Sweat, Cycles & Sugar Levels: Navigating T1D Through Your Menstrual Cycle
D-Coding the article : Type 1 Diabetes and the Menstrual Cycle: Where/How Does Exercise Fit in?
Published Date:
4 February 2023
Published By:
Saru Toor, Jane E Yardley, Zeinab Momeni
Approved By:
To be
Decoded By:
Asra H. Ahmed
MBA, PGCE in Assessment Learning disability, Head of Education at The Diabesties Foundation.
5 mins to read
- The T1D Takeaway
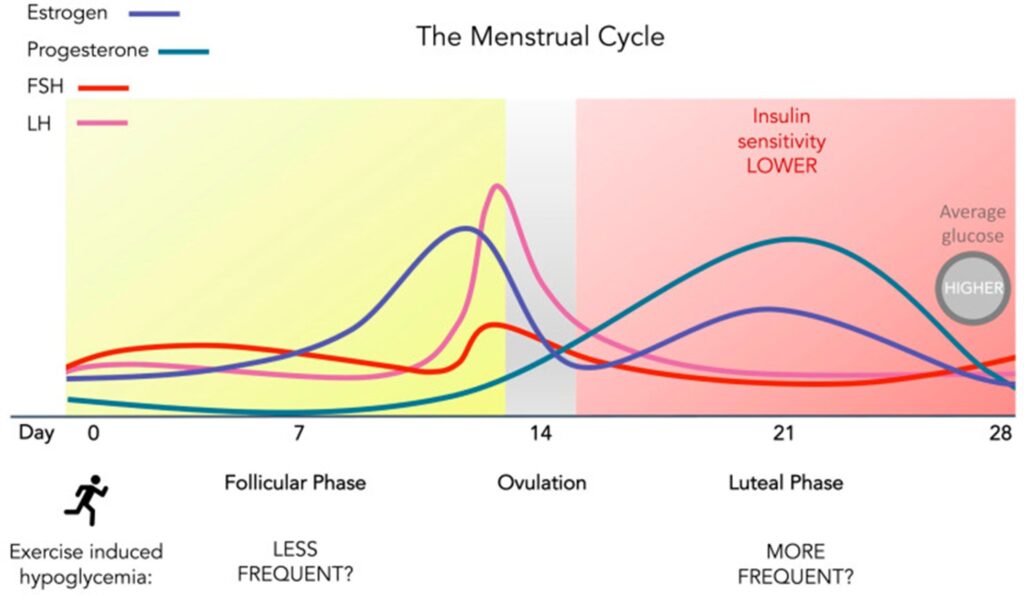
- Many people with type 1 diabetes notice glucose runs higher and insulin feels “weaker” in the second half of the cycle (after ovulation), but it varies a lot person to person. Ovulation is when the ovary releases an egg, usually mid-cycle.
- Because exercise can lower glucose during and for hours after activity, cycle phase can change whether you need a snack or an insulin tweak. Use your CGM plus a period tracker for 2–3 cycles to spot your pattern, then plan workouts, snacks, and insulin adjustments with your diabetes team.
- If you’re taking more insulin after ovulation, be extra cautious with exercise—lows can show up later the same day or overnight.
Word Wizard
- Exercise is strongly beneficial in T1D, but fear of lows is a major barrier—cycle-related glucose shifts can add another variability.
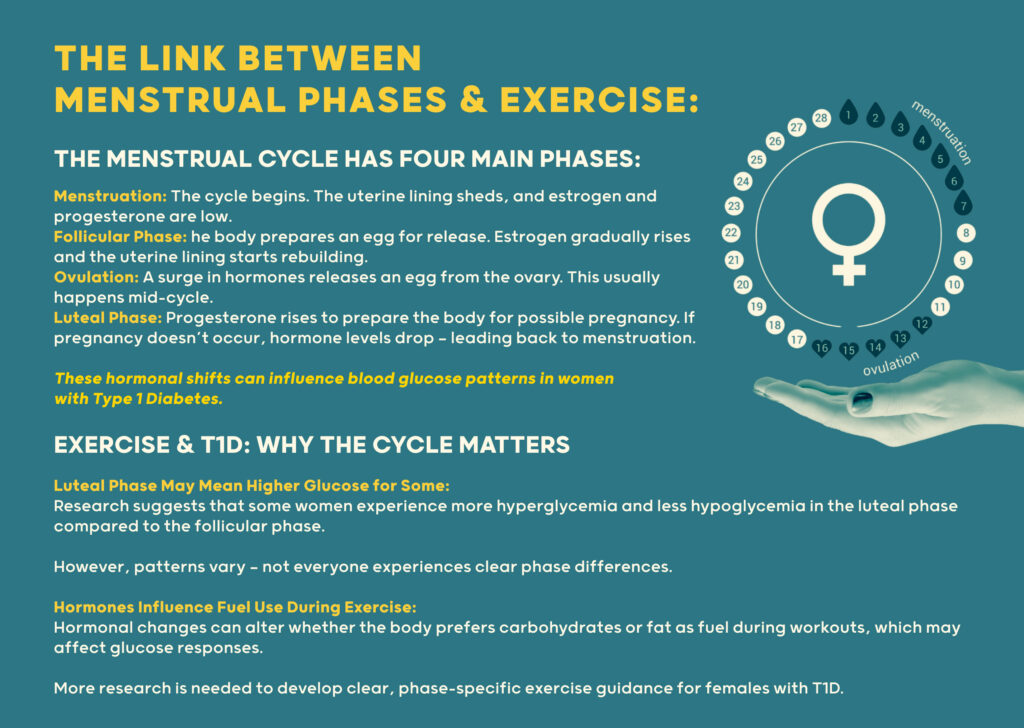
- Evidence suggests some women have more hyperglycemia and less hypoglycemia in the luteal phase compared with follicular phase.
- Not everyone shows the same pattern—some studies find little/no phase difference.
- Hormones can affect which fuel your body uses (carbs vs fat) during exercise, which may influence glucose responses.
- More research is needed to build clear, phase-specific exercise guidance for females with T1D.
Summary Snap
Shots
This narrative review pulls together what’s known about how menstrual-cycle hormones may affect glucose patterns and exercise responses in females living with T1D. A common theme is reduced insulin sensitivity and higher glucose in the luteal phase for some people, but findings are mixed and highly individual. Tracking personal patterns can help reduce exercise anxiety and improve safety.
Prime Insight
The paper explains the hormonal rhythm of the menstrual cycle (follicular, ovulatory, luteal) and reviews evidence on how these phases may influence insulin sensitivity, glucose trends, and fuel use during exercise.
The menstrual cycle can change how well insulin works because hormones rise and fall during the month. Many people with type 1 diabetes notice higher glucose and need more insulin in the second half of their cycle (after ovulation).
Exercise can lower glucose during activity and for hours after, and it can make your body more sensitive to insulin.
Same workout, different week of your cycle, your glucose response might change. Track the pattern, not the blame.

The authors say we still don’t have enough strong research, and we need more studies so exercise advice can be better designed for females living with type 1 diabetes.
This pattern is different for each person and can change from one month to the next. Many people with type 1 diabetes notice higher glucose and need more insulin in the second half of their cycle (after ovulation). This pattern is different for each person and can change from one month to the next.
Cycle phases can shift insulin sensitivity and glucose trends—often higher glucose in luteal phase, but not universal. If luteal phase brings higher glucose, it may reduce risk of exercise-related lows for some—but adjustments (like extra insulin) can swing risk back toward lows.
Practical best practice right now: individualized strategies based on CGM data, cycle tracking, workout type/intensity, and timing of insulin/food.
- A Deeper Dive
- The Sources Voice
The authors argue that better understanding menstrual-cycle effects could reduce exercise barriers in females with T1D and help create more informed exercise guidance.
- Curiosities Clarified
Progesterone is higher in the luteal phase and is linked with lower insulin sensitivity in many people.
Not always. If you take extra insulin to correct highs, the extra insulin during exercise can increase low risk.
Track cycle days + CGM + insulin/food/exercise for a few cycles, then build a personal plan with your clinician/educator.