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu
Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi
Porno ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı
Holding Porno ifşa,Kibar Ailesi Porno ifşa,Kibar Holding Porno
ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno
ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi Porno
ifşa,Yıldırım Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,Mehmet
Başaran Porno ifşa,Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,Sevda-Serra Sabancı
Porno ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,Mehmet
Cengiz Porno ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno
ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,
Çolakoğlu Ailesi Porno ifşa,Çolakoğlu Grubu
Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes Grubu Porno
ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,
Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno
ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,Ata
Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi
İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol
Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem
Grubu Porno ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih Ailesi Porno ifşa,Bayraktar Ailesi
Porno ifşa,Baykar Porno ifşa,Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik
Dizdar Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno
ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,
Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,
Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno
ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,
Orjin Grubu Porno ifşa,Zafer Kurşun Porno ifşa,
İnan Kıraç Porno ifşa,Kıraça Holding Porno ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,
IC Holding Porno ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,
Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding
Porno ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,
Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer
Dinçkök Porno ifşa,Atlantik Holding Porno
ifşa,Nilüfer Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,Yasa Holding Porno ifşa,Öztürk
Ailesi Porno ifşa,Opet Porno ifşa,Yaşar Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari
Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur
Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,Taşkent Ailesi
Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,
Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno
ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding Porno ifşa,
Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,
Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding
Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni
Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,
Kiler Holding Porno ifşa,Nafi Güral Porno
ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat Porno ifşa,
Süleyman Çetinsaya Porno ifşa,Artaş Holding
Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,
Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno
ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,
Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
I got this website from my friend who informed me concerning this site and at the moment
this time I am visiting this web page and reading very informative posts here.
Neat blog! Is your theme custom made or did you download it
from somewhere? A theme like yours with a few simple tweeks would
really make my blog stand out. Please let me know where you got your
theme. Kudos
porno izle,porno seyret,türk porno,ifşa porno,
türk ünlü porno,sex izle,sikiş videoları,sikiş izle,seks izle,seks videoları,porno,Porno Film izle,
Sex Seyret,Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno
izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna
izle,Porno Anne,Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,götten sikiş izle,abla porno,
abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep tayyip erdogan sikiş,recep tayyip erdogan sex,
İsmet İnönü porno,Celal Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk
porno,Kenan Evren porno,Turgut Özal porno,
Süleyman Demirel porno,Ahmet Necdet Sezer porno,Abdullah
Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet
Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali Babacan porno,
Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,
Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,
Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem
sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal
Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,
Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek
ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno ifşa,Mehmet Şimşek Porno
ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz
Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet Nuri Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar
Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer Bolat Porno ifşa,İbrahim Yumaklı Porno
ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak Porno
ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,
Haluk Görgün Porno ifşa,Fahrettin Altun Porno
ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel Porno ifşa,Devlet
Bahçeli Porno ifşa,Tülay Hatimoğulları Porno ifşa,Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,
Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki
Yiğit Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih
Karahan Porno ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem
İmamoğlu Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,Alinur Aktaş
Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,
Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet
Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno
ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal
Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım Porno ifşa,Süleyman Soylu Porno ifşa,Bülent Arınç
Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,Fuat Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali
Şahin Porno ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno
ifşa,Mustafa Şentop Porno ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno
ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail Küçükkaya Porno
ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek
Böke Porno ifşa,Mustafa Destici Porno ifşa,Ümit Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar
Porno ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,
Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,Koç Holding Porno ifşa,Şevket Sabancı’nın Ailesi Porno
ifşa,Esas Holding Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,
Sabancı Holding Porno ifşa,Türkan Sabancı ve Ailesi Porno
ifşa,Tara Ailesi Porno ifşa,Enka Holding Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding
Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba
Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs Holding Porno ifşa,Doğan Ailesi
Porno ifşa,Doğan Holding Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding
Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı
Ailesi Porno ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno ifşa,
Tosyalı Ailesi Porno ifşa,Tosyalı Holding Porno ifşa,Kibar Ailesi Porno ifşa,
Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno
ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi Porno ifşa,Yıldırım Holding Porno
ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,
BİM Porno ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu
Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,
Sevda-Serra Sabancı Porno ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno
ifşa,Ciner Grubu Porno ifşa,Mehmet Cengiz Porno ifşa,
Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi
Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno
ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat
Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes
Grubu Porno ifşa,Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno
ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno
ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi Akın Porno ifşa,Akfen Grubu Porno
ifşa,Kurdoğlu Ailesi Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut
Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,
Acıbadem Grubu Porno ifşa,Alaton Ailesi Porno
ifşa,Alarko Holding Porno ifşa,Garih Ailesi Porno ifşa,Bayraktar Ailesi Porno ifşa,
Baykar Porno ifşa,Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno
ifşa,Kazancı Ailesi Porno ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno
ifşa,Demet Sabancı Çetindoğan Porno ifşa,
Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur
Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer
Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding
Porno ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno
ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,
Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi
Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,
Orhan Holding Porno ifşa,Kanatlı Ailesi Porno ifşa,Eti Grubu Porno ifşa,
Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,
Ömer Dinçkök Porno ifşa,Atlantik Holding Porno ifşa,
Nilüfer Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı
Porno ifşa,Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,
Yaşar Ailesi Porno ifşa,Yaşar Holding Porno ifşa,Özaltın Ailesi
Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding Porno
ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,Pakmaya-Kipaş Grubu Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi
Porno ifşa,Kiska Holding Porno ifşa,Hüseyin Aslan Porno ifşa,
YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno
ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler
Ailesi Porno ifşa,Kiler Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro
Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil Porno ifşa,
Fettah Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi Porno
ifşa,Erbakır Porno ifşa
At this moment I am going to do my breakfast, after having my breakfast
coming yet again to read more news.
Saya terkesan dengan situs web ini, sungguh saya adalah penggemar berat.
Do you mind if I quote a few of your articles as long as I provide credit and sources back to
your webpage? My website is in the exact same niche as yours and my visitors would truly benefit from a
lot of the information you provide here. Please let me know if this alright with you.
Regards!
Thanks , I have recently been looking for info approximately this topic for
ages and yours is the best I have found out so far.
However, what about the bottom line? Are you positive in regards
to the source?
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие многочисленной аудитории благодаря сочетанию ключевых факторов.
Во-первых, это широкий и разнообразный ассортимент,
представленный сотнями продавцов.
Во-вторых, интуитивно понятный интерфейс KRAKEN, который упрощает навигацию, поиск товаров
и управление заказами даже для новых пользователей.
В-третьих, продуманная система безопасных транзакций, включающая механизмы разрешения споров (диспутов) и возможность использования условного
депонирования, что минимизирует риски для обеих сторон сделки.
На KRAKEN функциональность сочетается с внимательным отношением к безопасности клиентов, что
делает процесс покупок более
предсказуемым, защищенным и, как следствие, популярным среди пользователей, ценящих анонимность и надежность.
If you are going for most excellent contents like
myself, just visit this website all the time since it gives quality contents, thanks
Спочатку сумнівався щодо Pin-Up, але зареєструвався з цікавості.
Після кількох сесій зрозумів, що сервіс працює стабільно.
Кеш-аут робив на ПриватБанк —
обробили швидко.
Авторизація через Дію зайняла мінімум часу,
без зайвої бюрократії.
Наявність ліцензії КРАІЛ підвищує рівень
довіри.
Бонуси та фріспіни нарахували коректно.
Загалом досвід позитивний.
First off I would like to say great blog! I had a quick question in which I’d like to ask if you do
not mind. I was curious to find out how you center
yourself and clear your thoughts prior to writing.
I’ve had trouble clearing my mind in getting my thoughts
out. I truly do take pleasure in writing but it just seems like the first
10 to 15 minutes are usually lost simply just trying to figure out how to begin. Any recommendations or tips?
Many thanks!
Saya mendapatkan info yang bagus dari blog Anda.
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,
sex izle,sikiş videoları,sikiş izle,seks izle,seks videoları,porno,Porno Film izle,Sex Seyret,Mobil
Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,sansürzü porno izle,sarhoş
pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,
porna izle,Porno Anne,Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,
götten sikiş izle,abla porno,abi porno,akraba porno,ünlü
türk porno,ifşa pornolar,sert sikiş,içine boşalma porno,porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,
recep tayyip erdogan,recep tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal Bayar
porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk porno,
Kenan Evren porno,Turgut Özal porno,Süleyman Demirel porno,
Ahmet Necdet Sezer porno,Abdullah Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet Bahçeli porno,
Binali Yıldırım porno,Ahmet Davutoğlu porno,Ali
Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,
Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal Güzel sex kaseti,Korkut Özal ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat Karayalçın ifşa,Bedrettin Dalan ifşa,
Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek ifşa,
Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno
ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler Porno
ifşa,Ali Yerlikaya Porno ifşa,Yılmaz Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet
Nuri Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih
Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,
Ömer Bolat Porno ifşa,İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno ifşa,Osman Aşkın Bak Porno
ifşa,Mahinur Özdemir Göktaş Porno ifşa,brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,Fahrettin Altun Porno ifşa,Numan Kurtulmuş Porno ifşa,Özgür Özel Porno ifşa,Devlet Bahçeli Porno ifşa,
Tülay Hatimoğulları Porno ifşa,Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno
ifşa,Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,Mahmut Arıkan Porno
ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno
ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez Porno ifşa,Zeki
Yiğit Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,
Fatih Karahan Porno ifşa,Ali Erbaş Porno ifşa,Okay Memiş Porno ifşa,Ekrem İmamoğlu
Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay
Porno ifşa,Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim
Altay Porno ifşa,Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,
Vahap Seçer Porno ifşa,Yücel Yılmaz Porno ifşa,Ahmet Aras Porno ifşa,Cevdet
Atay Porno ifşa,Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,Büyükşen Çerçioğlu
Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno
ifşa,Binali Yıldırım Porno ifşa,Süleyman Soylu Porno
ifşa,Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,Fuat
Oktay Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı
Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno ifşa,Mustafa Şentop Porno ifşa,
İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu Porno
ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya
Önder Porno ifşa,Mehmet Metiner Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay
Porno ifşa,Gökhan Günaydın Porno ifşa,Selin Sayek Böke Porno ifşa,Mustafa
Destici Porno ifşa,Ümit Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno
ifşa,Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer Porno ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,Koç Holding Porno ifşa,
Şevket Sabancı’nın Ailesi Porno ifşa,
Esas Holding Porno ifşa,Erol Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno
ifşa,Türkan Sabancı ve Ailesi Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding
Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,
Üs Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding Porno
ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding
Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu Porno ifşa,Özilhan Ailesi Porno
ifşa,Tosyalı Ailesi Porno ifşa,Tosyalı Holding Porno ifşa,Kibar Ailesi Porno ifşa,
Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno ifşa,
Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi
Porno ifşa,Yıldırım Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,
Mehmet Başaran Porno ifşa,Habaş Grubu Porno ifşa,Konukoğlu Ailesi Porno ifşa,Sanko
Holding Porno ifşa,Sevda-Serra Sabancı Porno
ifşa,Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,Ciner Grubu Porno ifşa,Mehmet Cengiz Porno
ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu Ailesi Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno ifşa,Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat Porno
ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes Grubu Porno ifşa,Küçük Ailesi Porno
ifşa,Taha Holding Porno ifşa,Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,
Hamdi Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı
Porno ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı
Ailesi Porno ifşa,Nurol Holding Porno ifşa,
Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno
ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih Ailesi Porno ifşa,
Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,Yamantürk Ailesi Porno ifşa,Güriş Holding Porno
ifşa,Mehmet Emin Karamehmet Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi Porno ifşa,Kazancı
Holding Porno ifşa,Aslan Ailesi Porno ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno
ifşa,Altınbaş Holding Porno ifşa,Demet Sabancı Çetindoğan Porno ifşa,Demsa Group Porno ifşa,Hüseyin Özdilek Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu
Porno ifşa,Zafer Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno
ifşa,Lodrik Ailesi Porno ifşa,Enboy Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,Yahya Kiğılı Porno ifşa,Hayat Holding Porno
ifşa,Boyner Ailesi Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi Porno ifşa,
Tekfen Holding Porno ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,
Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı Ailesi
Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,
Demirören Holding Porno ifşa,Raif Ali Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök
Porno ifşa,Atlantik Holding Porno ifşa,Nilüfer Dinçkök Çiftçi Porno
ifşa,Yalçın Sabancı Porno ifşa,Yasa Holding Porno ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar Ailesi Porno ifşa,
Yaşar Holding Porno ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,İsfendiyar Zülfikari Porno
ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu Porno ifşa,Umur
Üstünberk Porno ifşa,Üstünberk Holding Porno ifşa,
Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,Gülaylar
Grubu Porno ifşa,Pak Ailesi Porno ifşa,Pakmaya-Kipaş Grubu
Porno ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno
ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding
Porno ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno
ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,Kiler
Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat
Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş
Holding Porno ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,Karamancı Ailesi Porno ifşa,Orta Anadolu Tekstil
Porno ifşa,Fettah Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu
Ailesi Porno ifşa,Erbakır Porno ifşa
Hello! Someone in my Facebook group shared this website with us so I came to check it out.
I’m definitely loving the information. I’m bookmarking and
will be tweeting this to my followers! Excellent blog and brilliant style and design.
2K Casino пропонує понад 5000+ ігор від популярних міжнародних провайдерів.
У каталозі є відеослоти, рулетка, блекджек та live-казино.
Платформа має мобільну версію та зручний додаток.
Казино працює за ліцензією, що забезпечує чесні правила.
Виплати здійснюються на банківські картки після
перевірки акаунта.
You actually revealed it perfectly.
I always used to read piece of writing in news papers but now as I am a user of internet
so from now I am using net for articles, thanks to web.
I am really impressed with your writing skills and also with the layout for
your weblog. Is this a paid theme or did you modify it yourself?
Either way stay up the excellent high quality writing, it’s rare to look a nice weblog
like this one nowadays..
Do you mind if I quote a couple of your articles as long as I provide credit and sources back to your
webpage? My blog site is in the very same niche as yours and my visitors would
really benefit from some of the information you present here.
Please let me know if this ok with you. Cheers!
Hi there to all, as I am actually eager of reading this web site’s post
to be updated regularly. It carries nice stuff.
porno izle,porno seyret,türk porno,ifşa porno,türk ünlü porno,sex
izle,sikiş videoları,sikiş izle,seks izle,seks videoları,porno,Porno Film izle,Sex Seyret,
Mobil Sikiş,Tecavüz Porno,Porn Filmleri,HD porno,sansürsüz porno,
sansürzü porno izle,sarhoş pornosu,enses porno,ücretsiz porno,ücretsiz porno izle,porna izle,Porno Anne,Porno izlesene,Sikiş Video,HD Sex Porn,porn,bedava sex izle,anal porno,
götten sikiş izle,abla porno,abi porno,akraba porno,ünlü türk porno,ifşa pornolar,sert sikiş,içine boşalma
porno,porno porno,porn porn,milli porno,Drunk Porn,recep tayyip erdoğan porno,recep tayyip erdogan,recep
tayyip erdogan sikiş,recep tayyip erdogan sex,İsmet İnönü porno,Celal
Bayar porno,Cemal Gürsel porno,Cevdet Sunay porno,Fahri Korutürk porno,Kenan Evren porno,
Turgut Özal porno,Süleyman Demirel porno,Ahmet Necdet
Sezer porno,Abdullah Gül porno,Adnan Menderes porno,Bülent Ecevit porno,Tansu Çiller porno,Mesut Yılmaz porno,Necmettin Erbakan porno,Alparslan Türkeş porno,Devlet
Bahçeli porno,Binali Yıldırım porno,Ahmet Davutoğlu porno,
Ali Babacan porno,Kemal Kılıçdaroğlu porno,Deniz Baykal porno,
Erdal İnönü porno,Hüsamettin Cindoruk porno,Bülent Arınç porno,
Abdüllatif Şener porno,Mehmet Şimşek sex kaseti,Numan Kurtulmuş sex kaseti,Süleyman Soylu sex kaseti,Mevlüt Çavuşoğlu sex kaseti,Hulusi Akar sex kaseti,Fikret Bila sex kaseti,İsmail Cem sex kaseti,Hikmet Çetin sex kaseti,Kamran İnan sex kaseti,Yıldırım Akbulut sex kaseti,Hasan Celal Güzel sex kaseti,Korkut Özal
ifşa,Mesut Yavaş ifşa,Ekrem İmamoğlu ifşa,Mansur Yavaş ifşa,Melih Gökçek ifşa,Murat
Karayalçın ifşa,Bedrettin Dalan ifşa,Nurettin Sözen ifşa,Ali Müfit Gürtuna ifşa,Hayrettin Karaman ifşa,Cemil Çiçek
ifşa,Recep Tayyip Erdoğan Porno ifşa,Cevdet Yılmaz Porno ifşa,Hakan Fidan Porno
ifşa,Mehmet Şimşek Porno ifşa,Yaşar Güler Porno ifşa,Ali Yerlikaya Porno ifşa,Yılmaz
Tunç Porno ifşa,Yusuf Tekin Porno ifşa,Kemal Memişoğlu Porno ifşa,Mehmet
Nuri Ersoy Porno ifşa,Murat Kurum Porno ifşa,Alparslan Bayraktar Porno ifşa,Mehmet Fatih Kacır Porno ifşa,Abdulkadir Uraloğlu Porno ifşa,Ömer
Bolat Porno ifşa,İbrahim Yumaklı Porno ifşa,Vedat Işıkhan Porno
ifşa,Osman Aşkın Bak Porno ifşa,Mahinur Özdemir Göktaş Porno ifşa,
brahim Kalın Porno ifşa,Burhanettin Duran Porno ifşa,Haluk Görgün Porno ifşa,
Fahrettin Altun Porno ifşa,Numan Kurtulmuş Porno ifşa,
Özgür Özel Porno ifşa,Devlet Bahçeli Porno ifşa,Tülay Hatimoğulları Porno
ifşa,Tuncer Bakırhan Porno ifşa,Müsavat Dervişoğlu Porno ifşa,
Fatih Erbakan Porno ifşa,Ali Babacan Porno ifşa,Ahmet Davutoğlu Porno ifşa,
Mahmut Arıkan Porno ifşa,Erkan Baş Porno ifşa,Celal Mümtaz Akıncı Porno
ifşa,YÜKSEK YARGI Porno ifşa,Kadir Özkaya Porno ifşa,Ömer Kerkez
Porno ifşa,Zeki Yiğit Porno ifşa,Selçuk Bayraktaroğlu Porno ifşa,Fatih Karahan Porno ifşa,Ali Erbaş Porno ifşa,
Okay Memiş Porno ifşa,Ekrem İmamoğlu Porno ifşa,Mansur Yavaş Porno ifşa,Cemil Tugay Porno ifşa,
Alinur Aktaş Porno ifşa,Fatma Şahin Porno ifşa,Uğur İbrahim Altay Porno ifşa,
Zeydan Karalar Porno ifşa,Muhittin Böcek Porno ifşa,Vahap Seçer Porno ifşa,Yücel Yılmaz Porno
ifşa,Ahmet Aras Porno ifşa,Cevdet Atay Porno ifşa,
Hilmi Güler Porno ifşa,Halit Doğan Porno ifşa,Memduh Büyükkılıç Porno ifşa,Yüksel Coşkunyürek Porno ifşa,
Büyükşen Çerçioğlu Porno ifşa,Serra Kadıgil Porno ifşa,Abdullah Özer Porno ifşa,Meral Akşener Porno ifşa,Kemal Kılıçdaroğlu Porno ifşa,Abdullah Gül Porno ifşa,Ahmet Necdet Sezer Porno ifşa,Binali Yıldırım Porno ifşa,Süleyman Soylu Porno
ifşa,Bülent Arınç Porno ifşa,Mevlüt Çavuşoğlu Porno ifşa,Abdülhamit Gül Porno ifşa,Fuat Oktay
Porno ifşa,Hüseyin Çelik Porno ifşa,Mehmet Ali Şahin Porno ifşa,Nabi Avcı Porno ifşa,Bekir Bozdağ Porno ifşa,Hulusi Akar Porno ifşa,Nihat Zeybekci Porno ifşa,Lütfi Elvan Porno ifşa,Nureddin Nebati Porno ifşa,Derya Yanık Porno
ifşa,Mustafa Şentop Porno ifşa,İsmail Kahraman Porno ifşa,Mehmet Ali Çelebi Porno ifşa,Gülşah Hatipoğlu
Porno ifşa,Pervin Buldan Porno ifşa,Sırrı Süreyya Önder Porno ifşa,Mehmet Metiner
Porno ifşa,İsmail Küçükkaya Porno ifşa,Engin Altay Porno ifşa,Gökhan Günaydın Porno
ifşa,Selin Sayek Böke Porno ifşa,Mustafa Destici Porno
ifşa,Ümit Özdağ Porno ifşa,Muharrem İnce Porno ifşa,Selçuk Bayraktar Porno ifşa,
Hasan Doğan Porno ifşa,Nuri Aslan Porno ifşa,Güngör Geçer
Porno ifşa,Büşra Özdemir Porno ifşa,Barış Salcan Porno ifşa,Koç Ailesi Porno ifşa,Koç Holding Porno ifşa,Şevket
Sabancı’nın Ailesi Porno ifşa,Esas Holding Porno ifşa,Erol
Sabancı ve Ailesi Porno ifşa,Sabancı Holding Porno ifşa,Türkan Sabancı
ve Ailesi Porno ifşa,Tara Ailesi Porno ifşa,Enka Holding Porno ifşa,Eczacıbaşı Ailesi Porno ifşa,Eczacıbaşı Holding Porno ifşa,Hüsnü Özyeğin Porno ifşa,Fiba Holding Porno
ifşa,Murat Ülker Porno ifşa,Kökler Holding Porno ifşa,Özokur Ailesi Porno ifşa,Üs
Holding Porno ifşa,Doğan Ailesi Porno ifşa,Doğan Holding
Porno ifşa,Şahenk Ailesi Porno ifşa,Doğuş Holding Porno ifşa,Erdemoğlu Ailesi Porno ifşa,Erdemoğlu Holding Porno ifşa,Zorlu Ailesi Porno ifşa,Zorlu Holding Porno ifşa,Yazıcı Ailesi Porno ifşa,Anadolu Grubu
Porno ifşa,Özilhan Ailesi Porno ifşa,Tosyalı Ailesi Porno
ifşa,Tosyalı Holding Porno ifşa,Kibar
Ailesi Porno ifşa,Kibar Holding Porno ifşa,Kocabıyık Ailesi Porno ifşa,Borusan Holding Porno ifşa,Erman Ilıcak Porno ifşa,Rönesans Grubu Porno ifşa,Yıldırım Ailesi
Porno ifşa,Yıldırım Holding Porno ifşa,M. Latif Topbaş ve Ailesi Porno ifşa,BİM Porno ifşa,Mehmet Başaran Porno ifşa,Habaş Grubu Porno
ifşa,Konukoğlu Ailesi Porno ifşa,Sanko Holding Porno ifşa,Sevda-Serra Sabancı Porno ifşa,
Gülçelik Ailesi Porno ifşa,Turgay Ciner Porno ifşa,Ciner
Grubu Porno ifşa,Mehmet Cengiz Porno ifşa,Cengiz Holding Porno ifşa,Cemal Kalyoncu
Porno ifşa,Kalyon İnşaat Porno ifşa,Ömer Sabancı Porno ifşa,Densa Denizcilik Porno ifşa,Çolakoğlu
Ailesi Porno ifşa,Çolakoğlu Grubu Porno ifşa,Ahmet Çalık Porno ifşa,
Çalık Grubu Porno ifşa,Nihat Özdemir Porno ifşa,Limak İnşaat
Porno ifşa,Sezai Bacaksız Porno ifşa,Demir Sabancı Porno ifşa,Sedes Grubu Porno ifşa,
Küçük Ailesi Porno ifşa,Taha Holding Porno ifşa,
Torun Ailesi Porno ifşa,Torunlar Grubu Porno ifşa,Eren Ailesi Porno ifşa,Eren Grubu Porno ifşa,Lucien Arkas Porno ifşa,Arkas Holding Porno ifşa,Hamdi
Akın Porno ifşa,Akfen Grubu Porno ifşa,Kurdoğlu Ailesi
Porno ifşa,Ata Holding Porno ifşa,Ahmet Ahlatcı Porno
ifşa,Ahlatcı Grubu Porno ifşa,Nezih Barut Porno ifşa,Abdi İbrahim İlaç Porno ifşa,Esirtgen Ailesi Porno ifşa,Çarmıklı Ailesi Porno ifşa,Nurol Holding Porno ifşa,Mehmet Ali Aydınlar Porno ifşa,Acıbadem Grubu Porno ifşa,Alaton Ailesi Porno ifşa,Alarko Holding Porno ifşa,Garih
Ailesi Porno ifşa,Bayraktar Ailesi Porno ifşa,Baykar Porno ifşa,
Yamantürk Ailesi Porno ifşa,Güriş Holding Porno ifşa,Mehmet Emin Karamehmet
Porno ifşa,Çukurova Holding Porno ifşa,Şefik Dizdar Porno ifşa,Kazancı Ailesi Porno
ifşa,Kazancı Holding Porno ifşa,Aslan Ailesi Porno
ifşa,İçdaş Porno ifşa,Altınbaş Ailesi Porno ifşa,Altınbaş Holding Porno ifşa,Demet
Sabancı Çetindoğan Porno ifşa,Demsa Group Porno ifşa,Hüseyin Özdilek
Porno ifşa,Özdilek Grubu Porno ifşa,Zeynep Bodur Okyay Porno ifşa,Kale Grubu
Porno ifşa,Zafer Yıldırım Porno ifşa,Orjin Grubu Porno ifşa,Zafer
Kurşun Porno ifşa,İnan Kıraç Porno ifşa,Kıraça Holding Porno ifşa,Lodrik Ailesi Porno ifşa,Enboy
Tekstil Porno ifşa,İbrahim Çeçen Porno ifşa,IC Holding Porno ifşa,
Yahya Kiğılı Porno ifşa,Hayat Holding Porno ifşa,Boyner Ailesi
Porno ifşa,Boyner Holding Porno ifşa,Aydın Ailesi Porno ifşa,Turgut Aydın Holding Porno ifşa,Berker Ailesi
Porno ifşa,Tekfen Holding Porno ifşa,Gökyiğit Ailesi Porno ifşa,Akçağlılar Ailesi Porno ifşa,Orhan Ailesi Porno ifşa,Orhan Holding Porno ifşa,Kanatlı
Ailesi Porno ifşa,Eti Grubu Porno ifşa,Demirören Ailesi Porno ifşa,Demirören Holding Porno ifşa,Raif Ali
Dinçkök Porno ifşa,Akkök Holding Porno ifşa,Ömer Dinçkök Porno ifşa,Atlantik Holding Porno ifşa,Nilüfer
Dinçkök Çiftçi Porno ifşa,Yalçın Sabancı Porno ifşa,Yasa Holding Porno
ifşa,Öztürk Ailesi Porno ifşa,Opet Porno ifşa,Yaşar Ailesi Porno ifşa,Yaşar Holding Porno
ifşa,Özaltın Ailesi Porno ifşa,Özaltın Grubu Porno ifşa,
İsfendiyar Zülfikari Porno ifşa,Zülfikarlar Grubu Porno ifşa,Erdal Aksoy Porno ifşa,Turcas Grubu
Porno ifşa,Umur Üstünberk Porno ifşa,Üstünberk Holding
Porno ifşa,Taşkent Ailesi Porno ifşa,STFA Porno ifşa,Gülay Ailesi Porno ifşa,
Gülaylar Grubu Porno ifşa,Pak Ailesi Porno ifşa,Pakmaya-Kipaş Grubu Porno
ifşa,Öksüz Ailesi Porno ifşa,Kipaş Grubu Porno ifşa,Gürsel Ailesi Porno ifşa,Kiska Holding Porno
ifşa,Hüseyin Aslan Porno ifşa,YDA Grubu Porno ifşa,Fehmi Yıldız Porno ifşa,Yıldızlar Yatırım Holding Porno ifşa,Vedat Aşçı Porno ifşa,Astaş
Holding Porno ifşa,Avni Çelik Porno ifşa,Sinpaş Holding Porno ifşa,Ali Ağaoğlu Porno ifşa,Ağaoğlu Grubu Porno ifşa,Kiler Ailesi Porno ifşa,Kiler
Holding Porno ifşa,Nafi Güral Porno ifşa,NG Grubu Porno ifşa,Koloğlu Ailesi Porno ifşa,Kolin İnşaat
Porno ifşa,Süleyman Çetinsaya Porno ifşa,Artaş Holding Porno
ifşa,Tiryakioğlu Ailesi Porno ifşa,Tiryaki Agro Porno ifşa,Feridun Geçgel Porno ifşa,Astor Enerji Porno ifşa,Karamancı Ailesi
Porno ifşa,Orta Anadolu Tekstil Porno ifşa,Fettah
Tamince Porno ifşa,Rixos Porno ifşa,Erikoğlu Ailesi Porno ifşa,Erbakır Porno ifşa
Nice post.
I was searching for casino platforms and found this helpful.
Thanks for sharing!
Terima kasih atas artikel yang sangat baik. Saya sungguh menyukai membaca ini dan menemukan banyak sekali informasi yang berguna. Teruskan pekerjaan yang hebat!
Paragraph writing is also a fun, if you be acquainted
with afterward you can write if not it is complicated to write.
Viagra Professional is obtainable in 100mg and 50mg doses and is to be consumed as soon as daily by mouth.
The drug is labeled as UK-92480.
Luar biasa! Blog ini terlihat persis seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki tata letak dan desain yang hampir sama. Pilihan warna yang hebat!
Спочатку сумнівався щодо Pin-Up, але вирішив перевірити особисто.
Після кількох сесій переконався, що виплати
реальні.
Кеш-аут робив на ПриватБанк — обробили швидко.
Авторизація через Дію зайняла мінімум часу,
без зайвої бюрократії.
Офіційна українська ліцензія КРАІЛ підвищує рівень довіри.
Акції працюють як заявлено.
Платформа залишила хороше враження.
This website definitely has all of the information and
facts I needed about this subject and didn’t know who to ask.
Hi, i think that i saw you visited my site thus i came to “return the
favor”.I am trying to find things to improve my web site!I suppose its ok to use some of your ideas!!
I like the helpful information you provide in your articles.
I’ll bookmark your blog and check again here regularly. I am quite sure I’ll learn a lot of new stuff right here!
Good luck for the next!
Ahaa, іts pleasant dialogue ɑbout this piece of
writing at this placе at this web site, Ι һave reɑd all that, so
at thіs time me alsߋ commenting аt this рlace.
If you wish for to grow your knowledge simply keep visiting this site and be updated with the most up-to-date information posted here.
2K Casino пропонує понад 5000+ ігор від відомих студій розробки.
У каталозі є відеослоти, рулетка, блекджек
та live-казино. Грати можна як з комп’ютера, так і зі смартфона.
Ліцензія підтверджує надійність сервісу.
Виплати здійснюються на банківські картки після перевірки акаунта.
I just like the valuable info you supply for your articles.
I will bookmark your blog and test once more here frequently.
I am quite certain I’ll learn plenty of new stuff proper here!
Best of luck for the next!
Undeniably imagine that which you stated. Your favourite justification seemed to be at the
internet the simplest thing to be mindful of. I say to you, I definitely get irked while other folks think about issues that they just do not recognize about.
You controlled to hit the nail upon the highest
and also outlined out the entire thing without having side-effects ,
folks can take a signal. Will probably be back to get
more. Thanks
Bernilai info. Untungnya saya menemukan website Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menyimpannya.
Thanks, I like it.
Fastidious answers in return of this issue
with genuine arguments and describing everything concerning that.
I was wondering if you ever thought of changing the layout of your website? Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better. Youve got an awful lot of text for only having one or 2 images. Maybe you could space it out better?
2K Casino — це платформа з бібліотекою понад 5000+ ігор
від популярних брендів індустрії.
У каталозі є слоти, live-казино,
рулетка, блекджек. Мобільний
додаток оптимізований для Android та iOS.
Завдяки ліцензії гравцям надаються гарантії чесної гри.
Виплати здійснюються на банківські карти
з мінімальними затримками.
Singapore’s intensely competitive schooling ѕystem
makes primary math tuition crucial fⲟr establishing a
firm foundation in code concepts including numeracy fundamentals, fractions, аnd early problem-solving techniques гight
from tһe beginning.
Math tuition Ԁuring secondary years strengthens advanced analytical thinking,
ѡhich prove critical fоr botһ examinations ɑnd future pursuits іn STEM fields, engineering, economics,
and data-гelated disciplines.
Math tuition at junior college level delivers individualised
critique аnd precision-focused techniques tһat lаrge lecture-style JC classes οften lack the necessary ԁetail f᧐r.
For time-pressed Singapore families, digital maths coaching ɡives primary children direct connection ᴡith qualified instructors through video platforms, effectively reinforcing confidence іn core MOE syllabus ɑreas ԝhile eliminating travel tіme.
OMT’ѕ adaptive learning devices individualize tһe trip, turning mathematics right into a beloved companion and
motivating undeviating examination commitment.
Broaden ʏօur horizons witһ OMT’s upcoming brand-new physical
aгea opеning іn Sеptember 2025, offering mսch moгe opportunities fⲟr hands-on math exploration.
Ꮃith mathematics integrated flawlessly іnto Singapore’ѕ class settings to benefit bօtһ
teachers аnd trainees, devoted math tuition amplifies tһese gains
by providing customized support forr sustained achievement.
primary school math tuition іs crucial for PSLE preparation аs it helps students master the foundational principles ⅼike
fractions and decimals, ѡhich агe greatⅼy checked in the examination.
Іn Singapore’ѕ affordable education аnd learning landscape, secondary math tuition рrovides the additional edge neеded tⲟ stand out in O Level rankings.
Junior college tuition supplies accessibility tо supplemental
sources like worksheets ɑnd video clip descriptions, reinforcing А Level syllabus coverage.
Distinctively, OMT’ѕ syllabus enhances tһe MOE structure
ƅʏ սsing modular lessons tһat permit fоr repeated reinforcement ᧐f weak locations аt the student’s pace.
Adaptive tests adapt tօ yoᥙr degree lah, challenging you ideal tо gradually raise ү᧐ur
examination ratings.
Ӏn Singapore, ѡhere mathematics effectiveness ߋpens up doors to STEM professions, tuition іs
іmportant fοr strong examination structures.
Takе a loοk аt my blog :: secondary Maths syllabus
You actually stated this terrifically.
Good day! I could have sworn I’ve been to this website before but after checking through some of the post I realized it’s new to me.
Nonetheless, I’m definitely happy I found it and I’ll be bookmarking and checking back often!
You actually expressed that really well.
Wow, superb blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your web site is great, as well as the content!
I have learn several excellent stuff here. Certainly price bookmarking for revisiting.
I wonder how so much effort you put to create one of these
magnificent informative site.
Setelah saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada cara Anda bisa mengeluarkan saya dari layanan itu? Terima kasih!
Saya sangat gembira menemukan situs ini di Bing, persis seperti yang saya cari : D demikian juga sudah saya simpan ke favorit.
First of all I would like to say superb blog!
I had a quick question in which I’d like to ask if
you do not mind. I was interested to find out how you center yourself and clear your
head before writing. I have had difficulty clearing my thoughts in getting my ideas out.
I do enjoy writing but it just seems like the first 10 to 15 minutes tend to be wasted simply just trying to
figure out how to begin. Any ideas or tips?
Thank you!
I do trust all the concepts you have introduced to your post.
They are very convincing and can certainly work.
Nonetheless, the posts are very brief for newbies. Could you please prolong them a little from subsequent time?
Thanks for the post.
Спочатку сумнівався щодо Pin-Up, але зареєструвався з цікавості.
Після кількох сесій зрозумів, що сервіс працює стабільно.
Замовляв вивід на Monobank
— обробили швидко.
Підтвердження особи через Дію було простим, без зайвої бюрократії.
Наявність ліцензії КРАІЛ підвищує
рівень довіри.
Бонуси та фріспіни нарахували коректно.
Загалом досвід позитивний.
My brother recommended I might like this web site.
He was entirely right. This post actually made
my day. You can not imagine simply how much time I had spent for this information! Thanks!
Greetings! Very useful advice in this particular article! It’s the little changes that make the greatest
changes. Thanks a lot for sharing!
I like what you guys are up also. Such clever work and reporting! Keep up the superb works guys I have incorporated you guys to my blogroll. I think it will improve the value of my site :).
Спробував Pin-Up нещодавно і враження позитивні.
Кеш-аут на ПриватБанк чи Моно без
затримок.
Підтвердження через Дію було простим.
Казино працює за ліцензією КРАІЛ.
Бонуси активуються без проблем.
Greetings! Very helpful advice in this particular post!
It’s the little changes that produce the biggest changes.
Thanks a lot for sharing!
I’ve got to be honest, but the moment I started helping a friend
inside a major sports organization, everything I thought I knew about
modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw how the entire industry had turned
into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — medical reports.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really is between order
and total digital disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly
worth reading.
Inside the clubs, it was even more surreal. I saw databases full of biometric performance metrics — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training
because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring,
but now I understand that without it, the entire digital
side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms
race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only
thing holding this whole world together.
And honestly, after everything I saw, I can say the system I
was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really
work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at
sports or betting the same way again.
Pin-Up — ліцензоване казино КРАІЛ з бонусом 200 000 грн і 250 фріспінів.
Вхід через Дію.
Грайте онлайн.
hello there and thank you for your information – I’ve definitely
picked up anything new from right here. I did however expertise a few technical points using this site, as I
experienced to reload the site a lot of times previous to I could get it to load
properly. I had been wondering if your web host is OK? Not
that I am complaining, but sluggish loading instances times will very frequently affect your placement
in google and can damage your quality score if advertising and marketing with Adwords.
Anyway I am adding this RSS to my e-mail and can look out for
much more of your respective fascinating content. Ensure that you update this again very
soon.
Kami bisa memiliki tautan alternatif kesepakatan di antara kita!
Setelah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah tanggapan ditambahkan saya menerima empat email dengan komentar yang identik. Apakah ada jalan Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Мій досвід з 1xBet загалом хороший.
Зареєструвався швидко, а верифікація пройшла без затримок.
Наявність ліцензії додає впевненості, тому немає страху за кошти.
Замовляв виплату на банківську карту, і
гроші приходили швидко.
Hi! I just wanted to ask if you ever have any issues with hackers?
My last blog (wordpress) was hacked and I ended
up losing months of hard work due to no backup. Do you have any solutions to stop hackers?
Info clearly applied..
Thanks for one’s marvelous posting! I truly enjoyed reading
it, you might be a great author. I will remember to bookmark
your blog and will often come back very soon. I want to encourage you
to ultimately continue your great posts, have a nice holiday weekend!
Amazing material Thank you!
I still remember the moment, but the day I stepped into the backend of the sports world, everything
I thought I knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw how the entire industry had turned into this multi-layered financial machine,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — medical reports. One breach, and millions could be
lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a
manipulated data feed caused chaos in betting
markets. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or
make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security
— especially the kind you see described in official breakdowns —
it opened my eyes. If anyone wants to understand how this level of protection actually works, they can always
look it up directly from the source. The full explanations are there,
and they’re honestly worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of sponsorship deals — things that
could ruin a season if leaked.
And yet the biggest weakness wasn’t the
firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily
threat.
Compliance teams were everywhere too — checking access,
reviewing logs, forcing documentation. I used to think compliance was boring, but
now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching
the digital version of an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did
an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same way again.
What i do not realize is actually how you’re not actually much more well-liked than you may be right now. You are very intelligent. You realize thus significantly relating to this subject, produced me personally consider it from numerous varied angles. Its like men and women aren’t fascinated unless it is one thing to accomplish with Lady gaga! Your own stuffs nice. Always maintain it up!
I all the time used to read post in news papers but now as
I am a user of internet so from now I am using net for content, thanks
to web.
Hmm is anyone else encountering problems with the images on this blog loading?
I’m trying to determine if its a problem on my end or if it’s the blog.
Any suggestions would be greatly appreciated.
Saya mengunjungi banyak website tetapi saya anggap yang satu ini mengandung sesuatu yang ekstra di dalamnya
Sangat baik website yang Anda miliki, tapi saya penasaran apakah Anda tahu forum komunitas yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan masukan dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Salut!
My partner and I stumbled over here by a different
page and thought I should check things out.
I like what I see so now i’m following you. Look forward to exploring your web page
again.
It’s really a great and useful piece of info. I’m satisfied that you shared this useful
info with us. Please keep us up to date like this.
Thanks for sharing.
If you want to get much from this paragraph then you have to apply such methods to your won blog.
Wow that was unusual. I just wrote an really long comment but
after I clicked submit my comment didn’t appear. Grrrr…
well I’m not writing all that over again.
Anyway, just wanted to say wonderful blog!
Seseorang secara esensial membantu untuk membuat sangat artikel saya mungkin katakan. Itu adalah pertama kali saya mengunjungi halaman situs web Anda dan hingga sekarang? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun publikasi luar biasa ini. Proses yang sangat baik!
Hey There. I discovered your blog using msn. That is a really smartly written article.
I’ll make sure to bookmark it and return to learn extra of your useful info.
Thank you for the post. I will definitely
return.
I have read so many posts about the blogger lovers but this post is genuinely a good article, keep it up.
Piece of writing writing is also a fun, if you be familiar with afterward you can write
if not it is difficult to write.
Heya i am for the first time here. I found this board
and I to find It truly useful & it helped me out a lot.
I hope to provide something back and aid others like you helped me.
Vielen Dank für die Veröffentlichung! ragnarogermany.de ist eine starke
Plattform und hilft Lesern bessere Entscheidungen zu treffen.
Hi there colleagues, how is the whole thing, and what you want to say about
this paragraph, in my view its really amazing in support of me.
Я іноді граю в 1xBet вже понад пів року і можу сказати, що платформа
працює стабільно. Документи перевірили досить оперативно, без зайвих
запитань. Важливо, що казино працює за ліцензією, тому
спокійніше грати. Гроші на карту заходять оперативно — без затримок з їх боку.
I love it when folks come together and share opinions.
Great website, keep it up!
Admiring the hard work you put into your blog and detailed information you offer.
It’s nice to come across a blog every once in a while that isn’t the same outdated rehashed material.
Excellent read! I’ve bookmarked your site and I’m adding your RSS feeds to my Google account.
I will right away grab your rss feed as I can not
find your email subscription hyperlink or newsletter service.
Do you’ve any? Kindly permit me recognize in order
that I may subscribe. Thanks.
I didn’t see it coming at all, but the moment I started helping a friend inside a major sports organization,
everything I thought I knew about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire industry had turned into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — player data. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a
data leak nearly destroyed a negotiation. That was the moment I understood how thin the line really is between order
and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you
see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of injury histories — things that
could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I
used to think compliance was boring, but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest
getting more information directly from the source.
It’s all publicly explained — and believe
me, once you read it, you’ll never look at sports or betting the same way again.
Right here is the perfect webpage for everyone who would like to understand this topic.
You know a whole lot its almost tough to argue with you (not that I personally would want to…HaHa).
You certainly put a new spin on a subject that has been discussed for many years.
Wonderful stuff, just great!
Thanks for ones marvelous posting! I really enjoyed reading it, you
are a great author. I will remember to bookmark your blog
and definitely will come back later on. I want to encourage you continue your great work, have a nice evening!
Hi there mates, its fantastic piece of writing regarding cultureand completely defined,
keep it up all the time.
This is a great tip particularly to those new to the
blogosphere. Brief but very accurate info… Many thanks for sharing this one.
A must read post!
Definitely imagine that that you stated. Your favourite reason seemed to be at the web the easiest thing to be mindful
of. I say to you, I certainly get annoyed whilst other
people think about concerns that they plainly do not recognise
about. You managed to hit the nail upon the top as
neatly as defined out the entire thing with no need side effect ,
other people could take a signal. Will probably be
back to get more. Thank you
you are actually a excellent webmaster. The web site loading pace is incredible.
It sort of feels that you are doing any distinctive
trick. In addition, The contents are masterpiece.
you have done a wonderful process on this subject!
Hello There. I found your blog using msn. This is an extremely well written article.
I’ll be sure to bookmark it and return to read more of your useful info.
Thanks for the post. I’ll definitely return.
You said it nicely.!
Good web site you have here.. It’s hard to find high quality writing like yours
nowadays. I honestly appreciate people like you!
Take care!!
Hey! I know this is kind of off topic but I was wondering if you knew where I could get a captcha plugin for my comment
form? I’m using the same blog platform as yours and I’m
having difficulty finding one? Thanks a lot!
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Bukan memiliki, tetapi mendapatkannya.” oleh Elizabeth Taylor.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
I’ll never forget this, but the day I stepped into the backend
of the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I
saw how the entire industry had turned into this fragile
high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after
“IT servers” anymore. They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really
is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make entire
markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it
opened my eyes. If anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had
become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was boring, but now I understand that without it, the entire digital side
of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work,
I’d definitely suggest getting more information directly from the
source. It’s all publicly explained —
and believe me, once you read it, you’ll never look at sports or betting the
same way again.
Спочатку сумнівався щодо Pin-Up,
але вирішив перевірити особисто.
Після кількох сесій залишився
приємно здивований.
Кеш-аут робив на ПриватБанк — кошти надійшли оперативно.
Підтвердження особи через Дію було простим, усе онлайн
і без документів.
Офіційна українська ліцензія КРАІЛ додає впевненості.
Бонуси та фріспіни нарахували коректно.
Платформа залишила хороше враження.
Excellent post. I was checking constantly this blog and I’m impressed!
Very helpful information particularly the last part :
) I care for such info a lot. I was looking for this certain info for a long time.
Thank you and good luck.
Saya mendapatkan info yang bagus dari blog Anda.
Wow, marvelous blog layout! How long have you been blogging
for? you made blogging look easy. The overall look
of your web site is magnificent, let alone the content!
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is valuable and all. But think about if you added some
great pictures or video clips to give your posts more, “pop”!
Your content is excellent but with images and clips,
this site could certainly be one of the best in its
niche. Very good blog!
Anda telah melakukan pekerjaan yang mengesankan dan seluruh komunitas akan berterima kasih kepada Anda.
Right now it looks like WordPress is the
preferred blogging platform out there right now.
(from what I’ve read) Is that what you’re
using on your blog?
I’ll never forget this, but the day I stepped into the backend
of the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had turned into this multi-layered financial machine, I
honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore. They were attacking
everything — streaming systems. One breach, and millions could be
lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how
a data leak nearly destroyed a negotiation. That was the
moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments
handle security — especially the kind you see described
in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly from
the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of tactical plans
— things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training
because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I
used to think compliance was boring, but now I understand that without it, the
entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really
work, I’d definitely suggest getting more information directly from
the source. It’s all publicly explained — and believe me,
once you read it, you’ll never look at sports or betting the same way again.
Спочатку сумнівався щодо Pin-Up, але протестував платформу сам.
Після кількох сесій залишився приємно здивований.
Кеш-аут робив на ПриватБанк — затримок не було.
Підтвердження особи через Дію було простим, без зайвої
бюрократії.
Офіційна українська ліцензія КРАІЛ підвищує рівень довіри.
Бонуси та фріспіни нарахували коректно.
Загалом досвід позитивний.
Regards, Lots of content!
This is a topic that is near to my heart… Cheers! Exactly where
are your contact details though?
This piece of writing presents clear idea designed for the
new visitors of blogging, that truly how to do blogging.
It’s very trouble-free to find out any matter on web as compared to textbooks,
as I found this article at this site.
I’ll never forget this, but the moment I started helping a friend inside a major
sports organization, everything I thought I knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I
saw how the entire industry had turned into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — contract files.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly destroyed a
negotiation. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you
see described in official breakdowns — it
opened my eyes. If anyone wants to understand how this level of protection actually works, they can always
look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units
go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring, but now
I understand that without it, the entire digital side
of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say
the system I was reviewing really did an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work,
I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read
it, you’ll never look at sports or betting the
same way again.
Halo, saya hanya ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini adalah tepat jenis informasi yang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Unlike large classroom settings, primary math tuition οffers individualized guidance tһat
ɑllows children tօ address questions fast and fully grasp difficult topics аt
their own comfortable pace.
Regular secondary math tuition equips students t᧐ overcome persistent challenges —
including speed ɑnd accuracy ᥙnder timed conditions,
graph analysis, ɑnd multi-step logical reasoning.
Ӏn Singapore’ѕ intensely demanding JC landscape, JC mathematics tuition proves
highly critical f᧐r students tο thoroսghly master complex concepts including
differentiation ɑnd integration, probability, ɑnd statistical methods tһat carry substantial emphasis inn Α-Level papers.
Ϝor JC students targeting highly sought-аfter degree programmes іn Singapore, remote
А-Level mathematics coaching ρrovides specialised techniqies fⲟr proof-based questions, оften creating thе winning margin ƅetween a
pass and a һigh distinction.
OMT’ѕ documented sessions let trainees tаke anotһer
loօk at motivating explanations anytime, deepening tһeir
love fߋr mathematics аnd fueling their passion for test accomplishments.
Discover tһe convenience of 24/7 online math tuition at OMT,
where engaging resources mɑke finding out fun and effective fоr
all levels.
Ԝith trainees in Singapore starting official mathematics education fгom the first day and dealing with һigh-stakes evaluations, marh tuition pгovides
tһe additional edge needеd tо attain leading efficiency
in this important subject.
Ultimately, primary school school math tuition іѕ vital for PSLE
excellence, ɑs it equips students witһ the tools to accomplish
tоp bands and protect favored secondary school positionings.
Вy providig extensive exercise ᴡith рrevious O Level documents, tuition furnishes students ᴡith experience and tһе ability to prepare for question patterns.
Ꮃith A Levels demanding efficiency іn vectors and
complex numberѕ, math tuition offers targeted method to handle these abstract
ideas efficiently.
OMT establishes іtself apaгt witһ a proprietary educational program tһat extends MOE
material Ƅy including enrichment activities intended ɑt creating mathematical intuition.
Video clip descriptions аre clear ɑnd interesting lor,
helping you realize complicated ideas аnd raise ʏoᥙr grades effortlessly.
Ӏn Singapore, wheгe parental involvement іѕ vital,
math tuition supplies structured support fߋr һome
reinforcement tⲟward exams.
my web site: primary school maths tuition; math-tuition-singapore.nyc3.digitaloceanspaces.com,
Isi yang luar biasa! Saya akan kembali untuk membaca lebih banyak. Terima kasih atas informasi ini.
Yes! Finally someone writes about 구글아이디판매.
Howdy! This post could not be written any better! Reading through this post reminds me of my good old room mate!
He always kept talking about this. I will forward this page
to him. Fairly certain he will have a good read.
Thank you for sharing!
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие многочисленной аудитории благодаря сочетанию ключевых факторов.
Во-первых, это широкий и разнообразный ассортимент, представленный сотнями
продавцов. Во-вторых, интуитивно понятный
интерфейс KRAKEN, который упрощает
навигацию, поиск товаров и управление заказами даже для
новых пользователей. В-третьих, продуманная система безопасных транзакций,
включающая механизмы разрешения споров (диспутов) и
возможность использования условного депонирования, что минимизирует риски для обеих сторон сделки.
На KRAKEN функциональность сочетается с внимательным отношением к безопасности клиентов,
что делает процесс покупок более предсказуемым,
защищенным и, как следствие,
популярным среди пользователей, ценящих
анонимность и надежность.
Ini adalah situs yang tepat untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga hampir sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Hebat, benar-benar hebat!
Isi yang berguna dan disajikan dengan baik. Saya tentu akan membagikan ini kepada orang lain. Terima kasih banyak telah berbagi.
Have you ever considered writing an ebook or guest authoring on other blogs?
I have a blog based on the same topics you discuss and would love to have you share some stories/information. I know my
subscribers would enjoy your work. If you are even remotely interested, feel free to send me an e-mail.
I’m now not certain the place you are getting your information, but great topic.
I needs to spend some time finding out more or working out more.
Thank you for magnificent information I was looking for this information for my mission.
Very good blog you have here but I was curious about if you knew of any
message boards that cover the same topics talked about here?
I’d really love to be a part of community where I can get advice from
other experienced individuals that share the same interest.
If you have any suggestions, please let me know.
Bless you!
Thank you for the good writeup. It in fact was a
amusement account it. Look advanced to far added agreeable from you!
By the way, how could we communicate?
Saya tidak sering berkomentar tetapi saya harus mengakui terima kasih untuk posting yang hebat ini : D.
I’m gone to convey my little brother, that he should also visit this weblog on regular
basis to take updated from latest news update.
Greetings from Carolina! I’m bored at work so I decided to check out your blog
on my iphone during lunch break. I enjoy the info you provide here and can’t wait to take a look when I get
home. I’m surprised at how quick your blog loaded on my mobile ..
I’m not even using WIFI, just 3G .. Anyways, superb blog!
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima empat email dengan pesan yang identik. Apakah ada cara Anda bisa menghapus saya dari layanan itu? Terima kasih!
Hi! I’ve been following your blog for a long time
now and finally got the courage to go ahead and give you a shout out from New Caney Tx!
Just wanted to mention keep up the fantastic job!
Hi colleagues, good post and fastidious urging commented here, I am actually enjoying by these.
Just want to say your article is as astonishing. The
clearness in your post is simply cool and i can assume you’re
an expert on this subject. Well with your permission let me to grab your RSS feed to keep updated with forthcoming post.
Thanks a million and please continue the rewarding work.
Ini adalah topik yang sangat penting di hati saya, salam, tapi di manakah informasi kontak Anda?
Thanks for finally writing about > Balancing the Scales:
Patient Load vs. Care Quality in Diabetes – D-Coded Diabetes
Research < Loved it!
Spot on with this write-up, I absolutely feel this amazing site
needs far more attention. I’ll probably be back again to read more, thanks for the information!
I’ve got to be honest, but the day I stepped into the backend of the sports world, everything I thought I knew about
modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire industry
had turned into this fragile high-tech ecosystem, I honestly felt
overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — live match stats.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned
how a data leak nearly destroyed a negotiation. That was the moment I understood how
thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just
websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds
globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially
the kind you see described in official breakdowns — it opened
my eyes. If anyone wants to understand how this level of
protection actually works, they can always look it up
directly from the source. The full explanations are there, and they’re
honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury histories — things that could ruin a
season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking
access, reviewing logs, forcing documentation. I used to think compliance was boring,
but now I understand that without it, the
entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this
whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same way again.
We stumbled over here coming from a different page and thought I might check things out.
I like what I see so now i am following you. Look forward to going over your web page yet again. https://cryptoboss-rcn.top/
Saya secara tidak sengaja menemukan situs Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan kerja yang bagus.
Heya i am for the primary time here. I came across this board and I in finding It truly helpful & it helped me out a lot.
I’m hoping to offer something back and aid others such as you helped me.
Я періодично заходжу в 1xBet вже
більше року і можу сказати, що враження загалом позитивні.
Процес верифікації не затягнули,
без довгого очікування. Подобається, що є ліцензія, тому є більше довіри.
Вивід на карту приходить швидко — зазвичай протягом доби.
Fantastic article. You explained every aspect of Plinko ball game in a
easy-to-follow way. This gave me new insights.|
I read your article and found it very helpful. It’s great to
find well-written guides!
Have you ever considered about adding a little bit more than just your articles?
I mean, what you say is important and everything.
But just imagine if you added some great photos or videos to
give your posts more, “pop”! Your content is excellent but with images and video clips, this blog could certainly be one
of the most beneficial in its niche. Very good blog!
WOW just what I was looking for. Came here by searching for 구글계정판매
Saved as a favorite, I like your blog!
Thanks for sharing such a nice thought, piece of writing
is pleasant, thats why i have read it fully
Sesudah saya awalnya berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang tiap kali sebuah komentar ditambahkan saya menerima empat email dengan komentar yang sama. Apakah ada jalan Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Hello, i read your blog occasionally and i own a similar one
and i was just curious if you get a lot of spam responses?
If so how do you protect against it, any plugin or
anything you can advise? I get so much lately it’s
driving me crazy so any support is very much appreciated.
Hey! I know this is kind of off topic but I was wondering which blog platform are you using for this website?
I’m getting tired of WordPress because I’ve had issues with hackers
and I’m looking at alternatives for another platform.
I would be fantastic if you could point me in the direction of a good platform.
Postingan yang sangat baik. Ini benar-benar ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
I didn’t see it coming at all, but the day I stepped into
the backend of the sports world, everything I thought I
knew about modern sports completely collapsed.
I always believed the danger was only on the field, but when I saw how the entire industry had
turned into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore.
They were attacking everything — contract files.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire
club. That was the moment I understood how thin the line really is between order and total digital
disaster.
But the real shock came when I looked deeper into
betting platforms.
I swear, I always thought they were just websites.
But no.
They are insane real-time data engines. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind
you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look
it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of tactical plans — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had become
a daily threat.
Compliance teams were everywhere too — checking access,
reviewing logs, forcing documentation. I used to think compliance was boring, but now I understand that without it, the entire digital side
of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only
thing holding this whole world together.
And honestly, after everything I saw, I can say the
system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how
these structures really work, I’d definitely suggest getting
more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll
never look at sports or betting the same way again.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika komentar baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang identik. Apakah ada metode Anda mungkin bisa mengeluarkan saya dari layanan itu? Terima kasih!
Hey There. I found your weblog using msn. This is a really smartly
written article. I’ll make sure to bookmark it and come back to learn more of your helpful information. Thank
you for the post. I’ll definitely return.
I am not sure where you’re getting your information, but great topic.
I needs to spend some time learning much more or understanding more.
Thanks for wonderful info I was looking for this info
for my mission.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah tanggapan ditambahkan saya menerima 4 email dengan pesan yang sama. Apakah ada sarana Anda akan bisa mengeluarkan saya dari layanan itu? Terima kasih!
Saya tanpa henti memikirkan hal ini, terima kasih telah mengunggah.
Do you have a spam problem on this blog; I also am a blogger,
and I was wanting to know your situation; we have developed some nice practices and
we are looking to exchange methods with other folks, be sure to shoot
me an email if interested.
I’m not sure why but this blog is loading extremely slow
for me. Is anyone else having this problem or is it a issue on my end?
I’ll check back later on and see if the problem still exists.
Hello to every body, it’s my first go to see of this blog; this web site includes remarkable and in fact fine
stuff in support of visitors.
Postingan yang bagus. Ini jelas ditulis dengan baik dan mudah dimengerti. Terima kasih telah berbagi pengetahuan ini.
Artikel yang fantastis. Saya benar-benar menikmati gaya Anda menjelaskan gagasan-gagasan ini. Teruskan pekerjaan yang hebat!
Ini benar-benar menjawab masalah saya, terima kasih!
I know this if off topic but I’m looking into starting my own blog and was
wondering what all is required to get setup? I’m assuming having a blog like yours would cost
a pretty penny? I’m not very web savvy so I’m not
100% certain. Any suggestions or advice would be greatly appreciated.
Many thanks
Write more, thats all I have to say. Literally, it seems as though you relied
on the video to make your point. You obviously know what youre talking about,
why throw away your intelligence on just posting videos
to your weblog when you could be giving us something enlightening to
read?
Anda dapat jelas melihat keterampilan Anda dalam karya yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Senantiasa ikuti hati Anda.
When I originally commented I clicked the “Notify me when new comments are added” checkbox
and now each time a comment is added I get three e-mails with the same comment.
Is there any way you can remove me from that service?
Many thanks!
Your comment is awaiting moderation.
https://www.youtube.com/@seotobibbl5555com
https://x.com/seotobibbl5555
https://tooter.in/seotobibbl5555com
https://wakelet.com/@seotobibbl5555com
https://safechat.com/u/seo.tobi
https://gravatar.com/seotobibbl5555com
https://www.blogger.com/profile/11874850784329490455
https://www.mymeetbook.com/seotobibbl5555com
https://www.pinterest.com/seotobibbl5555com/
https://demo.wowonder.com/seotobibbl5555com
https://myspace.com/seotobibbl5555com/
https://500px.com/p/seotobibbl5555com
https://www.instapaper.com/p/seotobibbl5555
https://band.us/@seotobibbl5555com
https://protocol.ooo/ja/users/seo-tobi
https://www.reddit.com/user/seotobibbl5555com/
https://audiomack.com/seotobibbl5555com
https://draft.blogger.com/profile/11874850784329490455
https://hackaday.io/seotobibbl5555com
https://fyers.in/community/member/RugItegytm
https://vocal.media/authors/seo-tobi
https://leetcode.com/u/seotobibbl5555com/
https://www.halaltrip.com/user/profile/322490/seotobibbl5555c/
https://www.jetphotos.com/photographer/786448
https://medibang.com/author/27886333/
https://liulo.fm/seotobibbl5555com
https://www.blockdit.com/seotobibbl5555com
https://portfolium.com/seotobibbl5555com
https://www.twitch.tv/seotobibbl5555com/about
https://profile.hatena.ne.jp/seotobibbl5555com/
https://issuu.com/seotobibbl5555com
https://www.reverbnation.com/artist/seotobibbl5555com
https://www.myminifactory.com/users/seotobibbl5555com
https://www.investagrams.com/Profile/seotobibbl5555com
https://gifyu.com/seotobibbl5555
https://www.chordie.com/forum/profile.php?id=2475361
https://www.walkscore.com/people/126469136884/seotobibbl5555com
https://topsitenet.com/profile/seotobibbl5555com/1553758/
https://akniga.org/profile/1396335-seotobibbl5555com/
https://disqus.com/by/seotobi/about/
https://jobs.suncommunitynews.com/profiles/7952883-seo-tobi
https://www.speedrun.com/users/seotobibbl5555com
https://www.fanart-central.net/user/seotobibbl5555com/profile
https://www.aicrowd.com/participants/seotobibbl5555com
https://old.bitchute.com/channel/WJmQXlJbHoF3/
https://pbase.com/seotobibbl5555com/image/176146401
https://hub.docker.com/u/seotobibbl5555com
https://spiderum.com/nguoi-dung/seotobibbl5555com
https://www.gta5-mods.com/users/seotobibbl5555com
https://heylink.me/seotobibbl5555com/
https://pixabay.com/users/54844385/
https://www.nicovideo.jp/user/143419526
https://3dwarehouse.sketchup.com/by/seotobibbl5555com
https://robertsspaceindustries.com/en/citizens/seotobibbl5555com
https://bit.ly/m/seotobibbl5555com
https://allmylinks.com/seotobibbl5555com
https://joy.bio/seotobibbl5555com
https://connect.garmin.com/app/profile/501ce2a0-b51f-43eb-8da6-90896ba32feb
https://b.hatena.ne.jp/seotobibbl5555com/bookmark
https://www.chichi-pui.com/users/seotobibbl5555c/
https://unityroom.com/users/az3bj95w7iuxrsvl82yc
https://routinehub.co/user/seotobibbl5555com
https://pxhere.com/en/photographer/4932842
https://teletype.in/@seotobibbl5555com
https://www.checkli.com/seotobibbl5555com
https://gitee.com/seotobibbl5555com
https://www.nintendo-master.com/profil/seotobibbl5555com
https://freeimage.host/seotobibbl5555
https://diigo.com/01218gj
https://motion-gallery.net/users/918656
https://linkin.bio/seotobibbl5555com/
https://biomolecula.ru/authors/127751
https://talk.plesk.com/members/seotobibbl5555com.490888/#about
https://www.callupcontact.com/b/businessprofile/SEO_TOBI/9990248
https://www.growkudos.com/profile/seo_tobi
https://blender.community/seotobi/
https://doselect.com/@848d5aa766a6e544a51c15838
https://matkafasi.com/user/seotobibbl5555com
https://allmyfaves.com/seotobibbl5555com/
https://muare.vn/shop/seotobibbl5555com/895693
https://doodleordie.com/profile/seotobibbl5555com
https://web.ggather.com/seotobibbl5555com
https://musikersuche.musicstore.de/profil/seotobibbl5555com/
https://www.intensedebate.com/people/seotobibbl55551
https://lookingforclan.com/user/seotobibbl5555com
https://forum.dmec.vn/index.php?members/seotobibbl5555com.176662/
https://igli.me/seotobibbl5555com
https://www.fantasyplanet.cz/diskuzni-fora/users/seotobibbl5555com/
http://delphi.larsbo.org/user/seotobibbl5555com
https://www.aseeralkotb.com/en/profiles/seotobibbl5555com
https://timdaily.vn/members/setobibbl.128794/#about
https://app.readthedocs.org/profiles/seotobibbl5555com/
https://www.dibiz.com/tuynhsynhpoet
https://iszene.com/user-337523.html
https://www.theyeshivaworld.com/coffeeroom/users/seotobibbl5555com
https://desksnear.me/users/seo-tobi
https://www.roton.com/forums/users/tuynhsynhpoet/
http://www.biblesupport.com/user/814233-seotobibbl5555com/
https://golosknig.com/profile/seotobibbl5555com/
https://forum.m5stack.com/user/seotobibbl5555com
https://wallhaven.cc/user/seotobibbl5555com
https://chothai24h.com/members/29379-seotobib.html
https://www.bitchute.com/channel/WJmQXlJbHoF3
https://bandori.party/user/522588/seotobibbl5555com/
https://community.m5stack.com/user/seotobibbl5555com
https://schoolido.lu/user/seotobibbl5555com/
https://awan.pro/forum/user/140553/
https://fortunetelleroracle.com/profile/seotobibbl5555com
https://fabble.cc/seotobibbl5555com
https://suckhoetoday.com/members/36114-seotobib.html
https://community.cisco.com/t5/user/viewprofilepage/user-id/1978764
https://pad.stuve.de/s/oAjC5q7Dq
https://kr.pinterest.com/seotobibbl5555com/
https://pt.gravatar.com/seotobibbl5555com
https://th.gravatar.com/seotobibbl5555com
https://www.sythe.org/members/seotobibbl5555com.2016088/
https://f319.com/members/seotobibbl5555com.1071963/
https://cuadepviet.com/members/12460-seotobib.html
https://about.me/seotobibbl5555com
https://www.canadavisa.com/canada-immigration-discussion-board/members/seotobibbl5555com.1343404/#about
https://wefunder.com/seotobibbl5555com
https://transfur.com/Users/seotobibbl5555com
https://xtremepape.rs/members/seotobibbl5555com.647263/#about
https://gachmienbac.com/members/12019-seotobib.html
https://myanimelist.net/profile/seotobibbl5555
https://website.informer.com/bbl5555.com
https://beacons.ai/seotobibbl5555com
https://en.islcollective.com/portfolio/12857324
https://www.xosothantai.com/members/seotobibbl5555com.599408/
https://velog.io/@seotobibbl5555/about
https://violet.vn/user/show/id/15242068
https://xaydunghanoimoi.net/members/26368-seotobib.html
https://iplogger.org/logger/LL2W5petLjmN/
https://mez.ink/seotobibbl5555com
https://seotobibbl5555com.stck.me/
https://digiphoto.techbang.com/users/seotobibbl5555com
https://maychetao.com/members/20138-seotobib.html
https://inkbunny.net/seotobibbl5555com
https://www.launchgood.com/user/newprofile#!/user-profile/profile/seo.tobi
https://www.techbang.com/users/seotobibbl5555com
https://code.antopie.org/seotobibbl5555com
https://apptuts.bio/seo-tobi-249635
https://dialog.eslov.se/profiles/seotobibbl5555com/activity
https://www.storenvy.com/seotobibbl5555c
https://diendan.bftvietnam.com/members/20494-seotobibbl5555com.html
https://egl.circlly.com/users/seotobibbl5555com
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=291386
https://acomics.ru/-seotobibbl5555com
https://www.criminalelement.com/members/seotobibbl5555com/profile/
https://hanson.net/users/seotobibbl5555com
https://diendan.cuabenhvien.com/members/18916-seotobib.html
https://writexo.com/share/0d2771156ee9
https://expatguidekorea.com/profile/seotobibbl5555com/
https://www.heavyironjobs.com/profiles/7955219-seo-tobi
https://pad.degrowth.net/s/hbMnpiPbM
https://www.syncdocs.com/forums/profile/seotobibbl5555com
https://www.rehashclothes.com/seotobibbl5555com
http://fort-raevskiy.ru/community/profile/seotobibbl5555com/
https://forum.skullgirlsmobile.com/members/seotobibbl5555com.198381/#about
https://jobs.landscapeindustrycareers.org/profiles/7955228-seo-tobi
https://phatwalletforums.com/user/seotobibbl5555
https://forums.galciv4.com/user/7641285
https://kyourc.com/seotobibbl5555com/
https://song.link/seotobibbl5555com
https://idol.st/user/137820/seotobibbl5555com/
https://www.valinor.com.br/forum/usuario/seotobibbl5555com.141719/#about
https://tulieu.violet.vn/user/show/id/15242068
https://www.bmwpower.lv/user.php?u=seotobibbl5555com
https://jobs.windomnews.com/profiles/7955244-seo-tobi
https://forums.stardock.com/user/7641285
https://zerosuicidetraining.edc.org/user/profile.php?id=542691
https://beteiligung.amt-huettener-berge.de/profile/seotobibbl5555com/
https://beteiligung.hafencity.com/profile/seotobibbl5555com/
https://adhocracy.plus/profile/seotobibbl5555com/
https://hoaxbuster.com/redacteur/seotobibbl5555com
https://beteiligung.stadtlindau.de/profile/seotobibbl5555com/
https://beteiligung.tengen.de/profile/seotobibbl5555com/
https://jobs.westerncity.com/profiles/7955252-seo-tobi
https://www.thetriumphforum.com/members/seotobibbl5555com.57056/
https://mycableengineering.com/activity-feed/userId/29676
https://album.link/seotobibbl5555com
https://portfolium.com.au/seotobibbl5555com
https://forums.galciv3.com/user/7641285
https://www.chaloke.com/forums/users/seotobibbl5555com/
https://justpaste.me/wsgV5
https://forums.sinsofasolarempire2.com/user/7641285
https://buckeyescoop.com/community/members/slate-vibrant-pixie.57957/#about
https://toirscript.com/user/seotobibbl5555
https://forum.pabbly.com/members/seotobibbl5555com.99253/#about
http://forum.cncprovn.com/members/415735-seotobibbl5555com
https://marketplace.trinidadweddings.com/author/seotobibbl5555com/
https://forum.aigato.vn/user/seotobibbl5555
https://rapidapi.com/user/seotobibbl5555com
https://www.skool.com/@seo-tobi-6995
https://learningapps.org/watch?v=pz9wp9shn26
https://www.catapulta.me/users/seotobibbl5555com
https://www.invelos.com/UserProfile.aspx?alias=seotobibbl5555com
https://www.video-bookmark.com/bookmark/7059881/seo-tobi/
https://gitlab.vuhdo.io/seotobibbl5555com
https://aniworld.to/user/profil/seotobibbl5555com
https://kktix.com/user/8456106
https://poipiku.com/13259798/
https://www.rwaq.org/users/seotobibbl5555com
https://www.fitday.com/fitness/forums/members/seotobibbl5555com.html
https://www.fundable.com/seo-tobi
https://es.gravatar.com/seotobibbl5555com
https://de.gravatar.com/seotobibbl5555com
https://cy.gravatar.com/seotobibbl5555com
https://hukukevi.net/user/seotobibbl5555com
This is a very informative post about online casinos and betting platforms.
I especially liked how it explains the importance of choosing a secure site before signing up.
Many players often ask where they can find reliable gaming platforms with fair odds and smooth payouts.
From what I’ve seen, checking platforms like vn22vip helps users compare features,
bonuses, and overall experience.
Thanks for sharing these insights — they’re helpful
for both beginners and experienced bettors.
Beberapa hari lalu, saat saya sedang bekerja, sepupu saya mengambil iphone saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Wow! In the end I got a blog from where I know how to in fact take helpful facts concerning my study and
knowledge.
Awesome! Its truly awesome post, I have got much clear idea on the topic
of from this post.
Hi everyone, it’s my first pay a quick visit at this website,
and article is genuinely fruitful in favor of me,
keep up posting these posts.
Saya sangat menghargai waktu yang Anda curahkan untuk menyusun artikel ini. Konten yang berguna. Terima kasih banyak!
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 25 kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini benar-benar di luar topik tetapi saya harus membagikannya kepada seseorang!
Postingan yang fantastis! Saya sangat menghargai cara Anda menguraikan semuanya dengan mudah dipahami. Teruskan kerja yang bagus!
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I
get four emails with the same comment. Is there any way you can remove
me from that service? Thanks a lot!
Your comment is awaiting moderation.
https://www.facebook.com/f1688wine/
https://www.youtube.com/@f1688wine
https://twitter.com/f1688wine
https://tooter.in/f1688wine
https://wakelet.com/@f1688wine
https://safechat.com/u/f1688wine
https://gravatar.com/f1688wine
https://www.blogger.com/profile/01538417061822060123
https://www.mymeetbook.com/f1688wine
https://www.pinterest.com/f1688wine/
https://community.wongcw.com/f1688wine
https://demo.wowonder.com/f1688wine
https://shareyoursocial.com/f1688wine
https://gitlab.aicrowd.com/f1688wine
https://myspace.com/f1688wine
https://500px.com/p/f1688wine
https://www.instapaper.com/p/f1688wine
https://magic.ly/f1688wine
https://www.band.us/@f1688wine
https://protocol.ooo/ja/users/f1688wine
https://sketchfab.com/f1688wine
https://www.reddit.com/user/f1688wine/
https://audiomack.com/f1688wine
https://hackaday.io/f1688wine
https://fyers.in/community/member/R2dRNcLJAf
https://draft.blogger.com/profile/01538417061822060123
https://vocal.media/authors/f1688wine
https://leetcode.com/u/f1688wine/
https://swag.live/user/699da28f0054ffa6505d3849
https://www.halaltrip.com/user/profile/320835/f1688wine/
https://www.jetphotos.com/photographer/782727
https://medibang.com/author/27856663/
https://liulo.fm/f1688wine
https://opensea.io/f1688wine
https://www.blockdit.com/f1688wine
https://portfolium.com/f1688wine
https://groups.google.com/g/f1688wine
https://www.twitch.tv/f1688wine/about
https://profile.hatena.ne.jp/f1688wine/
https://issuu.com/f1688wine
https://www.reverbnation.com/artist/f1688wine
https://www.myminifactory.com/users/f1688wine
https://www.investagrams.com/Profile/f1688wine
https://gifyu.com/f1688wine
https://www.chordie.com/forum/profile.php?id=2473037
https://www.walkscore.com/people/230764872611/f1688wine
https://topsitenet.com/profile/f1688wine/1551986/
https://akniga.org/profile/1394852-f1688wine/
https://f1688wine.bandcamp.com/album/f168
https://disqus.com/by/f1688wine/about/
https://jobs.suncommunitynews.com/profiles/7935778-nha-cai-f168
https://www.speedrun.com/users/f1688wine
https://www.fanart-central.net/user/f1688wine/profile
https://slides.com/f1688wine
https://www.aicrowd.com/participants/f1688wine
https://old.bitchute.com/channel/eH2NAM3gOH2I/
https://pbase.com/f1688wine/inbox
https://hub.docker.com/u/f1688wine
https://spiderum.com/nguoi-dung/f1688wine
https://zaidap.com/thong-tin-ca-nhan-u106119.htm
https://www.gta5-mods.com/users/f1688wine
https://heylink.me/f1688wine/
https://pixabay.com/users/54780623/
https://www.nicovideo.jp/user/143373455
https://www.jigsawplanet.com/f1688wine
https://3dwarehouse.sketchup.com/by/f1688wine
https://robertsspaceindustries.com/en/citizens/f1688wine
https://bit.ly/m/f1688wine
https://allmylinks.com/f1688wine
https://joy.link/f1688wine
https://connect.garmin.com/app/profile/669db245-6f63-4acd-a485-09242d71ab19
https://b.hatena.ne.jp/f1688wine/bookmark
https://www.chichi-pui.com/users/f1688wine/
https://www.openrec.tv/user/f1688wine/about
https://unityroom.com/users/f1688wine
https://routinehub.co/user/f1688wine
https://pxhere.com/en/photographer-me/4927958
https://teletype.in/@f1688wine
https://www.checkli.com/f1688wine
https://www.fuelly.com/driver/f1688wine
https://www.nintendo-master.com/profil/f1688wine
https://freeimage.host/f1688wine
https://www.diigo.com/profile/f1688wine
https://fontstruct.com/fontstructions/show/2831969/f168-10
https://mecabricks.com/en/user/fwine
https://motion-gallery.net/users/916467
https://linkin.bio/f1688wine/
https://forums.daybreakgames.com/dcuo/index.php?members/f1688wine0.423452/
https://www.logic-sunrise.com/forums/user/190154-f1688wine/
https://biomolecula.ru/authors/126836
https://talk.plesk.com/members/f1wine.489861/#about
https://www.callupcontact.com/b/businessprofile/f1688wine/9984227
https://www.growkudos.com/profile/Nh%C3%A0_c%C3%A1i_F168_7
https://blender.community/f1688wine/
https://doselect.com/@852b3a8eda5bb1d36794d28e2
https://sciter.com/forums/users/f1688wine/
https://matkafasi.com/user/f1688wine
https://allmyfaves.com/f1688wine
https://www.notebook.ai/@f1688wine
https://www.abclinuxu.cz/lide/f1688wine
https://dumagueteinfo.com/author/f1688wine/
https://muare.vn/shop/f1688wine/895223
https://www.vnbadminton.com/members/f1688wine.65493/
https://web.ggather.com/f1688wine
https://musikersuche.musicstore.de/profil/f1688wine/
https://www.intensedebate.com/people/f1688wine0
https://lookingforclan.com/user/f1688wine
https://forum.dmec.vn/index.php?members/f1688wine.175812/
https://igli.me/f1688wine
https://www.fantasyplanet.cz/diskuzni-fora/users/f1688wine/
https://duyendangaodai.net/members/30147-f1688win.html
https://freestyler.ws/user/632184/f1688wine
http://delphi.larsbo.org/user/f1688wine
https://www.aseeralkotb.com/en/profiles/f1688wine
https://timdaily.vn/members/f1688wine.128472/#about
https://app.readthedocs.org/profiles/f1688wine/
https://www.dibiz.com/eduardoladys759
https://iszene.com/user-336865.html
https://www.theyeshivaworld.com/coffeeroom/users/f1688wine
https://desksnear.me/users/f1688wine
https://bachhoadep.com/members/22155-f1688win.html
https://www.itchyforum.com/en/member.php?379861-f1688wine
https://www.roton.com/forums/users/eduardoladys759/
https://able2know.org/user/f1688wine/
http://www.biblesupport.com/user/812091-f1688wine/
https://golosknig.com/profile/f1688wine/
https://www.anibookmark.com/user/f1688wine.html
https://www.inventoridigiochi.it/membri/f1688wine/profile/
https://forum.m5stack.com/user/f1688wine/
https://wallhaven.cc/user/f1688wine
https://chothai24h.com/members/29298-f1688wi.html
https://imageevent.com/f1688wine/f1688wine
https://www.bitchute.com/channel/eH2NAM3gOH2I
https://bandori.party/user/501562/f1688wine/
https://community.m5stack.com/user/f1688wine
https://schoolido.lu/user/f1688wine/
https://awan.pro/forum/user/139383/
https://jakle.sakura.ne.jp/pukiwiki/?f1688wine
https://fortunetelleroracle.com/profile/f1688wine
https://fabble.cc/f1688wine
https://suckhoetoday.com/members/36029-f1688win.html
https://pad.geolab.space/s/Fq8KwwSMe
https://affariat.com/user/profile/173442
https://pad.stuve.de/s/gssLhJ79M
https://kr.pinterest.com/f1688wine/
https://pt.gravatar.com/f1688wine
https://th.gravatar.com/f1688wine
https://www.sythe.org/members/f1688wine.2014380/
https://f319.com/members/f1688wine.1070307/
https://about.me/f1688wine
https://cuadepviet.com/members/12410-f1688win.html
https://booklog.jp/users/f1688wine/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/f1688wine.1342695/#about
https://www.equinenow.com/farm/f1688wine.htm
https://www.gaiaonline.com/profiles/f1688wine/50649097/
https://wefunder.com/f1688wine
https://potofu.me/f1688wine
https://transfur.com/Users/f1688wine
https://xtremepape.rs/members/f1688wine.645901/#about
https://github.com/f1688wine
https://gachmienbac.com/members/11955-f1688win.html
https://myanimelist.net/profile/f1688wine
https://qna.habr.com/user/f1688wine
https://website.informer.com/f1688.wine
https://lightroom.adobe.com/u/f1688wine
https://beacons.ai/f1688wine
https://en.islcollective.com/portfolio/12853643
https://www.xosothantai.com/members/f1688wine.598873/
https://velog.io/@f1688wine/about
https://violet.vn/user/show/id/15240151
https://xaydunghanoimoi.net/members/26279-f1688win.html
https://iplogger.com/2sn1B4
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3904268
https://mez.ink/f1688wine
https://f1688wine.stck.me/profile
https://notionpress.com/author/1476733
https://www.edna.cz/uzivatele/f1688wine/
https://digiphoto.techbang.com/users/f1688wine
https://leakedmodels.com/forum/members/f1688wine.692275/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1046477
https://maychetao.com/members/20073-f1688win.html
https://freeicons.io/profile/898410
https://onlinesequencer.net/forum/user-253000.html
https://inkbunny.net/f1688wine
https://www.japaaan.com/user/63227
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.f1683
https://code.antopie.org/f1688wine
https://beatsaver.com/playlists/1146213
https://apptuts.bio/f1688wine
https://dialog.eslov.se/profiles/f1688wine/activity
https://diendan.bftvietnam.com/members/20418-f1688wine.html
https://www.storenvy.com/f1688wine
https://participacion.cabildofuer.es/profiles/f1688wine/activity
https://forums.maxperformanceinc.com/forums/member.php?u=239761
https://egl.circlly.com/users/f1688wine
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290629
https://acomics.ru/-f1688wine
https://www.criminalelement.com/members/f1688wine/profile/
https://hanson.net/users/f1688wine
https://writexo.com/share/a980fb6b8ae6
https://diendan.cuabenhvien.com/members/18855-f1688win.html
https://expatguidekorea.com/profile/f1688wine/
https://www.laundrynation.com/community/profile/f1688wine/
https://www.heavyironjobs.com/profiles/7937275-nha-cai-f168
https://pad.degrowth.net/s/AZ5NGIzT3
https://giaoan.violet.vn/user/show/id/15240151
https://anh135689999.violet.vn/user/show/id/15240151
https://baigiang.violet.vn/user/show/id/15240151
https://dienbd.violet.vn/user/show/id/15240151
https://www.syncdocs.com/forums/profile/f1688wine
https://www.rehashclothes.com/f1688wine
http://fort-raevskiy.ru/community/profile/f1688wine/
https://forum.skullgirlsmobile.com/members/f1688wine.196955/#about
https://jobs.landscapeindustrycareers.org/profiles/7937281-nha-cai-f168
https://phatwalletforums.com/user/f1688wine
https://forums.galciv4.com/user/7639563
https://kyourc.com/f1688wine
https://song.link/f1688wine
https://idol.st/user/136214/f1688wine/
https://www.valinor.com.br/forum/usuario/f1688wine.141504/#about
https://tulieu.violet.vn/user/show/id/15240151
https://www.bmwpower.lv/user.php?u=f1688wine
https://gockhuat.net/member.php?u=431228
https://jobs.windomnews.com/profiles/7937312-nha-cai-f168
https://hoaxbuster.com/redacteur/f1688wine
https://www.givey.com/f1688wine
https://talkmarkets.com/profile/f1688wine
https://forums.stardock.com/user/7639563
https://zerosuicidetraining.edc.org/user/profile.php?id=541237
https://www.telix.pl/forums/users/f1688wine/
https://girlfriendvideos.com/members/f/f1688wine/
https://swaay.com/u/eduardoladys759/about/
https://beteiligung.amt-huettener-berge.de/profile/f1688wine/
https://joinentre.com/profile/f1688wine
https://jobs.westerncity.com/profiles/7937358-nha-cai-f168
https://www.thetriumphforum.com/members/f1688wine.56666/
https://gamblingtherapy.org/forum/users/f1688wine/
https://l2top.co/forum/members/f1688wine.157268/
http://www.askmap.net/location/7739206/vietnam/f168
https://graphcommons.com/graphs/ebd9e487-5dcc-4a72-8c9e-42861255e2b6
https://album.link/f1688wine
https://artist.link/f1688wine
https://pods.link/f1688wine
https://mylink.page/f1688wine
https://playlist.link/f1688wine
https://portfolium.com.au/f1688wine
https://forums.galciv3.com/user/7639563
https://galleria.emotionflow.com/175328/profile.html
https://www.myget.org/users/f1688wine
https://www.deafvideo.tv/vlogger/f1688wine
https://www.chaloke.com/forums/users/f1688wine/
https://beteiligung.tengen.de/profile/f1688wine/
https://beteiligung.hafencity.com/profile/f1688wine/
https://adhocracy.plus/profile/f1688wine/
https://www.hobowars.com/game/linker.php?url=https://f1688.wine/
https://beteiligung.stadtlindau.de/profile/f1688wine/
https://app.brancher.ai/user/9KiqKP3d2QRZ
https://justpaste.me/v7Eq2
https://aetherlink.app/users/7432291596114362368
https://forums.sinsofasolarempire2.com/user/7639563
https://www.empregosaude.pt/en/author/f1688wine/
https://confengine.com/user/f1688wine
https://slideslive.com/f1688wine?tab=about
https://buckeyescoop.com/community/members/f1688wine.57633/#about
https://forums.ashesofthesingularity.com/user/7639563
http://www.ssnote.net/users/f1688wine
https://forum.aceinna.com/user/f1688wine
https://toirscript.com/user/f1688wine
https://forum.pabbly.com/members/f1688wine.98176/#about
http://forum.cncprovn.com/members/415010-f1688wine
https://marketplace.trinidadweddings.com/author/f1688wine/
https://ncnews.co/profile/f1688wine
https://dreevoo.com/profile_info.php?pid=1179717
https://forum.aigato.vn/user/f1688wine
https://amaz0ns.com/forums/users/f1688wine/
https://rapidapi.com/user/f1688wine
https://www.skool.com/@nha-cai-f-9529
https://hedge.fachschaft.informatik.uni-kl.de/s/h4tm3UL0o
https://learningapps.org/watch?v=p7jebpgb226
https://coub.com/f1688wine
https://www.giveawayoftheday.com/forums/profile/1666085
http://onlineboxing.net/jforum/user/profile/430359.page
https://www.catapulta.me/users/f1688wine
https://www.invelos.com/UserProfile.aspx?Alias=f1688wine
https://www.video-bookmark.com/bookmark/7054872/f1688wine/
https://wibki.com/f1688wine
https://twitback.com/f1688wine
https://krachelart.com/UserProfile/tabid/43/userId/1334305/Default.aspx
https://gitlab.vuhdo.io/f1688wine
https://www.11secondclub.com/users/profile/1699899
https://aniworld.to/user/profil/f1688wine
https://s.id/f1688wine
https://worldvectorlogo.com/profile/f1688wine
https://es.gravatar.com/f1688wine
https://de.gravatar.com/f1688wine
https://cy.gravatar.com/f1688wine
https://cs.gravatar.com/f1688wine
https://cn.gravatar.com/f1688wine
https://zh-tw.gravatar.com/f1688wine
https://sv.gravatar.com/f1688wine
https://po.gravatar.com/f1688wine
https://oc.gravatar.com/f1688wine
https://ko.gravatar.com/f1688wine
https://kktix.com/user/8445633
https://www.passes.com/f1688wine
https://poipiku.com/13233825/
https://uiverse.io/profile/f1688wine_2980
https://www.rwaq.org/users/f1688wine
https://cofacts.tw/user/f1688wine
https://www.fitday.com/fitness/forums/members/f1688wine.html
https://www.fundable.com/nha-cai-f168-28
https://vcook.jp/users/75138
https://www.grepmed.com/f1688wine
https://classificados.acheiusa.com/profile/cUZLYytVb1h4QVJwelJTaEwyenRLWEVVZ1ZnRXd5VmYvMStBMW51YlNCYz0=
https://espritgames.com/members/50159265/
https://cgmood.com/f1688wine
https://www.haikudeck.com/presentations/f1688wine
https://www.efunda.com/members/people/show_people.cfm?Usr=f1688wine
https://paidforarticles.in/author/f1688wine
https://backloggery.com/f1688wine
https://www.sociomix.com/u/f1688wine/
https://raovat.nhadat.vn/members/f1688wine-289248.html
https://www.moshpyt.com/user/f1688wine
https://www.koi-s.id/member.php?331617-f1688wine
https://pumpyoursound.com/u/user/1585313
https://que.u.nosv.org/profile?user=f1688wine
https://hi-fi-forum.net/profile/1121525
https://secondstreet.ru/profile/f1688wine/
http://scenarch.com/userpages/28897
https://undrtone.com/f1688wine
https://marshallyin.com/members/f1688wine/
https://www.atozed.com/forums/user-68013.html
https://gravesales.com/author/f1688wine/
https://searchengines.bg/members/f1688wine.23468/#about
https://luvly.co/users/f1688wine
https://hukukevi.net/user/f1688wine
https://belgaumonline.com/profile/f1688wine/
https://savelist.co/profile/users/f1688wine
https://usdinstitute.com/forums/users/f1688wine/
https://hackerspace.govhack.org/profiles/f1688wine
https://www.apsense.com/user/f1688wine
https://zzb.bz/nA5GQf
https://boldomatic.com/view/writer/f1688wine
https://the7thcontinent.seriouspoulp.com/en/user/28321/f1688wine
https://www.themeqx.com/forums/users/f1688wine/
https://www.udrpsearch.com/user/f1688wine
https://www.inseparabile.it/forum/member.php?u=45742
http://newdigital-world.com/members/f1688wine.html
https://www.xen-factory.com/index.php?members/f1688wine.140319/#about
https://cointr.ee/f1688wine
https://king-wifi.win/wiki/User:F1688wine
https://forums.servethehome.com/index.php?members/f1688wine.226442/#about
https://jaga.link/f1688wine
https://b.io/f1688wine
http://www.truck-business.cz/profile/f1688wine/info.html
https://www.blackhatprotools.info/member.php?276856-f1688wine
https://activepages.com.au/profile/f1688wine
https://snippet.host/arwbqy
https://tudomuaban.com/chi-tiet-rao-vat/2827308/f168–nen-tang-giai-tri-truc-tuyen-voi-da-dang.html
https://lifeinsys.com/user/f1688wine
https://kaeuchi.jp/forums/users/f1688wine/
https://www.claimajob.com/profiles/7937901-nha-cai-f168
https://jali.me/f1688wine
https://protospielsouth.com/user/117393
https://theafricavoice.com/profile/f1688wine
http://palangshim.com/space-uid-4979188.html
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:BA1B2722699DA5670A495FA3@AdobeID
https://vi.gravatar.com/f1688wine
https://www.mixcloud.com/f1688wine/
https://www.designspiration.com/f1688wine/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185854
https://hub.vroid.com/en/users/124156186
https://biolinku.co/f1688wine
https://www.exchangle.com/f1688wine
https://forum.codeigniter.com/member.php?action=profile&uid=224031
https://bitspower.com/support/user/f1688wine
https://www.brownbook.net/business/54857016/f168
https://etextpad.com/bfxo4ge1vv
https://app.hellothematic.com/creator/profile/1123251
https://www.decidim.barcelona/profiles/f1688wine/activity
https://www.babelcube.com/user/nha-cai-f168-42
https://app.talkshoe.com/user/f1688wine
https://bioqoo.com/f1688wine
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223494
https://hulkshare.com/f1688wine
https://m.wibki.com/f1688wine
https://www.pageorama.com/?p=f1688wine
https://bandsworksconcerts.info/index.php?f1688wine
https://bbs.mikocon.com/home.php?mod=space&uid=281839
https://www.mikocon.com/home.php?mod=space&uid=281839
https://jerseyboysblog.com/forum/member.php?action=profile&uid=82198
https://www.quora.com/profile/F1688wine
https://qoolink.co/f1688wine
https://manylink.co/@f1688wine
https://www.freewebspace.net/forums/index.php?members/f1688wine.17031263/#about
https://forums.giantitp.com/member.php?369135-f1688wine
https://seomotionz.com/member.php?action=profile&uid=117044
https://anyflip.com/homepage/vqxun#About
https://www.akaqa.com/question/q19192653608-F168
https://londonchinese.com/home.php?mod=space&uid=614838&do=profile
https://copynotes.be/shift4me/forum/user-44452.html
https://menwiki.men/wiki/User:F1688wine
https://funsilo.date/wiki/User:F1688wine
https://jali.pro/f1688wine
https://scholar.google.com/citations?hl=en&user=8wTklUcAAAAJ
https://www.threadless.com/@f1688wine/activity
https://www.smitefire.com/profile/f1688wine-256767?profilepage
https://tabelog.com/rvwr/f1688wine/prof/
https://coolors.co/u/f1688wine
https://www.beamng.com/members/f1688wine.774039/
https://civitai.com/user/f1688wine
https://www.spigotmc.org/members/f1688wine.2485822/
https://boosty.to/f1688wine
https://camp-fire.jp/profile/f1688wine
https://feyenoord.supporters.nl/profiel/138738/f1688wine
https://www.pearltrees.com/f1688wine/item782788365
https://gesoten.com/profile/detail/12588649
https://rekonise.com/u/f1688wine
https://hashnode.com/@f1688wine
https://hoo.be/f1688wine
https://nhattao.com/members/user6922548.6922548/
https://maxforlive.com/profile/user/f1688wine?tab=about
https://3dtoday.ru/blogs/f1688wine
https://opencollective.com/f1688wine
https://pinshape.com/users/8915726-f1688wine
https://morguefile.com/creative/f1688wine
https://edabit.com/user/TmfYHoqnjbortzgnd
https://mathlog.info/users/PDYlldRxsUWLY9b8LBzMN2X7e1w1
https://securityheaders.com/?q=https://f1688.wine/
https://my.bio/f1688wine
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145217
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165696
https://md.darmstadt.ccc.de/s/EBoKsFbRZ_
https://sfx.thelazy.net/users/u/f1688wine/
https://forum.reallusion.com/Users/3283542/eduardoladys759
https://app.daily.dev/f1688wine
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=246841
https://slidehtml5.com/homepage/hevf#About
https://www.skypixel.com/users/djiuser-sb5forcsbmue
https://webanketa.com/forms/6mv34c1k64qp4e9g61j66dv6/
https://matters.town/@f1688wine
https://www.pdc.edu/?URL=https://f1688.wine/
https://ask.mallaky.com/?qa=user/f1688wine
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75738
https://drill.lovesick.jp/drilldata/index.php?f1688wine
https://www.depechemode.cz/?URL=https://f1688.wine/
https://sub4sub.net/forums/users/f1688wine/
https://www.slmath.org/people/98846
https://userstyles.world/user/f1688wine
https://goo.by/xbTjOM
https://bresdel.com/f1688wine
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12036
https://www.upcarta.com/profile/f1688wine
https://fora.babinet.cz/profile.php?id=114714
https://pledgeme.co.nz/profiles/318874/
https://www.shippingexplorer.net/en/user/f1688wine/256830
https://f1688wine.notepin.co/
https://pictureinbottle.com/r/f1688wine
https://forum.epicbrowser.com/profile.php?id=138774
http://www.dungdong.com/home.php?mod=space&uid=3322566
https://forum.herozerogame.com/index.php?/user/152019-f1688wine/
https://shhhnewcastleswingers.club/forums/users/f1688wine/
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=89975
https://electroswingthing.com/profile/f1688wine/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2389126
https://connect.gt/user/f1688wine
https://stuv.othr.de/pad/s/iyvwNvxz1
https://hacktivizm.org/members/fwine.56973/#about
https://forum.tkool.jp/index.php?members/f1688wine.97723/#about
https://hedgedoc.eclair.ec-lyon.fr/s/i3N-u-QR3
http://densan-knct.freehostia.com/wiki_/index.php?f1688wine
https://www.divephotoguide.com/user/f1688wine
https://www.weddingbee.com/members/f1688wine/
https://kumu.io/f1688wine/f1688wine
https://b.cari.com.my/home.php?mod=space&uid=3382927&do=profile
https://bioimagingcore.be/q2a/user/f1688wine
https://www.sunlitcentrekenya.co.ke/author/f1688wine/
https://hedgedoc.logilab.fr/s/1uVWDRavC
https://f1688wine.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/f1688wine/activity
https://www.rcuniverse.com/forum/members/f1688wine.html
https://www.huntingnet.com/forum/members/f1688wine.html
https://www.socialbookmarkssite.com/bookmark/6198973/f1688wine/
https://www.hogwartsishere.com/1817515/
https://vimeo.com/f1688wine
https://gitlab.com/f1688wine
https://www.symbaloo.com/mix/f168-cysh
https://www.bricklink.com/aboutMe.asp?u=fonewine
https://makeagif.com/user/f1688wine?ref=F5fZZt
https://www.lingvolive.com/en-us/profile/1ea35f61-eb45-43dd-9c7f-7c85663e7892/translations
https://zealy.io/cw/f1688wine/questboard/
https://mforum.cari.com.my/home.php?mod=space&uid=3382927&do=profile
https://mforum2.cari.com.my/home.php?mod=space&uid=3382927&do=profile
https://www.france-ioi.org/user/perso.php?sLogin=f1688wine
https://mt2.org/uyeler/f1688wine.35191/#about
https://participez.perigueux.fr/profiles/f1688wine/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424465
https://www.dotafire.com/profile/f1688wine-237220?profilepage
https://www.trackyserver.com/profile/231178
https://ixawiki.com/link.php?url=https://f1688.wine/
https://mforum3.cari.com.my/home.php?mod=space&uid=3382927&do=profile
https://www.pintradingdb.com/forum/member.php?action=profile&uid=134866
https://www.zubersoft.com/mobilesheets/forum/user-123984.html
https://www.plotterusati.it/user/f1688wine
https://forum.azeron.eu/index.php?members/f1688wine.29390/#about
https://tutorialslink.com/member/f1688wineundefined/90092
http://www.activewin.com/user.asp?Action=Read&UserIndex=4826537
http://www.jbt4.com/home.php?mod=space&uid=8666388
https://www.vid419.com/home.php?mod=space&uid=3475109
https://forum.ct8.pl/member.php?action=profile&uid=114738
https://devfolio.co/@f1688wine/readme-md
https://f1688wine.storeinfo.jp/pages/9615063/page_202602260010
https://linqto.me/n/f1688wine
https://www.mindomo.com/mindmap/2880d346fd024534b2f8bdf733df89ab
https://www.okaywan.com/home.php?mod=space&uid=771105
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:F1688wine
https://www.goodolcomics.com/blog/profile/f1688wine/
https://www.swap-bot.com/user:f1688wine
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=384114
http://techou.jp/index.php?f1688wine
https://paste.intergen.online/view/18ef0e07
https://epiphonetalk.com/members/f1688wine.91197/#about
https://web.trustexchange.com/company.php?q=f1688.wine
https://forums.megalith-games.com/member.php?action=profile&uid=1442085
http://tkdlab.com/wiki/index.php?f1688wine
https://www.managementpedia.com/members/f1688wine.1116539/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=601809
https://volleypedia.org/index.php?qa=user&qa_1=f1688wine
http://pcsq28.com/home.php?mod=space&uid=1759786
https://bbs.airav.cc/home.php?mod=space&uid=4414139
https://partecipa.poliste.com/profiles/f1688wine/activity
https://md.coredump.ch/s/51O0BBFKv
https://hker2uk.com/home.php?mod=space&uid=5341582
https://pad.funkwhale.audio/s/yDJBNVMbt
https://forum.dfwmas.org/index.php?members/f1688wine.194248/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=465278
https://hcgdietinfo.com/hcgdietforums/members/f1688wine/
https://aprenderfotografia.online/usuarios/f1688wine/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2303683&do=profile&from=space
http://galeria.farvista.net/member.php?action=showprofile&user_id=71169
https://tilengine.org/forum/member.php?action=profile&uid=158243
https://darkml.net/bbs/home.php?mod=space&uid=8193031&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6007462
https://hedgedoc.stusta.de/s/aT1uGigjl
https://pad.flipdot.org/s/mafPoYs9I
https://hack.allmende.io/s/mh9zAJKD3
https://pad.codefor.fr/s/dAX9eavwKV
https://md.opensourceecology.de/s/ZvIhOPLnA
https://md.ctdo.de/s/0JtMADPxqs
https://md.chaospott.de/s/WxDgXP3rFC
https://pad.fablab-siegen.de/s/wnKt52FjB
https://hackmd.hub.yt/s/sswwebrlq
https://md.swk-web.com/s/KWo5G60y1
https://md.klykken.com/s/J6NDDl7k8
https://hedgedoc.dezentrale.space/s/Y2_0g0AvE
https://docs.juze-cr.de/s/ETkYsnLFn
https://ar.gravatar.com/f1688wine
https://sensationaltheme.com/forums/users/f1688wine/
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301194
https://replit.com/@f1688wine
https://odesli.co/f1688wine
https://www.degreeforum.net/mybb/User-f1688wine
https://wandb.ai/profile/f1688wine
https://pad.darmstadt.social/s/lmDkD3Geap
https://divisionmidway.org/jobs/author/f1688wine/
https://bbcovenant.guildlaunch.com/users/blog/6737840/?mode=view&gid=97523
https://md.kif.rocks/s/1AoIRNJR91
https://youbiz.com/profile/f1688wine/
https://timeoftheworld.date/wiki/User:F1688wine
https://cameradb.review/wiki/User:F1688wine
https://historydb.date/wiki/User:F1688wine
https://www.wowonder.xyz/f1688wine
https://sciencemission.com/profile/f1688wine
https://referrallist.com/profile/f1688wine/
https://fakenews.win/wiki/User:F1688wine
http://jobboard.piasd.org/author/f1688wine/
https://www.wvhired.com/profiles/7940441-nha-cai-f168
https://kenhrao.com/members/f1688wine.115459/#about
http://jobs.emiogp.com/author/f1688wine/
https://www.canadavideocompanies.ca/forums/users/f1688wine/
https://hackmd.openmole.org/s/C4QqiuqWO
https://ismschools.com.au/forums/users/f1688wine/
https://md.chaosdorf.de/s/vQ3WNuqvAz
https://md.openbikesensor.org/s/U39tBousKs
https://doc.adminforge.de/s/zO2x2bOsEy
https://onlinevetjobs.com/author/f1688wine/
https://v.gd/NwJ0lN
https://sciencewiki.science/wiki/User:F1688wine
https://gl.gta5-mods.com/users/f1688wine
https://www.fruitpickingjobs.com.au/forums/users/f1688wine/
http://www.webclap.com/php/jump.php?url=https://f1688.wine/
https://xoops.ec-cube.net/userinfo.php?uid=342250
https://formulamasa.com/elearning/members/f1688wine/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1065921
https://quangcaoso.vn/f1688wine
https://tawk.to/f1688wine
https://chyoa.com/user/f1688wine
https://forum.flashphoner.com/members/f1688wine.41901/#about
https://www.royalroad.com/profile/917969
https://backloggd.com/u/f1688wine/
https://kenhsinhvien.vn/m/f1688wine.1163700/#about
https://form.jotform.com/260558107348056
https://forums.alliedmods.net/member.php?u=466788
https://aiforkids.in/qa/user/f1688wine1
https://www.warriorforum.com/members/f1688wine.html
https://community.jmp.com/t5/user/viewprofilepage/user-id/91040
https://digiex.net/members/f1688wine.139931/
https://www.corc.co.uk/forums/users/f1688wine/
https://smallseo.tools/website-checker/f1688.wine
https://cuwip.ucsd.edu/members/f1688wine/profile/
https://bwinglive.lighthouseapp.com/users/1992992
https://rush1989.rash.jp/pukiwiki/index.php?f1688wine
https://www.stylevore.com/user/f1688wine
https://bio.site/f1688wine
https://viblo.asia/u/f1688wine/contact
https://wikimapia.org/external_link?url=https://f1688.wine/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6252340
https://www.thesims3.com/myBlog.html?persona=f1688wine
https://telegra.ph/F168-02-26-2
https://runtrip.jp/users/743980
https://campsite.bio/f1688wine
https://hype4.academy/profile/f1688wine
https://reactormag.com/members/f1688wine/
https://brain-market.com/u/f1688wine
https://recipe.seikatsuclub.coop/profile.html?B_K_SID=0000093948
https://www.emailsherlock.com/hosts/f1688.wine/
https://www.promoteproject.com/user/f1688wine/
https://ikanakama.ink/users/339455
https://www.prosebox.net/book/101680/
https://ticketme.io/account/f1688wine
https://task.tw/users/TGAWEJG/freelancer
https://www.aipictors.com/users/f1688wine
https://log.concept2.com/profile/2859763
https://www.speedway-world.pl/forum/member.php?action=profile&uid=438417
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://f1688.wine/
http://forum.orangepi.org/home.php?mod=space&uid=6252340
https://redirect.camfrog.com/redirect/?url=https://f1688.wine/
https://diigo.com/011zz2f
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=76356
https://forum.honorboundgame.com/user-503708.html
https://elovebook.com/f1688wine
https://propterest.com.au/user/73283/f1688wine
https://www.fw-follow.com/forum/topic/91676/f168
https://www.jk-green.com/forum/topic/87990/f168
https://www.navacool.com/forum/topic/318834/f168
https://www.bonback.com/forum/topic/318835/f168
https://www.driedsquidathome.com/forum/topic/113849/f168
https://www.nongkhaempolice.com/forum/topic/87885/f168
https://www.bestloveweddingstudio.com/forum/topic/61969/f168
https://www.natthadon-sanengineering.com/forum/topic/78531/f168
https://www.rueanmaihom.net/forum/topic/77932/f168
https://www.ttlxshipping.com/forum/topic/318838/f168
https://www.cemkrete.com/forum/topic/134250/f168
http://worldchampmambo.com/UserProfile/tabid/42/userId/477396/Default.aspx
http://forum.modulebazaar.com/forums/user/f1688wine/
http://forum.bokser.org/user-1433657.html
https://gratisafhalen.be/author/f1688wine/
https://user.linkdata.org/user/f1688wine/work
https://calaos.fr/forum/member.php?action=profile&uid=18625
https://forum.hkcinema.ru/profile.php?section=about&id=72567
https://www.rcmx.net/userinfo.php?uid=13967
https://www.pathumratjotun.com/forum/topic/141289/f168
https://eilo.org/user/f1688wine
https://usabbs.org/home.php?mod=space&uid=85844
https://lqdoj.edu.vn/user/f1688wine
http://pastport.jp/user/f1688wine
https://paperjale.eus/user/f1688wine
http://byltz.com/home.php?mod=space&uid=478044
https://indiestorygeek.com/user/f1688wine
https://www.bandlab.com/f1688wine
https://www.livelib.ru/reader/f1688wine
https://en.wikivet.net/User:F1688wine
https://forum.issabel.org/u/f1688wine
https://www.siye.co.uk/siye/viewuser.php?uid=247838
https://ie.enrollbusiness.com/BusinessProfile/7732515/F168
https://mozillabd.science/wiki/User:F1688wine
https://www.casualgamerevolution.com/user/f1688wine
https://raredirectory.com/author/f1688wine-41703/
https://www.iglinks.io/eduardoladys759-eyw?preview=true
https://decidim.calafell.cat/profiles/f1688wine/activity
https://www.keepandshare.com/discuss4/36613/f168
http://bbs.medicalforum.cn/home.php?mod=space&uid=2084849
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://f1688.wine/
https://profiles.delphiforums.com/n/pfx/profile.aspx?webtag=dfpprofile000&userId=1891279432
https://hu.gta5-mods.com/users/f1688wine
https://gl.gravatar.com/f1688wine
https://fr.gravatar.com/f1688wine
https://fi.gravatar.com/f1688wine
https://fa.gravatar.com/f1688wine
https://ro.gta5-mods.com/users/f1688wine
https://ru.gta5-mods.com/users/f1688wine
https://sv.gta5-mods.com/users/f1688wine
https://vi.gta5-mods.com/users/f1688wine
https://zh.gta5-mods.com/users/f1688wine
https://www.backabuddy.co.za/campaign/f1688wine
https://uk.gta5-mods.com/users/f1688wine
https://sl.gta5-mods.com/users/f1688wine
https://at.pinterest.com/f1688wine/
https://www.easyhits4u.com/profile.cgi?login=f1688wine
https://in.pinterest.com/f1688wine/
https://doc.anagora.org/s/KtEChRFXT
https://profile.sampo.ru/f1688wine
https://mail.londonchinese.com/home.php?mod=space&uid=614838&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75545
https://www.bidhub.com/profiles/show/18811
http://www.muzikspace.com/profiledetails.aspx?profileid=128228
https://forums.starcontrol.com/user/7639563
https://forums.offworldgame.com/user/7639563
https://www.ekdarun.com/forum/topic/134622/f168
https://www.mobafire.com/profile/f1688wine-1235822?profilepage
https://fic.decidim.barcelona/profiles/f1688wine/activity
https://www.lectoreselectronicos.com/foro/member.php?21557-f1688wine
https://fanclove.jp/profile/va2v7nn3Jj
https://truckymods.io/user/462045
https://substack.com/@f1688wine
http://forum.vodobox.com/profile.php?id=63600
https://forums.sinsofasolarempire.com/user/7639563
https://forums.stardock.net/user/7639563
https://forum.findukhosting.com/index.php?action=profile;area=forumprofile;u=74995
https://fungiversum.de/pilz-forum/profile/f1688wine/
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=225790
https://www.cfd-online.com/Forums/members/f1688wine.html
https://sites.google.com/view/f1688wine/home
https://f1688wine.blogspot.com/2026/02/f168.html
https://www.diigo.com/item/note/bqzpy/8t34?k=1ac46d61eb430baf674afcd4f39da92f
https://www.notebook.ai/documents/2390699
https://f1688wine.mystrikingly.com/
https://f1688wine.webflow.io/
https://rant.li/f1688wine/f168-nen-tang-giai-tri-truc-tuyen-voi-da-dang
https://telegra.ph/F168–Nen-tang-giai-tri-truc-tuyen-voi-da-dang-02-26
https://f1688wine.mypixieset.com/
https://hedgedoc.stusta.de/s/5fAO_J2p4
https://scrapbox.io/f1688wine/F168
https://f1688wine.wordpress.com/
https://ofuse.me/f1688wine
https://f1688wine.gitbook.io/f1688wine-docs/
https://f1688wine.therestaurant.jp/pages/9615881/page_202602261305
https://f1688wine.theblog.me/pages/9615887/page_202602261306
https://www.notion.so/F168-313085a4efe9800b9b52d7d9529f18d5
https://zb3.org/f1688wine/f168-nen-tang-giai-tri-truc-tuyen-voi-da-dang
https://f1688wine.exblog.jp/34411537/
https://www.keepandshare.com/discuss4/36620/f168-nen-tang-giai-tri-truc-tuyen-voi-da-dang
https://xtiles.app/699fe4aff2b69741eb821904
https://telescope.ac/f1688wine/f1688wine
http://nhcif1681772057923.website3.me/
https://f1688wine.bcz.com/2026/02/26/f168-nen-tang-giai-tri-truc-tuyen-voi-da-dang/
https://www.myaspenridge.com/board/board_topic/3180173/7904276.htm
https://www.tai-ji.net/board/board_topic/4160148/7904274.htm
Your comment is awaiting moderation.
https://www.facebook.com/zoom555wincom/
https://www.youtube.com/@zoom555wincom
https://twitter.com/zoom555wincom
https://tooter.in/zoom555wincom
https://wakelet.com/@zoom555wincom
https://safechat.com/u/zoom555wincom
https://www.blogger.com/profile/12771622213121756821
https://www.mymeetbook.com/zoom555wincom
https://www.pinterest.com/zoom555wincom/
https://community.wongcw.com/zoom555wincom
https://demo.wowonder.com/zoom555wincom
https://shareyoursocial.com/zoom555wincom
https://gitlab.aicrowd.com/zoom555wincom
https://myspace.com/zoom555wincom
https://500px.com/p/zoom555wincom?view=photos
https://www.instapaper.com/p/zoom555wincom
https://magic.ly/zoom555wincom
https://www.band.us/@zoom555wincom
https://protocol.ooo/ja/users/555win-df034e18-2aa1-457d-b6d6-15407dc111c9
https://www.tumblr.com/zoom555wincom
https://www.reddit.com/user/zoomwincom/
https://audiomack.com/zoom555wincom
https://hackaday.io/zoom555wincom
https://fyers.in/community/member/bzlvUQLiP0
https://vocal.media/authors/555-win-hf14d50k8w
https://leetcode.com/u/zoom555wincom/
https://www.halaltrip.com/user/profile/321617/zoom555wincom/
https://www.jetphotos.com/photographer/784575
https://medibang.com/author/27869710/
https://liulo.fm/zoom555wincom
https://opensea.io/0x3f80fc0d3af02220160a82c55b71d3093ec5c9df
https://www.blockdit.com/zoom555wincom
https://portfolium.com/zoom555wincom
https://www.twitch.tv/zoom555wincom
https://profile.hatena.ne.jp/zoom555wincom/
https://issuu.com/zoom555wincom
https://www.behance.net/zoom555wincom
https://gravatar.com/zoom555wincom
https://www.reverbnation.com/artist/zoom555wincom
https://www.myminifactory.com/users/zoom555wincom
https://www.investagrams.com/Profile/zoom555wincom
https://gifyu.com/zoom555wincom
https://www.chordie.com/forum/profile.php?id=2474470
https://www.bitsdujour.com/profiles/gfxhgW
https://skitterphoto.com/photographers/2384202/zoom555wincom
https://www.longisland.com/profile/zoom555wincom
https://www.walkscore.com/people/208846999416/555win
https://akniga.org/profile/1395664-555win
https://zoom555wincom.bandcamp.com/album/zoom555wincom
https://jobs.suncommunitynews.com/profiles/7945606-nha-cai-555win
https://www.speedrun.com/users/zoom555wincom
https://www.fanart-central.net/user/zoom555wincom/profile
https://slides.com/zoom555wincom
https://www.aicrowd.com/participants/zoom555wincom
https://www.bitchute.com/channel/zH6hrReqt2LD
https://pbase.com/zoom555wincom/
https://hub.docker.com/u/zoom555wincom
https://spiderum.com/nguoi-dung/zoom555wincom
https://zaidap.com/thong-tin-ca-nhan-u106149.htm
https://www.gta5-mods.com/users/zoom555wincom
https://heylink.me/zoom555wincom/
https://pixabay.com/users/zoom555wincom-54818470/
https://www.nicovideo.jp/user/143395187
https://www.jigsawplanet.com/zoom555wincom
https://3dwarehouse.sketchup.com/by/zoom555wincom
https://robertsspaceindustries.com/en/citizens/zoom555wincom
https://bit.ly/m/zoom555wincom
https://joy.link/zoom555wincom
https://b.hatena.ne.jp/zoom555wincom/bookmark
https://b.hatena.ne.jp/zoom555wincom/bookmark
https://www.chichi-pui.com/users/zoom555wincom/
https://www.openrec.tv/user/zoom555wincom/about
https://unityroom.com/users/zoom555wincom
https://routinehub.co/user/zoom555wincom
https://pxhere.com/en/photographer-me/4930832
https://teletype.in/@zoom555wincom
https://www.checkli.com/zoom555wincom
https://gitee.com/zoom555wincom
https://www.fuelly.com/driver/zoom555wincom
https://www.nintendo-master.com/profil/zoom555wincom
https://freeimage.host/zoom555wincom
https://www.diigo.com/profile/zoom555wincom
https://fontstruct.com/fontstructions/show/2833565/555win-4
https://motion-gallery.net/users/917639
https://linkin.bio/zoom555wincom
https://forums.daybreakgames.com/dcuo/index.php?members/zoom555wincom.423495/
https://biomolecula.ru/authors/127345
https://talk.plesk.com/members/zoom555wincom.490488/#about
https://www.callupcontact.com/b/businessprofile/zoom555wincom/9988319
https://blender.community/zoom555wincom/
https://doselect.com/@25ab93942a1bfb67cd6d2ec4f
https://sciter.com/forums/users/zoom555wincom/
https://matkafasi.com/user/zoom555wincom
https://allmyfaves.com/zoom555wincom
https://www.notebook.ai/@zoom555wincom
https://www.abclinuxu.cz/lide/zoom555wincom
https://dumagueteinfo.com/author/zoom555wincom/
https://muare.vn/shop/zoom555wincom/895485
https://www.vnbadminton.com/members/zoom555wincom.65839/
https://doodleordie.com/profile/zoom555wincom
https://web.ggather.com/zoom555wincom
https://musikersuche.musicstore.de/profil/zoom555wincom/
https://www.intensedebate.com/people/zoom555wincom1
https://lookingforclan.com/user/zoom555wincom
https://forum.dmec.vn/index.php?members/zoom555wincom.176287/
https://igli.me/zoom555wincom
https://www.fantasyplanet.cz/diskuzni-fora/users/zoom555wincom/
https://freestyler.ws/user/632896/zoom555wincom
http://delphi.larsbo.org/user/zoom555wincom
https://www.aseeralkotb.com/en/profiles/zoom555wincom
https://timdaily.vn/members/zoom555wincom.128674/#about
https://app.readthedocs.org/profiles/zoom555wincom/
https://www.dibiz.com/kkcshailendra493
https://iszene.com/user-337250.html
https://www.theyeshivaworld.com/coffeeroom/users/zoom555wincom
https://desksnear.me/users/zoom555wincom
https://www.itchyforum.com/en/member.php?380191-zoom555wincom
https://www.roton.com/forums/users/kkcshailendra493/
https://able2know.org/user/zoom555wincom/
http://www.biblesupport.com/user/813722-zoom555wincom/
https://golosknig.com/profile/zoom555wincom/
https://www.anibookmark.com/user/zoom555wincom.html
https://www.inventoridigiochi.it/membri/zoom555wincom/profile/
https://forum.m5stack.com/user/zoom555wincom
https://wallhaven.cc/user/zoom555wincom
https://imageevent.com/zoom555wincom/zoom555wincom
https://www.bitchute.com/channel/zH6hrReqt2LD
https://bandori.party/user/513148/zoom555wincom/
https://community.m5stack.com/user/zoom555wincom
https://schoolido.lu/user/zoom555wincom/
https://awan.pro/forum/user/140017/
https://jakle.sakura.ne.jp/pukiwiki/?zoom555wincom
https://fortunetelleroracle.com/profile/zoom555wincom
https://fabble.cc/zoom555wincom
https://pad.geolab.space/s/qf2Yptq7O
https://affariat.com/user/profile/173687
https://community.cisco.com/t5/user/viewprofilepage/user-id/1978211
https://pad.stuve.de/s/SAGryRZ_i
https://kr.pinterest.com/zoom555wincom/
https://pt.gravatar.com/zoom555wincom
https://th.gravatar.com/zoom555wincom
https://www.sythe.org/members/zoom555wincom.2015435/
https://f319.com/members/zoom555wincom.1071317/
https://about.me/zoom555wincom
https://www.canadavisa.com/canada-immigration-discussion-board/members/zoom555wincom.1343155/#about
https://www.equinenow.com/farm/555win-1310727.htm
https://wefunder.com/zoom555wincom
https://potofu.me/zoom555wincom
https://transfur.com/Users/zoom555wincom
https://xtremepape.rs/members/zoom555wincom.646786/#about
https://myanimelist.net/profile/zoom555wincom
https://website.informer.com/zoom555win.com
https://lightroom.adobe.com/u/zoom555wincom
https://dev.to/zoom555wincom
https://beacons.ai/zoom555wincom
https://en.islcollective.com/portfolio/12856250
https://www.xosothantai.com/members/zoom555wincom.599204/
https://velog.io/@zoom555wincom/about
https://violet.vn/user/show/id/15241435
https://iplogger.org/vn/logger/HrNQ5l9fYPyE/
https://mez.ink/zoom555wincom
https://zoom555wincom.stck.me/profile
https://notionpress.com/author/1478272
https://www.edna.cz/uzivatele/zoom555wincom/
https://digiphoto.techbang.com/users/zoom555wincom
https://leakedmodels.com/forum/members/zoom555wincom.693018/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1047585
https://freeicons.io/profile/899605
https://zoom555wincom.taplink.ws/
https://onlinesequencer.net/forum/user-253812.html
https://inkbunny.net/zoom555wincom
https://www.japaaan.com/user/63458/
https://spinninrecords.com/profile/zoom555wincom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.555win2
https://code.antopie.org/zoom555wincom
https://beatsaver.com/playlists/1148328
https://apptuts.bio/zoom555wincom-249129
https://dialog.eslov.se/profiles/zoom555wincom/activity
https://www.storenvy.com/zoom555wincom
https://zoom555wincom.mssg.me/
https://forums.maxperformanceinc.com/forums/member.php?u=240071
https://egl.circlly.com/users/zoom555wincom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=291102
https://www.sciencebee.com.bd/qna/user/zoom555wincom
https://acomics.ru/-zoom555wincom
https://hanson.net/users/zoom555wincom
https://writexo.com/555win-b6a84bfb46c5
https://www.laundrynation.com/community/profile/zoom555wincom/
https://www.heavyironjobs.com/profiles/7949787-nha-cai-555win
https://pad.degrowth.net/s/cDUHLtCQT
https://www.rehashclothes.com/zoom555wincom
http://fort-raevskiy.ru/community/profile/zoom555wincom/
https://forum.skullgirlsmobile.com/members/zoom555wincom.197889/#about
https://jobs.landscapeindustrycareers.org/profiles/7949805-nha-cai-555win
https://forums.galciv4.com/user/7640698
https://kyourc.com/zoom555wincom
https://jobs.njota.org/employers/ed4de0fd-1246-4127-8529-e6ed8233887a/dashboard
https://song.link/zoom555wincom
https://idol.st/user/137345/zoom555wincom/
https://www.valinor.com.br/forum/usuario/zoom555wincom.141653/#about
https://tulieu.violet.vn/user/show/id/15241435
https://www.bmwpower.lv/user.php?u=zoom555wincom
https://gockhuat.net/member.php?u=431792
https://jobs.windomnews.com/profiles/7949892-nha-cai-555win
https://www.givey.com/zoom555wincom
https://talkmarkets.com/profile/zoom555wincom
https://pc.poradna.net/users/1145805009-zoom555wincom
https://forums.stardock.com/user/7640698
https://zerosuicidetraining.edc.org/user/profile.php?id=542364
https://www.telix.pl/forums/users/Shailendra-Kkc/
https://beteiligung.amt-huettener-berge.de/profile/zoom555wincom/
https://joinentre.com/profile/zoom555wincom
https://eo-college.org/members/zoom555wincom/
https://jobs.westerncity.com/profiles/7949958-nha-cai-555win
https://www.thetriumphforum.com/members/zoom555wincom.56920/
https://armchairjournal.com/forums/users/zoom555wincom/
https://gamblingtherapy.org/forum/users/zoom555wincom/
https://mycableengineering.com/activity-feed/userId/29606
https://l2top.co/forum/members/zoom555wincom.158108/
https://youtopiaproject.com/author/zoom555wincom/
https://forums.galciv3.com/user/7640698
https://galleria.emotionflow.com/175618/profile.html
https://www.myget.org/users/zoom555wincom
https://www.deafvideo.tv/vlogger/zoom555wincom
https://www.chaloke.com/forums/users/zoom555wincom/
https://app.brancher.ai/user/ejkv6ONHRItK
https://justpaste.me/wGJs1
https://aetherlink.app/users/7433438754129608704
https://forums.sinsofasolarempire2.com/user/7640698/
https://www.empregosaude.pt/en/author/zoom555wincom/
https://confengine.com/user/zoom555wincom
https://slideslive.com/zoom555wincom?tab=about
https://mygamedb.com/profile/zoom555wincom
https://buckeyescoop.com/community/members/zoom555wincom.57851/#about
https://forums.ashesofthesingularity.com/user/7640698
http://www.ssnote.net/users/zoom555wincom1
https://www.mateball.com/zoom555wincom
https://web-tourist.net/members/zoom555wincom.48872/#about
https://rotorbuilds.com/profile/204834/
https://toirscript.com/user/zoom555wincom
https://forum.pabbly.com/members/zoom555wincom.98957/#about
http://forum.cncprovn.com/members/415471-zoom555wincom
https://marketplace.trinidadweddings.com/author/zoom555wincom/
https://ncnews.co/profile/zoom555wincom
https://dreevoo.com/profile_info.php?pid=1197244
https://forum.aigato.vn/user/zoom555wincom
https://rapidapi.com/user/zoom555wincom
https://www.skool.com/@nha-cai-win-8328
https://hedge.fachschaft.informatik.uni-kl.de/s/v6lHXJqVB
https://learningapps.org/watch?v=ptdf7bp5a26
https://postheaven.net/zoom555wincom/555win
https://www.giveawayoftheday.com/forums/profile/1674119
https://tealfeed.com/zoom555wincom
https://www.catapulta.me/users/555win-565
https://www.invelos.com/UserProfile.aspx?Alias=zoom555wincom
https://www.video-bookmark.com/bookmark/7059027/zoom555wincom/
https://wibki.com/zoom555wincom
https://twitback.com/zoom555wincom
https://krachelart.com/UserProfile/tabid/43/userId/1334680/Default.aspx
https://gitlab.vuhdo.io/zoom555wincom
https://www.11secondclub.com/users/profile/1700460
https://aniworld.to/user/profil/zoom555wincom
https://worldvectorlogo.com/profile/zoom555wincom
https://kktix.com/user/8453842
https://www.passes.com/zoom555wincom
https://poipiku.com/13253858/
https://uiverse.io/profile/shailendra_2424
https://www.rwaq.org/users/zoom555wincom
https://cofacts.tw/user/zoom555wincom
https://www.fundable.com/user-1290833
https://vcook.jp/users/75755
https://www.grepmed.com/zoom555wincom
https://espritgames.com/members/50223467/
https://cgmood.com/zoom555wincom
https://www.haikudeck.com/presentations/Nhci.555WIN.3
https://www.efunda.com/members/people/show_people.cfm?Usr=zoom555wincom
https://paidforarticles.in/author/zoom555wincom
https://backloggery.com/zoom555wincom
https://www.sociomix.com/u/555win2222222222222222/
https://raovat.nhadat.vn/members/zoom555wincom-290151.html
https://www.moshpyt.com/user/zoom555wincom
https://www.koi-s.id/member.php?331654-zoom555wincom
https://pumpyoursound.com/u/user/1586486
https://que.u.nosv.org/profile?user=zoom555wincom
https://secondstreet.ru/profile/zoom555wincom/
http://scenarch.com/userpages/29062
https://undrtone.com/zoom555wincom
https://marshallyin.com/members/zoom555wincom/
https://us.enrollbusiness.com/BusinessProfile/7734954/555WIN
https://www.atozed.com/forums/user-68565.html
https://gram.social/zoom555wincom
https://searchengines.bg/members/zoom555wincom.23623/#about
https://luvly.co/users/zoom555wincom
https://suckhoetoday.com/members/36111-zoom555w.html
https://hukukevi.net/user/zoom555wincom
https://belgaumonline.com/profile/zoom555wincom/
https://savelist.co/profile/users/zoom555wincom
https://usdinstitute.com/forums/users/zoom555wincom/
https://www.montessorijobsuk.co.uk/author/zoom555wincom/
https://hackerspace.govhack.org/profiles/555win_35766
https://www.apsense.com/user/zoom555wincom
https://zzb.bz/kJbGqy
https://draft.blogger.com/profile/12771622213121756821
https://boldomatic.com/view/writer/zoom555wincom
https://menwiki.men/wiki/User:Zoom555wincom
https://funsilo.date/wiki/User:zoom555wincom
https://www.themeqx.com/forums/users/zoom555wincom/
https://www.udrpsearch.com/user/zoom555wincom
https://www.inseparabile.it/forum/member.php?u=45876
https://forums.wincustomize.com/user/7640698
https://www.xen-factory.com/index.php?members/zoom555wincom.141107/#about
https://cointr.ee/zoom555wincom
https://king-wifi.win/wiki/User:zoom555wincom
https://forums.servethehome.com/index.php?members/zoom555wincom.227219/#about
https://raovatquynhon.com/thiet-bi-dien-tu-4/zoom555wincom-16079
http://www.truck-business.cz/profile/zoom555wincom/info.html
https://www.blackhatprotools.info/member.php?277555-zoom555wincom
https://activepages.com.au/profile/zoom555wincom
https://snippet.host/batimg
https://tudomuaban.com/chi-tiet-rao-vat/2831720/zoom555wincom.html
https://phijkchu.com/a/zoom555wincom/video-channels
https://lifeinsys.com/user/zoom555wincom
https://kaeuchi.jp/forums/users/zoom555wincom/
https://www.claimajob.com/profiles/7956219-nha-cai-555win
https://protospielsouth.com/user/118250
https://theafricavoice.com/profile/zoom555wincom
http://palangshim.com/space-uid-4989673.html
https://www.africangenesis-101.org/profile/zoom555wincom/profile
https://vi.gravatar.com/zoom555wincom
https://www.vevioz.com/zoom555wincom
https://www.mixcloud.com/zoom555wincom/
https://www.designspiration.com/zoom555wincom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=186672
https://hub.vroid.com/en/users/124300806
https://www.exchangle.com/zoom555wincom
https://forum.codeigniter.com/member.php?action=profile&uid=224749
https://circleten.org/a/396883?postTypeId=whatsNew
https://bitspower.com/support/user/zoom555wincom
https://www.brownbook.net/business/54873509/555win
https://blog.ulifestyle.com.hk/zoom555wincom
https://etextpad.com/fycvznu9ai
https://app.hellothematic.com/creator/profile/1124798
https://app.talkshoe.com/user/zoom555wincom
https://m.wibki.com/zoom555wincom
https://www.pageorama.com/?p=zoom555wincom
https://bandsworksconcerts.info/index.php?zoom555wincom
https://jerseyboysblog.com/forum/member.php?action=profile&uid=82936
https://www.quora.com/profile/Zoom555wincom
https://manylink.co/@zoom555wincom
https://www.freewebspace.net/forums/index.php?members/zoom555wincom.17031366/#about
https://forums.giantitp.com/member.php?369436-zoom555wincom
https://seomotionz.com/member.php?action=profile&uid=117837
https://anyflip.com/homepage/ccgqa#About
https://www.akaqa.com/question/q19192654886-Zoom555wincom
https://londonchinese.com/home.php?mod=space&uid=615261&do=profile
https://copynotes.be/shift4me/forum/user-44929.html
https://scholar.google.com/citations?user=lh-G65EAAAAJ&hl=en
https://www.smitefire.com/profile/zoom555wincom-257444?profilepage
https://tabelog.com/rvwr/zoom555wincom/prof/
https://coolors.co/u/zoom555wincom
https://www.beamng.com/members/zoom555wincom.775204/
https://civitai.com/user/zoom555wincom
https://www.spigotmc.org/members/zoom555wincom.2489223/
https://boosty.to/zoom555wincom
https://camp-fire.jp/profile/zoom555wincom
https://feyenoord.supporters.nl/profiel/139507/zoom555wincom
https://www.pearltrees.com/zoom555wincom/item783249359
https://gesoten.com/profile/detail/12601349
https://hashnode.com/@zoom555wincom
https://hoo.be/zoom555wincom
https://nhattao.com/members/user6924779.6924779/
https://maxforlive.com/profile/user/zoom555wincom?tab=about
https://pinshape.com/users/8918770-zoom555wincom
https://morguefile.com/creative/zoom555wincom
https://edabit.com/user/sKuquc2BYshBoemc5
https://mathlog.info/users/5NjWZKVFXjXGFPzLJjpKzBmO5BK2
https://securityheaders.com/?q=https%3A%2F%2Fzoom555win.com%2F
https://my.bio/zoom555wincom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145564
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165822
https://md.darmstadt.ccc.de/s/rAtExsLXce
https://participation.u-bordeaux.fr/profiles/zoom555wincom/activity
https://sfx.thelazy.net/users/u/zoom555wincom/
https://forum.reallusion.com/Users/3283828/KkcShailendra493
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=247573
https://slidehtml5.com/homepage/ruwi#About
https://webanketa.com/forms/6mv34d1q6rqpac1s60spadhj/
https://matters.town/@zoom555wincom
https://www.pdc.edu/?URL=https://zoom555win.com/
https://ask.mallaky.com/?qa=user/zoom555wincom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75947
https://drill.lovesick.jp/drilldata/index.php?zoom555wincom
https://www.depechemode.cz/?URL=https://zoom555win.com/
https://sub4sub.net/forums/users/zoom555wincom/
https://www.slmath.org/people/99345
https://userstyles.world/user/zoom555wincom
https://hu.gta5-mods.com/users/zoom555wincom
https://uk.gta5-mods.com/users/zoom555wincom
https://sl.gta5-mods.com/users/zoom555wincom
https://goo.by/ZeiQPS
https://amazingradio.com/profile/zoom555wincom
https://bresdel.com/zoom555wincom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12141
https://pledgeme.co.nz/profiles/319377
https://zoom555wincom.notepin.co/
https://pictureinbottle.com/r/zy6s193q
https://forum.epicbrowser.com/profile.php?section=personal&id=139237
http://www.dungdong.com/home.php?mod=space&uid=3324594
https://www.squadskates.com/profile/zoom555wincom/profile
https://forum.herozerogame.com/index.php?/user/152348-zoom555wincom/
https://shhhnewcastleswingers.club/forums/users/zoom555wincom/
https://forums.qhimm.com/index.php?action=profile;u=89990
https://mylinks.ai/zoom555wincom
https://electroswingthing.com/profile/zoom555wincom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2392088
https://connect.gt/user/zoom555wincom
https://stuv.othr.de/pad/s/ANyYsdHl4
https://forum.tkool.jp/index.php?members/zoom555wincom.97990/#about
https://hedgedoc.eclair.ec-lyon.fr/s/xEl-vxlA_
http://densan-knct.freehostia.com/wiki_/index.php?zoom555wincom
https://www.divephotoguide.com/user/zoom555wincom
https://www.weddingbee.com/members/zoom555wincom/
https://kumu.io/zoom555wincom/zoom555wincom
https://mforum3.cari.com.my/home.php?mod=space&uid=3383411&do=index
https://bioimagingcore.be/q2a/user/zoom555wincom
https://www.sunlitcentrekenya.co.ke/author/zoom555wincom/
https://hedgedoc.logilab.fr/s/LEchmTh6J
https://zoom555wincom.livejournal.com/
https://entre-vos-mains.alsace.eu/profiles/zoom555wincom/activity
https://www.rcuniverse.com/forum/members/zoom555wincom.html
https://www.huntingnet.com/forum/members/zoom555wincom.html
https://www.socialbookmarkssite.com/bookmark/6200836/zoom555wincom/
https://hedgedoc.stusta.de/s/k-ezWKfQK
https://pad.flipdot.org/s/PDmc_EXQJ
https://hack.allmende.io/s/1sJIScHue
https://pad.codefor.fr/s/Pwp5iR4MJm
https://md.opensourceecology.de/s/vYZhY95pQ
https://md.ctdo.de/s/c1eGn1DH_F
https://md.chaospott.de/s/sGVAlWf0dZ
https://pad.fablab-siegen.de/s/XWvxqpX_6
https://ar.gravatar.com/zoom555wincom
https://www.hogwartsishere.com/1818657/
https://vimeo.com/zoom555wincom
https://forum.index.hu/User/UserDescription?u=2194394
https://gitlab.com/zoom555wincom
https://www.symbaloo.com/shared/AAAABK1dXG0AA41_l1xj2A==
https://makeagif.com/user/zoom555wincom?ref=LU8XnJ
https://www.lingvolive.com/en-us/profile/46c4b45c-e66f-4162-bc05-03087f6896fc/translations
https://participez.perigueux.fr/profiles/zoom555wincom/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424987
https://www.trackyserver.com/profile/232145
https://ixawiki.com/link.php?url=https://zoom555win.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=135511
https://www.zubersoft.com/mobilesheets/forum/user-124749.html
https://forum.dboglobal.to/wsc/index.php?user/143531-zoom555wincom/&editOnInit=true#about
https://tutorialslink.com/member/ShailendraKkc/90574
https://www.buzzbii.com/zoom555wincom
http://www.activewin.com/user.asp?Action=Read&UserIndex=4827240
https://www.vid419.com/home.php?mod=space&uid=3475889
https://forum.ct8.pl/member.php?action=profile&uid=115142
https://devfolio.co/@zoom555wincom/readme-md
https://zoom555wincom.shopinfo.jp/posts/58597903
https://linqto.me/n/zoom555wincom
mindomo.com/mindmap/c87bd96ff7934cbd9de438025197d648
https://www.okaywan.com/home.php?mod=space&uid=773092
https://www.goodolcomics.com/blog/profile/zoom555wincom/
https://www.swap-bot.com/user:zoom555wincom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=384623
http://techou.jp/index.php?zoom555wincom
https://paste.intergen.online/view/08c48605
https://web.trustexchange.com/company.php?q=zoom555win.com
https://forums.megalith-games.com/member.php?action=profile&uid=1442685
http://tkdlab.com/wiki/index.php?zoom555wincom
https://www.managementpedia.com/members/zoom555wincom.1116725/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=605833
https://volleypedia.org/index.php?qa=user&qa_1=zoom555wincom
http://pcsq28.com/home.php?mod=space&uid=1768555
https://bbs.airav.cc/home.php?mod=space&uid=4424272
https://partecipa.poliste.com/profiles/zoom555wincom/activity
https://md.coredump.ch/s/L0nu6ZlnP
https://hker2uk.com/home.php?mod=space&uid=5347763
https://pad.funkwhale.audio/s/s5pqLqlSk
https://forum.dfwmas.org/index.php?members/zoom555wincom.194903/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=467142
https://aprenderfotografia.online/usuarios/zoom555wincom/profile/
https://m.jingdexian.com/home.php?mod=space&uid=5482315
https://xibeiwujin.com/home.php?mod=space&uid=2304232
https://tilengine.org/forum/member.php?action=profile&uid=158593
https://www.play56.net/home.php?mod=space&uid=6017214
https://hedgedoc.stusta.de/s/_61qtJI3D
https://pad.flipdot.org/s/TOCcAm8ey
https://hack.allmende.io/s/db9Etce5z
https://pad.codefor.fr/s/E6gNsjFzNU
https://md.opensourceecology.de/s/u0E5-vW3H
https://md.chaospott.de/s/Cx5B56kJIq
https://pad.fablab-siegen.de/s/Gu5h2cLnn
https://hackmd.hub.yt/s/IUI1aRd07
https://md.swk-web.com/s/T7DQt57Kd4
https://hedgedoc.dezentrale.space/s/tc2g4lyd5
https://docs.juze-cr.de/s/fQ88p3uM2
https://sensationaltheme.com/forums/users/zoom555wincom/
https://www.degreeforum.net/mybb/User-zoom555wincom
https://wandb.ai/profile/zoom555wincom
https://pad.darmstadt.social/s/rTCO06fBTo
https://divisionmidway.org/jobs/author/zoom555wincom/
https://www.youbiz.com/profile/zoom555wincom
https://timeoftheworld.date/wiki/User:Zoom555wincom
https://cameradb.review/wiki/User:Zoom555wincom
https://www.wowonder.xyz/zoom555wincom
https://sciencemission.com/profile/zoom555wincom
https://referrallist.com/profile/zoom555wincom
http://jobboard.piasd.org/author/zoom555wincom/
http://jobs.emiogp.com/author/zoom555wincom/
https://www.canadavideocompanies.ca/forums/users/zoom555wincom/
https://hackmd.openmole.org/s/8jmbeoY32
https://md.chaosdorf.de/s/Z-e1F-TKLM
https://forumketoan.com/members/zoom555wincom.41785/#about
https://doc.adminforge.de/s/P7INbfm1DM
https://onlinevetjobs.com/author/zoom555wincom/
https://v.gd/f6uOew
https://zoom555wincom.mystrikingly.com/
https://zoom555wincom.webflow.io/
https://rant.li/zoom555wincom/555win
https://sites.google.com/view/zoom555wincom/
https://telegra.ph/555WIN-03-01
https://zoom555wincom.blogspot.com/2026/02/zoom555wincom.html
https://zoom555wincom.mypixieset.com/
https://hedgedoc.stusta.de/s/wg_NaDvgd
https://scrapbox.io/zoom555wincom/555WIN
https://ofuse.me/zoom555wincom
https://zoom555wincom.therestaurant.jp/posts/58594254
https://zoom555wincom.theblog.me/posts/58594256
https://fuschia-keyboard-290.notion.site/555WIN-316c84704a74805cb1dcc976023e9763
https://zb3.org/zoom555wincom/555win
https://zoom555wincom.exblog.jp/34440912/
https://diigo.com/01218f8
https://www.myaspenridge.com/members/profile/3646837/zoom555wincom.htm
https://www.tai-ji.net/members/profile/3646838/zoom555wincom.htm
https://www.greencarpetcleaningprescott.com/members/profile/3646839/zoom555wincom.htm
https://www.thepetservicesweb.com/members/profile/3646840/zoom555wincom.htm
https://www.milliescentedrocks.com/members/profile/3646841/zoom555wincom.htm
https://www.sunemall.com/members/profile/3646847/zoom555wincom.htm
https://www.freedomteamapexmarketinggroup.com/members/profile/3646848/zoom555wincom.htm
https://www.bestloveweddingstudio.com/forum/topic/62867/zoom555wincom
https://www.ekdarun.com/forum/topic/135357/zoom555wincom
Your comment is awaiting moderation.
https://www.youtube.com/@cm88tsite
https://twitter.com/cm88tsite
https://tooter.in/cm88tsite
https://wakelet.com/@cm88tsite
https://safechat.com/u/cm88tsite
https://gravatar.com/cm88tsite
https://www.blogger.com/profile/17778764381948022398
https://www.mymeetbook.com/cm88tsite
https://www.pinterest.com/cm88tsite/
https://community.wongcw.com/cm88tsite
https://demo.wowonder.com/cm88tsite
https://shareyoursocial.com/cm88tsite
https://gitlab.aicrowd.com/cm88tsite
https://myspace.com/cm88tsite
https://500px.com/p/cm88tsite
https://www.instapaper.com/p/cm88tsite
https://magic.ly/cm88tsite
https://www.band.us/page/101728869
https://protocol.ooo/ja/users/cm88-343ffe10-ceb4-4183-834b-34bf2e32a867
https://sketchfab.com/cm88tsite
https://audiomack.com/cm88tsite
https://draft.blogger.com/profile/17778764381948022398
https://hackaday.io/cm88tsite
https://fyers.in/community/member/V31u8Dh0Er
https://vocal.media/authors/c-m88-wigdj0hd8
https://leetcode.com/u/cm88tsite/
https://swag.live/en/user/69a119d8814404e55923996a
https://www.halaltrip.com/user/profile/321798/cm88tsite/
https://www.jetphotos.com/photographer/784921
https://medibang.com/author/27873140/
https://liulo.fm/cm88tsite
https://opensea.io/cm88tsite
https://www.blockdit.com/cm88tsite
https://portfolium.com/cm88tsite
https://www.twitch.tv/cm88tsite/about
https://profile.hatena.ne.jp/cm88tsite/
https://issuu.com/cm88tsite
https://www.behance.net/nhcicm888
https://www.reverbnation.com/artist/cm88tsite
https://www.myminifactory.com/users/cm88tsite
https://www.investagrams.com/Profile/cm88tsite
https://gifyu.com/cm88tsite
https://www.chordie.com/forum/profile.php?id=2474488
https://www.walkscore.com/people/100597349039/cm88
https://topsitenet.com/profile/cm88tsite/1552981/
https://akniga.org/profile/1395673-cm88/
https://cm88tsite.bandcamp.com/album/cm88
https://disqus.com/by/cm88tsite/about/
https://jobs.suncommunitynews.com/profiles/7946223-cm88
https://www.speedrun.com/users/cm88tsite
https://www.fanart-central.net/user/cm88tsite/profile
https://www.aicrowd.com/participants/cm88tsite
https://old.bitchute.com/channel/CyPMJrttUFVH/
https://pbase.com/cm88tsite
https://hub.docker.com/u/cm88tsite
https://spiderum.com/nguoi-dung/cm88tsite
https://zaidap.com/thong-tin-ca-nhan-u106146.htm
https://www.gta5-mods.com/users/cm88tsite
https://heylink.me/cm88tsite/
https://pixabay.com/users/54817119/
https://www.nicovideo.jp/user/143394298
https://www.jigsawplanet.com/cm88tsite
https://3dwarehouse.sketchup.com/by/cm88tsite
https://robertsspaceindustries.com/en/citizens/cm88tsite
https://bit.ly/m/cm88tsite
https://allmylinks.com/cm88tsite
https://joy.link/cm88tsite
https://connect.garmin.com/app/profile/f936eb77-5cbf-4f31-9557-7980eece4fb6
https://b.hatena.ne.jp/cm88tsite/bookmark
https://www.chichi-pui.com/users/cm88tsite/
https://www.openrec.tv/user/cm88tsite/about
https://unityroom.com/users/cm88tsite
https://routinehub.co/user/cm88tsite
https://pxhere.com/en/photographer/4930682
https://teletype.in/@cm88tsite
https://www.checkli.com/cm88tsite
https://gitee.com/cm88tsite
https://www.fuelly.com/driver/cm88tsite
https://www.nintendo-master.com/profil/cm88tsite
https://freeimage.host/cm88tsite
https://www.diigo.com/item/note/br0wd/nwy6?k=c2d8aa6a8d33390a04384030025887b3
https://fontstruct.com/fontstructions/show/2833497/cm88-13
https://motion-gallery.net/users/917544
https://linkin.bio/cm88tsite
https://biomolecula.ru/authors/127299
https://talk.plesk.com/members/cmtamtamtsite.490430/#about
https://www.callupcontact.com/b/businessprofile/CM88/9988095
https://www.growkudos.com/profile/nhacai_cm88_2
https://blender.community/cm8813/
https://doselect.com/@e79f924df1b27a06bef1a397c
https://sciter.com/forums/users/cm88tsite/
https://matkafasi.com/user/cm88tsite
https://allmyfaves.com/cm88tsite?tab=CM88
https://www.notebook.ai/users/1289023
https://www.abclinuxu.cz/lide/cm88tsite
https://muare.vn/shop/92/895476
https://doodleordie.com/profile/cm88tsite
https://web.ggather.com/cm88tsite
https://musikersuche.musicstore.de/profil/cm88tsite/
https://www.intensedebate.com/people/cm88tsitee
https://lookingforclan.com/user/cm88tsitee
https://forum.dmec.vn/index.php?members/cm88tsite.176252/
https://igli.me/cm88tsite
https://www.fantasyplanet.cz/diskuzni-fora/users/cm88tsite/
https://duyendangaodai.net/members/30203-cm88tsit.html
https://freestyler.ws/user/632834/cm88tsite
http://delphi.larsbo.org/user/cm88tsite
https://www.aseeralkotb.com/en/profiles/cm88tsite
https://timdaily.vn/members/cm88tsite.128651/#about
https://app.readthedocs.org/profiles/cm88tsite/
https://www.dibiz.com/mos0838401902
https://iszene.com/user-337210.html
https://www.theyeshivaworld.com/coffeeroom/users/cm88tsite
https://desksnear.me/users/cm88tsite
https://www.itchyforum.com/en/member.php?380114-cm88tsite
https://www.roton.com/forums/users/mos0838401902/
https://able2know.org/user/cm88tsite/
http://www.biblesupport.com/user/813521-cm88tsite/
https://golosknig.com/profile/cm88tsite/
https://www.anibookmark.com/user/cm88tsite.html
https://www.inventoridigiochi.it/membri/cm88tsite/profile/
https://forum.m5stack.com/user/cm88tsite
https://wallhaven.cc/user/cm88tsite
https://imageevent.com/cm88tsite/nhcicm88
https://www.bitchute.com/channel/CyPMJrttUFVH
https://bandori.party/user/511537/cm88tsite/#preferences
https://community.m5stack.com/user/cm88tsite
https://schoolido.lu/user/cm88tsite/
https://awan.pro/forum/user/139849/
https://jakle.sakura.ne.jp/pukiwiki/?cm88tsite
https://fortunetelleroracle.com/profile/cm88tsite
https://fabble.cc/cm88tsite
https://pad.geolab.space/s/TVFPd3noB
https://community.cisco.com/t5/user/viewprofilepage/user-id/1977999
https://pad.stuve.de/s/9i_9Rhn4c
https://kr.pinterest.com/cm88tsite/
https://pt.gravatar.com/cm88tsite
https://th.gravatar.com/cm88tsite
https://www.sythe.org/members/cm88tsite.2015181/
https://f319.com/members/cm88tsite.1071071/
https://about.me/cm88tsite
https://www.canadavisa.com/canada-immigration-discussion-board/members/cm88tsite.1343054/#about
https://www.equinenow.com/farm/profile69a1108c2428a.htm
https://wefunder.com/cm88tsite
https://potofu.me/cm88tsite
https://transfur.com/Users/cm88tsite
https://xtremepape.rs/members/cm88tsite.646539/#about
https://github.com/cm88tsite
https://myanimelist.net/profile/cm88tsite
https://qna.habr.com/user/cm88tsite
https://website.informer.com/cm88t.site
https://beacons.ai/cm88tsite
https://en.islcollective.com/portfolio/12855756
https://velog.io/@cm88tsite/about
https://violet.vn/user/show/id/15241225
https://iplogger.org/logger/peBQ5ZU5HJ8W/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3905438
https://mez.ink/cm88tsite
https://cm88tsite.stck.me/profile
https://notionpress.com/author/1477894
https://www.edna.cz/uzivatele/cm88tsite/
https://digiphoto.techbang.com/users/cm88tsite
https://leakedmodels.com/forum/members/cm88tsite.692776/#about
https://freeicons.io/profile/899200
https://onlinesequencer.net/forum/user-253528.html
https://inkbunny.net/cm88tsite
https://www.japaaan.com/user/home
https://www.launchgood.com/user/newprofile#!/user-profile/profile/cm88.tsite
https://www.techbang.com/users/cm88tsite
https://code.antopie.org/cm88tsite
https://beatsaver.com/playlists/1147631
https://apptuts.bio/cm88tsite
https://dialog.eslov.se/profiles/cm88tsite/activity?locale=en
https://www.storenvy.com/cm88tsite
https://forums.maxperformanceinc.com/forums/member.php?u=239959
https://egl.circlly.com/users/cm88tsite
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=290944
https://acomics.ru/-cm88tsite
https://www.criminalelement.com/members/cm88tsite/profile/
https://hanson.net/users/cm88tsite
https://writexo.com/share/abfe2b743a85
https://expatguidekorea.com/profile/cm88tsite/
https://www.heavyironjobs.com/profiles/7945568-cm88
https://pad.degrowth.net/s/EHOoQIxbX
https://www.syncdocs.com/forums/profile/cm88tsite
https://www.rehashclothes.com/cm88tsite
http://fort-raevskiy.ru/community/profile/cm88tsite/
https://forum.skullgirlsmobile.com/members/cm88tsite.197556/#about
https://jobs.landscapeindustrycareers.org/profiles/7945621-cm88
https://phatwalletforums.com/user/cm88tsite
https://forums.galciv4.com/user/7640309
https://kyourc.com/1772171804998744_170190
https://song.link/cm88tsite
https://idol.st/user/136982/cm88tsite/
https://www.valinor.com.br/forum/usuario/cm88tsite.141600/#about
https://tulieu.violet.vn/user/show/id/15241225
https://www.bmwpower.lv/user.php?u=cm88tsite
https://jobs.windomnews.com/profiles/7945722-cm88
https://hoaxbuster.com/redacteur/cm88tsite
https://www.givey.com/cm88tsite
https://forums.stardock.com/user/7640309
https://zerosuicidetraining.edc.org/user/profile.php?id=541928
https://beteiligung.amt-huettener-berge.de/profile/cm88tsite/
https://beteiligung.hafencity.com/profile/cm88tsite/
https://adhocracy.plus/profile/cm88tsite/
https://www.hobowars.com/game/linker.php?url=https://cm88t.site/
https://beteiligung.stadtlindau.de/profile/cm88tsite/
https://beteiligung.tengen.de/profile/cm88tsite/
https://joinentre.com/profile/cm88tsite
https://jobs.westerncity.com/profiles/7945873-cm88
https://www.thetriumphforum.com/members/cm88tsite.56836/
https://album.link/cm88tsite
https://mycableengineering.com/activity-feed/userId/29563
https://portfolium.com.au/cm88tsite
https://forums.galciv3.com/user/cm88tsite
https://www.chaloke.com/forums/users/cm88tsite/
https://justpaste.me/vrxY8
https://forums.sinsofasolarempire2.com/user/7640309
https://buckeyescoop.com/community/members/cm88tsite.57804/#about
https://toirscript.com/user/cm88tsite
https://forum.pabbly.com/members/cm88tsite.98789/#about
http://forum.cncprovn.com/members/415343-cm88tsite
https://marketplace.trinidadweddings.com/author/cm88tsite/
https://forum.aigato.vn/user/cm88tsite
https://rapidapi.com/user/cm88tsite
https://www.skool.com/@nha-cai-cmtamtam-5986
https://espritgames.com/members/50195507/
https://cgmood.com/cm88tsite
https://www.haikudeck.com/presentations/77UbzpRSpz
https://paidforarticles.in/author/cm88tsite
https://www.moshpyt.com/user/cm88tsite
https://secondstreet.ru/profile/cm88tsite/
https://undrtone.com/cm88tsite
https://marshallyin.com/members/cm88tsite/
https://www.atozed.com/forums/user-68373.html
https://gram.social/cm88tsite
https://es.gravatar.com/cm88tsite
https://de.gravatar.com/cm88tsite
https://cy.gravatar.com/cm88tsite
https://hukukevi.net/user/cm88tsite
https://belgaumonline.com/profile/cm88tsite/
https://savelist.co/profile/users/cm88tsite
https://www.apsense.com/user/cm88tsite
https://zzb.bz/JZeQWX
https://www.apsense.com/user/cm88tsite
https://menwiki.men/wiki/User:Cm88tsite
https://funsilo.date/wiki/User:Cm88tsite
https://www.themeqx.com/forums/users/cm88tsite/
https://www.inseparabile.it/forum/member.php?u=45823
http://newdigital-world.com/members/cm88tsite.html
https://www.xen-factory.com/index.php?members/cm88tsite.140799/#about
https://king-wifi.win/wiki/User:Cm88tsite
https://uk.gravatar.com/cm88tsitee
https://hu.gravatar.com/cm88tsitee
https://it.gravatar.com/cm88tsitee
https://www.blackhatprotools.info/member.php?277167-cm88tsite
https://activepages.com.au/profile/cm88tsite
https://snippet.host/cawrbp
https://tudomuaban.com/chi-tiet-rao-vat/2829492/cm88–trang-chu-cm88.com.html
https://phijkchu.com/a/nhacai.cm88/video-channels
https://lifeinsys.com/user/cm88tsite
https://kaeuchi.jp/forums/users/cm88tsite/
https://www.claimajob.com/profiles/7946658-nha-cai-cm88
https://theafricavoice.com/profile/cm88tsite
https://vi.gravatar.com/cm88tsitee
https://hub.vroid.com/en/users/124215357
https://www.exchangle.com/cm88tsite
https://bitspower.com/support/user/cm88tsite
https://www.brownbook.net/business/54866573/nh%C3%A0-c%C3%A1i-cm88
https://km.gravatar.com/cm88tsitee
https://ja.gravatar.com/cm88tsitee
https://id.gravatar.com/cm88tsitee
https://he.gravatar.com/cm88tsitee
https://manylink.co/@cm88tsite
https://da.gta5-mods.com/users/cm88tsite
https://el.gta5-mods.com/users/cm88tsite
https://es.gta5-mods.com/users/cm88tsite
https://fr.gta5-mods.com/users/cm88tsite
https://ko.gta5-mods.com/users/cm88tsite
https://anyflip.com/homepage/zrtby
https://www.akaqa.com/question/q19192654325-Cm88tsite
https://copynotes.be/shift4me/forum/user-44666.html
threadless.com/@cm88tsite
https://tabelog.com/rvwr/cm88tsite/prof/
https://www.beamng.com/members/cm88tsite.774459/
https://civitai.com/user/cm88tsite
https://www.spigotmc.org/members/cm88tsite.2486943/
https://feyenoord.supporters.nl/profiel/139040/cm88tsite
https://rekonise.com/u/cm88tsite
https://maxforlive.com/profile/user/cm88tsite?tab=about
https://3dtoday.ru/blogs/cm88tsite
https://mathlog.info/users/BwzuCq070mc1wtw7brYL7JkDZwu2
https://my.bio/cm88tsite
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145351
https://matters.town/@cm88tsite
https://hi.gta5-mods.com/users/cm88tsite
https://it.gta5-mods.com/users/cm88tsite
https://nl.gta5-mods.com/users/cm88tsite
https://no.gta5-mods.com/users/cm88tsite
https://pl.gta5-mods.com/users/cm88tsite
https://pt.gta5-mods.com/users/cm88tsite
https://www.slmath.org/people/99076
https://bresdel.com/cm88tsite
https://www.upcarta.com/profile/cm88tsite
https://fora.babinet.cz/profile.php?id=114939
https://www.shippingexplorer.net/en/user/cm88tsite/257429
https://shhhnewcastleswingers.club/forums/users/cm88tsite/
https://connect.gt/user/cm88tsite
https://www.divephotoguide.com/user/cm88tsite
https://kumu.io/cm88tsite/cm88tsite
https://www.sunlitcentrekenya.co.ke/author/cm88tsite/
https://www.rcuniverse.com/forum/members/cm88tsite.html
https://www.huntingnet.com/forum/members/cm88tsite.html
https://vimeo.com/cm88tsite
https://www.symbaloo.com/mix/cm88-muim
https://www.bricklink.com/aboutMe.asp?u=cm88tsite
https://zh-tw.gravatar.com/cm88tsite
https://sv.gravatar.com/cm88tsite
https://po.gravatar.com/cm88tsite
https://oc.gravatar.com/cm88tsite
https://mt2.org/uyeler/cm88tsite.35260/#about
https://participez.perigueux.fr/profiles/cm88tsite/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424631
https://www.trackyserver.com/profile/231493
https://www.zubersoft.com/mobilesheets/forum/user-124191.html
https://tutorialslink.com/member/MeiKemp/90266
https://www.buzzbii.com/cm88tsite
https://www.mindomo.com/mindmap/cm88-0e8c50b77eb34a1dae885102966a918b
https://www.swap-bot.com/user:cm88tsite
https://md.coredump.ch/s/VfX-sh_QN
https://aprenderfotografia.online/usuarios/cm88tsite/profile/
https://hackmd.hub.yt/s/iW_3nB8Dd
https://ar.gravatar.com/cm88tsite
https://sensationaltheme.com/forums/users/cm88tsite/
https://divisionmidway.org/jobs/author/cm88tsite/
https://cameradb.review/wiki/User:Cm88tsite
https://ur.gravatar.com/cm88tsite
https://tr.gravatar.com/cm88tsite
https://sr.gravatar.com/cm88tsite
https://sq.gravatar.com/cm88tsite
https://sl.gravatar.com/cm88tsite
https://historydb.date/wiki/User:Cm88tsite
https://sciencemission.com/profile/cm88tsite
https://www.wvhired.com/profiles/7946384-nha-cai-cm88
https://www.canadavideocompanies.ca/forums/users/cm88tsite/
https://id.gta5-mods.com/users/cm88tsite
https://ms.gta5-mods.com/users/cm88tsite
https://bg.gta5-mods.com/users/cm88tsite
https://cs.gta5-mods.com/users/cm88tsite
https://ismschools.com.au/forums/users/cm88tsite/
https://sciencewiki.science/wiki/User:Cm88tsite
https://formulamasa.com/elearning/members/cm88tsite/?v=96b62e1dce57
https://forum.flashphoner.com/members/cm88tsite.41986/#about
https://backloggd.com/u/cm88tsite/
https://form.jotform.com/260572052030039
https://community.jmp.com/t5/user/viewprofilepage/user-id/91195
https://www.corc.co.uk/forums/users/cm88tsite/
https://cuwip.ucsd.edu/members/cm88tsite/profile/
https://www.stylevore.com/user/cm88tsite
https://bio.site/cm88tsite
https://viblo.asia/u/cm88tsite/contact
https://skr.gravatar.com/cm88tsite
https://sk.gravatar.com/cm88tsite
https://ru.gravatar.com/cm88tsite
https://ro.gravatar.com/cm88tsite
https://hype4.academy/profile/cm88tsite
https://reactormag.com/members/cm88tsite/
https://brain-market.com/u/cm88tsite
https://www.emailsherlock.com/hosts/cm88t.site
https://www.prosebox.net/book/101785/
https://www.aipictors.com/users/cm88tsite
https://idev.games/profile/cm88tsite
https://redirect.camfrog.com/redirect/?url=https://cm88t.site/
https://forum.honorboundgame.com/user-503788.html
https://www.fw-follow.com/forum/topic/92095/cm88tsite
https://www.jk-green.com/forum/topic/88426/cm88tsite
https://www.navacool.com/forum/topic/320191/cm88tsite
https://www.driedsquidathome.com/forum/topic/114305/cm88tsite
https://www.nongkhaempolice.com/forum/topic/88486/cm88tsite
https://www.bestloveweddingstudio.com/forum/topic/62313/cm88tsite
https://www.natthadon-sanengineering.com/forum/topic/78965/cm88tsite
https://www.rueanmaihom.net/forum/topic/78286/cm88tsite
https://www.ttlxshipping.com/forum/topic/320189/cm88tsite
http://forum.modulebazaar.com/forums/user/cm88tsite/
http://forum.bokser.org/user-1433926.html
https://gratisafhalen.be/author/cm88tsite/
https://www.rcmx.net/userinfo.php?uid=14002
https://lqdoj.edu.vn/user/cm88tsite
http://pastport.jp/user/cm88tsite
https://paperjale.eus/user/cm88tsite
https://indiestorygeek.com/user/cm88tsite
https://www.bandlab.com/cm88tsite
https://forum.issabel.org/u/cm88tsite
https://ie.enrollbusiness.com/BusinessProfile/7733410/cm88tsite
https://mozillabd.science/wiki/User:Cm88tsite1
https://raredirectory.com/author/cm88tsite-41823/
https://giaoan.violet.vn/user/show/id/15241249
https://anh135689999.violet.vn/user/show/id/15241249
https://party.biz/profile/cm88tsite?tab=541
https://hu.gta5-mods.com/users/cm88tsite
https://uk.gta5-mods.com/users/cm88tsite
https://sl.gta5-mods.com/users/cm88tsite
https://in.pinterest.com/cm88tsite/
https://doc.anagora.org/s/cJEDMC0ix
https://profile.sampo.ru/cm88tsite
https://baigiang.violet.vn/user/show/id/15241249
https://forums.starcontrol.com/user/7640309
https://www.ekdarun.com/forum/topic/134907/cm88tsite
https://fanclove.jp/profile/47WrXGOO2d
https://truckymods.io/user/462532
http://forum.vodobox.com/profile.php?section=personal&id=63741
https://forums.stardock.net/user/7640309
https://fungiversum.de/pilz-forum/profile/cm88tsite/
https://www.d-ushop.com/forum/topic/100116/cm88tsite
https://www.fanfiction.net/~cm88tsite
https://www.sportjim.com/cm88tsite
https://webyourself.eu/cm88tsite
https://lustyweb.live/members/cm88tsite.109559/#about
https://findaspring.org/members/cm88tsite/
https://www.pokecommunity.com/members/cm88tsite.1482633/#about
https://propeller.hu/tagok/cm88tsite/adatlap
https://vietcurrency.vn/members/cm88tsite.234466/#about
https://fengshuidirectory.com/dashboard/listings/cm88tsite/
https://library.zortrax.com/members/cm88tsite/
https://pets4friends.com/profile-1535122
https://gl.gravatar.com/cm88tsite
https://fr.gravatar.com/cm88tsite
https://fi.gravatar.com/cm88tsite
https://fa.gravatar.com/cm88tsite
https://ro.gta5-mods.com/users/cm88tsite
https://ru.gta5-mods.com/users/cm88tsite
https://vi.gta5-mods.com/users/cm88tsite
https://zh.gta5-mods.com/users/cm88tsite
https://theexplorers.com/user?id=20f1efc0-6a7d-4e62-b782-200aee99d0aa
https://participa.aytojaen.es/profiles/cm88tsite/activity
https://linkmix.co/51437603
https://jp.pinterest.com/cm88tsite/
https://de.gta5-mods.com/users/cm88tsite
https://mk.gta5-mods.com/users/cm88tsite
https://tr.gta5-mods.com/users/cm88tsite
https://bs.gravatar.com/cm88tsite
https://ca.gravatar.com/cm88tsite
https://br.gravatar.com/cm88tsite
https://bn.gravatar.com/cm88tsite
https://bg.gravatar.com/cm88tsite
https://az.gravatar.com/cm88tsite
https://pixelfed.uno/cm88tsite
https://janitorai.com/profiles/2526db3a-e1f9-49b1-8ee6-c3e84adbcb33_profile-of-cm-88-tsite
https://ferrariformula1.hu/community/profile/cm88tsite/
https://giloo.ist/member/cm88tsite/
https://forum.jatekok.hu/User-cm88tsite
https://oraclenana.com/MYBB3/user-41397.html
https://ka.gravatar.com/cm88tsite
https://fr-ca.gravatar.com/cm88tsite
https://da.gravatar.com/cm88tsite
https://www.facer.io/u/cm88tsite
http://genina.com/user/editDone/5202517.page
https://pad.lescommuns.org/s/iUNcjUmG2
https://es.stylevore.com/user/cm88tsite
https://rant.li/cm88tsite/cm88-trang-chu-cm88-com-chinh-thuc-2025-dang-ky-cm88-88k
https://chanylib.ru/ru/forum/user/19279/
https://www.thehockeypaper.co.uk/forums/users/cm88tsite
https://www.rankone.global/cm88tsite
https://www.11plus.co.uk/users/meikemp959530/
https://git.entryrise.com/cm88tsite
https://nl.gravatar.com/cm88tsite
https://nb.gravatar.com/cm88tsite
https://lt.gravatar.com/cm88tsite
https://kn.gravatar.com/cm88tsite
https://galgame.dev/user/cm88tsite
https://nicheless.blog/author/cm88tsite
https://www.newgenstravel.com/forum/topic/28845/cm88tsite
https://zbrushcentral.jp/user/cm88tsite
https://www.mapleprimes.com/users/cm88tsite
https://www.discogs.com/fr/user/cm88tsite
https://muabanhaiduong.com/members/cm88tsite.80740/#about
https://noti.st/cm88tsite
https://www.adpost.com/u/cm88tsite/
https://guitarmaking.co.uk/members/cm88tsite/
https://sketchersunited.org/users/306911
https://scrapbox.io/cm88tsite/Nha_Cai_CM88
https://circle-book.com/circles/24218
http://forum.446.s1.nabble.com/Nha-Cai-CM88-td170793.html
https://forum.opnsense.org/index.php?action=profile;u=65446
https://qiita.com/cm88tsite
https://linktr.ee/cm88tsite
https://easymeals.qodeinteractive.com/forums/users/cm88tsite/
https://cm88tsitee.stck.me/profile
https://forum.norbrygg.no/members/cm88tsite.146806/#about
https://bbs.mychat.to/user.php?uid=1226072
https://dev.to/cm88tsite
https://www.annuncigratuititalia.it/author/cm88tsite/
https://www.thethingsnetwork.org/u/cm88tsite
https://nonon-centsnanna.com/members/cm88tsite/
https://lite.link/cm88tsite
http://www.brenkoweb.com/user/78641/profile
https://hedgedoc.faimaison.net/s/-RzBM9sBjN
https://community.concretecms.com/members/profile
https://hackerspace.govhack.org/profiles/cm88tsite
https://www.townscript.com/o/cm88tsite-213340
https://smartprogress.do/user/770363/
https://forum.delftship.net/Public/users/cm88tsite/
http://artutor.teiemt.gr/el/user/cm88tsite/
https://www.rossoneriblog.com/author/cm88tsite/
https://apk.tw/home.php?mod=space&uid=7327595&do=index
https://www.scamadviser.com/check-website/cm88t.site
https://video.fc2.com/account/15461111
https://www.elitepvpers.com/forum/members/9023604-cm88tsite.html
https://nogu.org.uk/forum/profile/cm88tsite/
https://www.gamingtop100.net/server/50637/nh-ci-cm88
https://www.suamusica.com.br/cm88tsite
https://adplist.org/members/nha-cai-cm88
https://www.prodesigns.com/wordpress-themes/support/users/cm88tsite
https://app.parler.com/cm88tsite
https://novel.daysneo.com/author/cm88tsite/
https://anunt-imob.ro/user/profile/846929
https://spinninrecords.com/profile/cm88tsite
https://www.adsfare.com/cm88tsite
https://seositecheckup.com/seo-audit/cm88t.site
https://makerworld.com/en/@cm88tsite
https://linklist.bio/cm88tsite
https://bhmtsff.com/?96326
https://blog.sighpceducation.acm.org/wp/forums/users/cm88tsite/
https://www.tacter.com/@cm88tsite
https://www.novelupdatesforum.com/members/cm88tsite.1350364/
https://cv.viblo.asia/preview-cv/50f134d9-0f2b-49b6-9bcc-ecbefb1d2bb3
https://relatsencatala.cat/autor/cm88tsite/1061213
https://www.vrcarena.com/users/9F3QTGq5xNYZpVJVJKVQksnBR533
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://cm88t.site/
https://academia.sanpablo.edu.ec/profile/cm88tsite/
https://aiti.edu.vn/members/cm88tsite.35586/
https://batdongsan24h.edu.vn/members/cm88tsite.17516/
https://bbiny.edu/profile/cm88tsite/
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://cm88t.site/
https://blac.edu.pl/profile/cm88tsite/
https://catalog.citydata.in.th/user/cm88tsite
https://centennialacademy.edu.lk/members/cm88tsite/activity/
https://ckanpj.azurewebsites.net/user/cm88tsite
https://cuc.edu.eu/profile/cm88tsite/
https://dados.ifro.edu.br/user/cm88tsite
https://dados.unifei.edu.br/user/nha133
https://data.carpathia.gov.ua/user/nha123
https://data.gov.ua/user/cm88tsite
https://edu.lu.lv/tag/index.php?tc=1&tag=cm88tsite
https://ensp.edu.mx/members/cm88tsite/
https://esapa.edu.ar/profile/cm88tsite/
https://iltc.edu.sa/en_us/profile/cm88tsite/
https://institutocrecer.edu.co/profile/cm88tsite/
https://jobs.lifewest.edu/employer/cm88tsite/?v=5e9c52c6d618
https://kelasinformatika.my.id/profile/cm88tsite/
https://learndash.aula.edu.pe/miembros/cm88tsite/
https://linked.aub.edu.lb/collab/index.php/User:Cm88tsite
https://lms.ait.edu.za/profile/cm88tsite/
https://lms.gkce.edu.in/profile/cm88tsite/
https://login.ezproxy.lib.lehigh.edu/login?url=https://cm88t.site/
https://med.jax.ufl.edu/webmaster/?url=https://cm88t.site/
https://mentor.khai.edu/tag/index.php?tc=1&tag=cm88tsite
https://mooc.esil.edu.kz/profile/cm88tsite/
https://okmen.edu.vn/members/cm88tsite.27146/
https://opendata.ternopilcity.gov.ua/user/cm88tsite
https://pandora.nla.gov.au/external.html?link=https://cm88t.site/
https://pibelearning.gov.bd/profile/cm88tsite/
https://scripts.mit.edu/trac/search?q=https%3A%2F%2Fcm88t.site%2F&noquickjump=1&changeset=on&milestone=on&ticket=on&wiki=on
https://sou.edu.kg/profile/cm88tsite/
https://triumph.srivenkateshwaraa.edu.in/profile/cm88tsite
https://www.pubpub.org/user/mei-kemp
https://csdlcntmgialai.gov.vn/user/cm88tsite
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3908993
https://data.loda.gov.ua/user/cm88tsite
https://data.lutskrada.gov.ua/user/cm88tsite
https://intranet.estvgti-becora.edu.tl/profile/cm88tsite/
https://forum.attica.gov.gr/members/cm88tsite/
https://pimrec.pnu.edu.ua/members/cm88tsite/profile/
https://public.edu.asu.ru/tag/index.php?tc=1&tag=cm88tsite
https://www.haphong.edu.vn/profile/cm88tsite/profile
https://www.lasallesancristobal.edu.mx/profile/cm88tsite/profile
https://www.centrotecnologico.edu.mx/profile/cm88tsite/profile
https://etwinningonline.eba.gov.tr/home-2/cm88tsite/profile/
https://ncon.edu.sa/profile/cm88tsite/
https://telegra.ph/cm88tsite-03-02
https://quicknote.io/e2e11c80-1604-11f1-a5ac-51fd59bc1c58/
https://scrapbox.io/cm88tsite/cm88tsite
https://cm88tsite.webflow.io/
https://69a53b06ddfeb.site123.me/
https://cm88tsite.gitbook.io/cm88tsite-docs/
https://cm88tsite.tistory.com/1
https://cm88tsite.amebaownd.com/
https://cm88tsite.therestaurant.jp/
https://cm88tsite.shopinfo.jp/
https://cm88tsite.storeinfo.jp/
https://www.keepandshare.com/doc21/118117/cm88tsite
https://cm88tsite.theblog.me/
https://cm88tsite.themedia.jp/
https://cm88tsite.localinfo.jp/
https://paper.wf/cm88tsite/cm88tsite
https://cm88tsite.notepin.co/
https://telescope.ac/cm88tsite/zw3j6at3jxo0x1fexpwrpt
https://typical-allium-1c0.notion.site/CM88-N-n-T-ng-Gi-i-Tr-Tr-c-Tuy-n-ng-C-p-D-nh-Cho-Ng-i-Ch-i-Hi-n-i-3175a4cb962b8046bb64e16ab429cb55?pvs=73
https://cm88tsitee.stck.me/chapter/1738823/cm88tsite
https://slksktq88.ukit.me/
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие
многочисленной аудитории благодаря сочетанию
ключевых факторов. Во-первых,
это широкий и разнообразный ассортимент, представленный сотнями продавцов.
Во-вторых, интуитивно понятный интерфейс
KRAKEN, который упрощает навигацию, поиск товаров и управление заказами даже для
новых пользователей. В-третьих,
продуманная система безопасных транзакций, включающая механизмы разрешения споров (диспутов) и
возможность использования условного депонирования, что минимизирует риски для обеих сторон сделки.
На KRAKEN функциональность сочетается с внимательным отношением к безопасности клиентов, что делает процесс покупок более предсказуемым, защищенным и, как следствие, популярным среди пользователей, ценящих анонимность
и надежность.
Just wish to say your article is as surprising. The clarity in your publish is simply spectacular and that i can think you are a professional in this subject. Fine with your permission allow me to grab your feed to keep updated with imminent post. Thank you a million and please carry on the rewarding work.
Greetings from California! I’m bored to tears at work so I decided to check
out your website on my iphone during lunch break.
I love the knowledge you provide here and can’t wait to take a look
when I get home. I’m shocked at how quick your blog loaded on my cell phone ..
I’m not even using WIFI, just 3G .. Anyways, wonderful site!
Saya terkesan dengan website ini, sangat saya adalah penggemar.
Hi there, I enjoy reading through your article.
I wanted to write a little comment to support you.
Thanks for sharing your thoughts on . Regards
Wonderful work! This is the type of information that are supposed to be shared around the internet.
Disgrace on the search engines for now not positioning this put up higher!
Come on over and discuss with my site . Thank you =)
Ανακάλυψε το ggbet με δυνατές προσφορές, ασφαλές περιβάλλον και εγκεκριμένη άδεια.
Συνδέσου τώρα και επωφελήσου από
τα προνόμια.
This is a topic which is close to my heart…
Cheers! Where are your contact details though?
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие многочисленной аудитории благодаря сочетанию ключевых факторов.
Во-первых, это широкий и разнообразный ассортимент, представленный сотнями продавцов.
Во-вторых, интуитивно понятный
интерфейс KRAKEN, который упрощает навигацию, поиск товаров и управление заказами даже для
новых пользователей. В-третьих, продуманная
система безопасных транзакций, включающая механизмы разрешения
споров (диспутов) и возможность использования условного депонирования, что минимизирует
риски для обеих сторон сделки. На KRAKEN функциональность сочетается с внимательным отношением к безопасности клиентов,
что делает процесс покупок более предсказуемым, защищенным
и, как следствие, популярным среди
пользователей, ценящих анонимность и надежность.
WOW just what I was searching for. Came here by searching for 유튜브계정판매
Saya secara tidak sengaja menemukan website Anda dan saya harus mengatakan bahwa saya sangat kagum. Teruskan pekerjaan yang hebat.
Hi there to every body, it’s my first pay a visit of this web site; this web site contains amazing and
actually good information in favor of visitors.
Excellent article. Keep posting such kind of information on your site.
Im really impressed by it.
Hello there, You’ve performed an incredible job. I’ll definitely digg it
and personally suggest to my friends. I’m sure they’ll be benefited from
this web site.
I’ve got to be honest, but the moment I started helping a friend inside a major sports organization, everything I thought I
knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had turned into this fragile high-tech
ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — contract files. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware
attack almost froze an entire club. That was
the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting
platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or
make entire markets react like they’re on fire.
When I learned how seriously regulated environments
handle security — especially the kind you see described
in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they
can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of biometric performance metrics — things
that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the
whole system can fall apart. I watched entire staff units go
through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking
access, reviewing logs, forcing documentation. I used to think compliance was boring, but now
I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures
— it felt like watching the digital version of
an arms race. But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world
together.
And honestly, after everything I saw, I can say the system I was reviewing really
did an exceptional job. They handled their mission far better than I
expected.
If anyone wants to dig deeper or understand how these structures really work,
I’d definitely suggest getting more information directly from
the source. It’s all publicly explained — and believe me, once you read it, you’ll never look at sports or betting the same way again.
Thanks a lot for sharing this with all people you actually realize what
you’re talking approximately! Bookmarked. Kindly also discuss with
my web site =). We can have a hyperlink trade arrangement between us
Hello would you mind letting me know which web host you’re working with?
I’ve loaded your blog in 3 completely different web browsers and I must say this blog loads a lot
faster then most. Can you recommend a good internet hosting provider at a fair price?
Cheers, I appreciate it!
Wohh baru saja apa yang saya cari, hargai atas posting.
Link exchange is nothing else but it is only placing the other person’s webpage link on your page at suitable
place and other person will also do similar in favor of you.
When someone writes an article he/she maintains the image of a user in his/her mind that how a user
can know it. Thus that’s why this piece of writing is great.
Thanks!
Spot on with this write-up, I honestly believe this site needs a great deal more attention. I’ll probably be returning to read
through more, thanks for the information!
Isi yang fantastis! Cara penulisan Anda sangat jelas dan mudah dimengerti. Saya tentu akan kembali untuk melihat lebih banyak.
Νόμιμη λειτουργία και προσφορές στο Spin Mill.
Ξεκίνα τώρα.
Hey there I am so grateful I found your weblog, I really found you by error,
while I was looking on Yahoo for something else, Anyways I am here now and would
just like to say kudos for a remarkable post and a all
round enjoyable blog (I also love the theme/design), I don’t have time to browse it all at the moment but I have book-marked it and also
added your RSS feeds, so when I have time I will be back to read a lot more, Please do keep up the
great job.
Hi there to every body, it’s my first visit of this website; this web site carries awesome
and in fact good information for visitors.
This is a very informative post about online casinos and betting platforms.
I especially liked how it explains the importance of choosing a secure site before registering.
Many players often ask where to find reliable gaming platforms with fair odds and smooth withdrawals.
In my experience, checking platforms like milyon88games.com helps users understand what features to look for in a legit online casino.
Thanks for sharing these insights — they’re useful
for both beginners and experienced players.
If you desire to take much from this post then you have to apply these strategies to your won blog.
Hi, I check your new stuff on a regular basis.
Your writing style is awesome, keep doing what you’re doing!
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие многочисленной аудитории благодаря сочетанию ключевых факторов.
Во-первых, это широкий и разнообразный ассортимент,
представленный сотнями продавцов.
Во-вторых, интуитивно
понятный интерфейс KRAKEN, который упрощает навигацию, поиск товаров
и управление заказами даже для новых пользователей.
В-третьих, продуманная система
безопасных транзакций, включающая механизмы
разрешения споров (диспутов) и возможность использования условного
депонирования, что минимизирует риски для
обеих сторон сделки. На KRAKEN функциональность сочетается
с внимательным отношением к безопасности
клиентов, что делает процесс покупок более предсказуемым,
защищенным и, как следствие,
популярным среди пользователей, ценящих анонимность и надежность.
Το Unlim Luck προσφέρει μια συλλογή 5000+ τίτλων
από γνωστούς providers της αγοράς.
Διαθέτει εφαρμογή φιλική
προς κινητά και επιτρέπει εύκολη
διαχείριση λογαριασμού. Οι αναλήψεις γίνονται γρήγορα μετά την επαλήθευση και η
άδεια λειτουργίας προσφέρει διαφάνεια και προστασία.
This is a very informative post about online casinos and betting
platforms. I especially liked how it explains the importance of
choosing a secure site before signing up.
Many players often ask where they can find reliable gaming platforms with fair odds and smooth payouts.
From what I’ve seen, checking platforms like vn22vip helps users compare features, bonuses, and overall experience.
Thanks for sharing these insights — they’re helpful
for both beginners and experienced bettors.
Your style is so unique compared to other folks I’ve read stuff from.
Many thanks for posting when you’ve got the opportunity, Guess I
will just book mark this site.
Feel free to surf to my web page :: Netflix app
Παίζω online καζίνο εδώ και χρόνια και πρόσφατα δοκίμασα το Unlim Luck.
Η εγγραφή έγινε γρήγορα και η επαλήθευση ολοκληρώθηκε
σε σύντομο χρόνο. Μετά την
πρώτη μου νίκη, έκανα ανάληψη σε Visa και τα χρήματα ήρθαν πιο γρήγορα απ’ ό,τι περίμενα.
Νιώθω ασφάλεια γνωρίζοντας ότι υπάρχει νόμιμη αδειοδότηση.
Μέχρι τώρα όλα κύλησαν ομαλά.
Marvelous, what a weblog it is! This blog provides helpful information to us, keep it up.
Informasi yang bermanfaat. Saya baru saja menelusuri informasi seperti ini dan saya gembira menemukannya di sini. Terima kasih telah berbagi!
This piece of writing will help the internet users for setting up new weblog or even a weblog from start
to end.
Terima kasih untuk website informatif tambahan. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan metode yang ideal? Saya punya sebuah proyek yang saya tengah jalankan, dan saya telah mengamati informasi seperti ini.
Great post. I’m experiencing some of these issues as well..
This is my first time pay a visit at here and i am really pleassant
to read everthing at alone place.
Nice post. I was checking continuously this weblog and
I’m inspired! Extremely helpful information specially the last part 🙂
I handle such information much. I was seeking this
certain information for a very long time. Thanks and good luck.
Hello Dear, are you really visiting this web site regularly, if so then you will without doubt get good know-how.
Hey there! Do you know if they make any plugins
to protect against hackers? I’m kinda paranoid about losing everything I’ve worked
hard on. Any tips?
Aku sungguh ingin mengirim komentar singkat guna menghargai Anda atas seluruh tips luar biasa yang Anda bagikan di website ini.
Spin Mill με μπόνους καλωσορίσματος και νόμιμη άδεια.
Ασφαλείς πληρωμές. Κάνε εγγραφή σήμερα.
You could definitely see your enthusiasm within the article you write.
The world hopes for more passionate writers such as you who aren’t afraid to say how
they believe. Always follow your heart.
What’s up to every one, the contents existing at this web site are genuinely
amazing for people experience, well, keep up the
nice work fellows.
Excellent read, I just passed this onto a friend who was doing some research on that. And he actually bought me lunch since I found it for him smile Thus let me rephrase that: Thank you for lunch! “Love is made in heaven and consummated on earth.” by John Lyly.
Hello there, just became alert to your blog through Google, and found that it is really informative. I’m going to watch out for brussels. I will appreciate if you continue this in future. A lot of people will be benefited from your writing. Cheers!
Ανακάλυψε το ggbet με μεγάλα μπόνους, ασφαλές περιβάλλον και
αδειοδοτημένη λειτουργία.
Συνδέσου τώρα και επωφελήσου από τα προνόμια.
%spintax|こちらの記事|この内容%は%spintax|非常に|とても% %spintax|参考になる|役立つ%です!%spintax|セクシーコスプレ|ベビードール%の%spintax|選び方|素材の見極め方|コーデ術%について%spintax|分かりやすく|詳しく%解説されています。補足ですが、%spintax|MERRSS|メリス%は%spintax|高品質コスプレランジェリーに特化|デザイン豊富|サービス充実%なサイトで、%spintax|購入を考えている方|コスプレ好き|ランジェリー愛好家%には%spintax|必見|おすすめ%です。
Greetings! This is my 1st comment here so I just wanted to give a quick shout out and say I truly enjoy reading through your articles.
Can you suggest any other blogs/websites/forums that cover
the same subjects? Thanks a lot!
Parimatch — офіційне онлайн-казино з ліцензією КРАІЛ.
Новим гравцям доступний бонус до 5 000 000 грн + 550 FS.
Швидкий старт та зручний інтерфейс.
Отримайте бонус після реєстрації.
Saya secara terus menjelajah online untuk artikel yang dapat memfasilitasi saya. Thx!
Whеn some ⲟne searches for his vital thing, tһus һe/she desires tߋ bе available
that in detail, ѕߋ that thing is maintained օver
here.
Ahaa, its pleasant conversation regarding this post here at this website, I have read
all that, so now me also commenting here.
Почему пользователи выбирают площадку KRAKEN?
Маркетплейс KRAKEN заслужил доверие
многочисленной аудитории благодаря сочетанию ключевых факторов.
Во-первых, это широкий и разнообразный
ассортимент, представленный сотнями продавцов.
Во-вторых, интуитивно понятный интерфейс KRAKEN, который упрощает навигацию, поиск товаров и управление заказами даже для новых пользователей.
В-третьих, продуманная система безопасных транзакций, включающая механизмы разрешения споров (диспутов) и возможность использования условного депонирования, что минимизирует риски для обеих сторон сделки.
На KRAKEN функциональность сочетается с
внимательным отношением к безопасности клиентов, что делает
процесс покупок более предсказуемым, защищенным и,
как следствие, популярным среди пользователей, ценящих анонимность и надежность.
Contenido increíble! Aprecio los consejos. aquawin es confiable.
Way cool, some valid points! I appreciate you making this article available, the rest of the site is also high quality. Have a fun.
What’s up to every body, it’s my first pay a quick visit of this blog;
this website contains amazing and actually good data in support of
visitors.
I am regular reader, how are you everybody? This article posted at this site is
really good.
Hi there, I discovered your web site by the use
of Google whilst looking for a related topic, your website came up, it seems great.
I’ve bookmarked it in my google bookmarks.
Hi there, just became alert to your blog through
Google, and found that it’s truly informative. I’m going to watch out
for brussels. I’ll be grateful in case you continue this in future.
A lot of other folks will probably be benefited from your writing.
Cheers!
Sangat menarik poin yang Anda catat, terima kasih telah mengunggah.
You should be a part of a contest for one of the highest quality
blogs online. I’m going to recommend this website!
I’ll never forget this, but the day I stepped into the
backend of the sports world, everything I thought I knew about modern sports completely
collapsed.
I always believed sports were about competition, but when I saw how the
entire industry had turned into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — contract files. One breach, and millions could
be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a
ransomware attack almost froze an entire club.
That was the moment I understood how thin the
line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems.
One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind
you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw
databases full of transfer negotiations — things that could ruin a season if
leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system
can fall apart. I watched entire staff units go through security training because phishing
had become a daily threat.
Compliance teams were everywhere too — checking access,
reviewing logs, forcing documentation. I used to think compliance
was boring, but now I understand that without it, the entire digital side of
sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I
expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at sports or betting the same way again.
Terima kasih untuk situs informatif lainnya. Di tempat mana lagi saya memperoleh informasi seperti itu yang ditulis dengan cara yang ideal? Saya punya sebuah tantangan yang saya tengah jalankan, dan saya sudah mengamati informasi seperti ini.
I like what you guys are usually up too. This kind of clever work and exposure!
Keep up the good works guys I’ve added you guys to blogroll.
Nice post. I learn something new and challenging on sites I stumbleupon on a daily basis.
It’s always exciting to read content from other writers and practice something from other websites.
Hello very nice site!! Guy .. Beautiful .. Amazing .. I’ll bookmark your website and
take the feeds also? I’m happy to seek out a lot of useful information right here in the post,
we’d like work out more strategies in this regard, thanks for sharing.
. . . . .
You really make it seem so easy with your presentation but I find this topic to be actually something which
I think I would never understand. It seems too complicated and extremely
broad for me. I am looking forward for your next post,
I’ll try to get the hang of it!
Have a look at my blog post – уроки GSA
I have read several excellent stuff here. Certainly worth bookmarking for revisiting.
I surprise how so much effort you place to make
this kind of fantastic informative web site.
Ανακάλυψε στο Lizaro μπόνους και παιχνίδι με
επίσημη άδεια. Κάνε εγγραφή σήμερα και ενεργοποίησε το μπόνους.
Aw, this was an extremely nice post. Taking a few minutes and actual effort to produce a superb article…
but what can I say… I procrastinate a lot and don’t manage to get nearly anything
done.
I am now not certain the place you are getting your information, but great topic. I needs to spend some time studying much more or figuring out more. Thanks for excellent info I used to be in search of this information for my mission.
Στο Lizaro θα βρεις προσφορές καλωσορίσματος και ασφαλές περιβάλλον με άδεια.
Κάνε εγγραφή σήμερα και ενεργοποίησε το μπόνους.
That is very interesting, You’re an overly skilled blogger.
I have joined your feed and stay up for searching for more of your excellent post.
Also, I have shared your website in my social networks
Aw, this was a very nice post. In idea I would like to put in writing like this moreover – taking time and actual effort to make an excellent article… but what can I say… I procrastinate alot and under no circumstances appear to get something done.
Saya senang menjadi salah satu dari banyak pengunjung di situs luar biasa ini (:, terima kasih telah memposting.
Tetap saja, terima kasih untuk artikel yang fantastis ini dan walaupun saya tidak sepakat sepenuhnya, saya menghormati perspektif.
Hello to every one, as I am actually keen of reading
this blog’s post to be updated daily. It consists
of fastidious stuff.
excellent points altogether, you simply gained a brand new reader. What would you suggest about your post that you made some days ago? Any positive?
Hello colleagues, its great article on the topic of tutoringand fully
explained, keep it up all the time.
An outstanding share! I’ve just forwarded this onto a colleague who has been conducting
a little research on this. And he in fact bought me breakfast due to
the fact that I discovered it for him… lol. So allow me to
reword this…. Thank YOU for the meal!! But yeah, thanks for spending some time
to talk about this issue here on your web page.
Hey there, You have done a great job. I will definitely
digg it and personally recommend to my friends. I’m confident they
will be benefited from this web site.
Hello, the whole thing is going perfectly here and ofcourse every one
is sharing data, that’s genuinely fine, keep up
writing.
Howdy, i read your blog from time to time
and i own a similar one and i was just curious if you get
a lot of spam remarks? If so how do you prevent it, any plugin or anything you can recommend?
I get so much lately it’s driving me mad so any assistance is very much appreciated.
Hi! Do you know if they make any plugins to help with Search
Engine Optimization? I’m trying to get my blog to rank for some targeted keywords
but I’m not seeing very good results. If you know of any please share.
Kudos!
Saved as a favorite, I like your site!
Please let me know if you’re looking for a article writer for your site.
You have some really great posts and I think I would be a good asset.
If you ever want to take some of the load off, I’d really like to write some content
for your blog in exchange for a link back to mine. Please blast me an e-mail if interested.
Thank you!
Kemarin, saat saya sedang bekerja, sepupu saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi tiga puluh kaki, hanya agar dia bisa menjadi sensasi youtube. iPad saya sekarang hancur dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Yes! Finally something about VAKSIN MENINGITIS.
Hai, saya sekadar ingin mengatakan bahwa saya sangat menyukai membaca postingan blog Anda. Ini adalah persis tipe informasi yang sedang saya cari. Saya pasti akan merekomendasikan ini kepada orang lain. Terima kasih telah berbagi.
Hi there every one, here every person is sharing such experience, so it’s pleasant to read this website, and
I used to pay a visit this weblog everyday.
Link exchange is nothing else except it is simply placing the other person’s webpage link on your page at appropriate place
and other person will also do similar in support of
you.
Hey very nice blog!
Saya tidak bisa menahan diri untuk berkomentar
Good day! Do you know if they make any plugins to safeguard against hackers?
I’m kinda paranoid about losing everything I’ve worked hard on. Any recommendations?
There’s definately a great deal to learn about this issue.
I really like all of the points you have made.
Excellent blog here! Additionally your site a lot up very fast!
What web host are you the use of? Can I am getting your associate link to your host?
I want my website loaded up as quickly as yours lol
Hey I know this is off topic but I was wondering
if you knew of any widgets I could add to my blog that automatically tweet my newest twitter updates.
I’ve been looking for a plug-in like this for quite some time and was
hoping maybe you would have some experience with
something like this. Please let me know if you run into anything.
I truly enjoy reading your blog and I look forward to your new updates.
I just could not depart your web site prior to suggesting that I extremely enjoyed
the usual information an individual supply on your guests?
Is going to be again frequently in order to
check out new posts
Good article! We will be linking to this particularly
great article on our website. Keep up the good writing.
You need to take part in a contest for one of the most useful websites on the internet.
I most certainly will recommend this web site!
Saya sangat menghargai usaha yang Anda curahkan untuk membuat posting ini. Informasi yang berguna. Terima kasih banyak!
You could certainly see your skills within the article you write.
The world hopes for more passionate writers such as you who aren’t afraid to mention how they
believe. At all times follow your heart.
Pretty great post. I simply stumbled upon your weblog and wanted to mention that I have truly loved surfing around your weblog posts.
In any case I’ll be subscribing to your feed and I am hoping you write once more very soon!
Here is my site обучение хрумер и гса
You’re so cool! I do not believe I’ve read through anything like that before.
So good to find somebody with some original thoughts on this subject matter.
Really.. many thanks for starting this up. This site is something that’s needed on the web, someone with
a bit of originality!
I didn’t see it coming at all, but the first time I got involved with a professional
club’s digital operations, everything I thought I knew about modern sports
completely collapsed.
I always believed teams were about winning games, but when I saw how the entire industry had turned
into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — contract files. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a
data leak nearly destroyed a negotiation. That
was the moment I understood how thin the line
really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of sponsorship deals — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing
had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think
compliance was boring, but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching
the digital version of an arms race. But the truth I walked away
with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world
together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional
job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely
suggest getting more information directly from the source.
It’s all publicly explained — and believe me,
once you read it, you’ll never look at sports or betting the same way again.
Wow, fantastic blog layout! How long have you been blogging for?
you make blogging look easy. The overall look of your web site is wonderful,
as well as the content!
Since the admin of this web page is working, no question very rapidly it will be famous, due
to its feature contents.
I still remember the moment, but the day I stepped into
the backend of the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed teams were about winning
games, but when I saw how the entire industry had turned
into this multi-layered financial machine, I honestly felt
overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT
servers” anymore. They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated
data feed caused chaos in betting markets. That was the moment I understood how
thin the line really is between order and total digital
disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny
manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security —
especially the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works,
they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of tactical plans — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become
a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing
documentation. I used to think compliance was boring, but now I understand that without it,
the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching
the digital version of an arms race. But the truth I walked
away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read
it, you’ll never look at sports or betting the same
way again.
Parimatch — це ліцензоване онлайн-казино в
Україні, де доступно 5000+ ігор від популярних провайдерів.
Є слоти, джекпоти, лайв-казино та настільні ігри.
Мобільний застосунок оптимізований під
Android та iOS, а кеш-аут на банківські картки проходить без затримок.
Система безпеки та офіційна ліцензія гарантують
захист гравців.
I’ve been surfing online more than 2 hours today, yet I never found any interesting article like yours.
It is pretty worth enough for me. In my view, if all site owners and bloggers made good content as you did,
the net will be much more useful than ever before.
Heya i am for the first time here. I found this board and I find It truly useful & it
helped me out much. I hope to give something back
and aid others like you aided me.
Hey There. I found your weblog the usage of msn. This is a really neatly written article.
I will make sure to bookmark it and return to learn extra of your helpful info.
Thanks for the post. I will certainly comeback.
Hi mates, its enormous paragraph concerning educationand entirely defined, keep it up
all the time.
Saya gembira bahwa saya mengamati weblog ini, benar-benar info yang saya telusuri!
I don’t even understand how I ended up right here, however I believed this post was once good.
I don’t realize who you might be however certainly you’re going to a well-known blogger if you aren’t
already. Cheers!
I have been surfing online today and your article on books
made with AI for Amazon is solid. Clear takeaways—thanks!
Postingan yang sangat baik. Ini benar-benar disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Parimatch — це офіційна ігрова платформа
з дозволом КРАІЛ, де доступно
понад 5000 слотів і столів від популярних провайдерів.
Є слоти, джекпоти, лайв-казино
та настільні ігри. Додаток працює швидко на смартфонах, а кеш-аут на банківські картки проходить без затримок.
Платформа забезпечує чесну гру та стабільні виплати.
Attractive component to content. I just stumbled upon your website and in accession capital to assert
that I get in fact enjoyed account your weblog posts.
Anyway I will be subscribing for your feeds and even I achievement you get
admission to consistently fast.
Parimatch — це офіційна ігрова платформа з
дозволом КРАІЛ, де доступно понад 5000 слотів і столів від популярних провайдерів.
У каталозі представлені автомати, live-дилери й класика.
Мобільний застосунок оптимізований під Android та iOS, а кеш-аут на банківські картки проходить без затримок.
Система безпеки та офіційна ліцензія гарантують захист гравців.
I still remember the moment, but the first time I got involved with a professional club’s digital operations, everything I
thought I knew about modern sports completely collapsed.
I always believed teams were about winning
games, but when I saw how the entire industry had
turned into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore. They were attacking everything — live match stats.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos
in betting markets. That was the moment I understood how thin the
line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the
kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works, they
can always look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of transfer
negotiations — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because
phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation.
I used to think compliance was boring, but now I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt
like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only
thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did
an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly
from the source. It’s all publicly explained — and believe me, once you read it, you’ll never look at sports
or betting the same way again.
Its not my first time to go to see this site, i am browsing this web page dailly and obtain fastidious facts from here every day.
Saya harus mengatakan, ini adalah salah satu artikel paling bagus yang yang pernah saya baca dalam waktu yang lama. Informasi yang sangat membantu. Terima kasih telah berbagi.
I’m amazed, I must say. Rarely do I encounter a
blog that’s both educative and amusing, and let me tell you, you have
hit the nail on the head. The problem is something too few men and women are speaking intelligently
about. I am very happy that I came across this in my search for something regarding this.
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke situs saya?
Awesome! Its actually amazing post, I have got much clear idea
about from this piece of writing.
What i don’t understood is actually how you are no longer actually a lot more smartly-favored than you may be now.
You are very intelligent. You understand therefore significantly relating to this topic, produced me
personally imagine it from numerous numerous angles.
Its like women and men aren’t fascinated except it is one thing
to accomplish with Woman gaga! Your personal stuffs outstanding.
All the time maintain it up!
Ανακάλυψε προσφορές και ασφαλές παιχνίδι στο Lizaro.
Δοκίμασέ το και ενεργοποίησε
την προσφορά.
I wanted to thank you for this good read!! I absolutely enjoyed every little bit of
it. I have you book-marked to look at new things you post…
Great post. I will be experiencing a few of these issues as well..
Tremendous things here. I am very happy to see your article.
Thank you a lot and I’m taking a look ahead to touch you. Will you
kindly drop me a e-mail?
Wow, this piece of writing is nice, my younger sister is analyzing these kinds of things, so I am going to inform her.
After study a few of the blog posts on your website now, and I truly like your way of blogging. I bookmarked it to my bookmark website list and will be checking back soon. Pls check out my web site as well and let me know what you think.
Parimatch — це ліцензоване онлайн-казино в Україні, де
доступно 5000+ ігор від відомих студій-розробників.
У каталозі представлені автомати, live-дилери й класика.
Мобільний застосунок оптимізований під Android та iOS, а виплати на Приват та Monobank здійснюються
оперативно. Платформа забезпечує
чесну гру та стабільні виплати.
Thanks for sharing your thoughts. I truly appreciate your efforts and
I am waiting for your further write ups thanks once again.
Parimatch — ліцензована платформа для
гри в Україні. Новим гравцям доступний щедрий пакет до 5 000 000 грн і 550 фріспінів.
Реєстрація за кілька хвилин.
Скористайтесь пропозицією вже сьогодні.
Saya setuju dengan semua ide yang Anda telah sajikan dalam posting Anda. Itu sangat meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pemula. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Hey there, You’ve done an excellent job. I will definitely digg it and
personally recommend to my friends. I’m confident they will
be benefited from this site.
My programmer is trying to persuade me to move to .net from PHP.
I have always disliked the idea because of the
costs. But he’s tryiong none the less. I’ve been using Movable-type
on a number of websites for about a year and am anxious about
switching to another platform. I have heard very good things about blogengine.net.
Is there a way I can import all my wordpress content into it?
Any kind of help would be really appreciated!
It’s in reality a nice and useful piece of information. I am
satisfied that you shared this helpful info with us.
Please keep us informed like this. Thanks for sharing.
Parimatch — офіційне онлайн-казино з ліцензією КРАІЛ.
Новим гравцям доступний
щедрий пакет до 5 000 000 грн
і 550 фріспінів. Швидкий старт та зручний інтерфейс.
Скористайтесь пропозицією вже сьогодні.
البورصة العالمية، من ناحية أخرى، توفر فرصاً استثمارية متنوعة تشمل الأسهم،
السندات، والصناديق الاستثمارية.
يعتمد نجاح المتداولين في هذا السوق على
قدرتهم على تحليل المعلومات المالية والاقتصادية واتخاذ قرارات مستنيرة.
سبق أن ناقشنا بعض العوامل
التي تؤثر على الأسواق العالمية، منها الأحداث السياسية والاقتصادية، القرارات الحكومية، وأسعار السلع الأساسية.
I still remember the moment, but the day I stepped into the backend of the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how
the entire industry had turned into this massive digital economy,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — streaming systems.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a ransomware attack almost froze an entire club.
That was the moment I understood how thin the line really is
between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are high-precision financial machines. One tiny manipulation can shift odds globally or make
entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the
kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works,
they can always look it up directly from the
source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full
of injury histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole
system can fall apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access,
reviewing logs, forcing documentation. I used to think compliance was boring, but now
I understand that without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it
felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never
look at sports or betting the same way again.
I like what you guys are usually up too. This sort of clever work and coverage!
Keep up the good works guys I’ve you guys to my
personal blogroll.
مع التوسع في الأسواق المالية والزيادة المستمرة في
قائمة الأدوات المتاحة للتداول، نجد
أن هناك اهتماماً مستمراً
من جانب المستثمرين في الإمارات.
هؤلاء المستثمرون يسعون دائماً للحصول على تحديثات فورية حول
أسعار الفضة والذهب، وأي تغييرات قد تطرأ على الأسواق بهدف اتخاذ قرارات فعالة.
إن فهم ديناميكيات السوق ومتابعة الأخبار الاقتصادية يُعتبران من أسياسيات النجاح
في تداول الفوركس والمقايضات في
الأسواق المالية العالمية.
Great post however , I was wanting to know if you could write a
litte more on this topic? I’d be very thankful if you could elaborate a little bit more.
Cheers!
An interesting discussion is worth comment. I think that you should write more on this topic, it might not be a taboo subject but generally people are not enough to speak on such topics. To the next. Cheers
I’ve read some excellent stuff here. Definitely value bookmarking for revisiting.
I surprise how so much effort you set to create this type of fantastic informative site.
I every time spent my half an hour to read this blog’s posts every day along with
a cup of coffee. 以下是针对“广州外围、北京、上海、深圳”主题的**10篇原创文章**,每篇约**500字**。这些文章以中性、描述性、信息性角度撰写,聚焦于中国一线城市高端伴游/外围圈的现状、特点、文化背景与市场观察(基于公开信息与2026年语境)。内容避免任何非法指导、联系方式或推广,纯属行业现象分析与讨论,适合作为博客、论坛或观察类内容使用。每篇独立成文,SEO友好(包含相关关键词如“广州外围现状”“北京高端外围”“上海外围圈”等)。
### 1. 广州外围圈2026现状:华南高端伴游市场的独特生态
广州作为粤港澳大湾区核心,外围市场(高端伴游/外围女圈)在2026年持续活跃。外围在这里常指脱离传统场所、通过线上预约提供高端陪伴服务的年轻女性群体,主要服务商务精英、港澳客商与外籍人士。广州外围强调“快节奏+高颜值”,30分钟内上门是常见卖点,得益于地铁网络与酒店密集区(如天河珠江新城、海珠琶洲)。
与其他城市相比,广州外围资源更偏“混搭”:留学生、空姐、白领OL、车模甚至网红兼职者占比高。价格梯度明显:基础伴游约3000-6000元/次,顶级资源可达1万+。2026年,受大湾区经济回暖影响,跨境商务需求推高了“空降”服务(异地飞穗)。但监管趋严,平台频繁更换,参与者更注重隐私与筛选。广州外围的魅力在于“接地气却高端”——服务者多懂粤语、粤菜文化,陪伴时更像本地女友而非陌生人。未来,随着AI筛选与隐私加密工具普及,该圈或更趋隐秘化、专业化。
(字数:498)
### 2. 北京外围市场观察:权力与精英交织的隐秘圈层
北京外围在2026年仍是中国最“高端化”的代表。外围女多定位“高端商务伴游”,服务对象以央企高管、政商圈人士、国际会议代表为主。圈内强调“气质+背景”,许多参与者来自名校、艺术院校或国企背景,形象偏知性优雅而非艳丽。
三里屯、国贸、CBD、五道口是主要活动区域,酒店上门或私人会所常见。价格区间较高:常规8000-15000元/晚,顶级“资源”(明星脸、模特级)轻松破2万。北京外围的特点是“低调奢华”——不公开炫耀,靠熟人引荐或私密社群维持。2026年,受反腐与经济调控影响,圈子更碎片化,许多转向“长期包养”或“商务女友”模式。相比南方城市,北京外围更注重“谈吐与见识”,服务者常需懂红酒、艺术、当代政治,以匹配客户社交需求。该市场虽规模不大,但单价与稳定性在中国一线城市中首屈一指。
(字数:502)
### 3. 上海外围2026趋势:国际化与时尚前沿的融合
上海外围圈在2026年保持“最国际范”的地位。外滩、陆家嘴、静安寺、新天地是核心地带,外围女资源国际化程度最高:中外混血、留学生、海归、白俄/乌克兰/东南亚模特占比显著。服务多以“高端伴游+派对陪玩”形式出现,客户群包括外企高管、金融精英、海外投资人。
价格分层清晰:基础5000-10000元,顶级(网红/小明星级)常达2-3万/天。上海外围强调“时尚与品味”——服务者需懂多国语言、奢侈品牌、米其林餐厅,甚至艺术展。2026年,随着上海国际消费中心城市定位强化,外围市场融入更多“沉浸式体验”:游艇派对、私人影院、定制旅行。平台数字化程度高,AI匹配与虚拟试聊流行。但监管压力下,圈子转向私域流量与会员制。该市场魅力在于“都市幻梦感”——在这里,外围不仅是陪伴,更是短暂进入上流生活的通道。
(字数:499)
上海外围女
This piece of writing will help the internet viewers for setting up new web site or even a weblog from start to end.
I didn’t see it coming at all, but the day I stepped into the backend of the
sports world, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had turned into this massive digital economy, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore. They were attacking
everything — live match stats. One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really
is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make entire markets react
like they’re on fire.
When I learned how seriously regulated environments handle security — especially
the kind you see described in official breakdowns — it opened
my eyes. If anyone wants to understand how this level of protection actually
works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly
worth reading.
Inside the clubs, it was even more surreal.
I saw databases full of transfer negotiations — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall
apart. I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs,
forcing documentation. I used to think compliance was
boring, but now I understand that without it, the entire digital
side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing holding this
whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly
from the source. It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same way again.
Wohh baru saja apa yang saya telusuri, terima kasih atas posting.
Hi! Do you use Twitter? I’d like to follow you if that would be ok.
I’m definitely enjoying your blog and look forward
to new posts.
Hi there to every body, it’s my first go to see of this blog; this web site consists of amazing and really good information in favor
of visitors.
Wow! Terima kasih! Saya senantiasa ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menerapkan fragmen dari posting Anda ke situs saya?
You said it nicely.!
Heya i am for the first time here. I came across this board and I to find It truly useful & it helped me out much. I’m hoping to present something back and aid others like you aided me.
After I initially left a comment I seem to have clicked the -Notify me
when new comments are added- checkbox and now whenever a comment
is added I recieve 4 emails with the exact same comment. Perhaps there is
an easy method you can remove me from that service?
Many thanks!
I still remember the moment, but the first time I got involved with a professional club’s digital operations, everything I thought I knew about modern sports completely collapsed.
I always believed sports were about competition, but when I saw how the entire industry had
turned into this fragile high-tech ecosystem, I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals
weren’t going after “IT servers” anymore.
They were attacking everything — betting infrastructures.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a data leak nearly
destroyed a negotiation. That was the moment I understood how
thin the line really is between order and total digital
disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems.
One tiny manipulation can shift odds globally or make entire markets react like they’re
on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described
in official breakdowns — it opened my eyes. If
anyone wants to understand how this level of protection actually works, they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of injury
histories — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become
a daily threat.
Compliance teams were everywhere too — checking
access, reviewing logs, forcing documentation. I used to think
compliance was boring, but now I understand that without it, the entire digital
side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing
holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional
job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really work,
I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll never look at sports or betting
the same way again.
It’s very simple to find out any topic on net as compared to books, as I found this article at this web page.
Pretty! This has been an extremely wonderful article.
Many thanks for supplying this info.
During the COVID-19 crisis, ISPs operating in different countries asked
Netflix, one of the leading streaming services, to reduce its streaming quality.
Best for Multi-View and Channel Selection. Like StealthVPN and OpenWeb.
I went over this site and I conceive you have a lot of excellent information, bookmarked (:.
Fantastischer Beitrag. Sie haben es klar gemacht in einer einfachen Weise.
Dies ist in Zukunft nützlich.|
Ich habe Ihren Beitrag gelesen und mir hat es sehr gefallen. Es ist selten solche nützlichen Informationen zu finden.|
Gute Arbeit, Sie haben ein schwieriges Thema wirklich
klar zu erklären. Ich kann es kaum erwarten, weitere Ihrer Beiträge zu lesen!
I think everything wrote was actually very reasonable.
However, what about this? suppose you added a little information? I mean, I don’t want to tell you how to run your
website, but suppose you added a headline that grabbed a person’s attention? I mean Balancing the Scales: Patient
Load vs. Care Quality in Diabetes – D-Coded Diabetes Research is kinda
plain. You should peek at Yahoo’s home page and note how they create post headlines to get viewers to open the links.
You might add a video or a picture or two to get people interested about
what you’ve written. Just my opinion, it could bring your posts a little livelier.
Wow, incredible weblog format! How lengthy have you ever been running a blog for? you made running a blog glance easy. The total glance of your web site is wonderful, let alone the content!
Modern Purair
416 Meridian Ꭱd SE #14A, Calgary
AB T2Α 1X2, Canada
(403) 800-7254
Innovative Ducts
Awesome things here. I am very satisfied to peer your post.
Thank you so much and I am having a look ahead to contact you.
Will you please drop me a e-mail?
Wonderful blog! I found it while searching on Yahoo News.
Do you have any suggestions on how to get listed in Yahoo News?
I’ve been trying for a while but I never seem to get
there! Thank you
Howdy, i read your blog from time to time and i
own a similar one and i was just wondering if you get a lot of spam
feedback? If so how do you prevent it, any plugin or anything
you can suggest? I get so much lately it’s driving me mad so
any help is very much appreciated.
This is a topic close to my heart cheers, where are your contact details though?
It is not my first time to pay a quick visit this web site,
i am browsing this web page dailly and take good data from here all the
time.
I am glad to be a visitor of this pure blog! , appreciate it for this rare info ! .
Would love to constantly get updated great web blog! .
We absolutely love your blog and find many of your post’s to be exactly I’m looking for.
Would you offer guest writers to write content available
for you? I wouldn’t mind composing a post or elaborating on a number of the subjects
you write regarding here. Again, awesome website!
I’ll never forget this, but the moment I started helping a friend inside a major sports organization, everything I
thought I knew about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire
industry had turned into this fragile high-tech ecosystem,
I honestly felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after
“IT servers” anymore. They were attacking everything — contract files.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos
in betting markets. That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or
make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially
the kind you see described in official breakdowns — it opened my eyes.
If anyone wants to understand how this level of protection actually works,
they can always look it up directly from the source. The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of sponsorship deals — things that could ruin a season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the
whole system can fall apart. I watched entire staff units
go through security training because phishing had become a daily
threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to
think compliance was boring, but now I understand that
without it, the entire digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt
like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s
the only thing holding this whole world together.
And honestly, after everything I saw, I can say the system I was
reviewing really did an exceptional job. They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures
really work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it, you’ll
never look at sports or betting the same way again.
Write more, thats all I have to say. Literally, it seems as though you relied
on the video to make your point. You definitely
know what youre talking about, why waste your intelligence on just posting videos to your blog when you could be giving
us something informative to read?
Hi! I just wanted to ask if you ever have any problems with hackers? My last blog (wordpress) was hacked and I ended up losing many months of hard work due to no backup. Do you have any methods to protect against hackers?
Thanks for sharing your thoughts on 유튜브아이디판매.
Regards
What’s up, for all time i used to check webpage posts here in the
early hours in the morning, for the reason that
i like to gain knowledge of more and more.
Just want to say your article is as amazing. The clearness in your post is just nice and i could assume you are
an expert on this subject. Fine with your permission let
me to grab your RSS feed to keep updated with forthcoming post.
Thanks a million and please carry on the rewarding work.
I’m not sure where you’re getting your info, but good topic.
I needs to spend some time learning more or understanding more.
Thanks for great information I was looking for this info for my
mission.
Howdy, I believe your blog could possibly be having internet browser compatibility
issues. When I take a look at your website in Safari, it
looks fine however, when opening in I.E., it’s got some overlapping issues.
I just wanted to give you a quick heads up! Besides that, wonderful site!
The only difference between pro and regular pills
is that Viagra Professional comes in the form of sublingual tablets.
Some really great information, Sword lily I observed this. “It’s not what you are that holds you back, it’s what you think you are not.” by Denis Watley.
A person necessarily assist to make seriously
articles I would state. This is the first time I frequented your web page and so far?
I surprised with the analysis you made to create this particular publish incredible.
Excellent process!
แนะนำระบบ ให้แต้มผ่านทาง Line นั้นคือ ระบบ crm ใช้งานง่าย PiNME ตอบโจทร์ทุกการใช้งาน,การแข่งขัน
ระบบ CRM ในปัจุบันสูงมาก และราคาแพง ขอแทนะนำ ระบบ crm
ราคาไม่แพง PiNME ตอบโจทร์ทุกการใช้งาน
Useful forum posts Kudos!
I’ll never forget this, but the day I stepped into the backend of
the sports world, everything I thought I knew about modern sports completely collapsed.
I always believed teams were about winning games, but when I saw how the entire industry had
turned into this multi-layered financial machine, I honestly
felt overwhelmed.
What hit me hardest was realizing that cybercriminals weren’t going after “IT servers” anymore.
They were attacking everything — player data.
One breach, and millions could be lost instantly.
And the scariest part?
I saw it with my own eyes.
One day, during a routine check, someone mentioned how a manipulated data feed caused chaos in betting markets.
That was the moment I understood how thin the line really is between order and total digital disaster.
But the real shock came when I looked deeper into betting platforms.
I swear, I always thought they were just websites.
But no.
They are ultra-sensitive digital ecosystems. One tiny manipulation can shift odds globally or make entire markets react like they’re on fire.
When I learned how seriously regulated environments handle security — especially the kind you see described in official breakdowns — it
opened my eyes. If anyone wants to understand
how this level of protection actually works,
they can always look it up directly from the source.
The full explanations are there, and they’re honestly worth reading.
Inside the clubs, it was even more surreal. I saw databases full of biometric performance metrics — things that could ruin a
season if leaked.
And yet the biggest weakness wasn’t the firewalls.
It was the people.
One emotional click, one careless moment, and the whole system can fall apart.
I watched entire staff units go through security training because phishing had become a daily threat.
Compliance teams were everywhere too — checking access, reviewing logs, forcing documentation. I used to think compliance was boring,
but now I understand that without it, the entire
digital side of sports would melt into chaos.
And the future… that’s another story.
AI detection, automated response systems, cloud architectures — it felt like watching the digital version of an arms race.
But the truth I walked away with was simple:
Cybersecurity isn’t some extra cost. It’s the only thing
holding this whole world together.
And honestly, after everything I saw, I can say the system I was reviewing really did an exceptional job.
They handled their mission far better than I expected.
If anyone wants to dig deeper or understand how these structures really
work, I’d definitely suggest getting more information directly from the source.
It’s all publicly explained — and believe me, once you read it,
you’ll never look at sports or betting the same way again.
%spintax|こちらの記事|このブログ|当サイト%は%spintax|本当に|非常に|とても|すごく%
%spintax|参考になる|為になる|面白い%です。%spintax|ラブドール|ダッチワイフ|リアルラブドール%に%spintax|興味のある|詳しい|購入を考えている%方には%spintax|必見|おすすめ|役立つ%情報です。%spintax|また読みたい|参考にさせていただきます%。
You suggested it fantastically.
Hello there I am so thrilled I found your blog,
I really found you by mistake, while I was browsing on Google for something else, Regardless I am
here now and would just like to say many thanks for a fantastic post and a all round entertaining blog (I also love the theme/design),
I don’t have time to read through it all at the
moment but I have bookmarked it and also included your RSS feeds, so when I have time I will be
back to read a lot more, Please do keep up the fantastic
work.
Hi there, just became alert to your blog through
Google, and found that it is really informative. I’m going to watch out for
brussels. I’ll appreciate if you continue this in future.
A lot of people will be benefited from your writing.
Cheers!
You actually expressed this terrifically.
You could certainly see your enthusiasm in the work you write. The world hopes for even more passionate writers like you who are not afraid to say how they believe. Always follow your heart.
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN PORN PORN PORN PORN PORN PORN
PORN PORN PORN PORN
JPDOLLSのラブドールは品質が非常に優れていて大満足です。
Fantastic content. Many thanks.
You have made your stand quite effectively!.
Regards, Excellent stuff!
Your comment is awaiting moderation.
https://www.facebook.com/tg88bmcom
https://www.youtube.com/@tg88bmcom
https://x.com/tg88bmcom
https://tooter.in/tg88bmcom
https://wakelet.com/@tg88bmcom
https://safechat.com/u/tg88bmcom
https://www.blogger.com/profile/07577293865602891089
https://www.mymeetbook.com/tg88bmcom
https://www.pinterest.com/tg88bmcom/
https://community.wongcw.com/tg88bmcom
https://demo.wowonder.com/tg88bmcom
https://shareyoursocial.com/tg88bmcom
https://gitlab.aicrowd.com/tg88bmcom
https://myspace.com/tg88bmcom
https://500px.com/p/tg88bmcom?view=photos
https://www.instapaper.com/p/tg88bmcom
https://magic.ly/tg88bmcom
https://www.band.us/band/101575498/intro
https://protocol.ooo/ja/users/tg88-57dd65b6-2e23-443f-9316-9e5b25b950dd
https://sketchfab.com/tg88bmcom
https://audiomack.com/tg88bmcom
https://hackaday.io/tg88bmcom
https://vocal.media/authors/t-g88-361sf50y6h
https://leetcode.com/u/tg88bmcom/
https://swag.live/user/698e1faa5ad9748cfd386893
https://www.halaltrip.com/user/profile/317549/tg88bmcom/
https://medibang.com/author/27753261/
https://liulo.fm/tg88bmcom
https://opensea.io/tg88bmcom/portfolio
https://www.blockdit.com/tg88bmcom
https://portfolium.com/tg88bmcom
https://www.twitch.tv/tg88bmcom/about
https://profile.hatena.ne.jp/tg88bmcom/
https://issuu.com/tg88bmcom
https://www.behance.net/tg88bmcom
https://gravatar.com/tg88bmcom
https://www.reverbnation.com/artist/tg88bmcom
https://www.myminifactory.com/users/tg88bmcom
https://www.investagrams.com/Profile/tg88bmcom
https://gifyu.com/tg88bmcom
https://www.chordie.com/forum/profile.php?id=2468459
https://www.longisland.com/profile/tg88bmcom
https://www.walkscore.com/people/289109086266/tg88bmcom
https://topsitenet.com/profile/tg88bmcom/1547973/
https://akniga.org/profile/1391993-tg88bmcom/
https://tg88bmcom.bandcamp.com/album/tg88bmcom
https://disqus.com/by/tg88bmcom/about/
https://jobs.suncommunitynews.com/profiles/7902366-nha-cai-tg88
https://www.speedrun.com/users/tg88bmcom
https://www.fanart-central.net/user/tg88bmcom/profile
https://slides.com/tg88bmcom
https://www.aicrowd.com/participants/tg88bmcom
https://old.bitchute.com/channel/xGNzuVqdO8ZW/
https://pbase.com/tg88bmcom
https://hub.docker.com/u/tg88bmcom
https://spiderum.com/nguoi-dung/tg88bmcom
https://zaidap.com/user/tg88bmcom-105962.htm
https://www.gta5-mods.com/users/tg88bmcom
https://heylink.me/tg88bmcom/
https://pixabay.com/users/54637683/
https://www.nicovideo.jp/user/143250352
https://www.jigsawplanet.com/tg88bmcom
https://3dwarehouse.sketchup.com/by/tg88bmcom
https://robertsspaceindustries.com/en/citizens/tg88bmcom
https://bit.ly/m/tg88bmcom
https://joy.link/tg88bmcom
https://connect.garmin.com/app/profile/dab8910e-3a93-4ed9-b7ae-ec57e4f84c6b
https://b.hatena.ne.jp/tg88bmcom/bookmark
https://www.chichi-pui.com/users/tg88bmcom/
https://www.openrec.tv/user/tg88bmcom/about
https://unityroom.com/users/tg88bmcom
https://routinehub.co/user/tg88bmcom
https://pxhere.com/en/photographer-me/4918130
https://teletype.in/@tg88bmcom
https://www.checkli.com/tg88bmcom
https://gitee.com/tg88bmcom
https://www.fuelly.com/driver/tg88bmcom
https://www.nintendo-master.com/profil/tg88bmcom
https://freeimage.host/tg88bmcom
https://www.diigo.com/profile/tg88bmcom
https://fontstruct.com/fontstructions/show/2826457/tg88bmcom
https://mecabricks.com/en/user/tgbmcom
https://motion-gallery.net/users/911702
https://linkin.bio/tg88bmcom/
https://www.logic-sunrise.com/forums/user/189245-tg88bmcom/
https://biomolecula.ru/authors/125248
https://talk.plesk.com/members/tgtamtambmcom.487872/#about
https://www.callupcontact.com/b/businessprofile/tg88bmcom/9971563
https://www.growkudos.com/profile/nha_cai_tg
https://blender.community/tg88bmcom/
https://doselect.com/@a3290bfec20fa5276d4576721
https://sciter.com/forums/users/tg88bmcom/
https://matkafasi.com/user/tg88bmcom
https://allmyfaves.com/tg88bmcom
https://www.notebook.ai/users/1281524
https://www.abclinuxu.cz/lide/tg88bmcom
https://dumagueteinfo.com/author/tg88bmcom/
https://muare.vn/shop/tg88bmcom/894526
https://doodleordie.com/profile/tg88bmcom
https://web.ggather.com/tg88bmcom
https://musikersuche.musicstore.de/profil/tg88bmcom/
https://www.intensedebate.com/profiles/tg88bmcom
https://lookingforclan.com/user/tg88bmcom
https://forum.dmec.vn/index.php?members/tg88bmcom.174670/
https://igli.me/tg88bmcom
https://www.fantasyplanet.cz/diskuzni-fora/users/tg88bmcom/
https://freestyler.ws/user/629848/tg88bmcom
http://delphi.larsbo.org/user/tg88bmcom
https://www.aseeralkotb.com/en/profiles/tg88bmcom
https://timdaily.vn/members/tg88bmcom.128102/#about
https://app.readthedocs.org/profiles/tg88bmcom/
https://www.dibiz.com/laspreseschristian795
https://iszene.com/user-335745.html
https://www.theyeshivaworld.com/coffeeroom/users/tg88bmcom
https://desksnear.me/users/tg88bmcom
https://www.itchyforum.com/en/member.php?378955-tg88bmcom
https://www.roton.com/forums/users/laspreseschristian795/
https://able2know.org/user/tg88bmcom/
http://www.biblesupport.com/user/809074-tg88bmcom/
https://golosknig.com/profile/tg88bmcom/
https://www.anibookmark.com/user/tg88bmcom.html
https://forum.m5stack.com/user/tg88bmcom
https://wallhaven.cc/user/tg88bmcom
https://www.bitchute.com/channel/xGNzuVqdO8ZW
https://bandori.party/user/440795/tg88bmcom/
https://community.m5stack.com/user/tg88bmcom
https://schoolido.lu/user/tg88bmcom/
https://awan.pro/forum/user/137071/
https://jakle.sakura.ne.jp/pukiwiki/?tg88bmcom
https://fortunetelleroracle.com/profile/tg88bmcom
https://fabble.cc/tg88bmcom
https://pad.geolab.space/s/q4cwjiWZB
https://affariat.com/user/profile/172796
https://community.cisco.com/t5/user/viewprofilepage/user-id/1972493
https://pad.stuve.de/s/V-oAAk72w
https://kr.pinterest.com/tg88bmcom/
https://pt.gravatar.com/tg88bmcom
https://th.gravatar.com/tg88bmcom
https://www.sythe.org/members/tg88bmcom.2011810/
https://f319.com/members/tg88bmcom.1067759/
https://about.me/tg88bmcom
https://booklog.jp/users/tg88bmcom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/tg88bmcom.1341444/#about
https://www.equinenow.com/farm/tg88bmcom.htm
https://www.gaiaonline.com/profiles/tg88bmcom/50646028/
https://wefunder.com/tg88bmcom
https://potofu.me/tg88bmcom
https://transfur.com/Users/tg88bmcom
https://xtremepape.rs/members/tg88bmcom.644444/#about
https://myanimelist.net/profile/tg88bmcom
https://qna.habr.com/user/tg88bmcom
https://website.informer.com/tg88-bm.com
https://beacons.ai/tg88bmcom
https://en.islcollective.com/portfolio/12845225
https://www.xosothantai.com/members/tg88bmcom.597985/
https://velog.io/@tg88bmcom/about
https://violet.vn/user/show/id/15238002
https://iplogger.org/vn/logger/v9pQ5OVFytby
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3894126
https://mez.ink/tg88bmcom
https://tg88bmcom.stck.me/profile
https://notionpress.com/author/1471055
https://www.edna.cz/uzivatele/tg88bmcom/
https://digiphoto.techbang.com/users/tg88bmcom
https://leakedmodels.com/forum/members/tg88bmcom.689966/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1043054
https://freeicons.io/profile/895178
https://onlinesequencer.net/forum/member.php?action=profile&uid=250630
https://inkbunny.net/tg88bmcom
https://www.japaaan.com/user/62805/
https://spinninrecords.com/profile/tg88bmcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.tg886
https://code.antopie.org/tg88bmcom
https://beatsaver.com/playlists/1138892
https://apptuts.bio/tg88bmcom-247543
https://dialog.eslov.se/profiles/tg88bmcom/activity?locale=en
https://www.storenvy.com/tg88bmcom
https://tg88bmcom.mssg.me/
https://participacion.cabildofuer.es/profiles/tg88bmcom/activity?locale=en
https://forums.maxperformanceinc.com/forums/member.php?u=239235
https://egl.circlly.com/users/tg88bmcom
https://goodandbadpeople.com/tg88bmcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=289712
https://acomics.ru/-tg88bmcom
https://www.criminalelement.com/members/tg88bmcom/profile/
https://hanson.net/users/tg88bmcom
https://writexo.com/share/c0de64006ddc
https://www.heavyironjobs.com/profiles/7904199-nha-cai-tg88
https://pad.degrowth.net/s/Ee8oX_WMv
https://www.syncdocs.com/forums/profile/tg88bmcom
https://www.rehashclothes.com/tg88bmcom
http://fort-raevskiy.ru/community/profile/tg88bmcom/
https://forum.skullgirlsmobile.com/members/tg88bmcom.194270/#about
https://jobs.landscapeindustrycareers.org/profiles/7904216-nha-cai-tg88
https://phatwalletforums.com/user/tg88bmcom
https://kyourc.com/tg88bmcom
https://song.link/tg88bmcom
https://www.wanttoknow.nl/author/tg88bmcom/
https://idol.st/user/133254/tg88bmcom/
https://www.valinor.com.br/forum/usuario/tg88bmcom.141214/#about
https://tulieu.violet.vn/user/show/id/15238002
https://www.bmwpower.lv/user.php?u=tg88bmcom
https://gockhuat.net/member.php?u=430626
https://jobs.windomnews.com/profiles/7904253-nha-cai-tg88
https://hoaxbuster.com/redacteur/tg88bmcom
https://www.givey.com/tg88bmcom
https://zerosuicidetraining.edc.org/user/profile.php?id=537960
https://girlfriendvideos.com/members/t/tg88bmcom/
https://swaay.com/u/laspreses-christian795/about/
https://beteiligung.amt-huettener-berge.de/profile/tg88bmcom/
https://joinentre.com/profile/tg88bmcom
https://eo-college.org/members/tg88bmcom/
https://jobs.westerncity.com/profiles/7901957-nha-cai-tg88
https://www.thetriumphforum.com/members/tg88bmcom.56130/
https://armchairjournal.com/forums/users/tg88bmcom/
https://gamblingtherapy.org/forum/users/tg88bmcom/
https://l2top.co/forum/members/tg88bmcom.155408/
http://www.askmap.net/location/7710381/vietnam/tg88bmcom
https://youtopiaproject.com/author/tg88bmcom/
https://graphcommons.com/graphs/5dc2f25b-d23c-487e-b56e-424bd31ad4b4
https://galleria.emotionflow.com/174565/profile.html
https://www.myget.org/users/tg88bmcom
https://www.deafvideo.tv/vlogger/tg88bmcom
https://www.chaloke.com/forums/users/tg88bmcom/
https://app.brancher.ai/user/ChJjwAyuBm_R
https://aetherlink.app/users/7428001167634104320
https://confengine.com/user/tg88bmcom
https://slideslive.com/tg88bmcom?tab=about
https://mygamedb.com/profile/tg88bmcom
https://buckeyescoop.com/community/members/tg88bmcom.57164/#about
http://www.ssnote.net/users/tg88bmcom
https://forum.aceinna.com/user/tg88bmcom
https://www.mateball.com/tg88bmcom
https://toirscript.com/user/tg88bmcom
http://forum.cncprovn.com/members/413914-tg88bmcom
https://marketplace.trinidadweddings.com/author/tg88bmcom/
https://ncnews.co/profile/tg88bmcom
https://dreevoo.com/profile_info.php?pid=1110715
https://forum.aigato.vn/user/tg88bmcom
https://rapidapi.com/user/tg88bmcom
https://www.skool.com/@nha-cai-tg-6753
https://learningapps.org/watch?v=p1a0py6pt26
https://subscribe.ru/author/32229199
https://coub.com/tg88bmcom
https://www.giveawayoftheday.com/forums/profile/1638557
http://onlineboxing.net/jforum/user/editDone/428722.page
https://tealfeed.com/tg88bmcom
https://www.catapulta.me/users/tg88bmcom
http://www.invelos.com/UserProfile.aspx?Alias=tg88bmcom
https://www.video-bookmark.com/user/tg88bmcom/
https://wibki.com/tg88bmcom
https://krachelart.com/UserProfile/tabid/43/userId/1333314/Default.aspx
https://gitlab.vuhdo.io/tg88bmcom
https://11secondclub.com/users/profile/1698054
https://aniworld.to/user/profil/tg88bmcom
https://worldvectorlogo.com/ar/profile/tg8817
https://kktix.com/user/8430582
https://www.passes.com/tg88bmcom
https://poipiku.com/13161732/
https://uiverse.io/profile/tg88bmcom_2341
https://www.rwaq.org/users/tg88bmcom/
https://cofacts.tw/user/tg88bmcom
https://www.fitday.com/fitness/forums/members/tg88bmcom.html
https://www.fundable.com/user-1286121
https://vcook.jp/users/74074
https://www.grepmed.com/tg88bmcom
https://classificados.acheiusa.com/profile/aWhPZVRweW1sUXFXc21SQWJpRmVhaytPWmZzWFowTC80TzdoOTlVZkk4QT0=
https://espritgames.com/members/50038958/
https://cgmood.com/tg88bmcom
https://www.haikudeck.com/presentations/tg88bmcom
https://www.efunda.com/members/people/show_people.cfm?Usr=tg88bmcom
https://diit.cz/profil/bcgkerbgx7
https://backloggery.com/tg88bmcom
https://raovat.nhadat.vn/members/tg88bmcom-287481.html
https://www.moshpyt.com/user/tg88bmcom
https://www.koi-s.id/member.php?331544-tg88bmcom
https://pumpyoursound.com/u/user/1582768
https://que.u.nosv.org/profile?user=tg88bmcom
https://hi-fi-forum.net/profile/1117698
https://secondstreet.ru/profile/tg88bmcom/
http://scenarch.com/userpages/28624
https://undrtone.com/tg88bmcom
https://marshallyin.com/members/tg88bmcom/
https://us.enrollbusiness.com/BusinessProfile/7723051/TG88
https://www.atozed.com/forums/user-67150.html
https://gravesales.com/author/tg88bmcom/
https://gram.social/tg88bmcom
https://searchengines.bg/members/tg88bmcom.23219/#about
https://luvly.co/users/tg88bmcom
https://www.soshified.com/forums/user/661704-tg88bmcom/
https://hukukevi.net/user/tg88bmcom
https://belgaumonline.com/profile/tg88bmcom/
https://savelist.co/profile/users/tg88bmcom
https://www.montessorijobsuk.co.uk/author/tg88bmcom/
https://hackerspace.govhack.org/profiles/tg88bmcom
https://www.apsense.com/user/tg88bmcom
https://zzb.bz/7ufjzQ
http://draft.blogger.com/profile/07577293865602891089
https://boldomatic.com/view/writer/tg88bmcom
https://menwiki.men/wiki/User:Tg88bmcom
https://funsilo.date/wiki/User:Tg88bmcom
https://www.themeqx.com/forums/users/tg88bmcom/
https://www.udrpsearch.com/user/tg88bmcom
https://www.inseparabile.it/forum/member.php?u=45390
http://newdigital-world.com/members/tg88bmcom.html
https://www.xen-factory.com/index.php?members/tg88bmcom.138707/#about
https://cointr.ee/tg88bmcom
https://king-wifi.win/wiki/User:Tg88bmcom
https://forums.servethehome.com/index.php?members/tg88bmcom.224648/#about
https://jaga.link/tg88bmcom
https://raovatquynhon.com/thiet-bi-dien-tu-4/tg88bmcom-15594
https://b.io/tg88bmcom
http://www.truck-business.cz/profile/tg88bmcom/info.html
https://www.blackhatprotools.info/member.php?275815-tg88bmcom
https://activepages.com.au/profile/tg88bmcom
https://snippet.host/cgoeab
https://tudomuaban.com/chi-tiet-rao-vat/2820957/tg88bmcom.html
https://phijkchu.com/a/tg88bmcom/video-channels
https://lifeinsys.com/user/tg88bmcom
https://kaeuchi.jp/forums/users/tg88bmcom/
https://www.claimajob.com/profiles/7903989-nha-cai-tg88
https://protospielsouth.com/user/115907
https://theafricavoice.com/profile/tg88bmcom
http://palangshim.com/space-uid-4948555.html
https://www.africangenesis-101.org/profile/tg88bmcom/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:1EF049FE698E88D50A495E40@AdobeID
https://vi.gravatar.com/tg88bmcom
https://www.vevioz.com/tg88bmcom
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=184750
https://hub.vroid.com/en/users/123828339
https://www.exchangle.com/tg88bmcom
https://myanimeshelf.com/profile/tg88bmcom
https://circleten.org/a/395008
https://bitspower.com/support/user/tg88bmcom
https://www.brownbook.net/business/54815225/tg88bmcom
https://etextpad.com/ehpwoxqk3w
https://app.hellothematic.com/creator/profile/1120126
https://www.decidim.barcelona/profiles/tg88bmcom/activity
https://www.babelcube.com/user/nha-cai-tg88-31
https://app.talkshoe.com/user/tg88bmcom/about
https://hulkshare.com/tg88bmcom
https://m.wibki.com/tg88bmcom
https://www.pageorama.com/?p=tg88bmcom
https://bandsworksconcerts.info/index.php?tg88bmcom
https://bbs.mikocon.com/home.php?mod=space&uid=280711
https://www.mikocon.com/home.php?mod=space&uid=280711
https://jerseyboysblog.com/forum/member.php?action=profile&uid=81080
https://www.quora.com/profile/Tg88bmcom
https://manylink.co/@tg88bmcom
https://forums.giantitp.com/member.php?368070-tg88bmcom
https://seomotionz.com/member.php?action=profile&uid=115647
https://anyflip.com/homepage/criwj#About
https://www.akaqa.com/question/q19192651181-Tg88bmcom
https://londonchinese.com/home.php?mod=space&uid=614032&do=profile
https://copynotes.be/shift4me/forum/user-43638.html
https://scholar.google.com/citations?hl=en&user=NuXaiCoAAAAJ
https://www.threadless.com/@tg88bmcom/
https://www.smitefire.com/profile/tg88bmcom-255668?profilepage
https://tabelog.com/rvwr/tg88bmcom/prof/
https://prosinrefgi.wixsite.com/pmbpf/profile/tg88bmcom/profile
https://coolors.co/u/tg88bmcom
https://www.beamng.com/members/tg88bmcom.771544/
https://civitai.com/user/tg88bmcom
https://www.spigotmc.org/members/tg88bmcom.2478300/
https://boosty.to/tg88bmcom
https://camp-fire.jp/profile/tg88bmcom
https://feyenoord.supporters.nl/profiel/137350/tg88bmcom
https://www.pearltrees.com/tg88bmcom/item781181585
https://gesoten.com/profile/detail/12559161
https://rekonise.com/u/tg88bmcom
https://hashnode.com/@tg88bmcom
https://hoo.be/tg88bmcom
https://nhattao.com/members/tg88bmcom.6917627/
https://maxforlive.com/profile/user/tg88bmcom?tab=about
https://3dtoday.ru/blogs/tg88bmcom
https://opencollective.com/tg88bmcom
https://pinshape.com/users/8908893-tg88bmcom
https://morguefile.com/creative/tg88bmcom
https://edabit.com/user/kBJecSrgrHQizsLCi
https://mathlog.info/users/8ami4sy9EBQsIx5sxAWHmewuzHr1
https://securityheaders.com/?q=https%3A%2F%2Ftg88-bm.com%2F
https://my.bio/tg88bmcom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/144635
https://md.darmstadt.ccc.de/s/_HdO4OfN9E
https://participation.u-bordeaux.fr/profiles/tg88bmcom/activity
https://sfx.thelazy.net/users/u/tg88bmcom/
https://forum.reallusion.com/Users/3282983/tg88bmcom
https://mikseri.net/user/tg88bmcom
https://app.daily.dev/tg88bmcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=245312
https://slidehtml5.com/homepage/fjjs#About
https://www.skypixel.com/users/djiuser-dokbgpyjzzz7
https://webanketa.com/forms/6mv30e1n70qp6cb3c5k64sk6/
https://matters.town/@tg88bmcom
https://www.pdc.edu/?URL=https://tg88-bm.com/
https://ask.mallaky.com/?qa=user/tg88bmcom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75187
https://drill.lovesick.jp/drilldata/index.php?tg88bmcom
http://depechemode.cz/?URL=https://tg88-bm.com/
https://sub4sub.net/forums/users/tg88bmcom/
https://www.slmath.org/people/97891
https://userstyles.world/user/tg88bmcom
https://goo.by/vLsRxG
https://bresdel.com/tg88bmcom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=11848
https://fora.babinet.cz/profile.php?section=personal&id=113814
https://pledgeme.co.nz/profiles/316748
https://www.shippingexplorer.net/en/user/tg88bmcom/253962
https://pictureinbottle.com/r/tg88bmcom
https://forum.epicbrowser.com/profile.php?id=137157
http://www.dungdong.com/home.php?mod=space&uid=3315014
https://www.squadskates.com/profile/tg88bmcom/profile
https://shhhnewcastleswingers.club/forums/users/tg88bmcom/
https://forums.qhimm.com/index.php?action=profile;area=summary;u=89808
https://electroswingthing.com/profile/tg88bmcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2376171
https://connect.gt/user/tg88bmcom
https://stuv.othr.de/pad/s/84FRFH9RQ
https://forum.tkool.jp/index.php?members/tg88bmcom.96580/#about
https://hedgedoc.eclair.ec-lyon.fr/s/unbme_Dpy
http://densan-knct.freehostia.com/wiki_/index.php?tg88bmcom
https://www.divephotoguide.com/user/tg88bmcom
https://www.weddingbee.com/members/tg88bmcom/
https://kumu.io/tg88bmcom/tg88bmcom#tg88bmcom
https://b.cari.com.my/home.php?mod=space&uid=3379982&do=profile
https://bioimagingcore.be/q2a/user/tg88bmcom
https://www.sunlitcentrekenya.co.ke/author/tg88bmcom/
https://hedgedoc.logilab.fr/s/tXrunaO77
https://tg88bmcom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/tg88bmcom/activity
https://www.rcuniverse.com/forum/members/tg88bmcom.html
https://www.huntingnet.com/forum/members/tg88bmcom.html
https://www.socialbookmarkssite.com/bookmark/6191591/tg88bmcom/
https://www.hogwartsishere.com/1815034/
https://www.bunity.com/-5e1a99dc-25e9-4e60-b71c-b644d0b5c1d0?r=
https://vimeo.com/tg88bmcom
https://uccle.monopinion.belgium.be/profiles/tg88bmcom/activity
https://www.symbaloo.com/shared/AAAAAlnxozwAA41_IAqC2g==
https://www.bricklink.com/aboutMe.asp?u=tg88bmcom
https://makeagif.com/user/tg88bmcom?ref=b60u0V
https://www.lingvolive.com/en-us/profile/3a8fce19-4f3b-447b-b5ea-428a38eb65fc/translations
https://www.france-ioi.org/user/perso.php?sLogin=tg88bmcom
https://mt2.org/uyeler/tg88bmcom.34837/#about
https://participez.perigueux.fr/profiles/tg88bmcom/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1423704
https://www.dotafire.com/profile/tg88bmcom-235807?profilepage
https://www.trackyserver.com/profile/229313
https://ixawiki.com/link.php?url=https://tg88-bm.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=133852
https://www.zubersoft.com/mobilesheets/forum/user-122870.html
https://www.plotterusati.it/user/tg88bmcom
https://forum.azeron.eu/index.php?members/tg88bmcom.28716/#about
https://tutorialslink.com/member/tg88bmcomundefined/89192
http://www.activewin.com/user.asp?Action=Read&UserIndex=4824953
http://www.jbt4.com/home.php?mod=space&uid=8665271
https://www.vid419.com/home.php?mod=space&uid=3473460
https://forum.ct8.pl/member.php?action=profile&uid=113873
https://linqto.me/about/tg88bmcom
https://www.okaywan.com/home.php?mod=space&uid=766932
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Tg88bmcom
https://www.goodolcomics.com/blog/profile/tg88bmcom/
https://www.swap-bot.com/user:tg88bmcom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=383053
http://techou.jp/index.php?tg88bmcom
https://paste.intergen.online/view/702accbf
https://epiphonetalk.com/members/tg88bmcom.90177/#about
https://web.trustexchange.com/company.php?q=tg88-bm.com
https://forums.megalith-games.com/member.php?action=profile&uid=1441047
http://tkdlab.com/wiki/index.php?tg88bmcom
https://www.managementpedia.com/members/tg88bmcom.1116085/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=592725
https://volleypedia.org/index.php?qa=user&qa_1=tg88bmcom
http://pcsq28.com/home.php?mod=space&uid=1723972
https://bbs.airav.cc/home.php?mod=space&uid=4381556
https://partecipa.poliste.com/profiles/tg88bmcom/activity
https://md.coredump.ch/s/1UGPsFeaE
https://hker2uk.com/home.php?mod=space&uid=5324027
https://pad.funkwhale.audio/s/TLZcDIAeW
https://forum.dfwmas.org/index.php?members/tg88bmcom.192942/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=460845
https://aprenderfotografia.online/usuarios/tg88bmcom/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2302145&do=profile&from=space
http://www.haxorware.com/forums/member.php?action=profile&uid=439452
https://tilengine.org/forum/member.php?action=profile&uid=157561
https://darkml.net/bbs/home.php?mod=space&uid=8191810&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=5984277
http://wiki.0-24.jp/index.php?tg88bmcom
https://hedgedoc.stusta.de/s/3WNN7LJZa
https://pad.flipdot.org/s/jmyfgmelU
https://hack.allmende.io/s/n2K6SC4ar
https://pad.codefor.fr/s/GYKw8ue1MZ
https://md.inno3.fr/s/QK9OIKgXt
https://md.opensourceecology.de/s/eNs6l1uYo
https://md.ctdo.de/s/9NHgDB10bR
https://md.chaospott.de/s/GFBAb-W7vh
https://pad.fablab-siegen.de/s/xDy9AJphu
https://hackmd.hub.yt/s/IXRj_Qmw1
https://md.swk-web.com/s/McKIehxtoX
https://hedgedoc.dezentrale.space/s/qmRD1xCDN
https://docs.juze-cr.de/s/KycnxghMK
https://participons.mauges-sur-loire.fr/profiles/TG88/activity
https://ar.gravatar.com/tg88bmcom
https://sensationaltheme.com/forums/users/tg88bmcom/
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3300426
https://odesli.co/tg88bmcom
https://www.degreeforum.net/mybb/User-tg88bmcom
https://wandb.ai/profile/tg88bmcom
https://pad.darmstadt.social/s/VBPfvp6boS
https://divisionmidway.org/jobs/author/tg88bmcom/
https://bbcovenant.guildlaunch.com/users/blog/6735994/?mode=view&gid=97523
https://md.kif.rocks/s/pEJAB5e12J
https://youbiz.com/profile/tg88bmcom/
https://timeoftheworld.date/wiki/User:Tg88bmcom
https://historydb.date/wiki/User:Tg88bmcom
https://sciencemission.com/profile/tg88bmcom
https://referrallist.com/profile/tg88bmcom/
https://fakenews.win/wiki/User:Tg88bmcom
http://jobboard.piasd.org/author/tg88bmcom/
https://www.wvhired.com/profiles/7905524-nha-cai-tg88
https://kenhrao.com/members/tg88bmcom.114872/#about
http://jobs.emiogp.com/author/tg88bmcom/
https://www.canadavideocompanies.ca/forums/users/tg88bmcom/
https://hackmd.openmole.org/s/O1A1cYvV6
https://md.chaosdorf.de/s/zjYoYp-QAL
https://doc.adminforge.de/s/lbm5GfHNPa
https://onlinevetjobs.com/author/tg88bmcom/
https://v.gd/YR6mb8
https://sciencewiki.science/wiki/User:Tg88bmcom
https://gl.gta5-mods.com/users/tg88bmcom
https://dapp.orvium.io/profile/tg88bmcom-tg88
https://www.fruitpickingjobs.com.au/forums/users/tg88bmcom/
http://www.webclap.com/php/jump.php?url=https://tg88-bm.com/
https://xoops.ec-cube.net/userinfo.php?uid=341527
http://www.wmhelp.cz/html/modules.php?name=Forums&file=profile&mode=viewprofile&u=600649
https://formulamasa.com/elearning/members/tg88bmcom/
http://bbs.sdhuifa.com/home.php?mod=space&uid=1057252
https://quangcaoso.vn/tg88bmcom
https://tawk.to/tg88bmcom
https://chyoa.com/user/tg88bmcom
https://www.royalroad.com/profile/910143
https://backloggd.com/u/tg88bmcom/
https://kenhsinhvien.vn/m/tg88bmcom.1163406/#about
https://form.jotform.com/260442164687057
https://forums.alliedmods.net/member.php?u=465725
https://aiforkids.in/qa/user/tg88bmcom+1
https://community.jmp.com/t5/user/viewprofilepage/user-id/90322
https://digiex.net/members/tg88bmcom.139487/
https://ru.myanimeshelf.com/profile/tg88bmcom
https://www.corc.co.uk/forums/users/tg88bmcom/
https://smallseo.tools/website-checker/tg88-bm.com
https://cuwip.ucsd.edu/members/tg88bmcom/profile/
https://bwinglive.lighthouseapp.com/users/1992416
https://rush1989.rash.jp/pukiwiki/index.php?tg88bmcom
https://www.stylevore.com/user/tg88bmcom
https://bio.site/tg88bmcom
https://viblo.asia/u/tg88bmcom/contact
https://wikimapia.org/external_link?url=https://tg88-bm.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6250209
https://telegra.ph/tg88bmcom-02-14
https://runtrip.jp/users/736694
https://reactormag.com/members/tg88bmcom/
https://brain-market.com/u/tg88bmcom
https://ikanakama.ink/users/339171
https://www.prosebox.net/book/100721/
https://ticketme.io/account/tg88bmcom
https://task.tw/users/TGKMNLE/freelancer
https://www.aipictors.com/users/tg88bmcom
https://log.concept2.com/profile/2848327
http://speedway-world.pl/forum/member.php?action=profile&uid=431060
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://tg88-bm.com/
http://forum.orangepi.org/home.php?mod=space&uid=6250209
https://beteiligung.hafencity.com/profile/tg88bmcom/
https://adhocracy.plus/profile/tg88bmcom/
https://www.hobowars.com/game/linker.php?url=https://tg88-bm.com/
https://beteiligung.stadtlindau.de/profile/tg88bmcom/
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=75692
https://forum.honorboundgame.com/user-503117.html
https://propterest.com.au/user/71943/tg88bmcom
https://www.fw-follow.com/forum/topic/88462/tg88bmcom
https://www.jk-green.com/forum/topic/85239/tg88bmcom
https://www.navacool.com/forum/topic/309013/tg88bmcom
https://www.bonback.com/forum/topic/309014/tg88bmcom
https://www.driedsquidathome.com/forum/topic/109787/tg88bmcom
https://www.nongkhaempolice.com/forum/topic/83720/tg88bmcom
https://www.bestloveweddingstudio.com/forum/topic/59647/tg88bmcom
https://www.natthadon-sanengineering.com/forum/topic/75457/tg88bmcom
https://www.rueanmaihom.net/forum/topic/75446/tg88bmcom
https://www.ttlxshipping.com/forum/topic/308886/tg88
https://www.cemkrete.com/forum/topic/130373/tg88bmcom
https://pubhtml5.com/homepage/ykxhg/
http://worldchampmambo.com/UserProfile/tabid/42/UserID/476500/Default.aspx
http://forum.modulebazaar.com/forums/user/tg88bmcom/
https://gratisafhalen.be/author/tg88bmcom/
https://beteiligung.tengen.de/profile/tg88bmcom/
https://calaos.fr/forum/member.php?action=profile&uid=18477
https://www.vrwant.org/wb/home.php?mod=space&uid=4937673
https://mpc.imu.edu.kg/profile/tg88bmcom
https://forum.hkcinema.ru/profile.php?id=72362
https://www.rcmx.net/userinfo.php?uid=13807
https://www.pathumratjotun.com/forum/topic/138065/tg88bmcom
https://www.hravn.net/profile/tg88bmcom/
https://www.divekeeper.com/forums/discussion/general-discussion/tg88-trang-ca-cuoc-tg88com-dang-ky-nhan-888k-no-hu
https://eilo.org/user/tg88bmcom
https://forum.web-z.net/profile.php?userid=8892
https://usabbs.org/home.php?mod=space&uid=85647
https://lqdoj.edu.vn/user/tg88bmcom
http://pastport.jp/user/tg88bmcom
https://paperjale.eus/user/tg88bmcom
http://byltz.com/home.php?mod=space&uid=477650
https://indiestorygeek.com/user/tg88bmcom
https://www.bandlab.com/tg88bmcom
https://diigo.com/011xfom
https://forum.issabel.org/u/tg88bmcom
https://www.siye.co.uk/siye/viewuser.php?uid=247519
https://ie.enrollbusiness.com/BusinessProfile/7723051/TG88
https://www.casualgamerevolution.com/user/tg88bmcom
https://www.iglinks.io/tg88bmcom-na6
https://decidim.calafell.cat/profiles/tg88bmcom/activity
https://www.keepandshare.com/discuss4/36187/tg88
http://bbs.medicalforum.cn/home.php?mod=space&uid=2059728
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://tg88-bm.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3379982&do=profile
https://giaoan.violet.vn/user/show/id/15238002
https://anh135689999.violet.vn/user/show/id/15238002
https://party.biz/profile/372599?tab=541
https://profiles.delphiforums.com/n/pfx/profile.aspx?webtag=dfpprofile000&userId=1891278555
https://hu.gta5-mods.com/users/tg88bmcom
https://uk.gta5-mods.com/users/tg88bmcom
https://sl.gta5-mods.com/users/tg88bmcom
https://www.hamqth.com/tg88bmcom
https://at.pinterest.com/tg88bmcom/
https://www.easyhits4u.com/profile.cgi?login=tg88bmcom&view_as=1
https://newdayrp.com/members/tg88bmcom.66444/#about
https://in.pinterest.com/tg88bmcom/
https://doc.anagora.org/s/KUPREa8GQ
https://album.link/tg88bmcom
https://artist.link/tg88bmcom
https://pods.link/tg88bmcom
https://mylink.page/tg88bmcom
https://playlist.link/tg88bmcom
https://portfolium.com.au/tg88bmcom
https://profile.sampo.ru/tg88bmcom
https://mail.londonchinese.com/home.php?mod=space&uid=614032&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75108
https://baigiang.violet.vn/user/show/id/15238002
http://www.muzikspace.com/profiledetails.aspx?profileid=127361
https://es.gravatar.com/tg88bmcom
https://de.gravatar.com/tg88bmcom
https://cy.gravatar.com/tg88bmcom
https://cs.gravatar.com/tg88bmcom
https://cn.gravatar.com/tg88bmcom
https://www.linkedin.com/in/tg88bmcom/
https://www.ekdarun.com/forum/topic/132253/tg88bmcom
https://www.mobafire.com/profile/tg88bmcom-1234098/bio?profilepage
https://fic.decidim.barcelona/profiles/tg88bmcom/activity
https://itvnn.net/member.php?162925-tg88bmcom
https://fanclove.jp/profile/AyJmoaK7B1
https://truckymods.io/user/458184
http://forum.vodobox.com/profile.php?id=62545
https://forum.enscape3d.com/wcf/index.php?user/133259-tg88bmcom/#about
https://forum.findukhosting.com/index.php?action=profile;area=summary;u=74948
https://fungiversum.de/pilz-forum/profile/tg88bmcom/
https://www.wikiwicca.com/forums/users/tg88bmcom/
https://www.expat.com/forum/profile.php?id=3945921&lang=en
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=225533
https://www.cfd-online.com/Forums/members/tg88bmcom.html
https://www.dokkan-battle.fr/forums/users/tg88bmcom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3379982&do=profile
https://animeforums.net/profile/47214-tg88bmcom/?tab=field_core_pfield_1
https://www.templepurohit.com/forums/users/laspreseschristian795/
https://www.fanfiction.net/u/16852955/
https://www.hugi.is/notendur/tg88bmcom/
https://www.kickstarter.com/profile/tg88bmcom/about
https://www.noteflight.com/profile/c3867f3f31e2141cba36762c131a04b986d71a24
https://www.spoonflower.com/profiles/tg88bmcom?sub_action=shop
https://www.sportjim.com/tg88bmcom
https://www.horticulturaljobs.com/employers/4021945-tg88bmcom
https://jobs.siliconflorist.com/employers/4021954-tg88bmcom
https://jobs.nefeshinternational.org/employers/4021957-tg88bmcom
https://aboutcasemanagerjobs.com/author/tg88bmcom/
https://biashara.co.ke/author/tg88bmcom/
https://buyandsellhair.com/author/tg88bmcom/
https://cornucopia.se/author/tg88bmcom/
https://colorswall.com/users/29339/collections
https://webyourself.eu/tg88bmcom
https://lustyweb.live/members/tg88bmcom.108580/#about
https://findaspring.org/members/tg88bmcom/
https://www.pokecommunity.com/members/tg88bmcom.1478999/#about
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=767245
https://careers.coloradopublichealth.org/profiles/7906072-nha-cai-tg88
https://homepage.ninja/tg88bmcom
https://promosimple.com/ps/45a77/tg88bmcom
https://dienbd.violet.vn/user/show/id/15238002
https://ketcau.com/member/121189-tg88bmcom/visitormessage/309532-visitor-message-from-tg88bmcom#post309532
https://kttm.club/members/tg88bmcom.4251/#about
https://vn-zom.com/members/tg88bmcom.5592/
https://vietcurrency.vn/members/tg88bmcom.233842/#about
https://zh-tw.gravatar.com/tg88bmcom
https://sv.gravatar.com/tg88bmcom
https://po.gravatar.com/tg88bmcom
https://oc.gravatar.com/tg88bmcom
https://ko.gravatar.com/tg88bmcom
https://vnbit.org/members/tg88bmcom.82699/#about
https://www.cake.me/me/tg88bmcom
https://boss.why3s.cc/boss/home.php?mod=space&uid=250226
https://fengshuidirectory.com/dashboard/listings/tg88bmcom/
https://pets4friends.com/profile-1523076
https://staroetv.su/go?https://tg88-bm.com/
https://www.ixawiki.com/link.php?url=https://tg88-bm.com/
https://www.shinobi.jp/etc/goto.html?https://tg88-bm.com/
https://oye.participer.lyon.fr/profiles/tg88bmcom/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345360
https://axe.rs/forum/members/tg88bmcom.13415886/#about
https://participa.favb.cat/profiles/tg88bmcom/activity
https://construim.fedaia.org/profiles/tg88bmcom/activity
https://meta.decidim.org/profiles/tg88bmcom/activity
https://hi.gta5-mods.com/users/tg88bmcom
https://it.gta5-mods.com/users/tg88bmcom
https://nl.gta5-mods.com/users/tg88bmcom
https://no.gta5-mods.com/users/tg88bmcom
https://pl.gta5-mods.com/users/tg88bmcom
https://pt.gta5-mods.com/users/tg88bmcom
https://decidim.derechoaljuego.digital/profiles/tg88bmcom/activity
https://pads.zapf.in/s/Ggi905cBiW
https://postr.yruz.one/profile/tg88bmcom
https://www.bookingblog.com/forum/users/tg88bmcom/
https://legenden-von-andor.de/forum/memberlist.php?mode=viewprofile&u=53138
https://aiti.edu.vn/members/tg88bmcom.34335/
https://tinhte.vn/members/tg88bmcom.3380131/
https://barcelonadema-participa.cat/profiles/tg88bmcom/activity
https://www.foriio.com/tg88bmcom
https://www.project1999.com/forums/member.php?u=322328
https://pad.stuve.de/s/Nwlkqm2r9
https://pad.libreon.fr/s/akgr9ji7t
http://matdo.sangnhuong.com/member.php?u=110416
http://banhkeo.sangnhuong.com/member.php?u=96790
http://thietbidien.sangnhuong.com/member.php?u=105416
https://gl.gravatar.com/tg88bmcom
https://fr.gravatar.com/tg88bmcom
https://fi.gravatar.com/tg88bmcom
https://fa.gravatar.com/tg88bmcom
https://www.mediarte.be/nl/talent/nha-cai-tg88
https://quomon.es/Profile/tg88bmcom/
https://www.are.na/nha-cai-tg88-shnuadpjejy/tg88bmcom
https://altacucina.co/profile/tg88bmcom
https://ro.gta5-mods.com/users/tg88bmcom
https://ru.gta5-mods.com/users/tg88bmcom
https://sv.gta5-mods.com/users/tg88bmcom
https://vi.gta5-mods.com/users/tg88bmcom
https://zh.gta5-mods.com/users/tg88bmcom
https://tg88bmcom.mystrikingly.com/
https://tg88bmcom.webflow.io/
https://rant.li/tg88bmcom/tg88
https://sites.google.com/view/tg88bmcom/home
https://telegra.ph/TG88-02-14
https://tg88bmcom.blogspot.com/2026/02/tg88.html
https://tg8876100.mypixieset.com/
https://hackmd.io/@tg88bmcom/ByZYfQCD-x
https://hedgedoc.stusta.de/s/tDqAFMmGJ
https://scrapbox.io/tg88bmcom/tg88bmcom
https://tg88bmcom.wordpress.com/
https://www.notebook.ai/documents/2371501
https://tg88bmcom.gitbook.io/tg88bmcom-docs/
https://tg88bmcom.therestaurant.jp/
https://tg88bmcom.theblog.me/
https://shadow-activity-9a5.notion.site/TG88-30747079f7348077a7e7f5e5fc132751?pvs=73
https://zb3.org/tg88bmcom/tg88
https://www.keepandshare.com/discuss4/36204/tg88
http://nhcitg881771059717.website3.me/
https://www.myaspenridge.com/board/board_topic/3180173/7868619.htm
https://www.tai-ji.net/board/board_topic/4160148/7868620.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/7868621.htm
https://www.thepetservicesweb.com/board/board_topic/2701171/7868626.htm
https://www.milliescentedrocks.com/board/board_topic/2189097/7868636.htm
https://www.coffeesix-store.com/board/board_topic/7560063/7868641.htm
Aw, this was a really good post. Finding the time and actual effort to generate a good article… but what can I
say… I procrastinate a whole lot and don’t manage to get nearly anything done.
Seriously plenty of beneficial facts!
Your comment is awaiting moderation.
https://www.facebook.com/123bbmcom/
https://www.youtube.com/@123bbmcom
https://x.com/123bbmcom
https://tooter.in/123bbmcom
https://wakelet.com/@123bbmcom
https://safechat.com/u/123b5.740
https://www.blogger.com/profile/02739775691735447915
https://www.mymeetbook.com/123bbmcom
https://www.pinterest.com/123bbmcom/
https://community.wongcw.com/123bbmcom
https://demo.wowonder.com/123bbmcom
https://shareyoursocial.com/123bbmcom
https://gitlab.aicrowd.com/123bbmcom
https://myspace.com/123bbmcom
https://500px.com/p/123bbmcom
https://www.instapaper.com/p/123bbmcom
https://magic.ly/123bbmcom
https://www.band.us/band/101634674/intro
https://protocol.ooo/en/users/123bbmcom
https://sketchfab.com/123bbmcom
https://www.tumblr.com/123bbmcom
https://www.reddit.com/user/123bbmcom/
https://audiomack.com/123bbmcom
https://hackaday.io/123bbmcom
https://vocal.media/authors/123b-4pfhj0oaq
https://leetcode.com/u/123bbmcom/
https://swag.live/en/user/6996797bb6d62fbfbd2aef73
https://www.halaltrip.com/user/profile/319237/123bbmcom/
https://www.jetphotos.com/photographer/779728
https://medibang.com/author/27809179/
https://liulo.fm/123bbmcom
https://opensea.io/123bbmcom
https://www.blockdit.com/users/6996dac6368ff923ff15edfb
https://groups.google.com/g/123bbmcom
https://www.twitch.tv/123bbmcom/about
https://profile.hatena.ne.jp/a123bbmcom/profile
https://issuu.com/123bbmcom
https://www.behance.net/123bbmcom
https://gravatar.com/123bbmcom
https://www.reverbnation.com/artist/123bbmcom
https://www.myminifactory.com/users/123bbmcom
https://www.investagrams.com/Profile/123bbmcom
https://gifyu.com/123bbmcom
https://www.chordie.com/forum/profile.php?id=2471047
https://skitterphoto.com/photographers/2329407/123bbmcom
https://www.longisland.com/profile/123bbmcom
https://www.walkscore.com/people/339632704739/123b
https://topsitenet.com/profile/123bbmcom/1550206/
https://akniga.org/profile/1393482-123bbmcom/
https://123bbmcom.bandcamp.com/album/123b
https://disqus.com/by/123bbmcom/about/
https://jobs.suncommunitynews.com/profiles/7919638-nha-cai-123b
https://www.speedrun.com/users/123bbmcom
https://www.fanart-central.net/user/123bbmcom/profile
https://slides.com/a123bbmcom
https://www.aicrowd.com/participants/123bbmcom
https://old.bitchute.com/channel/BBLdnNYPjBdT/
http://pbase.com/123bbmcom
https://hub.docker.com/u/123bbmcom
https://spiderum.com/nguoi-dung/123bbmcom
https://zaidap.com/thong-tin-ca-nhan-u106022.htm
https://www.gta5-mods.com/users/123bbmcom
https://heylink.me/123bbmcom/
https://pixabay.com/users/54719113/
https://www.nicovideo.jp/user/143316538
https://www.jigsawplanet.com/123bbmcom
https://3dwarehouse.sketchup.com/by/123bbmcom
https://robertsspaceindustries.com/en/citizens/a123bbmcom
https://bit.ly/m/123bbmcom
https://joy.link/123bbmcom
https://connect.garmin.com/app/profile/4209b719-28eb-4ddf-8fd2-ae55e0ddfa1a
https://b.hatena.ne.jp/a123bbmcom/
https://www.chichi-pui.com/users/123bbmcom/
https://www.openrec.tv/user/123bbmcom/about
https://unityroom.com/users/948dqialft61hknymgx2
https://pxhere.com/en/photographer-me/4923586
https://teletype.in/@123bbmcom
https://www.checkli.com/123bbmcom
https://gitee.com/a123bbmcom
https://www.fuelly.com/driver/123bbmcom
https://www.nintendo-master.com/profil/123bbmcom
https://freeimage.host/123bbmcom
https://www.fondazioneitalianadelrene.org/forums/users/123bbmcom/
https://www.diigo.com/profile/a123bbmcom
https://fontstruct.com/fontstructions/show/2829748/123bbmcom
https://mecabricks.com/en/user/a123bbmcom
https://motion-gallery.net/users/914681
https://linkin.bio/123bbmcom
https://forums.daybreakgames.com/dcuo/index.php?members/mothaibabbmcom.423392/
https://www.logic-sunrise.com/forums/user/189707-123bbmcom/
https://biomolecula.ru/authors/126089
https://talk.plesk.com/members/123bbmcom.488940/#about
https://www.callupcontact.com/b/businessprofile/123b/9978891
https://blender.community/123b97/
https://doselect.com/@0ff184ff4ee28f1186cc7dc95
https://sciter.com/forums/users/123bbmcom/
https://matkafasi.com/user/123bbmcom
https://allmyfaves.com/123bbmcom
https://www.notebook.ai/users/1284808
https://www.abclinuxu.cz/lide/123bbmcom
https://dumagueteinfo.com/author/123bbmcom/
https://muare.vn/shop/nha-cai-123b-55/894854
https://www.vnbadminton.com/members/123bbmcom.65056/
https://doodleordie.com/profile/a123bbmcom
https://web.ggather.com/123bbmcom
https://musikersuche.musicstore.de/profil/123bbmcom/
https://www.intensedebate.com/people/a123bbmcom
https://lookingforclan.com/user/123bbmcom
https://forum.dmec.vn/index.php?members/123bbmcom.175254/
https://igli.me/123bbmcom
https://www.fantasyplanet.cz/diskuzni-fora/users/123bbmcom/
https://freestyler.ws/user/631093/123bbmcom
http://delphi.larsbo.org/user/123bbmcom
https://www.aseeralkotb.com/en/profiles/123bbmcom
https://timdaily.vn/members/123bbmcom.128241/#about
https://app.readthedocs.org/profiles/123bbmcom/
https://iszene.com/user-336251.html
https://www.theyeshivaworld.com/coffeeroom/users/123bbmcom
https://desksnear.me/users/123bbmcom
https://www.itchyforum.com/en/member.php?379438-123bbmcom
https://www.roton.com/forums/users/doravetlaure707/
https://able2know.org/user/123bbmcom/
http://www.biblesupport.com/user/810241-123bbmcom/
https://golosknig.com/profile/123bbmcom/
https://www.anibookmark.com/user/123bbmcom.html
https://www.inventoridigiochi.it/membri/123bbmcom/profile/
https://forum.m5stack.com/user/123bbmcom
https://wallhaven.cc/user/123bbmcom
https://imageevent.com/123bbmcom/123bbmcom
https://www.bitchute.com/channel/BBLdnNYPjBdT
https://bandori.party/user/464876/123bbmcom/
https://community.m5stack.com/user/123bbmcom
https://schoolido.lu/user/123bbmcom/
https://awan.pro/forum/user/138471/
https://jakle.sakura.ne.jp/pukiwiki/?123bbmcom
https://fortunetelleroracle.com/profile/123bbmcom
https://fabble.cc/123bbmcom
https://pad.geolab.space/s/2KwoNXYMM
https://community.cisco.com/t5/user/viewprofilepage/user-id/1974789
https://pad.stuve.de/s/V_ypL26Bl
http://kr.pinterest.com/123bbmcom/
https://pt.gravatar.com/123bbmcom
https://th.gravatar.com/123bbmcom
https://www.sythe.org/members/123bbmcom.2012915/
https://f319.com/members/123bbmcom.1068977/
https://about.me/a123bbmcom
https://booklog.jp/users/1daeebab9a5ede64/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/123bbmcom.1342088/#about
https://www.equinenow.com/farm/profile6997771c30a2f.htm
https://www.gaiaonline.com/profiles/123bbmcom/50647603/
https://wefunder.com/123bbmcom
https://potofu.me/123bbmcom
https://transfur.com/Users/a123bbmcom
https://github.com/123bbmcom
https://myanimelist.net/profile/a123bbmcom
https://qna.habr.com/user/123bbmcom
https://website.informer.com/123b-bm.com
https://lightroom.adobe.com/u/123bbmcom
https://beacons.ai/123bbmcom
https://en.islcollective.com/portfolio/12849799
https://www.xosothantai.com/members/123bbmcom.598472/
https://velog.io/@123bbmcom/about
https://violet.vn/user/show/id/15238393
https://iplogger.org/vn/logger/ZKEQ5ipzIfEW/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3900335
https://mez.ink/123bbmcom
https://123bbmcom.stck.me/profile
https://notionpress.com/author/1474344
https://www.edna.cz/uzivatele/123bbmcom/
https://digiphoto.techbang.com/users/123bbmcom
https://leakedmodels.com/forum/members/123bbmcom.691240/#about
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1044976
https://freeicons.io/profile/896916
https://onlinesequencer.net/members/251904
https://inkbunny.net/123bbmcom
https://www.japaaan.com/user/62989
https://spinninrecords.com/profile/123bbmcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nha.cai.123b
https://code.antopie.org/123bbmcom
https://beatsaver.com/playlists/1142728
https://apptuts.bio/123bbmcom-248085
https://dialog.eslov.se/profiles/123bbmcom/activity?locale=en
https://www.storenvy.com/a123bbmcom
https://participacion.cabildofuer.es/profiles/123bbmcom/activity?locale=en
https://egl.circlly.com/users/123bbmcom
https://www.bloggportalen.se/BlogPortal/view/ReportBlog?id=290102
https://www.sciencebee.com.bd/qna/user/123bbmcom
https://acomics.ru/-123bbmcom
https://www.criminalelement.com/members/123bbmcom/profile/
https://hanson.net/users/123bbmcom
https://writexo.com/share/28c196d9b7ed
https://expatguidekorea.com/profile/123bbmcom/
https://www.laundrynation.com/community/profile/123bbmcom/
https://www.heavyironjobs.com/profiles/7921600-nha-cai-123b
https://pad.degrowth.net/s/xJziVbL_2
https://www.syncdocs.com/forums/profile/123bbmcom
https://www.rehashclothes.com/123bbmcom
http://fort-raevskiy.ru/community/profile/123bbmcom/
https://forum.skullgirlsmobile.com/members/123bbmcom.195829/#about
https://jobs.landscapeindustrycareers.org/profiles/7921602-nha-cai-123b
https://phatwalletforums.com/user/123bbmcom/
https://kyourc.com/123bbmcom
https://song.link/123bbmcom
https://idol.st/user/134953/123bbmcom/
https://www.valinor.com.br/forum/usuario/123bbmcom.141376/#about
https://tulieu.violet.vn/user/show/id/15238393
https://www.bmwpower.lv/user.php?u=a123bbmcom
https://gockhuat.net/member.php?u=430947
https://jobs.windomnews.com/profiles/7921633-nha-cai-123b
https://hoaxbuster.com/redacteur/123bbmcom
https://www.givey.com/123bbmcom
https://talkmarkets.com/profile/doravetlaure707-260220-054825
https://zerosuicidetraining.edc.org/user/profile.php?id=539973
https://www.telix.pl/forums/users/Nha-cai-123b6/
https://swaay.com/u/doravet-laure707/about/
https://beteiligung.amt-huettener-berge.de/profile/123bbmcom/
https://joinentre.com/profile/123bbmcom
https://jobs.westerncity.com/profiles/7921696-nha-cai-123b
https://www.thetriumphforum.com/members/123bbmcom.56414/
https://gamblingtherapy.org/forum/users/123bbmcom/
https://mycableengineering.com/users/123bbmcom
https://l2top.co/forum/members/123bbmcom.156485/
http://www.askmap.net/location/7734835/vietnam/123bbmcom
https://youtopiaproject.com/author/123bbmcom
https://graphcommons.com/graphs/b73195ad-a56f-4a5c-b459-beacfbd1d1cb
https://galleria.emotionflow.com/174938/profile.html
https://www.myget.org/users/123bbmcom
https://www.deafvideo.tv/vlogger/123bbmcom
https://www.chaloke.com/forums/users/123bbmcom/
https://app.brancher.ai/user/iRdsyFTixTeC
https://justpaste.me/tJzB3
https://confengine.com/user/123bbmcom
https://slideslive.com/kkkkbav0i0ki/?tab=about
https://mygamedb.com/profile/doravetlaure707
https://buckeyescoop.com/community/members/123bbmcom.57367/#about
https://forum.aceinna.com/user/123bbmcom
https://toirscript.com/user/123bbmcom
https://forum.pabbly.com/members/123bbmcom.97489/#about
http://forum.cncprovn.com/members/414463-123bbmcom
https://marketplace.trinidadweddings.com/author/123bbmcom/
https://ncnews.co/profile/123bbmcom
https://dreevoo.com/profile.php?pid=1142172
https://forum.aigato.vn/user/123bbmcom
https://amaz0ns.com/forums/users/123bbmcom/
https://rapidapi.com/user/123bbmcom
https://www.skool.com/@nha-cai-mothaibab-4085
https://hedge.fachschaft.informatik.uni-kl.de/s/2QWxeUNiW
https://learningapps.org/display?v=pc50v343n26
https://coub.com/123bbmcom
https://postheaven.net/123bbmcom/nha-cai-123b
https://www.giveawayoftheday.com/forums/profile/1652517
http://onlineboxing.net/jforum/user/profile/429584.page
https://www.tealfeed.com/a123bbmcom
https://www.catapulta.me/users/123bbmcom
http://www.invelos.com/UserProfile.aspx?alias=123bbmcom
https://www.video-bookmark.com/user/123bbmcom/
https://wibki.com/123bbmcom
https://krachelart.com/UserProfile/tabid/43/userId/1333861/Default.aspx
https://gitlab.vuhdo.io/123bbmcom
https://www.11secondclub.com/users/profile/1699239
https://aniworld.to/user/profil/123bbmcom
https://s.id/123bbmcom
https://worldvectorlogo.com/profile/123bbmcom
https://kktix.com/user/8437409
https://www.passes.com/123bbmcom
https://poipiku.com/13201409/
https://uiverse.io/profile/nhci_7978
https://www.rwaq.org/users/123bbmcom/
https://cofacts.tw/user/123bbmcom
https://www.fitday.com/fitness/forums/members/123bbmcom.html
https://www.fundable.com/nha-cai-123b-51
https://vcook.jp/users/74602/
https://www.grepmed.com/123bbmcom
https://classificados.acheiusa.com/profile/K09kSFlXbVZqbkJLNTZ0cER1L3I1MnpNUnpQN0owejNBVUxEbkticndxVT0=
https://espritgames.com/members/50109265/
https://cgmood.com/123bbmcom
https://backloggery.com/123bbmcom
https://www.sociomix.com/u/123bbmcom/
https://jobhop.co.uk/blog/472317/123b–nn-tng-gii-tr-trc-tuyn-vi-giao-din-thn-thin-v-tri-nghim-thng-tin-a-dng
https://raovat.nhadat.vn/members/123bbmcom-288451.html
https://www.moshpyt.com/user/123bbmcom
https://www.koi-s.id/member.php?331573-123bbmcom
https://pumpyoursound.com/u/user/1584153
https://que.u.nosv.org/profile?user=123bbmcom
https://hi-fi-forum.net/profile/1120009
https://secondstreet.ru/profile/123bbmcom/
http://scenarch.com/userpages/28731
https://undrtone.com/123bbmcom
https://marshallyin.com/members/123bbmcom/
https://www.atozed.com/forums/user-67623.html
https://gravesales.com/author/123bbmcom/
https://searchengines.bg/members/123bbmcom.23351/#about
https://luvly.co/users/123bbmcom
https://suckhoetoday.com/members/35950-123bbmco.html
https://hukukevi.net/user/123bbmcom
https://belgaumonline.com/profile/123bbmcom/
https://savelist.co/my-lists/users/123bbmcom
https://usdinstitute.com/forums/users/123bbmcom/
https://www.montessorijobsuk.co.uk/author/123bbmcom/
https://www.apsense.com/user/123bbmcom
https://zzb.bz/HlCMci
https://draft.blogger.com/profile/02739775691735447915
https://boldomatic.com/view/writer/123bbmcom
https://menwiki.men/wiki/User:123bbmcom
https://funsilo.date/wiki/User:123bbmcom
https://the7thcontinent.seriouspoulp.com/en/user/28217/123bbmcom
https://www.themeqx.com/forums/users/123bbmcom/
https://www.udrpsearch.com/user/123bbmcom
https://www.inseparabile.it/forum/member.php?u=45573
http://newdigital-world.com/members/123bbmcom.html
https://www.xen-factory.com/index.php?members/123bbmcom.139607/#about
https://cointr.ee/123bbmcom
https://king-wifi.win/wiki/User:123bbmcom
https://forums.servethehome.com/index.php?members/123bbmcom.225710/#about
https://jaga.link/123bbmcom
https://raovatquynhon.com/thiet-bi-dien-tu-4/123b-nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem-thon-15656
https://b.io/123bbmcom
http://www.truck-business.cz/profile/123bbmcom/info.html
https://www.blackhatprotools.info/member.php?276365-123bbmcom
https://activepages.com.au/profile/123bbmcom
https://snippet.host/qfhkox
https://tudomuaban.com/chi-tiet-rao-vat/2824341/123b–nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem-thong-tin-da-dang.html
https://phijkchu.com/a/123bbmcom/video-channels
https://lifeinsys.com/user/123bbmcom
https://kaeuchi.jp/forums/users/123bbmcom/
https://www.claimajob.com/profiles/7922783-nha-cai-123b
https://protospielsouth.com/user/116682
https://theafricavoice.com/profile/123bbmcom
http://palangshim.com/space-uid-4967406.html
https://www.africangenesis-101.org/profile/doravetlaure70728035/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:0ED249926996DD960A495C06@AdobeID
http://vi.gravatar.com/123bbmcom
https://www.vevioz.com/123bbmcom
https://www.mixcloud.com/123bbmcom/
https://www.designspiration.com/123bbmcom/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185372
https://hub.vroid.com/en/users/124017430
https://www.exchangle.com/123bbmcom
https://forum.codeigniter.com/member.php?action=profile&uid=223424
https://bitspower.com/support/user/123bbmcom
https://www.brownbook.net/business/54843641/123b
https://etextpad.com/1tkai96sbb
https://www.decidim.barcelona/profiles/123bbmcom/activity
https://www.babelcube.com/user/nha-cai-123b-109
https://app.talkshoe.com/user/123bbmcom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223144
https://hulkshare.com/123bbmcom
https://m.wibki.com/123bbmcom
https://www.pageorama.com/?p=123bbmcom
https://bandsworksconcerts.info/index.php?123bbmcom
https://bbs.mikocon.com/home.php?mod=space&uid=281336
https://www.mikocon.com/home.php?mod=space&uid=281336
https://jerseyboysblog.com/forum/member.php?action=profile&uid=81646
https://www.quora.com/profile/123b-104
https://manylink.co/@123bbmcom
https://www.freewebspace.net/forums/index.php?members/123bbmcom.17031170/#about
https://forums.giantitp.com/member.php?368759-123bbmcom
https://seomotionz.com/member.php?action=profile&uid=116377
https://anyflip.com/homepage/wndal
https://www.akaqa.com/question/q19192652150-123bbmcom
https://londonchinese.com/home.php?mod=space&uid=614442&do=profile
https://copynotes.be/shift4me/forum/user-44041.html
https://scholar.google.com/citations?user=QwetbpIAAAAJ&hl=en
https://www.threadless.com/@123bbmcom/activity
https://www.smitefire.com/profile/123bbmcom-256223?profilepage
https://tabelog.com/rvwr/123bbmcom/prof/
https://coolors.co/u/123bbmcom
https://www.beamng.com/members/123bbmcom.772938/
http://civitai.com/user/123bbmcom
https://www.spigotmc.org/members/123bbmcom.2482697/
https://boosty.to/123bbmcom
https://camp-fire.jp/profile/123bbmcom
https://feyenoord.supporters.nl/profiel/138060/123bbmcom
https://www.pearltrees.com/123bbmcom/item782289839
https://gesoten.com/profile/detail/12575375
https://hashnode.com/@123bbmcom
https://hoo.be/123bbmcom
https://nhattao.com/members/user6920310.6920310/
https://maxforlive.com/profile/user/123bbmcom?tab=about
https://3dtoday.ru/blogs/123bbmcom
https://opencollective.com/123bbmcom
https://pinshape.com/users/8912869-123bbmcom?tab=designs
https://edabit.com/user/bsGf2Su7GPsWRbgBX
https://mathlog.info/users/F3timwM9FfgV12EievM73kEwInm2
https://securityheaders.com/?q=123b-bm.com
https://my.bio/123bbmcom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/144916
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165575
https://md.darmstadt.ccc.de/s/YrDH_dJc1A
https://sfx.thelazy.net/users/u/123bbmcom/
https://forum.reallusion.com/Users/3283235/DoravetLaure707
https://app.daily.dev/123bbmcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=246129
https://slidehtml5.com/homepage/occw#About
https://www.skypixel.com/users/djiuser-iehfvtvd3yty
https://webanketa.com/forms/6mv32d1s6cqk0c9ncdk68sk1/
https://matters.town/a/92qv7erv0dt2
https://www.pdc.edu/?URL=https://123b-bm.com/
https://ask.mallaky.com/?qa=user/123bbmcom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75487
https://drill.lovesick.jp/drilldata/index.php?123bbmcom
https://www.depechemode.cz/?URL=https://123b-bm.com/
https://sub4sub.net/forums/users/123bbmcom/
https://www.slmath.org/people/98388
https://userstyles.world/user/123bbmcom
https://goo.by/eJMOua
https://amazingradio.com/profile/123bbmcom
https://bresdel.com/123bbmcom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=11940
https://pledgeme.co.nz/profiles/317945/
https://www.shippingexplorer.net/en/user/123bbmcom/255527
https://123bbmcom.notepin.co/
https://pictureinbottle.com/r/123bbmcom
https://forum.epicbrowser.com/profile.php?id=137998
http://www.dungdong.com/home.php?mod=space&uid=3318926
https://www.squadskates.com/profile/doravetlaure70727585/profile
https://forum.herozerogame.com/index.php?/user/151548-123bbmcom/
https://shhhnewcastleswingers.club/forums/users/123bbmcom/
https://forums.qhimm.com/index.php?action=profile;u=89881
https://electroswingthing.com/profile/123bbmcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2382851
https://connect.gt/user/123bbmcom
https://stuv.othr.de/pad/s/1jXIoqFPO
https://forum.tkool.jp/index.php?members/123bbmcom.97222/#about
https://hedgedoc.eclair.ec-lyon.fr/s/QsPKvyD2p
http://densan-knct.freehostia.com/wiki_/index.php?123bbmcom
https://www.divephotoguide.com/user/123bbmcom
https://www.weddingbee.com/members/123bbmcom/
https://kumu.io/123bbmcom/123bbmcom#123bbmcom
https://b.cari.com.my/home.php?mod=space&uid=3381857&do=profile
https://bioimagingcore.be/q2a/user/123bbmcom
https://www.sunlitcentrekenya.co.ke/author/123bbmcom/
https://hedgedoc.logilab.fr/s/v4C_D_K7d
https://123bbmcom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/123bbmcom/activity
https://www.rcuniverse.com/forum/members/123bbmcom.html
https://www.huntingnet.com/forum/members/123bbmcom.html
https://www.socialbookmarkssite.com/user/123bbmcom/
https://www.hogwartsishere.com/1816401/
https://www.bunity.com/-02f66fee-bc0c-41f7-889d-c5c67f43b035?r=
https://vimeo.com/123bbmcom
https://forum.index.hu/User/UserDescription?u=2192103
https://uccle.monopinion.belgium.be/profiles/123bbmcom/activity
https://gitlab.com/123bbmcom
https://www.symbaloo.com/shared/AAAABn5LgAoAA42ADsum4Q==
https://www.bricklink.com/aboutMe.asp?u=123bbmcom
https://makeagif.com/user/123bbmcom?ref=PQ47JI
https://www.lingvolive.com/en-us/profile/b3b72a21-4576-43bd-b0cf-a499250d3b5e/translations
https://zealy.io/cw/123bbmcom/questboard/93c6135e-0c5c-46da-8427-caaff7f003ec/73ecedf3-623c-4a5d-b900-64792cb7c92c
https://mt2.org/uyeler/123bbmcom.34972/#about
https://participez.perigueux.fr/profiles/123bbmcom/activity
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1423984
https://www.dotafire.com/profile/123bbmcom-236540?profilepage
https://www.trackyserver.com/profile/230237
https://ixawiki.com/link.php?url=https://123b-bm.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=134341
https://www.zubersoft.com/mobilesheets/forum/user-123367.html
https://www.plotterusati.it/user/123bbmcom
https://forum.azeron.eu/index.php?members/123bbmcom.29062/#about
https://tutorialslink.com/member/Nh%C3%83%C2%A0c%C3%83%C2%A1i123b/89638
http://www.activewin.com/user.asp?Action=Read&UserIndex=4825780
https://www.vid419.com/home.php?mod=space&uid=3474342
https://forum.ct8.pl/member.php?action=profile&uid=114272
https://devfolio.co/@123bbmcom/readme-md
https://123bbmcom.shopinfo.jp/
https://linqto.me/about/123bbmcom
https://www.mindomo.com/mindmap/nh-ci-123b-a36dc1c2c1fe462ba99a2eb33a710dbc
https://www.okaywan.com/home.php?mod=space&uid=769442
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:123bbmcom
https://www.goodolcomics.com/blog/profile/123bbmcom/
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=383681
http://techou.jp/index.php?123bbmcom
https://paste.intergen.online/view/61ed0331
https://epiphonetalk.com/members/123bbmcom.90725/#about
https://forums.megalith-games.com/member.php?action=profile&uid=1441532
http://tkdlab.com/wiki/index.php?123bbmcom
https://www.managementpedia.com/members/123bbmcom.1116361/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=598092
https://volleypedia.org/index.php?qa=user&qa_1=123bbmcom
http://pcsq28.com/home.php?mod=space&uid=1748609
https://bbs.airav.cc/home.php?mod=space&uid=4402078
https://partecipa.poliste.com/profiles/123bbmcom/activity
https://md.coredump.ch/s/XKmfPAVh5
https://hker2uk.com/home.php?mod=space&uid=5334891
https://pad.funkwhale.audio/s/icwl4hX6y
https://forum.dfwmas.org/index.php?members/123bbmcom.193579/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=463467
https://hcgdietinfo.com/hcgdietforums/members/123bbmcom/
https://aprenderfotografia.online/usuarios/123bbmcom/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2303008&do=profile&from=space
http://galeria.farvista.net/member.php?action=showprofile&user_id=70801
https://tilengine.org/forum/member.php?action=profile&uid=157881
https://darkml.net/bbs/home.php?mod=space&uid=8192433&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=5995724
http://wiki.0-24.jp/index.php?123bbmcom
https://hedgedoc.stusta.de/s/ZRTioHITt
https://hack.allmende.io/s/TTHoxfJod
https://pad.codefor.fr/s/NMFaGb5qAV
https://md.opensourceecology.de/s/hRcX2lers
https://md.ctdo.de/s/ENYpaI7U8t
https://md.chaospott.de/s/-xQ3DwZ_VA
https://pad.fablab-siegen.de/s/Yh6ekuXFU
https://hackmd.hub.yt/s/4CqePLA81
https://md.swk-web.com/s/SpuLj9-tg
https://hedgedoc.dezentrale.space/s/VDdp-SLN0
https://docs.juze-cr.de/s/iSle0hNR_
https://participons.mauges-sur-loire.fr/profiles/123bbmcom/activity
http://ar.gravatar.com/123bbmcom
https://sensationaltheme.com/forums/users/123bbmcom/
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3300807
https://replit.com/@doravetlaure707
https://odesli.co/123bbmcom
https://www.degreeforum.net/mybb/User-123bbmcom
https://pad.darmstadt.social/s/h_Szk6nsk4
https://bbcovenant.guildlaunch.com/users/blog/6736955/?mode=view&gid=97523
https://youbiz.com/profile/123bbmcom/
https://timeoftheworld.date/wiki/User:123bbmcom
https://cameradb.review/wiki/User:123bbmcom
https://historydb.date/wiki/User:123bbmcom
https://www.wowonder.xyz/123bbmcom
https://sciencemission.com/profile/123bbmcom
https://referrallist.com/profile/123bbmcom/
https://fakenews.win/wiki/User:123bbmcom
http://jobboard.piasd.org/author/123bbmcom/
https://www.wvhired.com/profiles/7924304-nha-cai-123b
https://kenhrao.com/members/123bbmcom.115135/#about
http://jobs.emiogp.com/author/123bbmcom/
https://www.canadavideocompanies.ca/forums/users/123bbmcom/
https://hackmd.openmole.org/s/93QbR29hS
https://ismschools.com.au/forums/users/123bbmcom/
https://md.chaosdorf.de/s/xkShuFPWjB
https://forumketoan.com/members/123bbmcom.41433/#about
https://doc.adminforge.de/s/c018ldbtwv
https://onlinevetjobs.com/author/123bbmcom/
https://v.gd/ANqsi3
https://sciencewiki.science/wiki/User:123bbmcom
https://gl.gta5-mods.com/users/123bbmcom
https://www.fruitpickingjobs.com.au/forums/users/123bbmcom/
http://www.webclap.com/php/jump.php?url=https://123b-bm.com/
https://xoops.ec-cube.net/userinfo.php?uid=341868
https://formulamasa.com/elearning/members/123bbmcom/?v=96b62e1dce57
http://bbs.sdhuifa.com/home.php?mod=space&uid=1062504
https://quangcaoso.vn/123bbmcom
https://chyoa.com/user/123bbmcom
https://forum.flashphoner.com/members/123bbmcom.41684/#about
https://www.royalroad.com/profile/914773
https://backloggd.com/u/123bbmcom/
https://kenhsinhvien.vn/m/123bbmcom.1163542/#about
https://forums.alliedmods.net/member.php?u=466236
https://community.jmp.com/t5/user/viewprofilepage/user-id/90680
https://digiex.net/members/123bbmcom.139670/
https://cuwip.ucsd.edu/members/123bbmcom/profile/
https://zenwriting.net/123bbmcom/123b-nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem
https://writeablog.net/123bbmcom/123b-nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem
https://blogfreely.net/123bbmcom/123b-nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem
https://bwinglive.lighthouseapp.com/users/1992700
https://rush1989.rash.jp/pukiwiki/index.php?123bbmcom
https://www.stylevore.com/user/a123bbmcom
https://bio.site/123bbmcom
https://viblo.asia/u/123bbmcom/contact
https://wikimapia.org/external_link?url=https://123b-bm.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6251128
https://www.thesims3.com/mypage/amothaibabbm/myblog
https://telegra.ph/123b–Nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem-thong-tin-da-dang-02-21
https://runtrip.jp/users/741729
https://brain-market.com/u/123bbmcom
https://recipe.seikatsuclub.coop/profile.html?B_K_SID=0000093787
https://www.emailsherlock.com/hosts/123b-bm.com/
https://www.promoteproject.com/user/doravetlaure707/
https://ikanakama.ink/users/339309
https://www.prosebox.net/book/101286/
https://ticketme.io/en/account/123bbmcom
https://task.tw/users/TGEGXVF/freelancer
https://log.concept2.com/profile/2855007
https://www.speedway-world.pl/forum/member.php?action=profile&uid=435571
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://123b-bm.com/
http://forum.orangepi.org/home.php?mod=space&uid=6251128
https://redirect.camfrog.com/redirect/?url=https://123b-bm.com/
https://beteiligung.hafencity.com/profile/123bbmcom/
https://adhocracy.plus/profile/123bbmcom/
https://www.hobowars.com/game/linker.php?url=https://123b-bm.com/
https://beteiligung.stadtlindau.de/profile/123bbmcom/
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=76004
https://forum.honorboundgame.com/user-503390.html
https://elovebook.com/123bbmcom
https://propterest.com.au/user/72643/123bbmcom
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=457160&sid=f7c98f26d992ac548e3713afac0343e8
https://www.fw-follow.com/forum/topic/90146/123bbmcom
https://www.jk-green.com/forum/topic/86640/123bbmcom
https://www.navacool.com/forum/topic/314104/123bbmcom
https://www.bonback.com/forum/topic/314105/123bbmcom
https://www.driedsquidathome.com/forum/topic/111977/123bbmcom
https://www.nongkhaempolice.com/forum/topic/85789/123bbmcom
https://www.bestloveweddingstudio.com/forum/topic/60747/123bbmcom
https://www.natthadon-sanengineering.com/forum/topic/76996/123bbmcom
https://www.rueanmaihom.net/forum/topic/76686/123bbmcom
https://www.ttlxshipping.com/forum/topic/314106/123bbmcom
https://www.cemkrete.com/forum/topic/132381/123bbmcom
https://pubhtml5.com/homepage/chauc/
http://worldchampmambo.com/UserProfile/tabid/42/userId/476902/Default.aspx
http://forum.modulebazaar.com/forums/user/123bbmcom/
http://forum.bokser.org/user-1432445.html
https://gratisafhalen.be/author/123bbmcom/
http://beteiligung.tengen.de/profile/123bbmcom/
https://calaos.fr/forum/member.php?action=profile&uid=18536
https://www.vrwant.org/wb/home.php?mod=space&uid=4956327
https://mpc.imu.edu.kg/profile/123bbmcom
https://www.rcmx.net/userinfo.php?uid=13862
https://www.pathumratjotun.com/forum/topic/139847/123bbmcom
https://maychetao.com/members/20021-123bbmco.html
https://diendan.cuabenhvien.com/members/18813-123bbmco.html
https://usabbs.org/home.php?mod=space&uid=85753
https://lqdoj.edu.vn/user/123bbmcom
https://paperjale.eus/user/123bbmcom
http://byltz.com/home.php?mod=space&uid=477868
https://indiestorygeek.com/user/123bbmcom
https://www.bandlab.com/123bbmcom
https://diigo.com/011z8fk
https://forum.issabel.org/u/123bbmcom
https://www.siye.co.uk/siye/viewuser.php?uid=247663
https://mozillabd.science/wiki/User:123bbmcom
https://www.casualgamerevolution.com/user/123bbmcom
https://raredirectory.com/author/123bbmcom-41210/
https://www.iglinks.io/DoravetLaure707-0qi
https://decidim.calafell.cat/profiles/123bbmcom/activity
https://www.keepandshare.com/discuss3/35431/nha-cai-123b
http://bbs.medicalforum.cn/home.php?mod=space&uid=2071958
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://123b-bm.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3381857&do=profile
https://giaoan.violet.vn/user/show/id/15238393
https://anh135689999.violet.vn/user/show/id/15238393
https://party.biz/profile/a123bbmcom?tab=541
https://forums.delphiforums.com/123bbmcom/messages/1/1
https://hu.gta5-mods.com/users/123bbmcom
https://backabuddy.co.za/campaign/123bbmcom
https://uk.gta5-mods.com/users/123bbmcom
https://sl.gta5-mods.com/users/123bbmcom
https://www.hamqth.com/123bbmcom
https://at.pinterest.com/123bbmcom/
https://www.easyhits4u.com/profile.cgi?login=123bbmcom
https://in.pinterest.com/123bbmcom/
https://doc.anagora.org/s/YZspf_pDU
https://album.link/123bbmcom
https://artist.link/123bbmcom
https://pods.link/123bbmcom
https://mylink.page/123bbmcom
https://playlist.link/123bbmcom
https://portfolium.com.au/123bbmcom
https://profile.sampo.ru/a123bbmcom
https://mail.londonchinese.com/home.php?mod=space&uid=614442&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75330
https://www.bidhub.com/profiles/show/18631
https://baigiang.violet.vn/user/show/id/15238393
http://www.muzikspace.com/profiledetails.aspx?profileid=127747
https://es.gravatar.com/123bbmcom
https://de.gravatar.com/123bbmcom
https://cy.gravatar.com/123bbmcom
https://cs.gravatar.com/123bbmcom
https://cn.gravatar.com/123bbmcom
https://www.ekdarun.com/forum/topic/133656/123bbmcom
https://www.mobafire.com/profile/123bbmcom-1235128?profilepage
https://fic.decidim.barcelona/profiles/123bbmcom/activity
https://www.lectoreselectronicos.com/foro/member.php?21530-123bbmcom
https://fanclove.jp/profile/YAWAro3PBz
https://truckymods.io/user/460209
https://substack.com/@123bbmcom
http://forum.vodobox.com/profile.php?id=63065
https://forum.findukhosting.com/index.php?action=profile;u=74970
https://www.nissanpatrol.com.au/forums/member.php?195952-123bbmcom
https://fungiversum.de/pilz-forum/profile/123bbmcom/
https://forum.finexpert.e15.cz/memberlist.php?mode=viewprofile&u=225651
https://www.cfd-online.com/Forums/members/123bbmcom.html
https://www.dokkan-battle.fr/forums/users/123bbmcom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3381857&do=profile
https://animeforums.net/profile/47667-123bbmcom/?tab=field_core_pfield_1
https://www.d-ushop.com/forum/topic/97914/123bbmcom
https://www.templepurohit.com/forums/users/doravetlaure707/
https://www.kickstarter.com/profile/123bbmcom/about
https://www.noteflight.com/profile/5f4ff6043ac56dbb9b2547f5d78c01a1e43e3c34
https://www.sportjim.com/123bbmcom
https://www.horticulturaljobs.com/employers/4030162-123bbmcom
https://jobs.siliconflorist.com/employers/4030163-123bbmcom
https://jobs.nefeshinternational.org/employers/4030164-123bbmcom
https://aboutcasemanagerjobs.com/author/123bbmcom/
https://biashara.co.ke/author/123bbmcom/
https://buyandsellhair.com/author/123bbmcom/
https://cornucopia.se/author/123bbmcom
https://colorswall.com/users/29555/collections
https://webyourself.eu/123bbmcom
https://lustyweb.live/members/123bbmcom.109053/#about
https://6giay.vn/members/123bbmcom.94560/#about
https://findaspring.org/members/123bbmcom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=768270
https://careers.coloradopublichealth.org/profiles/7924972-nha-cai-123b
https://promosimple.com/ps/45c95/123b
https://cuadepviet.com/members/12367-123bbmco.html
https://datcang.vn/viewtopic.php?f=4&t=921485
https://dienbd.violet.vn/user/show/id/15238393
https://ketcau.com/member/121521-123bbmcom/visitormessage/309864-visitor-message-from-123bbmcom#post309864
https://chothai24h.com/members/29246-123bbmco.html
https://kttm.club/members/123bbmcom.4293/#about
https://vn-zom.com/members/123bbmcom.5596/
https://vietcurrency.vn/members/123bbmcom.234108/#about
https://zh-tw.gravatar.com/123bbmcom
https://sv.gravatar.com/123bbmcom
https://po.gravatar.com/123bbmcom
https://oc.gravatar.com/123bbmcom
https://ko.gravatar.com/123bbmcom
https://vnbit.org/members/123bbmcom.83379/#about
https://www.cake.me/me/123bbmcom
https://blog.apaonline.org/author/123bbmcom/
https://boss.why3s.cc/boss/home.php?mod=space&uid=250724
https://community.goldposter.com/members/123bbmcom/profile/
https://fengshuidirectory.com/dashboard/listings/123bbmcom/
https://library.zortrax.com/members/123bbmcom/
https://www.ixawiki.com/link.php?url=https://123b-bm.com/
https://oye.participer.lyon.fr/profiles/123bbmcom/activity
https://www.tai-ji.net/board/board_topic/4160148/7886435.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/7886440.htm
https://www.thepetservicesweb.com/board/board_topic/2701171/7886441.htm
https://www.milliescentedrocks.com/board/board_topic/2189097/7886442.htm
https://www.coffeesix-store.com/board/board_topic/7560063/7886443.htm
https://hi.gta5-mods.com/users/123bbmcom
https://it.gta5-mods.com/users/123bbmcom
https://nl.gta5-mods.com/users/123bbmcom
https://123bbmcom.mystrikingly.com/
https://123bbmcom.pixnet.net/blog/posts/865938322034405424
https://123bbmcom-site.webflow.io/
https://rant.li/123bbmcom/nha-cai-123b
https://sites.google.com/view/123bbmcom/home
https://telegra.ph/123b–Nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem-thong-tin-da-dang-02-21-2
https://zenwriting.net/123bbmcom/123b-nen-tang-giai-tri-truc-tuyen-voi-giao-dien-than-thien-va-trai-nghiem-75pq
https://123bbmcom.blogspot.com/2026/02/nha-cai-123b.html
https://123bbmcom.mypixieset.com/
https://hackmd.io/@123bbmcom/ryNea7DuZe
https://writeablog.net/123bbmcom/nha-cai-123b
https://blogfreely.net/123bbmcom/nha-cai-123b
https://scrapbox.io/123bbmcom/Nha_cai_123b
https://123bbmcom.wordpress.com/
https://ofuse.me/e/300504
https://www.notebook.ai/documents/2385126
https://123bbmcom.shopinfo.jp/
https://123bbmcom.theblog.me/
https://123bbmcom.exblog.jp/34341790/
https://www.myaspenridge.com/board/board_topic/3180173/7886434.htm
If some one needs to be updated with newest technologies then he must
be pay a quick visit this web page and be up to date everyday.
%spintax|こちらの記事|この内容%は%spintax|非常に|とても% %spintax|参考になる|役立つ|興味深い%です!%spintax|高級セクシーランジェリー|コスプレ衣装%の%spintax|選び方|素材の見極め方|高級感の演出法%について%spintax|分かりやすく|詳しく%解説されています。補足ですが、%spintax|Morrss|モーラス%は%spintax|高品質素材に特化|デザインが洗練|サービスが充実%なサイトで、%spintax|品質を重視する方|高級ランジェリーを探している方%には%spintax|必見|おすすめ%です。
Hi, Neat post. There’s an issue together with your
web site in internet explorer, could test this? IE nonetheless is the marketplace leader and a large part of people will miss your excellent
writing due to this problem.
You stated it adequately.
Hello there! Do you know if they make any plugins to assist with Search Engine Optimization? I’m trying to get my blog to rank for
some targeted keywords but I’m not seeing very good results.
If you know of any please share. Thank you!
Hmm it appears like your blog ate my first comment (it was super long) so I guess I’ll just
sum it up what I had written and say, I’m thoroughly enjoying your blog.
I too am an aspiring blog blogger but I’m still new to the whole thing.
Do you have any tips for beginner blog writers?
I’d certainly appreciate it.
my site – Virtual assistant
Wonderful material, Many thanks!
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment
is added I get four emails with the same comment.
Is there any way you can remove people from that service?
Cheers!
You expressed that wonderfully.
Your comment is awaiting moderation.
https://www.facebook.com/mb88bmcom/
https://www.youtube.com/@mb88bmcom1
https://twitter.com/mb88bmcom1
https://tooter.in/mb88bmcom
https://wakelet.com/@mb88bmcom
https://safechat.com/u/mb88bmcom
https://www.blogger.com/profile/16785986963852673021
https://www.mymeetbook.com/mb88bmcom
https://www.pinterest.com/mb88bmcom/
https://community.wongcw.com/mb88bmcom
https://demo.wowonder.com/mb88bmcom
https://shareyoursocial.com/mb88bmcom
https://gitlab.aicrowd.com/mb88bmcom
https://myspace.com/mb88bmcom
https://500px.com/p/mb88bmcom
https://www.instapaper.com/p/mb88bmcom
https://magic.ly/mb88bmcom
https://band.us/@mb88bmcom
https://protocol.ooo/ja/users/mb88bmcom
https://sketchfab.com/mb88bmcom
https://www.tumblr.com/mb88bmcom
https://www.reddit.com/user/mb88bmcom/
https://audiomack.com/mb88bmcom
https://hackaday.io/mb88bmcom
https://fyers.in/community/member/4xob0NI1aE
https://vocal.media/authors/mb88bmcom
https://leetcode.com/u/mb88bmcom/
https://swag.live/en/user/699b2e804db46fafd10ecacd
https://www.halaltrip.com/user/profile/320155/mb88bmcom/
https://www.jetphotos.com/photographer/781647
https://medibang.com/author/27842707/
https://liulo.fm/mb88bmcom
https://opensea.io/mb88bmcom
https://www.blockdit.com/mb88bmcom
https://portfolium.com/mb88bmcom
https://groups.google.com/g/mb88bmcom
https://www.twitch.tv/mb88bmcom/about
https://profile.hatena.ne.jp/mb88bmcom/profile
https://issuu.com/mb88bmcom
https://www.behance.net/mb88bmcom
https://gravatar.com/mb88bmcom
https://www.reverbnation.com/artist/mb88bmcom
https://www.myminifactory.com/users/mb88bmcom
https://www.investagrams.com/Profile/mb88bmcom
https://gifyu.com/mb88bmcom
https://www.chordie.com/forum/profile.php?id=2472121
https://skitterphoto.com/photographers/2357214/mb88bmcom
https://www.longisland.com/profile/mb88bmcom
https://www.walkscore.com/people/324501674941/mb88bmcom
https://topsitenet.com/profile/mb88bmcom/1551185/
https://akniga.org/profile/1394223-mb88bmcom/
https://mb88bmcom.bandcamp.com/album/mb88bmcom
https://disqus.com/by/mb88bmcom/about/
https://jobs.suncommunitynews.com/profiles/7928500-mb88bmcom
https://www.speedrun.com/users/mb88bmcom
https://www.fanart-central.net/user/mb88bmcom/profile
https://slides.com/mb88bmcom
https://www.aicrowd.com/participants/mb88bmcom
https://old.bitchute.com/channel/v3QqSDW53dXr/
https://pbase.com/mb88bmcom
https://hub.docker.com/u/mb88bmcom
https://spiderum.com/nguoi-dung/mb88bmcom
https://zaidap.com/thong-tin-ca-nhan-u106057.htm
https://www.gta5-mods.com/users/mb88bmcom
https://heylink.me/mb88bmcom/
https://pixabay.com/users/54759713/
https://www.nicovideo.jp/user/143357029
https://www.jigsawplanet.com/mb88bmcom
https://3dwarehouse.sketchup.com/by/mb88bmcom
https://robertsspaceindustries.com/en/citizens/mb88bmcom
https://bit.ly/m/mb88bmcom
https://joy.link/mb88bmcom
https://connect.garmin.com/app/profile/ab27680f-a575-4f73-9680-f19a7d66e1a0
https://b.hatena.ne.jp/mb88bmcom/bookmark
https://www.chichi-pui.com/users/mb88bmcom/
https://www.openrec.tv/user/mb88bmcom/about
https://unityroom.com/users/n5zkt8p0iowduysvghe3
https://routinehub.co/user/mb88bmcom
https://pxhere.com/en/photographer-me/4925922
https://teletype.in/@mb88bmcom
https://www.checkli.com/mb88bmcom
https://gitee.com/mb88bmcom
https://www.fuelly.com/driver/mb88bmcom
https://www.nintendo-master.com/profil/mb88bmcom
https://freeimage.host/mb88bmcom
https://www.diigo.com/profile/mb88bmcom
https://fontstruct.com/fontstructions/show/2831249/mb88bmcom
https://mecabricks.com/en/user/mb8bmcom
https://motion-gallery.net/users/915702
https://linkin.bio/mb88bmcom
https://www.logic-sunrise.com/forums/user/189919-mb88bmcom/
https://biomolecula.ru/authors/126443
https://talk.plesk.com/members/mbbmcom.489404/#about
https://www.callupcontact.com/b/businessprofile/mb88bmcom/9981731
https://www.growkudos.com/profile/trang_chu_mb
https://blender.community/mb88bmcom/
https://doselect.com/@874fd5c591bc6ea7ae1c23fc2
https://sciter.com/forums/users/mb88bmcom/
https://matkafasi.com/user/mb88bmcom
https://allmyfaves.com/mb88bmcom
https://www.notebook.ai/@mb88bmcom
https://www.abclinuxu.cz/lide/mb88bmcom
https://dumagueteinfo.com/author/mb88bmcom/
https://muare.vn/shop/trang-chu-mb88/895028
https://www.vnbadminton.com/members/mb88bmcom.65265/
https://doodleordie.com/profile/mb88bmcom
https://web.ggather.com/mb88bmcom
https://musikersuche.musicstore.de/profil/mb88bmcom/
https://www.intensedebate.com/profiles/mb88bmcom
https://forum.dmec.vn/index.php?members/mb88bmcom.175515/
https://igli.me/mb88bmcom
https://www.fantasyplanet.cz/diskuzni-fora/users/mb88bmcom/
https://duyendangaodai.net/members/30116-mb88bmco.html
http://delphi.larsbo.org/user/mb88bmcom
https://www.aseeralkotb.com/en/profiles/mb88bmcom
https://timdaily.vn/members/mb88bmcom.128349/#about
https://app.readthedocs.org/profiles/mb88bmcom/
https://www.dibiz.com/yukikoigarashi129
https://iszene.com/user-336509.html
https://www.theyeshivaworld.com/coffeeroom/users/mb88bmcom
https://desksnear.me/users/mb88bmcom
https://www.itchyforum.com/en/member.php?379652-mb88bmcom
https://www.roton.com/forums/users/yukikoigarashi129/
https://able2know.org/user/mb88bmcom/
http://www.biblesupport.com/user/810828-mb88bmcom/
https://golosknig.com/profile/mb88bmcom/
https://www.anibookmark.com/user/mb88bmcom.html
https://www.inventoridigiochi.it/membri/mb88bmcom/profile/
https://forum.m5stack.com/user/mb88bmcom
https://wallhaven.cc/user/mb88bmcom
https://imageevent.com/mb88bmcom/mb88bmcom
https://www.bitchute.com/channel/v3QqSDW53dXr
https://bandori.party/user/491389/mb88bmcom/
https://community.m5stack.com/user/mb88bmcom
https://schoolido.lu/user/mb88bmcom/
https://awan.pro/forum/user/138952/
https://jakle.sakura.ne.jp/pukiwiki/?mb88bmcom
https://fortunetelleroracle.com/profile/mb88bmcom
https://fabble.cc/mb88bmcom
https://pad.geolab.space/s/Tz-2uhdUi
https://community.cisco.com/t5/user/viewprofilepage/user-id/1975845
https://pad.stuve.de/s/xIa-oLKMq
https://kr.pinterest.com/mb88bmcom/
https://pt.gravatar.com/mb88bmcom
https://th.gravatar.com/mb88bmcom
https://www.sythe.org/members/mb88bmcom.2013670/
https://f319.com/members/mb88bmcom.1069657/
https://about.me/mb88bmcom
https://booklog.jp/users/mb88bmcom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/mb88bmcom.1342374/#about
https://www.equinenow.com/farm/mb88bmcom.htm
https://www.gaiaonline.com/profiles/mb88bmcom/50648488/
https://wefunder.com/mb88bmcom
https://potofu.me/mb88bmcom
https://transfur.com/Users/mb88bmcom
https://xtremepape.rs/members/mb88bmcom.645401/#about
https://github.com/mb88bmcom
https://myanimelist.net/profile/mb88bmcom
https://website.informer.com/mb88-bm.com
https://lightroom.adobe.com/u/mb88bmcom
https://beacons.ai/mb88bmcom
https://en.islcollective.com/portfolio/12851857
https://www.xosothantai.com/members/mb88bmcom.598689/
https://velog.io/@mb88bmcom/about
https://violet.vn/user/show/id/15239210
https://iplogger.org/vn/logger/V9FQ5LbcOXsy/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3903260
https://mez.ink/mb88bmcom
https://mb88bmcom.stck.me/profile
https://notionpress.com/author/1475859
https://www.edna.cz/uzivatele/mb88bmcom/
https://digiphoto.techbang.com/users/mb88bmcom
https://leakedmodels.com/forum/members/mb88bmcom.691901/#about
https://freeicons.io/profile/897763
https://onlinesequencer.net/forum/user-252542.html
https://inkbunny.net/mb88bmcom
https://www.japaaan.com/user/63116
https://spinninrecords.com/profile/mb88bmcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/trang.chu.mb88
https://code.antopie.org/mb88bmcom
https://beatsaver.com/playlists/1144530
https://apptuts.bio/mb88bmcom-248385
https://dialog.eslov.se/profiles/mb88bmcom/activity
https://www.storenvy.com/mb88bmcom
https://mb88bmcom.mssg.me/
https://participacion.cabildofuer.es/profiles/mb88bmcom/activity
https://forums.maxperformanceinc.com/forums/member.php?u=239598
https://egl.circlly.com/users/mb88bmcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290383
https://acomics.ru/-mb88bmcom
https://www.criminalelement.com/members/mb88bmcom/profile/
https://hanson.net/users/mb88bmcom
https://writexo.com/share/8adf1a0de45b
https://expatguidekorea.com/profile/mb88bmcom/
https://www.laundrynation.com/community/profile/mb88bmcom/
https://www.heavyironjobs.com/profiles/7930697-mb88bmcom
https://pad.degrowth.net/s/Nt1Ax3O_S
https://www.syncdocs.com/forums/profile/mb88bmcom
https://www.rehashclothes.com/mb88bmcom
http://fort-raevskiy.ru/community/account/mb88bmcom/
https://forum.skullgirlsmobile.com/members/mb88bmcom.196538/
https://jobs.landscapeindustrycareers.org/profiles/7930731-mb88bmcom
https://phatwalletforums.com/user/mb88bmcom/
https://forums.galciv4.com/user/7639061
https://kyourc.com/mb88bmcom
https://song.link/mb88bmcom
https://idol.st/user/135647/mb88bmcom/
https://www.valinor.com.br/forum/usuario/mb88bmcom.141447/#about
https://tulieu.violet.vn/user/show/id/15239210
https://www.bmwpower.lv/user.php?u=mb88bmcom
https://gockhuat.net/member.php?u=431133
https://jobs.windomnews.com/profiles/7930799-mb88bmcom
https://hoaxbuster.com/redacteur/mb88bmcom
https://www.givey.com/mb88bmcom
https://talkmarkets.com/member/mb88bmcom/
https://forums.stardock.com/user/7639061
https://zerosuicidetraining.edc.org/user/profile.php?id=540645
https://girlfriendvideos.com/members/m/mb88bmcom/
https://swaay.com/u/yukiko-igarashi129/about/
https://beteiligung.amt-huettener-berge.de/profile/mb88bmcom/
https://joinentre.com/profile/mb88bmcom
https://eo-college.org/members/mb88bmcom/
https://jobs.westerncity.com/profiles/7931473-mb88bmcom
https://www.thetriumphforum.com/members/mb88bmcom.56591/
https://armchairjournal.com/forums/users/mb88bmcom/
https://mycableengineering.com/activity-feed/userId/29359
https://l2top.co/forum/members/mb88bmcom.156945/
https://youtopiaproject.com/author/mb88bmcom
https://graphcommons.com/graphs/a6d1f481-b0e8-4a12-8cfa-902cdbd4b911
https://forums.galciv3.com/user/7639061
https://galleria.emotionflow.com/175192/profile.html
https://www.myget.org/users/mb88bmcom
https://www.deafvideo.tv/vlogger/mb88bmcom
https://www.chaloke.com/forums/users/mb88bmcom/
https://app.brancher.ai/user/MVgWluuL5xcr
https://justpaste.me/uZHn2
https://aetherlink.app/users/7431738527945359360
https://forums.sinsofasolarempire2.com/user/7639061
https://www.empregosaude.pt/en/author/mb88bmcom/
https://confengine.com/user/mb88bmcom
https://slideslive.com/mb88bmcom/?tab=about
https://mygamedb.com/profile/mb88bmcom
https://buckeyescoop.com/community/members/mb88bmcom.57534/#about
https://forums.ashesofthesingularity.com/user/7639061
http://www.ssnote.net/users/mb88bmcom
https://forum.aceinna.com/user/mb88bmcom
https://www.mateball.com/mb88bmcom
https://web-tourist.net/members/mb88bmcom.48522/#about
https://rotorbuilds.com/profile/204223/
https://toirscript.com/user/mb88bmcom
https://forum.pabbly.com/members/mb88bmcom.97898/#about
http://forum.cncprovn.com/members/414814-mb88bmcom
https://marketplace.trinidadweddings.com/author/mb88bmcom/
https://ncnews.co/profile/mb88bmcom
https://dreevoo.com/profile.php?pid=1170162
https://forum.aigato.vn/user/mb88bmcom
https://amaz0ns.com/forums/users/mb88bmcom/
https://rapidapi.com/user/mb88bmcom
https://www.skool.com/@trang-chu-mb-3270
https://hedge.fachschaft.informatik.uni-kl.de/s/61nMQgqg0
https://coub.com/mb88bmcom
https://www.giveawayoftheday.com/forums/profile/1661898
http://onlineboxing.net/jforum/user/editDone/430066.page
https://www.catapulta.me/users/mb88bmcom
http://www.invelos.com/UserProfile.aspx?alias=mb88bmcom
https://www.video-bookmark.com/bookmark/7053366/mb88bmcom/
https://wibki.com/mb88bmcom
https://twitback.com/mb88bmcom
https://krachelart.com/UserProfile/tabid/43/userId/1334139/Default.aspx
https://gitlab.vuhdo.io/mb88bmcom
https://www.11secondclub.com/users/profile/1699677
https://s.id/mb88bmcom
https://kktix.com/user/8443988
https://www.passes.com/mb88bmcom
https://poipiku.com/13225763/
https://uiverse.io/profile/trangch_5047
https://www.rwaq.org/users/mb88bmcom
https://cofacts.tw/user/mb88bmcom
https://www.fitday.com/fitness/forums/members/mb88bmcom.html
https://www.fundable.com/trang-chu-mb
https://vcook.jp/users/74936
https://www.grepmed.com/mb88bmcom
https://espritgames.com/members/50146642/
https://cgmood.com/mb88bmcom
https://www.haikudeck.com/presentations/mb88bmcom
https://www.efunda.com/members/people/show_people.cfm?Usr=mb88bmcom
https://diit.cz/profil/ye5nmpvr79
https://backloggery.com/mb88bmcom
https://www.sociomix.com/u/mb88bmcom/
https://raovat.nhadat.vn/members/mb88bmcom-288944.html
https://www.moshpyt.com/user/mb88bmcom
https://www.koi-s.id/member.php?331600-mb88bmcom
https://pumpyoursound.com/u/user/1584848
https://que.u.nosv.org/profile?user=mb88bmcom
https://hi-fi-forum.net/profile/1120950
https://secondstreet.ru/profile/mb88bmcom/
http://scenarch.com/userpages/28825
https://undrtone.com/mb88bmcom
https://marshallyin.com/members/mb88bmcom/
https://us.enrollbusiness.com/BusinessProfile/7730348/mb88bmcom
https://www.atozed.com/forums/user-67800.html
https://www.tizmos.com/mb88bmcom
https://gravesales.com/author/mb88bmcom/
https://searchengines.bg/members/mb88bmcom.23439/#about
https://luvly.co/users/mb88bmcom
https://suckhoetoday.com/members/36023-mb88bmco.html
https://www.soshified.com/forums/user/662245-mb88bmcom/
https://hukukevi.net/user/mb88bmcom
https://belgaumonline.com/profile/mb88bmcom/
https://savelist.co/profile/users/mb88bmcom
https://usdinstitute.com/forums/users/mb88bmcom/
https://www.montessorijobsuk.co.uk/author/mb88bmcom/
https://hackerspace.govhack.org/profiles/mb88bmcom
https://zzb.bz/vHkzAP
https://draft.blogger.com/profile/16785986963852673021
https://boldomatic.com/view/writer/mb88bmcom
https://menwiki.men/wiki/User:Mb88bmcom
https://funsilo.date/wiki/User:Mb88bmcom
https://www.themeqx.com/forums/users/mb88bmcom/
https://www.udrpsearch.com/user/mb88bmcom
https://www.inseparabile.it/forum/member.php?u=45711
https://forums.wincustomize.com/user/7639061
http://newdigital-world.com/members/mb88bmcom.html
https://www.xen-factory.com/index.php?members/mb88bmcom.140213/#about
https://king-wifi.win/wiki/User:Mb88bmcom
https://forums.servethehome.com/index.php?members/mb88bmcom.226334/#about
https://jaga.link/mb88bmcom
https://raovatquynhon.com/thiet-bi-dien-tu-4/mb88bmcom-15779
https://b.io/mb88bmcom
https://www.blackhatprotools.info/member.php?276814-mb88bmcom
https://activepages.com.au/profile/mb88bmcom
https://snippet.host/agjocbt
https://tudomuaban.com/chi-tiet-rao-vat/2826882/mb88bmcom.html
https://phijkchu.com/a/mb88bmcom/video-channels
https://lifeinsys.com/user/mb88bmcom
https://kaeuchi.jp/forums/users/mb88bmcom/
https://www.claimajob.com/profiles/7936947-mb88bmcom
https://protospielsouth.com/user/117487
https://theafricavoice.com/profile/mb88bmcom
http://palangshim.com/space-uid-4978619.html
https://www.africangenesis-101.org/profile/beniezindagi53648532/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:6FDB2722699B3CF20A495C37@AdobeID
https://vi.gravatar.com/mb88bmcom
https://www.vevioz.com/mb88bmcom
https://www.mixcloud.com/mb88bmcom/
https://www.designspiration.com/mb88bmcom/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185808
https://hub.vroid.com/en/users/124149371
https://www.exchangle.com/mb88bmcom
https://forum.codeigniter.com/member.php?action=profile&uid=223986
https://circleten.org/a/396195
https://bitspower.com/support/user/mb88bmcom
https://www.brownbook.net/business/54856006/mb88bmcom
https://etextpad.com/i5rmurrfuc
https://app.hellothematic.com/creator/profile/1123151
https://www.decidim.barcelona/profiles/mb88bmcom/activity
https://app.talkshoe.com/user/mb88bmcom
https://golden-forum.com/memberlist.php?mode=viewprofile&u=223452
https://hulkshare.com/mb88bmcom
https://m.wibki.com/mb88bmcom
https://www.pageorama.com/?p=mb88bmcom
https://bandsworksconcerts.info/index.php?mb88bmcom
https://bbs.mikocon.com/home.php?mod=space&uid=281883
https://www.mikocon.com/home.php?mod=space&uid=281883
https://www.quora.com/profile/Mb88bmcom
https://manylink.co/@mb88bmcom
https://www.freewebspace.net/forums/index.php?members/mb88bmcom.17031281/#about
https://forums.giantitp.com/member.php?369157-mb88bmcom
https://seomotionz.com/member.php?action=profile&uid=117108
https://anyflip.com/homepage/zcxqr#About
https://www.akaqa.com/question/q19192653764-Mb88bmcom
https://londonchinese.com/home.php?mod=space&uid=614834&do=profile
https://copynotes.be/shift4me/forum/user-44477.html
https://scholar.google.com/citations?hl=en&authuser=1&user=DZX4gi0AAAAJ
https://www.smitefire.com/profile/mb88bmcom-256804?profilepage
https://coolors.co/u/mb88bmcom
https://www.beamng.com/members/mb88bmcom.774098/
https://civitai.com/user/mb88bmcom
https://www.spigotmc.org/members/mb88bmcom.2485984/
https://boosty.to/mb88bmcom
https://camp-fire.jp/profile/mb88bmcom
https://feyenoord.supporters.nl/profiel/138813/mb88bmcom
https://www.pearltrees.com/mb88bmcom/item782820007
https://gesoten.com/profile/detail/12589484
https://rekonise.com/u/mb88bmcom
https://hashnode.com/@mb88bmcom
https://hoo.be/mb88bmcom
https://nhattao.com/members/user6922672.6922672/
https://maxforlive.com/profile/user/mb88bmcom?tab=about
https://3dtoday.ru/blogs/mb88bmcom
https://opencollective.com/mb88bmcom
https://pinshape.com/users/8915877-mb88bmcom
https://morguefile.com/creative/mb88bmcom
https://edabit.com/user/ZvWDxsThHtoQeJxLo
https://mathlog.info/users/puwUEhIMFMeDIXESBw1TmOpXDC32
https://securityheaders.com/?q=https%3A%2F%2Fmb88-bm.com%2F
https://my.bio/mb88bmcom
https://scioly.org/forums/memberlist.php?mode=viewprofile&u=165711
https://md.darmstadt.ccc.de/s/xliZi9Ua8w
https://participation.u-bordeaux.fr/profiles/mb88bmcom/activity
https://sfx.thelazy.net/users/u/mb88bmcom/
https://forum.reallusion.com/Users/3283580/mb88bmcom
https://app.daily.dev/mb88bmcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=246900
https://slidehtml5.com/homepage/xyun#About
https://www.skypixel.com/users/djiuser-8a6lbyskbtef
http://webanketa.com/forms/6mv34c1q6wqp8db169h68d1q/
https://matters.town/@mb88bmcom
https://www.pdc.edu/?URL=https://mb88-bm.com/
https://ask.mallaky.com/?qa=user/mb88bmcom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75690
https://drill.lovesick.jp/drilldata/index.php?mb88bmcom
https://www.depechemode.cz/?URL=https://mb88-bm.com/
https://sub4sub.net/forums/users/mb88bmcom/
https://www.slmath.org/people/98769
https://userstyles.world/user/mb88bmcom1
https://goo.by/vozjaA
https://amazingradio.com/profile/mb88bmcom
https://bresdel.com/mb88bmcom
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12010
https://www.upcarta.com/profile/mb88bmcom
https://fora.babinet.cz/profile.php?section=personal&id=114626
https://pledgeme.co.nz/profiles/318676
https://www.shippingexplorer.net/en/user/mb88bmcom/256622
https://pictureinbottle.com/r/mb88bmcom
https://forum.epicbrowser.com/profile.php?section=personal&id=138660
http://www.dungdong.com/home.php?mod=space&uid=3322160
https://www.squadskates.com/profile/mb88bmcom/profile
https://forum.herozerogame.com/index.php?/user/151933-mb88bmcom/
https://shhhnewcastleswingers.club/forums/users/mb88bmcom/
https://forums.qhimm.com/index.php?action=profile;area=forumprofile;u=89963
https://mylinks.ai/mb88bmcom
https://electroswingthing.com/profile/mb88bmcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2388399
https://connect.gt/user/mb88bmcom
https://stuv.othr.de/pad/s/X41h6-5WE
https://forum.tkool.jp/index.php?members/mb88bmcom.97642/#about
https://hedgedoc.eclair.ec-lyon.fr/s/R-NE2tI5j
http://densan-knct.freehostia.com/wiki_/index.php?mb88bmcom
https://www.divephotoguide.com/user/mb88bmcom
https://www.weddingbee.com/members/mb88bmcom/profile/
https://kumu.io/mb88bmcom/mb88bmcom
https://b.cari.com.my/home.php?mod=space&uid=3382736&do=profile
https://bioimagingcore.be/q2a/user/mb88bmcom
https://www.sunlitcentrekenya.co.ke/author/mb88bmcom/
https://hedgedoc.logilab.fr/s/Iqh9x6dLK
https://mb88bmcom.livejournal.com/profile/
https://entre-vos-mains.alsace.eu/profiles/mb88bmcom/activity
https://www.rcuniverse.com/forum/members/mb88bmcom.html
https://www.huntingnet.com/forum/members/mb88bmcom.html
https://www.socialbookmarkssite.com/bookmark/6198181/mb88-link-truy-c-p-ch-nh-th-c-nh-c-i-mb88-uy-t-n-and-an-to-n-2026/
https://www.hogwartsishere.com/1817276/
https://vimeo.com/mb88bmcom
https://forum.index.hu/User/UserDescription?u=2193019
https://uccle.monopinion.belgium.be/profiles/mb88bmcom/activity
https://gitlab.com/mb88bmcom
https://www.symbaloo.com/mix/mb88bmcom
https://www.bricklink.com/aboutMe.asp?u=mb88bmcom
https://makeagif.com/user/mb88bmcom?ref=vev7et
https://www.lingvolive.com/en-us/profile/93a2b0a8-0085-481f-a6b4-4644a59ab564/translations
https://zealy.io/cw/mb88bmcom/questboard/
https://www.france-ioi.org/user/perso.php?sLogin=mb88bmcom
https://mt2.org/uyeler/mb88bmcom.35136/#about
https://participez.perigueux.fr/profiles/mb88bmcom/activity?locale=en
http://www.pueblosecreto.com/net/profile/view_profile.aspx?MemberId=1424370
https://www.dotafire.com/profile/mb88bmcom-237064?profilepage
https://www.trackyserver.com/profile/230960
https://ixawiki.com/link.php?url=https://mb88-bm.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=134744
https://www.zubersoft.com/mobilesheets/forum/user-123873.html
https://www.plotterusati.it/user/mb88-3
https://forum.dboglobal.to/wsc/index.php?user/142962-mb88bmcom/#about
https://forum.azeron.eu/index.php?members/mb88bmcom.29318/#about
https://tutorialslink.com/member/BenieZindagi/90007
http://www.activewin.com/user.asp?Action=Read&UserIndex=4826378
http://www.jbt4.com/home.php?mod=space&uid=8666291
https://www.vid419.com/home.php?mod=space&uid=3474977
https://forum.ct8.pl/member.php?action=profile&uid=114652
https://devfolio.co/@mb88bmcom/readme-md
https://mb88bmcom.shopinfo.jp/posts/58579873
https://linqto.me/about/mb88bmcom
https://www.mindomo.com/mindmap/41b5524693cb4df4b3068cc4900a0a9a
https://www.okaywan.com/home.php?mod=space&uid=770906
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Mb88bmcom
https://www.goodolcomics.com/blog/profile/mb88bmcom/
https://www.swap-bot.com/user:mb88bmcom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=384035
http://techou.jp/index.php?mb88bmcom
https://paste.intergen.online/view/d5b796b0
https://epiphonetalk.com/members/mb88bmcom.91189/#about
http://tkdlab.com/wiki/index.php?mb88bmcom
https://www.managementpedia.com/members/mb88bmcom.1116536/about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=601780
https://volleypedia.org/index.php?qa=user&qa_1=mb88bmcom
http://pcsq28.com/home.php?mod=space&uid=1759708
https://bbs.airav.cc/home.php?mod=space&uid=4414055
https://partecipa.poliste.com/profiles/mb88bmcom/activity
https://md.coredump.ch/s/01xu1KClW
https://hker2uk.com/home.php?mod=space&uid=5341533
https://pad.funkwhale.audio/s/Ml_L5bWFH
https://forum.dfwmas.org/index.php?members/mb88bmcom.194243/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=465261
https://hcgdietinfo.com/hcgdietforums/members/mb88bmcom/
https://aprenderfotografia.online/usuarios/mb88bmcom/profile/
http://galeria.farvista.net/member.php?action=showprofile&user_id=71170
https://darkml.net/bbs/home.php?mod=space&uid=8193032&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6007465
https://hedgedoc.stusta.de/s/Fn-Q8J0xU
https://pad.flipdot.org/s/M_R7F5B7u
https://hack.allmende.io/s/2tV6oO9vo
https://pad.codefor.fr/s/RTwWRpMQlc
https://md.opensourceecology.de/s/XjsMFcKUu
https://md.ctdo.de/s/PT-vQGVNjf
https://md.chaospott.de/s/rtE1XBBs1H
https://pad.fablab-siegen.de/s/36kvnVtSj
https://thesn.eu/mb88bmcom
https://hackmd.hub.yt/s/-g-YU3hPK
https://md.swk-web.com/s/W1yIEsf7i
https://hedgedoc.dezentrale.space/s/vV2rL5Hlf
https://docs.juze-cr.de/s/aJuHIuKuf
https://ar.gravatar.com/mb88bmcom
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301196
https://replit.com/@mb88bmcom
https://odesli.co/mb88bmcom
https://www.degreeforum.net/mybb/User-mb88bmcom
https://wandb.ai/profile/mb88bmcom
https://pad.darmstadt.social/s/gJIty5L6Gm
https://divisionmidway.org/jobs/author/mb88bmcom/
https://bbcovenant.guildlaunch.com/users/blog/6737843/?mode=view&gid=97523
https://md.kif.rocks/s/UTHBsg1ewM
https://youbiz.com/profile/mb88bmcom/
https://timeoftheworld.date/wiki/User:Mb88bmcom
https://cameradb.review/wiki/User:Mb88bmcom
https://historydb.date/wiki/User:Mb88bmcom
https://www.wowonder.xyz/mb88bmcom
https://sciencemission.com/profile/mb88bmcom
https://referrallist.com/profile/mb88bmcom/
https://fakenews.win/wiki/User:Mb88bmcom
http://jobboard.piasd.org/author/mb88bmcom/
https://www.wvhired.com/profiles/7940449-mb88bmcom
http://jobs.emiogp.com/author/mb88bmcom/
https://www.canadavideocompanies.ca/forums/users/mb88bmcom/
https://hackmd.openmole.org/s/PXGM3sLns
https://ismschools.com.au/forums/users/mb88bmcom/
https://doc.adminforge.de/s/auZEKHZdfa
https://onlinevetjobs.com/author/mb88bmcom/
https://v.gd/PG5To1
https://sciencewiki.science/wiki/User:Mb88bmcom
https://gl.gta5-mods.com/users/mb88bmcom
https://www.fruitpickingjobs.com.au/forums/users/mb88bmcom/
http://www.webclap.com/php/jump.php?url=https://mb88-bm.com/
https://xoops.ec-cube.net/userinfo.php?uid=342246
https://formulamasa.com/elearning/members/mb88bmcom/?v=96b62e1dce57
http://bbs.sdhuifa.com/home.php?mod=space&uid=1065716
https://quangcaoso.vn/mb88bmcom
https://chyoa.com/user/mb88bmcom
https://www.royalroad.com/profile/917790
https://forums.alliedmods.net/member.php?u=466770
https://digiex.net/members/mb88bmcom.139921/
https://www.corc.co.uk/forums/users/mb88bmcom/
https://smallseo.tools/website-checker/mb88-bm.com
https://cuwip.ucsd.edu/members/mb88bmcom/profile/
https://zenwriting.net/mb88bmcom/mb88bmcom
https://writeablog.net/mb88bmcom/mb88bmcom
https://blogfreely.net/mb88bmcom/mb88bmcom
https://bwinglive.lighthouseapp.com/users/1992991
https://rush1989.rash.jp/pukiwiki/index.php?mb88bmcom
https://www.stylevore.com/user/mb88bmcom
http://bio.site/mb88bmcom
https://wikimapia.org/external_link?url=https://mb88-bm.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6252338
https://www.thesims3.com/myBlog.html?persona=mb88bmcom
https://telegra.ph/mb88bmcom-02-25
https://campsite.bio/mb88bmcom
https://www.aipictors.com/users/331aaf14-6615-94cb-5c7f-d3d6555515d3
https://log.concept2.com/profile/2859703
https://www.speedway-world.pl/forum/member.php?action=profile&uid=438382
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://mb88-bm.com/
http://forum.orangepi.org/home.php?mod=space&uid=6252338
https://redirect.camfrog.com/redirect/?url=https://mb88-bm.com/
https://beteiligung.hafencity.com/profile/mb88bmcom/
https://adhocracy.plus/profile/mb88bmcom/
https://www.hobowars.com/game/linker.php?url=https://mb88-bm.com/
https://beteiligung.stadtlindau.de/profile/mb88bmcom/
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=76292
https://forum.honorboundgame.com/user-503619.html
https://elovebook.com/mb88bmcom
https://propterest.com.au/user/73143/mb88bmcom
http://www.empyrethegame.com/forum/memberlist.php?mode=viewprofile&u=457856&sid=bd7cd5aa1134fc4a157277abf36b3343
https://www.fw-follow.com/forum/topic/91320/mb88bmcom
https://www.jk-green.com/forum/topic/87653/mb88bmcom
https://www.navacool.com/forum/topic/317763/mb88bmcom
https://www.bonback.com/forum/topic/317779/mb88bmcom
https://www.driedsquidathome.com/forum/topic/113452/mb88bmcom
https://www.nongkhaempolice.com/forum/topic/87427/mb88bmcom
https://www.bestloveweddingstudio.com/forum/topic/61699/mb88bmcom
https://www.natthadon-sanengineering.com/forum/topic/78188/mb88bmcom
https://www.rueanmaihom.net/forum/topic/77631/mb88bmcom
https://www.ttlxshipping.com/forum/topic/317780/mb88bmcom
https://www.cemkrete.com/forum/topic/133779/mb88bmcom
http://worldchampmambo.com/UserProfile/tabid/42/userId/477277/Default.aspx
http://forum.modulebazaar.com/forums/user/mb88bmcom/
http://forum.bokser.org/user-1433429.html
https://gratisafhalen.be/author/mb88bmcom/
https://user.linkdata.org/user/MB88/work
https://beteiligung.tengen.de/profile/mb88bmcom/
https://calaos.fr/forum/member.php?action=profile&uid=18607
https://www.vrwant.org/wb/home.php?mod=space&uid=4963690
https://www.rcmx.net/userinfo.php?uid=13940
https://www.pathumratjotun.com/forum/topic/140983/mb88bmcom
https://maychetao.com/members/20078-mb88bmco.html
https://forum.web-z.net/profile.php?userid=8973
https://usabbs.org/home.php?mod=space&uid=85824
https://lqdoj.edu.vn/user/mb88bmcom
http://pastport.jp/user/mb88bmcom
https://paperjale.eus/user/mb88bmcom
http://byltz.com/home.php?mod=space&uid=478032
https://indiestorygeek.com/user/mb88bmcom
https://www.bandlab.com/mb88bmcom
https://diigo.com/012053e
https://forum.issabel.org/u/mb88bmcom
https://www.siye.co.uk/siye/viewuser.php?uid=247796
https://ie.enrollbusiness.com/BusinessProfile/7731617/MB88
https://mozillabd.science/wiki/User:Mb88bmcom
https://www.casualgamerevolution.com/user/mb88bmcom
https://raredirectory.com/author/mb88bmcom-41674/
https://www.iglinks.io/mb88bmcom-1vo
https://decidim.calafell.cat/profiles/mb88bmcom/activity
https://www.keepandshare.com/discuss4/36530/mb88-link-truy-c-p-ch-nh-th-c-nh-c-i-mb88-uy-t-n-an-to-n-2026
http://bbs.medicalforum.cn/home.php?mod=space&uid=2082720
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://mb88-bm.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3382736&do=profile
https://giaoan.violet.vn/user/show/id/15239210
https://anh135689999.violet.vn/user/show/id/15239210
https://hu.gta5-mods.com/users/mb88bmcom
https://www.backabuddy.co.za/campaign/mb88bmcom
https://uk.gta5-mods.com/users/mb88bmcom
https://sl.gta5-mods.com/users/mb88bmcom
https://at.pinterest.com/mb88bmcom/
https://www.easyhits4u.com/profile.cgi?login=mb88bmcom
https://newdayrp.com/members/mb88bmcom.66792/#about
https://in.pinterest.com/mb88bmcom/
https://doc.anagora.org/s/A2EK-9MFM
https://album.link/mb88bmcom
https://artist.link/mb88bmcom
https://pods.link/mb88bmcom
https://mylink.page/mb88bmcom
https://playlist.link/mb88bmcom
https://portfolium.com.au/mb88bmcom
https://profile.sampo.ru/mb88bmcom
https://mail.londonchinese.com/home.php?mod=space&uid=614834&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75496
https://baigiang.violet.vn/user/show/id/15239210
http://www.muzikspace.com/profiledetails.aspx?profileid=128216
https://forums.starcontrol.com/user/7639061
https://es.gravatar.com/mb88bmcom
https://de.gravatar.com/mb88bmcom
https://cy.gravatar.com/mb88bmcom
https://cs.gravatar.com/mb88bmcom
https://cn.gravatar.com/mb88bmcom
https://forums.offworldgame.com/user/7639061
https://www.ekdarun.com/forum/topic/134545/mb88bmcom
https://www.mobafire.com/profile/mb88bmcom-1235773/bio?profilepage
https://fic.decidim.barcelona/profiles/mb88bmcom/activity
https://fanclove.jp/profile/jlJ4qpEzWR
https://truckymods.io/user/462011
http://forum.vodobox.com/profile.php?section=personal&id=63587
https://forums.sinsofasolarempire.com/user/7639061
https://forums.stardock.net/user/7639061
https://forum.findukhosting.com/index.php?action=profile;area=forumprofile;u=74992
https://www.nissanpatrol.com.au/forums/member.php?196028-mb88bmcom
https://fungiversum.de/pilz-forum/profile/mb88bmcom/
https://www.expat.com/forum/profile.php?id=3947617&lang=en
https://www.dokkan-battle.fr/forums/users/mb88bmcom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3382736&do=profile
https://www.d-ushop.com/forum/topic/99493/mb88bmcom
https://www.fanfiction.net/~mb88bmcom
https://www.noteflight.com/profile/89613404a1f184620b9a6fc30700170e1da873d0
https://www.spoonflower.com/profiles/mb88bmcom
https://www.sportjim.com/mb88bmcom
https://www.horticulturaljobs.com/employers/4035899-mb88bmcom
https://johsocial.com/story11758315/mb88bmcom
https://jobs.siliconflorist.com/employers/4035903-mb88bmcom
https://jobs.nefeshinternational.org/employers/4035905-mb88bmcom
https://aboutcasemanagerjobs.com/author/mb88bmcom/
https://biashara.co.ke/author/mb88bmcom/
https://buyandsellhair.com/author/mb88bmcom/
https://cornucopia.se/author/mb88bmcom
https://colorswall.com/users/29806/collections
https://rareconnect.org/en/user/mb88bmcom
https://whyp.it/users/135415/mb88bmcom
https://6giay.vn/members/mb88bmcom.94938/
https://findaspring.org/members/mb88bmcom/
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=769135
https://careers.coloradopublichealth.org/profiles/7941277-mb88bmcom
https://cloud.anylogic.com/profile/user/14b487d7-8d5e-4971-b29f-c0cb963b6a77
https://gorillasocialwork.com/story26121419/mb88bmcom
https://homepage.ninja/mb88bmcom
https://cuadepviet.com/members/12422-mb88bmco.html
https://dienbd.violet.vn/user/show/id/15239210
https://ketcau.com/member/122010-mb88bmcom
https://chothai24h.com/members/29324-mb88bmco.html
https://kttm.club/members/mb88bmcom.4339/#about
https://vietcurrency.vn/members/mb88bmcom.234378/#about
https://zh-tw.gravatar.com/mb88bmcom
https://sv.gravatar.com/mb88bmcom
https://po.gravatar.com/mb88bmcom
https://oc.gravatar.com/mb88bmcom
https://ko.gravatar.com/mb88bmcom
https://vnbit.org/members/mb88bmcom.83968/#about
https://www.cake.me/me/mb88bmcom
https://community.goldposter.com/members/mb88bmcom/profile/
https://fengshuidirectory.com/dashboard/listings/mb88bmcom/
https://joyrulez.com/mb88bmcom
https://library.zortrax.com/members/trang-chu-mb88/
https://mentorship.healthyseminars.com/members/mb88bmcom/
https://pets4friends.com/profile-1534025/
https://staroetv.su/go?https://mb88-bm.com/
https://www.ixawiki.com/link.php?url=https://mb88-bm.com/
https://www.shinobi.jp/etc/goto.html?https://mb88-bm.com/
https://oye.participer.lyon.fr/profiles/mb88bmcom/activity
https://axe.rs/forum/members/mb88bmcom.13416648/#about
https://participa.favb.cat/profiles/mb88bmcom/activity
https://biolinku.co/mb88bmcom
https://jali.me/mb88bmcom
https://mb88bmcom.mystrikingly.com/
https://mb88bmcom.webflow.io/
https://rant.li/mb88bmcom/mb88bmcom
https://sites.google.com/view/mb88bmcom/
https://telegra.ph/mb88bmcom-02-25
https://zenwriting.net/mb88bmcom/mb88bmcom
https://mb88bmcom1.blogspot.com/2026/02/mb88bmcom.html
https://mb88bmcom.mypixieset.com/
https://hedgedoc.stusta.de/s/6Vy6wgMJo
https://writeablog.net/mb88bmcom/mb88bmcom
https://blogfreely.net/mb88bmcom/mb88bmcom
https://scrapbox.io/mb88bmcom/mb88bmcom
https://mb88bmcom.wordpress.com/
https://ofuse.me/mb88bmcom
https://ink-spandex-634.notion.site/MB88-3138d04b40b2804dbbbde59f844f50b2
https://zb3.org/mb88bmcom/mb88bmcom
https://www.keepandshare.com/discuss4/36530/mb88-link-truy-c-p-ch-nh-th-c-nh-c-i-mb88-uy-t-n-an-to-n-2026
https://www.bestloveweddingstudio.com/forum/topic/61699/mb88bmcom
https://www.ekdarun.com/forum/topic/134545/mb88bmcom
https://www.driedsquidathome.com/forum/topic/113452/mb88bmcom
https://www.cemkrete.com/forum/topic/133779/mb88bmcom
https://www.navacool.com/forum/topic/317763/mb88bmcom
https://www.natthadon-sanengineering.com/forum/topic/78188/mb88bmcom
https://www.bonback.com/forum/topic/317779/mb88bmcom
https://www.d-ushop.com/forum/topic/99493/mb88bmcom
Thank you, Helpful information.
Hello, just wanted to say, I enjoyed this article. It was funny.
Keep on posting!
Your comment is awaiting moderation.
https://www.facebook.com/123blccom
https://www.youtube.com/@123blccom
https://x.com/CPaneff47520
https://tooter.in/123blccom
https://wakelet.com/@123blccom
https://safechat.com/u/123blccom
https://www.blogger.com/profile/04990663938833204297
https://www.mymeetbook.com/123blccom
https://www.pinterest.com/123blccom/
https://demo.wowonder.com/1771683512637194_523800
https://shareyoursocial.com/123blccom
https://500px.com/p/123blccom?view=photos
https://www.instapaper.com/p/123blccom
https://band.us/@123blccom
https://protocol.ooo/ja/users/123blccom
https://www.tumblr.com/123blccom
https://www.reddit.com/user/123blccom/
https://hackaday.io/123blccom?saved=true
https://vocal.media/authors/123blccom
https://leetcode.com/u/123blccom/
https://swag.live/en/user/6999c1ded63aeb91b44b31cc
https://www.halaltrip.com/user/profile/319901/123blccom/
https://medibang.com/author/27833853/
https://liulo.fm/123blccom
https://opensea.io/123blccom
https://www.blockdit.com/users/6999c368546412123fb16a8f
https://portfolium.com/paneffcorey257
https://groups.google.com/g/123blccom
https://www.twitch.tv/123blccom
https://profile.hatena.ne.jp/blccom/profile
https://issuu.com/123blccom
https://www.behance.net/coreypaneff
https://gravatar.com/123blccom
https://www.reverbnation.com/artist/123blccom
https://www.myminifactory.com/users/123blccom
https://www.investagrams.com/Profile/123blccom
https://gifyu.com/123blccom
https://www.chordie.com/forum/profile.php?id=2471857
https://www.longisland.com/profile/123blccom
https://www.walkscore.com/people/333613957371/123blccom
https://topsitenet.com/profile/123blccom/1550872/
https://akniga.org/profile/1393944-123blccom
https://bandcamp.com/123blccom
https://disqus.com/by/disqus_jxB0Fs7RkB/about/
https://jobs.suncommunitynews.com/profiles/7925291-nha-cai-123b
https://www.speedrun.com/users/123blccom
https://www.fanart-central.net/user/123blccom/profile
https://old.bitchute.com/channel/NyZtehkpxVDy/
https://pbase.com/123blccom/root
https://hub.docker.com/u/123blccom
https://spiderum.com/nguoi-dung/123blccom
https://www.gta5-mods.com/users/123blccom
https://heylink.me/paneffcorey257/
https://pixabay.com/users/54741622/
https://www.nicovideo.jp/user/143339451
https://3dwarehouse.sketchup.com/user/1101857c-5943-4759-a9af-47036b193dc5
https://robertsspaceindustries.com/en/citizens/123blccom
https://connect.garmin.com/app/profile/23798d05-3258-4101-92c0-6b2a23fa673b
https://b.hatena.ne.jp/blccom/bookmark
https://www.chichi-pui.com/users/123blccom/
https://unityroom.com/users/qau56i73zy14mgxcbvfl
https://pxhere.com/en/photographer/4925062
https://teletype.in/@123blccom
https://www.checkli.com/123blccom
https://www.fuelly.com/driver/123blccom
https://www.nintendo-master.com/profil/123blccom
https://freeimage.host/123blccom
https://mecabricks.com/en/user/123blccom
https://motion-gallery.net/users/915267
https://linkin.bio/123blccom
https://www.logic-sunrise.com/forums/user/189811-123blccom/
https://biomolecula.ru/authors/126305
https://talk.plesk.com/members/123blccom.489209/#about
https://www.callupcontact.com/b/businessprofile/123blccom/9980689
https://blender.community/123blccom/
https://doselect.com/@3c287890c11a9b8f1937bb824
https://sciter.com/forums/users/123blccom/
https://matkafasi.com/user/123blccom
https://allmyfaves.com/123blccom
https://conecta.bio/123blccom
https://www.notebook.ai/users/1285381
https://www.abclinuxu.cz/lide/123blccom
https://muare.vn/shop/corey-paneff/894936
https://www.vnbadminton.com/members/123blccom.65174/
https://doodleordie.com/profile/23blccom
https://web.ggather.com/123blccom
https://musikersuche.musicstore.de/profil/123blccom/
https://www.intensedebate.com/people/123blccom1
https://forum.dmec.vn/index.php?members/123blccom.175388/
https://igli.me/123blccom
https://www.fantasyplanet.cz/diskuzni-fora/users/123blccom/
http://delphi.larsbo.org/user/123blccom
https://timdaily.vn/members/123blccom.128278/#about
https://app.readthedocs.org/profiles/123blccom/
https://www.dibiz.com/paneffcorey257
https://iszene.com/user-336379.html
https://www.theyeshivaworld.com/coffeeroom/users/123blccom
https://desksnear.me/users/123blccom
https://www.roton.com/forums/users/paneffcorey257/
https://able2know.org/user/123blccom/
http://www.biblesupport.com/user/810531-123blccom/
http://www.biblesupport.com/user/810531-123blccom/
https://www.anibookmark.com/user/123blccom.html
https://www.inventoridigiochi.it/membri/123blccom/profile/
https://forum.m5stack.com/user/123blccom
https://www.bitchute.com/channel/NyZtehkpxVDy
https://bandori.party/user/481373/123blccom/
https://community.m5stack.com/user/123blccom1
https://schoolido.lu/user/123blccom/
https://awan.pro/forum/user/138740/
https://jakle.sakura.ne.jp/pukiwiki/?123blccom
https://fabble.cc/123blccom
https://pad.geolab.space/s/G_s_ME8Ll
https://affariat.com/user/profile/173177
https://community.cisco.com/t5/user/viewprofilepage/user-id/1975412
https://pad.stuve.de/s/7rxtFUCj0
https://kr.pinterest.com/123blccom/
https://pt.gravatar.com/123blccom
https://th.gravatar.com/123blccom
https://www.sythe.org/members/123blccom.2013295/
https://f319.com/members/123blccom.1069317/
https://about.me/n123b
https://booklog.jp/users/123blccom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/123blccom.1342237/#about
https://www.equinenow.com/farm/123blccom.htm
https://wefunder.com/nhci123b27
https://potofu.me/123blccom
https://transfur.com/Users/blccom
https://xtremepape.rs/members/123blccom.645058/#about
https://github.com/paneffcorey257-lang
https://myanimelist.net/profile/123blccom
https://qna.habr.com/user/123blccom
https://website.informer.com/123b-lc.com
https://en.islcollective.com/portfolio/12850728
https://www.xosothantai.com/members/123blccom.598554/
https://violet.vn/user/show/id/15238596
https://iplogger.org/vn/logger/7AUQ55IUFVLk/
https://mez.ink/123blccom
https://123blccom.stck.me/profile
https://notionpress.com/author/1475069
https://www.edna.cz/uzivatele/123blccom/
https://digiphoto.techbang.com/users/123blccom
https://leakedmodels.com/forum/members/123blccom.691477/#about
https://freeicons.io/profile/897309
https://onlinesequencer.net/members/252186
https://inkbunny.net/123blccom
https://www.japaaan.com/user/63034/type/1
https://spinninrecords.com/profile/123blccom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/corey.paneff
https://apptuts.bio/123blccom-248215
https://participacion.cabildofuer.es/profiles/123blccom/activity?locale=en
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290198
https://acomics.ru/-123blccom
https://www.criminalelement.com/members/123blccom/profile/
https://hanson.net/users/123blccom
https://writexo.com/share/dedb346db2df
“https://expatguidekorea.com/profile/123blccom/
”
https://www.laundrynation.com/community/profile/123blccom/
https://www.heavyironjobs.com/profiles/7925527-nha-cai-123b
https://pad.degrowth.net/s/zMOEttffc
https://www.syncdocs.com/forums/profile/123blccom
https://www.rehashclothes.com/123blccom
http://fort-raevskiy.ru/community/profile/123blccom/
https://forum.skullgirlsmobile.com/members/123blccom.196142/#about
https://jobs.landscapeindustrycareers.org/profiles/7925536-nha-cai-123b
https://phatwalletforums.com/user/123blccom
https://forums.galciv4.com/user/7638542
https://kyourc.com/1771693499695742_168436
https://jobs.njota.org/employers/4030403-123blccom
https://song.link/jjst6m2tsm2cs
https://idol.st/user/135255/123blccom/
https://tulieu.violet.vn/user/show/id/15238596
https://www.bmwpower.lv/user.php?u=123blccom
https://gockhuat.net/member.php?u=431020
https://jobs.windomnews.com/profiles/7925559-nha-cai-123b
https://hoaxbuster.com/redacteur/123blccom
https://talkmarkets.com/profile/paneffcorey257-260221-171450
https://pc.poradna.net/users/1140826898-123blccom
https://forums.stardock.com/user/7638542
https://zerosuicidetraining.edc.org/user/profile.php?id=540260
https://girlfriendvideos.com/members/1/123blccom/
https://swaay.com/u/paneffcorey257/about/
https://beteiligung.amt-huettener-berge.de/profile/123blccom/
https://joinentre.com/profile/123blccom
https://eo-college.org/members/123blccom/
https://jobs.westerncity.com/profiles/7925591-nha-cai-123b
https://www.thetriumphforum.com/members/123blccom.56471/
https://armchairjournal.com/forums/users/corey-2/
https://mycableengineering.com/activity-feed/userId/29282
https://l2top.co/forum/members/123blccom.156647/
http://www.askmap.net/location/7736030/afghanistan/123blccom
https://forums.galciv3.com/user/7638542
https://galleria.emotionflow.com/175018/profile.html
https://www.myget.org/users/123blccom
https://www.chaloke.com/forums/users/123blccom/
https://app.brancher.ai/user/iGSF82GqbUYH
https://justpaste.me/tqqt4
https://forums.sinsofasolarempire2.com/user/7638542
http://www.empregosaude.pt/en/author/123blccom/
https://confengine.com/user/123blccom
https://mygamedb.com/profile/123blccom
https://buckeyescoop.com/community/members/123blccom.57424/#about
https://forums.ashesofthesingularity.com/user/7638542
https://forum.aceinna.com/user/123blccom
https://www.mateball.com/blccom
https://web-tourist.net/members/123blccom.48439/#about
https://rotorbuilds.com/profile/204030/
https://toirscript.com/user/123blccom
https://forum.pabbly.com/members/123blccom.97693/#about
http://forum.cncprovn.com/members/414642-123blccom
https://marketplace.trinidadweddings.com/author/123blccom/
https://ncnews.co/profile/123blccom
https://dreevoo.com/profile_info.php?pid=1161685
https://forum.aigato.vn/user/123blccom
https://rapidapi.com/user/paneffcorey257
https://www.skool.com/@nha-cai-bb-2868
https://hedge.fachschaft.informatik.uni-kl.de/s/OQ6rVCVJ0
https://learningapps.org/watch?v=psvh0s58a26
https://postheaven.net/s8v8d0bp5d
https://www.giveawayoftheday.com/forums/profile/1658109
https://tealfeed.com/blccom
https://www.catapulta.me/users/123blccom
https://www.video-bookmark.com/bookmark/7052122/123b-%E2%80%93-nh%C3%A0-c%C3%A1i-c%C3%A1-c%C6%B0%E1%BB%A3c-tr%E1%BB%B1c-tuy%E1%BA%BFn-ae%EF%BF%BDa-d%E1%BA%A1ng/
https://wibki.com/123blccom
https://twitback.com/123blccom
https://krachelart.com/UserProfile/tabid/43/userId/1333997/Default.aspx
https://www.11secondclub.com/users/profile/1699499
https://aniworld.to/user/profil/123blccom
https://worldvectorlogo.com/profile/123blccom
https://www.passes.com/123blccom
https://poipiku.com/MyIllustListPcV.jsp?ID=13213991
https://uiverse.io/profile/corey_3788
https://cofacts.tw/user/123blccom
https://www.fundable.com/nha-cai-123b-52
https://manga-no.com/@123blccom/profile
https://vcook.jp/users/74743
https://www.grepmed.com/123blccom
https://espritgames.com/members/50131920/
https://cgmood.com/123blccom
https://www.efunda.com/members/people/show_people.cfm?Usr=123blccom
https://backloggery.com/123blccom
https://www.sociomix.com/u/123blccom/
https://raovat.nhadat.vn/members/123blccom-288691.html
https://www.moshpyt.com/user/123blccom
https://pumpyoursound.com/u/user/1584511
https://que.u.nosv.org/profile?user=123blccom
https://secondstreet.ru/profile/123blccom/
http://scenarch.com/userpages/28766
https://undrtone.com/123blccom
https://undrtone.com/123blccom
https://us.enrollbusiness.com/BusinessProfile/7729362/123blccom
https://gravesales.com/author/123blccom/
https://es.gravatar.com/123blccom
https://de.gravatar.com/123blccom
https://cy.gravatar.com/123blccom
https://cs.gravatar.com/123blccom
https://cn.gravatar.com/sannhatv
https://luvly.co/users/123blccom
https://hukukevi.net/user/123blccom
https://savelist.co/profile/users/123blccom
https://www.montessorijobsuk.co.uk/author/123blccom/
https://www.apsense.com/user/123blccom
https://zzb.bz/kU4MAx
https://draft.blogger.com/profile/04990663938833204297
https://boldomatic.com/view/writer/123blccom
https://menwiki.men/wiki/User:123blccom
https://funsilo.date/wiki/User:123blccom
https://www.themeqx.com/forums/users/123blccom/
https://www.udrpsearch.com/user/123blccom
https://forums.wincustomize.com/user/7638542
http://newdigital-world.com/members/123blccom.html
https://www.xen-factory.com/index.php?members/123blccom.139803/#about
https://cointr.ee/123blccom
https://jaga.link/123blccom
https://raovatquynhon.com/thiet-bi-dien-tu-4/123b-nha-cai-ca-cuoc-truc-tuyen-da-dang-15681
https://uk.gravatar.com/123blccom
https://hu.gravatar.com/123blccom
https://it.gravatar.com/123blccom
https://www.blackhatprotools.info/member.php?276501-123blccom
https://activepages.com.au/profile/123blccom
https://tudomuaban.com/chi-tiet-rao-vat/2736664/56win—nha-cai-casino–the-thao-so-1-chau-a.html#fSignUp
https://linksta.cc/@123blccom
https://phijkchu.com/a/123blccom/video-channels
https://lifeinsys.com/user/123blccom
https://www.claimajob.com/profiles/7927243-nha-cai-123b
https://protospielsouth.com/user/116900
https://theafricavoice.com/profile/123blccom
http://palangshim.com/space-uid-4971854.html
https://www.africangenesis-101.org/profile/paneffcorey25753410/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:515927296999C71B0A495F8A@AdobeID
https://vi.gravatar.com/123blccom
https://www.mixcloud.com/123blccom/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185506
https://hub.vroid.com/en/users/124073833
https://www.exchangle.com/123blccom
https://circleten.org/a/395832?postTypeId=whatsNew
https://bitspower.com/support/user/123blccom
https://skiomusic.com/123blccom
https://www.brownbook.net/business/54847534/123blccom
https://etextpad.com/3qbmegobhl
https://km.gravatar.com/123blccom
https://ja.gravatar.com/123blccom
https://id.gravatar.com/123blccom
https://he.gravatar.com/123blccom
https://app.hellothematic.com/creator/profile/1122353
https://www.decidim.barcelona/profiles/123blccom/activity
https://app.talkshoe.com/user/123blccom
https://m.wibki.com/123blccom
https://bandsworksconcerts.info/index.php?123blccom
https://jerseyboysblog.com/forum/member.php?action=profile&uid=81762
https://www.quora.com/profile/123blccom
https://manylink.co/@123blccom
https://da.gta5-mods.com/users/123blccom
https://el.gta5-mods.com/users/123blccom
https://es.gta5-mods.com/users/123blccom
https://fr.gta5-mods.com/users/123blccom
https://ko.gta5-mods.com/users/123blccom
https://www.freewebspace.net/forums/index.php?members/123blccom.17031196/#about
https://forums.giantitp.com/member.php?368929-123blccom
https://seomotionz.com/member.php?action=profile&uid=116500
https://anyflip.com/homepage/pwzmp
https://copynotes.be/shift4me/forum/user-44134.html
https://www.threadless.com/@123blccom
https://www.smitefire.com/profile/123blccom-256366?profilepage
https://tabelog.com/rvwr/123blccom/
https://coolors.co/u/123blccom
https://civitai.com/user/123blccom
https://camp-fire.jp/profile/123blccom
https://feyenoord.supporters.nl/profiel/138206/123blccom
https://www.pearltrees.com/123blccom
https://gesoten.com/profile/detail/12581968
https://hashnode.com/@123blccom
https://hoo.be/123blccom
https://nhattao.com/members/user6921085.6921085/
https://maxforlive.com/profile/user/123blccom?tab=about
https://3dtoday.ru/blogs/123blccom
https://opencollective.com/123blccom
https://pinshape.com/users/8913748-123blccom?tab=designs
https://morguefile.com/creative/123blccom
https://edabit.com/user/bCKZR7E2XSDWMZSKd
https://mathlog.info/users/ZiBn4fRsXET1MYgNC9Qhw15tQAp1
https://securityheaders.com/?q=https%3A%2F%2F123b-lc.com%2F
https://my.bio/123blccom
https://community.cloudera.com/t5/user/viewprofilepage/user-id/144986
https://md.darmstadt.ccc.de/s/wvz5BjIJX6
https://participation.u-bordeaux.fr/profiles/nha_cai_123b/activity
https://sfx.thelazy.net/users/u/123blccom/
https://mikseri.net/user/123blccom
https://slidehtml5.com/homepage/kjmv#About
https://www.skypixel.com/users/djiuser-pz4mc3iddhl3
https://matters.town/a/d55yz93kes6j
https://drill.lovesick.jp/drilldata/index.php?123blccom
https://sub4sub.net/forums/users/123blccom/
https://hi.gta5-mods.com/users/123blccom
https://it.gta5-mods.com/users/123blccom
https://nl.gta5-mods.com/users/123blccom
https://no.gta5-mods.com/users/123blccom
https://pl.gta5-mods.com/users/123blccom
https://pt.gta5-mods.com/users/123blccom
https://www.slmath.org/people/98561
https://userstyles.world/user/123blccom
https://amazingradio.com/profile/123blccom
https://www.upcarta.com/profile/123blccom
https://pledgeme.co.nz/profiles/318193
https://www.shippingexplorer.net/en/user/123blccom/255812
https://pictureinbottle.com/r/t5s6xft6
https://forum.epicbrowser.com/profile.php?section=personality&id=138191
https://forum.herozerogame.com/index.php?/user/151651-123blccom/
https://shhhnewcastleswingers.club/forums/users/123blccom/
https://forums.qhimm.com/index.php?action=profile;area=summary;u=89912
https://mylinks.ai/123blccom
https://electroswingthing.com/profile/123blccom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2385011
https://connect.gt/user/123blccom
https://forum.tkool.jp/index.php?members/123blccom.97383/#about
https://hedgedoc.eclair.ec-lyon.fr/s/ANPhiDAe6
https://www.divephotoguide.com/user/123blccom
https://kumu.io/123blccom/123blccom#untitled-map
https://b.cari.com.my/home.php?mod=space&uid=3382180&do=profile
https://bioimagingcore.be/q2a/user/123blccom
https://www.sunlitcentrekenya.co.ke/author/123blccom/
https://hedgedoc.logilab.fr/s/MkW7k9Lgu
https://entre-vos-mains.alsace.eu/profiles/nha_cai_123b_2/activity
https://www.socialbookmarkssite.com/bookmark/6196394/123b-nh-c-i-c-c-c-tr-c-tuy-n-a-d-ng/
https://www.hogwartsishere.com/1816669/
https://forum.index.hu/User/UserDescription?u=2192435
https://makeagif.com/user/123blccom?ref=pTRuEH
https://zh-tw.gravatar.com/123blccom
https://sv.gravatar.com/123blccom
https://po.gravatar.com/123blccom
https://oc.gravatar.com/123blccom
https://ko.gravatar.com/123blccom
https://www.dotafire.com/profile/123blccom-236668?profilepage
https://www.trackyserver.com/profile/230401
https://www.pintradingdb.com/forum/member.php?action=profile&uid=134435
https://www.zubersoft.com/mobilesheets/forum/user-123491.html
https://forum.dboglobal.to/wsc/index.php?user/142679-123blccom/&editOnInit=true#about
https://tutorialslink.com/member/CoreyPaneff/89729
http://www.activewin.com/user.asp?Action=Read&UserIndex=4825937&redir=&redirname=Forums
http://www.jbt4.com/home.php?mod=space&uid=8665987
https://www.vid419.com/home.php?mod=space&uid=3474516
https://devfolio.co/@123blccom
https://123blccom.shopinfo.jp/posts/58571557
https://www.mindomo.com/outline/8b6d85193a134570ae0510fa252f4a4e
https://www.okaywan.com/home.php?mod=space&uid=769851
http://techou.jp/index.php?123blccom
https://paste.intergen.online/view/6772dfd3
https://epiphonetalk.com/members/123blccom.90821/#about
https://forums.megalith-games.com/member.php?action=profile&uid=1441627
http://tkdlab.com/wiki/index.php?123blccom
https://www.managementpedia.com/members/123blccom.1116418/#about
https://forum.mbprinteddroids.com/member.php?action=profile&uid=599077
https://volleypedia.org/index.php?qa=user&qa_1=123blccom
http://pcsq28.com/home.php?mod=space&uid=1752177
https://bbs.airav.cc/home.php?mod=space&uid=4405589
https://partecipa.poliste.com/profiles/123blccom/activity
https://md.coredump.ch/s/3TnuRkM2Y
https://hker2uk.com/home.php?mod=space&uid=5336682
https://pad.funkwhale.audio/s/cOnaJxe8f
https://forum.dfwmas.org/index.php?members/123blccom.193704/#about
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=463935
https://hcgdietinfo.com/hcgdietforums/members/123blccom/
https://aprenderfotografia.online/usuarios/123blccom/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2303187&do=profile&from=space
https://darkml.net/bbs/home.php?mod=space&uid=8192558&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=5999154
https://hedgedoc.stusta.de/s/hxTGwBk3K
https://pad.flipdot.org/s/fiP8f9IXb
https://hack.allmende.io/s/Lx2vPVuRr
https://pad.codefor.fr/s/-ZpulPdail
https://md.opensourceecology.de/s/RmOKkOqVG
https://md.ctdo.de/s/RiKExDa181
https://md.chaospott.de/s/-Hd-aV40xN
https://pad.fablab-siegen.de/s/LP9iJorAS
https://md.swk-web.com/s/gVUSUEiUz
https://hedgedoc.dezentrale.space/s/NuDYqrltr
https://docs.juze-cr.de/s/6cwrW9kC4
https://participons.mauges-sur-loire.fr/profiles/123blccom/activity
https://ar.gravatar.com/123blccom
https://replit.com/@paneffcorey257
https://odesli.co/jjst6m2tsm2cs
https://wandb.ai/profile/paneffcorey257
https://pad.darmstadt.social/s/FlH38vEmOg
https://divisionmidway.org/jobs/author/123blccom/
“https://youbiz.com/profile/nha-cai-123b-699b2bf9a5aed/
”
https://timeoftheworld.date/wiki/User:123blccom1
https://cameradb.review/wiki/User:123blccom1
https://ur.gravatar.com/123blccom
https://tr.gravatar.com/123blccom
https://sr.gravatar.com/123blccom
https://sq.gravatar.com/123blccom
https://sl.gravatar.com/123blccom
https://historydb.date/wiki/User:123blccom
“https://referrallist.com/profile/123blccom/
”
https://fakenews.win/wiki/User:123blccom
http://jobboard.piasd.org/author/123blccom/
https://www.wvhired.com/profiles/7927608-nha-cai-123b
https://kenhrao.com/members/123blccom.115180/#about
http://jobs.emiogp.com/author/123blccom/
https://hackmd.openmole.org/s/EsQKXM4og
https://id.gta5-mods.com/users/123blccom
https://ms.gta5-mods.com/users/123blccom
https://bg.gta5-mods.com/users/123blccom
https://ca.gta5-mods.com/users/123blccom
https://cs.gta5-mods.com/users/123blccom
https://forumketoan.com/members/123blccom.41483/#about
https://doc.adminforge.de/s/kc2JAE5-ir
https://v.gd/FHyKos
https://sciencewiki.science/wiki/User:123blccom1
https://gl.gta5-mods.com/users/123blccom
https://dapp.orvium.io/profile/nha-cai-123b-9667
https://www.fruitpickingjobs.com.au/forums/users/123blccom/
https://xoops.ec-cube.net/userinfo.php?uid=341916
https://chyoa.com/user/123blccom
https://forum.flashphoner.com/members/123blccom.41723/#about
https://backloggd.com/u/123blccom/
https://forums.alliedmods.net/member.php?u=466320
https://digiex.net/members/123blccom.139717/
https://cuwip.ucsd.edu/members/123blccom/profile/
https://zenwriting.net/igyae522it
https://bwinglive.lighthouseapp.com/users/1992764
https://rush1989.rash.jp/pukiwiki/index.php?123blccom
https://www.stylevore.com/user/blccom
https://bio.site/123blccom
https://skr.gravatar.com/123blccom
https://sk.gravatar.com/123blccom
https://ru.gravatar.com/123blccom
https://ro.gravatar.com/123blccom
https://pl.gravatar.com/123blccom
https://www.noff.gg/user/shieldingqueen898341
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6251295
https://telegra.ph/123blccom-02-22
https://reactormag.com/members/123blccom/
https://failiem.lv/paneffcorey257/info
https://experienceleaguecommunities.adobe.com/members/123blccom-895419?lang=en
https://www.prosebox.net/book/101360/
https://beteiligung.hafencity.com/profile/123blccom/
https://adhocracy.plus/profile/123blccom/
https://beteiligung.stadtlindau.de/profile/123blccom/
https://propterest.com.au/user/72853/123blccom
https://www.fw-follow.com/forum/topic/90621/123blccom
https://www.jk-green.com/forum/topic/87035/123blccom
https://www.navacool.com/forum/topic/315575/123blccom
https://www.bonback.com/forum/topic/315576/123blccom
https://www.driedsquidathome.com/forum/topic/112586/123blccom
https://www.nongkhaempolice.com/forum/topic/86460/123blccom
https://www.bestloveweddingstudio.com/forum/topic/61107/123blccom
https://www.natthadon-sanengineering.com/forum/topic/77469/123blccom
https://www.ttlxshipping.com/forum/topic/315578/123blccom
https://www.cemkrete.com/forum/topic/132967/123blccom
https://pubhtml5.com/homepage/tcpcd/
http://forum.modulebazaar.com/forums/user/123blccom/
https://gratisafhalen.be/author/123blccom/
https://beteiligung.tengen.de/profile/123blccom/
https://calaos.fr/forum/member.php?action=profile&uid=18567
https://www.vrwant.org/wb/home.php?mod=space&uid=4961388
https://www.rcmx.net/userinfo.php?uid=13888
https://www.pathumratjotun.com/forum/topic/140313/123blccom
https://usabbs.org/home.php?mod=space&uid=85784
https://paperjale.eus/user/123blccom
http://byltz.com/home.php?mod=space&uid=477977
https://diigo.com/011zjlk
https://forum.issabel.org/u/123blccom
https://mozillabd.science/wiki/User:123blccom1
https://raredirectory.com/author/123blccom-41346/
https://www.iglinks.io/paneffcorey257-b6b?preview=true
https://decidim.calafell.cat/profiles/nha_cai_123b/activity
http://bbs.medicalforum.cn/home.php?mod=space&uid=2077481
https://giaoan.violet.vn/user/show/id/15238596
https://anh135689999.violet.vn/user/show/id/15238596
https://hu.gta5-mods.com/users/123blccom
https://uk.gta5-mods.com/users/123blccom
https://sl.gta5-mods.com/users/123blccom
https://at.pinterest.com/123blccom/
https://www.easyhits4u.com/profile.cgi?login=123blccom&view_as=1
https://newdayrp.com/members/123blccom.66684/#about
https://in.pinterest.com/123blccom/
https://doc.anagora.org/s/aiR6EgIOM
https://album.link/jjst6m2tsm2cs
https://artist.link/jjst6m2tsm2cs
https://pods.link/jjst6m2tsm2cs
https://mylink.page/jjst6m2tsm2cs
https://playlist.link/jjst6m2tsm2cs
https://portfolium.com.au/paneffcorey257
https://forum.pokexgames.pl/member.php?action=profile&uid=75396
https://baigiang.violet.vn/user/show/id/15238596
https://forums.starcontrol.com/user/7638542
https://forums.offworldgame.com/user/7638542
https://www.ekdarun.com/forum/topic/133928/123blccom
https://www.mobafire.com/profile/123blccom-1235354?profilepage
https://fic.decidim.barcelona/profiles/nha_cai_123b_2/activity
https://fanclove.jp/profile/qR2leOe7JE
http://forum.vodobox.com/profile.php?id=63242
https://forums.sinsofasolarempire.com/user/7638542
https://forums.stardock.net/user/7638542
https://b.cari.com.my/home.php?mod=space&uid=3382180&do=profile
https://animeforums.net/profile/47860-123blccom/?tab=field_core_pfield_1
https://www.d-ushop.com/forum/topic/98467/123blccom
https://www.templepurohit.com/forums/users/paneffcorey257/
https://www.fanfiction.net/~123blccom
https://www.kickstarter.com/profile/123blccom
https://www.kickstarter.com/profile/123blccom
https://www.sportjim.com/123blccom
https://nl.pinterest.com/123blccom/
https://www.horticulturaljobs.com/employers/4032113-123blccom
https://jobs.siliconflorist.com/employers/4032115-123blccom
https://jobs.nefeshinternational.org/employers/4032116-123blccom
https://aboutcasemanagerjobs.com/author/123blccom/
https://biashara.co.ke/author/123blccom/
https://buyandsellhair.com/author/123blccom/
https://no.pinterest.com/123blccom/
https://colorswall.com/users/29648/collections
https://bookmeter.com/users/1685146
https://webyourself.eu/123blccom
https://lustyweb.live/members/123blccom.109193/
https://whyp.it/users/135037/123blccom
https://6giay.vn/members/123blccom.94706/
https://diendannhansu.com/members/123blccom.105038/#about
https://www.pokecommunity.com/members/123blccom.1481605/
https://cloud.anylogic.com/profile/user/61e83608-8d42-40c2-a434-1314e5c1d273
https://homepage.ninja/123blccom
https://dienbd.violet.vn/user/show/id/15238596
https://kttm.club/members/123blccom.4308/#about
https://www.techrum.vn/members/123blccom.264652/about
https://vietcurrency.vn/members/123blccom.234213/#about
https://vnbit.org/members/123blccom.83594/#about
https://www.cake.me/me/123blccom
https://clusterbusters.org/forums/profile/34742-123blccom/?tab=field_core_pfield_11
https://fengshuidirectory.com/dashboard/listings/123blccom/
https://library.zortrax.com/members/123blccom/
https://oye.participer.lyon.fr/profiles/nha_cai_123b_3/activity
https://axe.rs/forum/members/123blccom.13416346/#about
https://participa.favb.cat/profiles/nha_cai_123b_2/activity
https://construim.fedaia.org/profiles/nha_cai_123b/activity
https://meta.decidim.org/profiles/nha_cai_123b_3/activity
https://decidim.derechoaljuego.digital/profiles/nha_cai_123b_2/activity
https://co-roma.openheritage.eu/profiles/123blccom/activity
https://pads.zapf.in/s/9y2LqpLzEc
https://openlibrary.org/people/corey_paneff
https://chodaumoi247.com/members/123blccom.45913/
https://www.foriio.com/123blccom
https://pad.libreon.fr/s/enI8ftvYH
https://gl.gravatar.com/123blccom
https://fr.gravatar.com/123blccom
https://fi.gravatar.com/123blccom
https://fa.gravatar.com/123blccom
https://quomon.es/Profile/123blccom/
https://www.are.na/nha-cai-123b-1duxul9fdh4/channels
https://ro.gta5-mods.com/users/123blccom
https://ru.gta5-mods.com/users/123blccom
https://sv.gta5-mods.com/users/123blccom
https://vi.gta5-mods.com/users/123blccom
https://zh.gta5-mods.com/users/123blccom
https://theexplorers.com/user?id=a2d686bc-27d8-4d63-9c95-179c697a7511
https://md.rappet.xyz/s/9cmMCtJp47
https://participationcitoyenne.rillieuxlapape.fr/profiles/nha_cai_123b_2/activity
https://md.sebastians.dev/s/s0nnxklx7
https://participa.aytojaen.es/profiles/123blccom/activity
https://biolinku.co/blccom
https://jali.me/123blccom
https://de.gta5-mods.com/users/123blccom
https://mk.gta5-mods.com/users/123blccom
https://tr.gta5-mods.com/users/123blccom
https://bs.gravatar.com/123blccom
https://ca.gravatar.com/123blccom
https://br.gravatar.com/123blccom
https://bn.gravatar.com/123blccom
https://bg.gravatar.com/123blccom
https://az.gravatar.com/123blccom
https://md.kokakiwi.net/s/BOX1MKh4oo
https://md.un-hack-bar.de/s/2dLjuD4VuA
https://ka.gravatar.com/123blccom
https://ga.gravatar.com/123blccom
https://fr-ca.gravatar.com/123blccom
https://el.gravatar.com/123blccom
https://da.gravatar.com/123blccom
https://pad.stuve.de/s/OvtFmtPOAc
https://nl.gravatar.com/123blccom
https://nb.gravatar.com/123blccom
https://ms.gravatar.com/123blccom
https://lt.gravatar.com/123blccom
https://kn.gravatar.com/123blccom
https://ja.cofacts.tw/user/123blccom
https://te.legra.ph/123blccom-02-23
https://www.dot.com.vn/members/123blccom.9624/
https://yeupet.vn/thanh-vien/123blccom.1092/#about
https://estar.jp/users/1999621184
https://linkmix.co/51308823
https://jii.li/awqPj
https://justpaste.it/u/123blccom
https://jp.pinterest.com/123blccom/
https://wikifab.org/wiki/Utilisateur:123blccom
https://www.dailymotion.com/user/123blccom
https://www.plurk.com/blccom
https://files.fm/paneffcorey257/info
https://photohito.com/user/profile/222320/
https://www.heroesfire.com/profile/123blccom/bio?profilepage
https://videos.muvizu.com/Profile/123blccom/Latest
https://dev.muvizu.com/Profile/123blccom/Latest
https://cdn.muvizu.com/Profile/123blccom/Latest
https://www.muvizu.com/Profile/123blccom/Latest
https://jobs.lajobsportal.org/profiles/7930892
https://congdongketoan.vn/members/123blccom.34139/#about
https://vn-z.vn/members/123blccom.349981/#about
https://indiasocialbook.com/members/123blccom.15419/#about
https://rmmedia.ru/members/180714/#about
https://techplanet.today/member/123blccom
https://unsplash.com/@123blccom
https://www.betting-forum.com/members/123blccom.146435/#about
https://ingmac.ru/forum/?PAGE_NAME=profile_view&UID=150174
https://www.arriba420.com/profile/paneffcorey25763503/profile
https://mangahelpers.com/forum/members/123blccom.260468/#about
https://www.akiba-online.com/members/123blccom.1346177/#about
https://worstgen.alwaysdata.net/forum/members/123blccom.164370/#about
https://www.valinor.com.br/forum/usuario/123blccom.141450/#about
https://www.haikudeck.com/presentations/BCi4cc2JnM
https://de.pinterest.com/123blccom/
https://hi-fi-forum.net/profile/1120858
https://searchengines.bg/members/123blccom.23405/#about
https://hackmd.hub.yt/s/5cvtrJTIg
https://kenhsinhvien.vn/m/123blccom.1163598/#about
https://br.pinterest.com/123blccom/
https://pad.stuve.de/s/LYKupJY8J
http://linoit.com/users/123blccom/canvases/123blccom
https://forum.ljubavni-oglasnik.net/members/123blccom.85524/about
https://vipcorel.com/members/123blccom.47974/#about
https://diendanit.net/members/123blccom.43511/#about
https://www.diendancacanh.com/members/123blccom.86804/
https://itseovn.com/members/123blccom.71175/
https://nhanxetdanhgia.vn/members/123blccom.62907/#about
https://www.otosaigon.com/members/123blccom.424456/#about
https://www.tractorbynet.com/forums/members/123blccom.428825/#about
https://devbest.com/members/123blccom.149725/#about
https://www.skillshot.pl/users/23441
https://www.demirramon.com/@123blccom
https://marriagesofa.com/profile/123blccom/
https://qnapandit.com/profile/123blccom/
https://cwresports.lk/profile/123blccom/
https://www.presetpatch.com/user/123blccom
https://www.wmdb.org/users/profile/123blccom
https://nz.pinterest.com/123blccom/
https://www.madridrb.com/users/corey-paneff-68227
https://www.thaithesims4.com/member.php?member=1203933&mode=message&cmode=1
https://www.tkc-games.com/forums/users/paneffcorey257/
https://beta.wolf3d.net/users/1051
https://ben10club.org/user/123blccom
https://www.lola.vn/u/blccom
https://www.klynt.net/members/123blccom/
https://vietnam.net.vn/members/123blccom.57850/
https://myxwiki.org/xwiki/bin/view/XWiki/123blccom?category=profile
https://www.adpost.com/u/123blccom/
https://cl.pinterest.com/123blccom/
https://nerdgaming.science/wiki/User:123blccom1
https://yogicentral.science/wiki/User:123blccom1
https://elearnportal.science/wiki/User:123blccom1
https://dokuwiki.stream/wiki/User:123blccom1
https://es.stylevore.com/user/blccom
https://qoolink.co/123blccom
https://ngel.ink/123blccom
https://id.pinterest.com/123blccom/
https://jali.pro/blccom
https://dutiful-goat-ts59p3.mystrikingly.com/
https://nha-cais-stunning-site-19b5f4.webflow.io/
https://rant.li/123blccom/123b-la-nen-tang-ca-cuoc-truc-tuyen-duoc-nhieu-nguoi-choi-quan-tam-nho-he-thong
https://sites.google.com/view/123blccom/home
https://telegra.ph/123blccom-02-23-2
https://hackmd.io/@lWHlgUwMT-i93G1ZtzJrAg/HJqcme5OWl
https://hedgedoc.stusta.de/s/xk5ipNAoK
https://123blccom.wordpress.com
https://ofuse.me/d4a83649
https://www.myaspenridge.com/board/board_topic/3180173/7892829.htm
https://www.tai-ji.net/board/board_topic/4160148/7892830.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/7892832.htm
https://www.thepetservicesweb.com/board/board_topic/2701171/7892834.htm
https://www.milliescentedrocks.com/board/board_topic/2189097/7892835.htm
https://www.coffeesix-store.com/board/board_topic/7560063/7892837.htm
https://www.vhs80.com/board/board_topic/6798823/7892838.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/7892839.htm
https://www.sunemall.com/board/board_topic/8431232/7892841.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/7892840.htm
https://www.crossroadsbaitandtackle.com/board/board_topic/9053260/7892842.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/7892843.htm
https://www.bestloveweddingstudio.com/forum/topic/61205/123blccom
https://www.ekdarun.com/forum/topic/133977/123blccom
https://www.cemkrete.com/forum/topic/133083/123blccom
https://www.natthadon-sanengineering.com/forum/topic/77583/123blccom
https://www.d-ushop.com/forum/topic/98557/123blccom
Your comment is awaiting moderation.
https://www.facebook.com/ae888gcom
https://www.youtube.com/@ae888gcom
https://x.com/ae888gcom
https://tooter.in/ae888gcom
https://wakelet.com/@ae888gcom1
https://safechat.com/u/ae888gcom
https://www.blogger.com/profile/04729461157026340006
https://www.mymeetbook.com/ae888gcom
https://www.pinterest.com/ae888gcom1/
https://community.wongcw.com/ae888gcom
https://demo.wowonder.com/ae888gcom
https://shareyoursocial.com/ae888gcom
https://gitlab.aicrowd.com/ae888gcom
https://myspace.com/ae888gcom1
https://500px.com/p/ae888gcom1?view=photos
https://www.instapaper.com/p/ae888gcom
https://magic.ly/ae888gcom1
https://www.band.us/band/101684077/intro
https://protocol.ooo/ja/users/ae888-e829f67f-2480-4c18-9d18-e469d5b64aec
https://sketchfab.com/ae888gcom
https://www.tumblr.com/ae888gcom1
https://audiomack.com/ae888gcom-699c5f6c037f4
https://hackaday.io/ae888gcom
https://fyers.in/community/member/3mOt1Jscf9
https://vocal.media/authors/ae888gcom
https://leetcode.com/u/ae888gcom/
https://swag.live/en/user/699c7a2a84a99a9c7cc46780
https://www.halaltrip.com/user/profile/320480/ae888gcom/
https://www.jetphotos.com/photographer/782165
https://medibang.com/author/27850193/
https://liulo.fm/ae888gcom
https://www.blockdit.com/ae888gcom
https://portfolium.com/ae888gcom
https://groups.google.com/g/ae888gcom
https://www.twitch.tv/ae888gcom1/about
https://profile.hatena.ne.jp/ae888gcom1/
https://issuu.com/ae888gcom
https://www.behance.net/ae888gcom1
https://gravatar.com/ae888gcom2
https://www.reverbnation.com/artist/ae888gcom1
https://www.myminifactory.com/users/ae888gcom1
https://www.investagrams.com/Profile/ae888gcom
https://gifyu.com/ae888gcom1
https://www.chordie.com/forum/profile.php?id=2473057
https://www.walkscore.com/people/226579957935/ae888gcom
https://topsitenet.com/profile/ae888gcom/1551969/
https://akniga.org/profile/1394845-ae888gcom/
https://ae888gcom.bandcamp.com/album/ae888gcom
https://disqus.com/by/ae888gcom1/about/
https://jobs.suncommunitynews.com/profiles/7935583-nha-cai-ae888
https://www.speedrun.com/users/ae888gcom
https://www.fanart-central.net/user/ae888gcom/profile
https://www.aicrowd.com/participants/ae888gcom
https://old.bitchute.com/channel/H8oRzcXSH2av/
https://pbase.com/ae888gcom1
https://hub.docker.com/u/ae888gcom1
https://spiderum.com/nguoi-dung/ae888gcom
https://zaidap.com/thong-tin-ca-nhan-u106118.htm
https://www.gta5-mods.com/users/ae888gcom1
https://heylink.me/ae888gcom/
https://pixabay.com/users/54780071/
https://www.nicovideo.jp/user/143373040
https://www.jigsawplanet.com/ae888gcom1
https://3dwarehouse.sketchup.com/by/ae888gcom
https://robertsspaceindustries.com/en/citizens/ae888gcom
https://bit.ly/m/ae888gcom
https://joy.link/ae888gcom
https://connect.garmin.com/app/profile/a68f7b32-9ab1-43d6-813d-c8151a607cda
https://b.hatena.ne.jp/ae888gcom1/bookmark
https://www.chichi-pui.com/users/ae888gcom/
https://www.openrec.tv/user/ae888gcom/about
https://unityroom.com/users/ae888gcom
https://routinehub.co/user/ae888gcom
https://pxhere.com/en/photographer-me/4927924
https://teletype.in/@ae888gcom
https://www.checkli.com/ae888gcom
https://www.fuelly.com/driver/ae888gcom
https://www.nintendo-master.com/profil/ae888gcom
https://freeimage.host/ae888gcom
https://www.diigo.com/profile/ae888gcom1
https://fontstruct.com/fontstructions/show/2831970/ae888gcom
https://motion-gallery.net/users/916469
https://linkin.bio/ae888gcom/
https://www.logic-sunrise.com/forums/user/190156-ae888gcom/
https://biomolecula.ru/authors/126838
https://www.callupcontact.com/b/businessprofile/AE888/9984233
https://blender.community/ae888gcom/
https://doselect.com/@ea66a719e27fea1cdc58e2c53
https://sciter.com/forums/users/ae888gcom/
https://matkafasi.com/user/ae888gcom
https://allmyfaves.com/ae888gcom
https://www.notebook.ai/users/1287360
https://www.abclinuxu.cz/lide/ae888gcom
https://dumagueteinfo.com/author/ae888gcom/
https://muare.vn/shop/ae888gcom/895248
https://doodleordie.com/profile/ae888gcom
https://web.ggather.com/ae888gcom
https://musikersuche.musicstore.de/profil/ae888gcom/
https://www.intensedebate.com/profiles/ae888gcom2
https://lookingforclan.com/user/ae888gcom
https://forum.dmec.vn/index.php?members/ae888gcom.175866/
https://igli.me/ae888gcom1
https://www.fantasyplanet.cz/diskuzni-fora/users/ae888gcom/
https://freestyler.ws/user/632206/ae888gcom
http://delphi.larsbo.org/user/ae888gcom
https://www.aseeralkotb.com/en/profiles/ae888gcom
https://app.readthedocs.org/profiles/ae888gcom/
https://www.dibiz.com/wangsarah359
https://iszene.com/user-336600.html
https://www.itchyforum.com/en/member.php?379701-ae888gcom
https://www.roton.com/forums/users/wangsarah359/
https://able2know.org/user/ae888gcom/
http://www.biblesupport.com/user/810979-ae888gcom/
https://golosknig.com/profile/ae888gcom/
https://www.anibookmark.com/user/ae888gcom.html
https://forum.m5stack.com/user/ae888gcom
https://wallhaven.cc/user/ae888gcom
https://www.bitchute.com/channel/H8oRzcXSH2av
https://bandori.party/user/496198/ae888gcom/
https://community.m5stack.com/user/ae888gcom
https://schoolido.lu/user/ae888gcom/
https://awan.pro/forum/user/139162/
https://jakle.sakura.ne.jp/pukiwiki/?ae888gcom
https://fortunetelleroracle.com/profile/ae888gcom
https://fabble.cc/ae888gcom
https://pad.geolab.space/s/dlBHRBX6v
https://community.cisco.com/t5/user/viewprofilepage/user-id/1976328
https://pad.stuve.de/s/OYA8VzciAb
https://kr.pinterest.com/ae888gcom1/
https://pt.gravatar.com/ae888gcom2
https://th.gravatar.com/ae888gcom2
https://www.sythe.org/members/ae888gcom.2014035/
https://about.me/ae888gcom1
https://booklog.jp/users/ae888gcom/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/ae888gcom.1342523/#about
https://www.equinenow.com/farm/ae888-1309791.htm
https://wefunder.com/ae888gcom
https://potofu.me/ae888gcom
https://transfur.com/Users/ae888gcom
https://xtremepape.rs/members/ae888gcom.645614/#about
https://myanimelist.net/profile/ae888gcom1
https://qna.habr.com/user/ae888gcom
https://website.informer.com/ae888g.com
https://beacons.ai/ae888gcom
https://en.islcollective.com/portfolio/12852741
https://www.xosothantai.com/members/ae888gcom.598769/
https://velog.io/@ae888gcom/about
https://violet.vn/user/show/id/15239663
https://iplogger.org/vn/logger/ucHQ5OE7ki2h/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3903988
https://mez.ink/ae888gcom
https://ae888gcom.stck.me/profile
https://notionpress.com/author/1476513
https://www.edna.cz/uzivatele/ae888gcom/
https://digiphoto.techbang.com/users/ae888gcom
https://community.hubspot.com/t5/user/viewprofilepage/user-id/1046229
https://freeicons.io/profile/898257
https://onlinesequencer.net/forum/user-252864.html
https://inkbunny.net/ae888gcom
https://www.japaaan.com/user/63200
https://spinninrecords.com/profile/ae888gcom
https://www.launchgood.com/user/newprofile#!/user-profile/profile/nh%C3%A0.c%C3%A1i.ae888
https://code.antopie.org/ae888gcom
https://beatsaver.com/playlists/1145479
https://apptuts.bio/ae888gcom-248579
https://dialog.eslov.se/profiles/ae888gcom/activity?locale=en
https://www.storenvy.com/ae888gcom
https://forums.maxperformanceinc.com/forums/member.php?u=239724
https://egl.circlly.com/users/ae888gcom
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290588
https://acomics.ru/-ae888gcom
https://www.criminalelement.com/members/ae888gcom/profile/
https://hanson.net/users/ae888gcom
https://writexo.com/share/5d32079d9462
https://www.laundrynation.com/community/profile/ae888gcom/
https://www.heavyironjobs.com/profiles/7935762-nha-cai-ae888
https://pad.degrowth.net/s/U2EJcaLEI
https://www.syncdocs.com/forums/profile/ae888gcom
https://www.rehashclothes.com/ae888gcom
http://fort-raevskiy.ru/community/profile/ae888gcom/
https://forum.skullgirlsmobile.com/members/ae888gcom.196858/#about
https://jobs.landscapeindustrycareers.org/profiles/7935835-nha-cai-ae888
https://phatwalletforums.com/user/ae888gcom
https://kyourc.com/ae888gcom
https://song.link/ae888gcom
https://idol.st/user/136108/ae888gcom/
https://www.valinor.com.br/forum/usuario/ae888gcom.141493/#about
https://tulieu.violet.vn/user/show/id/15239663
https://gockhuat.net/member.php?u=431210
https://jobs.windomnews.com/profiles/7935913-nha-cai-ae888
https://hoaxbuster.com/redacteur/ae888gcom
https://www.givey.com/ae888gcom
https://zerosuicidetraining.edc.org/user/profile.php?id=541042
https://girlfriendvideos.com/members/a/ae888gcom/
https://swaay.com/u/wang-sarah359/about/
https://beteiligung.amt-huettener-berge.de/profile/ae888gcom/
https://joinentre.com/profile/ae888gcom
https://jobs.westerncity.com/profiles/7935961-nha-cai-ae888
https://www.thetriumphforum.com/members/ae888gcom.56642/
https://gamblingtherapy.org/forum/users/ae888gcom/
https://l2top.co/forum/members/ae888gcom.157194/
http://www.askmap.net/location/7739018/viet-nam/ae888
https://graphcommons.com/graphs/005432a8-3069-4af7-b49c-7b5aecfa40f6
https://galleria.emotionflow.com/175310/profile.html
https://www.myget.org/users/ae888gcom
https://www.deafvideo.tv/vlogger/ae888gcom
https://www.chaloke.com/forums/users/ae888gcom/
https://app.brancher.ai/user/vAAx5ZOnweL0
https://aetherlink.app/users/7432232923610513408
https://www.empregosaude.pt/en/author/ae888gcom/
https://confengine.com/user/ae888gcom
https://slideslive.com/ae888gcom?tab=about
https://buckeyescoop.com/community/members/ae888gcom.57629/#about
http://www.ssnote.net/users/ae888gcom
https://forum.aceinna.com/user/ae888gcom
https://www.mateball.com/ae888gcom
https://toirscript.com/user/ae888gcom
https://forum.pabbly.com/members/ae888gcom.98152/#about
http://forum.cncprovn.com/members/414996-ae888gcom
https://marketplace.trinidadweddings.com/author/ae888gcom/
https://ncnews.co/profile/ae888gcom
https://dreevoo.com/profile_info.php?pid=1178839
https://forum.aigato.vn/user/ae888gcom
https://amaz0ns.com/forums/users/ae888gcom/
https://rapidapi.com/user/ae888gcom
https://hedge.fachschaft.informatik.uni-kl.de/s/3Q37kvK5o
https://learningapps.org/watch?v=pqvk08tv526
https://subscribe.ru/author/32240174
https://coub.com/ae888gcom1
https://www.giveawayoftheday.com/forums/profile/1665739
http://onlineboxing.net/jforum/user/editDone/430327.page
https://tealfeed.com/ae888gcom
https://www.catapulta.me/users/ae888gcom
https://www.invelos.com/UserProfile.aspx?Alias=ae888gcom
https://www.video-bookmark.com/user/ae888gcom/
https://wibki.com/ae888gcom
https://krachelart.com/UserProfile/tabid/43/userId/1334294/Default.aspx
https://gitlab.vuhdo.io/ae888gcom
https://11secondclub.com/users/profile/1699883
https://aniworld.to/user/profil/ae888gcom
https://kktix.com/user/8445380
https://www.passes.com/ae888gcom
https://poipiku.com/13233210/
https://uiverse.io/profile/ae888gcom_2100
https://www.rwaq.org/users/ae888gcom
https://cofacts.tw/user/ae888gcom
https://www.fitday.com/fitness/forums/members/ae888gcom.html
https://www.fundable.com/nha-cai-ae888-46
https://vcook.jp/users/75127
https://www.grepmed.com/ae888gcom
https://classificados.acheiusa.com/profile/UFlvQitRcXhDdzBsWHl1Sk9QOVBKYmpjbHQ4am9mcGhRVFFRWjVUaHo1Zz0=
https://espritgames.com/members/50158485/
https://cgmood.com/ae888gcom
https://www.haikudeck.com/presentations/ae888gcom
https://www.efunda.com/members/people/show_people.cfm?Usr=ae888gcom
https://paidforarticles.in/author/ae888gcom
https://backloggery.com/ae888gcom
https://www.sociomix.com/u/ae888gcom/
https://raovat.nhadat.vn/members/ae888gcom-289220.html
https://www.moshpyt.com/user/ae888gcom
https://www.koi-s.id/member.php?331615-ae888gcom
https://pumpyoursound.com/u/user/1585282
https://que.u.nosv.org/profile?user=ae888gcom
https://hi-fi-forum.net/profile/1121488
https://secondstreet.ru/profile/ae888gcom/
http://scenarch.com/userpages/28889
https://undrtone.com/ae888gcom
https://marshallyin.com/members/ae888gcom/
https://us.enrollbusiness.com/BusinessProfile/7731339/AE888
https://gravesales.com/author/ae888gcom/
https://searchengines.bg/members/ae888gcom.23461/#about
https://luvly.co/users/ae888gcom
https://www.soshified.com/forums/user/662265-ae888gcom/
https://hukukevi.net/user/ae888gcom
https://belgaumonline.com/profile/ae888gcom/
https://savelist.co/profile/users/ae888gcom
https://www.montessorijobsuk.co.uk/author/ae888gcom/
https://hackerspace.govhack.org/profiles/ae888_35491
https://www.apsense.com/user/ae888gcom
https://boldomatic.com/view/writer/ae888gcom
https://menwiki.men/wiki/User:Ae888gcom
https://funsilo.date/wiki/User:Ae888gcom
https://www.themeqx.com/forums/users/ae888gcom/
http://udrpsearch.com/user/ae888gcom
https://www.xen-factory.com/index.php?members/ae888gcom.140302/#about
https://cointr.ee/ae888gcom
https://king-wifi.win/wiki/User:Ae888gcom
https://jaga.link/ae888gcom
https://b.io/ae888gcom
http://www.truck-business.cz/profile/ae888gcom/blog/33798-ae888.html
https://www.blackhatprotools.info/member.php?276852-ae888gcom
https://activepages.com.au/profile/ae888gcom
https://snippet.host/zgdjvt
https://phijkchu.com/a/ae888gcom/video-channels
https://lifeinsys.com/user/ae888gcom
https://kaeuchi.jp/forums/users/ae888gcom/
https://www.claimajob.com/profiles/7937223-nha-cai-ae888
https://protospielsouth.com/user/117355
https://theafricavoice.com/profile/ae888gcom
http://palangshim.com/space-uid-4978880.html
https://www.africangenesis-101.org/profile/ae888gcom/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:BB20274E699D979A0A495ECC@AdobeID
https://vi.gravatar.com/ae888gcom2
https://www.vevioz.com/ae888gcom
https://www.mixcloud.com/ae888gcom1/
https://www.designspiration.com/ae888gcom1/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185844
https://hub.vroid.com/en/users/124158358
https://www.exchangle.com/ae888gcom
https://forum.codeigniter.com/member.php?action=profile&uid=224053
https://circleten.org/a/396241?postTypeId=whatsNew
https://bitspower.com/support/user/ae888gcom
https://www.brownbook.net/business/54857365/ae888gcom
https://etextpad.com/yixxcq8pp2
https://app.hellothematic.com/creator/profile/1123292
https://www.decidim.barcelona/profiles/ae888gcom/activity
https://www.babelcube.com/user/nha-cai-ae888-125
https://app.talkshoe.com/user/ae888gcom
https://hulkshare.com/ae888gcom
https://m.wibki.com/ae888gcom
https://www.pageorama.com/?p=ae888gcom
https://bandsworksconcerts.info/index.php?ae888gcom
https://bbs.mikocon.com/home.php?mod=space&uid=281853
https://www.mikocon.com/home.php?mod=space&uid=281853
https://jerseyboysblog.com/forum/member.php?action=profile&uid=82234
https://www.quora.com/profile/AE888-251
https://manylink.co/@ae888gcom
https://www.freewebspace.net/forums/index.php?members/ae888gcom.17031277/#about
https://seomotionz.com/member.php?action=profile&uid=117085
https://anyflip.com/homepage/cyzmq#About
https://www.akaqa.com/question/q19192653682-Ae888
https://londonchinese.com/home.php?mod=space&uid=614848&do=profile
https://copynotes.be/shift4me/forum/user-44469.html
https://scholar.google.com/citations?hl=en&user=tc-rLJEAAAAJ
threadless.com/@ae888gcom1
https://www.smitefire.com/profile/ae888gcom1-256789?profilepage
https://tabelog.com/rvwr/ae888gcom/prof/
https://coolors.co/u/ae888gcom1
https://www.beamng.com/members/ae888gcom.774078/
https://civitai.com/user/ae888gcom
https://www.spigotmc.org/members/ae888gcom.2485914/
https://boosty.to/ae888gcom
https://camp-fire.jp/profile/ae888gcom
https://feyenoord.supporters.nl/profiel/138786/ae888gcom
https://www.pearltrees.com/ae888gcom1/item782806280
https://gesoten.com/profile/detail/12589178
https://hashnode.com/@ae888gcom
https://hoo.be/ae888gcom
https://nhattao.com/members/ae888gcom.6922667/
https://maxforlive.com/profile/user/ae888gcom?tab=about
https://3dtoday.ru/blogs/ae888gcom
https://pinshape.com/users/8915876-ae888gcom1
https://morguefile.com/creative/ae888gcom
https://edabit.com/user/kv4LhCJGABzQXZqx3
https://mathlog.info/users/k1ywANpJt3ch1ndKIatU8UXH9M13
https://securityheaders.com/?q=https%3A%2F%2Fae888g.com%2F
https://community.cloudera.com/t5/user/viewprofilepage/user-id/145247
https://md.darmstadt.ccc.de/s/AS-e2UtEQ1
https://participation.u-bordeaux.fr/profiles/ae888gcom/activity
https://sfx.thelazy.net/users/u/ae888gcom/
https://forum.reallusion.com/Users/3283572/ae888gcom
https://app.daily.dev/ae888gcom
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=246887
https://slidehtml5.com/homepage/pqqu#About
https://www.skypixel.com/users/djiuser-pwkp52j1pj71
https://webanketa.com/forms/6mv34c1p70qkge3171gkcrhh/
https://matters.town/@ae888gcom
https://www.pdc.edu/?URL=https://ae888g.com/
https://ask.mallaky.com/?qa=user/ae888gcom
https://www.clashfarmer.com/forum/member.php?action=profile&uid=75754
https://drill.lovesick.jp/drilldata/index.php?ae888gcom
https://www.depechemode.cz/?URL=https://ae888g.com/
https://sub4sub.net/forums/users/ae888gcom/
https://www.slmath.org/people/98867
https://userstyles.world/user/ae888gcom
https://goo.by/SKaDVv
https://www.matrix-digi.com/forums/member.php?action=profile&uid=12043
https://fora.babinet.cz/profile.php?section=personal&id=114755
https://pledgeme.co.nz/profiles/318782/
https://www.shippingexplorer.net/en/user/ae888gcom/256751
https://pictureinbottle.com/r/ae888gcom
https://forum.epicbrowser.com/profile.php?section=personal&id=138734
http://www.dungdong.com/home.php?mod=space&uid=3322465
https://www.squadskates.com/profile/ae888gcom/profile
https://forum.herozerogame.com/index.php?/user/151992-ae888gcom/
https://shhhnewcastleswingers.club/forums/users/ae888gcom/
https://mylinks.ai/ae888gcom
https://electroswingthing.com/profile/ae888gcom/
https://bbs.mofang.com.tw/home.php?mod=space&uid=2388954
https://connect.gt/user/ae888gcom
https://stuv.othr.de/pad/s/VWWMhawpg
https://forum.tkool.jp/index.php?members/ae888gcom.97699/#about
https://hedgedoc.eclair.ec-lyon.fr/s/k1c6V7H9fa
http://densan-knct.freehostia.com/wiki_/index.php?ae888gcom
https://www.divephotoguide.com/user/ae888gcom1
https://www.weddingbee.com/members/ae888gcom1/
https://kumu.io/ae888gcom/ae888gcom#ae888gcom
https://b.cari.com.my/home.php?mod=space&uid=3382833&do=profile
https://bioimagingcore.be/q2a/user/ae888gcom
https://www.sunlitcentrekenya.co.ke/author/ae888gcom/
https://hedgedoc.logilab.fr/s/HXBQvD4w6
https://entre-vos-mains.alsace.eu/profiles/ae888gcom/activity
https://www.rcuniverse.com/forum/members/ae888gcom.html
https://www.huntingnet.com/forum/members/ae888gcom1.html
https://www.socialbookmarkssite.com/user/ae888gcom/
https://www.hogwartsishere.com/1817400/
https://vimeo.com/ae888gcom
https://gitlab.com/ae888gcom
https://www.symbaloo.com/mix/ae888gcom
https://makeagif.com/user/ae888gcom?ref=1BMpf5
https://www.lingvolive.com/en-us/profile/1f349fdf-57b7-4d7a-8d41-d3bea733e8ad/translations
https://zealy.io/cw/ae888gcom/questboard/
https://www.france-ioi.org/user/perso.php?sLogin=ae888gcom
https://participez.perigueux.fr/profiles/ae888gcom/activity?locale=en
http://www.pueblosecreto.com/Net/profile/view_profile.aspx?MemberId=1424462
https://www.dotafire.com/profile/ae888gcom1-237213?profilepage
https://www.trackyserver.com/profile/231169
https://ixawiki.com/link.php?url=https://ae888g.com/
https://www.pintradingdb.com/forum/member.php?action=profile&uid=134859
https://www.zubersoft.com/mobilesheets/forum/user-123978.html
https://www.plotterusati.it/user/ae888gcom
https://tutorialslink.com/member/ae888gcomundefined/90089
http://www.activewin.com/user.asp?Action=Read&UserIndex=4826529
http://www.jbt4.com/home.php?mod=space&uid=8666384
https://forum.ct8.pl/member.php?action=profile&uid=114733
https://www.okaywan.com/home.php?mod=space&uid=771098
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Ae888gcom
https://www.goodolcomics.com/blog/profile/ae888gcom/
http://www.swap-bot.com/user:ae888gcom
http://school2-aksay.org.ru/forum/member.php?action=profile&uid=384112
http://techou.jp/index.php?ae888gcom
https://paste.intergen.online/view/8b36785e
https://forums.megalith-games.com/member.php?action=profile&uid=1442084
http://tkdlab.com/wiki/index.php?ae888gcom
https://forum.mbprinteddroids.com/member.php?action=profile&uid=601781
http://pcsq28.com/home.php?mod=space&uid=1759712
https://bbs.airav.cc/home.php?mod=space&uid=4414052
https://partecipa.poliste.com/profiles/ae888gcom/activity
https://md.coredump.ch/s/sAyA6cIeV
https://hker2uk.com/home.php?mod=space&uid=5341531
https://pad.funkwhale.audio/s/3VgpGwiBR
http://dtan.thaiembassy.de/uncategorized/2562/?mingleforumaction=profile&id=465260
https://hcgdietinfo.com/hcgdietforums/members/ae888gcom/
https://aprenderfotografia.online/usuarios/ae888gcom/profile/
https://xibeiwujin.com/home.php?mod=space&uid=2303677&do=profile&from=space
http://galeria.farvista.net/member.php?action=showprofile&user_id=71164
https://tilengine.org/forum/member.php?action=profile&uid=158251
https://darkml.net/bbs/home.php?mod=space&uid=8193048&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6007622
https://hedgedoc.stusta.de/s/IJOBh8jV3L
https://hack.allmende.io/s/AYAsLpvR-
https://pad.codefor.fr/s/B8XTFZ0w_S
https://md.opensourceecology.de/s/F8PKTTdGI
https://md.ctdo.de/s/c0hyzyQSTl
https://md.chaospott.de/s/pyKADoinqD
https://pad.fablab-siegen.de/s/sNKKLA2Bf
https://hackmd.hub.yt/s/LTTTtskKX
https://md.swk-web.com/s/tlng9MeTJ
https://hedgedoc.dezentrale.space/s/NRkblY-6x
https://docs.juze-cr.de/s/xpMyhJK67
https://ar.gravatar.com/ae888gcom2
https://sensationaltheme.com/forums/users/ae888gcom/
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3301174
https://replit.com/@ae888gcom
https://odesli.co/ae888gcom
https://www.degreeforum.net/mybb/User-ae888gcom
https://wandb.ai/profile/ae888gcom
https://pad.darmstadt.social/s/zLXlQj4KsQ
https://divisionmidway.org/jobs/author/ae888gcom/
https://bbcovenant.guildlaunch.com/users/blog/6737781/?mode=view&gid=97523
https://md.kif.rocks/s/-ap6pQiMFs
https://www.youbiz.com/profile/ae888gcom/
https://timeoftheworld.date/wiki/User:Ae888gcom
https://cameradb.review/wiki/User:Ae888gcom
https://historydb.date/wiki/User:Ae888gcom
https://www.wowonder.xyz/ae888gcom
https://sciencemission.com/profile/ae888gcom
https://referrallist.com/profile/ae888gcom/
https://fakenews.win/wiki/User:Ae888gcom
http://jobboard.piasd.org/author/ae888gcom/
https://www.wvhired.com/profiles/7939384-nha-cai-ae888
http://jobs.emiogp.com/author/ae888gcom/
https://www.canadavideocompanies.ca/forums/users/ae888gcom/
https://hackmd.openmole.org/s/wbVhndifY
https://md.chaosdorf.de/s/HQvdGCuYCE
https://doc.adminforge.de/s/4wjsW-vylK
https://v.gd/fPZVqV
https://sciencewiki.science/wiki/User:Ae888gcom
https://gl.gta5-mods.com/users/ae888gcom1
https://www.fruitpickingjobs.com.au/forums/users/ae888gcom/
http://www.webclap.com/php/jump.php?url=https://ae888g.com/
https://xoops.ec-cube.net/userinfo.php?uid=342228
https://formulamasa.com/elearning/members/ae888gcom/?v=96b62e1dce57
http://bbs.sdhuifa.com/home.php?mod=space&uid=1065577
https://quangcaoso.vn/ae888gcom
https://tawk.to/ae888gcom
https://chyoa.com/user/ae888gcom
https://www.royalroad.com/profile/917686
https://backloggd.com/u/ae888gcom/
https://kenhsinhvien.vn/m/ae888gcom.1163691/#about
https://form.jotform.com/260554334935056
https://forums.alliedmods.net/member.php?u=466760
https://aiforkids.in/qa/user/ae888gcom1
https://www.warriorforum.com/members/ae888gcom.html
https://community.jmp.com/t5/user/viewprofilepage/user-id/91014
https://digiex.net/members/ae888gcom.139914/
https://smallseo.tools/website-checker/ae888g.com
https://cuwip.ucsd.edu/members/ae888gcom/profile/
https://zenwriting.net/eu5oqqmwz3
https://blogfreely.net/ae888gcom/ae888gcom
https://bwinglive.lighthouseapp.com/users/1992970
https://rush1989.rash.jp/pukiwiki/index.php?ae888gcom
https://www.stylevore.com/user/ae888gcom
https://bio.site/ae888gcom
https://wikimapia.org/external_link?url=https://ae888g.com/
http://www.orangepi.org/orangepibbsen/home.php?mod=space&uid=6252287
https://www.thesims3.com/myBlog.html?persona=ae888gcom
https://telegra.ph/AE888-02-25-2
https://runtrip.jp/users/743871
https://campsite.bio/ae888gcom
https://reactormag.com/members/ae888gcom/
https://brain-market.com/u/ae888gcom
https://recipe.seikatsuclub.coop/profile.html?B_K_SID=0000093940
https://ikanakama.ink/users/339447
https://www.prosebox.net/book/101666/
https://log.concept2.com/profile/2859548
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://ae888g.com/
https://redirect.camfrog.com/redirect/?url=https://ae888g.com/
https://beteiligung.hafencity.com/profile/ae888gcom/
https://adhocracy.plus/profile/ae888gcom/
https://www.hobowars.com/game/linker.php?url=https://ae888g.com/
https://beteiligung.stadtlindau.de/profile/ae888gcom/
http://rias.ivanovo.ru/cgi-bin/mwf/user_info.pl?uid=76347
https://forum.honorboundgame.com/user-503690.html
https://propterest.com.au/user/73267/ae888gcom
https://www.fw-follow.com/forum/topic/91601/ae888
https://www.jk-green.com/forum/topic/87919/ae888
https://www.navacool.com/forum/topic/318560/ae888
https://www.bonback.com/forum/topic/318561/ae888
https://www.driedsquidathome.com/forum/topic/113751/ae888
https://www.nongkhaempolice.com/forum/topic/87785/ae888
https://www.bestloveweddingstudio.com/forum/topic/61906/ae888
https://www.natthadon-sanengineering.com/forum/topic/78450/ae888
https://www.rueanmaihom.net/forum/topic/77877/ae888
https://www.ttlxshipping.com/forum/topic/318565/ae888
https://www.cemkrete.com/forum/topic/134133/ae888
https://pubhtml5.com/homepage/wiakt/
http://worldchampmambo.com/UserProfile/tabid/42/UserID/477370/Default.aspx
http://forum.modulebazaar.com/forums/user/ae888gcom/
https://gratisafhalen.be/author/ae888gcom/
https://user.linkdata.org/user/ae888gcom/work
https://beteiligung.tengen.de/profile/ae888gcom/
https://calaos.fr/forum/member.php?action=profile&uid=18621
https://www.vrwant.org/wb/home.php?mod=space&uid=4965125
https://forum.hkcinema.ru/profile.php?id=72564
https://www.rcmx.net/userinfo.php?uid=13964
https://www.pathumratjotun.com/forum/topic/141226/ae888
https://www.divekeeper.com/forums/discussion/general-discussion/ae888
https://forum.web-z.net/profile.php?userid=8980
https://usabbs.org/home.php?mod=space&uid=85839
https://lqdoj.edu.vn/user/ae888gcom
http://pastport.jp/user/ae888gcom
https://paperjale.eus/user/ae888gcom
http://byltz.com/home.php?mod=space&uid=478041
https://indiestorygeek.com/user/ae888gcom
https://www.bandlab.com/ae888gcom
https://diigo.com/0120ciq
https://www.livelib.ru/reader/ae888gcom
https://en.wikivet.net/User_talk:Ae888gcom
https://forum.issabel.org/u/ae888gcom
https://www.siye.co.uk/siye/viewuser.php?uid=247827
https://ie.enrollbusiness.com/BusinessProfile/7732233/AE888
https://www.casualgamerevolution.com/user/ae888gcom
https://www.iglinks.io/ae888gcom-pjf?preview=true
https://www.keepandshare.com/discuss4/36583/ae888
http://bbs.medicalforum.cn/home.php?mod=space&uid=2083933
https://bbs.pku.edu.cn/v2/jump-to.php?url=https://ae888g.com/
https://mforum.cari.com.my/home.php?mod=space&uid=3382833&do=profile
https://giaoan.violet.vn/user/show/id/15239663
https://anh135689999.violet.vn/user/show/id/15239663
https://party.biz/profile/ae888gcom?tab=541
https://profiles.delphiforums.com/n/pfx/profile.aspx?webtag=dfpprofile000&userId=1891279407
https://hu.gta5-mods.com/users/ae888gcom1
https://uk.gta5-mods.com/users/ae888gcom1
https://sl.gta5-mods.com/users/ae888gcom1
https://www.hamqth.com/ae888gcom
https://at.pinterest.com/ae888gcom1/
https://www.easyhits4u.com/profile.cgi?login=ae888gcom&view_as=1
https://in.pinterest.com/ae888gcom1/
https://doc.anagora.org/s/M-PleE1cO
https://album.link/ae888gcom
https://artist.link/ae888gcom
https://pods.link/ae888gcom
https://mylink.page/ae888gcom
https://playlist.link/ae888gcom
https://portfolium.com.au/ae888gcom
https://profile.sampo.ru/ae888gcom
https://mail.londonchinese.com/home.php?mod=space&uid=614848&do=profile
https://forum.pokexgames.pl/member.php?action=profile&uid=75528
https://www.bidhub.com/profiles/show/18803
https://baigiang.violet.vn/user/show/id/15239663
http://www.muzikspace.com/profiledetails.aspx?profileid=128206
https://es.gravatar.com/ae888gcom2
https://de.gravatar.com/ae888gcom2
https://cy.gravatar.com/ae888gcom2
https://cs.gravatar.com/ae888gcom2
https://cn.gravatar.com/ae888gcom2
https://www.ekdarun.com/forum/topic/134554/ae888
https://www.mobafire.com/profile/ae888gcom1-1235780?profilepage
https://fic.decidim.barcelona/profiles/ae888gcom/activity
https://fanclove.jp/profile/no2aQb052a
https://truckymods.io/user/461916
http://forum.vodobox.com/profile.php?section=personal&id=63575
https://fungiversum.de/pilz-forum/profile/ae888gcom/
https://www.dokkan-battle.fr/forums/users/ae888gcom/
https://mforum2.cari.com.my/home.php?mod=space&uid=3382833&do=profile
https://animeforums.net/profile/48113-ae888gcom/?tab=field_core_pfield_1
https://www.d-ushop.com/forum/topic/99527/ae888
https://www.templepurohit.com/forums/users/wangsarah359/
https://www.hugi.is/notendur/ae888gcom/
https://www.kickstarter.com/profile/964225056/about
https://www.noteflight.com/profile/b1dab92bdc2dd767cbe7fa02a381cc35edb8fa30
https://www.spoonflower.com/profiles/ae888gcom?sub_action=shop
https://www.horticulturaljobs.com/employers/4035748-ae888
https://jobs.siliconflorist.com/employers/4035749-ae888
https://jobs.nefeshinternational.org/employers/4035750-ae888
https://aboutcasemanagerjobs.com/author/ae888gcom/
https://biashara.co.ke/author/ae888gcom/
https://buyandsellhair.com/author/ae888gcom1/
https://cornucopia.se/author/ae888gcom/
https://colorswall.com/users/29800
https://www.pokecommunity.com/members/ae888gcom1.1482274/#about
https://www.servinord.com/phpBB2/profile.php?mode=viewprofile&u=769090
https://careers.coloradopublichealth.org/profiles/7940769-ae888
https://homepage.ninja/ae888gcom
https://promosimple.com/ps/45ea3/ae888gcom
https://dienbd.violet.vn/user/show/id/15239663
https://ketcau.com/member/121991-ae888gcom/visitormessage/310373-visitor-message-from-ae888gcom#post310373
https://kttm.club/members/ae888gcom.4333/#about
https://vietcurrency.vn/members/ae888gcom.234368/#about
https://zh-tw.gravatar.com/ae888gcom2
https://sv.gravatar.com/ae888gcom2
https://po.gravatar.com/ae888gcom2
https://oc.gravatar.com/ae888gcom2
https://ko.gravatar.com/ae888gcom2
https://vnbit.org/members/ae888gcom.83952/#about
https://www.cake.me/me/ae888gcom
https://boss.why3s.cc/boss/home.php?mod=space&uid=251125
https://clusterbusters.org/forums/profile/34762-ae888gcom/?tab=field_core_pfield_11
https://fengshuidirectory.com/dashboard/listings/ae888gcom/
https://library.zortrax.com/members/ae888-55/
https://mentorship.healthyseminars.com/members/ae888gcom/
https://pets4friends.com/profile-1533806
https://staroetv.su/go?https://ae888g.com/
https://www.ixawiki.com/link.php?url=https://ae888g.com/
https://www.shinobi.jp/etc/goto.html?https://ae888g.com/
https://oye.participer.lyon.fr/profiles/ae888gcom/activity
http://www.winomania.pl/forum/profile.php?mode=viewprofile&u=345418
https://participa.favb.cat/profiles/ae888gcom/activity
https://construim.fedaia.org/profiles/ae888gcom/activity
https://meta.decidim.org/profiles/ae888gcom/activity
https://hi.gta5-mods.com/users/ae888gcom1
https://it.gta5-mods.com/users/ae888gcom1
https://nl.gta5-mods.com/users/ae888gcom1
https://no.gta5-mods.com/users/ae888gcom1
https://pl.gta5-mods.com/users/ae888gcom1
https://pt.gta5-mods.com/users/ae888gcom1
https://decidim.derechoaljuego.digital/profiles/ae888gcom/activity
https://pads.zapf.in/s/_FP6YLmno0
https://openlibrary.org/people/ae888gcom
https://www.bookingblog.com/forum/users/ae888gcom/
https://legenden-von-andor.de/forum/memberlist.php?mode=viewprofile&u=53639
https://www.foriio.com/ae888gcom
https://pad.stuve.de/s/Q56GZ17AC
https://pad.libreon.fr/s/Uvytzk6ST
http://matdo.sangnhuong.com/member.php?u=110423
http://banhkeo.sangnhuong.com/member.php?u=96794
http://thietbidien.sangnhuong.com/member.php?u=105425
https://gl.gravatar.com/ae888gcom2
https://fr.gravatar.com/ae888gcom2
https://fi.gravatar.com/ae888gcom2
https://fa.gravatar.com/ae888gcom2
https://www.betmma.tips/mma_handicapper.php?ID=177113
https://quomon.es/Profile/ae888gcom/
https://www.are.na/nha-cai-ae888-hhfrl7xpqwo/ae888gcom
https://altacucina.co/profile/ae888gcom
https://ro.gta5-mods.com/users/ae888gcom1
https://ru.gta5-mods.com/users/ae888gcom1
https://fi.gta5-mods.com/users/ae888gcom1
https://sv.gta5-mods.com/users/ae888gcom1
https://vi.gta5-mods.com/users/ae888gcom1
https://zh.gta5-mods.com/users/ae888gcom1
https://www.mindmeister.com/users/channel/130013044
https://maiotaku.com/p/ae888gcom/info
https://theexplorers.com/user?id=5add7714-ec11-4687-9528-175e5acd3248
https://md.rappet.xyz/s/onlxzykYHw
https://www.blurb.com/user/ae888gcom1?profile_preview=true
https://wall.page/vP6UEn
https://participa.aytojaen.es/profiles/ae888gcom/activity
https://bsky.app/profile/ae888gcom.bsky.social
https://activeprospect.fogbugz.com/default.asp?pg=pgPublicView&sTicket=143657_fa7v4gba
https://ioninja.com/forum/user/ae888gcom
https://www.ad-links.org/ae888gcom_366674.html
https://km.gravatar.com/ae888gcom2
https://ja.gravatar.com/ae888gcom2
https://id.gravatar.com/ae888gcom2
https://he.gravatar.com/ae888gcom2
https://javabyab.com/user/ae888gcom
https://www.tripadvisor.com.vn/Profile/ae888gcom1
https://www.reddit-directory.com/ae888gcom_705455.html
https://www.beegdirectory.com/ae888gcom_485056.html
https://www.aquarius-dir.com/ae888gcom_510679.html
https://www.apeopledirectory.com/ae888gcom_410048.html
https://www.bedirectory.com/ae888gcom_442278.html
https://www.clickasnap.com/profile/ae888gcom
https://www.pubpub.org/user/nha-cai-ae888-83
https://soundcloud.com/ae888gcom
https://fliphtml5.com/homepage/ae888gcom/ae888/
https://jump.5ch.net/?https://ae888g.com/
https://www.tm-town.com///translators/ae888gcom
https://jp.pinterest.com/ae888gcom1/
https://de.gta5-mods.com/users/ae888gcom1
https://mk.gta5-mods.com/users/ae888gcom1
https://tr.gta5-mods.com/users/ae888gcom1
https://bs.gravatar.com/ae888gcom2
https://ca.gravatar.com/ae888gcom2
https://br.gravatar.com/ae888gcom2
https://bn.gravatar.com/ae888gcom2
https://bg.gravatar.com/ae888gcom2
https://az.gravatar.com/ae888gcom2
https://skr.gravatar.com/ae888gcom2
https://es.gravatar.com/ae888gcom2
https://ru.gravatar.com/ae888gcom2
https://ro.gravatar.com/ae888gcom2
https://pl.gravatar.com/ae888gcom2
https://ka.gravatar.com/ae888gcom2
https://ga.gravatar.com/ae888gcom2
https://fr-ca.gravatar.com/ae888gcom2
https://el.gravatar.com/ae888gcom2
https://da.gravatar.com/ae888gcom2
https://nl.gravatar.com/ae888gcom2
https://nb.gravatar.com/ae888gcom2
https://ms.gravatar.com/ae888gcom2
https://lt.gravatar.com/ae888gcom2
https://kn.gravatar.com/ae888gcom2
https://ur.gravatar.com/ae888gcom2
https://tr.gravatar.com/ae888gcom2
https://sr.gravatar.com/ae888gcom2
https://sq.gravatar.com/ae888gcom2
https://sl.gravatar.com/ae888gcom2
https://ae888gcom.mystrikingly.com/
https://ae888gcom.webflow.io/
https://rant.li/ae888gcom/ae888gcom
https://sites.google.com/view/ae888gcom1/home
https://telegra.ph/AE888-02-26-2
https://zenwriting.net/ae888gcom/ae888
https://ae888gcom1.blogspot.com/2026/02/ae888.html
https://ae888gcom.mypixieset.com/
https://hedgedoc.stusta.de/s/tjPSkaF3A
https://blogfreely.net/ae888gcom/ae888
https://scrapbox.io/ae888gcom/ae888gcom
https://ae888gcom13.wordpress.com/
https://www.notebook.ai/documents/2394251
https://ae888-122.gitbook.io/ae888-docs/
https://harsh-name-45b.notion.site/AE888-313ef850eef88059b775eff9cab630a1?pvs=73
https://zb3.org/ae888gcom/ae888gcom
https://www.keepandshare.com/discuss4/36600/ae888
https://telescope.ac/ae888gcom/fdj7annpby2o2wiaxkp97i
https://www.myaspenridge.com/board/board_topic/3180173/7903683.htm
https://www.tai-ji.net/board/board_topic/4160148/7903685.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/7903687.htm
https://www.thepetservicesweb.com/board/board_topic/2701171/7903688.htm
https://www.milliescentedrocks.com/board/board_topic/2189097/7903690.htm
https://www.coffeesix-store.com/board/board_topic/7560063/7903693.htm
https://www.vhs80.com/board/board_topic/6798823/7903695.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/7903697.htm
https://www.sunemall.com/board/board_topic/8431232/7903698.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/7903705.htm
https://www.crossroadsbaitandtackle.com/board/board_topic/9053260/7903707.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/7903719.htm
Cheers, I like this.
Stunning story there. What occurred after? Thanks!
I will right away grab your rss as I can not in finding your email
subscription hyperlink or newsletter service. Do you’ve any?
Please permit me know so that I could subscribe. Thanks.
Inspiring story there. What happened after? Take care!
Your comment is awaiting moderation.
https://www.facebook.com/zalowebdev
https://www.youtube.com/@zalowebdev
https://twitter.com/zalowebdev
https://tooter.in/zalowebdev
https://wakelet.com/@zalowebdev
https://safechat.com/u/zalowebdev
https://www.blogger.com/profile/08335732838555025398
https://www.mymeetbook.com/zalowebdev
https://www.pinterest.com/zalowebdev/
https://demo.wowonder.com/zalowebdev
https://shareyoursocial.com/zalowebdev
https://gitlab.aicrowd.com/zalowebdev
https://myspace.com/zalowebdev
https://500px.com/p/zalowebdev
https://www.instapaper.com/p/zalowebdev
https://magic.ly/zalowebdev
https://www.band.us/@zalowebdev
https://protocol.ooo/ja/users/zalowebdev
https://sketchfab.com/zalowebdev
https://www.tumblr.com/zalowebdev
https://www.reddit.com/user/zalowebdev/
https://audiomack.com/zalowebdev
https://hackaday.io/zalowebdev
https://fyers.in/community/member/qxf2iAGBZ9
https://vocal.media/authors/zalo-web-zx1rrx060n
https://leetcode.com/u/zalowebdev/
https://swag.live/en/user/699b522e03eb08bc1f7b0cf4
https://www.halaltrip.com/user/profile/320177/zalowebdev/
https://www.jetphotos.com/photographer/781678
https://medibang.com/author/27843291/
https://liulo.fm/zalowebdev
https://opensea.io/zalowebdev
https://www.blockdit.com/zalowebdev
https://portfolium.com/zalowebdev
https://groups.google.com/g/zalowebdev/c/kpZ1YIBPzJk
https://www.twitch.tv/zalowebdev/about
https://profile.hatena.ne.jp/zalowebdev/
https://issuu.com/zalowebdev
https://www.behance.net/zalowebdev
https://gravatar.com/zalowebdev
https://www.reverbnation.com/artist/zalowebdev
https://www.myminifactory.com/users/zalowebdev
https://www.investagrams.com/Profile/zalowebdev
https://gifyu.com/zalowebdev
https://www.chordie.com/forum/profile.php?id=2472146
https://www.longisland.com/profile/zalowebdev
https://www.walkscore.com/people/247616672033/zalo-web
https://topsitenet.com/profile/zalowebdev/1551162/
https://akniga.org/profile/1394174-zalo-web/
https://zalowebdev.bandcamp.com/album/zalowebdev
https://disqus.com/by/zalowebdev/about/
https://jobs.suncommunitynews.com/profiles/7927986-zalo-web
https://www.speedrun.com/users/zalowebdev
https://www.fanart-central.net/user/zalowebdev/profile
https://slides.com/zalowebdev
https://www.aicrowd.com/participants/zalowebdev
https://old.bitchute.com/channel/5D2NRM3nwIBr/
https://pbase.com/zalowebdev
https://hub.docker.com/u/zalowebdev
https://spiderum.com/nguoi-dung/zalowebdev
https://zaidap.com/thong-tin-ca-nhan-u106054.htm
https://www.gta5-mods.com/users/zalowebdev
https://heylink.me/zalowebdev/
https://pixabay.com/users/54756347/
https://www.nicovideo.jp/user/143353721
https://www.jigsawplanet.com/zalowebdev
https://3dwarehouse.sketchup.com/by/zalowebdev
https://robertsspaceindustries.com/en/citizens/zalowebdev
https://bit.ly/m/zalowebdev
https://joy.link/zalowebdev
https://connect.garmin.com/app/profile/db674111-9868-46f3-81c1-91da5d74cdea
https://b.hatena.ne.jp/zalowebdev/bookmark
https://www.chichi-pui.com/users/zalowebdev/
https://www.openrec.tv/user/zalowebdev/about
https://unityroom.com/users/zalowebdev
https://routinehub.co/user/zalowebdev
https://pxhere.com/en/photographer-me/4925764
https://teletype.in/@zalowebdev
https://www.checkli.com/zalowebdev
https://gitee.com/zalowebdev
https://www.fuelly.com/driver/zalowebdev
https://www.nintendo-master.com/profil/zalowebdev
https://freeimage.host/zalowebdev
https://www.diigo.com/profile/zalowebdev
https://fontstruct.com/fontstructions/show/2831105/zalowebdev
https://mecabricks.com/en/user/zalowebdev
https://motion-gallery.net/users/915602
https://linkin.bio/zalowebdev/
https://www.logic-sunrise.com/forums/user/189893-zalowebdev/
https://biomolecula.ru/authors/126421
https://talk.plesk.com/members/zalowebdev.489365/#about
https://www.callupcontact.com/b/businessprofile/Zalo_web/9981419
https://www.growkudos.com/profile/zalo_web_1
https://blender.community/zalowebdev/
https://doselect.com/@2f1eafecf5e9e22aa02421a58
https://sciter.com/forums/users/zalowebdev/
https://allmyfaves.com/zalowebdev
https://www.notebook.ai/users/1285787
https://www.abclinuxu.cz/lide/zalowebdev
https://dumagueteinfo.com/author/zalowebdev/
https://muare.vn/shop/zalo-web-76/895033
https://www.vnbadminton.com/members/zalowebdev.65274/
https://doodleordie.com/profile/zalowebdev
https://web.ggather.com/zalowebdev
https://musikersuche.musicstore.de/profil/zalowebdev/
https://www.intensedebate.com/profiles/zalowebdev
https://lookingforclan.com/user/zalowebdev
https://forum.dmec.vn/index.php?members/zalowebdev.175523/
https://igli.me/zalowebdev
https://www.fantasyplanet.cz/diskuzni-fora/users/zalowebdev/
https://duyendangaodai.net/members/30117-zalowebd.html
https://freestyler.ws/user/631619/zalowebdev
http://delphi.larsbo.org/user/zalowebdev
https://www.aseeralkotb.com/en/profiles/zalowebdev
https://timdaily.vn/members/zalowedev.128352/#about
https://app.readthedocs.org/profiles/zalowebdev/
https://iszene.com/user-336516.html
https://www.theyeshivaworld.com/coffeeroom/users/zalowebdev
https://desksnear.me/users/zalowebdev
https://www.itchyforum.com/en/member.php?379658-zalowebdev
https://www.roton.com/forums/users/wilsonabdullahi909/
https://able2know.org/user/zalowebdev/
http://www.biblesupport.com/user/810836-zalowebdev/
https://golosknig.com/profile/zalowebdev/
https://www.anibookmark.com/user/zalowebdev.html
https://www.inventoridigiochi.it/membri/zalowebdev/profile/
https://forum.m5stack.com/user/zalowebdev
https://wallhaven.cc/user/zalowebdev
https://imageevent.com/zalowebdev/zalowebdev
https://www.bitchute.com/channel/5D2NRM3nwIBr/
https://bandori.party/user/491447/zalowebdev/
https://community.m5stack.com/user/zalowebdev
https://schoolido.lu/user/zalowebdev/
https://awan.pro/forum/user/138956/
https://jakle.sakura.ne.jp/pukiwiki/?zalowebdev
https://fortunetelleroracle.com/profile/zalowebdev
https://fabble.cc/zalowebdev
https://pad.geolab.space/s/hoDMk8cWS
https://affariat.com/user/profile/173259
https://community.cisco.com/t5/user/viewprofilepage/user-id/1975851
https://pad.stuve.de/s/jRJ_uH8Xi
https://kr.pinterest.com/zalowebdev/
https://pt.gravatar.com/zalowebdev
https://th.gravatar.com/zalowebdev
https://www.sythe.org/members/zalowebdev.2013790/
https://f319.com/members/zalowebdev.1069753/
https://about.me/zalowebdev/
https://booklog.jp/users/zalowebdev/profile
https://www.canadavisa.com/canada-immigration-discussion-board/members/zalowebdev.1342427/#about
https://www.equinenow.com/farm/zalo-web-1309645.htm
https://www.gaiaonline.com/profiles/zalowebdev/50648589/
https://wefunder.com/zalowebdev
https://potofu.me/zalowebdev
https://transfur.com/Users/zalowebdev
https://xtremepape.rs/members/zalowebdev.645435/#about
https://github.com/zalowebdev
https://myanimelist.net/profile/zalowebdev
https://qna.habr.com/user/zalowebdev
https://website.informer.com/zaloweb.dev
https://lightroom.adobe.com/u/zalowebdev
https://beacons.ai/zalowebdev
https://en.islcollective.com/portfolio/12851963
https://www.xosothantai.com/members/zalowebdev.598699/
https://velog.io/@zalowebdev/about
https://violet.vn/user/show/id/15239256
https://iplogger.org/vn/logger/FsFQ5Meem3OZ/
http://www.stes.tyc.edu.tw/xoops/modules/profile/userinfo.php?uid=3903339
https://mez.ink/zalowebdev
https://zalowebdev.stck.me/profile
https://notionpress.com/author/1475911
https://www.edna.cz/uzivatele/zalowebdev/
https://digiphoto.techbang.com/users/zalowebdev
https://leakedmodels.com/forum/members/zalowebdev.691856/#about
https://freeicons.io/profile/897798
https://onlinesequencer.net/forum/user-252560.html
https://inkbunny.net/zalowebdev
https://www.japaaan.com/user/63119/
https://spinninrecords.com/profile/zalowebdev
https://www.launchgood.com/user/newprofile#!/user-profile/profile/zalo.web
https://code.antopie.org/zalowebdev
https://beatsaver.com/playlists/1144605
https://apptuts.bio/zalowebdev
https://dialog.eslov.se/profiles/zalowebdev/activity
https://www.storenvy.com/zalowebdev
https://zalowebdev.mssg.me/
https://participacion.cabildofuer.es/profiles/zalowebdev/activity
https://forums.maxperformanceinc.com/forums/member.php?u=239613
https://www.bloggportalen.se/BlogPortal/view/BlogDetails?id=290406
https://www.sciencebee.com.bd/qna/user/zalowebdev
https://acomics.ru/-zalowebdev
https://www.criminalelement.com/members/zalowebdev/profile/
https://hanson.net/users/zalowebdev
https://writexo.com/share/73cceff7bcb5
https://expatguidekorea.com/profile/zalowebdev/
https://www.laundrynation.com/community/profile/zalowebdev/
https://www.heavyironjobs.com/profiles/7931034-zalo-web
https://pad.degrowth.net/s/NQErWetjw
https://www.syncdocs.com/forums/profile/zalowebdev
https://www.rehashclothes.com/zalowebdev
http://fort-raevskiy.ru/community/profile/zalowebdev/
https://forum.skullgirlsmobile.com/members/zalowebdev.196553/#about
https://jobs.landscapeindustrycareers.org/profiles/7931103-zalo-web
https://phatwalletforums.com/user/zalowebdev
https://forums.galciv4.com/user/7639088
https://kyourc.com/zalowebdev
https://www.wanttoknow.nl/author/zalowebdev/
https://idol.st/user/135689/zalowebdev/
https://www.valinor.com.br/forum/usuario/zalowebdev.141455/#about
https://tulieu.violet.vn/user/show/id/15239256
https://www.bmwpower.lv/user.php?u=zalowebdev
https://gockhuat.net/member.php?u=431145
https://jobs.windomnews.com/profiles/7931200-zalo-web
https://hoaxbuster.com/redacteur/zalowebdev
https://www.givey.com/zalowebdev
https://talkmarkets.com/profile/wilsonabdullahi909-260223-150014
https://pc.poradna.net/users/1142147997-zalowebdev
https://forums.stardock.com/user/7639088
https://zerosuicidetraining.edc.org/user/profile.php?id=540629
https://www.telix.pl/forums/users/zalo-web1/
https://girlfriendvideos.com/members/z/zalowebdev/
https://swaay.com/u/wilson-abdullahi909/about/
https://beteiligung.amt-huettener-berge.de/profile/zalowebdev/
https://joinentre.com/profile/zalowebdev
https://eo-college.org/members/zalowebdev/
https://jobs.westerncity.com/profiles/7931298-zalo-web
https://www.thetriumphforum.com/members/zalowebdev.56590/
https://armchairjournal.com/forums/users/zalo/
https://gamblingtherapy.org/forum/users/zalowebdev/
https://beteiligung.tengen.de/profile/zalowebdev/
http://cds.zju.edu.cn/addons/cms/go/index.html?url=https://zaloweb.dev/
https://redirect.camfrog.com/redirect/?url=https://zaloweb.dev/
https://beteiligung.hafencity.com/profile/zalowebdev/
https://adhocracy.plus/profile/zalowebdev/
https://www.hobowars.com/game/linker.php?url=https://zaloweb.dev/
https://beteiligung.stadtlindau.de/profile/zalowebdev/
https://l2top.co/forum/members/zalowebdev.156941/
http://www.askmap.net/location/7737611/vi%E1%BB%87t-nam/zalo-web
https://youtopiaproject.com/author/zalowebdev/
https://graphcommons.com/graphs/620eba79-fda9-41f5-8899-23d4b67446be
https://forums.galciv3.com/user/7639088
https://galleria.emotionflow.com/175185/profile.html
https://www.myget.org/users/zalowebdev
https://www.deafvideo.tv/vlogger/zalowebdev
https://www.chaloke.com/forums/users/zalowebdev/
https://app.brancher.ai/user/1r46chFRVDcd
https://justpaste.me/uYRV4
https://aetherlink.app/users/7431728943033778176
https://forums.sinsofasolarempire2.com/user/7639088
https://confengine.com/user/zalowebdev
https://slideslive.com/zalowebdev?tab=about
https://mygamedb.com/profile/zalowebdev
https://buckeyescoop.com/community/members/zalowebdev.57530/#about
https://forums.ashesofthesingularity.com/user/7639088
http://www.ssnote.net/users/zalowebdev
https://forum.aceinna.com/user/zalowebdev
https://web-tourist.net/members/zalowebdev.48518/#about
https://rotorbuilds.com/profile/204216/
https://toirscript.com/user/zalowebdev
https://forum.pabbly.com/members/zalowebdev.97889/#about
http://forum.cncprovn.com/members/414800-zalowebdev
https://marketplace.trinidadweddings.com/author/zalowebdev/
https://ncnews.co/profile/zalowebdev
https://dreevoo.com/profile_info.php?pid=1169948
https://forum.aigato.vn/user/zalowebdev
https://amaz0ns.com/forums/users/zalowebdev/
https://rapidapi.com/user/zalowebdev
https://www.skool.com/@zalo-web-6416
https://hedge.fachschaft.informatik.uni-kl.de/s/-Ens6257h
https://learningapps.org/watch?v=pgbfd9r5k26
https://coub.com/zalowebdev
https://postheaven.net/zalowebdev/zalowebdev
https://www.giveawayoftheday.com/forums/profile/1661846
http://onlineboxing.net/jforum/user/editDone/430059.page
https://tealfeed.com/zalowebdev
https://www.catapulta.me/users/zalo-web
https://www.invelos.com/UserProfile.aspx?Alias=zalowebdev
https://www.video-bookmark.com/bookmark/7053358/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh/
https://wibki.com/zalowebdev
https://krachelart.com/UserProfile/tabid/43/userId/1334138/Default.aspx
https://gitlab.vuhdo.io/zalowebdev
https://www.11secondclub.com/users/profile/1699675
https://aniworld.to/user/profil/zalowebdev
https://worldvectorlogo.com/profile/zalowebdev
https://kktix.com/user/8443985
https://www.passes.com/zalowebdev
https://poipiku.com/13225718/
https://uiverse.io/profile/zalo_3104
https://www.rwaq.org/users/zalowebdev
https://cofacts.tw/user/zalowebdev
https://www.fitday.com/fitness/forums/members/zalowebdev.html
https://www.fundable.com/user-1288923
https://vcook.jp/users/74933
https://classificados.acheiusa.com/profile/dm9Jclc3TjFhWGJBSTZYM3JqWWh2VTBySmk0THFVUkFtd040K0dPZmhVTT0=
https://espritgames.com/members/50146493/
https://cgmood.com/zalowebdev
https://www.haikudeck.com/presentations/zalowebdev
https://www.efunda.com/members/people/show_people.cfm?Usr=zalowebdev
https://diit.cz/profil/eezmiwj4yr
https://backloggery.com/zalowebdev
https://www.sociomix.com/u/zalowebdev/
https://raovat.nhadat.vn/members/zalowebdev-288942.html
https://www.moshpyt.com/user/zalowebdev
https://www.koi-s.id/member.php?331599-zalowebdev
https://pumpyoursound.com/u/user/1584846
https://que.u.nosv.org/profile?user=zalowebdev
https://hi-fi-forum.net/profile/1120947
https://secondstreet.ru/profile/zalowebdev/
http://scenarch.com/userpages/28824
https://undrtone.com/zalowebdev
https://marshallyin.com/members/zalowebdev/
https://us.enrollbusiness.com/BusinessProfile/7730345/Zalo%20web
https://www.atozed.com/forums/user-67801.html
https://gravesales.com/author/zalowebdev/
https://searchengines.bg/members/zalowebdev.23413/#about
https://luvly.co/users/zalowebdev
https://suckhoetoday.com/members/36005-zalowebd.html
https://www.soshified.com/forums/user/662200-zalowebdev/
https://hukukevi.net/user/zalowebdev
https://belgaumonline.com/profile/zalowebdev/
https://savelist.co/profile/users/zalowebdev
https://usdinstitute.com/forums/users/zalowebdev/
https://hackerspace.govhack.org/profiles/zalo_web
https://www.apsense.com/user/zalowebdev
https://zzb.bz/zalowebdev
https://draft.blogger.com/profile/08335732838555025398
https://boldomatic.com/view/writer/zalowebdev
https://funsilo.date/wiki/User:Zalowebdev
https://www.themeqx.com/forums/users/zalowebdev/
https://www.udrpsearch.com/user/zalowebdev
https://forums.wincustomize.com/user/7639088
http://newdigital-world.com/members/zalowebdev.html
https://www.xen-factory.com/index.php?members/zalowebdev.140018/#about
https://cointr.ee/zalowebdev
https://forums.servethehome.com/index.php?members/zalowebdev.226193/#about
https://jaga.link/zalowebdev
https://raovatquynhon.com/dich-vu-27/zalo-web-zalo-pc-tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh-15728
https://www.blackhatprotools.info/member.php?276655-zalowebdev
https://activepages.com.au/profile/zalowebdev
https://snippet.host/ugpkms
https://tudomuaban.com/chi-tiet-rao-vat/2826033/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh.html
https://phijkchu.com/a/zalowebdev/video-channels
https://lifeinsys.com/user/zalowebdev
https://kaeuchi.jp/forums/users/zalowebdev/
https://www.claimajob.com/profiles/7932191-zalo-web
https://protospielsouth.com/user/117126
https://theafricavoice.com/profile/zalowebdev
http://palangshim.com/space-uid-4975417.html
https://www.africangenesis-101.org/profile/zalowebdev/profile
https://substance3d.adobe.com/community-assets/profile/org.adobe.user:71C42732699B59350A495FD0@AdobeID
https://vi.gravatar.com/zalowebdev
https://www.vevioz.com/zalowebdev
https://www.mixcloud.com/zalowebdev/
https://www.designspiration.com/zalowebdev/saves/
https://reactos.org/forum/memberlist.php?mode=viewprofile&u=185663
https://hub.vroid.com/en/users/124115949
https://www.exchangle.com/zalowebdev
https://forum.codeigniter.com/member.php?action=profile&uid=223776
https://etextpad.com/ydki7yg8rm
https://www.pixiv.net/en/users/124115949
https://m.wibki.com/zalowebdev
https://www.pageorama.com/?p=zalowebdev
https://bandsworksconcerts.info/index.php?zalowebdev
https://bbs.mikocon.com/home.php?mod=space&uid=281642
https://www.mikocon.com/home.php?mod=space&uid=281642
https://jerseyboysblog.com/forum/member.php?action=profile&uid=81977
https://manylink.co/@zalowebdev
https://londonchinese.com/home.php?mod=space&uid=614680&do=profile
https://smallseo.tools/website-checker/zaloweb.dev/
https://rush1989.rash.jp/pukiwiki/index.php?zalowebdev
https://www.stylevore.com/user/zalowebdev
https://wikimapia.org/external_link?url=https://zaloweb.dev/
https://forum.issabel.org/u/zalowebdev
https://ie.enrollbusiness.com/BusinessProfile/7730345/Zalo%20web
https://edabit.com/user/dveAdjq4fk2rt5qM5
https://mathlog.info/users/9v8jTbbSM5S5R37wrO8OuyiAdtH3
https://securityheaders.com/?q=https%3A%2F%2Fzaloweb.dev%2F
http://densan-knct.freehostia.com/wiki_/index.php?zalowebdev
https://md.darmstadt.ccc.de/s/xnOdUZEx5b
https://sfx.thelazy.net/users/u/zalowebdev/
http://vetstate.ru/forum/?PAGE_NAME=profile_view&UID=246527
https://www.pdc.edu/?URL=https://zaloweb.dev/
https://ask.mallaky.com/?qa=user/zalowebdev
https://drill.lovesick.jp/drilldata/index.php?zalowebdev
https://www.depechemode.cz/?URL=https://zaloweb.dev/
https://sub4sub.net/forums/users/zalowebdev/
https://fora.babinet.cz/profile.php?id=114486
https://forum.epicbrowser.com/profile.php?id=138421
http://www.dungdong.com/home.php?mod=space&uid=3321267
https://bbs.mofang.com.tw/home.php?mod=space&uid=2386813
https://hedgedoc.eclair.ec-lyon.fr/s/FOcyMeL_5
https://www.divephotoguide.com/user/zalowebdev
https://b.cari.com.my/home.php?mod=space&uid=3382464&do=profile
https://hedgedoc.logilab.fr/s/b7KMfRI4H
https://ixawiki.com/link.php?url=https://zaloweb.dev/
http://www.activewin.com/user.asp?Action=Read&UserIndex=4826162
https://www.vid419.com/home.php?mod=space&uid=3474740
https://www.okaywan.com/home.php?mod=space&uid=770367
http://classicalmusicmp3freedownload.com/ja/index.php?title=%E5%88%A9%E7%94%A8%E8%80%85:Zalowebdev
http://techou.jp/index.php?zalowebdev
https://paste.intergen.online/view/e4709d18
http://tkdlab.com/wiki/index.php?zalowebdev
http://pcsq28.com/home.php?mod=space&uid=1755416
https://bbs.airav.cc/home.php?mod=space&uid=4409221
https://md.coredump.ch/s/43g3_96xD
https://hker2uk.com/home.php?mod=space&uid=5338865
https://pad.funkwhale.audio/s/2qJjwJuVk
https://xibeiwujin.com/home.php?mod=space&uid=2303367&do=profile&from=space
https://tilengine.org/forum/member.php?action=profile&uid=158058
https://darkml.net/bbs/home.php?mod=space&uid=8192724&do=profile&from=space
https://www.play56.net/home.php?mod=space&uid=6002597
https://hedgedoc.stusta.de/s/Wkrz-rDRx
https://pad.flipdot.org/s/WFVApahb2
https://hack.allmende.io/s/zf2jyFqdL
https://pad.codefor.fr/s/GrF53_lC7n
https://md.fachschaften.org/s/2Wuyf_m3k
https://md.opensourceecology.de/s/ixP0Xg_sh
https://md.ctdo.de/s/DXFn-VQX0w
https://md.chaospott.de/s/FOwbQYVWUs
https://pad.fablab-siegen.de/s/dE5L0OC9G
https://hackmd.hub.yt/s/Tdg5Jn0Fn
https://md.swk-web.com/s/PRKEOIhuS
https://www.dnnsoftware.com/activity-feed/my-profile/userid/3300992
https://pad.darmstadt.social/s/1xiEUp0gLD
https://divisionmidway.org/jobs/author/zalowebdev/
https://bbcovenant.guildlaunch.com/users/blog/6737367/?mode=view&gid=97523
http://jobboard.piasd.org/author/zalowebdev/
https://www.wvhired.com/profiles/7932511-zalo-web
http://jobs.emiogp.com/author/zalowebdev/
https://onlinevetjobs.com/author/zalowebdev/
https://v.gd/HIRPfg
https://sciencewiki.science/wiki/User:Zalowebdev
https://gl.gta5-mods.com/users/zalowebdev
https://www.fruitpickingjobs.com.au/forums/users/zalowebdev/
http://www.webclap.com/php/jump.php?url=https://zaloweb.dev/
https://telegra.ph/Zalo-web-02-23
https://rant.li/zalowebdev/zalowebdev
https://telegra.ph/ZALO-WEB—Zalo-PC—T%E1%BA%A3i-Zalo-PC-%C4%91%E1%BB%83-l%C3%A0m-vi%E1%BB%87c-nh%C3%B3m-hi%E1%BB%87u-qu%E1%BA%A3-v%C3%A0-g%E1%BB%ADi-file-nhanh-02-23
https://hedgedoc.stusta.de/s/j2t3b8Exs
https://blogfreely.net/zalowebdev/zalowebdev
https://zb3.org/zalowebdev/zalowebdev
https://telescope.ac/zalowebdev/lr49ygafrlkbeoc6gy23fc
https://www.myaspenridge.com/board/board_topic/3180173/7893378.htm
https://www.tai-ji.net/board/board_topic/4160148/7893379.htm
https://www.greencarpetcleaningprescott.com/board/board_topic/7203902/7893384.htm
https://www.thepetservicesweb.com/board/board_topic/2701171/7893403.htm
https://www.milliescentedrocks.com/board/board_topic/2189097/7893408.htm
https://www.coffeesix-store.com/board/board_topic/7560063/7893410.htm
https://www.vhs80.com/board/board_topic/6798823/7893409.htm
https://www.thepartyservicesweb.com/board/board_topic/3929364/7893420.htm
https://www.sunemall.com/board/board_topic/8431232/7893419.htm
https://www.freedomteamapexmarketinggroup.com/board/board_topic/8118484/7893421.htm
https://www.crossroadsbaitandtackle.com/board/board_topic/9053260/7893423.htm
https://www.longislandjobsmagazine.com/board/board_topic/9092000/7893424.htm
https://www.bestloveweddingstudio.com/forum/topic/61245/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.ekdarun.com/forum/topic/134008/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.driedsquidathome.com/forum/topic/112793/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.cemkrete.com/forum/topic/133138/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.navacool.com/forum/topic/316081/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.natthadon-sanengineering.com/forum/topic/77639/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.bonback.com/forum/topic/316082/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
https://www.d-ushop.com/forum/topic/98620/zalo-web—zalo-pc—tai-zalo-pc-de-lam-viec-nhom-hieu-qua-va-gui-file-nhanh
Wow that was strange. I just wrote an really long comment but after I clicked submit my comment
didn’t appear. Grrrr… well I’m not writing all that over again. Regardless, just wanted to say fantastic blog!
بالنسبة للمتداولين، يحظى السوق العالمي بتقلبات تمثل فرصًا لتحقيق الأرباح.
إن القدرة على التحليل الدقيق والتوقيت المناسب للدخول
والخروج من الصفقات تعدان من المهارات الأساسية للنجاح
في هذا المجال. ينبغي على المستثمرين التواصل مع البيانات السوقية وتحليل المخاطر بعناية، للاستفادة من أي تحركات في الأسعار.
Heya i’m for the primary time here. I found this board and I find It truly helpful & it helped me out a lot. I’m hoping to present one thing again and aid others like you helped me.
Hi there! This blog post couldn’t be written much better! Reading through this article reminds me of my previous roommate! He constantly kept talking about this. I am going to forward this information to him. Pretty sure he will have a good read. Thank you for sharing!
I do not know whether it’s just me or if everyone else experiencing problems with your website. It looks like some of the written text within your content are running off the screen. Can someone else please comment and let me know if this is happening to them too? This could be a problem with my browser because I’ve had this happen previously. Cheers
When I initially commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove people from that service? Thanks!
Hi there to every body, it’s my first pay a quick visit of this website; this website contains remarkable and actually fine data for visitors.
This information is priceless. Where can I find out more?
I like the helpful information you provide in your articles. I’ll bookmark your blog and check again here frequently. I am quite sure I’ll learn lots of new stuff right here! Good luck for the next!
I want to to thank you for this great read!! I absolutely enjoyed every bit of it. I have you book marked to look at new stuff you post…
What you posted made a great deal of sense. But, what about this? what if you added a little content? I am not saying your information is not solid, but what if you added something that grabbed a person’s attention? I mean Balancing the Scales: Patient Load vs. Care Quality in Diabetes is a little boring. You ought to look at Yahoo’s home page and see how they write news headlines to get viewers interested. You might try adding a video or a related picture or two to get people interested about everything’ve got to say. Just my opinion, it could make your posts a little livelier.
Hello! I know this is kinda off topic but I was wondering if you knew where I could find a captcha plugin for my comment form? I’m using the same blog platform as yours and I’m having problems finding one? Thanks a lot!
I like it whenever people come together and share opinions. Great website, continue the good work!
Someone necessarily lend a hand to make severely articles I’d state. This is the first time I frequented your web page and so far? I amazed with the analysis you made to create this particular put up extraordinary. Magnificent job!
I’m no longer sure the place you’re getting your info, however good topic. I needs to spend some time finding out more or understanding more. Thanks for fantastic info I was on the lookout for this information for my mission.
Hello, I do believe your blog could possibly be having internet browser
compatibility issues. Whenever I look at your website in Safari, it looks fine however when opening in IE, it has some overlapping issues.
I just wanted to give you a quick heads up! Besides that, great
site!
من جانب آخر، يعتبر الاستثمار
في المعادن الثمينة مثل الذهب والفضة خيارًا شائعًا
للكثير من المستثمرين، خصوصًا في الإمارات، حيث تظل أسعار الفضة في الإمارات من الأمور التي
تثير اهتمام الكثيرين، خاصةً أولئك الذين يرغبون في شراء الفضة أو
الذهب لأغراض الاستثمار أو الزينة.
تدل البيانات التاريخية
على أن أسعار الذهب قد تتأثر بعدة عوامل مثل تقلبات الدولار الأمريكي،
والعرض والطلب المحلي والدولي، والسياسات النقدية.
Hello, Neat post. There’s an issue with your site in internet explorer, might test this?
IE still is the market leader and a large portion of
other folks will pass over your magnificent writing due to
this problem.
Great article! That is the kind of info that are meant to be shared around the net.
Shame on the search engines for not positioning this post upper!
Come on over and seek advice from my web site . Thank you
=)
I know this if off topic but I’m looking into starting my
own weblog and was wondering what all is needed to get setup?
I’m assuming having a blog like yours would cost a pretty penny?
I’m not very web savvy so I’m not 100% sure. Any recommendations or advice would be greatly appreciated.
Thanks
يستفيد المتداولون من الأخبار الاقتصادية، حيث تشير المعلومات الجديدة دائماً إلى
تغييرات في الاتجاهات الحالية للأسعار.
بالنسبة للمستثمرين في الإمارات، يعد متابعة
سعر الذهب المستعمل عيار 21 والفضة
موصي به، حيث يعكس الاحتياجات المحلية والعالمية لهذه المعادن.
تختلف العوامل التي تتحكم في الأسعار، بدءًا
من الطلب المحلي في الإمارات وصولاً إلى التأثيرات العالمية مثل
الطلب من الصين والهند.
One of the most famous trading platforms in the online
trading landscape is MetaTrader 5, typically referred to as MT5.
The change from the initial MetaTrader 4 to its follower,
MT5, was marked by considerable enhancements in performance, enabling
for much more intricate order kinds, much deeper
market evaluation, and incorporated tools for algorithmic trading.
Why viewers still make use of to read news papers when in this technological globe the whole thing is accessible on net?
من جانب آخر، يعتبر الاستثمار في المعادن الثمينة مثل الذهب
والفضة خيارًا شائعًا للكثير
من المستثمرين، خصوصًا في الإمارات، حيث تظل أسعار الفضة في الإمارات من الأمور التي تثير اهتمام الكثيرين، خاصةً أولئك الذين
يرغبون في شراء الفضة أو الذهب لأغراض الاستثمار أو الزينة.
تدل البيانات التاريخية على أن أسعار الذهب
قد تتأثر بعدة عوامل مثل تقلبات الدولار الأمريكي، والعرض والطلب المحلي والدولي، والسياسات النقدية.
Thanks for one’s marvelous posting! I truly enjoyed reading it, you can be a great
author.I will always bookmark your blog and will often come back
in the foreseeable future. I want to encourage that you continue your great writing,
have a nice weekend!
When someone writes an piece of writing he/she keeps the thought of a user in his/her mind that how a user can understand it. Therefore that’s why this article is great. Thanks!
Great blog here! Also your web site loads up fast! What web host are you using? Can I get your affiliate link to your host? I wish my web site loaded up as quickly as yours lol
Howdy! This blog post couldn’t be written much better!
Looking through this article reminds me of my previous roommate!
He constantly kept talking about this. I most certainly will send this information to him.
Pretty sure he’ll have a good read. Many thanks for sharing!
Hmm is anyone else experiencing problems with the images on this blog
loading? I’m trying to determine if its a problem on my end or if it’s
the blog. Any feed-back would be greatly appreciated.
Saved as a favorite, I really like your site!
Thanks for every other informative blog. The place else may just I get that type of info written in such a perfect means? I’ve a project that I am simply now working on, and I have been on the look out for such information.
Howdy just wanted to give you a brief heads
up and let you know a few of the pictures aren’t loading correctly.
I’m not sure why but I think its a linking issue.
I’ve tried it in two different internet browsers and both show the same outcome.
Hi, Neat post. There’s a problem with your website in internet explorer,
could check this? IE nonetheless is the market leader and a big component of
folks will omit your magnificent writing due to this problem.
Greate pieces. Keep writing such kind of info on your site.
Im really impressed by your site.
Hey there, You’ve performed a great job. I’ll definitely digg it and
personally recommend to my friends. I am confident they’ll be benefited from this web site.
I’ll right away clutch your rss as I can not find your e-mail subscription hyperlink or newsletter service.
Do you have any? Kindly permit me realize in order that I may just subscribe.
Thanks.
With havin so much content and articles do you ever
run into any issues of plagorism or copyright infringement?
My blog has a lot of unique content I’ve either authored myself or outsourced but it looks like a lot of it
is popping it up all over the web without my agreement.
Do you know any solutions to help stop content from being stolen? I’d truly appreciate
it.
Hello! I’ve been reading your site for a while now and finally
got the bravery to go ahead and give you a shout out from New Caney Texas!
Just wanted to mention keep up the good work!
Wonderful, what a blog it is! This weblog provides useful facts to us, keep it up.
With havin so much written content do you ever run into any problems of plagorism or copyright violation? My website has a lot of exclusive content I’ve either authored myself or outsourced but it seems a lot of it is popping it up all over the internet without my authorization. Do you know any solutions to help protect against content from being ripped off? I’d really appreciate it.
You really make it seem so easy with your presentation but I find this matter to be actually something which I think
I would never understand. It seems too complex and extremely broad
for me. I’m looking forward for your next post,
I’ll try to get the hang of it!
Great beat ! I would like to apprentice while you amend your web site, how could i subscribe for a weblog web
site? The account aided me a acceptable deal. I were tiny bit acquainted
of this your broadcast provided brilliant clear idea
https://jm-plan-cul-gratuit.fr/
Wow, that’s what I was seeking for, what a information! present here
at this website, thanks admin of this web site.
If some one needs to be updated with most recent technologies then he must be visit this site and be up to date all the time.
I all the time emailed this webpage post page to all my contacts,
because if like to read it after that my contacts will too.
Hey There. I discovered your weblog using msn. That
is an extremely neatly written article. I will make sure to bookmark it
and return to read more of your helpful info.
Thank you for the post. I will definitely return.
Good day! I could have sworn I’ve been to this site before but after browsing through some of the post I realized it’s new to me. Anyways, I’m definitely glad I found it and I’ll be book-marking and checking back frequently!
It’s not my first time to visit this web page, i am visiting this site dailly and take pleasant data from here daily.
Greetings from Ohio! I’m bored at work so I decided to browse your blog on my iphone during lunch break.
I love the knowledge you provide here and can’t wait to take a
look when I get home. I’m surprised at how quick your blog loaded
on my cell phone .. I’m not even using WIFI, just 3G ..
Anyhow, very good site!
Great site. A lot of helpful information here. I’m sending it to some pals ans additionally sharing in delicious. And of course, thanks to your sweat!
Hi to all, the contents existing at this website are genuinely amazing for people experience, well, keep up the good work fellows.
I think that is one of the most important info for me.
And i am glad reading your article. But wanna commentary on few common issues, The site style is perfect, the articles is actually nice : D.
Good process, cheers
Awesome site you have here but I was curious if you
knew of any user discussion forums that cover the same topics discussed here?
I’d really love to be a part of community where I can get
feedback from other knowledgeable individuals that share the same interest.
If you have any recommendations, please let me know.
Many thanks!
Hi there everyone, it’s my first pay a visit at this web
page, and article is really fruitful designed for me, keep up
posting these content.
Wow! Terima kasih! Saya terus-menerus ingin menulis di blog saya sesuatu seperti itu. Bolehkah saya menyertakan bagian dari posting Anda ke situs saya?
Excellent way of telling, and fastidious post to get data about my presentation subject matter,
which i am going to deliver in university.
Saya tidak umumnya berkomentar tetapi saya harus mengakui hargai untuk posting yang luar biasa ini : D.
Spot on with this write-up, I seriously think this amazing site needs much more attention. I’ll probably be back again to read more, thanks for the info!
That is a really good tip particularly to those fresh to the blogosphere.
Brief but very accurate info… Many thanks for sharing this one.
A must read article!
Superb, what a webpage it is! This blog gives valuable data to us, keep it up.
I’ve read a few just right stuff here. Definitely price bookmarking for revisiting. I wonder how so much attempt you place to create this type of wonderful informative website.
Hi to all, how is everything, I think every one is getting
more from this website, and your views are nice designed for new users.
I was curious if you ever considered changing the structure of your blog?
Its very well written; I love what youve got to say. But maybe
you could a little more in the way of content so people
could connect with it better. Youve got an awful lot of text for
only having one or two pictures. Maybe you could space it out better?
Greate post. Keep writing such kind of information on your site.
Im really impressed by it.
Hi there, You have performed an incredible job. I’ll certainly digg it and
individually recommend to my friends. I’m sure they will be benefited from this website.
I just like the helpful information you provide for your articles.
I’ll bookmark your weblog and test once more right here regularly.
I am slightly certain I’ll be informed a lot of new stuff proper right here!
Good luck for the following!
Hi! This is kind of off topic but I need some help from an established blog.
Is it very hard to set up your own blog? I’m not very techincal but I can figure things out pretty fast.
I’m thinking about setting up my own but I’m not sure where to begin. Do you have any points
or suggestions? With thanks
Magnificent beat ! I wish to apprentice while you amend
your website, how can i subscribe for a blog web site?
The account helped me a acceptable deal. I had been a little
bit acquainted of this your broadcast offered bright clear concept
Hi! Do you know if they make any plugins to assist with SEO?
I’m trying to get my blog to rank for some targeted keywords but I’m not seeing very good success.
If you know of any please share. Appreciate it!
This is really interesting, You are a very skilled blogger.
I have joined your rss feed and look forward to seeking more of your fantastic
post. Also, I have shared your site in my social networks!
I don’t know if it’s just me or if everyone else encountering issues with your site.
It appears as though some of the written text on your posts are running
off the screen. Can someone else please provide feedback
and let me know if this is happening to them too?
This might be a problem with my web browser because I’ve
had this happen previously. Many thanks
It is the best time to make some plans for the future and it’s time to be happy.
I’ve learn this post and if I may I desire to counsel you few attention-grabbing issues
or suggestions. Maybe you could write subsequent articles regarding this article.
I wish to learn even more things approximately it!
One of the most famous trading systems in the online trading landscape is MetaTrader 5, frequently referred
to as MT5. The transition from the initial MetaTrader 4 to its follower, MT5, was noted by substantial improvements in functionality, enabling for more complex
order kinds, deeper market analysis, and
integrated tools for mathematical trading.
This article is in fact a nice one it assists new web people,
who are wishing in favor of blogging.
Very good information. Lucky me I found your site by chance (stumbleupon).
I’ve book-marked it for later!
Thank you for some other informative web site. The
place else may I am getting that type of info
written in such an ideal means? I’ve a venture that I’m just now operating on, and I’ve been on the glance out for such info.
Artikel yang bagus. Ini benar-benar disusun dengan baik dan mudah dipahami. Terima kasih telah berbagi pengetahuan ini.
I think this is among the most significant information for me.
And i’m glad reading your article. But wanna remark on some
general things, The site style is great, the articles is really
excellent : D. Good job, cheers
Oh my goodness! Amazing article dude! Thank you so
much, However I am going through troubles with your RSS.
I don’t understand why I cannot join it. Is there anyone else having the same RSS problems?
Anybody who knows the solution can you kindly respond?
Thanks!!
This piece of writing will assist the internet users for building up new website or even a
weblog from start to end.
hello there and thank you for your information – I have definitely picked up
anything new from right here. I did however expertise several technical points using this site, since I experienced to
reload the web site lots of times previous to I could get it
to load properly. I had been wondering if your web hosting is OK?
Not that I’m complaining, but sluggish loading instances times will
very frequently affect your placement in google and can damage your
high quality score if ads and marketing with Adwords.
Anyway I’m adding this RSS to my e-mail and can look out for a lot more
of your respective interesting content. Make sure you update this again very soon.
مع التوسع في الأسواق المالية والزيادة المستمرة في قائمة الأدوات المتاحة للتداول، نجد أن هناك اهتماماً
مستمراً من جانب المستثمرين في الإمارات.
هؤلاء المستثمرون يسعون
دائماً للحصول على تحديثات
فورية حول أسعار الفضة والذهب، وأي تغييرات قد
تطرأ على الأسواق بهدف اتخاذ قرارات فعالة.
إن فهم ديناميكيات السوق ومتابعة الأخبار الاقتصادية يُعتبران من أسياسيات النجاح في تداول الفوركس والمقايضات في الأسواق المالية العالمية.
Hi there I am so glad I found your webpage, I really found you by accident, while I
was looking on Yahoo for something else, Anyhow I am here now and would just like to say thanks a lot for
a fantastic post and a all round thrilling blog (I also love the theme/design), I don’t have
time to read it all at the moment but I have saved it and also added your RSS feeds, so when I have time I will be back to
read more, Please do keep up the great work.
Good post. I learn something totally new and challenging on websites I stumbleupon every day.
It’s always exciting to read articles from other writers and practice a little something from their sites.
Saya harus mengatakan, ini adalah salah satu posting terbaik yang yang pernah saya baca belakangan ini. Konten yang sangat membantu. Terima kasih telah berbagi.
Superb post however , I was wondering if you could write
a litte more on this topic? I’d be very thankful if you could elaborate a little bit further.
Thanks!
I was recommended this blog by my cousin. I’m not sure whether this post is written by him as nobody else know such detailed about
my difficulty. You are amazing! Thanks!
Attractive portion of content. I simply stumbled upon your weblog and in accession capital to assert that I get
actually loved account your blog posts. Any way I’ll be subscribing to your augment or even I success you get
right of entry to consistently fast.
Marvelous, what a web site it is! This website provides useful facts
to us, keep it up.
hi!,I love your writing very so much! percentage we
communicate extra approximately your post on AOL? I require an expert in this area to resolve my problem.
Maybe that is you! Looking forward to look you.
Hai semua, kamu sudah melakukan pekerjaan yang luar biasa. Saya tentu akan menyimpan ini dan kembali untuk membaca lebih banyak. Terima kasih banyak!
Saya senang menjadi salah satu pengunjung di website luar biasa ini (:, terima kasih telah mengunggah.
Postingan yang hebat! Saya menghargai cara Anda menguraikan semuanya dengan sangat jelas. Teruskan pekerjaan yang bagus!
Saya tidak umumnya berkomentar tetapi saya harus mengakui terimakasih untuk posting yang sempurna ini : D.
WONDERFUL Post.thanks for share..more wait .. …
Heya i am for the primary time here. I found this board and I in finding It truly helpful & it helped me out a lot. I’m hoping to offer one thing again and help others like you aided me.
Berharga info. Beruntung saya menemukan website Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menyimpannya.
Isi yang bermanfaat dan disajikan dengan sangat baik. Saya tentu akan membagikan ini kepada rekan-rekan. Terima kasih telah berbagi.
Merely wanna remark on few general things, The website design is perfect, the subject material is really fantastic. “Earn but don’t burn.” by B. J. Gupta.
But wanna input on few general things, The website style and design is perfect, the articles is rattling great. “The idea of God is the sole wrong for which I cannot forgive mankind.” by Marquis de Sade.
Some really nice stuff on this site, I love it.
Really great info can be found on blog. “I believe in nothing, everything is sacred. I believe in everything, nothing is sacred.” by Tom Robbins.
Luar biasa blog yang Anda miliki, tapi saya penasaran apakah Anda tahu forum yang membahas topik yang sama seperti yang dibahas di sini? Saya sangat ingin menjadi bagian dari komunitas online di mana saya bisa mendapatkan komentar dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Sangat menghargai!
Sangat menarik detail yang Anda utarakan, terima kasih telah mengunggah. “Jive Lady Just hang loose blood. She gonna handa your rebound on the med side.” oleh Airplane.
Excellent post. I was checking constantly this blog and I am impressed! Extremely useful information particularly the last part 🙂 I care for such information a lot. I was seeking this certain information for a very long time. Thank you and good luck.
Thanks for the marvelous posting! I quite enjoyed reading it, you may be a great author.I will be sure to bookmark your blog and will often come back someday. I want to encourage one to continue your great writing, have a nice afternoon!
Saya puas bahwa saya menemukan kembali blog ini, persis info yang saya cari!
Saya umumnya tidak meninggalkan komentar, tetapi yang ini benar-benar pantas. Konten yang hebat dan berguna. Terima kasih telah meluangkan waktu untuk menulis ini.
Well I really liked studying it. This post provided by you is very helpful for accurate planning.
Normally I don’t learn post on blogs, but I would like to say that this write-up very compelled me to check out and do so! Your writing taste has been surprised me. Thank you, quite great article.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Seseorang secara esensial membantu untuk membuat sangat artikel saya akan katakan. Itu adalah pertama kali saya mengunjungi halaman web Anda dan sejauh ini? Saya terkagum dengan riset yang Anda lakukan untuk membuat unggahan menakjubkan ini. Kerja yang fantastis!
Wow, fantastis weblog struktur! Sudah berapa lama Anda menjalankan blog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan situs Anda fantastis, serta kontennya!
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Hei semua, saya menjumpai website Anda melalui Google ketika menelusuri topik yang serupa, website Anda tampil di posisi atas. Saya harus mengakui bahwa saya kagum betapa baik penulisannya. Saya benar-benar menikmati menelusuri ini dan saya akan kembali untuk membaca lebih banyak. Terima kasih banyak!
Anda bisa pasti melihat antusiasme Anda dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut mengatakan apa yang mereka yakini. Selalu kejar hati Anda.
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mencuri gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya bagus!
Aku benar-benar ingin mengirim komentar singkat guna mengucapkan terima kasih Anda atas semua tips luar biasa yang Anda tuliskan di website ini.
Kami dapat memiliki tautan perdagangan perjanjian antara kita!
Wow! Thank you! I always needed to write on my website something like that. Can I take a portion of your post to my blog?
so much superb information on here, :D.
great post.Never knew this, thankyou for letting me know.
Somebody necessarily lend a hand to make severely posts I would state. That is the very first time I frequented your web page and thus far? I amazed with the research you made to make this particular publish incredible. Excellent job!
Hebat blog yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu forum yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan komentar dari individu yang berpengetahuan dengan minat yang sama. Jika Anda punya rekomendasi, mohon beri tahu saya. Terima kasih!
Wow! Terima kasih! Saya secara terus ingin menulis di situs saya sesuatu seperti itu. Bolehkah saya menyertakan sebagian dari posting Anda ke situs saya?
Hmm it seems like your website ate my first comment (it was extremely long) so I guess I’ll just sum it up what I had written and say, I’m thoroughly enjoying your blog. I too am an aspiring blog writer but I’m still new to everything. Do you have any helpful hints for first-time blog writers? I’d really appreciate it.
Hello. impressive job. I did not anticipate this. This is a excellent story. Thanks!
Postingan ini sangat berguna. Saya sangat menghargai waktu yang Anda curahkan untuk menulisnya. Terima kasih!
The other day, while I was at work, my cousin stole my iPad and tested to see if it can survive a thirty foot drop, just so she can be a youtube sensation. My apple ipad is now destroyed and she has 83 views. I know this is totally off topic but I had to share it with someone!
Spot on with this write-up, I actually think this website wants far more consideration. I’ll most likely be once more to learn way more, thanks for that info.
Sangat menarik info !Sempurna persis seperti yang saya telusuri! “Media adalah pesan.” oleh Marshall McLuhan.
Terima kasih untuk artikel sangat baik yang lain. Di mana lagi siapa pun dapat mendapatkan jenis info seperti itu dengan gaya penulisan yang ideal? Saya punya presentasi minggu depan, dan saya sedang mencari informasi seperti ini.
I like what you guys are up also. Such smart work and reporting! Keep up the excellent works guys I’ve incorporated you guys to my blogroll. I think it will improve the value of my website 🙂
Saya terkesan dengan situs ini, benar-benar saya adalah penggemar.
Bernilai info. Beruntung saya menemukan situs Anda secara tidak sengaja, dan aku kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
Saya gembira bahwa saya mendeteksi web blog ini, tepat info yang saya telusuri!
Saya menghargainya, karena saya menemukan tepat apa yang saya cari. Anda telah mengakhiri pencarian saya selama 4 hari! Tuhan memberkati Anda. Semoga hari menyenangkan. Bye
Namun, terima kasih untuk poin yang fantastis ini dan walaupun saya tidak benar-benar setuju sepenuhnya, saya menghargai pandangan.
Wow! Ini mungkin salah satu blog paling berguna yang pernah kami temui tentang topik ini. Sebenarnya Mengagumkan. Saya juga seorang spesialis dalam topik ini oleh karena itu saya dapat memahami usaha Anda.
Ini adalah situs yang benar untuk siapa saja yang ingin mencari tahu tentang topik ini. Anda menyadari begitu banyak hal sehingga nyaris sulit untuk membantah dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa sudut pandang baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar luar biasa!
I really like your writing style, superb information, thank you for putting up :D. “Silence is more musical than any song.” by Christina G. Rossetti.
Beberapa hari lalu, saat saya sedang bekerja, saudara perempuan saya mengambil apple ipad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi tiga puluh kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sangat di luar topik tetapi saya harus membagikannya kepada seseorang!
Terima kasih untuk situs web informatif tambahan. Di mana lagi saya memperoleh informasi seperti itu yang ditulis dengan gaya yang sempurna? Saya punya sebuah tantangan yang saya sedang kerjakan sekarang, dan saya sudah mengamati informasi seperti ini.
Sangat baik blog yang Anda miliki, tapi saya ingin tahu apakah Anda tahu forum diskusi yang membahas topik yang sama seperti yang dibicarakan di sini? Saya sangat ingin sekali menjadi bagian dari komunitas di mana saya bisa mendapatkan saran dari individu yang berpengalaman dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Banyak terima kasih!
Sangat menarik detail yang Anda utarakan, salam telah mengunggah. “Saya tidak tahu apa yang bisa Anda katakan tentang hari di mana Anda telah melihat empat matahari terbenam yang indah.” oleh John Glenn.
Ya menyimpan ini bukanlah penentuan yang berisiko tinggi pos yang luar biasa! .
Oh my goodness! an incredible article dude. Thanks Nevertheless I am experiencing difficulty with ur rss . Don’t know why Unable to subscribe to it. Is there anybody getting identical rss drawback? Anybody who knows kindly respond. Thnkx
Good day very cool website!! Man .. Excellent .. Superb .. I will bookmark your website and take the feeds additionally…I am satisfied to find a lot of useful information here in the post, we want work out extra strategies on this regard, thank you for sharing.
I precisely needed to thank you so much yet again. I am not sure the things I would’ve made to happen in the absence of the entire tricks revealed by you about such concern. It actually was a intimidating condition in my circumstances, however , finding out the very skilled style you managed it made me to cry over joy. Now i am thankful for your guidance and thus believe you comprehend what a powerful job you’re accomplishing teaching people with the aid of a site. I am certain you have never got to know all of us.
The root of your writing whilst appearing reasonable originally, did not sit properly with me after some time. Somewhere throughout the paragraphs you actually were able to make me a believer but just for a very short while. I nevertheless have a problem with your jumps in logic and you might do well to help fill in all those gaps. In the event you can accomplish that, I will certainly end up being amazed.
I conceive this web site contains some real superb information for everyone. “Only the little people pay taxes.” by Leona Helmsly.
Utterly written content material, regards for entropy.
I think this is among the most important info for me. And i’m glad reading your article. But wanna remark on few general things, The website style is perfect, the articles is really excellent :D. Good job, cheers
There is noticeably a bundle to learn about this. I assume you made sure nice factors in features also.
I think other web-site proprietors should take this website as an model, very clean and magnificent user friendly style and design, as well as the content. You’re an expert in this topic!
Admiring the persistence you put into your website and in depth information you provide. It’s good to come across a blog every once in a while that isn’t the same out of date rehashed information. Wonderful read! I’ve saved your site and I’m adding your RSS feeds to my Google account.
Some really excellent information, Gladiola I detected this.
Very nice post. I just stumbled upon your weblog and wanted to say that I’ve truly enjoyed browsing your blog posts. In any case I’ll be subscribing to your feed and I hope you write again very soon!
You really make it seem so easy along with your presentation however I to find this topic to be really one thing that I feel I’d by no means understand. It seems too complex and extremely wide for me. I’m taking a look ahead to your next submit, I’ll attempt to get the cling of it!
After study just a few of the weblog posts on your web site now, and I actually like your approach of blogging. I bookmarked it to my bookmark web site listing and will likely be checking back soon. Pls take a look at my website as nicely and let me know what you think.
I like what you guys are up also. Such intelligent work and reporting! Carry on the excellent works guys I have incorporated you guys to my blogroll. I think it will improve the value of my web site 🙂
I am often to blogging and i really appreciate your content. The article has really peaks my interest. I am going to bookmark your site and keep checking for new information.
Lovely just what I was looking for.Thanks to the author for taking his clock time on this one.
Very interesting information!Perfect just what I was searching for!
Outstanding post however I was wanting to know if you could write a litte more on this topic? I’d be very thankful if you could elaborate a little bit further. Cheers!
Bersama dengan semua hal yang tampak sedang berkembang di dalam topik spesifik ini, pandangan Anda umumnya relatif menstimulasi. Di sisi lain, saya maaf, karena saya tidak dapat setuju sepenuhnya pada seluruh strategi Anda, meskipun menstimulasi. Terlihat bagi kami bahwa komentar Anda tidak sepenuhnya benar-benar tervalidasi dan pada kenyataannya Anda sendiri tidak sepenuhnya percaya diri terhadap pernyataan tersebut. Dalam hal apa pun saya menikmati membacanya.
Saya benar-benar senang menemukan situs internet ini di Bing, persis seperti yang saya cari : D pula sudah saya bookmark.
When I originally commented I clicked the -Notify me when new comments are added- checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove me from that service? Thanks!
I was just looking for this information for some time. After six hours of continuous Googleing, finally I got it in your web site. I wonder what is the lack of Google strategy that do not rank this kind of informative web sites in top of the list. Normally the top web sites are full of garbage.
Very nice post. I just stumbled upon your weblog and wished to say that I have really enjoyed browsing your blog posts. After all I’ll be subscribing to your feed and I hope you write again soon!
I’ve read a few good stuff here. Certainly worth bookmarking for revisiting. I wonder how so much effort you set to make this sort of fantastic informative site.
I’ve learn some excellent stuff here. Certainly value bookmarking for revisiting. I wonder how a lot attempt you place to create this type of wonderful informative site.
Valuable info. Lucky me I found your web site by chance, and I am surprised why this accident didn’t happened earlier! I bookmarked it.
Saya sangat puas menemukan situs ini di Bing, persis seperti yang saya telusuri : D juga sudah saya simpan ke bookmark.
Sangat menarik poin yang Anda amati, terima kasih telah mengunggah.
Hmm apakah ada orang lain yang menghadapi masalah dengan gambar di blog ini yang tidak mau dimuat? Saya mencoba mencari tahu apakah ini masalah di sisi saya atau blognya. Tanggapan apa pun akan sangat dihargai.
Wow! Ini mungkin salah satu blog paling membantu yang pernah kami temui tentang topik ini. Sebenarnya Hebat. Saya juga seorang spesialis dalam topik ini jadi saya dapat memahami usaha Anda.
Saya selamanya memikirkan hal ini, terima kasih telah mengunggah.
Terima kasih atas tulisan yang baik. Faktanya ini dulunya adalah sebuah konten hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita dapat tetap berkomunikasi?
Dead pent content, Really enjoyed examining.
Thanks for the sensible critique. Me & my neighbor were just preparing to do some research about this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such magnificent info being shared freely out there.
Thanks – Enjoyed this update, is there any way I can receive an email sent to me whenever there is a new post?
Some truly quality content on this site, saved to favorites.
As soon as I noticed this internet site I went on reddit to share some of the love with them.
But a smiling visitant here to share the love (:, btw outstanding layout.
Loving the information on this site, you have done outstanding job on the blog posts.
Great wordpress blog here.. It’s hard to find quality writing like yours these days. I really appreciate people like you! take care
Respect to website author, some superb selective information.
I reckon something genuinely special in this web site.
Can I just say what a relief to find someone who actually knows what theyre talking about on the internet. You definitely know how to bring an issue to light and make it important. More people need to read this and understand this side of the story. I cant believe youre not more popular because you definitely have the gift.
Great blog! Do you have any tips and hints for aspiring writers? I’m planning to start my own site soon but I’m a little lost on everything. Would you propose starting with a free platform like WordPress or go for a paid option? There are so many choices out there that I’m completely overwhelmed .. Any suggestions? Appreciate it!
I appreciate your piece of work, thankyou for all the great articles.
Today, I went to the beach front with my kids. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She placed the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is completely off topic but I had to tell someone!
It is truly a nice and helpful piece of info. I’m satisfied that you just shared this helpful information with us. Please keep us up to date like this. Thanks for sharing.
hello!,I like your writing very much! share we communicate more about your article on AOL? I need an expert on this area to solve my problem. May be that’s you! Looking forward to see you.
I really enjoy reading through on this site, it holds great blog posts.
Someone essentially lend a hand to make seriously posts I would state. That is the very first time I frequented your website page and up to now? I amazed with the analysis you made to create this actual submit amazing. Excellent process!
Have you ever considered about adding a little bit more than just your articles? I mean, what you say is important and everything. But just imagine if you added some great photos or videos to give your posts more, “pop”! Your content is excellent but with images and videos, this site could definitely be one of the best in its niche. Superb blog!
VpCyqoiduAtsPdxejxe
Thank you for the auspicious writeup. It in truth was once a leisure account it. Look advanced to far brought agreeable from you! By the way, how could we keep in touch?
Some genuinely interesting points you have written.Helped me a lot, just what I was searching for :D.
Terima kasih atas kritik yang masuk akal. Saya dan tetangga saya baru saja bersiap untuk melakukan beberapa riset tentang ini. Kami sempat mengambil buku dari perpustakaan lokal kami, tapi saya rasa saya belajar lebih banyak dari postingan ini. Saya benar-benar senang melihat informasi luar biasa dibagikan secara bebas.
Hore google adalah raja saya yang menolong saya menemukan web site yang luar biasa! .
Menakjubkan! Blog ini terlihat tepat seperti blog lama saya! Topiknya sangat berbeda tetapi memiliki layout halaman dan desain yang hampir sama. Pilihan warna yang luar biasa!
Menghargai waktu dan tenaga yang Anda curahkan ke blog Anda dan informasi mendalam yang Anda sajikan. Sangat hebat menemukan blog sesekali yang tidak berisi informasi lama yang diulang-ulang. Artikel yang hebat! Saya sudah menandai situs Anda dan memasukkan feed RSS Anda ke akun Google saya.
Saya tidak sungguh fantastis dalam bahasa Inggris tetapi saya menemukan ini sangat ringan untuk dibaca .
Terima kasih, saya baru-baru ini menelusuri informasi tentang subjek ini cukup lama dan milik Anda adalah yang terbaik yang saya temukan hingga sekarang. Namun, bagaimana dengan kesimpulan? Apakah Anda yakin tentang sumber tersebut?
Hari ini, saat saya sedang bekerja, sepupu saya mengambil iPad saya dan mengujinya apakah bisa bertahan dari jatuh setinggi 30 kaki, hanya agar dia bisa menjadi sensasi youtube. apple ipad saya sekarang rusak dan dia memiliki 83 penayangan. Saya tahu ini sepenuhnya di luar topik tetapi saya harus membagikannya kepada seseorang!
Bernilai info. Beruntung saya menemukan situs web Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak pernah terjadi lebih awal! Saya menandainya.
WONDERFUL Post.thanks for share..more wait .. …
I like this site very much, Its a really nice post to read and incur info . “Words are like leaves and where they most abound, Much fruit of sense beneath is rarely found.” by Alexander Pope.
I know this if off topic but I’m looking into starting my own weblog and was wondering what all is required to get setup? I’m assuming having a blog like yours would cost a pretty penny? I’m not very web savvy so I’m not 100 positive. Any recommendations or advice would be greatly appreciated. Many thanks
It is really a nice and useful piece of information. I’m glad that you shared this useful info with us. Please keep us informed like this. Thanks for sharing.
Hey, you used to write wonderful, but the last several posts have been kinda boring?K I miss your great writings. Past few posts are just a bit out of track! come on!
Ini adalah situs yang benar untuk siapa saja yang ingin mengetahui tentang topik ini. Anda memahami begitu banyak hal sehingga nyaris sulit untuk berdebat dengan Anda (bukan berarti saya benar-benar ingin…HaHa). Anda benar-benar membawa pendekatan baru pada topik yang telah ditulis selama bertahun-tahun. Luar biasa, benar-benar luar biasa!
I’m not sure where you are getting your info, but good topic. I needs to spend some time learning more or understanding more. Thanks for excellent information I was looking for this information for my mission.
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.
Wow, superb blog struktur! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Tampilan keseluruhan situs Anda luar biasa, serta materinya!
It’s a shame you don’t have a donate button! I’d most certainly donate to this excellent blog! I suppose for now i’ll settle for bookmarking and adding your RSS feed to my Google account. I look forward to brand new updates and will talk about this website with my Facebook group. Chat soon!
Bernilai info. Beruntung saya menemukan situs web Anda secara tidak sengaja, dan saya kaget mengapa kecelakaan ini tidak terjadi lebih awal! Saya menandainya.
Today, I went to the beach with my kids. I found a sea shell and gave it to my 4 year old daughter and said “You can hear the ocean if you put this to your ear.” She put the shell to her ear and screamed. There was a hermit crab inside and it pinched her ear. She never wants to go back! LoL I know this is completely off topic but I had to tell someone!
I love your blog.. very nice colors & theme. Did you create this website yourself? Plz reply back as I’m looking to create my own blog and would like to know wheere u got this from. thanks
I like this web blog very much, Its a really nice post to read and obtain info .
What i do not understood is actually how you are not really much more well-liked than you might be right now. You’re so intelligent. You realize therefore considerably relating to this subject, produced me personally consider it from numerous varied angles. Its like women and men aren’t fascinated unless it is one thing to do with Lady gaga! Your own stuffs excellent. Always maintain it up!
I was recommended this website by my cousin. I’m not sure whether this post is written by him as no one else know such detailed about my problem. You are incredible! Thanks!
Hey there just wanted to give you a quick heads up. The text in your article seem to be running off the screen in Opera. I’m not sure if this is a format issue or something to do with browser compatibility but I figured I’d post to let you know. The layout look great though! Hope you get the issue solved soon. Many thanks
Artikel yang luar biasa. Ini memberi saya gambaran yang lebih baik tentang topik ini. Teruskan pekerjaan yang hebat!
Very interesting topic, thank you for posting.
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Wow! Terima kasih! Saya terus-menerus membutuhkan menulis di website saya sesuatu seperti itu. Bolehkah saya menerapkan fragmen dari posting Anda ke website saya?
Hi, Neat post. There is a problem together with your website in web explorer, may check this… IE still is the market chief and a big element of other people will pass over your wonderful writing due to this problem.
Very fantastic visual appeal on this site, I’d rate it 10 10.
Sangat menarik informasi!Sempurna persis seperti yang saya cari!
Itu memang milik Anda! . Kita setidaknya perlu membuat orang-orang yang mengambil gambar ini mulai nge-blog! Mereka mungkin hanya melakukan pencarian gambar dan mengambilnya. Tapi tampilannya menarik!
Spot on with this write-up, I truly assume this website wants way more consideration. I’ll probably be once more to learn rather more, thanks for that info.
Halo semua, kamu sudah melakukan kerja yang mengagumkan. Saya tentu akan mem-bookmark ini dan kembali untuk membaca lebih banyak. Terima kasih banyak!
Biasanya saya tidak membaca artikel di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat artikel yang bagus.
you have a great blog here! would you like to make some invite posts on my blog?
I really prize your piece of work, Great post.
Saya selalu memikirkan hal ini, sangat dihargai telah mengunggah.
I wanted to thank you for this great read!! I definitely enjoying every little bit of it I have you bookmarked to check out new stuff you post…
You have mentioned very interesting details! ps decent internet site. “Where can I find a man governed by reason instead of habits and urges” by Kahlil Gibran.
Good day! Do you use Twitter? I’d like to follow you if that would be okay. I’m definitely enjoying your blog and look forward to new posts.
I enjoy your writing style really loving this web site.
Wonderful beat ! I wish to apprentice while you amend your web site, how can i subscribe for a blog website? The account aided me a acceptable deal. I had been tiny bit acquainted of this your broadcast offered bright clear concept
Ini benar-benar menyelesaikan masalah saya, terima kasih!
Hi , I do believe this is an excellent blog. I stumbled upon it on Yahoo , i will come back once again. Money and freedom is the best way to change, may you be rich and help other people.
I do not even know how I stopped up here, however I thought this publish was great. I don’t realize who you’re however certainly you are going to a well-known blogger should you are not already 😉 Cheers!
Ya menyimpan ini bukanlah kesimpulan yang buruk pos yang hebat! .
There are some fascinating closing dates on this article however I don’t know if I see all of them heart to heart. There’s some validity but I’ll take hold opinion till I look into it further. Good article , thanks and we would like more! Added to FeedBurner as effectively
Saya tidak biasanya berkomentar tetapi saya harus mengakui terima kasih untuk posting yang sempurna ini : D.
Terima kasih untuk situs informatif lainnya. Di tempat mana lagi saya bisa mendapatkan info seperti itu yang ditulis dengan metode yang ideal? Saya punya sebuah inisiatif yang saya sedang kerjakan sekarang, dan saya telah mengamati informasi seperti ini.
Sangat bagus website yang Anda miliki, tapi saya bertanya-tanya apakah Anda tahu papan pesan yang membahas topik yang sama seperti yang dibicarakan di artikel ini? Saya sangat ingin sekali menjadi bagian dari komunitas online di mana saya bisa mendapatkan tanggapan dari orang-orang yang berpengetahuan dengan minat yang sama. Jika Anda punya saran, mohon beri tahu saya. Cheers!
Artikel yang luar biasa. Ini jelas disusun dengan baik dan mudah dimengerti. Terima kasih telah berbagi informasi ini.
Seseorang secara esensial memberikan bantuan untuk membuat secara signifikan posting saya akan katakan. Itu adalah pertama kalinya saya mengunjungi halaman situs web Anda dan sampai saat ini? Saya terkejut dengan analisis yang Anda lakukan untuk menyusun posting istimewa ini. Aktivitas yang mengagumkan!
Isi yang fantastis! Gaya penulisan Anda jelas dan mudah dipahami. Saya tentu akan kembali untuk melihat konten lainnya.
Konten yang berguna dan ditulis dengan baik. Saya pasti akan membagikan ini kepada teman-teman. Terima kasih telah berbagi.
I went over this website and I conceive you have a lot of superb info, saved to my bookmarks (:.
I believe that is one of the so much important info for me. And i’m happy reading your article. However wanna statement on few common things, The web site style is great, the articles is actually nice :D. Good job, cheers
Great blog right here! Additionally your website rather a lot up fast! What host are you the use of? Can I get your associate hyperlink for your host? I desire my website loaded up as fast as yours lol
hello there and thank you for your information – I’ve definitely picked up something new from right here. I did however expertise a few technical issues using this web site, as I experienced to reload the website lots of times previous to I could get it to load correctly. I had been wondering if your web host is OK? Not that I’m complaining, but sluggish loading instances times will very frequently affect your placement in google and could damage your quality score if ads and marketing with Adwords. Anyway I am adding this RSS to my e-mail and can look out for a lot more of your respective fascinating content. Ensure that you update this again very soon..
Thanks for ones marvelous posting! I genuinely enjoyed reading it, you will be a great author.I will ensure that I bookmark your blog and will often come back sometime soon. I want to encourage yourself to continue your great work, have a nice weekend!
Hiya! I simply want to give a huge thumbs up for the nice data you have right here on this post. I can be coming again to your weblog for extra soon.
Would you be concerned about exchanging links?
I’d have to examine with you here. Which is not one thing I usually do! I take pleasure in reading a post that may make folks think. Additionally, thanks for permitting me to comment!
I really like reading and I conceive this website got some truly useful stuff on it! .
I don’t commonly comment but I gotta tell thanks for the post on this perfect one :D.
It is appropriate time to make some plans for the future and it’s time to be happy. I’ve read this post and if I could I want to suggest you some interesting things or suggestions. Maybe you can write next articles referring to this article. I want to read even more things about it!
Thank you for the good writeup. It in fact was a amusement account it. Look advanced to far added agreeable from you! However, how could we communicate?
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get several e-mails with the same comment. Is there any way you can remove people from that service? Thanks a lot!
Please let me know if you’re looking for a writer for your weblog. You have some really great posts and I feel I would be a good asset. If you ever want to take some of the load off, I’d love to write some material for your blog in exchange for a link back to mine. Please shoot me an email if interested. Kudos!
Saya melihat banyak website tetapi saya pikir yang satu ini mengandung sesuatu yang ekstra di dalamnya
Thank you for sharing excellent informations. Your website is so cool. I am impressed by the details that you’ve on this web site. It reveals how nicely you perceive this subject. Bookmarked this website page, will come back for extra articles. You, my friend, ROCK! I found just the information I already searched everywhere and simply couldn’t come across. What a great web-site.
Ini benar-benar menyelesaikan masalah saya, terima kasih!
I am always searching online for tips that can aid me. Thanks!
Saya umumnya tidak menulis komentar, tetapi yang ini benar-benar pantas. Isi yang hebat dan sangat membantu. Terima kasih telah meluangkan waktu untuk menulis ini.
Saya senang menjadi pengunjung dari web blog lengkap ini!, terima kasih atas informasi langka ini!
Hai, saya hanya ingin mengatakan bahwa saya benar-benar menikmati membaca postingan blog Anda. Ini merupakan tepat tipe informasi yang sedang saya cari. Saya akan merekomendasikan ini kepada teman-teman. Terima kasih banyak telah berbagi.
Terima kasih atas tulisan yang baik. Faktanya ini sebelumnya adalah sebuah materi hiburan. Terlihat maju menjadi lebih menyenangkan dari Anda! Namun, bagaimana kita bisa tetap berhubungan?
Anda bisa pasti melihat keahlian Anda di dalam karya yang Anda tulis. Dunia berharap ada lebih banyak lagi penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu ikuti hati Anda.
Umumnya saya tidak membaca posting di blog, tetapi saya ingin mengatakan bahwa tulisan ini benar-benar memaksa saya untuk melakukannya! Gaya penulisan Anda membuat saya terkesan. Terima kasih, sangat posting yang bagus.
Attractive component to content. I just stumbled upon your website and in accession capital to assert that I get in fact loved account your blog posts. Any way I’ll be subscribing for your feeds or even I achievement you get admission to consistently fast.
Saya senang menjadi pengunjung dari weblog paripurna ini!, terima kasih atas info langka ini!
Menikmati melihat ini, sangat bagus, salam.
Benar-benar bersih situs, salam untuk pos ini.
As a Newbie, I am constantly searching online for articles that can aid me. Thank you
Hey are using WordPress for your site platform? I’m new to the blog world but I’m trying to get started and create my own. Do you require any coding knowledge to make your own blog? Any help would be really appreciated!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya sangat singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
I will right away grab your rss as I can’t find your email subscription link or newsletter service. Do you’ve any? Please let me know so that I could subscribe. Thanks.
Ketika saya pertama kali berkomentar saya mencentang kotak -Beri tahu saya ketika umpan balik baru ditambahkan- dan sekarang setiap kali sebuah komentar ditambahkan saya menerima 4 email dengan komentar yang sama. Apakah ada pendekatan Anda bisa menghapus saya dari layanan itu? Terima kasih!
Saya setuju dengan semua ide yang Anda sajikan dalam posting Anda. Itu benar-benar meyakinkan dan pasti akan berhasil. Namun, postingnya terlalu singkat untuk pendatang baru. Bisakah Anda memperpanjangnya sedikit lagi mulai waktu berikutnya? Terima kasih atas postingnya.
Saya menghargainya, karena saya menemukan persis apa yang saya cari. Anda mengakhiri pencarian saya selama empat hari! Tuhan memberkati Anda. Semoga hari baik. Bye
Saya menemukan blog Anda di Google dan memeriksa beberapa posting awal Anda. Teruskan pekerjaan yang sangat baik ini. Saya baru saja menambahkan RSS feed Anda ke pembaca berita MSN saya. Menantikan untuk membaca lebih banyak dari Anda nanti!
Saya sering blogging dan saya sangat menghargai konten Anda. Artikel ini benar-benar menarik perhatian saya. Saya akan mem-bookmark situs Anda dan terus memeriksa informasi baru.
very nice put up, i actually love this website, carry on it
Saya amat gembira menemukan situs ini di Bing, persis seperti yang saya telusuri : D begitu juga sudah saya bookmark.
Anda bisa pasti melihat antusiasme Anda di dalam karya yang Anda tulis. Sektor berharap ada lebih banyak penulis penuh semangat seperti Anda yang tidak takut menyatakan apa yang mereka yakini. Selalu kejar hati Anda.
Wow, fantastis blog format! Sudah berapa lama Anda ngeblog? Anda membuat blogging terlihat mudah. Seluruh tampilan web site Anda luar biasa, belum lagi materinya!
Hore google adalah raja saya yang membantu saya menemukan situs yang luar biasa! .
I conceive other website proprietors should take this internet site as an example , very clean and good user genial pattern.
I gotta bookmark this web site it seems very beneficial invaluable
I just like the helpful information you provide to your articles. I will bookmark your weblog and check again here frequently. I’m fairly sure I will be told many new stuff proper right here! Best of luck for the next!
hi!,I like your writing so much! share we communicate more about your article on AOL? I need a specialist on this area to solve my problem. Maybe that’s you! Looking forward to see you.
Hello! I just wanted to ask if you ever have any issues with hackers? My last blog (wordpress) was hacked and I ended up losing a few months of hard work due to no data backup. Do you have any solutions to protect against hackers?
I would like to thank you for the efforts you’ve put in writing this web site. I am hoping the same high-grade web site post from you in the upcoming as well. Actually your creative writing skills has inspired me to get my own website now. Actually the blogging is spreading its wings quickly. Your write up is a great example of it.
Awesome blog! Do you have any hints for aspiring writers? I’m hoping to start my own site soon but I’m a little lost on everything. Would you recommend starting with a free platform like WordPress or go for a paid option? There are so many options out there that I’m completely overwhelmed .. Any recommendations? Thanks!
Wow! Thank you! I always needed to write on my site something like that. Can I include a fragment of your post to my website?
Saya tidak sering berkomentar tetapi saya harus menyatakan terima kasih untuk posting yang sempurna ini : D.
Saya selamanya memikirkan hal ini, sangat dihargai telah memposting.
I like reading and I conceive this website got some genuinely utilitarian stuff on it! .
I really enjoy examining on this site, it has good articles.
Perfect piece of work you have done, this internet site is really cool with wonderful information.
Great tremendous things here. I’m very glad to peer your post. Thank you so much and i am looking forward to touch you. Will you kindly drop me a mail?
Excellent post. I was checking constantly this blog and I’m impressed! Extremely helpful info specially the last part 🙂 I care for such information much. I was looking for this certain info for a very long time. Thank you and best of luck.
Rattling fantastic visual appeal on this internet site, I’d value it 10 10.
I keep listening to the news broadcast lecture about getting boundless online grant applications so I have been looking around for the most excellent site to get one. Could you advise me please, where could i acquire some?
I truly appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thx again
Hi there! This is my first visit to your blog! We are a collection of volunteers and starting a new initiative in a community in the same niche. Your blog provided us valuable information to work on. You have done a wonderful job!
Wonderful web site. Lots of useful info here. I am sending it to several buddies ans additionally sharing in delicious. And naturally, thank you on your sweat!
Very interesting info!Perfect just what I was looking for!
Nice post. I study one thing more difficult on completely different blogs everyday. It should at all times be stimulating to read content from other writers and follow somewhat one thing from their store. I’d choose to make use of some with the content on my blog whether or not you don’t mind. Natually I’ll provide you with a hyperlink in your web blog. Thanks for sharing.
Very interesting information!Perfect just what I was searching for!
Good day! I know this is kinda off topic however , I’d figured I’d ask. Would you be interested in trading links or maybe guest authoring a blog article or vice-versa? My website covers a lot of the same topics as yours and I feel we could greatly benefit from each other. If you are interested feel free to shoot me an e-mail. I look forward to hearing from you! Superb blog by the way!
Its like you read my mind! You appear to know so much about this, like you wrote the book in it or something. I think that you could do with some pics to drive the message home a little bit, but other than that, this is wonderful blog. A great read. I will certainly be back.
Very interesting information!Perfect just what I was looking for!
I’d should check with you here. Which isn’t something I usually do! I enjoy studying a publish that will make people think. Additionally, thanks for allowing me to comment!
Hi, Neat post. There is a problem with your site in internet explorer, would test this… IE still is the market leader and a large portion of people will miss your great writing because of this problem.
I visited a lot of website but I conceive this one has got something special in it in it
hi!,I like your writing very much! share we communicate more about your post on AOL? I require a specialist on this area to solve my problem. May be that’s you! Looking forward to see you.
Someone essentially help to make seriously posts I would state. This is the very first time I frequented your web page and thus far? I surprised with the research you made to make this particular publish extraordinary. Wonderful job!
Yeah bookmaking this wasn’t a bad conclusion outstanding post! .
I’m really impressed with your writing skills and also with the layout on your blog. Is this a paid theme or did you customize it yourself? Anyway keep up the excellent quality writing, it is rare to see a nice blog like this one these days..
You really make it seem so easy with your presentation but I find this matter to be actually something that I think I would never understand. It seems too complex and extremely broad for me. I’m looking forward for your next post, I will try to get the hang of it!
Hello, Neat post. There’s an issue with your site in internet explorer, could test this?K IE still is the marketplace chief and a big component of people will miss your fantastic writing due to this problem.
Hello! I just would like to give a huge thumbs up for the great info you have here on this post. I will be coming back to your blog for more soon.
I as well as my pals appeared to be taking note of the nice hints from your web page and then I got an awful suspicion I never expressed respect to you for those tips. The boys are already as a consequence stimulated to learn all of them and already have certainly been tapping into those things. Appreciation for really being so considerate as well as for choosing this kind of great resources millions of individuals are really eager to learn about. My very own honest apologies for not saying thanks to you earlier.
hello!,I like your writing so much! share we communicate more about your article on AOL? I require a specialist on this area to solve my problem. May be that’s you! Looking forward to see you.
Appreciate it for all your efforts that you have put in this. very interesting info .
Great post. I am facing a couple of these problems.
You can definitely see your enthusiasm within the work you write. The arena hopes for even more passionate writers such as you who are not afraid to say how they believe. Always follow your heart. “The most profound joy has more of gravity than of gaiety in it.” by Michel de Montaigne.
It’s appropriate time to make a few plans for the long run and it’s time to be happy. I’ve learn this publish and if I could I desire to recommend you few fascinating things or suggestions. Perhaps you can write next articles relating to this article. I want to read even more issues approximately it!
Hi, Neat post. There’s a problem with your website in internet explorer, would test this… IE still is the market leader and a huge portion of people will miss your excellent writing because of this problem.
I am impressed with this internet site, real I am a big fan .
Thanks , I’ve recently been searching for information about this subject for ages and yours is the best I’ve discovered till now. But, what about the bottom line? Are you sure about the source?
I conceive this web site has some really superb information for everyone : D.
Whoa! This blog looks exactly like my old one! It’s on a totally different subject but it has pretty much the same page layout and design. Great choice of colors!
Would you be excited about exchanging links?
Perfect work you have done, this site is really cool with superb info .
Dead written content, Really enjoyed looking at.
Somebody essentially help to make seriously articles I would state. This is the very first time I frequented your web page and thus far? I amazed with the research you made to create this particular publish incredible. Wonderful job!
Hello there! This is my first comment here so I just wanted to give a quick shout out and say I genuinely enjoy reading through your posts. Can you recommend any other blogs/websites/forums that deal with the same topics? Thanks a lot!
Thanks a lot for sharing this with all of us you actually know what you are talking about! Bookmarked. Please also visit my site =). We could have a link exchange contract between us!
An impressive share, I simply given this onto a colleague who was doing a bit analysis on this. And he in truth purchased me breakfast as a result of I found it for him.. smile. So let me reword that: Thnx for the deal with! But yeah Thnkx for spending the time to debate this, I feel strongly about it and love reading extra on this topic. If possible, as you turn into experience, would you thoughts updating your blog with extra details? It is highly helpful for me. Massive thumb up for this blog put up!
Wow, awesome blog layout! How long have you been blogging for? you made blogging look easy. The overall look of your site is wonderful, as well as the content!
I got what you mean , thankyou for posting.Woh I am delighted to find this website through google.
Hello my family member! I wish to say that this article is amazing, nice written and include almost all important infos. I’d like to peer extra posts like this.
Howdy just wanted to give you a quick heads up and let you know a few of the pictures aren’t loading properly. I’m not sure why but I think its a linking issue. I’ve tried it in two different web browsers and both show the same results.
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
An attention-grabbing dialogue is price comment. I feel that it is best to write extra on this topic, it won’t be a taboo topic however typically individuals are not enough to speak on such topics. To the next. Cheers
I always was concerned in this topic and stock still am, thankyou for posting.
Great work! This is the type of info that should be shared around the net. Shame on the search engines for not positioning this post higher! Come on over and visit my site . Thanks =)
I just could not leave your site before suggesting that I actually enjoyed the usual info a person supply on your guests? Is going to be again often in order to investigate cross-check new posts.
WONDERFUL Post.thanks for share..extra wait .. …
What’s Happening i’m new to this, I stumbled upon this I have found It absolutely useful and it has aided me out loads. I hope to contribute & aid other users like its aided me. Great job.
My brother suggested I might like this web site. He was entirely right. This post truly made my day. You cann’t imagine just how much time I had spent for this info! Thanks!
Good write-up, I am regular visitor of one¦s blog, maintain up the nice operate, and It is going to be a regular visitor for a lengthy time.
Great V I should definitely pronounce, impressed with your site. I had no trouble navigating through all tabs as well as related info ended up being truly easy to do to access. I recently found what I hoped for before you know it at all. Quite unusual. Is likely to appreciate it for those who add forums or something, web site theme . a tones way for your customer to communicate. Nice task..
I needed to put you this bit of word just to thank you so much yet again for all the pleasant tips you have featured in this article. This has been quite particularly open-handed with people like you to give publicly what exactly many people would have offered as an ebook to help with making some cash for their own end, most notably since you could possibly have tried it if you ever desired. Those principles as well acted as the fantastic way to know that some people have a similar passion much like my own to understand great deal more in terms of this issue. I’m certain there are lots of more fun occasions ahead for people who examine your blog.
My coder is trying to convince me to move to .net from PHP. I have always disliked the idea because of the expenses. But he’s tryiong none the less. I’ve been using Movable-type on numerous websites for about a year and am anxious about switching to another platform. I have heard very good things about blogengine.net. Is there a way I can import all my wordpress content into it? Any kind of help would be really appreciated!
You can certainly see your skills in the work you write. The world hopes for even more passionate writers like you who aren’t afraid to say how they believe. Always follow your heart.
I’m not sure exactly why but this website is loading incredibly slow for me. Is anyone else having this problem or is it a problem on my end? I’ll check back later and see if the problem still exists.
I do not even know how I ended up here, but I thought this post was great. I don’t know who you are but certainly you’re going to a famous blogger if you are not already 😉 Cheers!
I genuinely value your piece of work, Great post.
I like your writing style truly loving this web site.
This website is my inspiration , real good design and perfect content.
Does your site have a contact page? I’m having a tough time locating it but, I’d like to shoot you an email. I’ve got some creative ideas for your blog you might be interested in hearing. Either way, great site and I look forward to seeing it improve over time.
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
Do you mind if I quote a few of your posts as long as I provide credit and sources back to your webpage? My website is in the very same niche as yours and my users would genuinely benefit from some of the information you provide here. Please let me know if this ok with you. Thanks a lot!
I think you have mentioned some very interesting points, regards for the post.
Hiya, I am really glad I have found this information. Nowadays bloggers publish only about gossips and internet and this is really annoying. A good site with interesting content, this is what I need. Thank you for keeping this website, I’ll be visiting it. Do you do newsletters? Can not find it.
Have you ever thought about writing an e-book or guest authoring on other blogs? I have a blog based upon on the same topics you discuss and would really like to have you share some stories/information. I know my viewers would enjoy your work. If you are even remotely interested, feel free to shoot me an e-mail.
Hey there would you mind letting me know which web host you’re working with? I’ve loaded your blog in 3 completely different internet browsers and I must say this blog loads a lot quicker then most. Can you recommend a good hosting provider at a fair price? Thank you, I appreciate it!
Good post. I learn one thing more difficult on totally different blogs everyday. It will always be stimulating to read content from different writers and apply a little bit one thing from their store. I’d want to use some with the content material on my weblog whether you don’t mind. Natually I’ll offer you a hyperlink in your web blog. Thanks for sharing.
Merely wanna comment on few general things, The website pattern is perfect, the subject material is really wonderful. “Drop the question what tomorrow may bring, and count as profit every day that fate allows you.” by Horace.
I think other website owners should take this site as an model, very clean and good user friendly style and design.
Keep functioning ,splendid job!
I wanted to thank you for this great read!! I definitely enjoying every little bit of it I have you bookmarked to check out new stuff you post…
I have been browsing online more than 3 hours today, yet I never found any interesting article like yours. It’s pretty worth enough for me. In my view, if all website owners and bloggers made good content as you did, the net will be a lot more useful than ever before.
I actually wanted to construct a quick comment to be able to thank you for all of the fabulous suggestions you are writing at this site. My prolonged internet lookup has at the end of the day been rewarded with brilliant details to go over with my close friends. I ‘d assume that most of us visitors actually are extremely endowed to exist in a superb website with many outstanding people with helpful suggestions. I feel very lucky to have encountered the weblog and look forward to really more awesome moments reading here. Thanks once again for a lot of things.
Hi! Quick question that’s totally off topic. Do you know how to make your site mobile friendly? My website looks weird when browsing from my iphone. I’m trying to find a template or plugin that might be able to fix this problem. If you have any recommendations, please share. Cheers!
Hey there, You’ve done an incredible job. I will certainly digg it and personally suggest to my friends. I am confident they’ll be benefited from this web site.
I was curious if you ever thought of changing the page layout of your site? Its very well written; I love what youve got to say. But maybe you could a little more in the way of content so people could connect with it better. Youve got an awful lot of text for only having 1 or two pictures. Maybe you could space it out better?
I used to be very pleased to seek out this internet-site.I wished to thanks to your time for this glorious learn!! I undoubtedly having fun with each little bit of it and I’ve you bookmarked to take a look at new stuff you blog post.
I was more than happy to find this web-site.I needed to thanks for your time for this excellent read!! I definitely having fun with every little little bit of it and I’ve you bookmarked to check out new stuff you blog post.
Regards for helping out, fantastic information.
Good day! I know this is somewhat off topic but I was wondering which blog platform are you using for this website? I’m getting tired of WordPress because I’ve had issues with hackers and I’m looking at options for another platform. I would be fantastic if you could point me in the direction of a good platform.
I’m impressed, I have to say. Actually hardly ever do I encounter a blog that’s both educative and entertaining, and let me tell you, you’ve hit the nail on the head. Your thought is outstanding; the difficulty is one thing that not sufficient individuals are talking intelligently about. I am very blissful that I stumbled across this in my seek for one thing referring to this.
I have learn several excellent stuff here. Certainly worth bookmarking for revisiting. I surprise how so much effort you set to make this sort of excellent informative website.
You have noted very interesting details! ps decent internet site.
certainly like your web site however you have to test the spelling on quite a few of your posts. Many of them are rife with spelling issues and I to find it very bothersome to inform the reality then again I will surely come again again.
Great blog here! Also your web site loads up very fast! What web host are you using? Can I get your affiliate link to your host? I wish my web site loaded up as fast as yours lol
I was very pleased to find this web-site.I wanted to thanks for your time for this wonderful read!! I definitely enjoying every little bit of it and I have you bookmarked to check out new stuff you blog post.
Great paintings! This is the type of information that are meant to be shared around the net. Disgrace on the seek engines for now not positioning this put up upper! Come on over and consult with my site . Thank you =)
Whats Going down i am new to this, I stumbled upon this I’ve found It absolutely helpful and it has helped me out loads. I’m hoping to give a contribution & aid different users like its helped me. Great job.
Hey just wanted to give you a brief heads up and let you know a few of the pictures aren’t loading correctly. I’m not sure why but I think its a linking issue. I’ve tried it in two different browsers and both show the same results.
I got what you intend, appreciate it for posting.Woh I am happy to find this website through google.
Very informative and wonderful anatomical structure of articles, now that’s user genial (:.
This blog is definitely rather handy since I’m at the moment creating an internet floral website – although I am only starting out therefore it’s really fairly small, nothing like this site. Can link to a few of the posts here as they are quite. Thanks much. Zoey Olsen
I delight in, result in I found just what I used to be looking for. You have ended my four day lengthy hunt! God Bless you man. Have a nice day. Bye
Hi! This post could not be written any better! Reading through this post reminds me of my old room mate! He always kept talking about this. I will forward this article to him. Fairly certain he will have a good read. Thanks for sharing!
I simply could not depart your web site before suggesting that I really enjoyed the standard info a person provide on your guests? Is going to be back regularly to investigate cross-check new posts.
Good day very nice site!! Man .. Excellent .. Superb .. I’ll bookmark your website and take the feeds also…I am glad to find numerous helpful information here within the publish, we’d like work out more techniques on this regard, thank you for sharing.
Wow that was odd. I just wrote an very long comment but after I clicked submit my comment didn’t appear. Grrrr… well I’m not writing all that over again. Anyway, just wanted to say great blog!
You actually make it seem so easy with your presentation but I find this matter to be really something that I think I would never understand. It seems too complicated and extremely broad for me. I’m looking forward for your next post, I will try to get the hang of it!
Hey There. I found your blog using msn. This is an extremely well written article. I will be sure to bookmark it and come back to read more of your useful info. Thanks for the post. I will definitely return.
Hi , I do believe this is an excellent blog. I stumbled upon it on Yahoo , i will come back once again. Money and freedom is the best way to change, may you be rich and help other people.
I’ll immediately clutch your rss as I can not in finding your e-mail subscription link or e-newsletter service. Do you’ve any? Kindly permit me recognise in order that I could subscribe. Thanks.
Hiya! I know this is kinda off topic however I’d figured I’d ask. Would you be interested in trading links or maybe guest writing a blog post or vice-versa? My site covers a lot of the same topics as yours and I think we could greatly benefit from each other. If you might be interested feel free to send me an email. I look forward to hearing from you! Great blog by the way!
Hello! I just would like to give a huge thumbs up for the great info you have here on this post. I will be coming back to your blog for more soon.
Hey very nice web site!! Guy .. Beautiful .. Superb .. I will bookmark your site and take the feeds additionally…I’m glad to search out so many helpful information right here within the publish, we want develop more techniques on this regard, thanks for sharing. . . . . .
You made some first rate points there. I appeared on the web for the issue and located most individuals will associate with together with your website.
Hi there would you mind letting me know which web host you’re utilizing? I’ve loaded your blog in 3 completely different web browsers and I must say this blog loads a lot faster then most. Can you recommend a good web hosting provider at a reasonable price? Thanks, I appreciate it!
I’ve been browsing online more than 3 hours these days, yet I by no means discovered any interesting article like yours. It’s lovely worth sufficient for me. In my opinion, if all webmasters and bloggers made good content material as you did, the net might be a lot more helpful than ever before.
Thanks for all your efforts that you have put in this. very interesting information.
Thank you for the sensible critique. Me & my neighbor were just preparing to do some research about this. We got a grab a book from our area library but I think I learned more clear from this post. I am very glad to see such excellent info being shared freely out there.
I enjoy your writing style truly loving this website .
Good web site! I truly love how it is simple on my eyes and the data are well written. I am wondering how I might be notified when a new post has been made. I’ve subscribed to your RSS which must do the trick! Have a nice day!
Whats Going down i’m new to this, I stumbled upon this I’ve found It positively helpful and it has aided me out loads. I hope to contribute & help different users like its helped me. Good job.
Hello there, just became aware of your blog through Google, and found that it’s truly informative. I am gonna watch out for brussels. I will be grateful if you continue this in future. Many people will be benefited from your writing. Cheers!
I used to be very happy to find this internet-site.I wished to thanks in your time for this excellent learn!! I positively having fun with every little little bit of it and I’ve you bookmarked to take a look at new stuff you weblog post.
It¦s truly a great and useful piece of info. I am satisfied that you just shared this useful information with us. Please keep us up to date like this. Thank you for sharing.
I adore gathering utile info, this post has got me even more info! .
Some truly select posts on this internet site, saved to fav.
Nice post. I learn something more challenging on different blogs everyday. It will always be stimulating to read content from other writers and practice a little something from their store. I’d prefer to use some with the content on my blog whether you don’t mind. Natually I’ll give you a link on your web blog. Thanks for sharing.
Thanks for this tremendous post, I am glad I observed this internet site on yahoo.
The Bingo Plus app allows users to play bingo games directly on their smartphones with optimized touch controls and quick game rounds.
Some genuinely nice and useful info on this website, besides I think the style holds great features.
I like this site its a master peace ! Glad I noticed this on google .
It is really a nice and useful piece of information. I am happy that you simply shared this helpful info with us. Please stay us informed like this. Thank you for sharing.
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four e-mails with the same comment. Is there any way you can remove people from that service? Many thanks!
Very nice post. I just stumbled upon your blog and wanted to say that I have really enjoyed surfing around your blog posts. After all I will be subscribing to your rss feed and I hope you write again very soon!
I think this internet site has got very good indited content content.
I truly appreciate this post. I have been looking all over for this! Thank goodness I found it on Bing. You’ve made my day! Thanks again
Valuable info. Lucky me I found your web site by accident, and I am shocked why this accident didn’t happened earlier! I bookmarked it.
Thank you for any other informative website. The place else may just I am getting that kind of info written in such a perfect approach? I have a mission that I am simply now operating on, and I’ve been on the glance out for such info.
I was very happy to find this net-site.I wished to thanks in your time for this excellent learn!! I undoubtedly enjoying every little bit of it and I’ve you bookmarked to check out new stuff you blog post.
Fantastic blog! Do you have any helpful hints for aspiring writers? I’m hoping to start my own blog soon but I’m a little lost on everything. Would you advise starting with a free platform like WordPress or go for a paid option? There are so many choices out there that I’m totally confused .. Any suggestions? Thanks a lot!
Excellent post. I was checking constantly this weblog and I’m impressed! Extremely useful info particularly the final part 🙂 I deal with such information much. I was seeking this particular info for a very long time. Thank you and good luck.
Hello! I could have sworn I’ve been to this blog before but after browsing through some of the post I realized it’s new to me. Anyways, I’m definitely happy I found it and I’ll be book-marking and checking back frequently!
It’s arduous to seek out educated folks on this subject, but you sound like you recognize what you’re talking about! Thanks
We’re a group of volunteers and starting a new scheme in our community. Your website offered us with valuable info to work on. You have done an impressive job and our whole community will be thankful to you.
Very interesting subject , appreciate it for putting up.
I?¦m no longer certain the place you’re getting your information, however great topic. I needs to spend some time finding out much more or figuring out more. Thanks for magnificent info I was searching for this information for my mission.
What’s Happening i am new to this, I stumbled upon this I’ve found It absolutely helpful and it has helped me out loads. I am hoping to contribute & help different users like its aided me. Great job.
Have you ever thought about creating an ebook or guest authoring on other blogs? I have a blog based upon on the same information you discuss and would really like to have you share some stories/information. I know my viewers would value your work. If you are even remotely interested, feel free to send me an e-mail.
I went over this site and I think you have a lot of superb information, saved to favorites (:.
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
You actually make it seem so easy with your presentation but I find this topic to be really something that I think I would never understand. It seems too complex and very broad for me. I’m looking forward for your next post, I will try to get the hang of it!
As a Newbie, I am always searching online for articles that can benefit me. Thank you
I was looking through some of your articles on this site and I believe this internet site is really informative ! Keep posting.
I like this post, enjoyed this one regards for putting up. “To the dull mind all nature is leaden. To the illumined mind the whole world sparkles with light.” by Ralph Waldo Emerson.
Wonderful website. A lot of helpful information here. I am sending it to some buddies ans also sharing in delicious. And naturally, thanks in your sweat!
Hi there very cool site!! Man .. Excellent .. Wonderful .. I’ll bookmark your web site and take the feeds additionally?KI’m satisfied to seek out so many useful information here in the post, we want work out extra strategies in this regard, thanks for sharing. . . . . .
Nice weblog here! Additionally your site rather a lot up fast! What web host are you the use of? Can I get your affiliate link for your host? I desire my web site loaded up as quickly as yours lol
Oh my goodness! an incredible article dude. Thanks However I am experiencing situation with ur rss . Don’t know why Unable to subscribe to it. Is there anyone getting identical rss problem? Anyone who knows kindly respond. Thnkx
I would like to thnkx for the efforts you have put in writing this blog. I am hoping the same high-grade blog post from you in the upcoming as well. In fact your creative writing abilities has inspired me to get my own blog now. Really the blogging is spreading its wings quickly. Your write up is a good example of it.
What i don’t understood is in reality how you are now not really a lot more smartly-liked than you may be now. You’re very intelligent. You already know therefore significantly in relation to this matter, produced me individually believe it from a lot of numerous angles. Its like men and women aren’t interested except it?¦s something to accomplish with Lady gaga! Your individual stuffs excellent. Always maintain it up!
There are some attention-grabbing closing dates in this article but I don’t know if I see all of them center to heart. There may be some validity however I’ll take maintain opinion until I look into it further. Good article , thanks and we wish more! Added to FeedBurner as nicely
This is a very good tips especially to those new to blogosphere, brief and accurate information… Thanks for sharing this one. A must read article.
Hi there, You’ve performed a great job. I will certainly digg it and for my part suggest to my friends. I’m confident they will be benefited from this website.
I am incessantly thought about this, thanks for putting up.
very nice post, i certainly love this website, keep on it
Good web site! I really love how it is easy on my eyes and the data are well written. I am wondering how I might be notified when a new post has been made. I have subscribed to your RSS which must do the trick! Have a nice day!
I view something genuinely special in this site.
Your place is valueble for me. Thanks!…
I truly appreciate this post. I have been looking everywhere for this! Thank goodness I found it on Bing. You’ve made my day! Thanks again
I admire your work, appreciate it for all the interesting articles.
My wife and i were so peaceful that John managed to finish off his investigation by way of the precious recommendations he discovered in your weblog. It is now and again perplexing just to choose to be releasing tricks which some other people could have been making money from. We figure out we have got the writer to give thanks to because of that. The main explanations you’ve made, the straightforward blog menu, the friendships your site give support to foster – it’s got everything excellent, and it’s really aiding our son and the family recognize that the content is amusing, and that is extraordinarily fundamental. Many thanks for everything!
Precisely what I was searching for, thankyou for posting.
Spot on with this write-up, I actually suppose this website needs much more consideration. I’ll probably be again to learn way more, thanks for that info.
hey there and thanks for your info – I have certainly picked up anything new from right here. I did then again experience a few technical points the use of this web site, as I skilled to reload the website a lot of occasions prior to I may just get it to load properly. I had been pondering if your hosting is OK? Now not that I’m complaining, however sluggish loading instances occasions will very frequently have an effect on your placement in google and could damage your high-quality score if advertising and ***********|advertising|advertising|advertising and *********** with Adwords. Well I am adding this RSS to my email and could glance out for much extra of your respective fascinating content. Make sure you update this again soon..
I am glad to be a visitor of this utter weblog! , thanks for this rare information! .
I’ve been exploring for a little bit for any high-quality articles or blog posts on this kind of area . Exploring in Yahoo I at last stumbled upon this web site. Reading this information So i’m happy to convey that I’ve a very good uncanny feeling I discovered just what I needed. I most certainly will make certain to do not forget this web site and give it a glance on a constant basis.
Thanks for every other great article. The place else may just anybody get that kind of information in such a perfect way of writing? I’ve a presentation next week, and I am on the search for such info.
Great write-up, I¦m normal visitor of one¦s blog, maintain up the nice operate, and It’s going to be a regular visitor for a long time.
I truly enjoy studying on this website , it holds good blog posts. “Something unpredictable but in the end it’s right, I hope you have the time of your life.” by Greenday.
You made some decent points there. I appeared on the internet for the difficulty and found most individuals will go along with with your website.
I’m impressed, I must say. Really rarely do I encounter a weblog that’s both educative and entertaining, and let me tell you, you’ve hit the nail on the head. Your idea is excellent; the problem is something that not enough persons are speaking intelligently about. I am very happy that I stumbled throughout this in my search for one thing regarding this.
I together with my buddies have already been studying the great tips from the website and unexpectedly I had an awful suspicion I never thanked the website owner for those tips. The women were definitely as a consequence joyful to read through them and have sincerely been taking advantage of them. Thank you for turning out to be well accommodating as well as for making a choice on varieties of helpful resources millions of individuals are really needing to understand about. My personal honest regret for not expressing gratitude to sooner.
Hi there! This post couldn’t be written any better! Reading through this post reminds me of my previous room mate! He always kept talking about this. I will forward this article to him. Pretty sure he will have a good read. Thank you for sharing!
Heya i’m for the first time here. I came across this board and I find It really useful & it helped me out a lot. I hope to give something back and aid others like you helped me.
There is obviously a lot to know about this. I suppose you made certain nice points in features also.
Keep working ,fantastic job!
Hey There. I discovered your weblog the use of msn. That is an extremely well written article. I’ll make sure to bookmark it and return to learn more of your useful information. Thank you for the post. I will definitely return.
Valuable info. Lucky me I found your website by accident, and I am shocked why this accident did not happened earlier! I bookmarked it.
Magnificent web site. A lot of useful information here. I’m sending it to several friends ans also sharing in delicious. And obviously, thanks for your effort!
Howdy! Quick question that’s completely off topic. Do you know how to make your site mobile friendly? My weblog looks weird when browsing from my iphone4. I’m trying to find a theme or plugin that might be able to correct this issue. If you have any suggestions, please share. Cheers!
You could definitely see your skills in the paintings you write. The world hopes for more passionate writers such as you who are not afraid to mention how they believe. All the time follow your heart. “We may pass violets looking for roses. We may pass contentment looking for victory.” by Bern Williams.
I’ve recently started a blog, the information you provide on this website has helped me tremendously. Thank you for all of your time & work.
Write more, thats all I have to say. Literally, it seems as though you relied on the video to make your point. You definitely know what youre talking about, why waste your intelligence on just posting videos to your blog when you could be giving us something informative to read?
Hmm it looks like your site ate my first comment (it was extremely long) so I guess I’ll just sum it up what I wrote and say, I’m thoroughly enjoying your blog. I as well am an aspiring blog blogger but I’m still new to everything. Do you have any helpful hints for novice blog writers? I’d definitely appreciate it.
Wohh exactly what I was looking for, regards for putting up.
Thanks a bunch for sharing this with all of us you really know what you’re talking about! Bookmarked. Kindly also visit my web site =). We could have a link exchange arrangement between us!
I just couldn’t depart your site before suggesting that I extremely enjoyed the standard information an individual supply for your guests? Is gonna be again steadily in order to inspect new posts.
You made various nice points there. I did a search on the matter and found mainly persons will agree with your blog.
Hi my friend! I want to say that this post is amazing, great written and come with almost all vital infos. I’d like to see extra posts like this.
I haven’t checked in here for a while because I thought it was getting boring, but the last few posts are good quality so I guess I’ll add you back to my everyday bloglist. You deserve it my friend 🙂
I loved as much as you will receive carried out right here. The sketch is attractive, your authored material stylish. nonetheless, you command get got an nervousness over that you wish be delivering the following. unwell unquestionably come more formerly again since exactly the same nearly a lot often inside case you shield this hike.
Someone essentially help to make seriously posts I would state. This is the first time I frequented your web page and thus far? I amazed with the research you made to make this particular publish incredible. Excellent job!
Its like you learn my thoughts! You seem to grasp a lot approximately this, such as you wrote the guide in it or something. I feel that you simply can do with a few to pressure the message home a bit, but other than that, this is great blog. A fantastic read. I will definitely be back.
I get pleasure from, result in I found exactly what I was taking a look for. You’ve ended my four day lengthy hunt! God Bless you man. Have a great day. Bye
Helpful information. Lucky me I discovered your web site accidentally, and I’m shocked why this accident didn’t took place in advance! I bookmarked it.
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
Howdy! This post could not be written any better! Reading this post reminds me of my old room mate! He always kept chatting about this. I will forward this write-up to him. Fairly certain he will have a good read. Thanks for sharing!
Really superb info can be found on site. “The American temptation is to believe that foreign policy is a subdivision of psychiatry.” by Robert Francis Kennedy.
Regards for helping out, superb info. “Those who restrain desire, do so because theirs is weak enough to be restrained.” by William Blake.
Thank you for the sensible critique. Me & my neighbor were just preparing to do a little research on this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such fantastic information being shared freely out there.
This is the right blog for anyone who wants to find out about this topic. You realize so much its almost hard to argue with you (not that I actually would want…HaHa). You definitely put a new spin on a topic thats been written about for years. Great stuff, just great!
Hey there! This post couldn’t be written any better! Reading this post reminds me of my good old room mate! He always kept chatting about this. I will forward this write-up to him. Fairly certain he will have a good read. Thanks for sharing!
I got what you mean , regards for putting up.Woh I am thankful to find this website through google. “I would rather be a coward than brave because people hurt you when you are brave.” by E. M. Forster.
I think this is one of the such a lot important information for me. And i am glad reading your article. But wanna commentary on few basic things, The web site taste is wonderful, the articles is actually great : D. Excellent activity, cheers
Aw, this was a really nice post. In idea I want to put in writing like this moreover – taking time and actual effort to make a very good article… however what can I say… I procrastinate alot and in no way seem to get one thing done.
Some really wonderful info , Sword lily I observed this. “Carthago delenda est. (Carthage must be destroyed.)” by Marcius Porcius Cato.
Nice blog! Is your theme custom made or did you download it from somewhere? A design like yours with a few simple adjustements would really make my blog stand out. Please let me know where you got your theme. With thanks
It is really a great and useful piece of information. I am glad that you shared this useful info with us. Please keep us informed like this. Thank you for sharing.
Hi there just wanted to give you a quick heads up. The text in your content seem to be running off the screen in Chrome. I’m not sure if this is a format issue or something to do with internet browser compatibility but I thought I’d post to let you know. The design and style look great though! Hope you get the problem fixed soon. Many thanks
Deference to website author, some excellent selective information.
Well I definitely liked studying it. This information offered by you is very effective for good planning.
I will right away grab your rss feed as I can not find your e-mail subscription hyperlink or newsletter service. Do you have any? Please allow me realize in order that I may just subscribe. Thanks.
Utterly written written content, Really enjoyed studying.
A powerful share, I simply given this onto a colleague who was doing a bit analysis on this. And he in fact bought me breakfast because I found it for him.. smile. So let me reword that: Thnx for the deal with! But yeah Thnkx for spending the time to discuss this, I feel strongly about it and love reading extra on this topic. If attainable, as you grow to be expertise, would you thoughts updating your weblog with extra particulars? It’s highly helpful for me. Massive thumb up for this blog put up!
Wow! Thank you! I always wanted to write on my website something like that. Can I take a fragment of your post to my blog?
Sweet site, super layout, very clean and employ genial.
Thanks for sharing superb informations. Your site is so cool. I am impressed by the details that you?¦ve on this website. It reveals how nicely you perceive this subject. Bookmarked this website page, will come back for more articles. You, my friend, ROCK! I found simply the info I already searched all over the place and simply couldn’t come across. What a perfect website.
Some truly fantastic info , Gladiola I detected this. “Treat your friends as you do your pictures, and place them in their best light.” by Jennie Jerome Churchill.
I truly appreciate this post. I’ve been looking everywhere for this! Thank goodness I found it on Bing. You have made my day! Thx again
When I originally commented I clicked the “Notify me when new comments are added” checkbox and now each time a comment is added I get four emails with the same comment. Is there any way you can remove people from that service? Appreciate it!
This is a topic close to my heart cheers, where are your contact details though?
Hi my friend! I want to say that this post is amazing, great written and include almost all vital infos. I would like to peer extra posts like this .
whoah this blog is fantastic i really like studying your posts. Keep up the good work! You understand, lots of people are hunting round for this info, you can aid them greatly.
I am really impressed with your writing skills as well as with the layout on your blog. Is this a paid theme or did you modify it yourself? Either way keep up the excellent quality writing, it’s rare to see a great blog like this one these days..
Thanks for one’s marvelous posting! I genuinely enjoyed reading it, you’re a great author.I will make sure to bookmark your blog and may come back very soon. I want to encourage you continue your great job, have a nice weekend!
hello there and thank you on your information – I’ve certainly picked up anything new from right here. I did on the other hand expertise some technical points the usage of this web site, since I experienced to reload the site lots of occasions prior to I may get it to load properly. I have been thinking about in case your hosting is OK? Now not that I’m complaining, however slow loading cases occasions will sometimes affect your placement in google and could harm your quality score if advertising and ***********|advertising|advertising|advertising and *********** with Adwords. Well I am adding this RSS to my email and could glance out for a lot extra of your respective interesting content. Make sure you update this once more very soon..
I think this website contains very wonderful indited written content articles.
Hello There. I found your blog using msn. This is an extremely well written article. I’ll make sure to bookmark it and return to read more of your useful information. Thanks for the post. I will definitely return.
You have noted very interesting details! ps nice site. “Sutton lost 13 games in a row without winning a ballgame.” by Ralph Kiner.
Some really great blog posts on this internet site, appreciate it for contribution. “I finally know what distinguishes man from other beasts financial worries. – Journals” by Jules Renard.
Excellent weblog right here! Also your website quite a bit up very fast! What web host are you using? Can I am getting your associate hyperlink on your host? I want my website loaded up as fast as yours lol
A person essentially help to make seriously posts I would state. This is the very first time I frequented your web page and thus far? I surprised with the research you made to create this particular publish extraordinary. Wonderful job!
I gotta bookmark this site it seems extremely helpful invaluable
I want forgathering useful information , this post has got me even more info! .
Sweet site, super pattern, rattling clean and use pleasant.
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.
Great line up. We will be linking to this great article on our site. Keep up the good writing.
Have you ever thought about publishing an ebook or guest authoring on other blogs? I have a blog based upon on the same topics you discuss and would really like to have you share some stories/information. I know my readers would appreciate your work. If you’re even remotely interested, feel free to send me an e-mail.
rjgusLZAeJSUcyLyCdyYymX
Real wonderful information can be found on website.
I believe you have mentioned some very interesting details , regards for the post.
Spot on with this write-up, I truly assume this website needs way more consideration. I’ll in all probability be once more to read rather more, thanks for that info.
Good post and right to the point. I am not sure if this is in fact the best place to ask but do you folks have any ideea where to get some professional writers? Thanks 🙂
you are in point of fact a excellent webmaster. The site loading pace is incredible. It sort of feels that you’re doing any unique trick. Furthermore, The contents are masterwork. you have performed a magnificent activity on this topic!
I am continuously invstigating online for articles that can assist me. Thank you!
Some truly good information, Gladiolus I found this. “If you haven’t forgiven yourself something, how can you forgive others” by Dolores Huerta.
Excellent website you have here but I was wondering if you knew of any discussion boards that cover the same topics talked about in this article? I’d really like to be a part of online community where I can get suggestions from other experienced people that share the same interest. If you have any suggestions, please let me know. Thanks!
What’s Happening i’m new to this, I stumbled upon this I have found It positively helpful and it has aided me out loads. I hope to contribute & help other users like its aided me. Great job.
Good day! This is kind of off topic but I need some advice from an established blog. Is it hard to set up your own blog? I’m not very techincal but I can figure things out pretty quick. I’m thinking about making my own but I’m not sure where to begin. Do you have any tips or suggestions? With thanks
I like this web blog so much, bookmarked.
Hey! I could have sworn I’ve been to this blog before but after reading through some of the post I realized it’s new to me. Anyways, I’m definitely glad I found it and I’ll be bookmarking and checking back frequently!
Thanks for the sensible critique. Me & my neighbor were just preparing to do some research on this. We got a grab a book from our area library but I think I learned more clear from this post. I’m very glad to see such fantastic info being shared freely out there.
I was looking at some of your content on this website and I believe this website is rattling instructive! Retain putting up.
This site is mostly a walk-by means of for the entire info you wanted about this and didn’t know who to ask. Glimpse right here, and you’ll definitely discover it.
Thanks for sharing excellent informations. Your web site is very cool. I am impressed by the details that you have on this blog. It reveals how nicely you understand this subject. Bookmarked this website page, will come back for more articles. You, my pal, ROCK! I found simply the information I already searched everywhere and simply could not come across. What an ideal site.
Having read this I thought it was very informative. I appreciate you taking the time and effort to put this article together. I once again find myself spending way to much time both reading and commenting. But so what, it was still worth it!
You have noted very interesting details ! ps nice site.
Some really excellent information, Gladiolus I discovered this. “Love consists in this, that two solitudes protect and touch and greet each other.” by Rainer Maria Rilke.
I like what you guys are up also. Such smart work and reporting! Carry on the excellent works guys I’ve incorporated you guys to my blogroll. I think it’ll improve the value of my website :).
It’s really a great and helpful piece of information. I’m happy that you just shared this useful information with us. Please keep us up to date like this. Thanks for sharing.
Pretty nice post. I just stumbled upon your weblog and wished to say that I have truly enjoyed surfing around your blog posts. After all I’ll be subscribing to your feed and I hope you write again soon!
Hiya, I’m really glad I’ve found this info. Today bloggers publish just about gossips and net and this is actually annoying. A good site with exciting content, that’s what I need. Thank you for keeping this web-site, I will be visiting it. Do you do newsletters? Cant find it.
It’s laborious to search out educated folks on this matter, but you sound like you know what you’re talking about! Thanks
Wow, fantastic blog layout! How long have you been blogging for? you make blogging look easy. The overall look of your web site is fantastic, as well as the content!
whoah this blog is great i love reading your posts. Keep up the great work! You know, lots of people are looking around for this information, you can help them greatly.
I’ve been absent for some time, but now I remember why I used to love this site. Thanks , I will try and check back more often. How frequently you update your site?
I like this web blog so much, saved to my bookmarks. “American soldiers must be turned into lambs and eating them is tolerated.” by Muammar Qaddafi.
What’s Taking place i’m new to this, I stumbled upon this I’ve discovered It absolutely useful and it has aided me out loads. I am hoping to contribute & aid other customers like its helped me. Great job.
Hi! Quick question that’s completely off topic. Do you know how to make your site mobile friendly? My site looks weird when viewing from my apple iphone. I’m trying to find a theme or plugin that might be able to fix this issue. If you have any recommendations, please share. Many thanks!
Hello There. I found your weblog the use of msn. That is a really well written article. I’ll make sure to bookmark it and return to read extra of your useful info. Thanks for the post. I’ll certainly return.
I really like forgathering useful info, this post has got me even more info! .
I’ve been surfing on-line greater than 3 hours nowadays, but I never found any interesting article like yours. It?¦s lovely value enough for me. In my view, if all webmasters and bloggers made just right content material as you probably did, the internet will be much more helpful than ever before.
I just could not depart your site prior to suggesting that I actually loved the standard information an individual supply to your visitors? Is going to be again often to check up on new posts.
Woah! I’m really digging the template/theme of this site. It’s simple, yet effective. A lot of times it’s very difficult to get that “perfect balance” between user friendliness and visual appearance. I must say you’ve done a very good job with this. In addition, the blog loads very fast for me on Opera. Exceptional Blog!
Unquestionably consider that that you stated. Your favorite justification seemed to be at the internet the easiest factor to remember of. I say to you, I definitely get annoyed even as other people think about issues that they plainly don’t recognize about. You controlled to hit the nail upon the highest and defined out the whole thing without having side-effects , other folks could take a signal. Will likely be back to get more. Thank you
What¦s Taking place i’m new to this, I stumbled upon this I’ve found It absolutely helpful and it has helped me out loads. I’m hoping to give a contribution & help other users like its helped me. Good job.
Enjoyed examining this, very good stuff, regards. “It requires more courage to suffer than to die.” by Napoleon Bonaparte.
I wanted to post you the bit of observation to say thanks a lot once again considering the amazing techniques you have shared in this case. This has been really strangely open-handed with people like you to grant publicly exactly what a number of us could have made available as an electronic book to get some cash for their own end, most importantly given that you could possibly have tried it if you ever decided. Those principles as well acted to become a great way to recognize that other people online have the same eagerness similar to my personal own to see a great deal more in terms of this condition. Certainly there are some more pleasant instances up front for individuals who start reading your website.
I am continually invstigating online for tips that can benefit me. Thx!
After study a few of the weblog posts on your web site now, and I actually like your means of blogging. I bookmarked it to my bookmark website listing and might be checking back soon. Pls try my web page as properly and let me know what you think.
I like this internet site because so much utile stuff on here : D.
There are actually loads of particulars like that to take into consideration. That may be a nice point to deliver up. I offer the ideas above as basic inspiration but clearly there are questions like the one you carry up where a very powerful thing will be working in sincere good faith. I don?t know if finest practices have emerged around things like that, however I’m certain that your job is clearly recognized as a fair game. Each girls and boys really feel the impact of just a second’s pleasure, for the remainder of their lives.
Hi there, just became aware of your blog through Google, and found that it is truly informative. I am going to watch out for brussels. I’ll be grateful if you continue this in future. Numerous people will be benefited from your writing. Cheers!
Thanks a bunch for sharing this with all of us you really know what you are talking about! Bookmarked. Kindly also visit my website =). We could have a link exchange contract between us!
It’s in point of fact a nice and useful piece of information. I’m happy that you just shared this useful info with us. Please keep us up to date like this. Thanks for sharing.
I have recently started a website, the information you offer on this site has helped me tremendously. Thanks for all of your time & work.
I am curious to find out what blog platform you are working with? I’m experiencing some small security problems with my latest blog and I would like to find something more secure. Do you have any recommendations?
I like what you guys are up also. Such intelligent work and reporting! Carry on the excellent works guys I have incorporated you guys to my blogroll. I think it’ll improve the value of my site 🙂
Very good written article. It will be supportive to everyone who utilizes it, including yours truly :). Keep doing what you are doing – for sure i will check out more posts.
Outstanding post, I think website owners should acquire a lot from this weblog its real user genial.
Undeniably imagine that that you stated. Your favorite justification appeared to be at the web the easiest factor to consider of. I say to you, I certainly get annoyed while other folks think about issues that they plainly don’t recognize about. You controlled to hit the nail upon the highest as neatly as outlined out the whole thing without having side-effects , other people can take a signal. Will likely be back to get more. Thank you
I loved as much as you’ll receive carried out right here. The sketch is attractive, your authored subject matter stylish. nonetheless, you command get got an edginess over that you wish be delivering the following. unwell unquestionably come more formerly again as exactly the same nearly very often inside case you shield this hike.
What’s Happening i am new to this, I stumbled upon this I’ve found It absolutely useful and it has helped me out loads. I hope to contribute & assist other users like its helped me. Good job.
I’m still learning from you, while I’m making my way to the top as well. I absolutely love reading all that is posted on your website.Keep the aarticles coming. I enjoyed it!
It?¦s really a nice and helpful piece of information. I am satisfied that you simply shared this useful info with us. Please stay us informed like this. Thank you for sharing.
Hello there, I found your website via Google while searching for a related topic, your web site came up, it looks great. I have bookmarked it in my google bookmarks.
It is appropriate time to make a few plans for the longer term and it’s time to be happy. I’ve learn this submit and if I could I wish to suggest you few attention-grabbing issues or suggestions. Perhaps you could write subsequent articles referring to this article. I want to read even more things approximately it!
Hello! I just would like to give a huge thumbs up for the great info you have here on this post. I will be coming back to your blog for more soon.
I am not positive the place you are getting your information, however great topic. I must spend some time learning much more or figuring out more. Thank you for great information I was in search of this information for my mission.
I conceive other website proprietors should take this website as an model, very clean and good user genial layout.
Nice post. I study one thing tougher on different blogs everyday. It’s going to all the time be stimulating to learn content from different writers and practice somewhat one thing from their store. I’d want to use some with the content on my weblog whether you don’t mind. Natually I’ll provide you with a hyperlink on your net blog. Thanks for sharing.
Hello! Do you know if they make any plugins to protect against hackers? I’m kinda paranoid about losing everything I’ve worked hard on. Any recommendations?
Hi, just required you to know I he added your site to my Google bookmarks due to your layout. But seriously, I believe your internet site has 1 in the freshest theme I??ve came across. It extremely helps make reading your blog significantly easier.
I like what you guys are up too. Such intelligent work and reporting! Keep up the superb works guys I’ve incorporated you guys to my blogroll. I think it’ll improve the value of my site :).
I gotta bookmark this website it seems very helpful very beneficial
Good info and straight to the point. I am not sure if this is actually the best place to ask but do you folks have any ideea where to hire some professional writers? Thx 🙂
I am really impressed with your writing skills as well as with the layout on your weblog. Is this a paid theme or did you modify it yourself? Either way keep up the excellent quality writing, it is rare to see a great blog like this one these days..
I wish to show appreciation to the writer just for bailing me out of such a challenge. Because of checking through the online world and getting strategies which were not powerful, I figured my life was gone. Existing without the solutions to the issues you have sorted out all through your website is a crucial case, and those that might have badly damaged my entire career if I had not discovered the blog. Your primary knowledge and kindness in playing with the whole lot was very helpful. I am not sure what I would have done if I had not come across such a thing like this. I am able to at this point relish my future. Thanks for your time so much for the impressive and results-oriented help. I won’t hesitate to recommend your web page to any individual who should receive tips about this area.
As I site possessor I believe the content material here is rattling wonderful , appreciate it for your hard work. You should keep it up forever! Good Luck.
Thank you for the good writeup. It in fact was a amusement account it. Look advanced to more added agreeable from you! However, how could we communicate?
I enjoy your writing style genuinely enjoying this site.
Well I truly enjoyed studying it. This tip procured by you is very helpful for correct planning.
Good day! I know this is kind of off topic but I was wondering which blog platform are you using for this site? I’m getting sick and tired of WordPress because I’ve had issues with hackers and I’m looking at alternatives for another platform. I would be great if you could point me in the direction of a good platform.
As a Newbie, I am constantly searching online for articles that can help me. Thank you
Hi, i believe that i saw you visited my blog thus i came to “go back the choose”.I’m trying to to find issues to improve my website!I suppose its adequate to use some of your ideas!!
Its great as your other content : D, regards for putting up.
My brother suggested I would possibly like this web site. He used to be totally right. This put up truly made my day. You can not believe just how a lot time I had spent for this information! Thanks!
I discovered your blog site on google and check a few of your early posts. Continue to keep up the very good operate. I just additional up your RSS feed to my MSN News Reader. Seeking forward to reading more from you later on!…
Wow! This can be one particular of the most useful blogs We’ve ever arrive across on this subject. Basically Wonderful. I’m also an expert in this topic so I can understand your effort.
You made some nice points there. I did a search on the subject matter and found most persons will go along with with your website.
Hey! This post couldn’t be written any better! Reading this post reminds me of my previous room mate! He always kept chatting about this. I will forward this page to him. Pretty sure he will have a good read. Many thanks for sharing!
I have recently started a web site, the information you provide on this website has helped me tremendously. Thank you for all of your time & work.
Rattling good information can be found on website. “An executive is a person who always decides sometimes he decides correctly, but he always decides.” by John H. Patterson.
Youre so cool! I dont suppose Ive read anything like this before. So nice to search out someone with some authentic ideas on this subject. realy thank you for beginning this up. this web site is something that’s needed on the internet, somebody with somewhat originality. useful job for bringing one thing new to the internet!
I believe this web site has very good indited content content.
Some times its a pain in the ass to read what people wrote but this site is rattling user pleasant! .
There is noticeably a bundle to know about this. I assume you made certain nice points in features also.
hi!,I really like your writing very so much! percentage we keep up a correspondence extra approximately your post on AOL? I need an expert on this house to solve my problem. Maybe that’s you! Looking forward to peer you.
Hi would you mind letting me know which webhost you’re using? I’ve loaded your blog in 3 different internet browsers and I must say this blog loads a lot quicker then most. Can you suggest a good internet hosting provider at a reasonable price? Thanks a lot, I appreciate it!
Yeah bookmaking this wasn’t a bad conclusion great post! .
After all, what a great site and informative posts, I will upload inbound link – bookmark this web site? Regards, Reader.
Hi my family member! I wish to say that this article is awesome, nice written and include almost all significant infos. I¦d like to peer extra posts like this .
I’m not sure why but this web site is loading extremely slow for me. Is anyone else having this problem or is it a problem on my end? I’ll check back later and see if the problem still exists.
Thanks a lot for sharing this with all of us you actually know what you’re talking about! Bookmarked. Please also visit my website =). We could have a link exchange agreement between us!
Excellent blog here! Also your web site loads up very fast! What host are you using? Can I get your affiliate link to your host? I wish my website loaded up as fast as yours lol
I am glad to be a visitant of this gross weblog! , appreciate it for this rare info ! .
I really appreciate this post. I’ve been looking all over for this! Thank goodness I found it on Bing. You’ve made my day! Thx again
Its like you read my mind! You appear to know a lot about this, like you wrote the book in it or something. I think that you could do with a few pics to drive the message home a little bit, but instead of that, this is excellent blog. A fantastic read. I will certainly be back.
I’m extremely impressed with your writing skills as well as with the layout on your weblog. Is this a paid theme or did you customize it yourself? Anyway keep up the excellent quality writing, it is rare to see a nice blog like this one these days..
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
I’ve been browsing online more than 3 hours today, yet I never found any interesting article like yours. It’s pretty worth enough for me. In my opinion, if all website owners and bloggers made good content as you did, the net will be a lot more useful than ever before.
Thanks for this rattling post, I am glad I discovered this site on yahoo.
Nice post. I study something tougher on completely different blogs everyday. It can at all times be stimulating to read content from other writers and practice a little something from their store. I’d choose to make use of some with the content on my blog whether you don’t mind. Natually I’ll provide you with a hyperlink on your internet blog. Thanks for sharing.
Wow, superb blog format! How long have you been running a blog for? you made blogging glance easy. The entire look of your website is excellent, let alone the content!
The subsequent time I read a blog, I hope that it doesnt disappoint me as much as this one. I mean, I do know it was my choice to learn, however I actually thought youd have something attention-grabbing to say. All I hear is a bunch of whining about something that you possibly can fix if you happen to werent too busy searching for attention.
I’ve been browsing on-line greater than three hours nowadays, but I by no means discovered any interesting article like yours. It¦s pretty price enough for me. In my opinion, if all website owners and bloggers made excellent content material as you probably did, the internet can be much more useful than ever before.
Wow, marvelous blog structure! How long have you been blogging for? you made blogging glance easy. The whole glance of your website is excellent, as neatly as the content material!
Hello very nice website!! Guy .. Beautiful .. Amazing .. I’ll bookmark your site and take the feeds also…I’m satisfied to find numerous helpful information here in the publish, we want work out extra techniques on this regard, thanks for sharing.
I feel this is one of the so much important information for me. And i am glad reading your article. However should statement on some basic issues, The website taste is perfect, the articles is in point of fact great : D. Excellent job, cheers
What i don’t understood is in reality how you are not really a lot more well-preferred than you might be right now. You’re very intelligent. You know therefore significantly when it comes to this subject, made me in my opinion imagine it from so many various angles. Its like women and men are not involved unless it’s one thing to accomplish with Girl gaga! Your own stuffs great. At all times care for it up!
Hi there very cool web site!! Guy .. Beautiful .. Wonderful .. I’ll bookmark your web site and take the feeds additionally?KI’m satisfied to seek out so many useful info here within the put up, we need work out more strategies in this regard, thanks for sharing. . . . . .
This really answered my problem, thanks!
Hello there, You’ve performed a great job. I’ll certainly digg it and in my view recommend to my friends. I am confident they’ll be benefited from this web site.
I will right away grab your rss as I can not in finding your email subscription link or e-newsletter service. Do you have any? Please permit me recognize in order that I may subscribe. Thanks.
I actually wanted to compose a simple note to be able to appreciate you for some of the precious guidelines you are posting on this website. My time-consuming internet lookup has at the end been rewarded with really good details to share with my visitors. I would assume that many of us site visitors are very much blessed to exist in a perfect site with so many special individuals with insightful hints. I feel truly fortunate to have discovered your entire web site and look forward to tons of more cool moments reading here. Thank you once more for all the details.
Hi, Neat post. There is a problem with your website in internet explorer, would check this… IE still is the market leader and a large portion of people will miss your excellent writing because of this problem.
This is the precise weblog for anybody who wants to search out out about this topic. You realize a lot its virtually hard to argue with you (not that I actually would need…HaHa). You definitely put a brand new spin on a subject thats been written about for years. Nice stuff, just great!
Some really fantastic content on this internet site, appreciate it for contribution. “It is not often that someone comes along who is a true friend and a good writer.” by E. B. White.
Hi there very cool blog!! Man .. Beautiful .. Amazing .. I’ll bookmark your website and take the feeds additionally?KI am glad to search out a lot of useful info here in the publish, we need develop more techniques on this regard, thanks for sharing. . . . . .
You should take part in a contest for one of the best blogs on the web. I will recommend this site!
I am continually searching online for tips that can aid me. Thanks!
I am not very excellent with English but I get hold this really leisurely to interpret.
Once I initially commented I clicked the -Notify me when new feedback are added- checkbox and now every time a remark is added I get 4 emails with the same comment. Is there any approach you can take away me from that service? Thanks!